Advocacy &Drug Quality &Invest in Malaria Control &IPTp &Malaria in Pregnancy &Treatment Bill Brieger | 22 Apr 2015
World Malaria Day 2015 Blog Postings Help #DefeatMalaria
 A special World Malaria Day 2015 Blog has been established. So far nine postings are available at http://www.worldmalariaday.org/blog. Please read and share with colleagues.
A special World Malaria Day 2015 Blog has been established. So far nine postings are available at http://www.worldmalariaday.org/blog. Please read and share with colleagues.
1. “Investing in integrated health services to defeat malaria”BY ELAINE ROMAN, MCSP Malaria Team Lead.
2. “Fake antimalarials: how big is the problem?”
BY DÉBORA MIRANDA, Technical Communications Officer, ACT Consortium (UK).
3. “Why antimalarial medicines matter”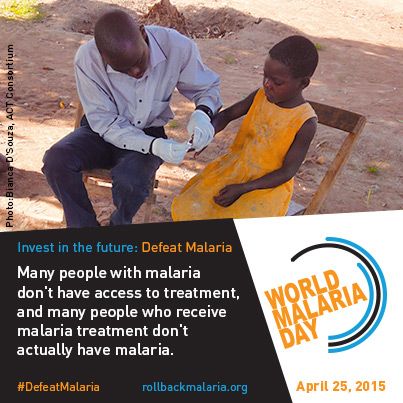
BY PROFESSOR PAUL NEWTON AND ANDREA STEWART, Worldwide Antimalarial Resistance Network and Laos Oxford University Mahosot Hospital Wellcome Trust Research Unit.
4. “Malaria as an entry point for addressing other conditions”
BY HELEN COUNIHAN, Senior Public Health Specialist, Community Health Systems.
5. “Bridging the Care-Seeking Gap with ProAct”
BY MATT McLAUGHLIN, Program Manager of Peace Corps Stomping Out Malaria in Africa initiative.
 6. “Defeating Malaria in Pregnancy”
6. “Defeating Malaria in Pregnancy”
BY CATHERINE NDUNGU, ELAINE ROMAN AND AUGUSTINE NGINDU, Jhpiego.
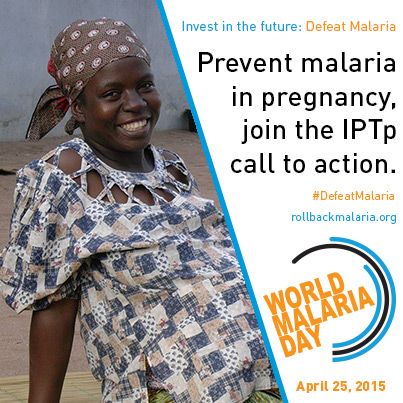
7. “Intermittent Preventive Treatment, a Key Tool to Prevent and Control Malaria in Pregnancy”
BY CLARA MENÉNDEZ, Director of ISGlobal’s Maternal Child and Reproductive Health Initiative.
8. “Widespread artemisinin resistance could wipe out a decade of malaria investment”
BY TIM FRANCE, Asia Pacific Leaders Malaria Alliance.
9. “The long walk to a malaria-free world”
BY DAVID REDDY, CEO Medicines for Malaria Venture.
Invest in Malaria Control &IRS &Malaria in Pregnancy Bill Brieger | 15 Apr 2015
Investing in Antenatal Care to Defeat Malaria
For many years malaria in pregnancy (MIP) was the proverbial neglected step-child of malaria control programs. Partly this was due to structural problems – the challenge of coordination between different units and departments within a ministry of health – malaria programs and reproductive health programs in separate and parallel divisions.
Another reason for neglect may lie in the fact that it is been difficult to achieve the MDG 5 as outlined in the United Nations’ 2014 Millennium Development Goals Report. One still finds that worldwide, almost 300,000 women died in 2013 from causes related to pregnancy and childbirth. Maternal death is mostly preventable and much more needs to be done to provide care to pregnant women.
Maternal death prevention includes providing pregnant women 3 or more doses of sulphadoxine-pyrimethamine (SP) for intermittent preventive treatment in pregnancy (IPTp) and ensuring women have AND sleep under insecticide treated bednets (ITNs) during antenatal care (ANC). Unfortunately recent Demographic and Health Surveys (DHS) and Malaria Information Surveys (MIS) from endemic countries show slow or stagnating progress in reaching Roll Back Malaria goals of 80% coverage of pregnant women with these interventions. Recent DHS/MIS have found that only 15% of recently pregnant women got two doses of IPTp in Nigeria, with only slightly better coverage in Burkina Faso (46%). Now that targets have shifted to three or more doses, the coverage challenge is even greater.
 The irony is that these same DHS reports show that a large proportion (>90%) of pregnant women in malaria endemic countries of Africa get registered for ANC. In order to achieve full coverage of IPTp pregnant women should attend ANC at least four times, but the recommended minimum of four ANC visits is difficult to achieve. According to WHO, “The proportion of pregnant women in developing countries who attended at least four antenatal care visit has increased from approximately 37% in 1990 to about 52% in 2012 but, in low-income countries, only 38% of pregnant women attended four times or more antenatal care during 2006-2013.”
The irony is that these same DHS reports show that a large proportion (>90%) of pregnant women in malaria endemic countries of Africa get registered for ANC. In order to achieve full coverage of IPTp pregnant women should attend ANC at least four times, but the recommended minimum of four ANC visits is difficult to achieve. According to WHO, “The proportion of pregnant women in developing countries who attended at least four antenatal care visit has increased from approximately 37% in 1990 to about 52% in 2012 but, in low-income countries, only 38% of pregnant women attended four times or more antenatal care during 2006-2013.”
In their article, “The quality–coverage gap in antenatal care: toward better measurement of effective coverage,” Stephen Hodgins and Alexis D’Agostino offer an explanation. They point out that it is not the number of ANC contacts alone that matters; it is the content of each visit that is equally important. They explain that a “coverage gap” exists when women who attended ANC four or more times did not receive the elements of basic package of services spelled out in the concept of Focused Antenatal Care (FANC).
Specific findings from Hodgins and D’Agostino’s DHS review showed that, “Blood pressure and tetanus toxoid performed best, with median quality–coverage gaps of 5% and 18%, respectively. The greatest gaps were for iron–folate supplementation (72%) and malaria prevention (86%).” Simply put, the lesson is that attending ANC does not equal receiving lifesaving maternal health services.
Many factors affect the quality of ANC services ranging from the major gaps in availability of trained health workers at the frontline in endemic countries to poor procurement and supply systems for even the cheapest drugs like SP. Even when health workers are in place, their understanding of and attitudes toward using SP for IPTp may be inadequate. These issues are where the gap between attending ANC and receiving needed services emerges. We will not be able to defeat malaria in pregnancy until we invest in strengthening the whole ANC system and pay better attention of women’s health.
ITNs &Malaria in Pregnancy Bill Brieger | 12 Apr 2015
RBM Consensus: Continuous Distribution of Long-Lasting Insecticidal Nets in Africa through Antenatal and Immunization Services
 This statement is issued by the Roll Back Malaria (RBM) Partnership Working Groups on Malaria in Pregnancy and Vector Control, together with the Alliance for Malaria Prevention. Our aim is to appeal for more complete implementation of the WHO Recommendations for Achieving Universal Coverage With Long-Lasting Insecticidal Nets in Malaria Control (released September 2013, revised March 2014) [1]. In particular we wish to draw attention to this recommendation regarding long-lasting insecticidal nets (LLINs): “Continuous distribution channels should be functional before, during, and after the mass distribution campaigns to avoid any gaps in universal access to LLINs”.
This statement is issued by the Roll Back Malaria (RBM) Partnership Working Groups on Malaria in Pregnancy and Vector Control, together with the Alliance for Malaria Prevention. Our aim is to appeal for more complete implementation of the WHO Recommendations for Achieving Universal Coverage With Long-Lasting Insecticidal Nets in Malaria Control (released September 2013, revised March 2014) [1]. In particular we wish to draw attention to this recommendation regarding long-lasting insecticidal nets (LLINs): “Continuous distribution channels should be functional before, during, and after the mass distribution campaigns to avoid any gaps in universal access to LLINs”.
Rationale
 In most settings, pregnant women, infants and children under 5 years of age are at considerably higher risk of contracting malaria and developing severe disease than the general population. In sub- Saharan Africa, up to 90 percent of deaths due to malaria occur in infants and children under age 5. LLINs together with effective case management and intermittent preventive treatment in pregnancy (IPTp) are essential interventions for these vulnerable populations.
In most settings, pregnant women, infants and children under 5 years of age are at considerably higher risk of contracting malaria and developing severe disease than the general population. In sub- Saharan Africa, up to 90 percent of deaths due to malaria occur in infants and children under age 5. LLINs together with effective case management and intermittent preventive treatment in pregnancy (IPTp) are essential interventions for these vulnerable populations.
Antenatal care (ANC) and childhood vaccination clinics (i.e. those implementing the Expanded Program on Immunization, or EPI) offer effective channels for continuous distribution of LLINs since these provide a venue for structured visits targeting pregnant women, infants and young children. The use of ANC and EPI clinics for this purpose is further supported by the following considerations:
- In most countries a large proportion of pregnant women attend ANC at least
- EPI is one of the most equitable programs in child health, with high coverage globally.
- Availability of LLINs in ANC and EPI sessions provides an incentive to attend and thus improves coverage of ANC and
- Visits to ANC and immunization sessions are key opportunities for counseling pregnant women and mothers to promote the use of LLINs by pregnant women, infants and young
Other LLIN distribution channels may also offer good opportunities for achieving and maintaining universal coverage in addition to mass campaigns [1]. Each national malaria control program should develop its own LLIN distribution strategy that includes both mass distribution and continuous distribution channels, based on an analysis of the context of its local opportunities and constraints, and then document this in the national strategic plan. Program planning and implementation of continuous LLIN distribution should be conducted under the leadership of the national malaria control program, in conjunction with maternal health and EPI programs, as appropriate. Program implementers have an opportunity to reinforce counseling on the use of LLINs at ANC and immunization services.
Challenge
Some countries are faced with the challenge of insufficient LLIN stocks. Reports from several countries indicate that LLINs have been reallocated from ANC/EPI services to mass campaigns, as a means of compensating for shortfalls in stocks. However, we are concerned about this practice in the absence of an analysis of the impact on LLIN coverage of vulnerable groups. All possible efforts must be made to achieve or maintain universal coverage and, in the absence of sufficient LLINs, to avoid compromising coverage of vulnerable groups. Recognizing that intermittent mass campaigns are essential to maintaining high levels of coverage, and acknowledging that there may be disruption of routine systems during mass campaigns, every effort should be made to minimize these disruptions. The potential reallocation of LLINs from routine distribution channels to mass campaigns must be informed by local data indicating that this will not compromise protection of vulnerable groups such as pregnant women, infants and children under 5 years of age.
Action
The RBM Working Groups and the Alliance for Malaria Prevention therefore strongly urge national program managers responsible for malaria control, ANC and immunization services, and all health professionals concerned with these services, to heed and rapidly implement the WHO recommendations, which indicate that in addition to mass campaigns, a high priority should also be given to continuous distribution of LLINs during and after mass campaigns – such as through ANC, EPI services, and mother and child health weeks/months campaigns, as appropriate to the local context [1].
Reference
1. WHO recommendations for achieving universal coverage with long-lasting insecticidal nets in malaria control. Geneva: World Health Organization, Global Malaria Programme; 2013 (revised March 2014). Available from: http://www.who.int/malaria/publications/atoz/who_recommendation_coverage_llin/en/
This statement was developed among the following Partners:

IPTp &Malaria in Pregnancy Bill Brieger | 11 Apr 2015
RBM Consensus Statement on Folic Acid Supplementation During Pregnancy
 The Roll Back Malaria (RBM) Partnership Malaria in Pregnancy Working Group supports the following for all pregnant women living in sub-Saharan Africa:
The Roll Back Malaria (RBM) Partnership Malaria in Pregnancy Working Group supports the following for all pregnant women living in sub-Saharan Africa:
In malaria-endemic areas, intermittent preventive treatment using sulfadoxine-pyrimethamine (IPTp-SP) should be provided to pregnant women at each scheduled antenatal care (ANC) visit for protection against malaria. This should start early in the second trimester and continue until the time of delivery, with the doses given at least one month apart [1].
- IPTp-SP has been shown to reduce maternal anemia, antenatal maternal parasitemia, low birthweight infants and neonatal deaths.
- Co-trimoxazole provides some protection through its antimalarial activity; however, IPTp-SP should NOT be given to women who are taking daily co-trimoxazole prophylaxis (i.e. mainly those living with HIV) as this increases the risk of adverse event
Daily oral supplementation of 30–60 mg elemental iron and 400 µg (0.4 mg) folic acid should be provided as early as possible in pregnancy to meet iron and folic acid requirements [2]. In cases where a combined folic acid–iron tablet is not available, a daily dose of 400 µg (0.4 mg) folic acid can be used separately.
There is evidence that high doses of folic acid (i.e. 5,000 µg or more) may interfere with the efficacy of sulfadoxine-pyrimethamine as an antimalarial [3]. The higher 5,000 µg (5 mg) dose for pregnant women should be restricted for use in very specific clinical cases.
High doses of folic acid are not needed during low-risk pregnancies and may counteract the efficacy of both sulfadoxine-pyrimethamine and co-trimoxazole as antimalarials [4]. The RBM Malaria in Pregnancy Working Group strongly advises that countries currently prioritize the procurement and distribution of the available combined dose of 400 µg (0.4 mg) folic acid plus 30–60 mg elemental iron (The current iron and folic acid preparation is 400 ?g (0.4 mg) of folic acid plus 60 mg of elemental iron) as part of routine ANC. It also recommends that countries substantially reduce current stores and supplies of folic acid at a dose of 5,000 µg (5 mg) or higher at all facilities, as this dose should only be used for specific medical conditions as outlined by the World Health Organization (WHO) [2]
References:
- Policy brief for the implementation of intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine (IPTp-SP). Geneva: World Health Organization; 20
- Guideline: daily iron and folic acid supplementation in pregnant w Geneva: World Health Organization; 2012.
- Peters PJ, Thigpen MC, Parise ME, Newman RD. Safety and toxicity of sulfadoxine-pyrimethamine: implications for malaria prevention in pregnancy using intermittent preventive Drug Saf. 2007 June; 30(6):481–501.
- Cotrimoxazole (Septrin) [Internet]. NAM Aidsmap; 2015. Available from: http://www.aidsmap.com/Cotrimoxazole-iSeptrini/page/1731332/
Partners involved in this statement include …

Frequently asked questions about iron and folic acid during pregnancy
1. What daily dose of iron and folic acid supplementation does WHO recommend during pregnancy?
Folate requirements are increased in pregnancy because of the rapidly dividing cells in the fetus and elevated urinary losses. Increased iron is needed to meet the demands for iron of the developing fetus and cell mass expansion. WHO recommends iron and folic acid supplementation for pregnant women, starting early in pregnancy and at a daily dose of 30–60 mg of elemental iron plus 400 µg (0.4 mg) of folic acid, as this has been shown to reduce the risk of low birthweight, maternal anemia and iron deficiency [2]. In settings where anemia in pregnant women is a severe public health problem (i.e. 40 percent or higher) a daily dose of 60 mg of elemental iron is preferred over a lower dose. If a woman is diagnosed with anemia, WHO recommends daily treatment with 120 mg of elemental iron and 400 µg (0.4 mg) of folic acid until her hemoglobin concentration rises to a normal level [5,6].
A combined dose of 60 mg of elemental iron and 400 µg (0.4 mg) of folic acid is included on the WHO Model List of Essential Medicines [7] and is provided by the United Nations Children’s Fund (UNICEF). Using this preparation to treat anemia would provide 800 µg (0.8 mg) of folic acid daily, which would not interfere with sulfadoxine-pyrimethamine as an antimalarial [8]. A trial conducted on pregnant women in Gambia using a 1,500 µg (1.5 mg) daily dose of folic acid showed no reduction in sulfadoxine-pyrimethamine efficacy [9]. However, to date, no data are available on sulfadoxine- pyrimethamine efficacy when administered with daily folic acid doses between 1,500 µg (1.5 mg) and less than 5,000 µg (5 mg) in pregnant women.
Women should be counseled when they receive iron and folic acid supplements to inform them why these supplements are needed, how to take them and for what duration. They should also receive information about how to manage the possible side effects of iron supplementation (mainly mild gastrointestinal symptoms), which may occur in some women.
2. What are the clinical indications for higher dose folic acid during pregnancy?
Folic acid insufficiency is associated with an increased risk of neural tube defects, a debilitating congenital anomaly in which the neural tube does not close properly. This occurs in 0.5–6.5 out of every 1,000 pregnancies. The neural tube forms in the first month after conception, with closure by about 28 days; thus, in order to prevent neural tube defects maternal intake of folic acid should begin before conception and continue through early pregnancy.
There are limited cases (e.g. for prevention of recurrent cases of neural tube defects [10] and for women on anticonvulsant treatment, diabetics and women with sickle cell anemia) where it is recommended that pregnant women take folic acid at a daily dose of 5,000 µg (5 mg).
In particular, women who have had a previous pregnancy resulting in a baby with neural tube defects are at higher risk of having another baby with neural tube defects. These women should receive folic acid at a dose of 5,000 µg (5 mg) a day starting at least one month – though preferably two to three months – before they conceive, and continuing until 12 weeks of gestation, while increasing their dietary folate intake. Given the need for supplementation prior to conception, fortification of staple foods with folic acid should also be considered as a cost-effective public health measure to reduce the incidence of neural tube defects [11].
3. How does folic acid interfere with the efficacy of sulfadoxine- pyrimethamine against malaria?
Folic acid is an essential nutrient for all organisms. Humans get folate from food or dietary supplements. Other organisms, such as the malaria parasite, synthesize folic acid de novo, or endogenously. Both sulfadoxine-pyrimethamine and co-trimoxazole are anti-folates and prevent malaria by blocking the synthesis of folic acid. Without folic acid, the parasite cannot complete its lifecycle. However, if blood folate concentrations are high enough, the malaria parasite can use this folate instead of making its own, allowing the infection to continue unchecked.
Additional References
5. World Health Organization (WHO), United Nations Children’s Fund (UNICEF), United Nations University (UNU). Iron deficiency anaemia assessment, prevention, and control: a guide for programme Geneva: WHO; 2001
6. Iron and folate Integrated Management of Pregnancy and Childbirth (IMPAC). In: Standards for maternal and neonatal care, 1.8. Geneva: World Health Organization; 2007.
7. WHO model list of essential medicines, 18th Geneva: World Health Organization; 2013. Available from: http://apps.who.int/iris/bitstream/10665/93142/1/EML_18_eng.pdf
8. Ouma P, Parise ME, Hamel MJ, et Randomized controlled trial of folate supplementation when treating malaria in pregnancy with sulfadoxine-pyrimethamine. PLoS Clin Trials. 2006 Oct 20; 1:e28. Available from: http://journals.plos.org/plosclinicaltrials/article?id=10.1371/journal.pctr.0010028
9. Mbaye A, Richardson K, Balajo B, et Lack of inhibition of the anti-malarial action of sulfadoxine-pyrimethamine by folic acid supplementation when used for intermittent preventive treatment in Gambian primigravidae. Am J Trop Med Hyg. 2006 Jun; 74(6):960–4. Available from: http://www.ajtmh.org/ content/74/6/960.long
10. Prevention of neural tube Integrated Management of Pregnancy and Childbirth (IMPAC). In: Standards for maternal and neonatal care, 1.5. Geneva: World Health Organization; 2007.
11. World Health Organization (WHO), Food and Agriculture Organization (FAO). Guidelines on food fortification with micr Geneva: WHO; 2006.
Suggested citation: Roll Back Malaria Partnership Malaria in Pregnancy Working Group: Consensus Statement on folic acid supplementation during pregnancy. Geneva; 2015.
Advocacy &Malaria in Pregnancy Bill Brieger | 24 Mar 2015
Supporting one Another: Female Nurses in Senegal helping Women have Malaria-free Pregnancies
Yacine Djibo, Founder & President of Speak Up Africa is helping focus International Women’s Day (March 8th) on efforts to protect women from malaria in Senegal. She is highlighting the  commitments of 8 strong and beautiful women, in Senegal, that are dedicated to eliminating malaria in their country. These commitments are part of an inclusive mass communication campaign that aims to launch a national movement in favor of malaria elimination in Senegal: the “Zero Malaria! Count Me In” campaign
commitments of 8 strong and beautiful women, in Senegal, that are dedicated to eliminating malaria in their country. These commitments are part of an inclusive mass communication campaign that aims to launch a national movement in favor of malaria elimination in Senegal: the “Zero Malaria! Count Me In” campaign
International Women’s Day, represents an opportunity to celebrate the achievements of women all around the world. This year’s theme is “Empowering Women – Empowering Humanity: Picture it” envisions a world where each woman and girl can exercise her choices, such as participating in politics, getting an education or fighting malaria. Below is the eighth and final feature on women fighting malaria in Senegal ……
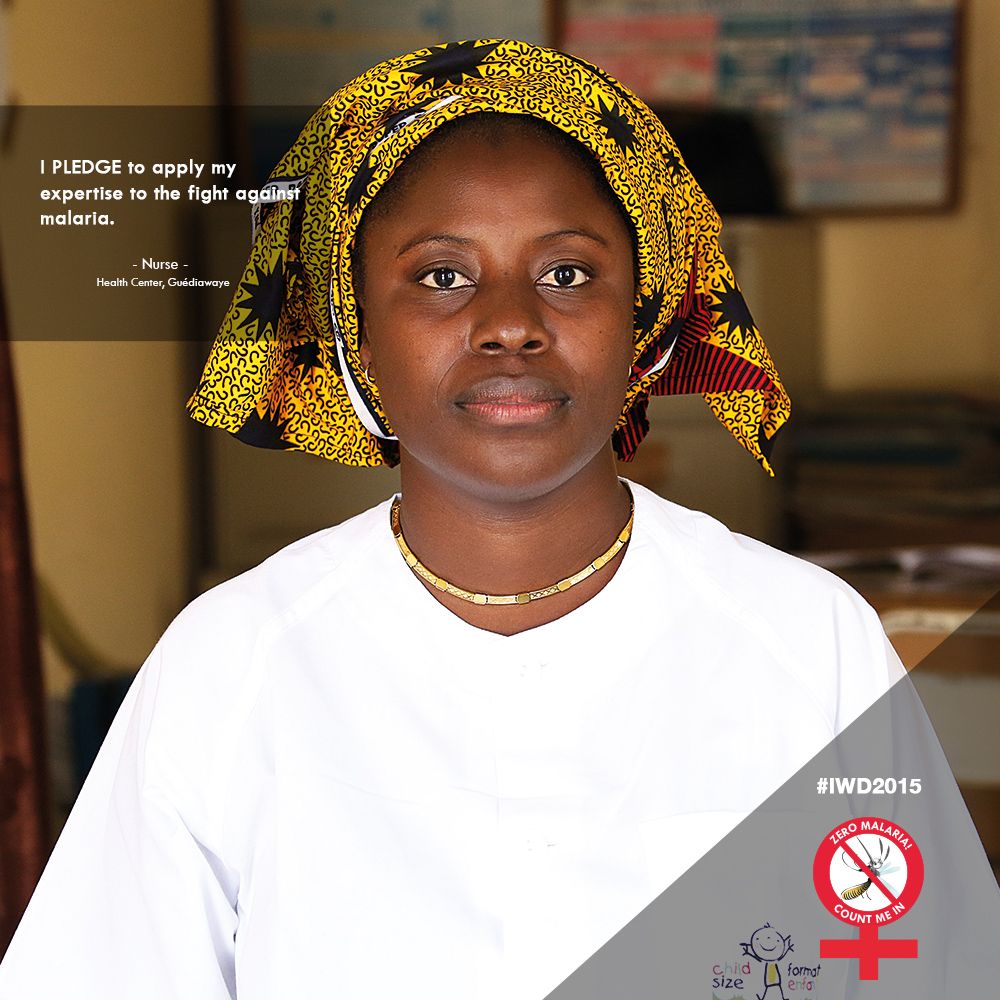
Nurse, Health Center, Guédiawaye District, Senegal
Nurses at the health center in Senegal’s Guédiawaye district bring their expertise to tirelessly provide essential malaria services to all community members. Of particular importance are pregnant women, a vulnerable group which must have access to prevention and treatment tools to ensure healthy pregnancies and healthy newborns.
Reducing the rate of infection to protect mothers and children is key, and remains one of the most pressing health issues facing the malaria community today. Pregnant women are at a higher risk for malaria as pregnancy reduces a woman’s immunity. Without the acquisition and use of insecticide treated mosquito nets and intermittent preventive treatment in pregnancy (IPTp), there is an increased risk of women (particularly those in their first and second pregnancies) contracting malaria, which can result in premature birth, low birth weight, and stillbirth.
 Each nurse’s job is twofold, to ensure women have the proper information and tools to prevent and treat malaria cases, and to ensure clear communication with her health post for what is needed in the community. Nurses are essential and their work is applauded on International Women’s day, as we recognize amazing examples of women supporting their fellow women to ensure health needs are met.
Each nurse’s job is twofold, to ensure women have the proper information and tools to prevent and treat malaria cases, and to ensure clear communication with her health post for what is needed in the community. Nurses are essential and their work is applauded on International Women’s day, as we recognize amazing examples of women supporting their fellow women to ensure health needs are met.
*****
Headquartered in Dakar, Senegal, Speak Up Africa is a creative health communications and advocacy organization dedicated to catalyzing African leadership, enabling policy change, securing resources and inspiring individual action for the most pressing issue affecting Africa’s future: child health.
Health Systems &HIV &Malaria in Pregnancy &Treatment Bill Brieger | 02 Dec 2014
Update on Malaria and HIV/AIDS
 World AIDS Day is a time to reflect on the broader impact of HIV and its interactions with other infectious and chronic conditions that must be managed through an integrated health system. The past few months have yielded a variety of published studies on the HIV-Malaria link ranging from pharmacological, and physiological to health systems issues. A brief summary follows.
World AIDS Day is a time to reflect on the broader impact of HIV and its interactions with other infectious and chronic conditions that must be managed through an integrated health system. The past few months have yielded a variety of published studies on the HIV-Malaria link ranging from pharmacological, and physiological to health systems issues. A brief summary follows.
Having HIV does have consequences on malaria infection. Serghides et al. studied malaria-specific immune responses are altered in HIV/malaria co-infected individuals. Fortunately these researchers learned about “the importance of HIV treatment and immune re-constitution in the context of co-infection.”
Malaria, HIV and Pregnancy
Pregnant women are an important group in the population to protect from both HIV and malaria. The link between the diseases may not be one of influencing each other but in the fact that they both appear in the same population with similar negative consequences. Women are at increased risk of anemia in pregnancy due to malaria and/or HIV infection according to Ononge and co-workers. Normally a pregnant woman in a malaria endemic area passes on malaria antibodies to their newborns.
Moro et al. learned that, “Placental transfer of antimalarial antibodies is reduced in pregnant women with malaria and HIV infection.” Chihana and colleagues studied HIV status in Malawian pregnant women and follow-up their children. They reported that, “Maternal HIV status had little effect on neonatal mortality but was associated with much higher mortality in the post-neonatal period and among older children.”
Drug Interactions and Issues
Hoglund and colleagues studied interactions between common antimalarial and HIV medications. They found that, “There are substantial drug interactions between artemether-lumefantrine and efavirenz, nevirapine and ritonavir/lopinavir. Given the readily saturable absorption of lumefantrine, the dose adjustments predicted to be necessary will need to be evaluated prospectively in malaria-HIV coinfected patients.”
 Drugs taken during pregnancy to prevent malaria are influenced by HIV status. It is known that Intermittent Preventive Treatment with sulfadoxine-pyrimethamine should not be administered to HIV-positive pregnant women taking cotrimoxazole prophylaxis. González et al. wanted to learn whether mefloquine (MQ) could be used by HIV+ pregnant women. Unfortunately they learned that, “MQ was not well tolerated, limiting its potential for IPTp … (and) … MQ was associated with an increased risk of mother to child transmission of HIV.”
Drugs taken during pregnancy to prevent malaria are influenced by HIV status. It is known that Intermittent Preventive Treatment with sulfadoxine-pyrimethamine should not be administered to HIV-positive pregnant women taking cotrimoxazole prophylaxis. González et al. wanted to learn whether mefloquine (MQ) could be used by HIV+ pregnant women. Unfortunately they learned that, “MQ was not well tolerated, limiting its potential for IPTp … (and) … MQ was associated with an increased risk of mother to child transmission of HIV.”
Health Systems Issues
Haji and co-investigators reported that malaria care seeking was delayed in Ethiopia because “Children whose guardians believed that covert testing for HIV was routine clinical practice presented later for investigation of suspected malaria.”
The need to adjust clinical guidance and practice as prevalence of malaria changes was addressed by Mahende et al. in Tanzania. They observed that, “Although the burden of malaria in many parts of Tanzania has declined, the proportion of children with fever has not changed.” More accurate diagnosis is needed as demonstrated by the various causes of febrile illness they found including in addition to malaria, respiratory illnesses, blood infections, urine infections, gastrointestinal illness and even HIV.
Finally Mbeye and colleagues report that cotrimoxazole prophylactic treatment reduces incidence of malaria and mortality in children in sub-Saharan Africa and appears to be beneficial for HIV-infected and HIV-exposed as well as HIV-uninfected children. This lesson from HIV programming can have broader implications for malaria control strategies.
Integrated control of infectious diseases is essential for population health, especially at the primary care level. Hopefully research as shown above can assist in planning better services for people living in areas that are endemic to both malaria and HIV.
Health Systems &IPTp &Malaria in Pregnancy Bill Brieger | 07 Nov 2014
Health Systems Strengthening: Achieving Lasting Results for IPTp
 At the Call to Action for Intermittent Preventive Treatment of Malaria in Pregnancy (IPTp) during the just concluded American Society of Tropical Medicine and Hygiene Annual Meeting, Elaine Roman of Jhpiego/MCSP advocated for strengthened health systems as a basic approach to enhancing IPTp coverage. Below is a summary of her remarks.
At the Call to Action for Intermittent Preventive Treatment of Malaria in Pregnancy (IPTp) during the just concluded American Society of Tropical Medicine and Hygiene Annual Meeting, Elaine Roman of Jhpiego/MCSP advocated for strengthened health systems as a basic approach to enhancing IPTp coverage. Below is a summary of her remarks.
Why should we strengthen the Health System? Addressing the health system at all levels leads to improved outcomes and comprehensive coverage. Increasing IPTp uptake requires strengthening antenatal care (ANC) and other components of the health system.
ANC within a strong health system provides an opportunity to improve the health of pregnant women and their newborns. Malaria in pregnancy (MIP) is a maternal and newborn health issue. When health systems are weak, there is greater likelihood of negative consequences on mother and newborn.
 Improving Health Systems for enhanced IPTp addresses the following health systems components:
Improving Health Systems for enhanced IPTp addresses the following health systems components:
- Integration: Reproductive Health Programs and National Malaria Control Programs
- Policies and Guidelines: Consistency across national documents
- Capacity Development: Bother In-Service Training and Pre-Service Education
- Quality Assurance: Linked directly with support supervision
- Community Engagement: Promotion of early ANC and Promotion of IPTp uptake
- Commodities: Ensuring availability at ANC of sulfadoxine-pyrimethamine (SP) and supplies, as well as long-lasting insecticide-treated bed nets
- Monitoring and Evaluation: Facility-level data collection and Data for decision- making
- Finance: Sustained and comprehensive services
 Systems strengthening works. Strengthened Health Systems for IPTp in Kenya resulted from community engagement, training, supervision: leading to IPTp1 coverage of 91.6% and IPTp2 (or more doses) coverage at 61.1%.
Systems strengthening works. Strengthened Health Systems for IPTp in Kenya resulted from community engagement, training, supervision: leading to IPTp1 coverage of 91.6% and IPTp2 (or more doses) coverage at 61.1%.
In Ghana, Capacity development, commodities, community engagement improvements resulted in IPTp2 (or more doses) coverage of 44% to 65%
In Zambia development of clear policy, integrated training, supervision led to IPTp2 (or more doses) coverage increasing from 63% in 2007 to 72% in 2012.
Moving forward we must advocate for strengthening health systems that will lead to increased IPTp uptake and lasting gains. We must focus on ANC, complemented by efforts at community and policy levels. Finally we must address each health system component, based on country context.
IPTp &Malaria in Pregnancy &Private Sector Bill Brieger | 04 Nov 2014
A role for the private sector increasing uptake of intermittent preventive treatment for malaria in pregnancy in Kenya
Jhpiego staff will again present a poster at the Tuesday noon (Nov 4) session of the American Society of Tropical Medicine and Hygiene Annual Meeting. Augustine M. Ngindu, Muthoni M. Kariuki, Sanyu Kigondu, Johnstone Akatu, Isaac M. Malonza, with support from USAID’s Maternal and Child Health Integrated Project (MCHIP) will share experiences with a poster titled, “Improving maternal and neonatal health: Complementary role of the private sector increasing uptake of intermittent preventive treatment for malaria in pregnancy in Kenya.” The abstract is provided below.
 Malaria in pregnancy (MIP) is associated with poor pregnancy outcomes including maternal anaemia, intrauterine growth retardation and low birth weight. Kenya changed its policy on intermittent preventive treatment using Sulfadoxine Pyrimethamine (IPTp-SP) in 1998. However, IPTp coverage rates have remained low: 4% in 2003, 14% in 2007, 15% in 2008 and 25 % in 2010.
Malaria in pregnancy (MIP) is associated with poor pregnancy outcomes including maternal anaemia, intrauterine growth retardation and low birth weight. Kenya changed its policy on intermittent preventive treatment using Sulfadoxine Pyrimethamine (IPTp-SP) in 1998. However, IPTp coverage rates have remained low: 4% in 2003, 14% in 2007, 15% in 2008 and 25 % in 2010.
To increase the coverage rate, MCHIP supported malaria control and reproductive health divisions of the ministry of health, first to harmonize knowledge among service providers on provision of IPTp-SP in 2011, and second to train community health workers (CHWs) on sensitization of pregnant women to start early antenatal care (ANC) attendance in 2012.
 A community survey conducted in 2013 showed a significant increase in the proportion of pregnant women receiving two or more IPTp doses from 25% to 63%, the highest increase in IPTp uptake since 1998. Following the successful scale up of IPTp, one sub-county conducted an assessment of its health facilities to determine quality of data on ANC clients accessing IPTp-SP.
A community survey conducted in 2013 showed a significant increase in the proportion of pregnant women receiving two or more IPTp doses from 25% to 63%, the highest increase in IPTp uptake since 1998. Following the successful scale up of IPTp, one sub-county conducted an assessment of its health facilities to determine quality of data on ANC clients accessing IPTp-SP.
A total of 15 (58%) out all 26 health facilities in the sub-county (public – 6 out of 8, faith-based – 2 out 3 and private – 7 out of 15) were selected. Data on new ANC clients, revisits and IPTp doses given was collected from the ANC registers.
Among th e assessed health facilities 13 (87%) out of the 15 were registering new ANC cases, revisits and provided IPTp-SP (public 6, faith based 2, private 5. One private clinic provided ANC services to revisits and IPTp2 doses only after the clients had been registered in public facilities, the second did not offer ANC services.
e assessed health facilities 13 (87%) out of the 15 were registering new ANC cases, revisits and provided IPTp-SP (public 6, faith based 2, private 5. One private clinic provided ANC services to revisits and IPTp2 doses only after the clients had been registered in public facilities, the second did not offer ANC services.
In 2013 the government declared provision of free maternity services in public facilities but ANC clients have continued to utilize services from the private sector. This is an indication of the untapped potential in the private sector in increasing access to high impact interventions and importance of supporting the sector by all partners to provide these interventions.
Such complementary efforts if implemented will not only result in enabling the country to move towards achievement of set targets but also improve pregnancy outcomes through reduction in effects of
malaria in pregnancy.
IPTp &Malaria in Pregnancy Bill Brieger | 03 Nov 2014
Call to Action at ASTMH – Intermittent Preventive Treatment of Malaria in Pregnancy
If you are interested in preventing malaria in pregnancy (MIP) join a special symposium at the American Society of Tropical Medicine and Hygiene 2014 Annual Meeting on Wednesday afternoon/evening, November 5th. The seminar is organized by the Malaria in Pregnancy Consortium and the Roll Back Malaria Malaria in Pregnancy Working Group, with support from Medicines for Malaria Venture (MMV) and London School of Hygiene and Tropical Medicine (LSHTM). The agenda can be found below.
SESSION 1 Current coverage and delivery of IPTp 3:45 – 4:15
- Welcome Koki Agarwal, Roll Back Malaria MIP Working Group, Jhpiego / Maternal and Child Survival Program
- Current coverage estimates of IPTp Annemieke van Eijk, Liverpool School of Tropical Medicine
- Factors affecting delivery of IPTp: Findings from quantitative and qualitative studies in Mali and Kenya, Jayne Webster: London School of Hygiene & Tropical Medicine
 SESSION 2 MOVING FORWARD: OPPORTUNITIES TO SCALE UP IPTp: 4:15 – 5.15
SESSION 2 MOVING FORWARD: OPPORTUNITIES TO SCALE UP IPTp: 4:15 – 5.15
- IPTp and WHO’s Global Malaria Programme, Pedro Alonso, Global Malaria Programme of the World, Health Organization
- Interventions to improve uptake of IPTp in Ghana, Harry Tagbor, Kwame Nkrumah University of Science & Technology
- Studies of cost-effectiveness of IPTp-SP: IPTp-SP2 vs. placebo in Mozambique and a meta analysis of IPTp-SP3 + vs. SP2 in a range of African settings, Elisa Sicuri Barcelona Centre for International Health Research
- Can acceptability be enhanced? Findings from quantitative and qualitative studies on IPTp against malaria and curable STIs/RTIs, Matthew Chico, London School of Hygiene & Tropical Medicine
- Delivering IPTp in the antenatal care platform, Kate Mitchell, Harvard School of Public Health/ Maternal, Health Task Force
- Health systems strengthening: Achieving lasting results for IPTp, Elaine Roman. Jhpiego / Maternal and Child Health Program
SESSION 3 Call to Action: 5:15 – 6:00
- Defining the Call to Action (group facilitation) – Koki Agarwal, Roll Back Malaria MIP Working Group, Jhpiego / Maternal and Child Survival Program, Intermittent Preventive Treatment of Malaria in Pregnancy
Health Systems &Human Resources &IPTp &Malaria in Pregnancy &Monitoring Bill Brieger | 03 Nov 2014
Jhpiego at ASTMH: Performance Quality Improvement for IPTp in Kenya
Monday afternoon (3 October 2014) at the American Society for Tropical Medicine and Hygiene Annual Meeting in New Orleans, Jhpiego and USAID/PMI are sponsoring a panel on “Integrating and Innovating: Strengthening Care for Mothers and Children with Infectious Diseases.” If you are at the meeting please attend to learn more about our Malaria activities in Kenya.
 One of the panel presentations is “Performance Quality Improvement Lending to Corrected Documented Outcomes for Intermittent Preventive Treatment in Kenya,” by Jhpiego staff Muthoni Kariuki, Augustine Ngindu Isaac Malonza, and Sanyu Kigondu, who are working with USAID’s Maternal & Child Health Integrated Project (MCHIP).
One of the panel presentations is “Performance Quality Improvement Lending to Corrected Documented Outcomes for Intermittent Preventive Treatment in Kenya,” by Jhpiego staff Muthoni Kariuki, Augustine Ngindu Isaac Malonza, and Sanyu Kigondu, who are working with USAID’s Maternal & Child Health Integrated Project (MCHIP).
According to Malaria policy in Kenya all pregnant women in malaria endemic areas receive free intermittent preventive treatment with SP have access to free malaria diagnosis and treatment when presenting with fever have access to LLINs (National Malaria Strategy (NMS) 2009–2017).
By 2013 80% of people living in malaria risk areas should be using appropriate malaria preventive interventions. Intermittent Preventive Treatment of malaria in pregnancy using Sulfadoxine Pyrimethamine (IPTp-SP) intervention is recommended for use in malaria endemic region.
 MCHIP broadly implemented Capacity Development and service delivery and improvement interventions that also had impact on the delivery of malaria in pregnancy services through collaboration with the Ministry of Health divisions/units at national level: (malaria, reproductive health, community health).
MCHIP broadly implemented Capacity Development and service delivery and improvement interventions that also had impact on the delivery of malaria in pregnancy services through collaboration with the Ministry of Health divisions/units at national level: (malaria, reproductive health, community health).
At county level scale up provision of IPTp at facility level took place in 14 malaria endemic counties. This included 8 counties in the lake endemic region including Bondo sub-county (the MCHIP model sub-county) and 6 in the coastal endemic region.
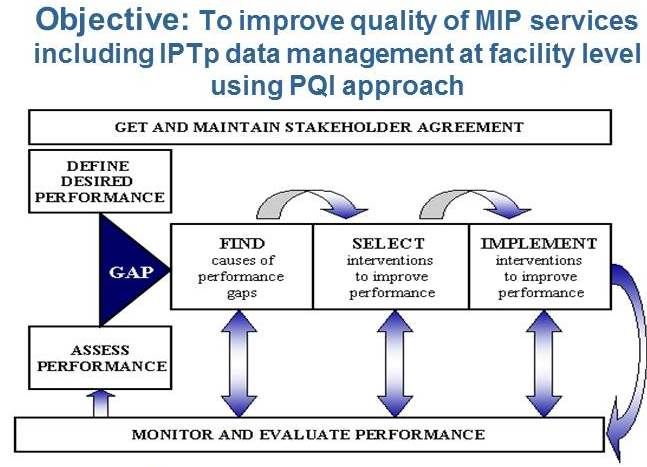
Quality Improvement through Performance Quality Improvement (PQI) process was instituted to enhance service delivery. The MCHIP era in Bondo Strengthened ANC Services using the following:
- Development of MIP Standards-Based Management and Recognition (SBM-R) standards
- Orientation of facility in-charges, supervisors and service providers on the standards
- Monitoring of IPTp uptake using DHIS2 data
- Feedback to facility in-charges and supervisors on DHIS2 findings
- Collection of ANC data from ANC registers (2011-2013)
- Feedback to facility in-charges and supervisors on ANC data
Quality improvement in the malaria in pregnancy component was undertaken with the objective to improve quality of MIP services including IPTp data management at facility level using PQI approach. An Example of a MIP SBM-R standard is seen below.
 In-service training focused on orientation of facility in-charges on PQI who then continued orientation at Facility Level. Overall we oriented 1200 facility in-charges and 100 supervisors on the standards. Facility in-charges cascaded orientation to 2,441 service providers.
In-service training focused on orientation of facility in-charges on PQI who then continued orientation at Facility Level. Overall we oriented 1200 facility in-charges and 100 supervisors on the standards. Facility in-charges cascaded orientation to 2,441 service providers.
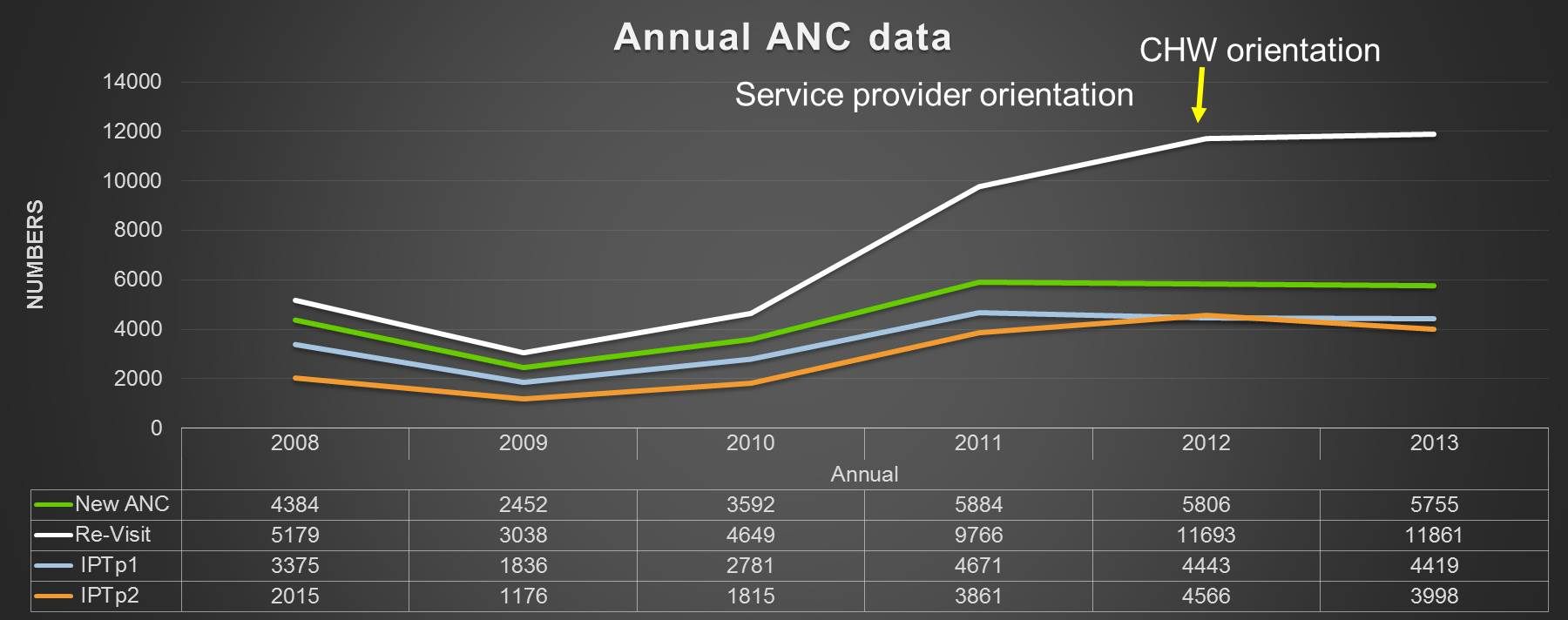 We then analysed ANC data from DHIS (2011-2013) indicated proportion of pregnant women receiving IPTp2 was higher than IPTp1 (IPTp2+ doses reported as IPTp2 dose). We helped improve reporting by service providers not oriented on use of the ANC register in order to reduce data errors.
We then analysed ANC data from DHIS (2011-2013) indicated proportion of pregnant women receiving IPTp2 was higher than IPTp1 (IPTp2+ doses reported as IPTp2 dose). We helped improve reporting by service providers not oriented on use of the ANC register in order to reduce data errors.
In conclusion, PQI is a best practice in provision of MIP services. Standardization of knowledge among service providers is essential in provision of quality MIP services. Development of facility in-charges as mentors in the facility to ensure continued orientation of new service providers.
Use of appropriate monitoring tools is necessary to assist in assessment of quality of services provided including data management. Feedback to service providers is one of the performance rewards and encourages participation in knowledge acquisition