Malaria in Pregnancy &Mentoring &mHealth Bill Brieger | 18 Nov 2020
Mentorship to Strengthen Quality of Malaria Case Management & Malaria in Pregnancy, Zimbabwe
Gilson Mandigo et al. examine how mentoring can be achieved from a distance in Zimbabwe. Their presentation at the 69th Annual Meeting of American Society of Tropical Medicine and Hygiene of “Mentorship to Strengthen Quality of Malaria Case Management And Malaria in Pregnancy (MIP) in Zimbabwe: Lessons Learned From One Year of Implementation” is shared below.
 Despite significant investment in training and supervision of facility-based health workers in Zimbabwe, persistent malaria case management and MIP gaps remain. National Malaria Control Program and US President’s Malaria Initiative developed and implemented a mentorship intervention in five high burden malaria districts to motivate provider performance and improve quality services.
Despite significant investment in training and supervision of facility-based health workers in Zimbabwe, persistent malaria case management and MIP gaps remain. National Malaria Control Program and US President’s Malaria Initiative developed and implemented a mentorship intervention in five high burden malaria districts to motivate provider performance and improve quality services.
From June 2018 – June 2019, 25 health workers proficient in malaria service delivery were selected and trained in clinical mentorship. These individuals mentored 98 providers at 25 facilities, covering clinical case reviews, bedside coaching, simulations, and records review. USAID’s Zimbabwe Assistance Project in Malaria subsequently assessed the mentorship program through review of patient records, feedback from mentors and mentees, and engagement of stakeholders.
Record review compared practices before and after implementation, using a checklist that noted completeness and appropriateness of case management across multiple parameters, including physical examination, diagnosis, classification and treatment. Mentored facilities documented improvements in recommended practices across registers: 58% to 63% for outpatient clinical settings, 53% to 64% for integrated management of neonatal and childhood illnesses, and 72% to 76% for antenatal care.
A phone-based e-survey of 49 mentees and 21 mentors elicited positive feedback on the mentorship approach: 62% of mentors were “very satisfied” with the program, 67% reported quality improvement and 86% benefited from learning new skills. Among mentees:
- 60% were “very satisfied”,
- 67% said that the program has improved service quality and
- 97% benefited from learning new skills
Common challenges included mentor transportation, mentee availability, and commodity availability. Through a review meeting, stakeholders recommended the intervention continue, as it was acceptable, feasible and achieved promising results. Recommendations include prioritizing high-volume facilities, integrating management of mentorship into District Health Executive functions and use of low-cost communication platforms to aid virtual mentorship.
Authors and Affiliations
Gilson Mandigo(1), Anthony Chisada(1), Noe Rakotondrajaona(2), Paul Matsvimbo(3), Christie Billingsley(4), Chantelle Allen(5), Katherine Wolf(5), Patience Dhliwayo(3). 1.ZAPIM/Jhpiego, Harare, Zimbabwe, 2.ZAPIM/Abt, Harare, Zimbabwe, 3.MOHCC, Harare, Zimbabwe, 4.PMI, Harare, Zimbabwe, 5.Jhpiego HQ, Baltimore, MD, United States
Antenatal Care (ANC) &Malaria in Pregnancy Bill Brieger | 18 Nov 2020
Group Antenatal Care to Improve Malaria in Pregnancy & ANC in Geita, Tanzania
 Jasmine Chadewa and colleagues are sharing their work on Group Antenatal Care (GANC): A Baseline Initiative to Improve Malaria in Pregnancy & ANC Indicators. A Case from Geita Tanzania at the virtual 69th Annual Meeting of American Society of Tropical Medicine and Hygiene. See their findings below.
Jasmine Chadewa and colleagues are sharing their work on Group Antenatal Care (GANC): A Baseline Initiative to Improve Malaria in Pregnancy & ANC Indicators. A Case from Geita Tanzania at the virtual 69th Annual Meeting of American Society of Tropical Medicine and Hygiene. See their findings below.
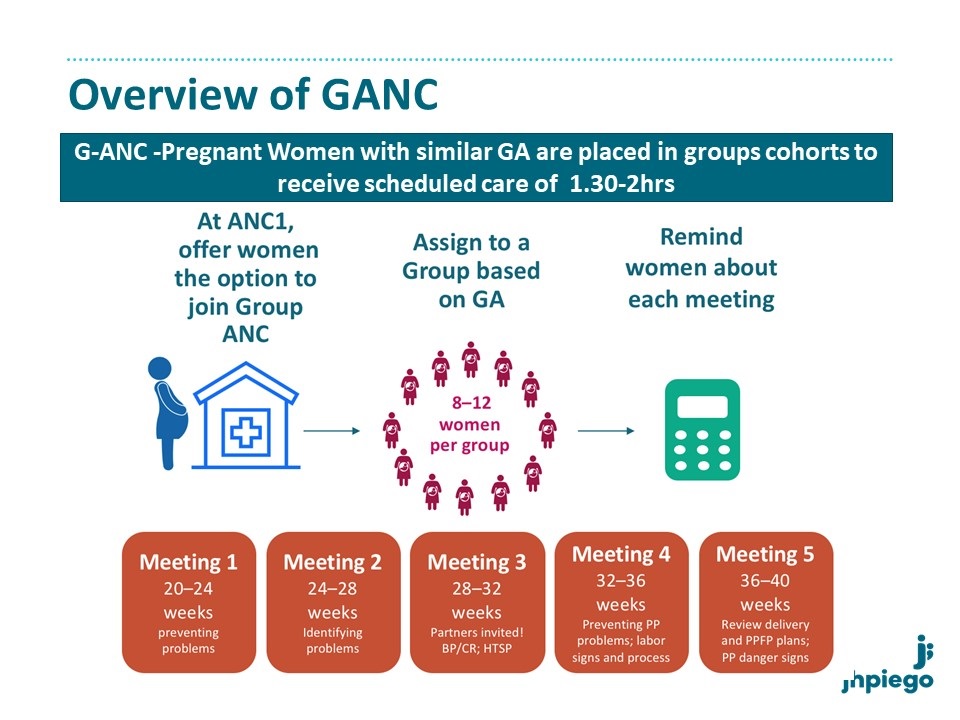
Malaria in pregnancy (MiP) is a major public health concern contributing to poor maternal and newborn health outcomes. Early and frequent Antenatal Care attendance (ANC) could address this problem. Early ANC booking is still low in Tanzania. USAID Boresha Afya and Tanzania Ministry of Health introduced a Group Antenatal Care (GANC) initiative in Geita region where malaria prevalence is high. This model brings 8-15 pregnant women of similar gestational age together for ANC. Group contacts last 1.5-2 hours, and include clinical care, information sharing, and peer support to improve quality of care and women’s engagement, leading to better retention in care.
 Prior to implementation, a baseline cross-sectional household survey was conducted in December 2019 in 40 communities across Geita region. The survey was intended to identify gaps and targets in MiP services delivery which could be addressed through GANC. Women who had delivered a live born infant in the preceding 12 months were included. We interviewed 1111 women; mean age was 27 years. One-third had no education and only 9% had secondary education.
Prior to implementation, a baseline cross-sectional household survey was conducted in December 2019 in 40 communities across Geita region. The survey was intended to identify gaps and targets in MiP services delivery which could be addressed through GANC. Women who had delivered a live born infant in the preceding 12 months were included. We interviewed 1111 women; mean age was 27 years. One-third had no education and only 9% had secondary education.
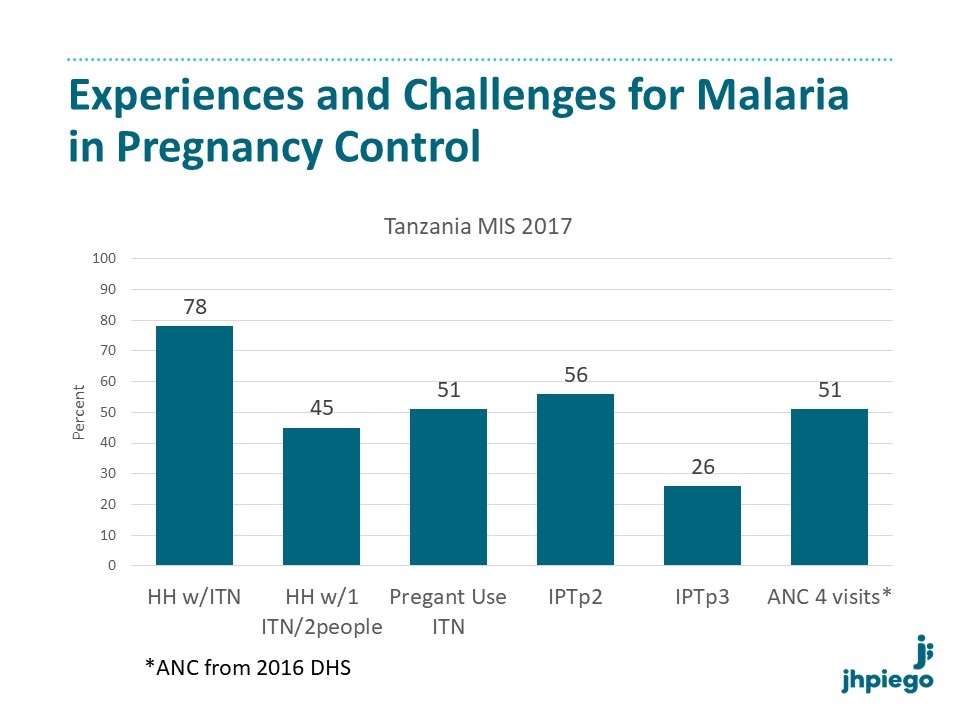 Nearly all 95% of women lived in a house with an Insecticide Treated Net (ITN); 87% reported receiving an ITN during their last pregnancy and 90% reported ITN use on the night before the survey. Nearly all 98% attended ANC at least once, with 17% attending in first trimester. Only 45% attended ?4 visits; 6% of women were stopped by their husbands from attending ANC.
Nearly all 95% of women lived in a house with an Insecticide Treated Net (ITN); 87% reported receiving an ITN during their last pregnancy and 90% reported ITN use on the night before the survey. Nearly all 98% attended ANC at least once, with 17% attending in first trimester. Only 45% attended ?4 visits; 6% of women were stopped by their husbands from attending ANC.
 Median total time spent away from the home for each ANC was 4 hours. 88% received Intermittent Preventive Treatment of malaria in pregnancy (IPTp), with 53% receiving the recommended 3 or more doses. Among those who did not receive IPTp, 42% reported that the provider did not offer it and 25% reported it was not available at the facility. Receipt of other interventions varied: 64% reported that their blood pressure was checked, 95% and 57% had blood and urine samples collected, 74% had received adequate doses of tetanus vaccination, and 94% received iron/folate supplements.
Median total time spent away from the home for each ANC was 4 hours. 88% received Intermittent Preventive Treatment of malaria in pregnancy (IPTp), with 53% receiving the recommended 3 or more doses. Among those who did not receive IPTp, 42% reported that the provider did not offer it and 25% reported it was not available at the facility. Receipt of other interventions varied: 64% reported that their blood pressure was checked, 95% and 57% had blood and urine samples collected, 74% had received adequate doses of tetanus vaccination, and 94% received iron/folate supplements.
We will assess whether GANC improves MiP services as well as quality of ANC care, to promote positive pregnancy outcomes.
Authors and Affiliations
Jasmine Chadewa1, Mary Drake1, Chonge Kitojo2, Ryan Lash3, Stephanie Suhowatsky4, Abdalah Lusasi5, Japhet Simeo6, Goodluck Tesha7, Ruth Lemwayi1, Issa Garimo5, Agnes Kosia1, Alice Christensen1, Rita Noronha1, Zahra Mkomwa7, Naomi Serbantez2, Melkior Assenga1, Erik Reaves8, Samwel Lazaro5, Miriam Kombe9, Alen Kinyina1, Alen Kinyina1, Ally Mohamed5, Gladys Tetteh4, Bill Brieger10, Edward Kenyi4, Annette Almeida1, Julie Gutman3
1USAID Boresha Afya Project -Jhpiego Tanzania, Dar es Salaam, Tanzania, United Republic of, 2President’s Malaria Initiative/United States Agency for International Development, Tanzania, Dar es Salaam, Tanzania, United Republic of, 3Malaria Branch, Division of Parasitic Diseases and Malaria, Center for Global Health, Centers for Disease Control and Prevention, Dar es Salaam, Tanzania, United Republic of, 4Jhpiego Headquarter U.S.A, Baltimore, MD, United States, 5National Malaria Control Program-Tanzania Ministry of Health, Community Development, Gender, Elderly and Children, Dar es Salaam, Tanzania, United Republic of, 6Regional Health Management Team, Dar es Salaam, Tanzania, United Republic of, 7USAID Boresha Afya Project –Path Tanzania, Dar es Salaam, Tanzania, United Republic of, 8President’s Malaria Initiative, Centers for Disease Control and Prevention Tanzania, Dar es Salaam, Tanzania, United Republic of, 9USAID, Dares Salaam, Dar es Salaam, Tanzania, United Republic of, 10Jhpiego Headquarter U.S.A, Dar es Salaam, Tanzania, United Republic of
Uncategorized Bill Brieger | 17 Nov 2020
Advantages of Virtual Technical and Skills Training Courses on Malaria During COVID-19 in Myanmar
Aung K. Zaw et al. share in a poster their experiences with malaria and COVID-19 in Myanmar through the Defeat Malaria USAID/PMI Project. This can be found at the website of the 69th Annual Meeting of American Society of Tropical Medicine and Hygiene Which is virtual. Their presentation is see below.
 The President’s Malaria Initiative-supported Defeat Malaria Project aims to enhance the technical and operational capacity of the NMCP and health care providers in four States/Regions of Myanmar between 2016-2021. The project designed a capacity development strategy for staff and the NMCP using cascade training.
The President’s Malaria Initiative-supported Defeat Malaria Project aims to enhance the technical and operational capacity of the NMCP and health care providers in four States/Regions of Myanmar between 2016-2021. The project designed a capacity development strategy for staff and the NMCP using cascade training.
Master mentors (MM) from new Regions of the project were trained November/December 2019 who will train a cadre of general trainers (GT) at district and township level. Then GT will conduct onsite courses for integrated community malaria volunteers (ICMV).
However, due to the current COVID-19 situation travel and movement restrictions are in place. The project shifted from classroom-based to virtual training via Zoom for a 5-day training of GT and to develop 11 GT on malaria and other ICMV-managed diseases and training skills.
Participatory classroom training methodology was used for virtual training, including knowledge update and skills and attitudes development. Pre and post-training knowledge assessments and skills assessments were carried out to measure knowledge improvement. Daily and end course evaluations were done to gauge participants’ perception of virtual training. 64% of participants passed (score ?80%) the pre-training knowledge assessment, and 100% achieved ?80% on the post-training assessment.
 Training skills (facilitation and demonstration of skills) were assessed using checklists during practice with RDTs and all participants passed. Coaching skills could not be assessed in this virtual training. Daily evaluation results showed that participants’ expectations and objectives were met. 75% stated that they felt more confident in planning and conducting a training course.
Training skills (facilitation and demonstration of skills) were assessed using checklists during practice with RDTs and all participants passed. Coaching skills could not be assessed in this virtual training. Daily evaluation results showed that participants’ expectations and objectives were met. 75% stated that they felt more confident in planning and conducting a training course.
According to the final evaluation, 83% of participants felt positive about the virtual training methodology. On the other hand, 17% noted occasional difficulty hearing due to unstable internet connections. From a logistics and cost standpoint, it is feasible to continue the use of the virtual training platform for technical and training skills courses at the township level.
Authors and Affiliations
Aung K. Zaw(1), May Khin(1), Thiha Soe(1), Khin Zin(1), Ni Ni Aye(1), May Aung Lin(2), Thin Chit(2), Naung Naung(2), Paing Lin(2), Soe Tun(2), Wai Paing(2), Arkar Thant(2) – 1.Jhpiego, Myanmar/PMI Defeat Malaria, Yangon, Myanmar, 2.University Research Co., Myanmar/PMI Defeat Malaria, Yangon, Myanmar
Communication &Community &IPTp &Malaria in Pregnancy Bill Brieger | 17 Nov 2020
What could hinder IPTp uptake?
Cristina Enguita-Fernàndez and colleagues share findings on from a qualitative study on the acceptability of a community-based approach to IPTp delivery in 4 sub-Saharan countries in the UNITAID TiPTop project. Their poster is available at the vitrual 69th Annual Meeting of American Society of Tropical Medicine and Hygiene.
Increasing uptake of intermittent preventive treatment of malaria in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP) is key to improving maternal health indicators in malaria endemic countries, yet current coverage rates remain low. This qualitative study is part of a project evaluating the acceptability of a community-based approach to the delivery of IPTp (C-IPTp) through community health workers (CHWs) in 4 countries: the Democratic Republic of Congo (DRC), Madagascar, Mozambique and Nigeria.
 Between March 2018 and February 2020 a total of 435 in-depth interviews and 181 focus group discussions were carried out in the four country sites with pregnant women, relatives, women of reproductive age, community leaders, CHWs, and health providers. These were combined with direct observations of both community and facility based IPTp delivery.
Between March 2018 and February 2020 a total of 435 in-depth interviews and 181 focus group discussions were carried out in the four country sites with pregnant women, relatives, women of reproductive age, community leaders, CHWs, and health providers. These were combined with direct observations of both community and facility based IPTp delivery.
Grounded theory guided the study design and data collection, and data were analysed following a combination of content and thematic analysis to identify barriers to IPTp uptake. Although the novel C-IPTp intervention overcomes some access barriers (such as distance from health care providers, and travel costs), the study identified important barriers, some of which cut across delivery mechanisms and others that are specific to the C-IPTp approach.
Cross-cutting barriers consisted of perceived attributes of SP that explain treatment refusal. These consisted of sensorial characteristics, including the drug’s perceived foul smell, taste and large size; experiences with adverse drug effects, such as nausea and weakness; fears of adverse pregnancy outcomes, such as miscarriages or oversized babies leading to C-sections.
Attributes originated either in individual experiences of SP intake or were socially transmitted. Barriers specific to C-IPTp were centered around concerns over trust in CHWs as adequate providers of maternal healthcare and their competence in delivering IPTp. Despite sensitization activities, misinformation could still be determining these barriers. Ensuring an improved awareness of SP effects and its use, as well as a better understanding of the intervention should lead to enhanced C-IPTp adherence
Authors and Affiliations
Cristina Enguita-Fernàndez1, Yara Alonso1, Wade Lusengi2, Alain Mayembe2, Aimée M. Rasoamananjaranahary3, Estêvão Mucavele4, Ogonna Nwankwo5, Elaine Roman6, Franco Pagnoni1, Clara Menéndez1, Khátia Munguambe4 – 1ISGlobal – Barcelona Institute for Global Health, Barcelona, Spain, 2Bureau d’Étude et de Gestion de l’Information Statistique, Kinshasa, Congo, Democratic Republic of the, 3Malagasy Associates for Numerical Information and Statistical Analysis, Antananarivo, Madagascar, 4Centro de Investigação em Saúde de Manhiça, Maputo, Mozambique, 5University of Calabar, Calabar, Nigeria, 6Jhpiego, affiliate of Johns Hopkins University, Baltimore, MD, United States
coronavirus &COVID-19 &Mentoring Bill Brieger | 16 Nov 2020
Remote mentoring to ensure continuity of malaria service delivery during the COVID-19 pandemic in Zimbabwe, Cote d’Ivoire, and Cameroon
Katherine Wolf and colleagues address the need for mentoring in malaria programs across three countries when COVID-19 restricts travel and in-person work. They presented at the 69th Annual Meeting of American Society of Tropical Medicine and Hygiene and share the information below on e-mentoring.
 After the COVID-19 pandemic emerged in March 2020, global health experts warned that significant disruptions to malaria programs could lead to a doubling of malaria deaths in 2020, with a major spike overwhelming fragile health systems. To ensure the continuity and safety of malaria service delivery during the pandemic and associated lockdowns, Zimbabwe, Cote d’Ivoire (CI), and Cameroon transitioned from in-person, facility-based mentorship for health care providers to phone-based e-mentorship.
After the COVID-19 pandemic emerged in March 2020, global health experts warned that significant disruptions to malaria programs could lead to a doubling of malaria deaths in 2020, with a major spike overwhelming fragile health systems. To ensure the continuity and safety of malaria service delivery during the pandemic and associated lockdowns, Zimbabwe, Cote d’Ivoire (CI), and Cameroon transitioned from in-person, facility-based mentorship for health care providers to phone-based e-mentorship.
Working with the 3 National Malaria Control Programs, an e-mentoring package was developed and provided to mentors including technical guidance on malaria service delivery during COVID-19, a sample call guide, and a call tracker. Mentorship calls focused on continuity of malaria service delivery and applying WHO and PMI COVID-related guidance on triaging of patients and infection control measures.
From April to June, Zimbabwe reached 134 providers in 24 of 25 health facilities that previously received in-person mentorship. CI reached 41 providers in 33 facilities, where mentors already worked with staff in-person. Cameroon reached 179 providers in 116 lower performing facilities. In Zimbabwe, e-mentorship identified malaria commodity shortfalls and over-stocking, and facilitated re-distribution. Mentors advocated successfully for provision of PPE.
 E-mentorship identified a facility that had incorrectly stopped providing routine services; mentors were able to clarify COVID-related guidance from central authorities and assist in re-establishing routine services. In CI, the most frequently discussed topics were malaria commodities and case management. In Cameroon, frequent stockouts reported were better understood, and national stakeholders contacted for better solutions, including redeployment of medicines and commodities from overstocked sites to stocked-out areas.
E-mentorship identified a facility that had incorrectly stopped providing routine services; mentors were able to clarify COVID-related guidance from central authorities and assist in re-establishing routine services. In CI, the most frequently discussed topics were malaria commodities and case management. In Cameroon, frequent stockouts reported were better understood, and national stakeholders contacted for better solutions, including redeployment of medicines and commodities from overstocked sites to stocked-out areas.
All 3 countries demonstrated that e-mentorship successfully offers health care providers support and guidance to deliver quality malaria services during a crisis. Lessons learned can be applied in the context of natural disasters, political instability, and other potential disruptions to malaria programs.
Authors and Affiliations
Katherine Wolf1, Chantelle Allen2, Gilson Mandigo3, Leocadia Mangwanya3, Cyprien Noble1, Eric Tchinda4, Mathurin Dodo5, Arthur Konan1, Jacques Kouakou6, Lolade Oseni1
1Jhpiego/Impact Malaria, Baltimore, MD, United States, 2Jhpiego, Baltimore, MD, United States, 3ZAPIM/Jhpiego, Harare, Zimbabwe, 4Jhpiego/Impact Malaria, Kribi, Cameroon, 5Jhpiego/Impact Malaria, Ouagadougou, Burkina Faso, 6Jhpiego/Impact Malaria, Abidjan, Côte D’Ivoire
Antenatal Care (ANC) &CHW &IPTp Bill Brieger | 16 Nov 2020
Increasing Access to Malaria in Pregnancy Services through Community Health Units and Enhanced Supportive Supervision of Community Health Volunteers
Donald Apat and colleagues address the importance of community health workers and appropriate supervision in their study from Kenya. This was presented today at the 69th Annual Meeting of American Society of Tropical Medicine and Hygiene which is virtual. See their findings below.
According to the 2018 Kenya malaria program review, the uptake of malaria in pregnancy interventions by rural communities in Kenya remains low due to late first presentation to antenatal care (ANC), leading to sub-optimal intermittent preventive treatment in pregnancy (IPTp) coverage. Poor healthcare provider-client communication and low investment in advocacy, communication, and social mobilization contribute to late ANC presentation.
 Kenya is using community health volunteers (CHVs) supervised by community health assistants (CHAs) in community health units (CHUs) to increase demand for ANC services and uptake of IPTp but tracking of progress is hampered by a lack of accurate data on the number of estimated pregnancies at the sub-national level and poor household coverage by CHVs at the community level.
Kenya is using community health volunteers (CHVs) supervised by community health assistants (CHAs) in community health units (CHUs) to increase demand for ANC services and uptake of IPTp but tracking of progress is hampered by a lack of accurate data on the number of estimated pregnancies at the sub-national level and poor household coverage by CHVs at the community level.
In July 2019, Impact Malaria supported malaria-endemic Teso South sub-county of Busia county with the reorientation of 354 CHVs (92%) and 14 CHAs (100%), to identify and track pregnant women at the household level within the government established CHUs, provide social and behavior change communication messages, and enhance monthly supervision and reporting by CHAs.
CHVs identified and tracked 917 pregnant women from 32,758 (89.6%) households and identified and referred 273 ANC defaulters. We compared the uptake of IPTp before intervention (January to June 2019) and during the intervention (July to December 2019) using programmatic and Kenya health information system (KHIS) data.
At pre-intervention, 32,898 (90%) households were visited, with 2,160 new ANC visits and 5,342 ANC revisits. During the intervention period, 35,910 (98.3%) households were visited with 1,934 new ANC visits and 5,904 ANC revisits. Uptake of IPTp1 increased from 83.6% to 92.6%; IPTp2 from 73.5% to 87%; and IPTp3 from 51.9% to 75.4%.
Enhanced supervision of CHVs by CHAs to conduct and improve household visits enabled identification and referral of ANC defaulters and contributed to increased IPTp uptake. Supportive supervision and optimal CHU coverage in tracking pregnant women if conducted routinely may provide accurate denominators to track IPTp coverage and inform targeted interventions.
Authors and Affiliations
Donald Apat1, Willis Akhwale1, Moses Kidi1, Edwin Onyango2, James Andati1, Hellen Gatakaa1, Augustine Ngindu1, Lolade Oseni3, Gladys Tetteh3, Daniel Wacira4
1PMI-Impact Malaria, Nairobi, Kenya, 2Department of Health, Busia County, Kenya, 3Jhpiego, Baltimore, MD, United States, 4PMI, Nairobi, Kenya
CHW &Community &IPTp &Malaria in Pregnancy Bill Brieger | 16 Nov 2020
Community health workers’ sex and variation in uptake of malaria in pregnancy services in Ebonyi State, Nigeria

Ebonyi members of Integrated Health Data Management Team (IHDTM) providing mentorship to HCWs during RDQA visit to Akpaka
Bartholomew Odio et al. work with CHWs who promote community delivery of intermittent preventive treatment for pregnant women in Ebonyi State, Nigeria for the UNITAID/Jhpiego TiPToP Project. They shared below some of their findings from the virtual 69th Annual Meeting of American Society of Tropical Medicine and Hygiene this week. (Photos are from Bright Orji)
In Nigeria, malaria remains a high burden disease and pregnant women are among the most vulnerable. According to the 2019, World Malaria Report only 31% of pregnant women received the World Health

CHWs at data validation meeting during COVID 19 pandemic social distancing
Organization recommended minimum of three doses of IPTp with Sulfadoxine-Pyrimethamine (SP) compared to 17% in Nigeria (DHS, 2018). In order to expand the coverage of this life-saving intervention, the Transforming Intermittent Preventive Treatment for Optimal Pregnancy project engaged community health workers (CHWs) to introduce the delivery of community IPTp (C-IPTp) to eligible pregnant women, in addition to women being able to access IPTp at antenatal care in Ohaukwu district of Ebonyi State, Nigeria.

Community meeting in Bosso
As findings from studies in Nepal and Uganda showed that the sex of CHWs were correlated with uptake of iCCM services, we examined routine project data to determine if the sex of the CHWs was correlated with uptake of IPTp. Of the 462 CHWs selected, 49% were male and 51% were female and were deployed at a ratio of one CHW to 27 pregnant women. All CHWs were trained on early identification of pregnant women, referral to antenatal care and provision of C-IPTp using SP.
A trained data analyst extracted routine data from the national community health management information system for 13,733 pregnant women who received IPTp from CHWs between June and November 2019. Data abstracted included CHW sex and number of PW that received IPTp. Findings showed that female CHWs distributed 60% of IPTp1, 65% IPTp2, and 61% IPTp3 (p-value=0.00 for all comparisons). The data suggest that trained female CHWs may reach more pregnant women than their male counterparts in community directed IPTp interventions.
Authors and Affiliations
Bartholomew Odio(1), Onyinye Udenze(1), Chinyere Nwani(1), Herbert Onuoha(1), Elizabeth Njoku(1), Lawrence Nwankwo(2), Oniyire Adetiloye(1), Bright Orji(1) 1.Jhpiego, Nigeria, Abuja, Nigeria, 2.State Ministry of Health, Nigeria, Abuja, Nigeria. This is part of the TiPToP Project funded by UNITAID.
Antenatal Care (ANC) &IPTp &Malaria in Pregnancy Bill Brieger | 16 Nov 2020
Achieving antenatal care attendance and intermittent preventive treatment in pregnancy in Geita, Tanzania
Ryan Lash and colleagues examined factors associated with achieving antenatal care (ANC) attendance and intermittent preventive treatment in pregnancy (IPTp) and made recommendations in Geita Region, Tanzania, 2019. There findings are being presented at the virtual 69th Annual Meeting of American Society of Tropical Medicine and Hygiene.
Malaria in pregnancy results in an estimated 10,000 maternal and 100,000 infant deaths globally each year. To reduce this burden, the World Health Organization (WHO) recommends pregnant women in high to moderate malaria transmission areas receive at least 3 doses of intermittent preventive treatment in pregnancy (IPTp3) with sulfadoxine-pyrimethamine (SP) starting in the second trimester as part of routine antenatal care (ANC). Tanzania has national coverage goals of 80% coverage for women receiving IPTp3 and at least four ANC visits (ANC4).
 We surveyed women 15-49 years who had given birth in the last 12 months from randomly selected households across 40 communities in Geita Region, Tanzania. ANC attendance and IPTp uptake was recorded from respondent ANC cards if available, or self-reported. Predictors of ANC4 and IPT3 uptake were identified using logistic regression modeling, accounting for clustering and controlling for gravidity.
We surveyed women 15-49 years who had given birth in the last 12 months from randomly selected households across 40 communities in Geita Region, Tanzania. ANC attendance and IPTp uptake was recorded from respondent ANC cards if available, or self-reported. Predictors of ANC4 and IPT3 uptake were identified using logistic regression modeling, accounting for clustering and controlling for gravidity.
Of 1,111 women surveyed, 505 (51.9%) received IPTp3 and 472 (43.4%) achieved ANC4. Among women who achieved ANC4, 295 (62.5%) received IPTp3. IPTp3 was associated with basic knowledge about ANC and IPTp (aOR 2.4, CI 1.9 -3.1), initiating ANC <20 weeks (aOR 1.7, CI 1.3-2.3), waiting at the facility for <120 minutes (aOR 1.4, CI 1.1-1.9), and receiving advice from a health worker about SP (aOR 1.7, CI 1.3-2.2).
ANC4 was associated with better access to care (aOR 1.9, CI 1.3-2.8, for travelling <3.75 km to ANC and aOR 1.9, CI 1.1-2.2, for waiting <90 minutes for the provider), initiating ANC at <20 weeks gestation (aOR 10.7, CI 8.2-14.1), and basic knowledge about ANC and IPTp (aOR 1.4, CI 1.0-1.9). Poor access to care and late initiation of ANC reduced the likelihood that women will attend 4 ANC visits. Knowledge was a predictor of both ANC attendance and IPTp uptake; increasing women’s health literacy may overcome some of the barriers associated with retention in ANC.
New approaches to delivering ANC that focus on improving knowledge and the experience of care among ANC clients could help close coverage gaps for ANC4 and IPTp3 in Tanzania
Authors and Affiliations
R. Ryan Lash(1), Ruth Lemwayi(2), Melkior Assenga(2), Alen Kinyina(2), Annette Almeida(2), Samwel L. Nhiga(3), Lia Florey(4), Chonge Kitojo(5), Erik Reaves(6), Miriam Kombe(5), Ally Mohamed(3), Japhet Simeo(7), Stephanie Suhowatsky(8), Mary Drake(2), Julie Gutman(1) 1.US Centers for Disease Control and Prevention, Atlanta, GA, United States, 2.Jhpiego Tanzania, Dar es Salaam, Tanzania, United Republic of, 3.National Malaria Control Program, Tanzania, Dar es Salaam, Tanzania, United Republic of, 4.US Agency for International Development, Washington, DC, United States, 5.US President’s Malaria Initiative / US Agency for International Development Tanzania, Dar es Salaam, Tanzania, United Republic of, 6.US Centers for Disease Control and Prevention / US President’s Malaria Initiative Tanzania, Atlanta, GA, United States, 7.Regional Medical Office, Geita, Geita, Tanzania, United Republic of, 8.Jhpiego, Baltimore, MD, United States
Communication &Health Workers &IPTp &ITNs &Malaria in Pregnancy Bill Brieger | 16 Nov 2020
Provider Communication about IPTp and ITNs for Pregnant Women in Tanzania
Courtney Emerson and co-workers address the issues of Intermittent Preventive Treatment of Malaria with Sulfadoxine Pyrimethamine and Provision of Insecticide Treated Nets in Geita, Tanzania: Provider Communication and Opportunities at the virtual 69th Annual Meeting of American Society of Tropical Medicine and Hygiene. See their findings below.
 Intermittent preventive treatment of malaria in pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP) is a life-saving intervention to reduce morbidity and mortality among pregnant women and their infants. Additionally, provision and use of insecticide treated nets (ITNs) to prevent malaria is critical to improving pregnancy outcomes.
Intermittent preventive treatment of malaria in pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP) is a life-saving intervention to reduce morbidity and mortality among pregnant women and their infants. Additionally, provision and use of insecticide treated nets (ITNs) to prevent malaria is critical to improving pregnancy outcomes.
To assess implementation of malaria in pregnancy services and related health communications, we surveyed 1111 women who had delivered a live born infant in the preceding 12 months (recently pregnant women), as well as 1194 adults from randomly selected households without a recently pregnant woman in Geita Region, Tanzania in 2019. Most (88.2%) recently pregnant women reported receiving any IPTp dose; 45.5% received 3 doses. 72.3% of women received their first dose in the second trimester, as recommended by national guidelines, but only 14.4% received IPTp in the 4th month; 20.3% of women did not receive IPTp until third trimester.
There was a significant difference between ITN ownership and use among households (HH) with and without a recent pregnancy: ownership of at least one net was 95.2% vs 87.9%, respectively (p<0.0001), and use was 90% vs 77.8%, respectively (p<.0001). Despite this, few HHs had enough ITNs to cover all residents; on average, HHs had 1 ITN for every 3 rather than every 2 people, as recommended. Notably, only 21.2% and 26.2% of HH with and without a recent pregnancy had sufficient ITNS (p=0.005), despite 87.3% of recently pregnant women receiving an ITN during their last pregnancy.
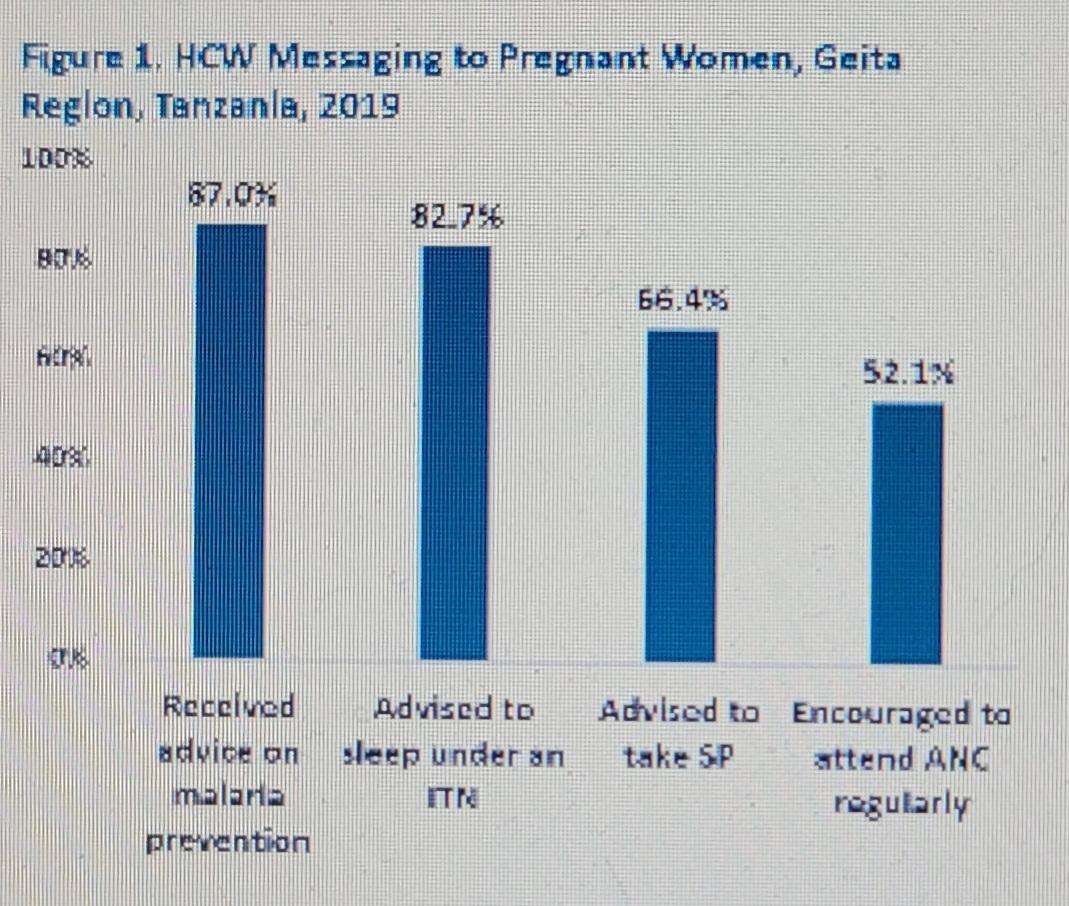 Of recently pregnant women, 87% received advice on preventing malaria from a health worker. Of these, 82.7% were advised to sleep under an ITN, but only 66.4% were advised to take SP, and 52.1% to attend ANC regularly. Although uptake of any IPTp was high, there are critical messages that need to be more consistently communicated to pregnant women by ANC providers including the importance of attending ANC regularly during pregnancy. To improve outcomes among pregnant women, additional net distribution may be warranted due to the unexpectedly low access.
Of recently pregnant women, 87% received advice on preventing malaria from a health worker. Of these, 82.7% were advised to sleep under an ITN, but only 66.4% were advised to take SP, and 52.1% to attend ANC regularly. Although uptake of any IPTp was high, there are critical messages that need to be more consistently communicated to pregnant women by ANC providers including the importance of attending ANC regularly during pregnancy. To improve outcomes among pregnant women, additional net distribution may be warranted due to the unexpectedly low access.
Authors and Affiliations
Courtney Nicole Emerson(1), Ryan Lash(1), Ruth Lemwayi(2), Melkior Assenga(2), Alen Kinyina(2), Annette Almeida(2), Samwel L. Nhiga(3), Lia Florey(4), Chonge Kitojo(5), Erik Reaves(6), Miriam Kombe(5), Peter Winch(7), Stephanie Suhowatsky(7), Mary Drake(2), Julie Gutman(1) 1.US Centers for Disease Control and Prevention, Atlanta, GA, United States, 2.Jhpiego, Dar es Salaam, United Republic of Tanzania, 3.National Malaria Control Program, Tanzania, Dar es Salaam, United Republic of Tanzania, 4.US Agency for International Development (USAID), Washington DC, DC, United States, 5.US Agency for International Development (USAID), Dar es Salaam, United Republic of Tanzania, 6.US Centers for Disease Control and Prevention, Dar es Salaam, United Republic of Tanzania, 7.Jhpiego, Baltimore, MD, United States
IPTp &ITNs &Malaria in Pregnancy Bill Brieger | 16 Nov 2020
Scoping Review of the Key Determinants and Indicators of Malaria in Pregnancy, Madagascar (2010-2019)
This year the 69th Annual Meeting of American Society of Tropical Medicine and Hygiene is virtual. Catherine Dentinger and colleagues (see authors below) gathered information to guide partner planning to combat malaria in pregnancy in Madagascar. Here are their findings.
 Malaria in pregnancy (MIP) increases the risk of poor maternal and infant outcomes; to prevent this, the World Health Organization (WHO) recommends insecticide-treated net (ITN) use, intermittent preventive treatment during pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP), and prompt case management. In Madagascar, IPTp uptake remains low; 10% of targeted women receive 3 doses.
Malaria in pregnancy (MIP) increases the risk of poor maternal and infant outcomes; to prevent this, the World Health Organization (WHO) recommends insecticide-treated net (ITN) use, intermittent preventive treatment during pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP), and prompt case management. In Madagascar, IPTp uptake remains low; 10% of targeted women receive 3 doses.
To determine if additional data are needed to improve MIP activities, we conducted a scoping review to identify barriers to antenatal care (ANC) and IPTp uptake. We searched PubMed, Google Scholar and USAID’s files (Development Experience Catalog) using the terms “Madagascar” and “pregnancy” and “malaria” and collected materials from stakeholders. We included English and French documents from 2010 to 2019 with quantitative or qualitative data regarding malaria during pregnancy.
 Documents were reviewed and categorized as MIP background information, care seeking, and facility readiness. Of 69 project reports, surveys and published articles, 15 (22%) met the inclusion criteria; 4 (27%) were categorized as care seeking, 4 (27%) as background, and 7 (47%) as facility readiness.
Documents were reviewed and categorized as MIP background information, care seeking, and facility readiness. Of 69 project reports, surveys and published articles, 15 (22%) met the inclusion criteria; 4 (27%) were categorized as care seeking, 4 (27%) as background, and 7 (47%) as facility readiness.
Eight (53%) articles mentioned SP stock outs, 3 (20%) mentioned poor provider knowledge of IPTp guidelines despite recent training, and 5 (33%) discussed barriers to ANC including distance, wait times, poor service quality, cost, and unfriendly providers. One study found only 30% of targeted health workers received recommended supervision. A 2015 survey of 52 health facilities revealed limited access to ANC due to financial and geographic barriers; 2018 surveys revealed similar findings. Self-treatment and care-seeking delays were reported even when distance was not a barrier.
Our review revealed well-documented barriers to MIP services that could be mitigated by reducing stock outs, improving access to healthcare by removing fees and providing services closer to women’s homes, and targeted behavior change. These findings can be used to guide coordinated donor and government efforts to address management, financial, and human resource gaps to improve MIP services.
Authors and Affiliations
Catherine Dentinger(1), Natasha Hansen(2), Susan Youll(2), Annett Cotte(1), Mary Lindsay(3), Chiarella Matten(4), Vololoniala Aimee Ravaoarinosy(5). 1.Centers for Disease Control and Prevention, Atlanta, GA, United States, States, 3.US Agency for International Development, Washington, DC, United States, 4.Institut Pasteur de Madagascar, Antananarivo, Madagascar, 5.National Malaria Control Program, Antananarivo, Madagascar 2.US Agency for International Development, Washington DC, DC, United States