Rural areas in Bangladesh, like Zakiganj, a subdistrict located in northeastern border region of Sylhet district, continue to face significant health challenges despite the nation’s overall progress in healthcare. With a population of approximately 250,000, Zakiganj is served by only one 50-beded government health center. The inadequate infrastructure, shortage of trained healthcare providers and low healthcare services contributes to the higher maternal and infant mortality rates compared to surrounding regions.
The photo shoes a community health worker of PRF visiting a household during surveillance, Zakiganj. According to UNICEF, in 2014, Sylhet had the lowest disparities in key maternal and newborn health interventions compared to most districts in Bangladesh. This is of great concern and requires policy level discussions with key stakeholders and intervention to improve maternal and child health.
The statistics are provided from Maternal and Newborn Health Disparities, Bangladesh, UNICEF.To address these issues, we advocate for enhanced policy measures focusing on increasing healthcare funding, expanding the number of healthcare facilities, improving infrastructure, and implementing comprehensive training programs for healthcare workers. Such measures can ensure that mothers and children in Zakiganj receive the quality care they need. Even newborn health care is possible in rural areas like Zakiganj.
We urge the Ministry of Health and Family Welfare to prioritize maternal and child health in Zakiganj by increasing funding and resources. Collaborating with organizations like PRF and BRAC will provide the necessary evidence including their years of research in this region, and pilot programs to support these policy changes. Immediate action is very important to reduce mortality rates and improve the overall health of mothers and children in rural Zakiganj.
Recent publications in Malaria Journal, The Lancet and eLife tackle several challenges to saving lives and malaria elimination. Problems include low access to bednets for children in Ethiopia, high prevalence of asymptomatic malaria in Ghanaian adults, risk of co-infection with other infectious diseases, and gaps in current interventions to prevent malaria in pregnancy and children. On the hopeful side, new targets for drug therapy are being identified. Read more on each by following the links below.
Long-lasting insecticide-treated bed net ownership, utilization and associated factors among school-age children in Southern Ethiopia
Dara Mallo and Uba Debretsehay districts because malaria is one of the major causes of morbidity and mortality among school-age children (SAC) in sub-Saharan Africa. This study was part of a baseline assessment in a cluster-randomized controlled trial.
The ownership of at least one LLIN by households of school-aged children (SAC) was about 19.3% (95% CI 17.7–21.0%) but only 10.3% % (95% CI 7.7–13.7%) of these households had adequate access of bed nets to the household members. Ownership of bed net was lower than universal coverage of at least one bed net for two individuals. It is important to monitor replacement needs and educate mothers with low education level with their SAC on the benefit of consistent utilization of bed nets.
Prevalence of and risk factors for Plasmodium spp. co-infection with hepatitis B virus: a systematic review and meta-analysis
Kotepui and Kotepui observed that Plasmodium spp. and hepatitis B virus (HBV) are among the most common infectious diseases in underdeveloped countries. Therefore they examined co-infection in people living in endemic areas of both diseases. The PubMed, Web of Science, and Scopus databases were searched. Observational cross-sectional studies and retrospective studies assessing the prevalence of Plasmodium species and HBV co-infection were examined. and found 22 studies to include in a systematic review and meta-analysis. Overall, the pooled prevalence estimate of Plasmodium spp. and HBV co-infection was 6% (95% CI 4–7%, Cochran’s Q statistic?<?0.001, I2: 95.8%).
No difference in age or gender and risk of Plasmodium spp. and HBV co-infection group was found. The present study revealed the prevalence of Plasmodium spp. and HBV co-infection, which will help in understanding co-infection and designing treatment strategies. Future studies assessing the interaction between Plasmodium spp. and HBV are recommended.
High prevalence of asymptomatic malaria infections in adults, Ashanti Region, Ghana, 2018
Melina Heinemann and co-researchers noted that Ghana is among the high-burden countries for malaria infections and recently reported a notable increase in malaria cases. While asymptomatic parasitaemia is increasingly recognized as a hurdle for malaria elimination, studies on asymptomatic malaria are scarce, and usually focus on children and on non-falciparum species. Therefore asymptomatic adult residents from five villages in the Ashanti Region, Ghana, were screened for Plasmodium species by rapid diagnostic test (RDT) and polymerase chain reaction (PCR) during the rainy season. Samples tested positive were subtyped using species-specific real-time PCR.
Molecular prevalence of asymptomatic Plasmodium infection was 284/391 (73%); only 126 (32%) infections were detected by RDT. While 266 (68%) participants were infected with Plasmodium falciparum, 33 (8%) were infected with Plasmodium malariae and 34 (9%) with P. ovale. The sub-species P. ovale curtisi and P. ovale wallikeri were identified to similar proportions. Non-falciparum infections usually presented as mixed infections with P. falciparum.
Most adult residents in the Ghanaian forest zone are asymptomatic Plasmodium carriers. The high Plasmodium prevalence not detected by RDT in adults highlights that malaria eradication efforts must target all members of the population. Beneath Plasmodium falciparum, screening and treatment must also include infections with P. malariae, P. o. curtisi and P. o. wallikeri.
Scientists shed new light on mechanisms of malaria parasite motility
eLife reports a new insight on the molecular mechanisms that allow malaria parasites to move and spread disease within their hosts has just been published. The first X-ray structures of the molecular complex that allows malaria parasites to spread disease highlight a novel target for antimalarial treatments.
The movement and infectivity of the parasite Plasmodium falciparum, and ultimately its ability to spread malaria among humans, rely on a large molecular complex called the glideosome. The new findings provide a blueprint for the design of future antimalarial treatments that target both the glideosome motor and the elements that regulate it.
New Lancet Series: Malaria in early life
Malaria infections are harmful to both the pregnant mother and the developing fetus. Malaria is associated with a 3–4 times increased risk of miscarriage and a substantially increased risk of stillbirth, and it disproportionately affects children younger than 5 years. Falciparum malaria is responsible for more than 200 000 child deaths per year in Africa and vivax malaria causes excess mortality in children in Asia and Oceania. In a duet of papers, we review 1) the deleterious effects of malaria in pregnancy on the developing fetus and 2) the current strategies for prevention and treatment of malaria in children.
Paper 1 is “Deleterious effects of malaria in pregnancy on the developing fetus: a review on prevention and treatment with antimalarial drugs” by Makoto Saito, Valérie Briand, Aung Myat Min, and Rose McGready. The authors are concerned that one in ten maternal deaths in malaria endemic countries may result from Plasmodium falciparum infection, that malaria is associated with a 3–4 times increased risk of miscarriage and a substantially increased risk of stillbirth. While current treatment and prevention strategies reduce, but do not eliminate, malaria’s damaging effects on pregnancy outcomes. They conclude that there is a need for alternative strategies to prevent malaria in pregnancy.
Paper 2 is “Treatment and prevention of malaria in children” by Elizabeth A Ashley and Jeanne Rini Poespoprodjo. They examine the following interventions: Triple antimalarial combination therapies, the RTS,S/AS01 vaccine, seasonal malaria chemoprevention and preventing relapse in Plasmodium vivax infection with primaquine.
Eyelachew Desta shares thoughts as a guest blogger in time for Mothers’ Day. Concern is expressed about ensuring increased access for low cost essential lifesaving Maternal newborn and child health supplies in Ethiopia. This posting appeared originally at Social & Cultural Basis for Community and Primary Health Programs.
Can you imagine? At this time of Mother’s Day celebration, there are thousands of women living in low income country , unlucky to be a mother to enjoy the celebration of mother’s day because of preventable birth complications due to lack of accesses to essential low cost medicines and commodities necessary for maternal, Child and New born Health. One of these low-income countries is Ethiopia where maternal and child mortality is still high.
According to an analysis published by Reproductive Health Supplies Coalition (RHSC), a quarter of all deaths between 2009 and 2013 occurred in Ethiopia are maternal mortality. This study indicated “postpartum hemorrhage (PPH)— uncontrolled bleeding after childbirth—and preeclampsia/eclampsia (PP/E)- a condition which causes high blood pressure and seizures during pregnancy”, among others, are the two leading causes of maternal deaths in Ethiopia ,could be treated by low cost and effective medicines, Oxytocin and Misoprostol.
See Photo Credit for UNICEF
The availability of accessible, reliable and low cost essential maternal health commodities is indispensable to address maternal and child mortality in Ethiopia. However according to an assessment study conducted in Ethiopia, there are gaps in the supply chain management of commodities for maternal, neonatal, and child health.
According to this study one of these gaps is “The supply chain system for MNCH commodities is inconsistent and has not been integrated into the Integrated Pharmaceutical Logistics System (IPLS)” of Ethiopia. Further the study indicated that family planning, HIV, tuberculosis, and malaria have been included in this IPLS, but not MNCH commodities. This study also identified that there is a lack of common understanding at lower level of the health system about the national policy and protocols as well as its implementation to provide MNCH services and commodities free of charge at primary health care units.
To address these gaps, there is a need of immediate actions as well as strong commitment among all stakeholders involved and engaged in the funding, monitoring, regulating and administering the logistic supply of MNCH commodities in Ethiopia. The Federal Ministry of Health (FMOH) should develop a strategy to provide continues education and training at all levels of the health system about its policy of provision of MNCH services and commodities free of charge at primary health care units , ensure policy protocols are implemented properly.
In addition to these the FMOH should strengthen its monitoring system to identify gaps in the implementation of the MNCH services and commodities policy and take measures to narrow those gaps. The Ethiopia Pharmaceuticals Fund and Supply Agency should revise its Integrated Pharmaceutical Logistics System (IPLS) to insure MNCH commodities are integrated in the system by 2020. Ultimately international donors like USAID needs to continue and strengthen their financial and technical support to the overall MNCH program of Ethiopia .
Intermittent Preventive Treatment of malaria in pregnancy (IPTp) using sulfadoxine-pyrimethamine (SP) has been a long standing intervention to protect pregnant women and their unborn children from the dangerous effects of malaria in stable transmission settings. Placental malaria deprives the fetus of nutrients leading to low birth weight, still birth and miscarriages. The mother herself suffers anemia and potentially, death.
There had always been a challenge to getting pregnant women to obtain at least two doses of IPTp-SP due to a variety of factors ranging from health system lapses to late antenatal care attendance by mothers. This phenomenon of dropping out of multi-contact interventions is not uncommon and seen equally in programs such as childhood immunization. Therefore when the World Health Organization raised the bar and recommended IPTp starting in the 13th week of pregnancy and monthly thereafter, the challenge of providing three or more doses arose.
The Malaria Indicator Surveys (MIS) and the Demographic and Health Surveys (DHS) are an ideal was to trace the progress of malaria intervention over multiple years. With the release of the preliminary results of 2017 Tanzania MIS it is now possible to track this service from over a decade. The Attached chart, using MIS/DHS reports shows that so far Tanzania has not come near achieving 80% coverage of this indicator. While there had been major increases over recent years, reports of IPTp coverage in 2017 show only 56% of recently pregnant women received at least two doses, and only 26% received three or more.
It should be noted that countries are beginning to stratify their interventions according to available transmission data. Therefore as noted in the US President’s Malaria Initiative Malaria Operations Plan for 2018, Zanzibar where transmission is low, has stopped IPTp and focuses on prompt and appropriate case management, while the mainland of Tanzania continues with all MIP interventions. Of interest is the most recent child prevalence map found in the 2017 MIS results that shows other parts of the mainland may also be approaching very low transmission.
Moving forward it will be useful if Tanzania and other endemic countries not only gather epidemiological data to help stratify appropriate interventions (as suggested in the WHO malaria elimination framework), but go further to focus reporting by strata. That said, the health system and community difficulties in achieving high IPTp coverage wherever it is appropriate will remain a challenge if services remain based in static health facilities. Community roles must be explored.
According to the Every Woman Every Child website (EWEC), “A strong focus on reproductive, maternal, child and newborn health (RMCNH) is integral to improving global health. RMNCH is linked to all 8 Millennium Development Goals (MDGs). MDGs 4 (Reduce Child Mortality), 5 (Improve Maternal Health) and 6 (combat HIV/AIDS, malaria and other diseases) each have specific targets and indicators related to RMNCH.” In order to achieve these goals life saving commodities must be made available to all women and children, and as implied in the statement above, they must include commodities that prevent and treat malaria in pregnancy.
The website further states that, “Based on these criteria, an initial list of 13 affordable, effective, but underutilized life-saving commodities were identified for consideration by the Commission. The UN Commission on Life-Saving Commodities for Women and Children aims to increase access to life-saving medicines and health supplies for the world’s most vulnerable people.” Ironically this suggestive list does not include medicine for intermittent preventive treatment of malaria in pregnancy (IPTp), insecticide treated nets (ITNs), malaria rapid diagnostic tests or artemisinin-based combination therapy medicines for malaria treatment.
Yes the list is only suggestive, and yes it is a global list, but WHO estimates that nearly 50 million women will become pregnant in malaria endemic areas each year. That’s a pretty big chunk of the world’s population to neglect.
EWEC does refer to two partner documents for more details on these essential commodities. One document is “The Essential Interventions, Commodities and Guidelines for Reproductive, Maternal, Newborn and Child Health – A global review of the key interventions related to reproductive, maternal, newborn and child Health.” This document mentions generically “Prevention and management of malaria with insecticide treated nets and antimalarial medicines.”
The second document, “Priority medicines for mothers’ and children’s health, 2011”, also identifies medicines that are in need of enhanced attention and utilization in order to avoid preventable deaths of women and children. This document mentions that commodities exist for malaria services, but refers the reader to the very detailed Global Malaria Program’s “Guidelines for the treatment of malaria” (2nd ed. Geneva, World Health Organization, 2010) that discusses medications for all species of Plasmodium and does not have an easy to view take away on the essential life saving commodities within.
Over the past year the Global Malaria Program of WHO has issued guidance for updating malaria in pregnancy interventions, including more frequency IPTp with sulphadoxine-pyrimethamine (SP). The briefing companion document to this new guidance spells out the following life saving benefits if IPTp with appropriate references:
IPTp-SP prevents the adverse consequences of malaria on maternal and fetal outcomes, such as placental infection, clinical malaria, maternal anaemia, fetal anaemia, low birth weight and neonatal mortality.
IPTp-SP has recently been shown to be highly cost-effective for both prevention of maternal malaria and reduction of neonatal mortality in areas with moderate or high malaria transmission.
Despite the spread of SP resistance, IPTp-SP continues to provide significant benefit, resulting in protection against both neonatal mortality (protective efficacy 18%) and low birth weight (21% reduction in LBW) under routine program conditions.
Over the years rarely has IPTp if ever achieved high and sustained coverage. Factors relating to late antenatal care attendance are often mentioned first, but experience has shown that one of the key factors is stock-out of SP. Once SP was no longer a first line treatment drug, it was forgotten – a neglected medicine needed by an often neglected but vulnerable portion of the population. Now is the time to advocate strongly for direct and unconditional listing of SP for IPTp, ITNs and other malaria products among any list of RNMCH life saving commodities.
During its final day the Malaria in Pregnancy meeting in Istanbul addressed barriers to achieving malaria in pregnancy (MIP) goals at four levels: community, district/facility, national and global.
The Global Level Group looked at global issues. At the Global Level there is need to stress and strengthen multiple intervention package for antenatal care including malaria in pregnancy services. The group stressed that we can learn from the HIV community who promote PMTCT in ANC to and thus better promote MIP interventions in ANC.
The group also emphasized the need revise global guidance on essential drugs so Sulphadoxine-Pyrimethamine (SP) is used only for IPTp in MIP, not for malaria treatment. The group noted that there are many manufacturers of SP, but are not part of WHO pre-qualification (drug quality) process – improve quality of MIP drugs.
The Global Group observed that it takes long time for policies and evidence to filter to local level – need speed up dissemination of MIP information. The group also pushed for harmonization of MIP guidance needed even within global organizations like WHO. We must also identify and address inconsistencies in MIP policies and messages from global level to health facility level.
They recommended MIP champions to help prioritize high burden malaria and maternal mortality areas and promote scale-up MIP services. This champion or advocacy process should take advantage of global fora and initiatives such as ‘Every Woman, Every Child’, Woman Deliver, ALMA and GMHC to share the latest evidence based information on MIP. Global advocacy should also include publications in international journals like The Lancet on MIP and ANC packages.
The National level working group pointed out confusing guidelines as a major barrier to IPTp uptake. We cannot always wait for clarification from international partners, they noted – What to do while we wait? We we do update guidelines we need to ensure representation of all programs when updating guidelines (malaria, RH, MCH) for malaria in pregnancy. Also, countries need to simplify MIP guidelines based on learning about their own implementation barriers that can be easily overcome locally.
At national level we must focus on more than guidelines. We also need harmonized training and Monitoring and Evaluation across programs (malaria, RH, MCH) on malaria in pregnancy service delivery. At present there is often ack of coordination and harmonization across programs for that deliver MIP services. We must sit together but also harmonization implementation.
The group addressing district and facility level barriers to MIP service uptake called for user friendly services. They noted that health services must also be ‘friendly’ to the provider. In order to retain providers we must also address quality of life for staff.
Standards based management/performance improvement processes at district and facility level based on incentives including recognition may not only enhance MIP performance but give staff at these levels the tools needed to identify and solve their own problems using locally available resources and ideas.
Better tracking of commodities is needed to ensure that clients are not disappointed. We can redistribute commodities like SP within or among districts to ensure services succeed. We must prioritize SP provision as part of an essential ANC supply package.
The group stated emphatically that traditional cascade training out, that we need innovative and facility based approaches like champions at facility and text based training for malaria in pregnancy instead. Clinical mentoring and checklists can help promote malaria in pregnancy service skills, which can lead to greater consumer satisfaction and utilization.
Even when there has been traditional workshop based training the problem is that staff are often not trained on national guidelines. There is need for supervision that is also based on guidelines, not the personal beliefs and references of the supervisors. Also, without the commodities, staff can not practice what they learned.
The community focused working group started with a recognition that the ‘knowledge’ problem is a two-way street. It is not only that community members may not understand our scientific approach to defining, treating and preventing malaria. We too may fail to communicate with the community and create demand for services because we do not understand their perspectives.
The community group suggested that we combine community resource people and media and private sector actions for comprehensive malaria communication. Mass medial can reinforce information that is shared by trusted community leaders and health volunteers.
The group debated the cost problems communities face in in accessing MIP servivces. This may include direct costs of services in some countries as well as indirect costs to the family. Women’s access to funds and income need to be considered, hence collaboration withy other sectors of the development community such as micro-finance.
The problem of linear communication from health workers to community without learning community knowledge and dialogue can be overcome if health workers are encouraged to engage in deeper dialogue with mothers, fathers, grandmothers and community leaders and become learners first, before they hope to teach about MIP.
On Monday, “Secretary of State Hillary Rodham Clinton will deliver a speech commemorating the 15th anniversary of the International Conference on Population and Development (ICPD),” held at Cairo. “At this event, Secretary Clinton will declare the U.S. Government’s renewed support for and dedication to reaching the ICPD and other related UN agreements, including the Millennium Development Goals, by 2015,” which include reducing both maternal mortality and malaria.
In a publication marking 15 years since the Cairo Conference, UNFPA has published an update entitled, “Healthy Expectations: Celebrating Achievements of the Cairo Consensus and Highlighting the Urgency for Action.” The document explains that …
In 2005, the lifetime risk of death from maternal causes was 1 in 22 for women in sub-Saharan Africa, compared with less than 1 in 6,000 for women in more developed countries. For each woman who dies, 20 additional women suffer pregnancy-related disabilities … Most maternal deaths occur to women who live in sub-Saharan Africa and South Asia. The number of maternal deaths in sub-Saharan Africa has increased as the number of women in the childbearing ages has grown.
When Secretary Clinton speaks she will remind us that, “Millions of lives have been improved and saved through effective and affordable reproductive health programs, which have proven to prevent the deaths of women and children, reduce the spread of HIV/AIDS, grow economies, and preserve natural resources.” These programs should include malaria in pregnancy control as an integral part of antenatal care.
It is useful in this context to think of the ICPD guiding principles. Principle 4 addresses “Advancing gender equality and equity and the empowerment of women.” For malaria control this means ensuring malaria in pregnancy control programs are fully funded and operational since pregnant women suffer more from malaria than other adults in endemic areas.
Principle 8 recognizes the right of people to space their children. This process can be frustrated due to fetal loss during malaria in pregnancy or from peri-natal and infant mortality when children are born with low birth weight and are less likely to survive.
Neither our reproductive health nor our malaria programs are complete until we plan to meet the needs of pregnant women who are risk from this deadly parasitic disease. Integrated planning and service delivery is required.
Population Action International made an important point that the Global Fund to Fight AIDS, TB and Malaria could save even more lives it it addressed reproductive health issues. In particular PAI explains that, “After just a few short years, the Global Fund has saved over 1.8 million lives worldwide. Just think what can be accomplished—how many more lives saved—if the Global Fund partnered with the life-saving work of sexual and reproductive health providers.”
In the area of Malaria control, GFATM funds to contribute toward improving reproductive health through a variety of malaria in pregnancy (MIP) interventions including 1) Intermittent Preventive Treatment (IPTp) with sulfadoxine-pyrimethamine (SP), 2) long lasting insecticide-treated bednets (LLINs) and prompt and appropriate case management with artemisinin-based combination therapy (ACTs)
Of course the potential for including MIP in GF proposals and the actual emphasis on MIP in reality are sometimes different. Since SP is so cheap, its procurement is often overlooked. A recent visit to rural Kenyan clinics found plenty of ACT stocks, but stockouts of SP. ACTs are procured with GAFTM funds through international contracts, while SP is often purchased locally when funds are available in national health budgets. LLINs are often distributed widely to children under five years of age through well publicized campaigns, while it is difficult to get a bednet as part of regular antenatal care in come countries. Often GFATM projects are implemented through the vertical disease units in health agencies, leaving little opportunity for reproductive health, or even integrated management of childhood illness units to become involved.
So in short, while we might point out that reproductive health issues can already be part of GFATM activities in principle, we agree with Population Action International that active involvement of reproductive health services, particularly in our area of malaria control, is urgently needed.
Sign up for daily or weekly articles from Bill highlighting the most noteworthy developments in newspapers and scientific journals. Click here to register.
 The photo shoes a community health worker of PRF visiting a household during surveillance, Zakiganj. According to UNICEF, in 2014, Sylhet had the lowest disparities in key maternal and newborn health interventions compared to most districts in Bangladesh. This is of great concern and requires policy level discussions with key stakeholders and intervention to improve maternal and child health.
The photo shoes a community health worker of PRF visiting a household during surveillance, Zakiganj. According to UNICEF, in 2014, Sylhet had the lowest disparities in key maternal and newborn health interventions compared to most districts in Bangladesh. This is of great concern and requires policy level discussions with key stakeholders and intervention to improve maternal and child health. The statistics are provided from Maternal and Newborn Health Disparities, Bangladesh, UNICEF.To address these issues, we advocate for enhanced policy measures focusing on increasing healthcare funding, expanding the number of healthcare facilities, improving infrastructure, and implementing comprehensive training programs for healthcare workers. Such measures can ensure that mothers and children in Zakiganj receive the quality care they need. Even newborn health care is possible in rural areas like Zakiganj.
The statistics are provided from Maternal and Newborn Health Disparities, Bangladesh, UNICEF.To address these issues, we advocate for enhanced policy measures focusing on increasing healthcare funding, expanding the number of healthcare facilities, improving infrastructure, and implementing comprehensive training programs for healthcare workers. Such measures can ensure that mothers and children in Zakiganj receive the quality care they need. Even newborn health care is possible in rural areas like Zakiganj.
 Molecular prevalence of asymptomatic Plasmodium infection was 284/391 (73%); only 126 (32%) infections were detected by RDT. While 266 (68%) participants were infected with Plasmodium falciparum, 33 (8%) were infected with Plasmodium malariae and 34 (9%) with P. ovale. The sub-species P. ovale curtisi and P. ovale wallikeri were identified to similar proportions. Non-falciparum infections usually presented as mixed infections with P. falciparum.
Molecular prevalence of asymptomatic Plasmodium infection was 284/391 (73%); only 126 (32%) infections were detected by RDT. While 266 (68%) participants were infected with Plasmodium falciparum, 33 (8%) were infected with Plasmodium malariae and 34 (9%) with P. ovale. The sub-species P. ovale curtisi and P. ovale wallikeri were identified to similar proportions. Non-falciparum infections usually presented as mixed infections with P. falciparum.
 e-pyrimethamine (SP) has been a long standing intervention to protect pregnant women and their unborn children from the dangerous effects of malaria in stable transmission settings. Placental malaria deprives the fetus of nutrients leading to low birth weight, still birth and miscarriages. The mother herself suffers anemia and potentially, death.
e-pyrimethamine (SP) has been a long standing intervention to protect pregnant women and their unborn children from the dangerous effects of malaria in stable transmission settings. Placental malaria deprives the fetus of nutrients leading to low birth weight, still birth and miscarriages. The mother herself suffers anemia and potentially, death. The Malaria Indicator Surveys (MIS) and the Demographic and Health Surveys (DHS) are an ideal was to trace the progress of malaria intervention over multiple years. With the release of the preliminary results of 2017 Tanzania MIS it is now possible to track this service from over a decade. The Attached chart, using MIS/DHS reports shows that so far Tanzania has not come near achieving 80% coverage of this indicator. While there had been major increases over recent years, reports of IPTp coverage in 2017 show only 56% of recently pregnant women received at least two doses, and only 26% received three or more.
The Malaria Indicator Surveys (MIS) and the Demographic and Health Surveys (DHS) are an ideal was to trace the progress of malaria intervention over multiple years. With the release of the preliminary results of 2017 Tanzania MIS it is now possible to track this service from over a decade. The Attached chart, using MIS/DHS reports shows that so far Tanzania has not come near achieving 80% coverage of this indicator. While there had been major increases over recent years, reports of IPTp coverage in 2017 show only 56% of recently pregnant women received at least two doses, and only 26% received three or more.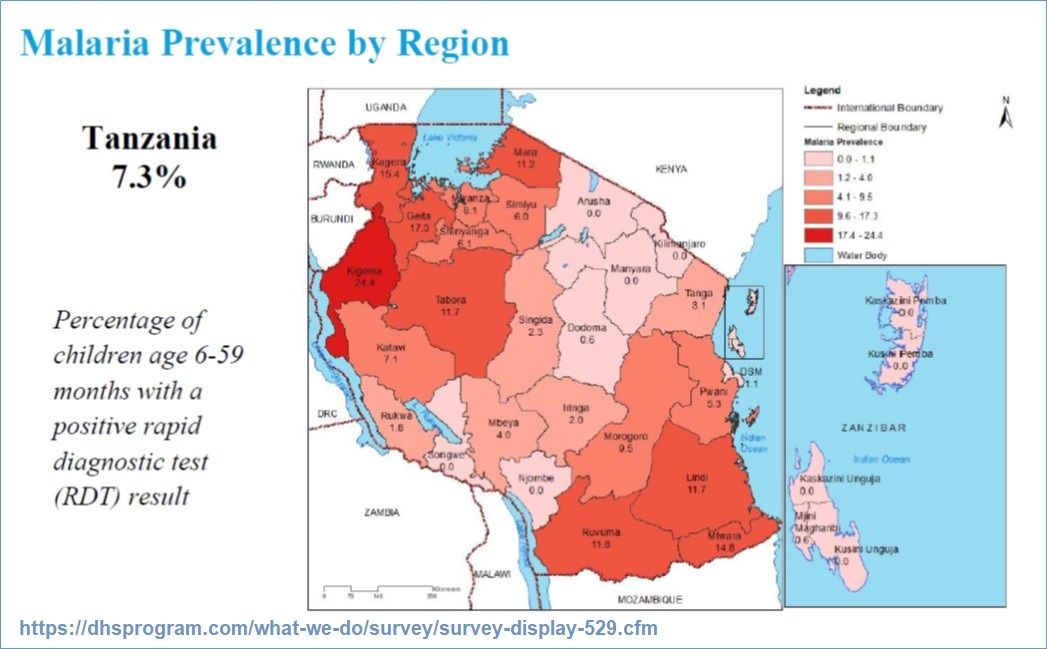 It should be noted that countries are beginning to stratify their interventions according to available transmission data. Therefore as noted in the US President’s Malaria Initiative Malaria Operations Plan for 2018, Zanzibar where transmission is low, has stopped IPTp and focuses on prompt and appropriate case management, while the mainland of Tanzania continues with all MIP interventions. Of interest is the most recent child prevalence map found in the 2017 MIS results that shows other parts of the mainland may also be approaching very low transmission.
It should be noted that countries are beginning to stratify their interventions according to available transmission data. Therefore as noted in the US President’s Malaria Initiative Malaria Operations Plan for 2018, Zanzibar where transmission is low, has stopped IPTp and focuses on prompt and appropriate case management, while the mainland of Tanzania continues with all MIP interventions. Of interest is the most recent child prevalence map found in the 2017 MIS results that shows other parts of the mainland may also be approaching very low transmission.
 The second document, “Priority medicines for mothers’ and children’s health, 2011”, also identifies medicines that are in need of enhanced attention and utilization in order to avoid preventable deaths of women and children. This document mentions that commodities exist for malaria services, but refers the reader to the very detailed Global Malaria Program’s “Guidelines for the treatment of malaria” (2nd ed. Geneva, World Health Organization, 2010) that discusses medications for all species of Plasmodium and does not have an easy to view take away on the essential life saving commodities within.
The second document, “Priority medicines for mothers’ and children’s health, 2011”, also identifies medicines that are in need of enhanced attention and utilization in order to avoid preventable deaths of women and children. This document mentions that commodities exist for malaria services, but refers the reader to the very detailed Global Malaria Program’s “Guidelines for the treatment of malaria” (2nd ed. Geneva, World Health Organization, 2010) that discusses medications for all species of Plasmodium and does not have an easy to view take away on the essential life saving commodities within. The attached map from UNFPA shows heightened maternal mortality in just the same regions of the world where malaria is most prevalent.
The attached map from UNFPA shows heightened maternal mortality in just the same regions of the world where malaria is most prevalent.