Burden &Funding &Health Education &Health Systems &Invest in Malaria Control &ITNs &Management Bill Brieger | 19 Nov 2018
Malaria funding may never be enough, but better program management should be possible
 The World Malaria Report shows that malaria cases are up, and even though there are fewer reported cases in 2017 than 2010, the number is greater than 2016. So once again high burden countries are being targeted. Today this focus is on “High Burden to High Impact”, but in 2012-13 it was the “Malaria Situation Room” that also focused on 10 high burden countries.
The World Malaria Report shows that malaria cases are up, and even though there are fewer reported cases in 2017 than 2010, the number is greater than 2016. So once again high burden countries are being targeted. Today this focus is on “High Burden to High Impact”, but in 2012-13 it was the “Malaria Situation Room” that also focused on 10 high burden countries.
Progress was being made up to around 2015-16, it then started to reverse. The challenge was not just funding. As the WHO Director General noted in the foreword to the 2018 World Malaria Report (WMR), “Importantly, ‘High burden to high impact’ calls for increased funding, with an emphasis on domestic funding for malaria, and better targeting of resources. The latter is especially pertinent because many people who could have benefited from malaria interventions missed out because of health system inefficiencies.”
 Over the years there have never been enough pledged funds to fully achieve targets, but as funding has never reached desired levels, attention is now being drawn more and more to the source of that funding (more emphasis on domestic/endemic countries) and especially how the health system functions to use the funds that are made available. In 1998 during one of the early meetings establishing the Roll Back Malaria Partnership, a speaker stressed that malaria control could not succeed without concomitant health systems strengthening and reform. That 20-year-old thought was prescient for today’s dilemma.
Over the years there have never been enough pledged funds to fully achieve targets, but as funding has never reached desired levels, attention is now being drawn more and more to the source of that funding (more emphasis on domestic/endemic countries) and especially how the health system functions to use the funds that are made available. In 1998 during one of the early meetings establishing the Roll Back Malaria Partnership, a speaker stressed that malaria control could not succeed without concomitant health systems strengthening and reform. That 20-year-old thought was prescient for today’s dilemma.
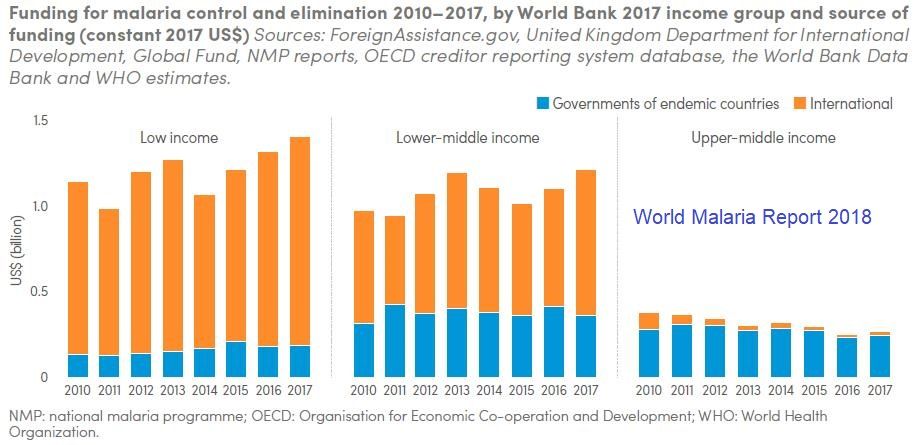
First, what is the funding situation? As outlined in the World Malaria Report …
- In 2017, an estimated US$ 3.1 billion was invested in malaria control and elimination efforts globally by governments of malaria endemic countries and international partners – an amount slighter higher than the figure reported for 2016.
- Governments of endemic countries contributed 28% of total funding (US$ 900 million) in 2017, a figure unchanged from 2016.
- Funding for malaria has remained relatively stable since 2010
- To reach the Global Technical Strategy 2030 targets, it is estimated that annual malaria funding will need to increase to at least US$ 6.6 billion per year by 2020
 The question remains – does investment lead to results. The WMR shows, for example, that “Between 2015 and 2017, a total of 624 million insecticide-treated mosquito nets (ITNs/LLINs), were reported by manufacturers as having been delivered globally. This represents a substantial increase over the previous period 2012–2014, when 465 million ITNs were delivered globally”.
The question remains – does investment lead to results. The WMR shows, for example, that “Between 2015 and 2017, a total of 624 million insecticide-treated mosquito nets (ITNs/LLINs), were reported by manufacturers as having been delivered globally. This represents a substantial increase over the previous period 2012–2014, when 465 million ITNs were delivered globally”.
At the same time the report states that, “Households with at least one ITN for every two people doubled to 40% between 2010 and 2017. However, this figure represents only a modest increase over the past 3 years, and remains far from the target of universal coverage.” Is it simply a matter of funding to reach the other 60% of households, or are there serious management problems on the ground?
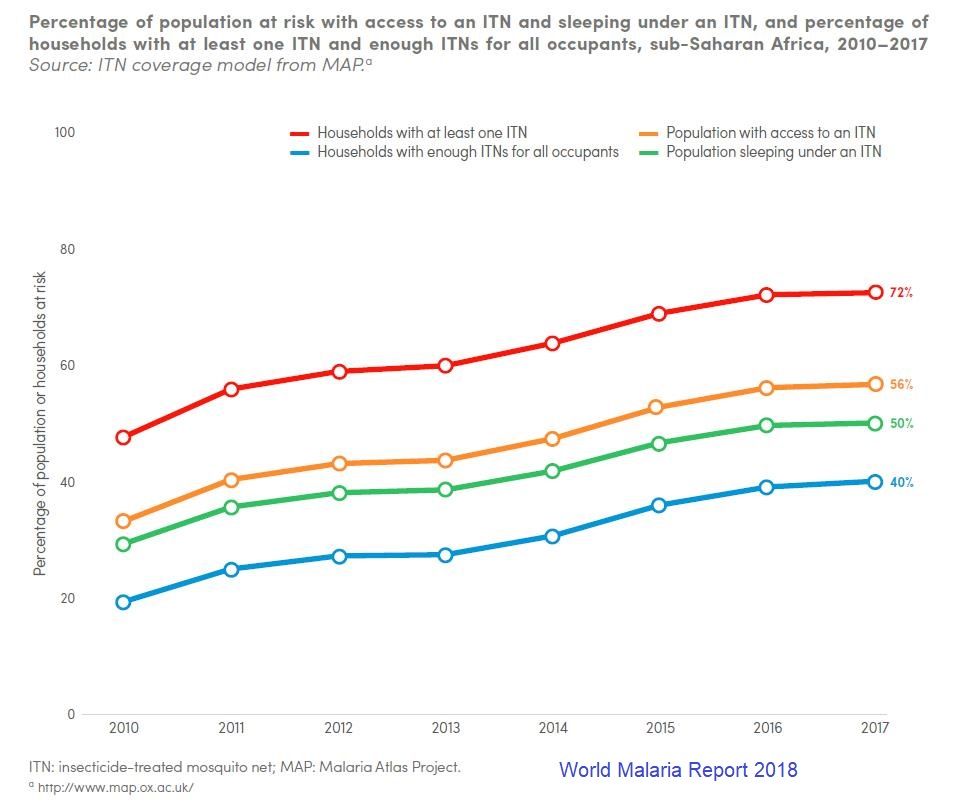 Then there is the issue of using nets. The WMR traces new ownership and use from 2010 to 2017, and we can see that overall the proportion of the population at risk who slept under a net increased from around 30% to 50%, but only 56% of those with access to a net were sleeping under them. This can be attributed in part but not completely to the adequacy of nets in a household.
Then there is the issue of using nets. The WMR traces new ownership and use from 2010 to 2017, and we can see that overall the proportion of the population at risk who slept under a net increased from around 30% to 50%, but only 56% of those with access to a net were sleeping under them. This can be attributed in part but not completely to the adequacy of nets in a household.
We should ask are enough nets getting to the right places, and also are efforts in place to promote their use. Behavior change efforts should be a major component of malaria program management. Even the so called biological challenges to malaria control have a human element. Monkey malaria transmission to people results from deforestation. Malaria parasite resistance to medicines comes from poor drug management on individual and systems levels.
The target year 2030 will be here before we know it. Will malaria still be here, or will countries and donors get serious about malaria financing AND program management?