Case Management &Community &ITNs &Training Bill Brieger | 15 Nov 2017
Community Based Intervention in Malaria Training in Myanmar
 Nu Nu Khin of Jhpiego who is working on the US PMI “Defeat Malaria Project” led by URC shares observations on the workshop being held in Yangon with national and regional/state malaria program staff to plan how to strengthen malaria interventions at the community level. The workshop has adapted Jhpiego’s Community Directed Intervention training package to the local setting.
Nu Nu Khin of Jhpiego who is working on the US PMI “Defeat Malaria Project” led by URC shares observations on the workshop being held in Yangon with national and regional/state malaria program staff to plan how to strengthen malaria interventions at the community level. The workshop has adapted Jhpiego’s Community Directed Intervention training package to the local setting.
 Yesterday’s opening speech was being hailed as a significant milestone to give Community-Based Intervention (CBI) training teams the knowledge, skills, and attitudes they need to effectively provide quality malaria services and quality malaria information.
Yesterday’s opening speech was being hailed as a significant milestone to give Community-Based Intervention (CBI) training teams the knowledge, skills, and attitudes they need to effectively provide quality malaria services and quality malaria information.
 This core team is going to train the critical groups of community-level implementers including CBI focal persons and malaria volunteers at the community level.
This core team is going to train the critical groups of community-level implementers including CBI focal persons and malaria volunteers at the community level.
We embarked this important step yesterday with the collaboration of Johns Hopkins University, Myanmar Ministry of Health and Sports, and World Health Organization Myanmar.
 Participants will be developing action plans to apply the community approach to malaria efforts in townships and villages in three high transmission Rakhine State, Kayin State and Tanintharyi Region.
Participants will be developing action plans to apply the community approach to malaria efforts in townships and villages in three high transmission Rakhine State, Kayin State and Tanintharyi Region.
Health Workers &IPTp &Malaria in Pregnancy Bill Brieger | 09 Nov 2017
Improving intermittent preventive treatment for pregnant women (IPTp) coverage in 5 districts in Chad and Cameroon
 Kodjo Morgah and Naibei Mbaïbardoum of Jhpiego with support from the ExxonMobil Foundation ave been working to increase interventions that protect pregnant women from malaria. The results below were shared at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Kodjo Morgah and Naibei Mbaïbardoum of Jhpiego with support from the ExxonMobil Foundation ave been working to increase interventions that protect pregnant women from malaria. The results below were shared at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Malaria is the leading cause of morbidity and mortality in Cameroon and Chad, where an estimated 500,000 and 1.5 million cases occur every year, respectively. In Cameroon, 55% of hospitalizations and 241 deaths among pregnant women reported in 2010 were due to malaria. In Chad, malaria accounted for 30% of hospital admissions and 41% of deaths among pregnant women in 2013.
 To improve uptake of intermittent preventive treatment for pregnant women (IPTp) for malaria in 5 districts in Chad and the Kribi district of Cameroon, Jhpiego adopted strategies targeting the 4 levels of the health system in each country: updating national policies and guidelines, building capacity of providers, building community health workers’ (CHWs) capacity, and engaging in behavior change communication.
To improve uptake of intermittent preventive treatment for pregnant women (IPTp) for malaria in 5 districts in Chad and the Kribi district of Cameroon, Jhpiego adopted strategies targeting the 4 levels of the health system in each country: updating national policies and guidelines, building capacity of providers, building community health workers’ (CHWs) capacity, and engaging in behavior change communication.
 Nationally, Jhpiego provided technical guidance to the Ministries of Health to develop tools including: training and malaria in pregnancy (MIP) reference manuals for providers and CHWs, guidelines on IPTp, and key supervision and data collection tools. At the regional/district levels, 38 supervisors were trained, and they conducted 248 supervisory visits in both countries, reaching 137 health facilities.
Nationally, Jhpiego provided technical guidance to the Ministries of Health to develop tools including: training and malaria in pregnancy (MIP) reference manuals for providers and CHWs, guidelines on IPTp, and key supervision and data collection tools. At the regional/district levels, 38 supervisors were trained, and they conducted 248 supervisory visits in both countries, reaching 137 health facilities.
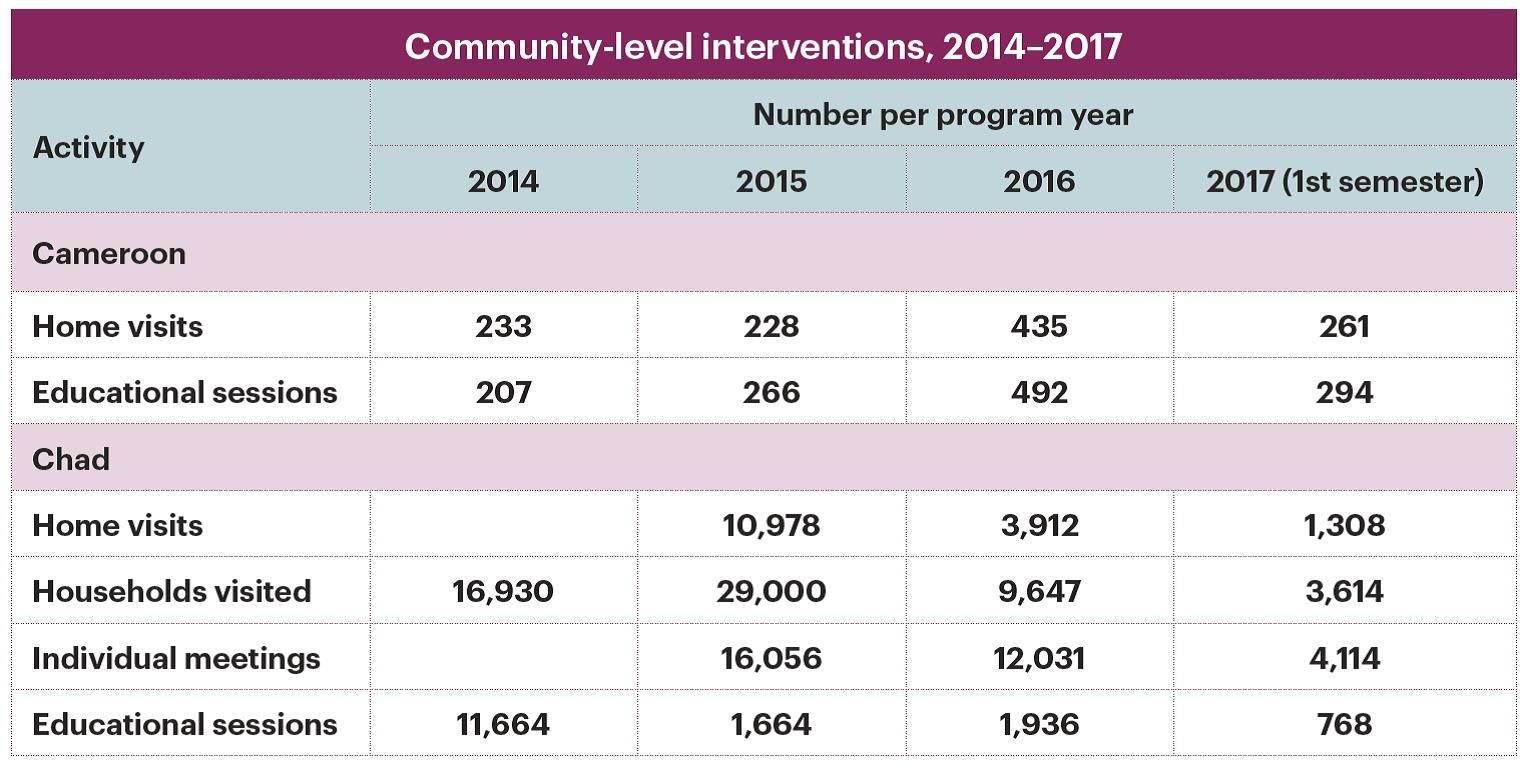
 At the facility level, 234 providers were trained in malaria prevention and management, MIP, data collection and commodity management. At the community level, 146 CHWs in both countries were trained to raise awareness on malaria prevention and control.
At the facility level, 234 providers were trained in malaria prevention and management, MIP, data collection and commodity management. At the community level, 146 CHWs in both countries were trained to raise awareness on malaria prevention and control.
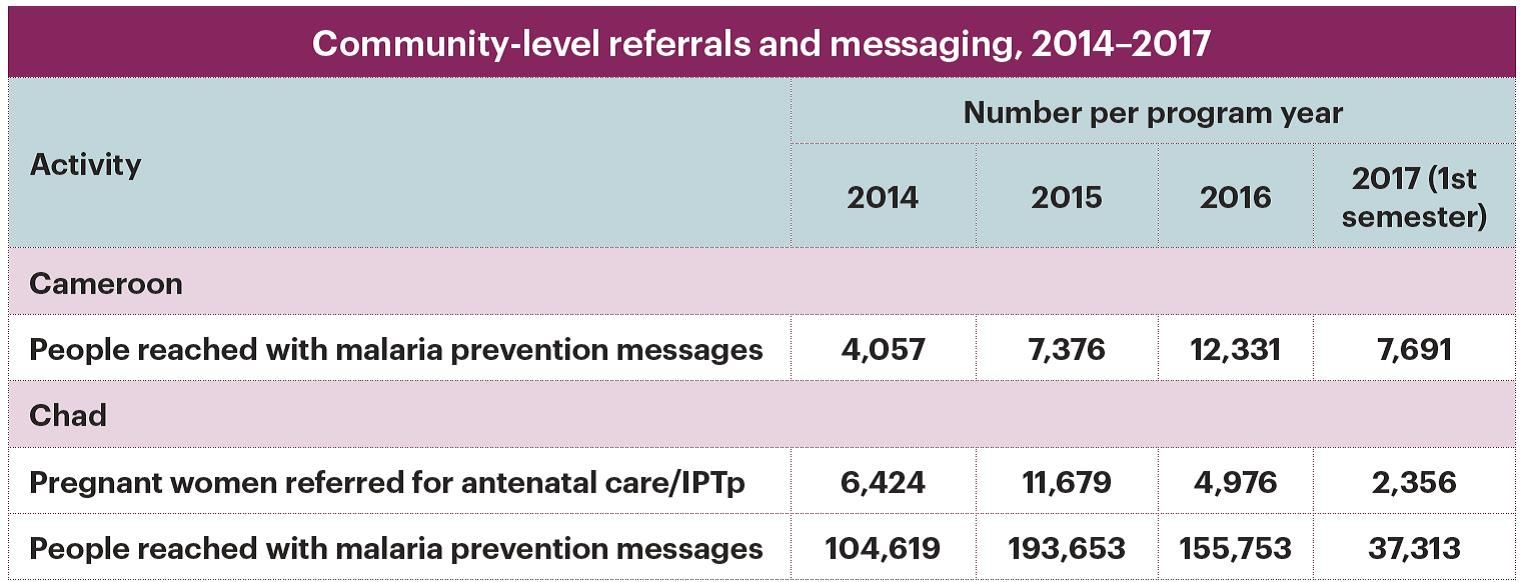
 In Chad, CHWs referred 6424 pregnant women for antenatal care/IPTp and 11679 pregnant women for malaria treatment in 2014 and 2015. Health facility and CHW data collection tools were revised and monthly validation of district data was implemented to improve data reliability, completeness, and readiness.
In Chad, CHWs referred 6424 pregnant women for antenatal care/IPTp and 11679 pregnant women for malaria treatment in 2014 and 2015. Health facility and CHW data collection tools were revised and monthly validation of district data was implemented to improve data reliability, completeness, and readiness.
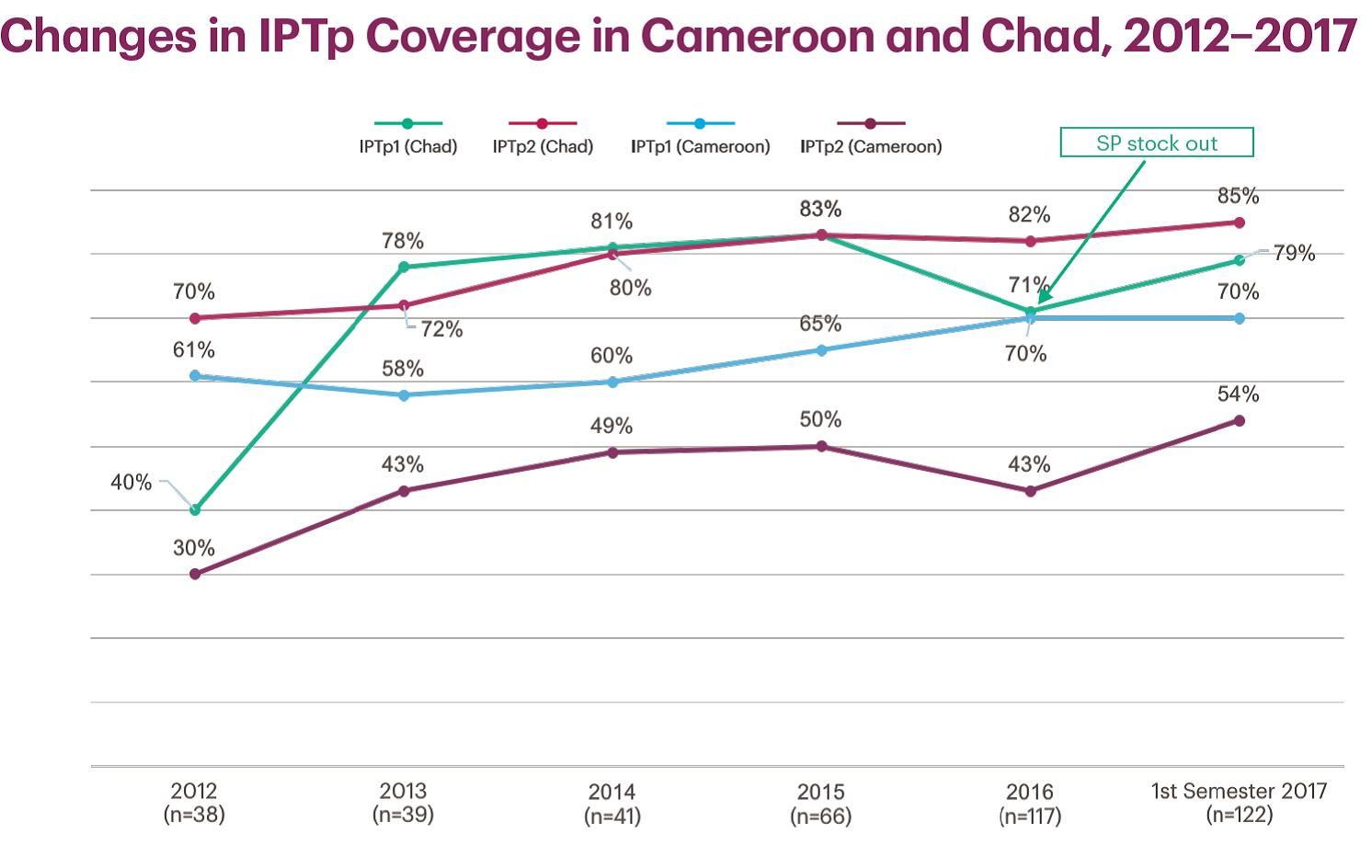
As a result of Jhpiego’s activities in Kribi, IPTp rates increased from the start of the project in 2012 to 2015: from 70% to 83% (IPTp1), 61% to 80% (IPTp2), and 12.7% to 28.1% (IPTp3). Similarly, from 2012 to 2015 in Chad, IPTp1 rates increased from 40% to 83% and from 30% to 50% for IPTp2. These gains are a result of training paired with coaching and supervision activities of trained providers and targeted facilities.
Health Workers &IPTp &Malaria in Pregnancy &Performance &Quality of Services Bill Brieger | 09 Nov 2017
Results of an evaluation of the Toolkit to Improve Early and Sustained Intermittent Preventive Treatment in Pregnancy (IPTp) Uptake in Mozambique and Madagascar
 Lalanirina Ravony, Elana Fiekowsky, Lisa Noguchi, Patricia P. Gomez, Jean Pierre Rakotovao, Eliane Razafimandimby, Armindo Tiago, Kathryn Smock, Arsene Ratsimbarisoa, Kristen Vibbert, and Robert Sellke shared their efforts to apply a toolkit to enable health providers to ensure better uptake of intermittent preventive treatment for malaria during antenatal clinics. As seen below, they presented their findings at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Lalanirina Ravony, Elana Fiekowsky, Lisa Noguchi, Patricia P. Gomez, Jean Pierre Rakotovao, Eliane Razafimandimby, Armindo Tiago, Kathryn Smock, Arsene Ratsimbarisoa, Kristen Vibbert, and Robert Sellke shared their efforts to apply a toolkit to enable health providers to ensure better uptake of intermittent preventive treatment for malaria during antenatal clinics. As seen below, they presented their findings at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
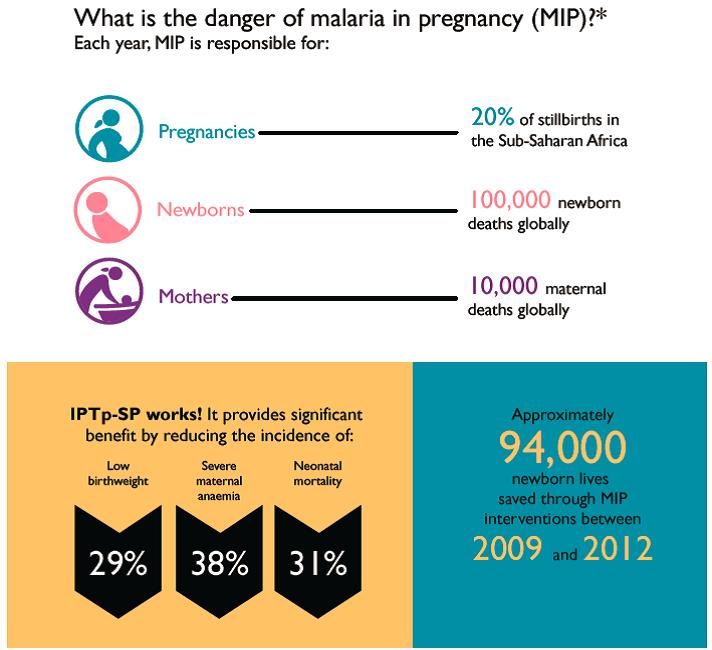
Malaria in pregnancy (MIP) is a leading cause of maternal and newborn morbidity and mortality; however uptake of intermittent preventive treatment in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP), an effective prevention tool, remains alarmingly low across sub-Saharan Africa, including Mozambique and Madagascar.
 The WHO 2012 policy recommendations to prevent MIP include early enrollment into antenatal care (ANC), accurate estimation of gestational age (GA) and administration of IPTp-SP during ANC visits beginning early in the second trimester, spaced at least one month apart. Preventing MIP remains a challenge in settings with inconsistent application of these recommendations and inadequate provider training in estimating GA.
The WHO 2012 policy recommendations to prevent MIP include early enrollment into antenatal care (ANC), accurate estimation of gestational age (GA) and administration of IPTp-SP during ANC visits beginning early in the second trimester, spaced at least one month apart. Preventing MIP remains a challenge in settings with inconsistent application of these recommendations and inadequate provider training in estimating GA.
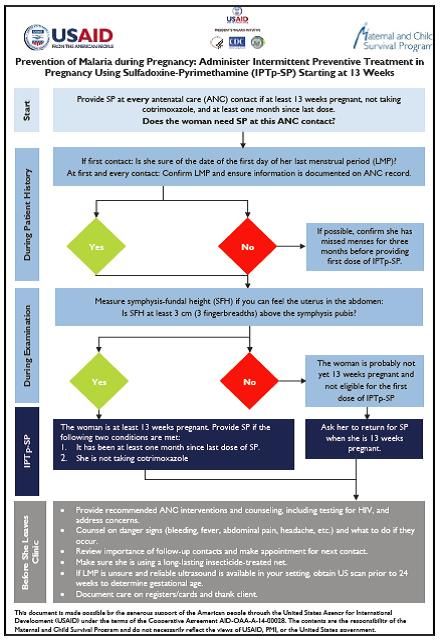 To improve adherence to these recommendations, a toolkit was designed which includes a job aid with an algorithm to guide providers during ANC visits to determine IPTp-SP eligibility. Twenty-four providers from 24 facilities in Madagascar and 29 providers from seven facilities in Mozambique were trained on use of the job aid and interviewed three months later about their experience.
To improve adherence to these recommendations, a toolkit was designed which includes a job aid with an algorithm to guide providers during ANC visits to determine IPTp-SP eligibility. Twenty-four providers from 24 facilities in Madagascar and 29 providers from seven facilities in Mozambique were trained on use of the job aid and interviewed three months later about their experience.
Individual providers were interviewed using a questionnaire to assess the clarity and utility to the job aid, and their opinions of the practicality of the orientation. Interviewers also gathered information on years of experience and clinical certification. All providers reported that the job aid reminded them to estimate GA and measure fundal height, which is particularly helpful since few women remember the date of their last menstrual period (LMP).
 Health workers also reported that the job helped them encourage the use of long-lasted insecticide treated nets, and reminded them of the proper timing to start IPTp-SP. We conclude that the toolkit is useful to prompt providers to calculate GA and offer IPTp as early as possible in the second trimester.
Health workers also reported that the job helped them encourage the use of long-lasted insecticide treated nets, and reminded them of the proper timing to start IPTp-SP. We conclude that the toolkit is useful to prompt providers to calculate GA and offer IPTp as early as possible in the second trimester.
Future potential directions include revision of all Toolkit components to reflect input from this evaluation, including development of a wall poster version to enhance readability, and inclusion of a pregnancy wheel to facilitate calculation of GA and estimated date of delivery.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Uncategorized Bill Brieger | 09 Nov 2017
A New Approach for provider performance improvement with Clinical and Quality Assurance Components in Moramanga, Madagascar
Norohaingo Andrianaivo, Eliane Razafimandimby, Jean Pierre Rakotovao, Marc Eric Rajaonarison Razakariasy, and Lalanirina Ravony share their presentation on ensuring standardized malaria in pregnancy service delivery in Madagascar. The poster was viewed at the 66th Annual Meeting of the American Society of Tropical
 Malaria is endemic in 90% of Madagascar. However, the entire population is considered to be at risk for the disease, with pregnant women particularly vulnerable. Madagascar adopted the IPT in pregnancy policy in 2004.
Malaria is endemic in 90% of Madagascar. However, the entire population is considered to be at risk for the disease, with pregnant women particularly vulnerable. Madagascar adopted the IPT in pregnancy policy in 2004.
The Malaria Indicator Survey in 2016 in Madagascar showed only 10% of Malagasy pregnant women receiving three doses of SP (IPT3). MCSP previously conducted health provider training in antenatal care in workshop style, with usually one provider per facility attending each training.
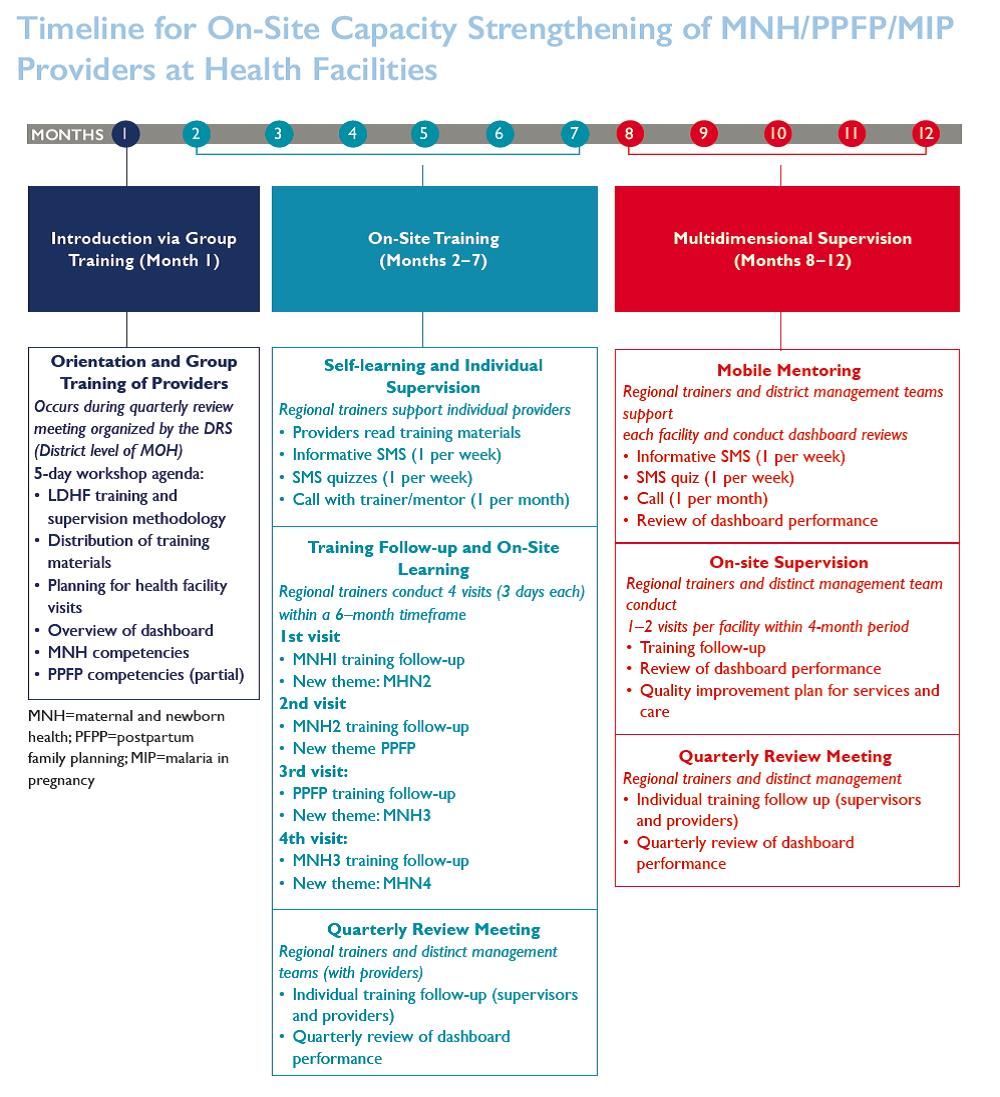 To increase the number of providers offering standardized service according to the new WHO recommendations for IPTp, in 2016 MCSP Madagascar began implementing a new low dose/high frequency training approach, with routine supportive supervision. On-site training and supportive supervision provide the opportunity for the trainer and providers to discuss the barriers to delivery of IPTp-SP.
To increase the number of providers offering standardized service according to the new WHO recommendations for IPTp, in 2016 MCSP Madagascar began implementing a new low dose/high frequency training approach, with routine supportive supervision. On-site training and supportive supervision provide the opportunity for the trainer and providers to discuss the barriers to delivery of IPTp-SP.
Additionally, with the addition of a new IPTp indicator in the facility dashboard, the trainer/supervisor can monitor the indicator, and discuss plan of action with providers as needed. To date, in Moramanga District, 16 providers in six facilities have benefited from this performance improvement approach.
 The qualitative and quantitative study of provider performance and results from January 2017 to May 2017 shows that Providers do follow the WHO’s new recommendations on IPT. Adequate action plans were implemented to prevent SP stock out and to commit community health workers.
The qualitative and quantitative study of provider performance and results from January 2017 to May 2017 shows that Providers do follow the WHO’s new recommendations on IPT. Adequate action plans were implemented to prevent SP stock out and to commit community health workers.
The increase of antenatal care utilization rate in these facilities. The IPT uptake increased This intervention is expected to show that IPT uptake and other maternal and newborn outcomes are improving in Madagascar.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Communication &Health Workers &IPTp &Malaria in Pregnancy Bill Brieger | 09 Nov 2017
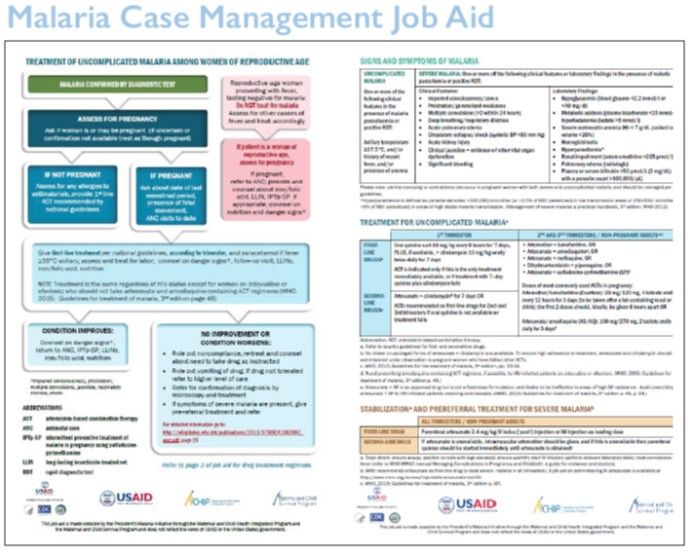
Results from a Formative Evaluation of the Malaria in Pregnancy Case Management Job Aid in Nigeria
Job Aids can provide valuable assistance to health workers, but it is important to evaluate if they serve the intended purpose. With support from USAID’s Maternal and Child Survival Program, Bright Orji, Enobong Ndekhedehe, Elana Fiekowsky, Patricia Gomez, Aimee Dickerson, Reena Sethi, Bibian Udeh, Kristin Vibbert, and Robert Sellke reported at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene on their evaluation of a Job Aid for Nigeria on the prevention of malaria in pregnancy as seen below.
 Annually, nearly 7 million pregnant women in Nigeria are at risk of malaria in pregnancy (MIP). Although antenatal care is the platform for the prevention and treatment of MIP, malaria is also treated at outpatient departments.
Annually, nearly 7 million pregnant women in Nigeria are at risk of malaria in pregnancy (MIP). Although antenatal care is the platform for the prevention and treatment of MIP, malaria is also treated at outpatient departments.
It is known that women of reproductive age (WRA) are often treated for malaria without assessing pregnancy status, although artemisinin combination therapies are contraindicated in the first trimester of pregnancy, and many pregnant women do not receive the recommended low cost interventions.
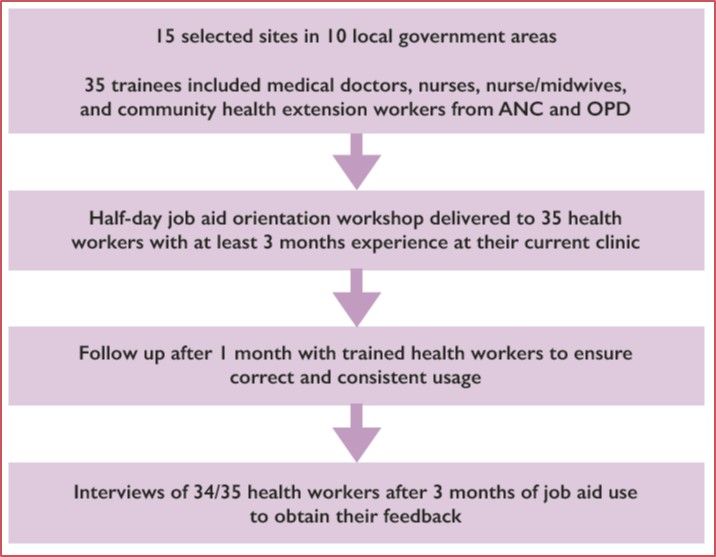 In order to increase access to these MIP interventions, the President’s Malaria Initiative supported the Maternal and Child Survival Program and partners to develop a two-page job aid for case management of uncomplicated malaria among WRA. In collaboration with the Nigeria Malaria Elimination Program, the job aid was evaluated in Ebonyi State, a high malaria burden area, to determine providers’ perceptions of its clarity, acceptability, and utility.
In order to increase access to these MIP interventions, the President’s Malaria Initiative supported the Maternal and Child Survival Program and partners to develop a two-page job aid for case management of uncomplicated malaria among WRA. In collaboration with the Nigeria Malaria Elimination Program, the job aid was evaluated in Ebonyi State, a high malaria burden area, to determine providers’ perceptions of its clarity, acceptability, and utility.
 A half-day workshop on use of the job aid was provided to 35 health workers (nurses – 20%; nurse-midwives – 20%; community health extension workers – 48%; and medical doctors – 12%) already trained on MIP case management, selected from 15 facilities where WRA seek care. After 3 months of use, a one-page questionnaire was administered to 34 health workers.
A half-day workshop on use of the job aid was provided to 35 health workers (nurses – 20%; nurse-midwives – 20%; community health extension workers – 48%; and medical doctors – 12%) already trained on MIP case management, selected from 15 facilities where WRA seek care. After 3 months of use, a one-page questionnaire was administered to 34 health workers.
One-hundred percent stated that the job aid helped them to do the following: identify pregnant women among the WCBA presenting with fever; use rapid diagnostic tests to diagnose malaria; and treat uncomplicated MIP. Sixty-eight percent used the job aid to provide correct treatment for severe malaria and 88% used it while providing services all or most of the time.
The results indicated that after a half-day orientation on use of the job aid, health workers were able to use it to help them identify women who may be pregnant and provide appropriate treatment for uncomplicated MIP. They are also able to explain its use to colleagues.
It is suggested that a poster-size version could be printed and disseminated to appropriate cadres of health workers in clinics where WRA seek care for fever, as it is anticipated that providers could benefit from its use.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Case Management Bill Brieger | 09 Nov 2017
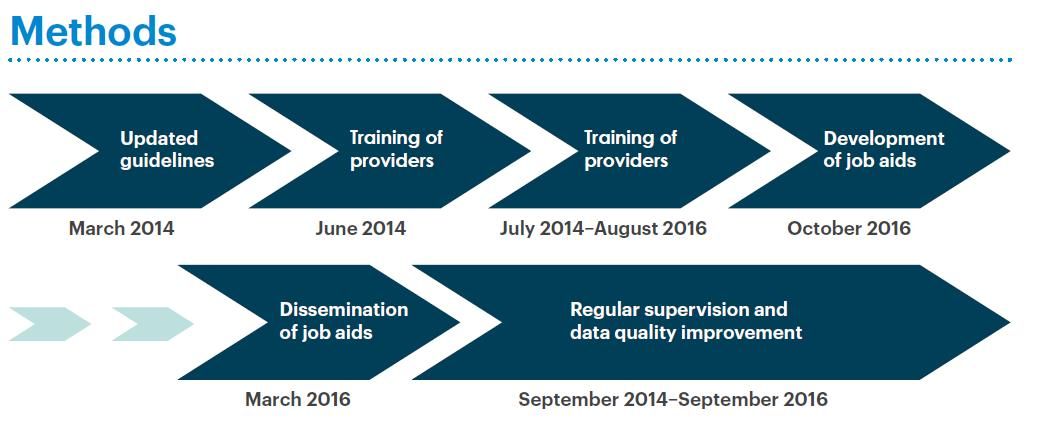
Contribution of the Improving Malaria Care (IMC) Project to Improving Malaria Case Management in Burkina Faso
 Malaria case management including diagnosis and treatment is an essential component of malaria control and elimination. Ousmane Badolo, Mathurin Dodo, and Bonkoungou Moumouni of Jhpiego working on the USAID Improving Malaria Care Project in Burkina Faso explained at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene how they worked to improve case management by Strengthening the capacity of health care providers. There findings follow:
Malaria case management including diagnosis and treatment is an essential component of malaria control and elimination. Ousmane Badolo, Mathurin Dodo, and Bonkoungou Moumouni of Jhpiego working on the USAID Improving Malaria Care Project in Burkina Faso explained at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene how they worked to improve case management by Strengthening the capacity of health care providers. There findings follow:
 Malaria kills mostly children under five and pregnant women in Burkina Faso, and is the leading reason for medical consultation and hospitalization. Improving case management is a real challenge in reducing morbidity and mortality. The goal of the National Malaria Control Program (NMCP) was to reduce the morbidity by 75% by end of 2000 and malaria mortality to close to zero by the end of 2015.
Malaria kills mostly children under five and pregnant women in Burkina Faso, and is the leading reason for medical consultation and hospitalization. Improving case management is a real challenge in reducing morbidity and mortality. The goal of the National Malaria Control Program (NMCP) was to reduce the morbidity by 75% by end of 2000 and malaria mortality to close to zero by the end of 2015.
 The United States Agency for International Development-supported Improving Malaria Care (IMC) project aims to reduce malaria morbidity and mortality. This includes strengthening the capacity of health providers to deliver high quality management- diagnosis and treatment, of malaria cases.
The United States Agency for International Development-supported Improving Malaria Care (IMC) project aims to reduce malaria morbidity and mortality. This includes strengthening the capacity of health providers to deliver high quality management- diagnosis and treatment, of malaria cases.
Between 2014 and 2016 IMC and the NMCP revised malaria guidelines, oriented 163 national trainers, trained 1,819 providers at all levels and organized supportive supervision of these staff. As a result correct diagnostic testing of malaria cases increased from 62% to 82%.
 The proportion of people with uncomplicated malaria who received artemisinin combination therapy (ACT) increased from 85% to 94%. Strengthening of the data management system facilitated this information to be collected.
The proportion of people with uncomplicated malaria who received artemisinin combination therapy (ACT) increased from 85% to 94%. Strengthening of the data management system facilitated this information to be collected.
Training these providers based on national guidelines and reinforcing their learning through supervision has enabled the NMCP to have a pool of health providers capable of treating the most vulnerable population and helping to reduce malaria mortality level in Burkina Faso.
 This training is accompanied by the implementation of formative supervision. Continued supervision and quality data management positions the NMCP to reach and document its goals.
This training is accompanied by the implementation of formative supervision. Continued supervision and quality data management positions the NMCP to reach and document its goals.
Funding for this effort was provided by the United States President’s Malaria Initiative. This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of the Improving Malaria Care Project and do not necessarily reflect the views of USAID or the United States Government.
Malaria in Pregnancy &Quality of Services Bill Brieger | 09 Nov 2017
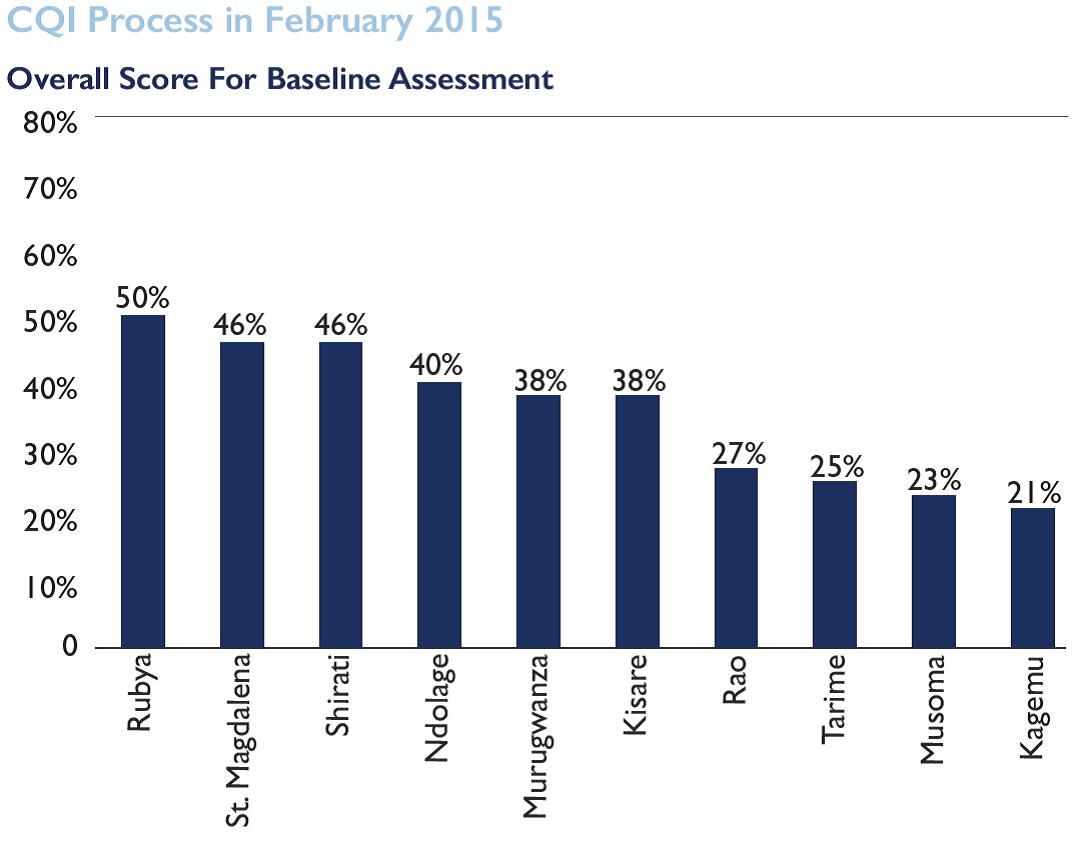
Using the Antenatal Care Quality Improvement Tool and targeted training to strengthen ANC Services including MiP in Tanzania
 Malaria prevention in pregnancy (MIP) is a major component of antenatal services in endemic countries. Jasmine Chadewa, Dunstan Bishanga, Elaine Roman, Godlisten Martin, Kristen Vibbert, Lauren Borsa, Agrey Mbilinyi, Jeremie Zoungrana, and Hussein Kidanto describe how they applied a quality improvement tool to strengthen ANC and MIP services at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings follow:
Malaria prevention in pregnancy (MIP) is a major component of antenatal services in endemic countries. Jasmine Chadewa, Dunstan Bishanga, Elaine Roman, Godlisten Martin, Kristen Vibbert, Lauren Borsa, Agrey Mbilinyi, Jeremie Zoungrana, and Hussein Kidanto describe how they applied a quality improvement tool to strengthen ANC and MIP services at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings follow:
Malaria in Pregnancy (MiP) is a major, preventable cause of maternal morbidity and poor birth outcomes. In collaborations with partners, Tanzania’s National Malaria Control Program (NMCP) and the Reproductive and Child Health Unit has been working to promote the World Health Organization’s three-pronged approach to address the burden of MiP.
 A malaria training for 180 supervisors and 360 ANC providers from 221 health facilities was conducted in the Kagera and Mara regions. Updates included an orientation on MiP as well as malaria case management, screening, data management and ITN promotion.
A malaria training for 180 supervisors and 360 ANC providers from 221 health facilities was conducted in the Kagera and Mara regions. Updates included an orientation on MiP as well as malaria case management, screening, data management and ITN promotion.
Prior to the training, facility baseline assessments were conducted using the Ministry of Health, Community Development, Gender, Elderly and Children (MOHCDGEC) antenatal care quality improvement (ANC QI) tool to identify gaps in knowledge and skills of health providers to better target trainings to improving the quality of ANC services.
A second assessment took place six months post training. Both assessments included hospital, health facility and dispensary levels and included observation, interviews, record reviews and skills assessments.
 Results demonstrated that over 90% of the facilities scored below 30% across all categories in the overall baseline assessment with a high score of 35 %, while the 2nd assessment showed a large improvement with 40% of the facilities scoring below 30% and a high score of 70%.
Results demonstrated that over 90% of the facilities scored below 30% across all categories in the overall baseline assessment with a high score of 35 %, while the 2nd assessment showed a large improvement with 40% of the facilities scoring below 30% and a high score of 70%.
The ANC QI tool is effective in determining the impact of ANC health provider’s knowledge and skills to target training to improve ANC service quality.
The presentation was made possible through support provided to the USAID Boresha Afya Project, under the terms of the Cooperative Agreement AID-621-A-16-00003 by the President’s Malaria Initiative via the United States Agency for International Development (USAID), an inter-agency agreement with Centers for Disease Control and Prevention (CDC). The opinions expressed herein are those of the author(s) and do not necessarily reflect the views of the President’s Malaria Initiative via the US Agency for International Development.
Health Workers &Quality of Services Bill Brieger | 09 Nov 2017
Strengthening Nursing & Midwifery Training Through Implementation of Continuous Quality Improvement Process in Tanzania
Annamagreth Mukwenda, John George, Mary Rose Giatas, Gustav Moyo, and Justine Ngenda have been promoting Continuous Quality Improvement and mentoring with nurses and midwives in Tanzania. They shared their experiences working with the Maternal and Child Survival Program and Tanzanian Government agencies at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
 Tanzania is one of the countries with critical shortage of human resource for health. The coverage of skilled birth attendants is about 50%, which connote sub-optimal quality of care contributing to poor neonatal and maternal outcomes.
Tanzania is one of the countries with critical shortage of human resource for health. The coverage of skilled birth attendants is about 50%, which connote sub-optimal quality of care contributing to poor neonatal and maternal outcomes.
 Training and deploying adequate numbers of competent health workers is one of the objectives of the Tanzania National Health Policy. The government of Tanzania and partners like Jhpiego led Maternal and Child Health Survival Program, are working to improve the training environment hence competent graduates.
Training and deploying adequate numbers of competent health workers is one of the objectives of the Tanzania National Health Policy. The government of Tanzania and partners like Jhpiego led Maternal and Child Health Survival Program, are working to improve the training environment hence competent graduates.
In support of quality trainings, Jhpiego in collaboration with the Ministry of Health are implementing the Continuous Quality Improvement (CQI) process which encourages health training institutions to improve quality teaching and learning by focusing on Classroom and Practical Instructions, Clinical instruction and practice, Institutional Infrastructure, Learning and Teaching Materials and Institutional Governance and Administration.
 A baseline assessment was done using the CQI guide in 10 training institutions to assess the quality of training and educational process, output and outcomes for the provision of quality nursing and midwifery care. Results indicated substandard outcomes with scores less than 50% at most schools.
A baseline assessment was done using the CQI guide in 10 training institutions to assess the quality of training and educational process, output and outcomes for the provision of quality nursing and midwifery care. Results indicated substandard outcomes with scores less than 50% at most schools.
All 10 schools were oriented on CQI process including its implementation. Quarterly assessment by a team comprised of institutions’ quality improvement teams, Ministry of Health and Jhpiego were done and gaps identified addressed through supportive supervision and mentorship.
 Training institution are progressively improving their training capabilities. The teaching learning environment has improved substantially with an average score 95% during external verification from 45% baseline score. After eighteen months of program implementation, three schools have been recognized for their outstanding performance and were presented with trophies and certificates as a motivation. This translates into increased number of skilled health care workers from rural nursing schools with required competency to avert maternal and neonatal deaths.
Training institution are progressively improving their training capabilities. The teaching learning environment has improved substantially with an average score 95% during external verification from 45% baseline score. After eighteen months of program implementation, three schools have been recognized for their outstanding performance and were presented with trophies and certificates as a motivation. This translates into increased number of skilled health care workers from rural nursing schools with required competency to avert maternal and neonatal deaths.
Case Management &Health Workers &IPTp &Quality of Services Bill Brieger | 08 Nov 2017
Contribution of the Standards-Based Management and Recognition (SBM-R) approach to fighting malaria in Burkina Faso
Quality improvement tools play an important role in ensuring better malaria services. Moumouni Bonkoungou, Ousmane Badolo, and Thierry Ouedraogo describe how

Standards Based Management and Recognition Approach to Quality Improvement
Jhpiego’s quality approach, Standards-Based Management and Recognition, was applied to enhancing the provision of malaria services in Burkina Faso at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their work was supported through the President’s Malaria Initiative and the USAID Improving Malaria Care Project.
In 2015, Burkina Faso recorded 8,286,463 malaria cases, including 450,024 severe cases with 5379 deaths. The main reasons for these death are: Inadequate application of national malaria diagnosis and treatment guidelines, delays in seeking health care and poor quality of case management.
The Standards-Based Management and Recognition (SBM-R) approach is used to improve quality of care using performance standards based on national guidelines. SBM-R includes the following steps:
- set performance standards
- implement the standards
- monitor progress and
- recognize as well as celebrate achievements
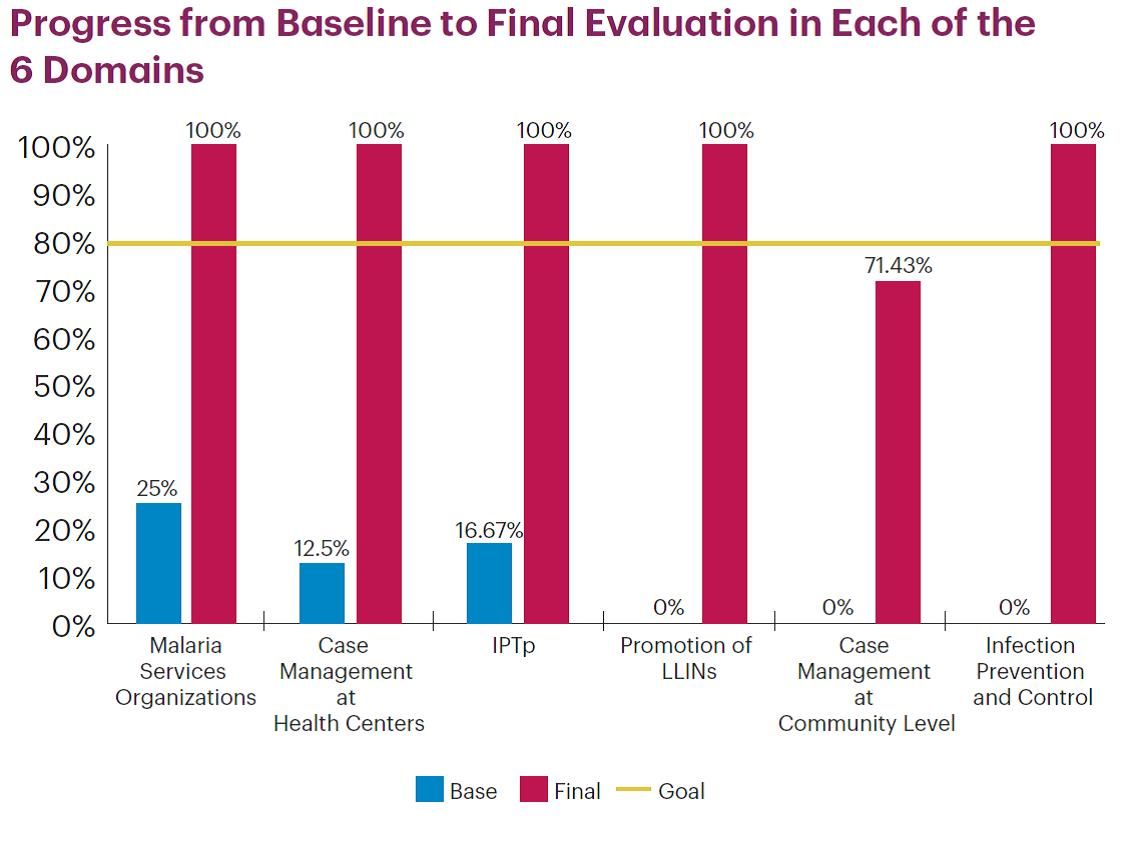 Areas or domains assessed by the approach are: services organization, case management at both health center and community, Intermittent Preventive Treatment in Pregnancy (IPTp), promotion of Long Lasting Insecticide treated Nets (LLIN) use and infection prevention and control.
Areas or domains assessed by the approach are: services organization, case management at both health center and community, Intermittent Preventive Treatment in Pregnancy (IPTp), promotion of Long Lasting Insecticide treated Nets (LLIN) use and infection prevention and control.
Since June 2016, 26 health facilities in three regions have been implementing SBMR. Therefore, 105 health workers have been trained. Performance progress was measured through 5 evaluations including baseline. Baseline has shown the highest score was 47% (Kounda) while the lowest was 9% (Niangoloko).
The main issues observed were: lack of program activities, management tools, handwashing facilities, LLINs and misuse of Rapid Diagnosis Tests. Their cause was determined and an improvement plan was developed by each site. The second, third and final evaluations revealed a change in performance scores for all sites.
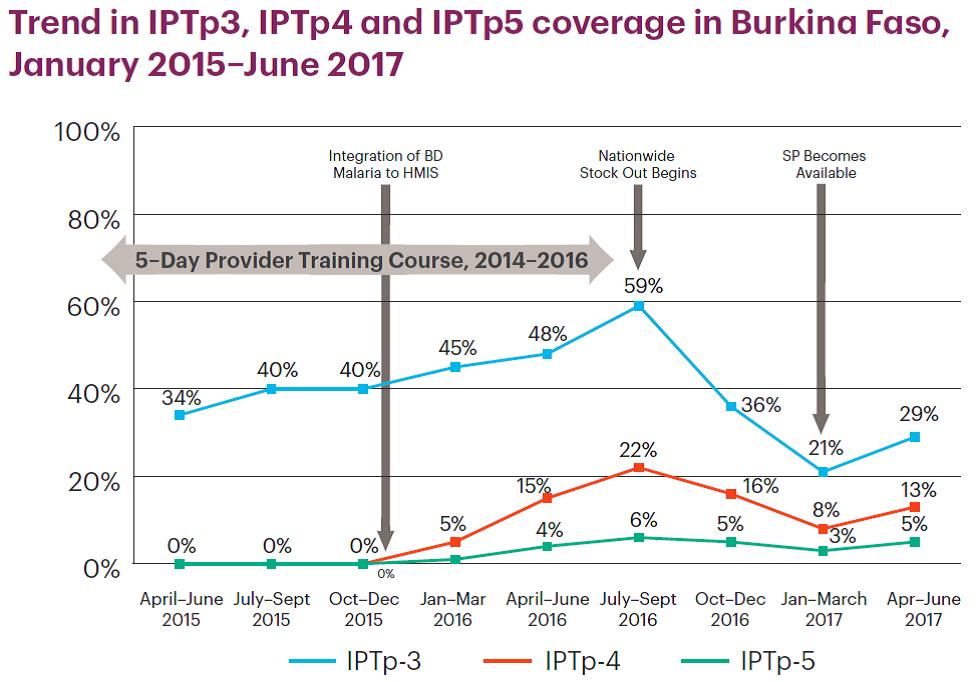
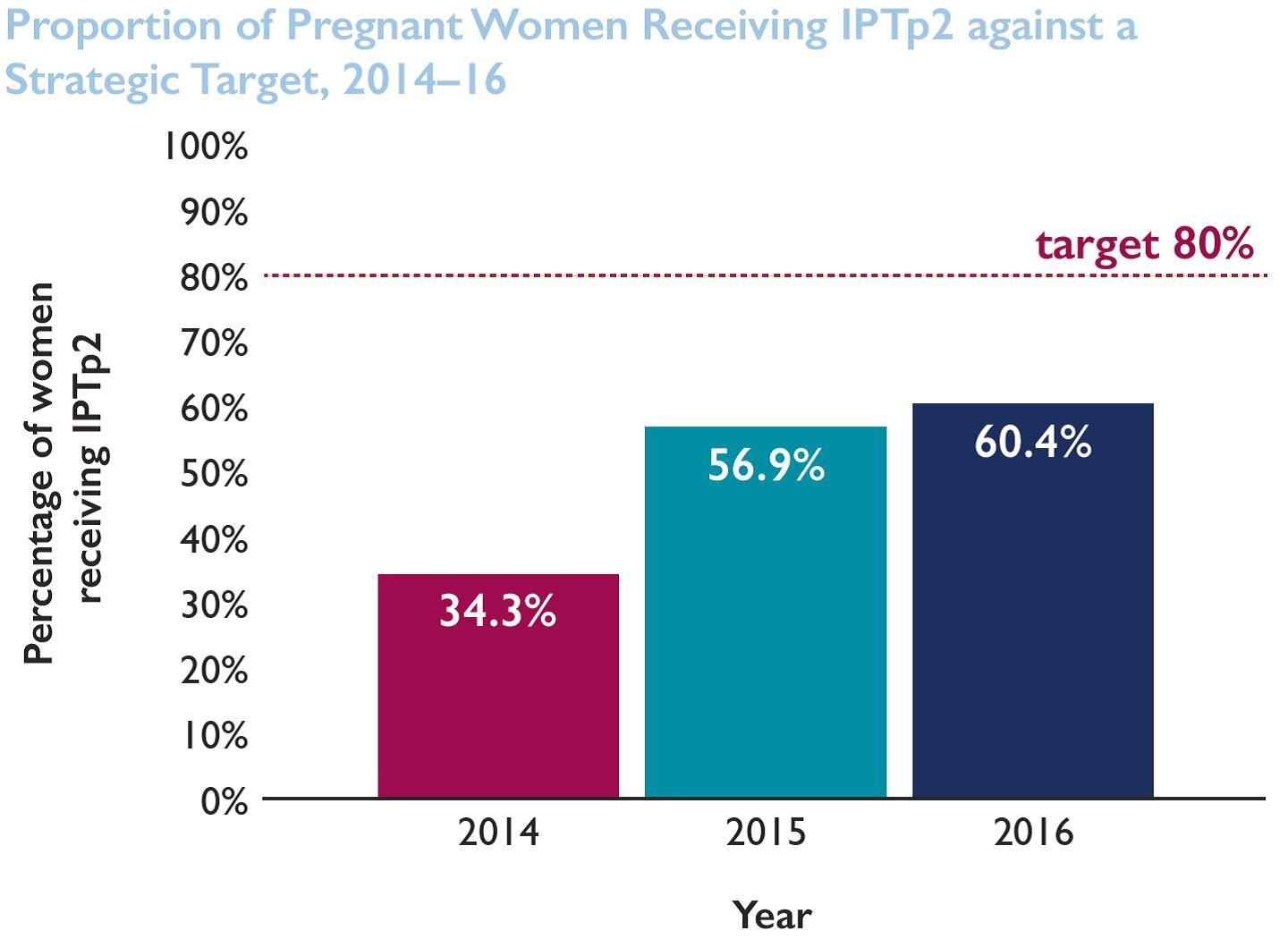
 The external evaluation showed 17 out of 26 health facilities with a score higher than 60%; among them 10 with a score above 80% (Bougoula, 94%). At the same time, IPTp 3 increased from 34.48% in 2014 to 78.38% in 2016 and no malaria death has been registered since October 2015.
The external evaluation showed 17 out of 26 health facilities with a score higher than 60%; among them 10 with a score above 80% (Bougoula, 94%). At the same time, IPTp 3 increased from 34.48% in 2014 to 78.38% in 2016 and no malaria death has been registered since October 2015.
For the site under 80% the key reasons were: staff turnover, commodities stock-out and lack of infrastructure. The process continues with recognition of health facilities and supporting others (those at less than 80%) to reach the desired performance level. The SBM-R approach appears to be a great tool for improving quality and performance of health facilities.
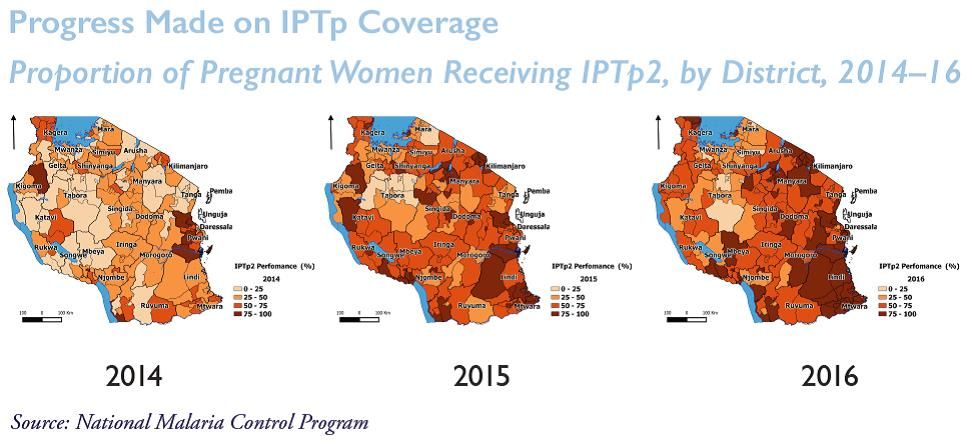
IPTp &Malaria in Pregnancy Bill Brieger | 08 Nov 2017
Missed Opportunities for Uptake of Intermittent Preventative Treatment for Malaria in Pregnancy in Tanzania
 A major reason that coverage targets for intermittent treatment of malaria in pregnancy fall short are missed opportunities at health service sites. Jasmine Chadewa, Yusuph Kulindwa, Dunstan Bishanga, Mary Drake, Jeremie Zoungrana, Elaine Roman, Hussein Kidanto, Naomi Kaspar, Kristen Vibbert, and Lauren Borsa share what they have learned about this issue at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
A major reason that coverage targets for intermittent treatment of malaria in pregnancy fall short are missed opportunities at health service sites. Jasmine Chadewa, Yusuph Kulindwa, Dunstan Bishanga, Mary Drake, Jeremie Zoungrana, Elaine Roman, Hussein Kidanto, Naomi Kaspar, Kristen Vibbert, and Lauren Borsa share what they have learned about this issue at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
 About 35 million people in Tanzania are at risk of malaria, with pregnant women and under five children being the most vulnerable. The Tanzania National Malaria Control Program’s (NMCP) Strategic Plan for 2007–2012 reports that malaria accounts for 30% of the national disease burden, with about 1.7 million cases per year among pregnant women.
About 35 million people in Tanzania are at risk of malaria, with pregnant women and under five children being the most vulnerable. The Tanzania National Malaria Control Program’s (NMCP) Strategic Plan for 2007–2012 reports that malaria accounts for 30% of the national disease burden, with about 1.7 million cases per year among pregnant women.
 To prevent the effect of malaria in pregnancy, the Tanzania Government adopted IPTp3+ therapy for pregnant women per the WHO recommendations for IPTp-SP. This study explores missed opportunities to deliver IPT by looking at predictors causing the drop between coverage of IPTp2 (34%) and IPTp3+ (7%).
To prevent the effect of malaria in pregnancy, the Tanzania Government adopted IPTp3+ therapy for pregnant women per the WHO recommendations for IPTp-SP. This study explores missed opportunities to deliver IPT by looking at predictors causing the drop between coverage of IPTp2 (34%) and IPTp3+ (7%).
The study examined Tanzania Demographic and Health Survey (TDHS) 2015/2016 data on women aged 15-49 with a live birth in the two years preceding the survey and at least 2 doses or more of IPTp during ANC (n=4219) to identify factors associated with differences in IPTp uptake. Variables of interest were identified, recoded and generated as required. Data was analyzed using STATA v14, whereby frequency distributions were calculated and cross-tabs and logistic regressions were done comparing dependent and independent variables.
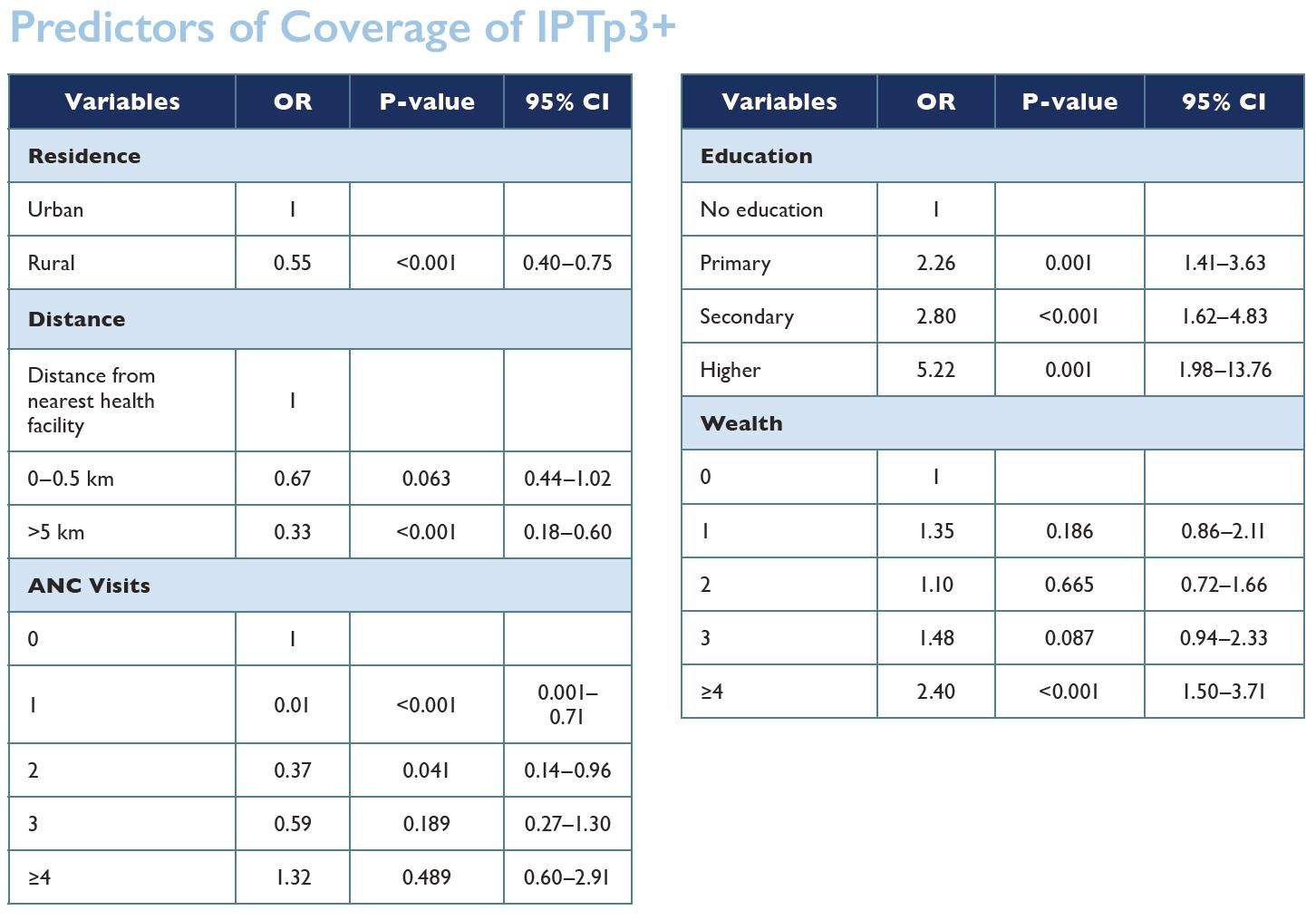 The analysis shows the factors contributing to the drop of IPTp uptake include wealth (the richest people are 2.5 times more likely to take at least three doses of IPTp) and education (those with no education are less likely to take more doses of IPTp compared to those who are educated). Residency is the largest contributing factor: 50% of pregnant mothers in rural areas are less likely to take three or more doses of SP.
The analysis shows the factors contributing to the drop of IPTp uptake include wealth (the richest people are 2.5 times more likely to take at least three doses of IPTp) and education (those with no education are less likely to take more doses of IPTp compared to those who are educated). Residency is the largest contributing factor: 50% of pregnant mothers in rural areas are less likely to take three or more doses of SP.
Clients living within 5 km of health facilities have higher uptake of IPTp3+ compared to their counterparts who live further from the health facilities (33% less likely). However, our analysis shows that there is no correlation between IPTp3+ uptake and number of ANC visits, health insurance or number of children.
Based on these results, it is important to strategize to make health services and education more accessible to the population in order to increase IPTp uptake among pregnant women.