Diagnosis &Health Systems &IPTp &ITNs &Universal Coverage Bill Brieger | 31 Mar 2018
Universal Health Coverage – Where is Malaria?
 Universal Health Coverage (UHC) is the theme of the 2018 World Health Day on April 7th. The concept was applied to malaria in 2009 regarding the provision of long lasting insecticide-treated nets (LLINs aka ITNs) with the definition of universal meaning one net for every two persons in a household. Up until that time coverage targets for malaria interventions set at the 2000 Abuja Declaration had focused on achieving by the year 2010, 80% of people (particularly pregnant women and children below the age of 5 years) sleeping under ITNs, 80% of children receiving appropriate malaria treatment with artemisinin-based combination therapy (ACTs) within 24 hours of onset of illness and 80% of pregnant women receiving two doses of Intermittent Preventive Treatment (IPTp) for malaria as part of antenatal care (ANC).
Universal Health Coverage (UHC) is the theme of the 2018 World Health Day on April 7th. The concept was applied to malaria in 2009 regarding the provision of long lasting insecticide-treated nets (LLINs aka ITNs) with the definition of universal meaning one net for every two persons in a household. Up until that time coverage targets for malaria interventions set at the 2000 Abuja Declaration had focused on achieving by the year 2010, 80% of people (particularly pregnant women and children below the age of 5 years) sleeping under ITNs, 80% of children receiving appropriate malaria treatment with artemisinin-based combination therapy (ACTs) within 24 hours of onset of illness and 80% of pregnant women receiving two doses of Intermittent Preventive Treatment (IPTp) for malaria as part of antenatal care (ANC).
 Definitions have evolved since the Abuja Declaration. The target for ITNs was extended to all household members (thus universal). The ACT target was modified to require treatment based on parasitological testing (microscopy or rapid diagnostic tests). IPTp targets were extended to achieving monthly dosing from the 13th week of pregnancy, which depending on the point in pregnancy when a women entered the ANC system could be 3, 4 or more doses. In addition to these changes, the US President’s malaria Initiative upped the Abuja targets from 80% to 85% in the countries where it supported national malaria programs.
Definitions have evolved since the Abuja Declaration. The target for ITNs was extended to all household members (thus universal). The ACT target was modified to require treatment based on parasitological testing (microscopy or rapid diagnostic tests). IPTp targets were extended to achieving monthly dosing from the 13th week of pregnancy, which depending on the point in pregnancy when a women entered the ANC system could be 3, 4 or more doses. In addition to these changes, the US President’s malaria Initiative upped the Abuja targets from 80% to 85% in the countries where it supported national malaria programs.
We are eight years past 2010. It had been assumed that if scale up to 80% had been achieved by then and sustained for five or more years, malaria deaths would come close to zero and elimination of the disease would be in sight. National surveys have shown that reaching these targets has not been simple.
 The example of ITNs is a good place to start, as is Nigeria with the highest burden of malaria. The attached chart shows findings from the Demographic and Health or Malaria Information Surveys in 2010, 2013 and 2015. Whether one measures universal coverage by the house possessing at least one net per two residents or by the proportion who actually use/sleep under the nets, we can see that UHC for this intervention is difficult to achieve. Even when households possess nets, not everyone sleeps under them either because of adequacy of nets, preferred sleeping arrangements, internal household power structure or other factors.
The example of ITNs is a good place to start, as is Nigeria with the highest burden of malaria. The attached chart shows findings from the Demographic and Health or Malaria Information Surveys in 2010, 2013 and 2015. Whether one measures universal coverage by the house possessing at least one net per two residents or by the proportion who actually use/sleep under the nets, we can see that UHC for this intervention is difficult to achieve. Even when households possess nets, not everyone sleeps under them either because of adequacy of nets, preferred sleeping arrangements, internal household power structure or other factors.
In 2015 the majority of nets that existed in households were obtained through campaigns (77%), 14% were acquired from the health services, and 7% were purchased. These systems are not keeping up with the need.
 Four endemic countries reported a malaria Information Survey in 2016, Liberia, Ghana, Madagascar, and Sierra Leone. The chart shows that they too have had difficulty in achieving universal coverage of malaria interventions. Of note the chart only includes whether appropriate malaria parasitological diagnosis was done on children who had fever in the preceding two weeks. Data on provision of ACTs is based on fever, not test results, so there is no way to know whether it was appropriate. Generally 20-30% more febrile children received ACTs than were tested.
Four endemic countries reported a malaria Information Survey in 2016, Liberia, Ghana, Madagascar, and Sierra Leone. The chart shows that they too have had difficulty in achieving universal coverage of malaria interventions. Of note the chart only includes whether appropriate malaria parasitological diagnosis was done on children who had fever in the preceding two weeks. Data on provision of ACTs is based on fever, not test results, so there is no way to know whether it was appropriate. Generally 20-30% more febrile children received ACTs than were tested.
 All three malaria interventions, ACTs, Diagnostics and ITNs, require contact with the health system (including community health workers). If malaria services are indicative of other health interventions, then universal coverage including seeking interventions, getting them and ultimately using them is still a distant goal. To achieve universal coverage there also needs to be universal commitment by countries, donors and technical partners.
All three malaria interventions, ACTs, Diagnostics and ITNs, require contact with the health system (including community health workers). If malaria services are indicative of other health interventions, then universal coverage including seeking interventions, getting them and ultimately using them is still a distant goal. To achieve universal coverage there also needs to be universal commitment by countries, donors and technical partners.
Gender &Leadership &Women Bill Brieger | 23 Mar 2018
Women Making Malaria History
March is Women’s History Month and thus a time to examine the role of women in bringing an end to malaria. For many years studies at the household level have told us that women often lack the financial independence or social support to make important decisions about malaria treatment and prevention for themselves and their children. Furthermore, as WHO notes, “Gender norms and values … influence the division of labour, leisure patterns, and sleeping arrangements may lead to different patterns of exposure to mosquitoes for men and women.” As part of the solution to these problems, it is important to look at women role models in the fight against the disease – at women making malaria history.
 One of these role models is Tu Youyou who became one of three scientists to win the 2015 Nobel Prize for medicine. Her work of over 40 years was virtually unknown to the outside world until then, but her study of artemisinin medicinal compounds has saved the lives of millions.
One of these role models is Tu Youyou who became one of three scientists to win the 2015 Nobel Prize for medicine. Her work of over 40 years was virtually unknown to the outside world until then, but her study of artemisinin medicinal compounds has saved the lives of millions.
 Moving from the lab to the community one can find role models who have broken role stereotypes. A few years ago President’s Malaria Initiative-funded Africa Indoor Residual Spraying (AIRS) project drew out attention to Maimouna Sanogo as a woman making a difference. She helped protect people in her country from malaria through her work as a supervisor on AIRS indoor residual spraying project in Mali. The AIRS project reported that, “As a woman in a leadership role, Maimouna is a trailblazer. In Mali, only 37% of women participate in the labor force, while participation is nearly double among Malian men (70%).”
Moving from the lab to the community one can find role models who have broken role stereotypes. A few years ago President’s Malaria Initiative-funded Africa Indoor Residual Spraying (AIRS) project drew out attention to Maimouna Sanogo as a woman making a difference. She helped protect people in her country from malaria through her work as a supervisor on AIRS indoor residual spraying project in Mali. The AIRS project reported that, “As a woman in a leadership role, Maimouna is a trailblazer. In Mali, only 37% of women participate in the labor force, while participation is nearly double among Malian men (70%).”
Women have played crucial leadership roles in national malaria programs. Dr TO Sofola as Director of Nigeria’s National Malaria Control Program (NMCP, now National Malaria Elimination Program) guided the transition of case management policy to the use of artemisinin-based combination therapy, oversaw planning for the first massive national LLIN campaign, guided development of the World Bank Booster Program support, helped strengthen Nigeria’s first Global Fund Malaria Grants, and brought state level malaria control programs into the national strategy process. Women have also led NMCPs in Malawi, Kenya and other countries.
 Dr Rose Leke, Emeritus Professor of Immunology and Parasitology, Faculty of Medicine and Biomedical Sciences, University of Yaounde, Cameroon, was one of six people to be given the Kwame Nkrumah Scientific Award for Women in 2011. Dr Leke explained the challenges facing women, “Science is still a challenging field for women to enter, and even more so in which to progress. At the university, I have seen many promising young women finish their studies and start jobs as assistants only to either get stuck in that position indefinitely or eventually leave to take care of their families. There just wasn’t the mentorship or financial support for research needed for them to be able to progress. It was an issue I really took to heart.” Therefore, Dr Leke and colleagues started the HIGHER Women Consortium in Cameroon. We provided training and mentorship to young women researchers.
Dr Rose Leke, Emeritus Professor of Immunology and Parasitology, Faculty of Medicine and Biomedical Sciences, University of Yaounde, Cameroon, was one of six people to be given the Kwame Nkrumah Scientific Award for Women in 2011. Dr Leke explained the challenges facing women, “Science is still a challenging field for women to enter, and even more so in which to progress. At the university, I have seen many promising young women finish their studies and start jobs as assistants only to either get stuck in that position indefinitely or eventually leave to take care of their families. There just wasn’t the mentorship or financial support for research needed for them to be able to progress. It was an issue I really took to heart.” Therefore, Dr Leke and colleagues started the HIGHER Women Consortium in Cameroon. We provided training and mentorship to young women researchers.
Women in academics, research, government and front line programs have and continue to make history in the efforts to eliminate malaria. As Dr Leke’s example shows, these women leaders can make sure no one stands in the way of ensuring that the next generation of women scientists, managers and field workers make malaria history.
NTDs &Snakebite Bill Brieger | 17 Mar 2018
Modern Day St Patrick Needed to Drive out Snakes and NTDs

https://www.catholic.org/saints/saint.php?saint_id=89
While St. Patrick, the Christian missionary supposedly rid Ireland of snakes during the fifth century A.D., “Nigel Monaghan, who has trawled through vast collections of fossil and other records of Irish animals, has found no evidence of snakes ever existing in Ireland.” The rest of the world, of course, does not rest as easily, and therefore, “On June 9th, 2017 WHO categorized snakebite envenomation into the Category A of the Neglected Tropical Diseases.”
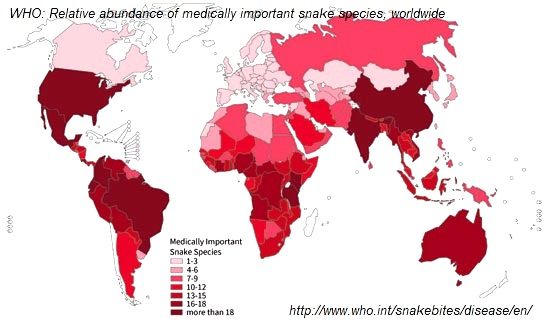
The World Health Organization explains that, “Snakebite envenoming is a potentially life-threatening disease that typically results from the injection of a mixture of different toxins (“venom”) following the bite of a venomous snake. Envenoming can also be caused by having venom sprayed into the eyes by certain species of snakes that have the ability to spit venom as a defense measure.” The organization notes that our of over 3,000 snake species globally, 250 are medically important because of their harmful venom. These can be found in 160 countries.
In preparation for the World Health Assembly, “the 142nd session of the World Health Organization’s Executive Board has recommended a resolution on snakebite envenoming to the 71st World Health Assembly, setting the scene for its possible adoption in May 2018.” The resolution calls on all countries to take definitive steps to stop the death, disability and suffering that snakebite inflicts on many of the poorest and most vulnerable of the world’s people.
A recent WHO report notes that, “As for other neglected tropical diseases, estimation of global morbidity, disability and mortality due to snakebite envenoming is problematic.” Rough estimates of the burden of snakebite include –
- 8 million to 2.7 million cases of snakebite envenoming per year
- 81 000 to 138 000 deaths per year
- 400,000 people a year face permanent disabilities, including blindness, extensive scarring and contractures, restricted mobility and amputation following snakebite envenoming
Mapping is a first important step for countries attempting to tackle this neglected disease. Sri Lanka was able develop snakebite risk maps to identify snakebite hotspots and cold spots in the country. A national survey in India found that, “Snakebite deaths occurred mostly in rural areas (97%), were more common in males (59%) than females (41%), and peaked at ages 15–29 years (25%) and during the monsoon months of June to September.” Costa Rica is using geographical information systems to identify populations in need of improved accessibility to anti-venom treatment for snakebite envenoming.
As Jose Mar?a Gutierrez and colleagues stress, “the need for incorporation of the proposed snakebite initiatives within the general struggle against all the NTDs will result in a significant and more logistically efficient reduction of human suffering.” This can be accomplished by having snakebite become part of the existing unified strategy for several NTDs that, “simplifies drug distribution, reduces duplication, and lessens some of the demands on health systems and staff.”
Thus with a unified approach we can hope to drive out snakes, worms, and other parasites from the homes, communities and countries of those suffering from the neglected diseases of poverty.
Elimination &Eradication &Monkeys &Zoonoses Bill Brieger | 16 Mar 2018
The Monkey on the Back of Malaria Elimination
Concerning malaria elimination, “WHO grants this certification when a country has proven, beyond reasonable doubt, that the chain of local transmission of all human (emphasis added) malaria parasites has been interrupted nationwide for at least the past 3  consecutive years.” This target is challenging enough, but becomes more complicated when we consider that zoonotic transmission of malaria among monkeys and humans has been documented in Brazil and Southeast Asia. We cannot expect monkeys to sleep under bednets, so creative and realistic solutions are needed.
consecutive years.” This target is challenging enough, but becomes more complicated when we consider that zoonotic transmission of malaria among monkeys and humans has been documented in Brazil and Southeast Asia. We cannot expect monkeys to sleep under bednets, so creative and realistic solutions are needed.
The Malaria Eradication Research Agenda (malERA) recognizes this problem. Plasmodium knowlesi, originally found in macaque monkeys in Southeast Asia has been dubbed the fifth human malaria due to its spread to people as deforestation has disturbed the habitat of the monkeys. In particular malERA addresses the challenge of understanding the upward trend of this malaria infection in that region and the need for better understanding of transmission dynamics and proper diagnosis.
The danger of P. knowlesi is heightened by difficulties in diagnosing it and distinguishing it from other malaria species. “Recently, the prevalence of human infection with a simian malaria parasite, P. knowlesi, has become an important issue in a wide area of Southeast Asia. The identification of this parasite by microscopy is very difficult because it resembles the P. malariae parasite. However, the symptoms caused by P. malariae and P. knowlesi are very different, with only P. knowlesi causing severe and life-threatening malaria” (Komaki-Yasuda et al.)
 Reports from Brazil highlight another ‘simian hotspot.’ While P. Knowlesi represents monkey infections reaching humans, the opposite may have happened to establish a reservoir in the New World. “P. vivax lineages appearing to originate from Melanesia that were putatively carried by the Australasian peoples who contributed genes to Native Americans. Importantly, mitochondrial lineages of the P. vivax-like species P. simium are shared by platyrrhine monkeys and humans in the Atlantic Forest ecosystem, but not across the Amazon, which most likely resulted from one or a few recent human-to-monkey transfers.” But looking even further back in natural history, Escalante and colleagues found, “compelling evidence that P. vivax is derived from a species that inhabited macaques in Southeast Asia.”
Reports from Brazil highlight another ‘simian hotspot.’ While P. Knowlesi represents monkey infections reaching humans, the opposite may have happened to establish a reservoir in the New World. “P. vivax lineages appearing to originate from Melanesia that were putatively carried by the Australasian peoples who contributed genes to Native Americans. Importantly, mitochondrial lineages of the P. vivax-like species P. simium are shared by platyrrhine monkeys and humans in the Atlantic Forest ecosystem, but not across the Amazon, which most likely resulted from one or a few recent human-to-monkey transfers.” But looking even further back in natural history, Escalante and colleagues found, “compelling evidence that P. vivax is derived from a species that inhabited macaques in Southeast Asia.”
A recent study in this area found the worrying results that, “The low incidence of cases and the low frequency of asymptomatic malaria carriers investigated make it unlikely that the transmission chain in the region is based solely on human hosts, as cases are isolated one from another by hundreds of kilometers and frequently by long periods of time, reinforcing instead the hypothesis of zoonotic transmission.”
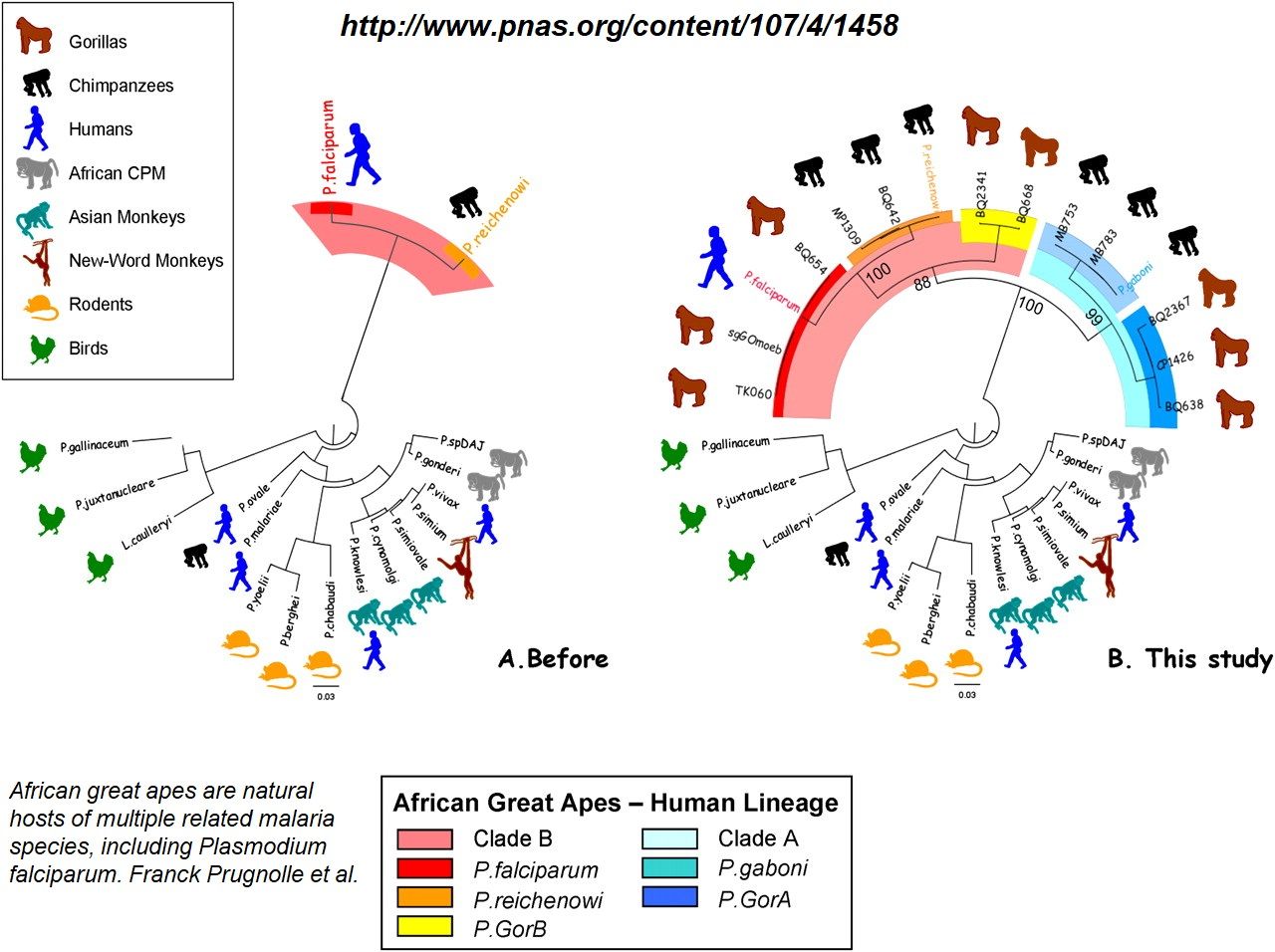
In Africa, Linda Duval and co-researchers, who found P. falciparum in blood samples from two chimpanzees belonging to two different subspecies, warn that, “If malignant malaria were eradicated from human populations, chimpanzees, in addition to gorillas, might serve as a reservoir for P. falciparum,”
It appears that the dynamics between monkeys, malaria and humans has a long history. Even once certified malaria-free countries face the threat of imported malaria from people crossing borders. Now we must recognize that the threat may already live within borders. So since existing malaria interventions to protect humans from malaria cannot be applied to monkeys, accelerated research on the genetics of the parasite and the mosquito is needed to prevent both primate groups from getting malaria.
Education &Health Systems &Primary Health Care &Social/Cultural &Training Bill Brieger | 15 Mar 2018
New Fully Online Global Health Learning Programs at JHU
Continuing professional development has often been a challenge for people in the field.  They may not be able to get study leave, but they do need advanced training in order to progress. The Johns Hopkins Bloomberg School of Public Health as started a new Online Programs for Applied Learning (OPAL) that offers completely online Masters and Certificate degrees.
They may not be able to get study leave, but they do need advanced training in order to progress. The Johns Hopkins Bloomberg School of Public Health as started a new Online Programs for Applied Learning (OPAL) that offers completely online Masters and Certificate degrees.
The Department of International Health is Offering three Master of Applied Learning (MAS) and one Certificate covering global health. The Certificate can be completed in one year minimum and the MAS in two years minimum. More information on these programs can be obtained at the links below.
- Request information for fully online Master of Applied Science in Community-based Primary Health Care Programs in Global Health
 Also get information for fully online Master of Applied Science in Master of Applied Science in Global Health Planning and Management
Also get information for fully online Master of Applied Science in Master of Applied Science in Global Health Planning and Management- Learn more about fully online Certificate in Global Health Practice, a stand alone or first year for our 2 Global Health Masters of Applied Science
- Master of Applied Science in Humanitarian Health

CHW &Community &Equity &Health Workers &ITNs Bill Brieger | 12 Mar 2018
Malaria by the numbers: are the statistics real or are they a barrier to community involvement?
 George Mwinnyaa grew up in a small village in Ghana, West Africa. “I witnessed the death of several people including my siblings and my father. I became a health volunteer and later a community health worker.” George presented at the Johns Hopkins University TEDx event on 10 March 2018. Below are excerpts from that talk focused on his experiences in malaria interventions in Ghana and reflects on numbers found in public health interventions and questions what these numbers really mean to community members on the ground. George is currently an MHS student studying infectious disease epidemiology at the JHU Bloomberg School of Public Health.
George Mwinnyaa grew up in a small village in Ghana, West Africa. “I witnessed the death of several people including my siblings and my father. I became a health volunteer and later a community health worker.” George presented at the Johns Hopkins University TEDx event on 10 March 2018. Below are excerpts from that talk focused on his experiences in malaria interventions in Ghana and reflects on numbers found in public health interventions and questions what these numbers really mean to community members on the ground. George is currently an MHS student studying infectious disease epidemiology at the JHU Bloomberg School of Public Health.
——-
 I have always been very skeptical with numbers, particularly numbers that indicate program accomplishments from the developing world. Whenever I see numbers reporting a problem such as the mortality relating to malaria, Pneumonia, or diarrheal diseases- it puzzles me because these are all diseases that have received great attention, and there have been many interventions implemented. Yet these problems still exist, and the question is why?
I have always been very skeptical with numbers, particularly numbers that indicate program accomplishments from the developing world. Whenever I see numbers reporting a problem such as the mortality relating to malaria, Pneumonia, or diarrheal diseases- it puzzles me because these are all diseases that have received great attention, and there have been many interventions implemented. Yet these problems still exist, and the question is why?
Today malaria is still among the top causes of infant mortality in many African countries, including Ghana, yet we have mosquito nets, coils, sprays, long sleeved shirts that have been circulating in the country for years……and sometimes I wonder: why?
Total funding for malaria prevention and control was 2.7 billion dollars in 2016. Between 2014-2016, 582 million nets were distributed, of which 505 million were distributed in Africa, yet the number of malaria cases increased from 211 million in 2015 to 216 million in 2016 (WHO-malaria fact sheet, 2017).
I was once a supervisor for the distribution of long-lasting insecticide treated nets in rural communities. The numbers driven world saw big numbers that showed that many pregnant women were not sleeping under mosquito nets and so the solution to solve the malaria problem was to give them mosquito nets.
 First, they started out by selling the nets and people would not buy them, then they offered them free to pregnant women and that did not change anything, next they distributed to families in a household and that did not change anything, and finally they implemented what is known as the hanging of long lasting insecticide treated bed nets.
First, they started out by selling the nets and people would not buy them, then they offered them free to pregnant women and that did not change anything, next they distributed to families in a household and that did not change anything, and finally they implemented what is known as the hanging of long lasting insecticide treated bed nets.
This time we went into a house with a hammer, nails and ropes, and families showed us their bedroom and we hung the net for them. And yet malaria still rules. What happened with the free bed nets is now widely reported across different countries in Africa.
What do the numbers we measure mean to the people they represent?
 As an example, there was a man in a small fishing village with seven children. His biggest worry was how to get food for his family. So the world of numbers develops numbers-based interventions, numbers-driven solutions. Reporters found months after the family received the mosquito nets that no one in the family slept under the mosquito nets; instead the man had sown the nets together and used them for fishing to feed his family.
As an example, there was a man in a small fishing village with seven children. His biggest worry was how to get food for his family. So the world of numbers develops numbers-based interventions, numbers-driven solutions. Reporters found months after the family received the mosquito nets that no one in the family slept under the mosquito nets; instead the man had sown the nets together and used them for fishing to feed his family.
Frustrations abound on both ends of the system, for public health agents and community members. Numbers act as the barrier between the two ends of the “system”, and our goal must be to break the barrier. The numbers that drive interventions can be meaningless to the community people they represent unless we engage the community and learn how our interventions can really help them.
Ebola &Hearing Loss &Lassa Fever &Zika Bill Brieger | 03 Mar 2018
World Hearing Day and the Problem of Infectious and Tropical Diseases
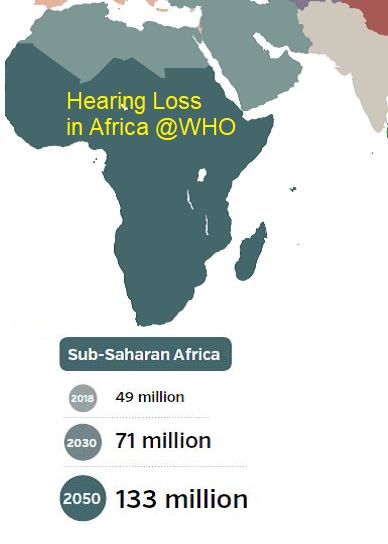
 March 3rd marks the annual World Health Day. The World Health Organization explains that the purpose of this day is to raise awareness on how to prevent deafness and hearing loss and promote ear and hearing care across the world. WHO notes that, “Unless action is taken, by 2030 there will be nearly 630 million people with disabling hearing loss.”
March 3rd marks the annual World Health Day. The World Health Organization explains that the purpose of this day is to raise awareness on how to prevent deafness and hearing loss and promote ear and hearing care across the world. WHO notes that, “Unless action is taken, by 2030 there will be nearly 630 million people with disabling hearing loss.”
Factors associated with health loss and disability include ageing of the population, environmental noise exposure, certain medications, and infectious diseases. It is the latter that we address here.
 Globally there are several infectious diseases associated with hearing loss. In children these include congenital rubella infections a direct result of bacterial meningitis infections, although with improved immunization rates these are less of a problem. In contrast Congenital cytomegalovirus infection has been on the increase.
Globally there are several infectious diseases associated with hearing loss. In children these include congenital rubella infections a direct result of bacterial meningitis infections, although with improved immunization rates these are less of a problem. In contrast Congenital cytomegalovirus infection has been on the increase.
Continuing study of Ebola, Lassa Fever and Zika point to infectious tropical diseases as another serious concern. The large scale of infection and survisorship in Ebola outbreak in West Africa made it possible to study on a large scale reported symptoms of “post-Ebolavirus disease syndrome” (PEVDS) that include, “chronic joint and muscle pain, fatigue, anorexia, hearing loss, blurred vision, headache, sleep disturbances, low mood and short-term memory problems.” A study of 277 Ebola Survivors in one Sierra Leone community found the following clinical sequelae were common: arthralgias (76%), new ocular symptoms (60%), uveitis (18%), and auditory symptoms (24%).
 Lassa Fever has unfortunately made a strong showing in West Africa this dry season. Mateer and colleagues noted an association between Lassa fever (LF) and sudden-onset sensorineural hearing loss (SHNL) was confirmed clinically in 1990. Their literature review found that, “Although LF-induced SNHL has been documented, the prevalence and economic impact in endemic regions may be underestimated.”
Lassa Fever has unfortunately made a strong showing in West Africa this dry season. Mateer and colleagues noted an association between Lassa fever (LF) and sudden-onset sensorineural hearing loss (SHNL) was confirmed clinically in 1990. Their literature review found that, “Although LF-induced SNHL has been documented, the prevalence and economic impact in endemic regions may be underestimated.”
Finally, while much of the focus on the complications of Zika have focused on microcephaly, other problems occur. Zare Mehrjardi et al. documented that Zika Virus may cause “other central nervous system abnormalities such as brain parenchymal atrophy with secondary ventriculomegaly, intracranial calcification, malformations of cortical development (such as polymicrogyria, and lissencephaly-pachygyria), agenesis/hypoplasia of the corpus callosum, cerebellar and brainstem hypoplasia, sensorineural hearing-loss, and ocular abnormalities as well as arthrogryposis in the infected fetuses.”

The benefits of vaccines for rubella and meningitis should spur on immunization research for Ebola, Zika and Lassa Fever. In the meantime there are some preventive measures. One would not have thought that using personal protective equipment by health workers would protect hearing, but it is a practice that should be enabled and encouraged for multiple reasons. Household and community control of Aedes aegypti and rodent breeding to prevent Zika and Lassa, respectively, can also help. By protecting our communities from infection we can also protect their hearing.