Diagnosis &Elimination &Ivermectin &MDA &Treatment Bill Brieger | 20 Nov 2016
Leadership and Support for Malaria Pre-Elimination in Nepal
Emmanuel Le Perru, Jhpiego field staff in Nepal, shared his experiences in aiding the malaria pre-elimination efforts in the country during a retreat that preceded the 65th Annual Meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. Here are some highlights of his talk.
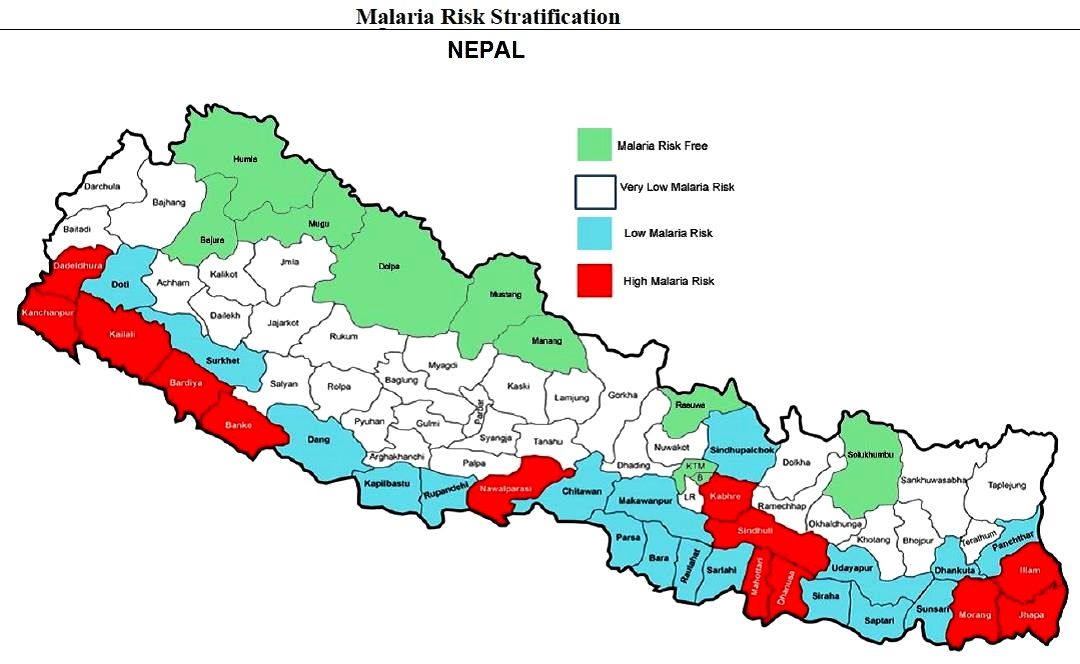 Malaria Pre-Elimination efforts are targeting 0 deaths as well as investigation of 100% of confirmed cases in Nepal. Systematic entomology investigation/interventions are required. Glucose-6-Phosphate Dehydrogenase deficiency (enzyme genetic defect causing hemolysis with primaquine) testing for Plasmodium vivax in high G6PDd prevalence communities is required. Cases should receive treatment within 72 hours of symptoms for Pf (to quickly prevent transmission and gametocyte reservoir). There is also a need to distinguish between indigenous and imported cases.
Malaria Pre-Elimination efforts are targeting 0 deaths as well as investigation of 100% of confirmed cases in Nepal. Systematic entomology investigation/interventions are required. Glucose-6-Phosphate Dehydrogenase deficiency (enzyme genetic defect causing hemolysis with primaquine) testing for Plasmodium vivax in high G6PDd prevalence communities is required. Cases should receive treatment within 72 hours of symptoms for Pf (to quickly prevent transmission and gametocyte reservoir). There is also a need to distinguish between indigenous and imported cases.
Jhpiego is providing technical assistance and capacity building for Nepal’s Ministry of Health pre-elimination efforts as follows:
- Integrated Vector Management
- Micro-stratification
- Entomology curriculum to be conducted in medical college (need new positions)
- Case-based Surveillance guidelines
- Private-sector engagement (for increased reporting and product quality control/procurement such as Antigen RDTs)
- Capacity Assessments in 9 health systems strengthening components at central and district levels (Jhpiego Malaria Implementation Guide)
- Human resources: clear job descriptions and performance goals
- Leadership & Management development program
 Program highlights include the fact that the Global Fund malaria grant rating improved from B2 (inadequate but demonstrating potential) in January 2016, but now A2 (meeting expectations) in November 2016. Concept note for operational research at 2 or 3 border check points has been developed in order to determine whether such intervention (communication & voluntary screening) is cost-effective and relevant to catch/target imported cases, raise awareness on malaria available services, detect/prevent sources of potential outbreaks. This will inform GFATM on the relevance to fund such intervention. A similar approach was done at the China-Myanmar border but was not recognized by not WHO.
Program highlights include the fact that the Global Fund malaria grant rating improved from B2 (inadequate but demonstrating potential) in January 2016, but now A2 (meeting expectations) in November 2016. Concept note for operational research at 2 or 3 border check points has been developed in order to determine whether such intervention (communication & voluntary screening) is cost-effective and relevant to catch/target imported cases, raise awareness on malaria available services, detect/prevent sources of potential outbreaks. This will inform GFATM on the relevance to fund such intervention. A similar approach was done at the China-Myanmar border but was not recognized by not WHO.
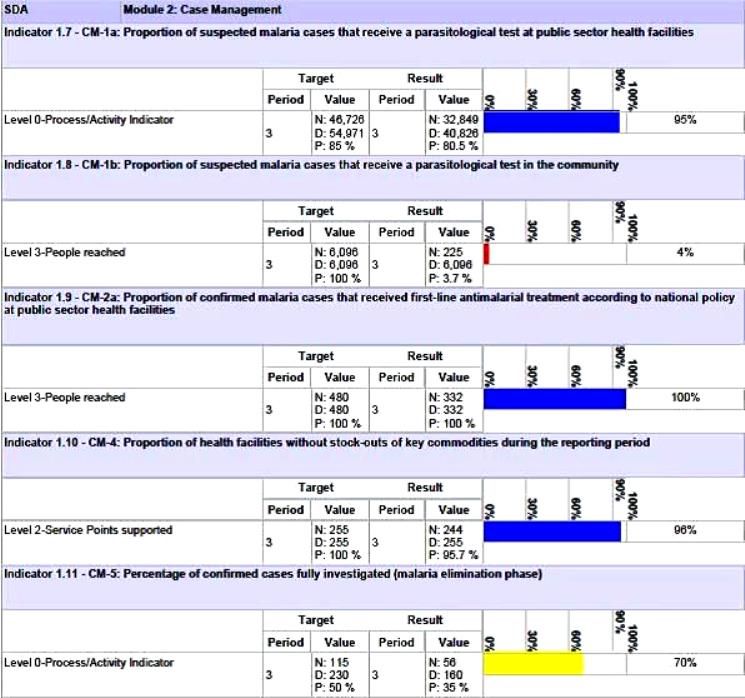
Nepal’s Global Fund Grant Indicators for Malaria Case Management
Although the National Malaria Strategic Plan refers to high risk groups (forest workers, national parks security personnel, refugees, prisoners, etc.) evidence is needed to back this up. A study or improved investigation forms are needed to identify such groups and use this information to design appropriate behavior change communications and other interventions.
Special Programming Highlights include proposing a focus on Closed/Isolated Settings/Foci (limited migration, duration and population) to WHO and GFATM. Considering a targeted mass drug administration (MDA) Plasmodium vivax (not yes recommended by WHO) with Primaquine/G6PD testing. Consideration is being given to new drugs in the pipeline such as Ivermectin. Molecular Testing using Polymerase Chain Reaction (PCR) to detect low parasitemia, asymptomatic or re-infection cases (Pv includes inactive/dormant sporozoites known as hypnozoites) is being proposed.
Community based testing as proposed in the Global Fund grant needs strengthening. Therefore RDT use by Female Community Health Volunteer is being considered. Active case detection is another possibility for those areas moving toward pre-elimination. As mentioned, there is also need for studies of asymptomatic infection.
Lessons learned so far for best practices for efforts in identifying specific pre-elimination interventions include the value of getting consensus at national level through the Malaria Technical Working Group. There is also need to challenge WHO recommendations and engage dialogue to get creative. At present there is a risk of a Catch 22 situation wherein the GFATM asks for innovative interventions but at the same time tries to adhere strictly WHO to existing guidance.
The Nepalese malaria program is in constant dialogue with the GFATM Fund Portfolio Manager and team on the local context and technical challenges in order to get them involved in looking for innovative solutions.
Challenges arise in malaria diagnostics. While systematic microscopy is the gold standard, quality can be poor because of low stain/re-agent quality, constant staff turnover and donor reluctance to fund additional training. Also microscopy confirmation and slide quality control are time consuming, and often this process is not clear or well followed. PCR require specific equipment, training and qualifications. Takes time to be operational.
There are opportunities moving forward. Progress could be made if there were more “elimination experts” to position to influencer to WHO to seek and propose new interventions for the pre-elimination stage. Nepal provides an ideal opportunity to test new ideas. It will also be necessary for the national malaria program staff to receive regular technical updates on program issues such as new drugs (Ivermectin?) and on-going pilots of MDA.
Diagnosis &NTDs &Schistosomiasis Bill Brieger | 19 Nov 2016
Identifying a More Accurate Test for Schistosomiasis in The Gambia
During the recently concluded 65th Annual Meeting of the American Society of Tropical Meicine and Hygiene colleagues from The Gambian Ministry of Health and Social Welfare, the World Health Organization and the NTD Support Center presented a poster entitled, “Field Performance of a Circulating Cathodic Antigen Rapid Test at Point-Of-Care for Mapping Schistosomiasis-Endemic Districts in Gambia.” The authors included Bakary Sanneh, Kristen Renneker, Joof Ebrima, Sanyang M. Abdoulie, Camara Yaya, Sambou M. Sana, Sey Alhagie Papa, Jagne Sherifo, Baldeh Ignacious, Louis-Albert Tchuem Tchuente, Patrick J Lammie, and Kisito Ogoussan. Their abstract appears below.
 Background: The traditional parasitological Kato Katz smears and urine filtration methods recommended by the World Health Organization (WHO) to implement mapping of schistosomiasis have been found to be less sensitive in the detection of light-intensity schistosomiasis infections. Field surveys in Sub-Sahara Africa have shown that the Circulating Cathodic Antigen (CCA) point-of-care (POC) test is more accurate for detecting Schistosoma mansonia than the microscopic Kato Katz technique.
Background: The traditional parasitological Kato Katz smears and urine filtration methods recommended by the World Health Organization (WHO) to implement mapping of schistosomiasis have been found to be less sensitive in the detection of light-intensity schistosomiasis infections. Field surveys in Sub-Sahara Africa have shown that the Circulating Cathodic Antigen (CCA) point-of-care (POC) test is more accurate for detecting Schistosoma mansonia than the microscopic Kato Katz technique.
Aim: To establish the field sensitivity and specificity of POC CCA as mapping tool to provide the endemicity of schistosomiasis in The Gambia.
Methods: A cross-section study …
- Ten school per region in 4 regions with historical known risk
- Fifty children aged 7 to 14 years: 25 boys and 25 girls (WHO Mapping sampling guide)
- Stool, urine and finger pricks samples were examined for Schistosomiasis
- Parasitological tests: 2 Kato-katz slides to read from each stool sample, and urine filtration technique, urine dip-stick and Circulating Cathodic Antigen (CCA) techniques,
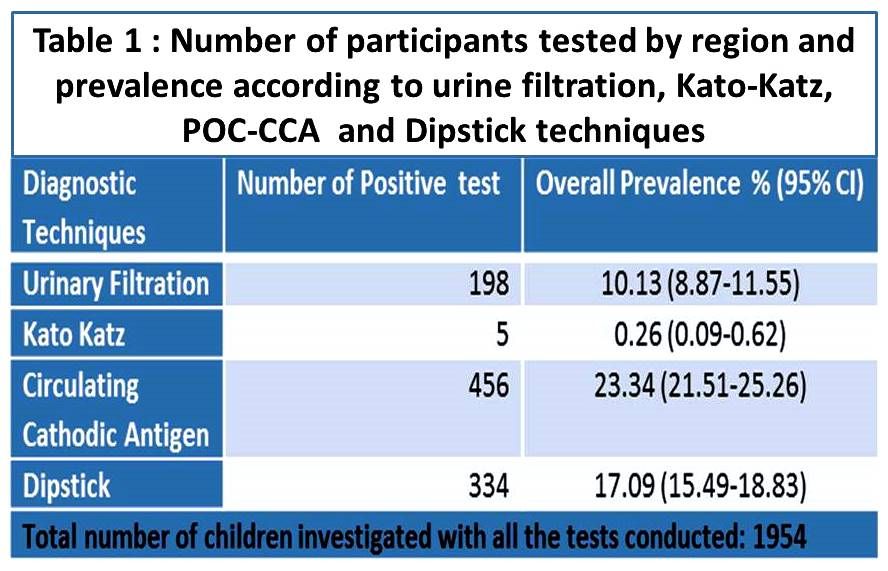 Discussion: The CCA prevalence in this study was 23.34% (95% CI, 21.51-25.26%) two times higher than the prevalence based on egg-detection for S. haematobium and S.mansoni (10.13,95% CI 8.87-11.55; and 0.26%, (95% CI, 0.09-0.62, respectively). Although The Gambia is thought to be endemic for only S. haematobium, yet 5 subjects were found to harbor S. mansoni. Three of the 5 individuals from the high endemic schistosomiasis regions were co-infected with S. haematobium and S. mansoni.
Discussion: The CCA prevalence in this study was 23.34% (95% CI, 21.51-25.26%) two times higher than the prevalence based on egg-detection for S. haematobium and S.mansoni (10.13,95% CI 8.87-11.55; and 0.26%, (95% CI, 0.09-0.62, respectively). Although The Gambia is thought to be endemic for only S. haematobium, yet 5 subjects were found to harbor S. mansoni. Three of the 5 individuals from the high endemic schistosomiasis regions were co-infected with S. haematobium and S. mansoni.
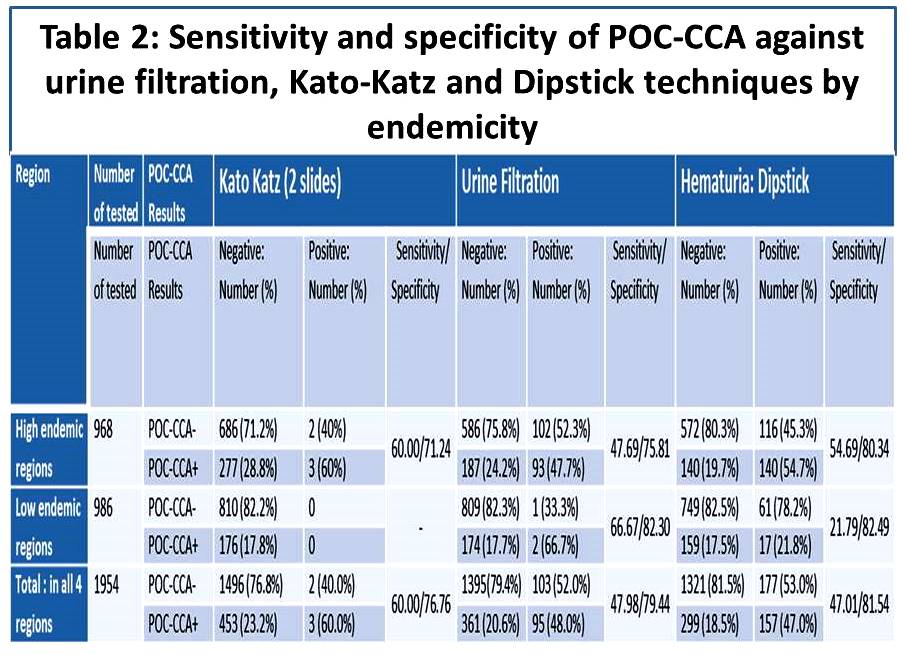 The sensitivity of the POC-CCA proved to be relatively high (60.0%), using double Kato-Katz as a reference for S. mansoni detection, although few infections were found, 5 out 1954 tested. The specificity of the POC CCA was 76.8%, respectively. Using urine filtration as reference standard for the detection of S. haematobium, the sensitivity of POC-CCA was 47.9% and the specificity was 79.4%.
The sensitivity of the POC-CCA proved to be relatively high (60.0%), using double Kato-Katz as a reference for S. mansoni detection, although few infections were found, 5 out 1954 tested. The specificity of the POC CCA was 76.8%, respectively. Using urine filtration as reference standard for the detection of S. haematobium, the sensitivity of POC-CCA was 47.9% and the specificity was 79.4%.
Conclusion: The Gambia is endemic for both urinary and intestinal schistosomiasis although most of the infections are due to S. haematobium in the 4 regions investigated. The results of the study showed a low sensitivity of the POC-CCA test in detecting S. haematobium and therefore we conclude further research is needed to develop an ideal rapid diagnosis tool for urinary schistosomiasis.
 Acknowledgement: Thanks to the Mapping Team, Consultants, MoHSW, WHO, Task Force for Global Health (TFGH) for all their support. For questions please contact: Dr. Kisito Ogoussan, kogoussan@taskforce.org; or Mr. Bakary Sanneh, sheikbakary@yahoo.com
Acknowledgement: Thanks to the Mapping Team, Consultants, MoHSW, WHO, Task Force for Global Health (TFGH) for all their support. For questions please contact: Dr. Kisito Ogoussan, kogoussan@taskforce.org; or Mr. Bakary Sanneh, sheikbakary@yahoo.com
Community &Eradication &Malaria in Pregnancy &Women Bill Brieger | 18 Nov 2016
Malaria Mass Drug Administration: Ensuring Safe Care of Reproductive Age Women
The potential impact of mass malaria drug administration (MDA) on pregnant women was the focus of Symposium 146 at the recent 65th Annual Meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The symposium was co-chaired by Clara Menéndez and Larry Slutsker who opened the session with an overview.
 As malaria control interventions are scaled up and sustained and malaria transmission levels decline and prevalence falls, an increasing number of countries are starting to see elimination on the horizon. For pregnant women, the antimalarial antibodies that have provided some level of protection in moderate to high malaria transmission settings are reduced as malaria transmission declines.
As malaria control interventions are scaled up and sustained and malaria transmission levels decline and prevalence falls, an increasing number of countries are starting to see elimination on the horizon. For pregnant women, the antimalarial antibodies that have provided some level of protection in moderate to high malaria transmission settings are reduced as malaria transmission declines.
Current evidence shows that as transmission levels decline, the consequences from P. falciparum malaria are even greater for pregnant women. As countries enter pre-elimination stage and move towards eventual elimination, it will be important to address the needs of pregnant women given their increased vulnerability.
To help achieve elimination, countries are exploring strategies involving widespread distribution of anti-malarials, primarily artemisinin-combination therapies (ACTs), to asymptomatic individuals, including both mass drug administration (MDA) and mass screen and treat (MSaT).
Animal studies have suggested potential embryo toxicity and teratogenic effects of artemisinin drugs in the first trimester of pregnancy.
Given the limited human data, ACTs are currently contraindicated in first trimester, except in documented cases of clinical malaria illness where quinine is unavailable. This poses a challenge in mass campaigns, as it requires the identification of women in early pregnancy who are not yet obviously pregnant. Screening including offering pregnancy tests and/or interview to ask a woman her pregnancy status directly may not work as many may not wish to reveal their pregnancy status.
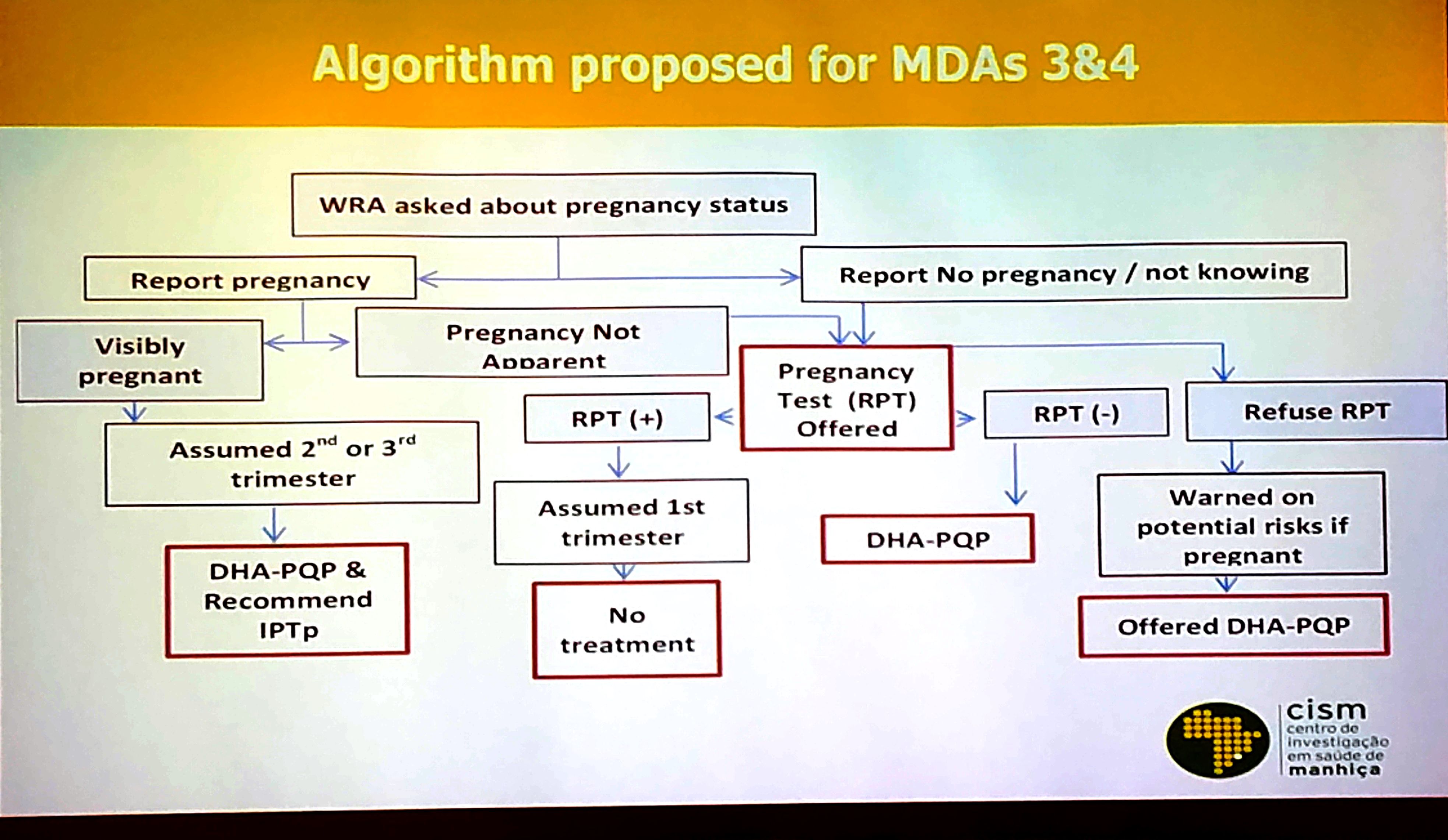
Final Algorithm for Screening Prior to MDA in Mozambique
While only about 5% of the population is pregnant at any given time, and only 1/3 of those are in the first trimester, approximately 20% of the population is comprised of women of reproductive age who may be pregnant. Thus, the number of women who need to be screened for pregnancy is substantial across countries. In addition to privacy issues, costs of screening processes are another barrier.
During the symposium Francisco Saúte from Mozambique and Samuel J. Smith from Sierra Leone shared experiences. Clara Menéndez addressed ethical issues involved in the potential risk of MDA with the ACT Dihydroartemisinin-Piperaquine (DHA-P). These two countries have addressed pregnant women in MDAs in two widely different contexts.
Mozambique is learning whether MDA is a valuable component to malaria elimination in the low transmission areas in the southern part of the country. In Sierra Leone MDA was seen as a lifesaving tool to prevent malaria deaths during the Ebola epidemic when taking blood samples for diagnosis was a major risk.
Over several rounds of MDA, Mozambique refined its pregnancy screening procedures over several rounds of MDA as seen in the attached slide. Costs, confidentiality, convenience and efficiency entered into the equation that saw a greater focus on communicating with women rather that testing. Lessons learned from MDA in Mozambique included –
- Screening for early pregnancy in the context of MDA is challenging, particularly among teenage girls where disclosing pregnancy can be problematic
- Need to train field workers (preferably women) about the need to ensure confidentiality of pregnancy testing/results
- Confidentiality is also crucial to ensure adherence to t

MDA Rationale in Sierra Leone during Ebola Outbreak
he pregnancy testing
- Women not accepting pregnancy test must be warned on risks/ benefits of ACTs in 1st trimester
- Health authorities must understand that IPTp and MDA are not mutually exclusive

The Ebola epidemic in Sierra Leone and its neighbors, Liberia and Guinea, devastated the health workforce, and the availability of any sort of testing supplies was low. The country experienced a major drop in utilization of clinic based MCH services including those for malaria during the period.

MDA Goals in Sierra Leone
Because of initial similarities in presenting symptoms between Ebola and malaria, people were often fearful of going to the health center in case they were detained for Ebola care or were exposed to other patients who had Ebola. Community MDA seemed to be one way to protect the population from malaria in this emergency situation. The attached slide offers a rational for the MDA. A second slide explains Sierra Leone’s goal for MDA with Artesunate-Amodiaquine in the context of Ebola. Though not completely, the Sierra Leone MDAs were able to exclude pregnancy women in their first trimester.

Pregnant women excluded from MDA in Sierra Leone
In conclusion MDA is a tool conceived primarily for countries and areas of countries as part of the pre-elimination strategy. It presents a variety of logistical challenges, but a major concern should also be the ethical issues of giving a potentially toxic drug to women in their first trimester of pregnancy. Alternative strategies to protect these women, including insecticide treated nets, must be explored.
Diagnosis &Ebola Bill Brieger | 17 Nov 2016
Mobile suitcase laboratory: A tool for the rapid detection of emerging and endemic infectious disease
Ahmed Abd El Wahed who is based at Georg-August University, Goettingen, Germany shares his experiences with development and use of field diagnostics that can fit in a suitcase. This work received support from the UNICEF/UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases, Geneva, Switzerland. He explains the concept here …
Laboratory diagnosis mainly depends on nucleic acid detection by real-time polymerase chain reaction (PCR), which is available in central laboratories and has a turnaround time of more than two hours. Since real-time RT-PCR assays are not suitable for on-site screening, samples collected from local hospitals, treatment center or at the site of an outbreak have to be sent to laboratories over long distances for testing.
In developing countries, the necessary equipment for diagnosis is only available in few central laboratories, which are not accessible and of limited capacity to test large numbers of incoming samples. Moreover, transport conditions of samples are inadequate and therefore lead to unreliable results.
 For decentralizing of the molecular diagnostics, there is a need for a simple molecular point-of-need test. We have developed a mobile suitcase laboratory (62+49+30 cm) containing all reagents and equipment for the detection of the nucleic acid of infectious agents using the recombinase polymerase amplification (RPA) technology. The RPA assay run at a constant temperature (42°C) for a maximum of 15 minutes.
For decentralizing of the molecular diagnostics, there is a need for a simple molecular point-of-need test. We have developed a mobile suitcase laboratory (62+49+30 cm) containing all reagents and equipment for the detection of the nucleic acid of infectious agents using the recombinase polymerase amplification (RPA) technology. The RPA assay run at a constant temperature (42°C) for a maximum of 15 minutes.
Moreover, all reagents are cold-chain independent and the mobile laboratory is operated by a solar power battery. The nucleic acid extraction is performed by a magnetic bead based method, in which a simple fast lysis protocol is applied. In case of highly infectious agents such as Ebola virus, the inactivation step was performed in a glovebox.
The suitcase lab is designed to detect almost 30 pathogens such as Dengue, Zika, Chikungunya, Ebola, Coronaviruses as well as Tuberculosis, Leptospira, Salmonella typhi and paratyphi, malaria, avian influenza, and Leishmania.
The suitcase lab featured in a presentation at the 65th Annual Meeting of the American Society of Tropical Medicine in Atlanta under the title of “Novel Extraction Protocol and Recombinase Polymerase Amplification Assay for Detection of Leishmania Donovani In 30 Minutes.” Authors/presenters included Dinesh Mondal, Prakash Ghosh, Md. Anik Ashfaq Khan, Faria Hossain, Susanne Böhlken-Fascher, Greg Matlashewski, Axel Kroeger, Piero Olliaro, and Ahmed Abd El Wahed.
Their work highlighted Leishmania donovani (LD), a protozoan parasite transmitted to humans by sand flies, which causes Visceral Leishmaniasis (VL). Currently, diagnosis is based on presence of anti-LD antibodies and clinical symptoms. Molecular diagnosis would require real-time PCR, which is not easy to implement at field settings.
In this study, we report on the development and testing of a novel extraction protocol in combination with recombinase polymerase amplification (RPA) assay for the detection of LD. The LD RPA assay detected equivalent to one LD genomic DNA. The RPA assay was performed at constant temperature (42°C) and the total assay runtime including the extraction procedure was 30 minutes.
The RPA assay also detected other Leishmania species (L. major, L. aethiopica and L. infantum), but did not identify nucleic acid of other pathogens. Forty-eight samples from VL, asymptomatic and post-kala-azar dermal leishmaniasis subjects were detected positive and 48 LD negative samples were negative by both LD RPA and real-time PCR assays, which indicates 100% agreement.
To allow the use of the assay at field settings, a mobile suitcase laboratory (56+45.5+26.5 cm) was developed and operated at the local hospital in Mymensingh, Bangladesh by using a solar-powered battery. DNA extraction was performed by a novel magnetic bead based method, in which a simple fast lysis protocol was applied.
Community &IPTp &Malaria in Pregnancy Bill Brieger | 16 Nov 2016
Gaining an early start to IPTp through promotion of MIP at the community level in Kenya
 A poster entitled “Community health: Improving start of IPTp early in second trimester through promotion of MIP at the community level in Kenya” was presented by Augustine Ngindu, Gathari Ndirangu, E Nyapada, David Omoit, and Mildred Mudany from Jhpiego’s Kenya Team at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
A poster entitled “Community health: Improving start of IPTp early in second trimester through promotion of MIP at the community level in Kenya” was presented by Augustine Ngindu, Gathari Ndirangu, E Nyapada, David Omoit, and Mildred Mudany from Jhpiego’s Kenya Team at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
WHO policy recommends that pregnant women living in moderate to high malaria transmission areas start receiving intermittent preventive treatment in pregnancy (IPTp) with sulfadoxine pyrimethamine (SP) early in second trimester to prevent malaria in pregnancy (MIP).

Training Community Health Volunteers in Bungoma
In Bungoma County, Kenya, 52% of pregnant women start IPTp in their third trimester. Between June and September 2015, 197 Community Health Assistants (CHAs) were trained, who in-turn trained 2,344 Community Health Volunteers (CHVs) in Bungoma County.
Following the training, CHVs registered new pregnant women at their homes and encouraged them to seek antenatal care (ANC) and start taking IPTp early in the second trimester. The CHVs also helped to identify previously registered women who were not attending ANC and refer them to ANC for MIP services.
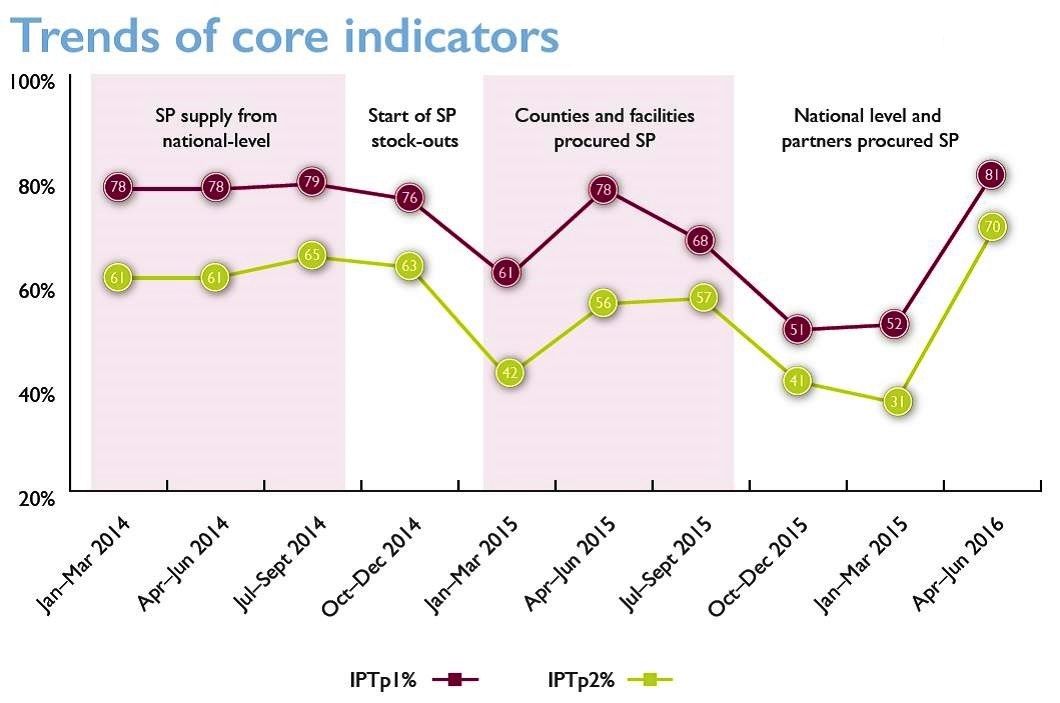
The CHVs, with CHA supervision, reached 44,133 pregnant women with MIP messages on starting IPTp early in the second trimester and use of a net. Data from 70 health facility registers was collected biannually and showed a 12% increase (24%-36%) in the proportion of pregnant women starting ANC attendance ? 20 weeks of pregnancy between October 2014 and March 2016.

Community Health Volunteers Encourage ANC Attendance
Although there was a decline in the proportion of women receiving IPTp-SP between October 2014 and January 2015 and between October 2015 and February 2016 due to SP stock-outs, this did not significantly affect ANC attendance. The 12% increase in early ANC attendance is likely associated with CHV efforts in sensitizing women to start IPTp early in the second trimester and indicates a positive change in health seeking behaviour that can be sustained over time provided the commodities are available.
The success with CHVs promoting MIP at the community level has led to it being replicated in three additional counties and it will be extended in phases in other malaria endemic counties.
Advocacy &IPTi &Malaria in Pregnancy Bill Brieger | 16 Nov 2016
Country Updates on Global Call to Action to Increase Coverage of Intermittent Preventive Treatment in Pregnancy
Symposium 87 at the 65th Annual Meeting of the American Society of Tropical Medicine and Hygiene focused on the Global Call to Action to Increase Coverage of Intermittent Preventive Treatment in Pregnancy: Progress and Lessons Learned. The original Global Call was initiated at a previous ASTMH meeting. Elaine Roman of Jhpiego chaired the session. Panelists included Julie Gutman of the US CDC, Frank Chacky of the NMCP in Tanzania, Yacouba Savadogo of the NMCP in Burkina Faso and Fannie Kachale of the Reproductive Health Directorate in the Malawi MOH.
 The symposium speakers reviewed country progress in sub-Saharan Africa (SSA) in increasing intermittent preventative treatment in pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP). They described how Ministries of Health and donors and partners are working to increase IPTp-SP coverage to address malaria in pregnancy (MiP).
The symposium speakers reviewed country progress in sub-Saharan Africa (SSA) in increasing intermittent preventative treatment in pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP). They described how Ministries of Health and donors and partners are working to increase IPTp-SP coverage to address malaria in pregnancy (MiP).
Following the release of the World Health Organization’s (WHO) 2012 updated policy on IPTp-SP, a number of global stakeholders came together through the Roll Back Malaria-Malaria in Pregnancy Working Group, to elaborate the Global Call to Action: To Increase National Coverage with IPTp of MiP for Immediate Impact. The Call to Action calls upon countries and partners to immediately scale up IPTp-SP to improve health outcomes for mothers and their newborns. Scaling up IPTp-SP across most countries in sub-Saharan Africa remains a critical weapon to prevent the devastating consequences of MiP.
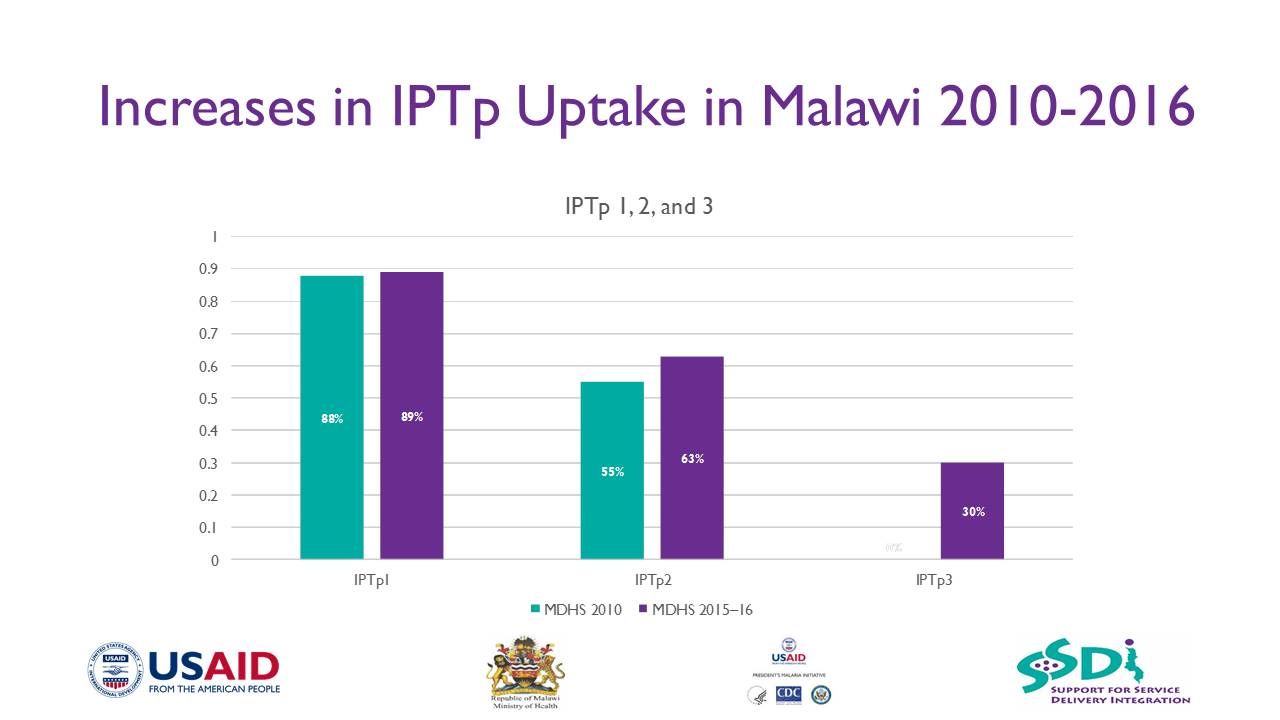
IPTp3+ has been started in Malawi following WHO recommendations
However, the low proportion of eligible pregnant women receiving at least one dose of IPTp-SP (52%) and IPTp3-SP (17%) in 2014 is unacceptable. Despite growing parasite resistance to SP in some areas, IPTp-SP remains Tuesday a highly cost-effective, life-saving strategy to prevent the adverse effects of MiP in the vast majority of SSA.
Completion of the recommended three or more doses of IPTp-SP decreases the incidence of low birthweight (LBW) by 27%, severe maternal anemia by 40% and neonatal mortality by 38%. This symposium will feature presentations from WHO and the President’s Malaria Initiative on how they are prioritizing support to scale up MiP interventions including IPTp-SP across SSA.
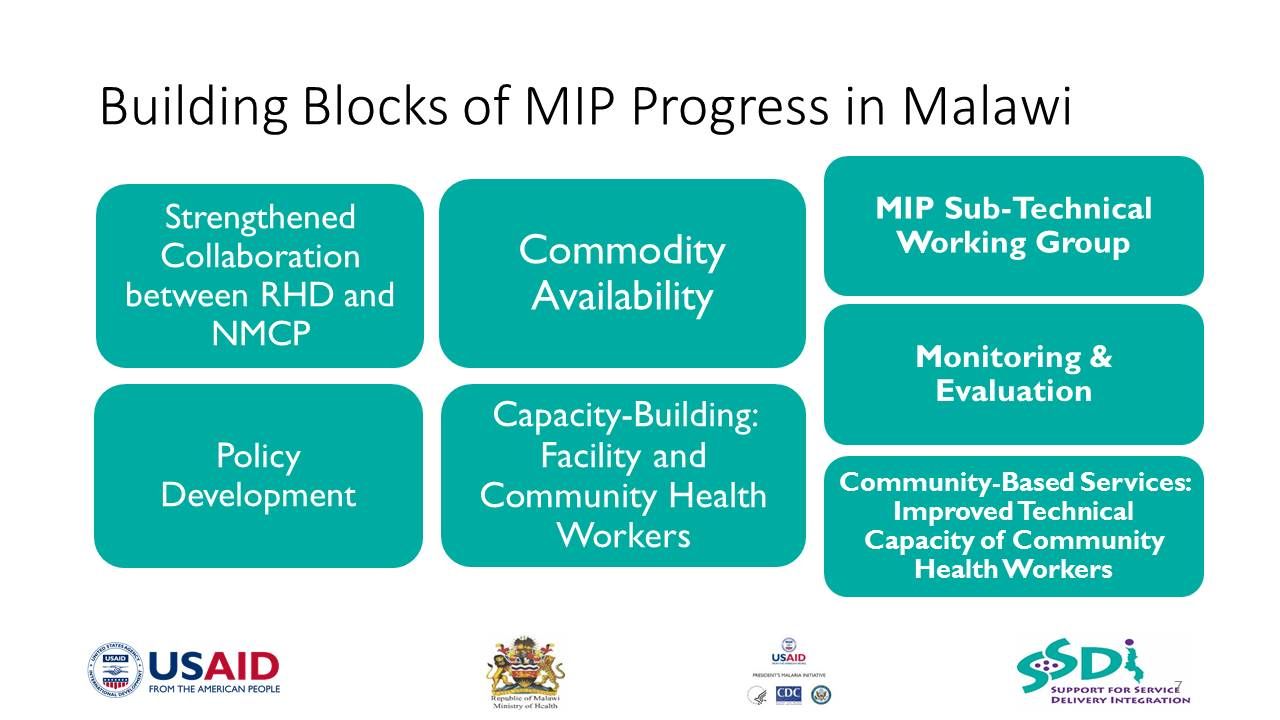
Panelists from Burkina Faso, Malawi and Tanzania discussed how they were able to dramatically scale up IPTp-SP through a health systems approach that addresses MiP from community to district to national level.
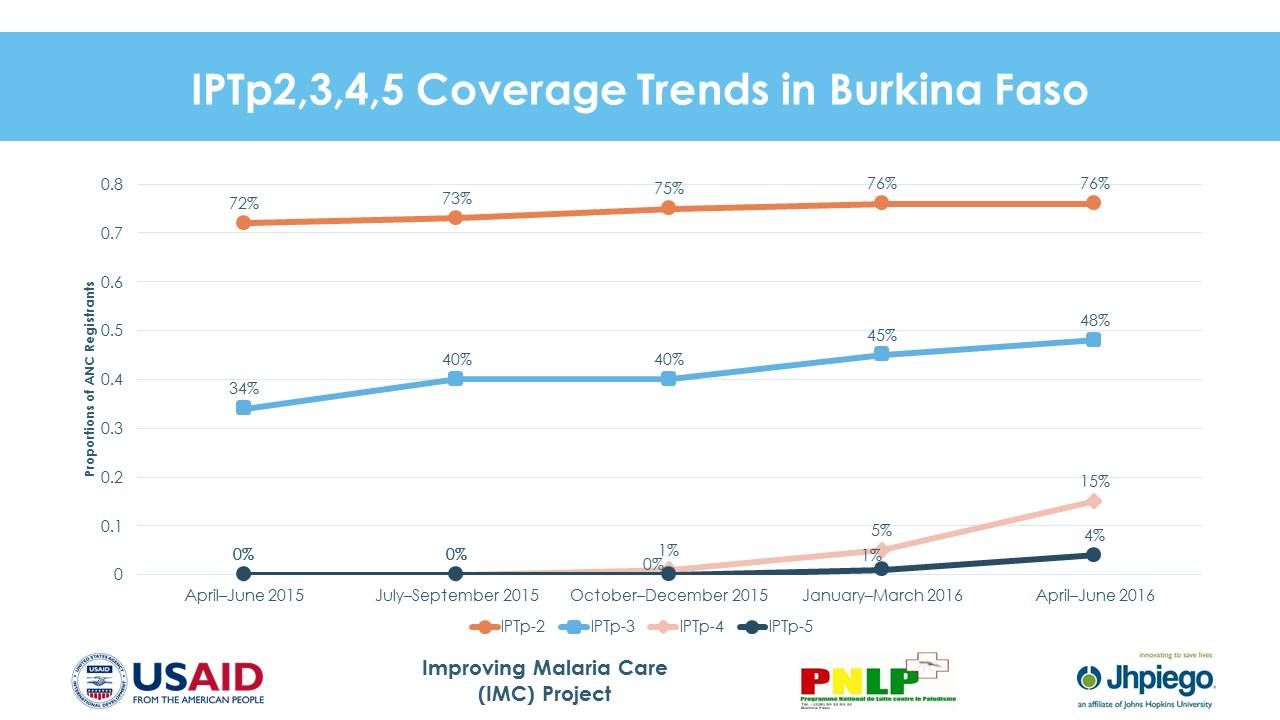 In Burkina Faso, IPTp2-SP increased from 54.8% in 2013 to 82.3% nationally in 2015 and IPTp3-SP increased from 13.5% in 2014 to 41.2% nationally in 2015. Moving ahead Burkina Faso will Improve SP supply chain management, Pilot an IPTp distribution at the community level in three districts, Provide job aids throughout ANC clinics, and Provide support to district team for data review and analysis.
In Burkina Faso, IPTp2-SP increased from 54.8% in 2013 to 82.3% nationally in 2015 and IPTp3-SP increased from 13.5% in 2014 to 41.2% nationally in 2015. Moving ahead Burkina Faso will Improve SP supply chain management, Pilot an IPTp distribution at the community level in three districts, Provide job aids throughout ANC clinics, and Provide support to district team for data review and analysis.
In Malawi, in targeted project sites across 15 districts, IPTp1 uptake increased from 44% in 2012 to 87% in 2015, while IPT2 increased from 16% to 61% over the same time period. Lessons learned from scale up include –
- Consistent availability of SP for IPTp is critical to increasing coverage
- A clear policy put in place to guide IPTp implementation is crucial

- A strong partnership between the Reproductive Health Directorate and National Malaria Control Programme is necessary
- Intensification of information, education, and communication is crucial to increase uptake of ANC services
- Strong collaboration, planning, and coordination between partners and other stakeholders improve ANC attendance
- Antenatal clinics offers enormous opportunities for delivering the malaria prevention package, such as IPTp and insecticide-treated nets, to pregnant women
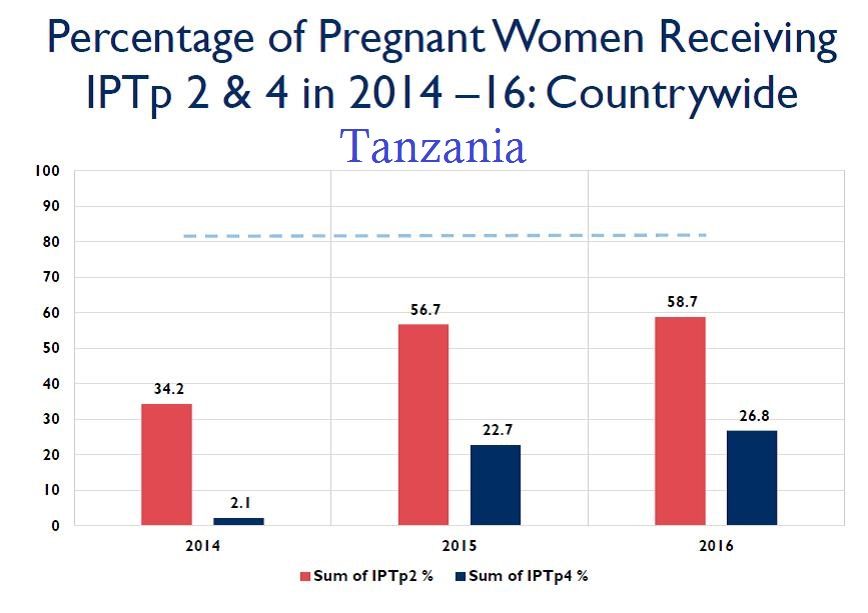 In Tanzania, IPTp2-SP increased from 34% in 2014 to 57% in 2015 and IPTp4-SP was reported at 22% in 225 facilities across 16 districts, in 2015. Program learning in Tanzania identified that consistent availability of commodities at facility level can complement Government’s and partners’ efforts to ensure provision of quality MiP services. Despite increased number of trained health care workers and regular supportive supervision and mentoring, increasing uptake of IPTp will continue to be a challenge unless malaria commodities such as mRDT and SP are available at health facilities. Redistribution of commodities among facilities could be crucial balancing the stock.
In Tanzania, IPTp2-SP increased from 34% in 2014 to 57% in 2015 and IPTp4-SP was reported at 22% in 225 facilities across 16 districts, in 2015. Program learning in Tanzania identified that consistent availability of commodities at facility level can complement Government’s and partners’ efforts to ensure provision of quality MiP services. Despite increased number of trained health care workers and regular supportive supervision and mentoring, increasing uptake of IPTp will continue to be a challenge unless malaria commodities such as mRDT and SP are available at health facilities. Redistribution of commodities among facilities could be crucial balancing the stock.
 Moving forward Tanzania plans to use alternative funding to procure malaria commodities at health facility (e.g., Community Health Fund, National Health Insurance Fund, basket fund). Other efforts will include conducting onsite mentorship and coaching, data collection and interpretation, selecting sentinel sites for collecting IPTp3, working with Ministry of Health HMIS to revise HMIS tools when opportunity arises, and training Community Health Workers (CHWs) on maternal, neonatal and child health interventions including early booking of ANC services.
Moving forward Tanzania plans to use alternative funding to procure malaria commodities at health facility (e.g., Community Health Fund, National Health Insurance Fund, basket fund). Other efforts will include conducting onsite mentorship and coaching, data collection and interpretation, selecting sentinel sites for collecting IPTp3, working with Ministry of Health HMIS to revise HMIS tools when opportunity arises, and training Community Health Workers (CHWs) on maternal, neonatal and child health interventions including early booking of ANC services.
These three country examples demonstrate that progress is challenging but possible. The call to action for increased IPTp access and use is stronger today.
IPTi &Malaria in Pregnancy &Procurement Supply Management Bill Brieger | 15 Nov 2016
Improving IPTp uptake and mitigating Stock-outs in Bungoma County, Kenya
A poster entitled “Improving Pregnancy Outcomes: Alleviating Stock-Outs of Sulfadoxine-Pyrimethamine in Bungoma, Kenya” was presented by Augustine Ngindu, Gathari Ndirangu, Waqo Ejersa, David Omoit, and Mildred Mudany from Jhpiego’s Kenya Team at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
 WHO recommends intermittent preventive treatment of malaria in pregnancy using sulfadoxine pyrimethamine (IPTp-SP) to be provided at antenatal care (ANC) clinic. The Malaria Policy in Kenya requires that All pregnant women in malaria-endemic areas receive free intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine (IPTp-SP), have access to free malaria diagnosis and treatment when presenting with fever, and have access to long-lasting insecticidal nets.
WHO recommends intermittent preventive treatment of malaria in pregnancy using sulfadoxine pyrimethamine (IPTp-SP) to be provided at antenatal care (ANC) clinic. The Malaria Policy in Kenya requires that All pregnant women in malaria-endemic areas receive free intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine (IPTp-SP), have access to free malaria diagnosis and treatment when presenting with fever, and have access to long-lasting insecticidal nets.
Kenya’s Strategic Direction between 2014–2018 was revised to reflect the following:
- All pregnant women in the 14 malaria-endemic counties shall receive at least three doses of IPTp-SP
- Annual quantification of SP based on consumption to ensure adequate supplies
- Training, retraining and supervision of health care workers
- Dissemination of appropriate IPTp messages and materials
 Ministry of Health (MOH) used to procure SP until 2013 when health services were devolved to counties and procurement of became the responsibility of county governments. This presented a major challenge as counties had not factored SP in their budgets. Consequently, counties experienced SP stock-outs from October 2014. In Bungoma County the number of pregnant women receiving IPTp dropped by 51% from 7,845 in October 2014 to 3,865 in February 2015.
Ministry of Health (MOH) used to procure SP until 2013 when health services were devolved to counties and procurement of became the responsibility of county governments. This presented a major challenge as counties had not factored SP in their budgets. Consequently, counties experienced SP stock-outs from October 2014. In Bungoma County the number of pregnant women receiving IPTp dropped by 51% from 7,845 in October 2014 to 3,865 in February 2015.
To alleviate the situation (MOH) at national level requested counties to procure SP. Advocacy efforts with Bungoma County by the Maternal and Child Survival Program focused on prioritization of SP procurement at least once every quarter. As a result of this intervention, Bungoma County procured SP from February to July 2015.
 The county advised health facilities to procure additional SP doses if the supplied stocks ran out. The procurement led to a 117% increase in the number of pregnant women receiving IPTp; from 3,865 in February to 8,404 in July 2015.
The county advised health facilities to procure additional SP doses if the supplied stocks ran out. The procurement led to a 117% increase in the number of pregnant women receiving IPTp; from 3,865 in February to 8,404 in July 2015.
The fiscal year ended in June 2015 and no funds were available to procure additional SP until October 2015. This contributed to a 33% decrease in the number of pregnant women receiving IPTp from 8,404 in July to 5,672 in October 2015. As a response to support counties, MOH at national level procured 2.24 million SP doses in November/December for 14 MIP-focus counties which were received at health facilities in February 2016.
In conclusion, Bungoma County applied feasible mitigation measures including county level procurement of SP, supplemented by additional procurement at health facility and national levels. This is a practice which is replicable in other counties to ensure continued availability of SP to protect pregnant women from effects of malaria in pregnancy.
Integration &IPTp &Malaria in Pregnancy Bill Brieger | 15 Nov 2016
Joint efforts, a key to success for the Malaria in Pregnancy Program in Luanda, Angola
A poster entitled “Joint efforts, a key to success for the Malaria in Pregnancy Program in Luanda, Angola” was presented by Jhony Juarez, Adolfo Sampaio, William R. Brieger, and Domingos F. Gueve from Jhpiego’s Angola Team at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
 Angola, in response to WHO’s 2012 updated guidance on Intermittent Preventive Treatment in pregnancy (IPTp), revised its national malaria protocol to better address the fact that 25% of maternal mortality is caused by the disease. The new protocol was a collaborative effort of a national technical working group assisting the National Malaria Control Program (NMCP) including the National Reproductive Health Program, the national AIDS Institute, WHO, UNICEF, UNFPA and implementing partners of the U.S. Presidents Malaria Initiative (PMI).
Angola, in response to WHO’s 2012 updated guidance on Intermittent Preventive Treatment in pregnancy (IPTp), revised its national malaria protocol to better address the fact that 25% of maternal mortality is caused by the disease. The new protocol was a collaborative effort of a national technical working group assisting the National Malaria Control Program (NMCP) including the National Reproductive Health Program, the national AIDS Institute, WHO, UNICEF, UNFPA and implementing partners of the U.S. Presidents Malaria Initiative (PMI).
The updated Prevention and Treatment Manual for Malaria in Pregnancy, based on the revised protocol, was approved in 2014, and efforts continued with reviewing and updating training modules, job aids and monitoring tools that would reflect the additional doses of IPTp. The Ministry of Health, with support from partners, then disseminated these materials in the provinces and municipalities where they worked. USAID’s ForçaSaúde program, with support from PMI, worked with the Provincial Health Directorate of Luanda to build capacity of 297 health professionals to implement the new guidance in 78 health facilities of four municipalities, Belas, Cazenga, Cacuaco and Viana, with a combined population of 4.3 million.
 Comparing the IPTp data from the four municipalities between 2014 and 2015, one can see that the new guidance has started to take effect. In both years approximately 70,000 pregnant women received the first dose or around 60% of women registering for antenatal care (ANC). For the new third dose there was an increase of 85% (from 12,490 women to 23,046), and receipt of the fourth dose rose by 164% (3,345 to 8,839).
Comparing the IPTp data from the four municipalities between 2014 and 2015, one can see that the new guidance has started to take effect. In both years approximately 70,000 pregnant women received the first dose or around 60% of women registering for antenatal care (ANC). For the new third dose there was an increase of 85% (from 12,490 women to 23,046), and receipt of the fourth dose rose by 164% (3,345 to 8,839).
Two major challenges remain: increasing ANC registration and addressing missed opportunities to provide ANC doses for those who do attend including ensuring regular supplies of sulfadoxine-pyrimethamine for IPTp. Future progress requires continued inter-departmental collaboration among NMCP, Reproductive Health and the AIDs Institute, on-the-job training, enhanced statistical capacity, and supervision.
Community &IPTp &Malaria in Pregnancy Bill Brieger | 15 Nov 2016
Accelerating IPTp uptake through updated WHO IPTp guidance in Malawi
A poster entitled “Building Capacity to accelerate IPTp uptake through the adoption of 2012 WHO IPTp guidance in Malawi” was presented by John Munthali, Lolade Oseni, Dan Wendo, Kabango Malewezi, and Tambudzai Rashidi from Jhpiego’s Malawi Team at the

Community activities encourage IPTp uptake in Malawi
65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
Malawi adopted the World Health Organization’s updated guidance on intermittent preventive treatment in pregnancy (IPTp) in 2013. Support from the US President’s Malaria Initiative through USAID funded health projects, enabled collaboration between the National Malaria Control Program (NMCP) and the Reproductive Health Directorate (RHD) of the Ministry of Health, to build capacity from national to district to frontline health facility levels to implement the updated IPTp policy.
 These partners updated IPTp policy in the National Malaria Treatment Guidelines, and developed appropriate training manuals. All 5708 health workers from the 304 facilities in the 15 project districts were trained on the IPTp policy and guidelines. Post-training test scores of health staff increased over pre-test by an average of 40 percentage points.
These partners updated IPTp policy in the National Malaria Treatment Guidelines, and developed appropriate training manuals. All 5708 health workers from the 304 facilities in the 15 project districts were trained on the IPTp policy and guidelines. Post-training test scores of health staff increased over pre-test by an average of 40 percentage points.
The community action cycle approach engages community volunteers and local community based organizations to identify and solve local problems and was used to encourage pregnant women to attend antenatal care (ANC) and receive IPTp and long lasting insecticide-treated nets.
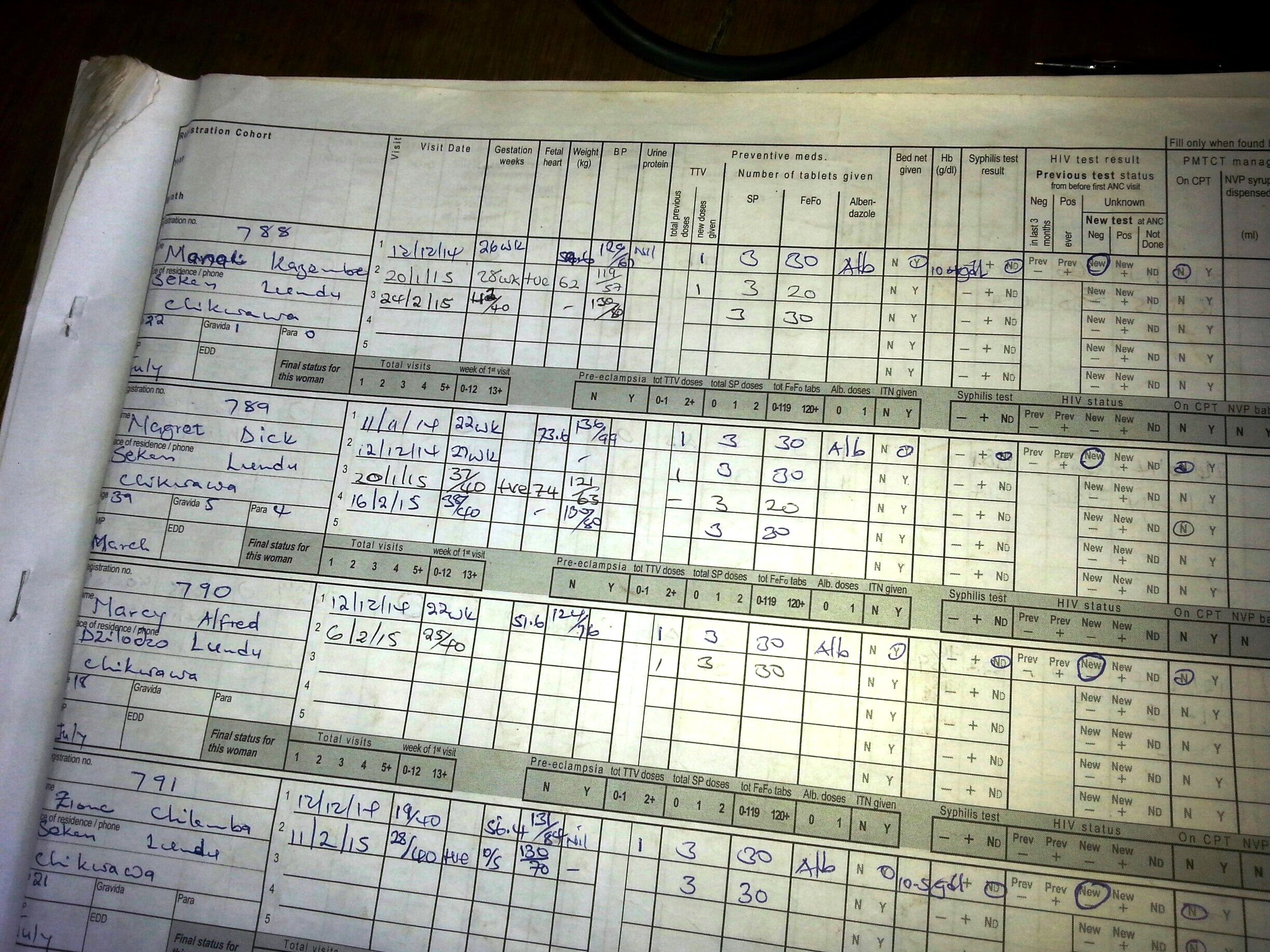
Sample page from ANC register showing delivery of IPTp3 and 4, but these data are not yet recorded on summary HMIS forms
Health information system data from the 15 Districts were used to compare ANC and IPTp coverage for 2012 and 2015 fiscal years (Oct.-Sept.). ANC registration in the project area rose from 113,683 to 394,116. IPTp1 as a proportion of ANC registration rose from 52% to 87%, and IPTp2 increased from 17% to 62%. While IPTp3 doses were recorded in the ANC registers, reporting forms in 2015 still did not include space to enter this IPTp3.
Observations at clinics showed IPTp3 and 4 were provided. Malawi’s experience shows that collaboration between NMCP and RHD as well as between clinics and communities not only disseminated knowledge of the new policy, but resulted in increased uptake of services and protection of pregnant women from malaria.
Diagnosis &Surveillance Bill Brieger | 14 Nov 2016
Towards Malaria Pre-Elimination in Rwanda: Active Case Investigation in a Low Endemic District
A poster entitled “Towards Malaria Pre-Elimination in Rwanda: Active Case Investigation in a Low Endemic District” was presented by members of Jhpiego’s Rwanda Team and colleagues:
Noella Umulisa, Angelique Mugirente, Veneranda Umubyeyi, Beata Mukarugwiro, Stephen Mutwiwa, Jean Pierre Habimana, and Corrine Karema, at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
 Rwanda has seen an increase in malaria cases recently with an increase from 514,173 cases in 2012 to 1,957,402 cases in 2015. This change can be attributed to an increase in temperature, rainfall, and resistance to insecticides.
Rwanda has seen an increase in malaria cases recently with an increase from 514,173 cases in 2012 to 1,957,402 cases in 2015. This change can be attributed to an increase in temperature, rainfall, and resistance to insecticides.
Despite this setback, Rwanda is aiming to reach the pre-elimination phase by 2018. In January 2015, 11 health facilities in Rubavu, a low endemic district, started implementing reactive active case detection after training 55 health care providers and 11 lab technicians on the topic. This strategy involves screening and treating individuals living in close proximity to passively detected cases, also known as index cases. Index cases can be used to identify population groups that are sources of infection.
 From January 2015 to December 2015, 16,434 cases of Malaria were detected and treated at 11 health facilities in Rubavu District. Among these cases, 2,917(17.8%) index cases were investigated and 4,943 individuals (between 1 and 2 contacts for each index case) living in proximity of index cases were tested using rapid diagnostic tests by health care providers. Of these, 508 (10.3%) tested positive for malaria and were treated according to national guidelines.
From January 2015 to December 2015, 16,434 cases of Malaria were detected and treated at 11 health facilities in Rubavu District. Among these cases, 2,917(17.8%) index cases were investigated and 4,943 individuals (between 1 and 2 contacts for each index case) living in proximity of index cases were tested using rapid diagnostic tests by health care providers. Of these, 508 (10.3%) tested positive for malaria and were treated according to national guidelines.
These data shows that the number of investigated cases is still lower than the national guidelines of screening 5 individuals residing between 100 to 500 meters of every confirmed case. This low rate could be due to the increase of malaria cases in Rwanda which has placed a burden on health care providers and health facilities in areas like Rubavu which used to be low endemic malaria areas. Additionally, data gathered through supervision activities has indicated a need for additional training on screening investigations in order to adhere to national guidelines and conduct the investigations more efficiently.
Active case investigation could be improved by training and involving more health care providers such as community health workers who could reduce the burden on health center staff. The additional support for case investigation activities and improved training can help to achieve higher coverage of individuals located near index cases.