Antenatal Care (ANC) &IPTp &Malaria in Pregnancy &Maternal Health &Surveys Bill Brieger | 16 Nov 2024
Using National Survey Data to Learn Impact of Intermittent Preventive Treatment of Malaria in Pregnancy on Birth weight in Nigeria
Bright C. Orji, Charity I. Anoke, William Robert Brieger presented a poster at ASTMH 2024 in New Orleans that analyzed the ability of national surveys to detect health program outcomes.
 Intermittent preventive treatment of malaria in pregnant women (IPTp) promotes health of the mother and unborn child. One noteworthy benefit is reduction of low birth weight (LBW, less than 2.5kg). Large survey data sets aid learning about such benefits on a national scale.
Intermittent preventive treatment of malaria in pregnant women (IPTp) promotes health of the mother and unborn child. One noteworthy benefit is reduction of low birth weight (LBW, less than 2.5kg). Large survey data sets aid learning about such benefits on a national scale.
 We analyzed data from the 2018 Nigeria Demographic and Health Survey (DHS) to document the impact of IPTp on birth weight. Key variables included IPTp which based on national guidelines is given monthly at antenatal clinics from the 13th week, aiming to provide a minimum of 3 doses. DHS obtained this information from women giving birth in the previous two years.
We analyzed data from the 2018 Nigeria Demographic and Health Survey (DHS) to document the impact of IPTp on birth weight. Key variables included IPTp which based on national guidelines is given monthly at antenatal clinics from the 13th week, aiming to provide a minimum of 3 doses. DHS obtained this information from women giving birth in the previous two years.
 Birth weight included women giving birth in the previous five years. A quarter had a record of newborn weight reported from a health facility.
Birth weight included women giving birth in the previous five years. A quarter had a record of newborn weight reported from a health facility.
Since many did not, women were also asked to estimate the size of the baby at birth: very small, smaller than average, average, larger than average, and very large. We combined the latter three categories into “average or larger”.
 Of those giving birth in the past 2 years, 23% took only one dose, 24% took 2 doses, while 17% had 3 or more doses. In the broader sample of those giving birth in the previous 5 years 2.8% estimated that their baby was very small.
Of those giving birth in the past 2 years, 23% took only one dose, 24% took 2 doses, while 17% had 3 or more doses. In the broader sample of those giving birth in the previous 5 years 2.8% estimated that their baby was very small.
Among those women with a record of birth weight, 7% were LBW. Preliminary analysis comparing perceived size and IPTp doses found 3% receiving only one dose thought their baby was “very small” at birth, as did 3% of those taking 2 doses and 4% receiving 3 or more.
Among the subset with a recorded birth weight, 9% who took only one dose of IPTp had LBW baby, as did 7% who received 2 doses, and 6% who got 3 or more doses. It appears possible to compare outcomes (LBW) with interventions (IPTp), but data type and availability may limit conclusions.
Even though a smaller subset of women had access to a recorded birth weight (most women delivered outside a health facility), birth weight appears to provide a better indication of IPTp effectiveness than subjective perceptions of child’s size at birth.
The findings even with limitations show the value of national surveys to justify policies protecting pregnant women from malaria.
Antenatal Care (ANC) &IPTp &Malaria in Pregnancy &Maternal Health Bill Brieger | 19 Oct 2023
Progress and Challenges for Intermittent Preventive Treatment of Malaria in Pregnancy: Nigeria
Bill Brieger and Bright Orji conducted an examination of national surveys and program reviews to document achievement of antenatal care and IPTp targets in Nigerian preparation for a poster presentation at the 2023 American Society of Tropical Medicine and Hygiene annual meeting in Chicago.
 In 2012, the World Health Organization updated the Intermittent Preventive Treatment of malaria during pregnancy (IPTp) coverage indicator to a minimum of three doses. In 2014, Nigeria set the national target of 100% of women attending ANC to receive IPTp.
In 2012, the World Health Organization updated the Intermittent Preventive Treatment of malaria during pregnancy (IPTp) coverage indicator to a minimum of three doses. In 2014, Nigeria set the national target of 100% of women attending ANC to receive IPTp.
This study reviewed national survey data for antenatal care (ANC) attendance and IPTp provision from the 2013 and 2018 Demographic Health Surveys (DHS) and the 2015 and 2021 Malaria Indicator Surveys (MIS). Extracted from the national malaria program reviews (MPR) of the National Malaria Strategic Plans (NMSP) of 2014 and 2019 were explanations of program implementation issues. ANC4 attendance and IPTp uptake (1st and 3rd doses) were compared using descriptive statistics.
 The 2015 MIS did not document ANC 4th visit, so attendance in the remaining surveys was 51%, 57%, and 52% (X2=160.0, df2, p <0.0001). The slow increase of ANC attendance and drop in 2021 meant that opportunity to acquire three IPTp doses was not possible for most women. Over the four surveys, IPT1 increased from 23% to 47% to 64%, then dropped to 58%. IPTp3 rose from 6% to 19% then dropped to 16.6% before increasing to 31% (X2= 1755, df3, p<0.0001).
The 2015 MIS did not document ANC 4th visit, so attendance in the remaining surveys was 51%, 57%, and 52% (X2=160.0, df2, p <0.0001). The slow increase of ANC attendance and drop in 2021 meant that opportunity to acquire three IPTp doses was not possible for most women. Over the four surveys, IPT1 increased from 23% to 47% to 64%, then dropped to 58%. IPTp3 rose from 6% to 19% then dropped to 16.6% before increasing to 31% (X2= 1755, df3, p<0.0001).
 The MPR reports identified four factors inhibiting achievement of the ANC and IPTp targets including insecurity (terrorism, civil unrest), poor integration of malaria in pregnancy into reproductive and maternal health programs, inadequate procurement and stock-outs of SP, and logistical hurdles (lack of vehicles and fuel). By not meeting ANC4 and IPTp1 targets, limits were set for IPTp3 uptake.
The MPR reports identified four factors inhibiting achievement of the ANC and IPTp targets including insecurity (terrorism, civil unrest), poor integration of malaria in pregnancy into reproductive and maternal health programs, inadequate procurement and stock-outs of SP, and logistical hurdles (lack of vehicles and fuel). By not meeting ANC4 and IPTp1 targets, limits were set for IPTp3 uptake.
As other researchers have suggested, NMSPs embody global targets and may not reflect local realities. Local governments, who deliver the bulk of ANC and IPTp services, must be part of the process of setting and planning how to achieve targets.
IPTp &Malaria in Pregnancy &Resistance Bill Brieger | 02 Mar 2023
Are we prepared to protect pregnant women from malaria as SP resistance spreads
Adegbola and colleagues note that “the efficacy of SP-IPTp is threatened by the emergence of sulfadoxine-pyrimethamine resistant malaria parasites, “which has been observed in East Africa. They therefore, studied the situation in Nigeria, the country with the highest malaria burden in the continent. Their study showed that “the prevalence of VAGKGS haplotype seems to be increasing in prevalence.”
In conclusion, they worried that, “If this is similar in effect to the emergence of 581G in East Africa, the efficacy of SP-IPTp in the presence of these novel Pfdhps mutants should be re-assessed” in Nigeria. This situation threatens the use of sulfadoxine-pyrimethamine (SP) in two major prevention programs including intermittent preventive treatment during pregnancy (IPTp) and seasonal malaria chemoprevention (SMC) for children.
The benefits of IPTp using SP is the ability to administer chemoprevention in a single directly observed dose. Alternative medications are being explored, but from the behavioral intervention perspective, the low cost and simplicity afforded by SP is ideal.
 The IPTp strategy had been modified a decade ago from requiring 2 doses, to monthly doses from the second trimester onwards because of parasite resistance or what is also termed drug tolerance by the parasite. Tolerance implies that the drug may still work, but at higher or more frequent doses. Such changes have cost and behavior change implications. Many country reports from the Malaria Indicator Surveys show an expected drop-off in uptake of SP between the first and third doses. For example in the 2021 Nigeria MIS IPTp1 uptake was 58%, while IPTp3 had reduced to 31%.
The IPTp strategy had been modified a decade ago from requiring 2 doses, to monthly doses from the second trimester onwards because of parasite resistance or what is also termed drug tolerance by the parasite. Tolerance implies that the drug may still work, but at higher or more frequent doses. Such changes have cost and behavior change implications. Many country reports from the Malaria Indicator Surveys show an expected drop-off in uptake of SP between the first and third doses. For example in the 2021 Nigeria MIS IPTp1 uptake was 58%, while IPTp3 had reduced to 31%.
A related problem in Nigeria is the ubiquitous availability of SP in medicine shops across the country in contrast to official policy limiting it to use in IPTp and SMC. The challenge is finding affordable and feasible alternative medicines for IPTp. In the meantime, we have not even reached coverage targets using SP nor fully achieved rollout of companion interventions such as the use of Insecticide Treated Nets. Much work is still needed to protect pregnant women and fetuses from the malaria induced problems of anemia, low-birth-weight, stillbirth, and more.
A related study from Cameroon: The occurrence of sub-microscopic P. falciparum parasites resistant to SP and intense malaria transmission poses persistent risk of malaria infection during pregnancy in the area. ITN usage and monitoring spread of resistance are critical.
https://malariajournal.biomedcentral.com/articles/10.1186/s12936-023-04485-7
CHW &Integration &IPTi &IPTp &Malaria in Pregnancy &Maternal Health &Seasonal Malaria Chemoprevention Bill Brieger | 12 Dec 2022
Malaria Chemoprevention in 2021 as Seen in The World Malaria Report of 2022
 Dr Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization, reminds us in this year’s edition of the World Malaria Report (WMR 2022) that, “Although hard hit, most countries held the line and were able to maintain services to prevent, detect and treat malaria – a remarkable feat in the midst of a pandemic. Nonetheless, more than 600 000 people still die of malaria every year – most of them children. Even with the heroic efforts to maintain services during the pandemic, malaria control efforts face many hurdles in addition to the already significant COVID-related disruptions and other health system challenges.”
Dr Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization, reminds us in this year’s edition of the World Malaria Report (WMR 2022) that, “Although hard hit, most countries held the line and were able to maintain services to prevent, detect and treat malaria – a remarkable feat in the midst of a pandemic. Nonetheless, more than 600 000 people still die of malaria every year – most of them children. Even with the heroic efforts to maintain services during the pandemic, malaria control efforts face many hurdles in addition to the already significant COVID-related disruptions and other health system challenges.”
Even though there was an increase in cases between 2020 and 2021, there are now more strategies in the malaria control and elimination toolkit than ever before. One in particular is an updated take on an old concept of chemoprophylaxis, which fell out of use due to mounting drug resistance. Years of research with pregnant women and young children led to the development over time of using regularly scheduled treatment doses of malaria medicines as chemoprevention. Intermittent Preventive Treatment for pregnant women (IPTp) and Seasonal Malaria Chemoprevention for young children, both targeted to appropriate epidemiological settings, are now common. Countries are also exploring IPT for children in other settings.
 We were, therefore, curious what the current WMR shares on chemoprevention initiatives. Specifically, the WMR summarized WHO recommendations as follows: “Updated guidelines provide recommendations on intermittent preventive treatment of malaria in pregnancy (IPTp), perennial malaria chemoprevention (PMC) and seasonal malaria chemoprevention (SMC), intermittent preventive treatment of malaria in school-aged children (IPTsc), post-discharge malaria chemoprevention (PDMC), mass drug administration (MDA) and elimination.”
We were, therefore, curious what the current WMR shares on chemoprevention initiatives. Specifically, the WMR summarized WHO recommendations as follows: “Updated guidelines provide recommendations on intermittent preventive treatment of malaria in pregnancy (IPTp), perennial malaria chemoprevention (PMC) and seasonal malaria chemoprevention (SMC), intermittent preventive treatment of malaria in school-aged children (IPTsc), post-discharge malaria chemoprevention (PDMC), mass drug administration (MDA) and elimination.”
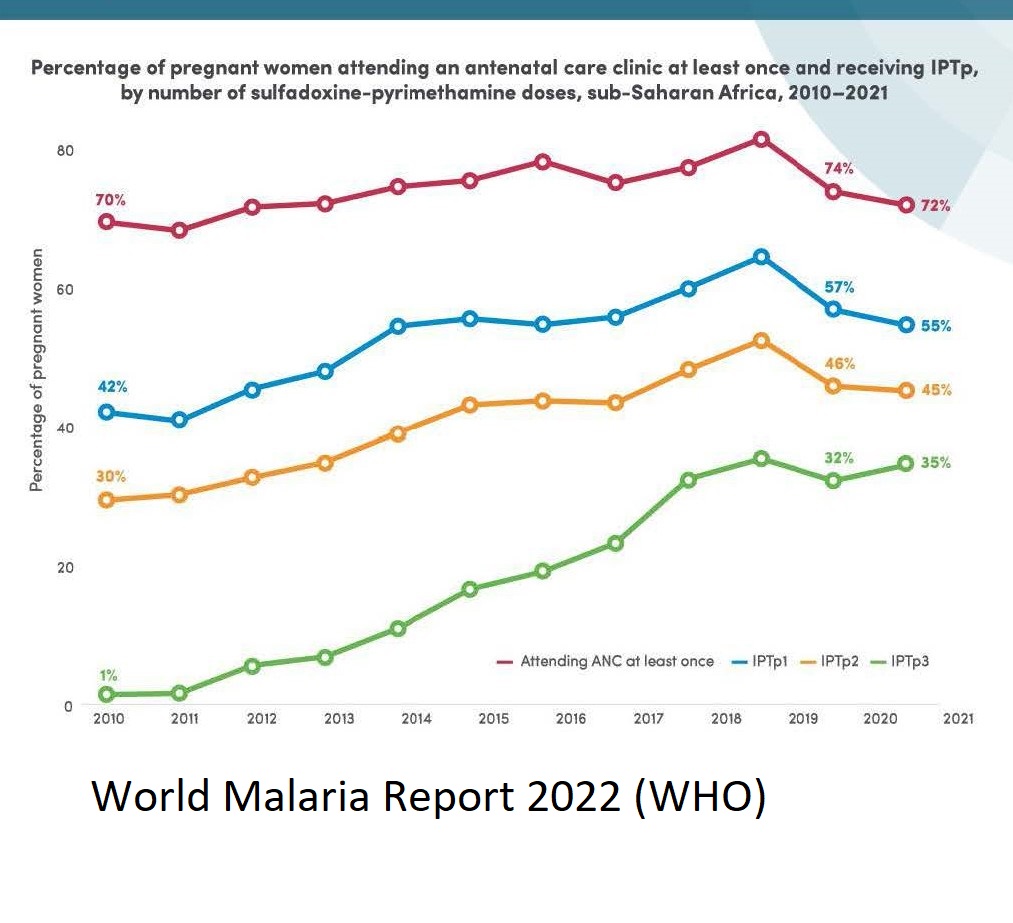
In summary, WMR 2022 notes that, “The average number of children treated per cycle of SMC increased from about 0.2 million in 2012 to almost 45 million in 2021,” and “Using data from 33 countries in the WHO African Region, the percentage of IPTp use by dose was computed. In 2021, 72% of pregnant women used ANC services at least once during their pregnancy. About 55% of pregnant women received one dose of IPTp, 45% received two doses and 35% received three doses.” This is not just progress over time, but also represents an expansion targets and work required for success. For pregnant women the increase represented a change in target from only two doses during pregnancy to a minimum of three. Starting with pilot efforts, SMC now covers children in 15 countries.
 The targeted three doses for IPTp shows that two thirds of women who register for antenatal (prenatal) care (ANC), fail to achieve full coverage. Stronger collaboration is needed between malaria control and maternal health programs to ensure that pregnant women actually attend ANC and do so early and often enough to receive 3 monthly doses minimum in their second and third trimesters. More emphasis is needed on community IPTp distribution, since we know that community health workers have been crucial in achieving SMC as well as integrated community case management efforts.
The targeted three doses for IPTp shows that two thirds of women who register for antenatal (prenatal) care (ANC), fail to achieve full coverage. Stronger collaboration is needed between malaria control and maternal health programs to ensure that pregnant women actually attend ANC and do so early and often enough to receive 3 monthly doses minimum in their second and third trimesters. More emphasis is needed on community IPTp distribution, since we know that community health workers have been crucial in achieving SMC as well as integrated community case management efforts.
Similar challenges exist for SMC as research looks into whether additional doses are needed based on mosquito breeding and malaria transmission season factors in endemic countries. Adding extra months to the program will tax resources, but also save lives.
Both maternal and child efforts at chemoprevention will need to address research that first shows increasing resistance to the common medicines used, and the potential for introducing new drug combinations in light of that resistance. Challenges here reflect another aspect of SMC, the need for CHWs to guarantee that on any given distribution round, three doses on medicine are required. Recent reports show that within any given round, community adherence to SMC has been good. We need to apply those lessons to IPTp when the regimen changes.
Ultimately, chemoprevention has proven to be an important life saving tool. The challenges of multiple contacts and doses that lead to success rely not only on having effective medicines, but also on culturally appropriate behavior change strategies and well-funded efforts to strengthen the health systems that deliver preventive treatments.
Antenatal Care (ANC) &IPTp Bill Brieger | 31 Oct 2022
Comparative analysis of facility and community distribution of intermittent preventive treatment of malaria in pregnancy
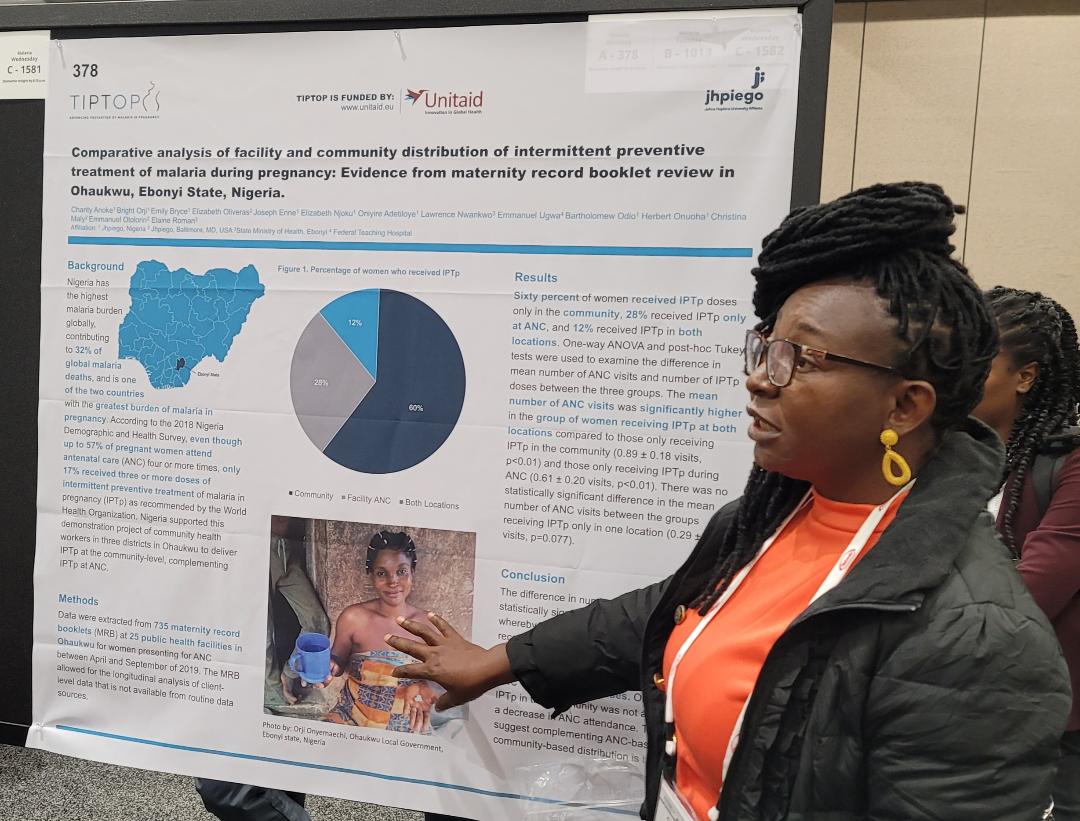 Charity Anoke, Bright Orji, Emily Bryce, Elizabeth Oliveras, Joseph Enne, Elizabeth Njoku, Lawrence Nwankwo, Emmanuel Ugwa, Bartholomew Odio, Herbert Onuoha, Christina Maly, Emmanuel Otolorin, Elaine Roman, and Oniyire Adetiloye are presenting a poster for the TiPToP project at the American Society of Tropical Medicine and Hygiene’s Annual Meeting in Seattle. Below is the evidence from maternity record booklets in Ohaukwu, Ebonyi State Nigeria.
Charity Anoke, Bright Orji, Emily Bryce, Elizabeth Oliveras, Joseph Enne, Elizabeth Njoku, Lawrence Nwankwo, Emmanuel Ugwa, Bartholomew Odio, Herbert Onuoha, Christina Maly, Emmanuel Otolorin, Elaine Roman, and Oniyire Adetiloye are presenting a poster for the TiPToP project at the American Society of Tropical Medicine and Hygiene’s Annual Meeting in Seattle. Below is the evidence from maternity record booklets in Ohaukwu, Ebonyi State Nigeria.
Nigeria has the highest malaria burden globally, contributing to 31.9% of global malaria deaths, and is one of the two countries with the greatest burden of malaria during pregnancy. According to the 2018 Nigeria Demographic and Health Survey (DHS), even though up to 57% of pregnant women attend ANC four or more times, only 17% received three or more doses of IPTp as recommended by the WHO.
 Nigeria supported this demonstration project of CHWs in delivering intermittent preventive treatment of malaria in pregnancy (IPTp) at the community-level, complementing IPTp at antenatal care (ANC) in three districts. Data were extracted from 735 maternity record booklets (MRB) at 25 public health facilities in Ohaukwu for women presenting for ANC between April and September of 2019. The MRB allowed for the longitudinal analysis of client-level data that is not available from routine data sources.
Nigeria supported this demonstration project of CHWs in delivering intermittent preventive treatment of malaria in pregnancy (IPTp) at the community-level, complementing IPTp at antenatal care (ANC) in three districts. Data were extracted from 735 maternity record booklets (MRB) at 25 public health facilities in Ohaukwu for women presenting for ANC between April and September of 2019. The MRB allowed for the longitudinal analysis of client-level data that is not available from routine data sources.
Sixty percent of women received IPTp doses only in the community, while 28% received IPTp only at ANC and 12% received IPTp in both locations. One-way ANOVA and post-hoc Tukey tests were used to examine the difference in mean number of ANC visits and number of IPTp doses between the three groups. The mean number of ANC visits was significantly higher in the group of women receiving IPTp at both locations compared to those only receiving IPTp in the community (0.89 ± 0.18 visits, p<0.01) and those only receiving IPTp during ANC (0.61 ± 0.20 visits, p<0.01).
 There was no statistically significant difference in the mean number of ANC visits between the groups receiving IPTp only in one location (0.29 ± 0.13 visits, p=0.077). The difference in number of doses was statistically significant across all groups, whereby women in the facility-only group received the fewest IPTp doses. Receipt of IPTp in both locations was associated with both greater numbers of ANC visits and IPTp doses. Only receiving IPTp in the community was not associated with a decrease in ANC attendance.
There was no statistically significant difference in the mean number of ANC visits between the groups receiving IPTp only in one location (0.29 ± 0.13 visits, p=0.077). The difference in number of doses was statistically significant across all groups, whereby women in the facility-only group received the fewest IPTp doses. Receipt of IPTp in both locations was associated with both greater numbers of ANC visits and IPTp doses. Only receiving IPTp in the community was not associated with a decrease in ANC attendance.
These data suggest complementing ANC-based IPTp distribution with community-based distribution is beneficial.
Children &COVID-19 &Diagnosis &IPTp &ITNs &Malaria in Pregnancy &Treatment Bill Brieger | 06 Oct 2022
2021 DHS and MIS Findings from Six Malaria Endemic Countries
The Demographic and Health Survey Program has released final and summary reports for both DHS and Malaria Indicator Surveys (MIS) for 2021 from several malaria endemic African countries. Below is a brief summary of some of the findings from Madagascar, Nigeria, Burkina Faso, Mali, Côte d’Ivoire, and Senegal. Click the link on each country to download a copy for yourself.
The proportion of the population who slept under an insecticide treated bednet the night before the survey varied. In Madagascar it was 49%, While in Nigeria it was 59%. Mali achieved the highest coverage at 73%, while Burkina Faso had the lowest previous night coverage at 41%.
 Senegal showed a worrying decrease from 63% in 2016 to 46% in 2021. Côte d’Ivoire did not report total household use, but indicated that 72% of homes had at least one net, with 58% of children below 5 years of age and 64% of pregnant women sleeping under them.
Senegal showed a worrying decrease from 63% in 2016 to 46% in 2021. Côte d’Ivoire did not report total household use, but indicated that 72% of homes had at least one net, with 58% of children below 5 years of age and 64% of pregnant women sleeping under them.
At least three doses of sulfadoxine-pyremethamine is recommended for Intermittent preventive treatment of malaria in pregnant women. The national average was 38% for at least 3 doses in Senegal, although ironically 92% had been reached with the first dose. In Mali only 35% received at least a third dose. Burkina Faso started out with 92% for the first dose, but reached 57% with three or more. Côte d’Ivoire started with 80% receiving their first dose and concluded with only 35% receiving a third. Both Madagascar and Nigeria had the lowest 3-dose coverage at 31%.
Malaria testing and treatment using rapid diagnostic tests and artemisinin-based combination therapy (ACT) was reported. Nigeria demonstrates the challenges of following guidelines. Although 63% of children under 5 years of age were reported to have had a fever in the two weeks preceding the survey, only 24% of those received a diagnostic test. The summary results report that 74% of those with fever “who took any anti-malaria medicine” used the recommended ACT. The implication is that many received medicine without confirmatory testing such that some may have gotten ACT who needed another medicine and some who actually had malaria may have missed the correct treatment.
 A similar low level of testing was seen in Senegal (22%), Mali (23%), and Madagascar (20%). Côte d’Ivoire reported 38% of febrile children having been tested. Burkina Faso performed better for testing with 65%.
A similar low level of testing was seen in Senegal (22%), Mali (23%), and Madagascar (20%). Côte d’Ivoire reported 38% of febrile children having been tested. Burkina Faso performed better for testing with 65%.
These brief findings indicate that implementation of Malaria interventions are far from ideal. We know that some of the blame can be placed on health service disruptions due to demands of COVID-19 activities by health ministries and partners. Still, with 8 years remaining until 2030, Reinvigorated efforts are needed in all endemic countries if these six examples are indicative of the challenges we face.
Antenatal Care (ANC) &CHW &IPTp Bill Brieger | 19 Nov 2021
Changes in ANC Attendance and IPTp Uptake after Introduction of Complimentary Community Interventions
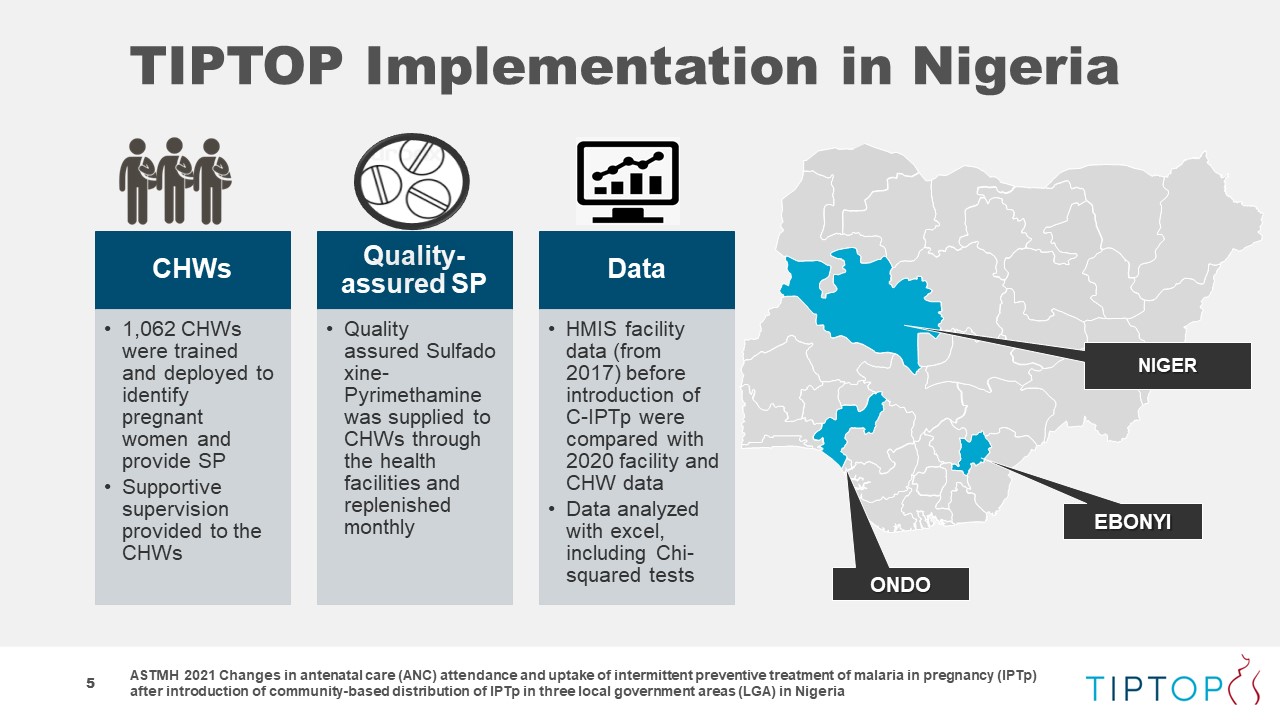 The TiPToP malaria in pregnancy project of Jhpiego and Unitaid has been aiming to increase coverage of Intermittent Preventive Treatment of malaria in pregnancy. The abstract below shares experiences from Nigeria, one of 4 TiPToP countries, is being presented at the 2021 American Society of Tropical Medicine and Hygiene Annual Meeting. Described are Changes in antenatal care (ANC) attendance and uptake of intermittent preventive treatment of malaria in pregnancy (IPTp) after introduction of community-based distribution of IPTp in three local government areas (LGA) in Nigeria. See Author List below.
The TiPToP malaria in pregnancy project of Jhpiego and Unitaid has been aiming to increase coverage of Intermittent Preventive Treatment of malaria in pregnancy. The abstract below shares experiences from Nigeria, one of 4 TiPToP countries, is being presented at the 2021 American Society of Tropical Medicine and Hygiene Annual Meeting. Described are Changes in antenatal care (ANC) attendance and uptake of intermittent preventive treatment of malaria in pregnancy (IPTp) after introduction of community-based distribution of IPTp in three local government areas (LGA) in Nigeria. See Author List below.
 In Nigeria, community health workers (CHWs) from three LGAs were engaged to introduce community delivery of IPTp (C-IPTp) with quality-assured sulfadoxine-pyrimethamine to prevent malaria. This approach, which complements IPTp delivery during ANC visits, was carried out in Ohaukwu, Akure South, and Bosso LGAs. C-IPTp was introduced in September 2018 in Ohaukwu and in December 2019 in Akure South and Bosso.
In Nigeria, community health workers (CHWs) from three LGAs were engaged to introduce community delivery of IPTp (C-IPTp) with quality-assured sulfadoxine-pyrimethamine to prevent malaria. This approach, which complements IPTp delivery during ANC visits, was carried out in Ohaukwu, Akure South, and Bosso LGAs. C-IPTp was introduced in September 2018 in Ohaukwu and in December 2019 in Akure South and Bosso.
A total of 1,062 CHWs were trained on early identification of pregnant women, referral to ANC, IPTp administration, and use of mobile phones to capture and report data. CHWs conduct household visits, provide malaria health education, refer and encourage pregnant women to attend ANC, and provide IPTp.
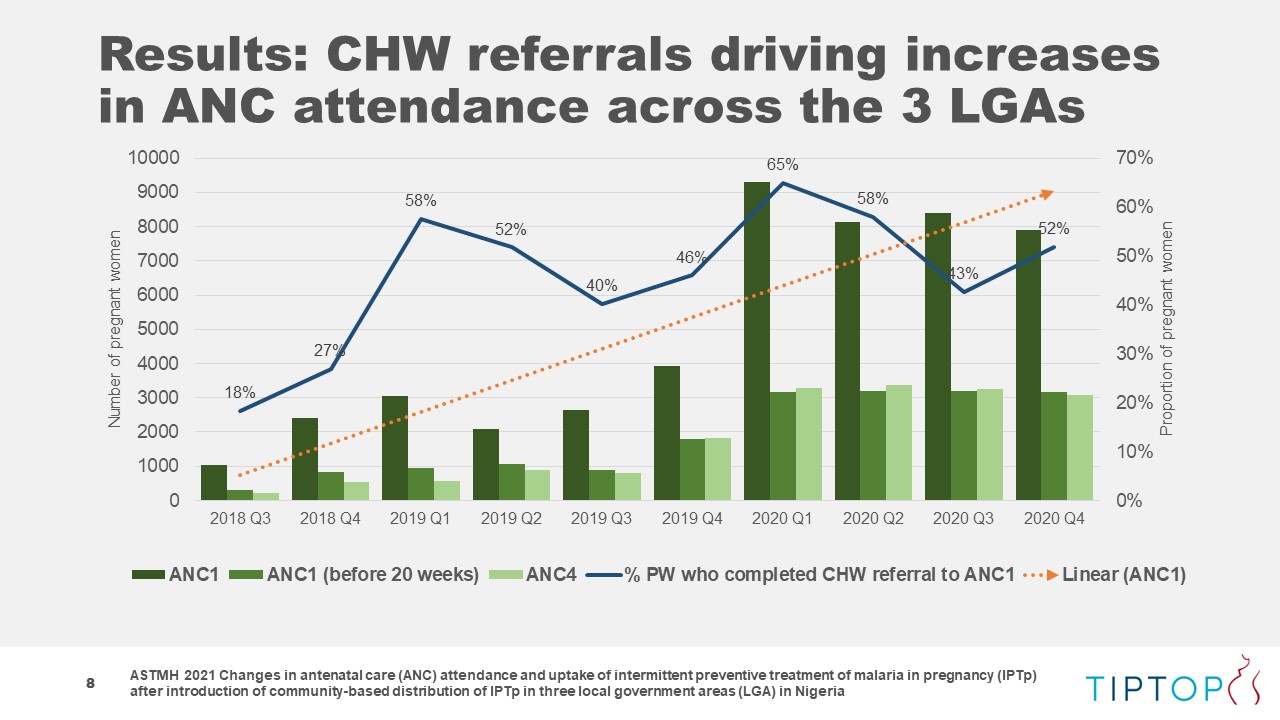
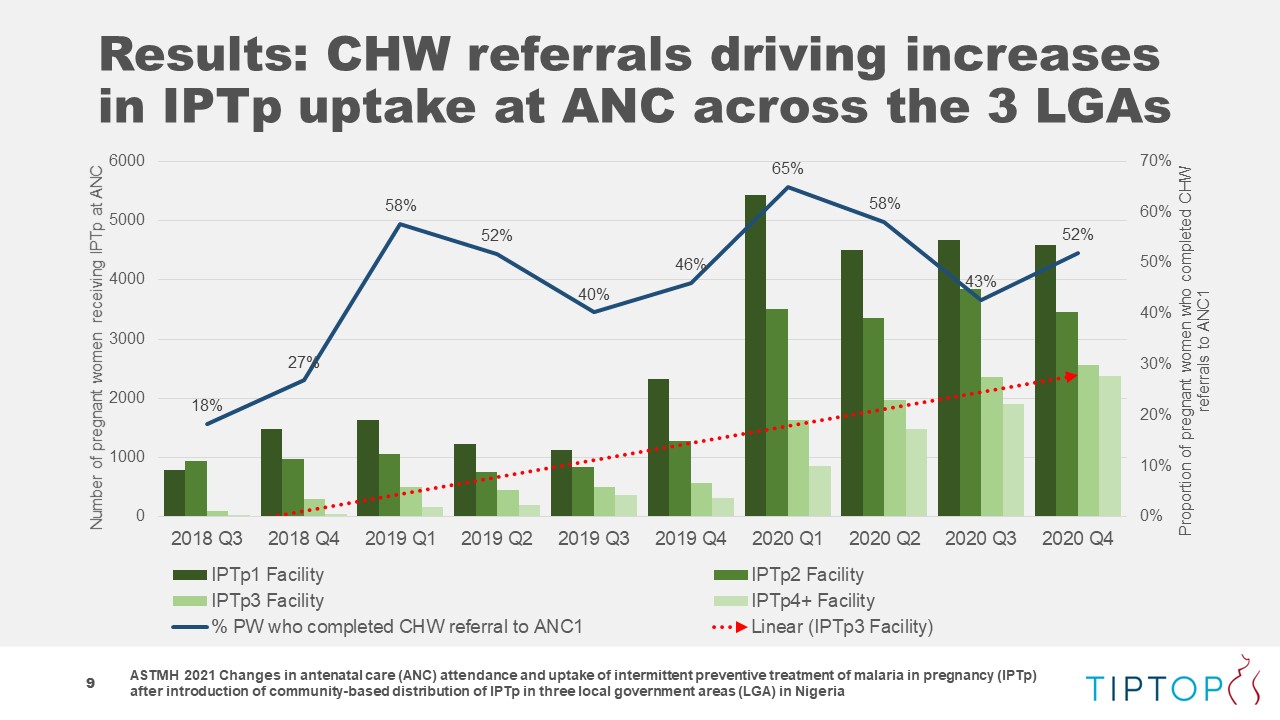 Routine facility data from 2017 before introduction of C-IPTp were compared with 2020 facility and CHW data to understand the effect of C-IPTp across the LGAs. Before C-IPTp, 43% of the estimated number of pregnant women in these areas attended at least one ANC visit as compared to 57% in 2020 (p<.05).
Routine facility data from 2017 before introduction of C-IPTp were compared with 2020 facility and CHW data to understand the effect of C-IPTp across the LGAs. Before C-IPTp, 43% of the estimated number of pregnant women in these areas attended at least one ANC visit as compared to 57% in 2020 (p<.05).
 Attending at least four ANC (ANC4) visits increased in Ohaukwu by ten percentage points to 29% in 2020 (p<.05). In Akure South, ANC4 remained steady Bosso pre-C-IPTp data on ANC4 visits were of too poor quality to conduct a meaningful analysis. Though this project focused on C-IPTp, it also resulted in statistically significant increases in IPTp distribution during ANC visits.
Attending at least four ANC (ANC4) visits increased in Ohaukwu by ten percentage points to 29% in 2020 (p<.05). In Akure South, ANC4 remained steady Bosso pre-C-IPTp data on ANC4 visits were of too poor quality to conduct a meaningful analysis. Though this project focused on C-IPTp, it also resulted in statistically significant increases in IPTp distribution during ANC visits.
From 2017 to 2020, coverage of IPTp doses 1, 2, and 3 all saw increases across the three sites: IPTp1 increased from 54%?to 57%; IPTp2 from 36% to 42%; and IPTp3 increased 20 percentage points from 5% to 25%. Of pregnant women receiving all doses of IPTp, 39% did so through ANC with 61% receiving IPTp from CHWs.
 These data suggest that in addition to contributing to overall increases in IPTp coverage, C-IPTp may also contribute to increases IPTp delivery in ANC and ANC attendance.
These data suggest that in addition to contributing to overall increases in IPTp coverage, C-IPTp may also contribute to increases IPTp delivery in ANC and ANC attendance.
AUTHORS LIST:
Herbert Enyeribe Onuoha1, Bartholomew Odio1, Christina Maly2, Lawrence Nwankwo3, Folayan Waheed Adewale4, Elizabeth Njoku1, Oniyire Adetiloye1, Orji Bright1, Emmanuel Dipo Otolorin1, Elaine Roman2 — 1Jhpiego, Abakaliki, Nigeria, 2Jhpiego, Baltimore, MD, United States, 3Ebonyi State Ministry of Health, Abakaliki, Nigeria, 4Ondo State Ministry of Health, Alagbaka, Akure, Nigeria
Antenatal Care (ANC) &Communication &Community &COVID-19 &IPTp &Malaria in Pregnancy &mHealth Bill Brieger | 18 Nov 2021
SMS to support health worker knowledge retention of maternal health and malaria interventions
The TiPToP malaria in pregnancy project of Jhpiego and Unitaid has been adjusting to the COVID-19 pandemic. Their abstract below is being presented at the 2021 American Society of Tropical Medicine and Hygiene Annual Meeting and explains the use of bulk SMS to support health worker knowledge retention on antenatal care and the use of intermittent preventive treatment of malaria in pregnancy during COVID-19 in Bosso local government area of Niger State, Nigeria. See Author List below.
 In light of COVID-19 travel restrictions, bulk SMS were used to support knowledge retention of health workers following an in-person training held before the pandemic. In December 2019, 72 facility health workers and 260 community health workers (CHWs) in Bosso local government area of Niger State, Nigeria participated in a 12-day training about benefits of early antenatal care (ANC) attendance, CHW referrals to ANC, and use of intermittent preventive treatment in pregnancy (IPTp) with sulphadoxine-pyrimethamine to prevent malaria.
In light of COVID-19 travel restrictions, bulk SMS were used to support knowledge retention of health workers following an in-person training held before the pandemic. In December 2019, 72 facility health workers and 260 community health workers (CHWs) in Bosso local government area of Niger State, Nigeria participated in a 12-day training about benefits of early antenatal care (ANC) attendance, CHW referrals to ANC, and use of intermittent preventive treatment in pregnancy (IPTp) with sulphadoxine-pyrimethamine to prevent malaria.
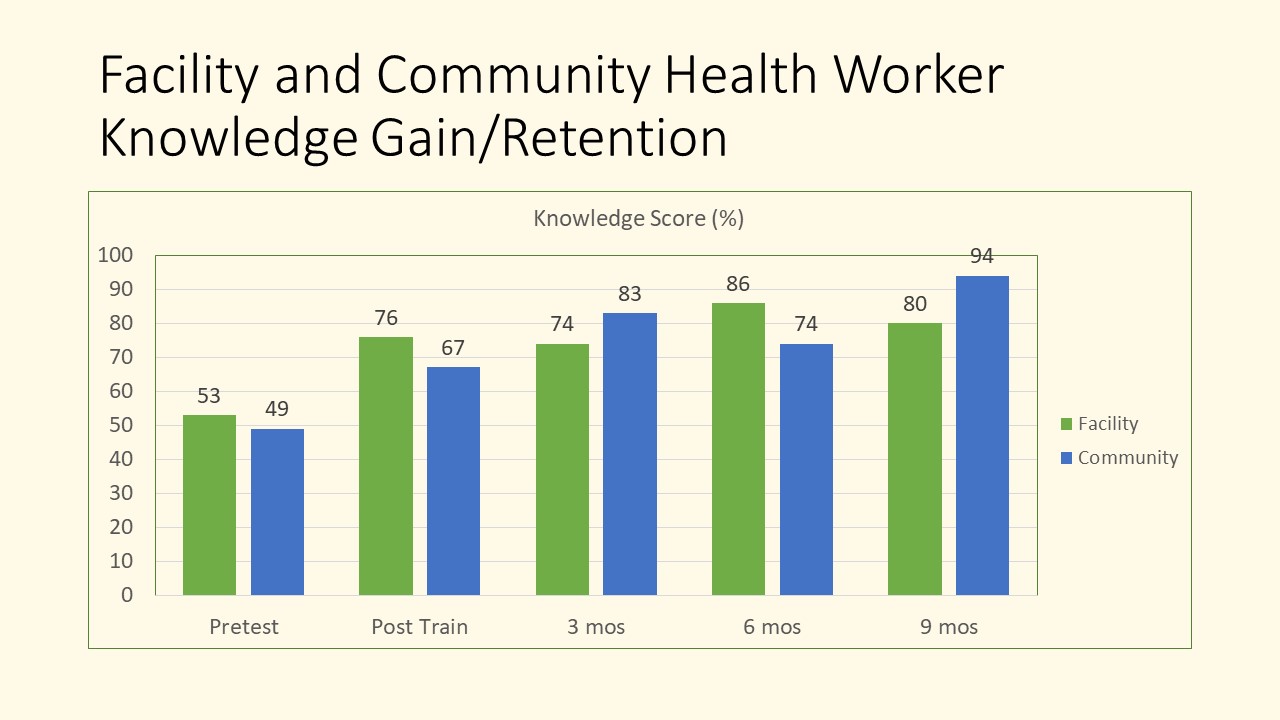 In-person supervision visits were conducted 3 months following training, although three months later in-person supervision was no longer possible due to COVID-19 related travel restrictions. Post-training support transitioned to use of bulk SMS which were sent twice a week to each cadre for two 3-month rounds of messaging.
In-person supervision visits were conducted 3 months following training, although three months later in-person supervision was no longer possible due to COVID-19 related travel restrictions. Post-training support transitioned to use of bulk SMS which were sent twice a week to each cadre for two 3-month rounds of messaging.
Knowledge tests comprised of 10 multiple choice questions linked to key ANC and IPTp guidelines were administered at 5 time points: 1) baseline; 2) post-training; 3) at in-person supervision visit 3 months after training; 4) after first round of bulk SMS (6 months post-training); and 5) after second round of bulk SMS (9 months post-training).
Average test scores for each cadre were calculated at each time point and T-tests were used to assess differences in scores. The results show that facility health workers scored an average of 53% on the pre-test followed by scores of 76%, 74%, 86%, and ending at 80% 9 months following training. CHWs started with an average score of 49% which increased to 67% post-training; subsequent average scores were 83%, 74%, and 94%.
Results were compelling with facility health worker knowledge improving from 76% immediately post-training to 80% 9 months later (p-value<0.05) and for CHWs the improvement was from 67% to 94% (p-value<0.05). These findings suggest that use of SMS can support knowledge retention of key ANC and IPTp guidelines following an in-person training. Program managers, trainers and supervisors may consider using this approach to support health workers where resources and/or movement are restricted.
AUTHOR INFORMATION:
Charity Anoke 1, Orji Bright 1, Joseph Enne 1, Bartholomew Odio 1, Christina Maly 2, Amina Zimro 3, Ibrahim Idris 3, Elizabeth Njoku 1, Oniyire Adetiloye 1, Emmanuel Dipo Otolorin 1, Elaine Roman 2 — 1Jhpiego, Abuja, Nigeria, 2Jhpiego, Baltimore, MD, United States, 3Niger State Ministry of Health, Minna, Nigeria
Community &Diagnosis &Guidelines &Health Workers &IPTp &Malaria in Pregnancy &Monitoring &Treatment Bill Brieger | 02 Nov 2021
Updating Malaria Guidelines and Tools: The Kenya Example
 Kenya Division of National Malaria Program (DNMP) with support from PMI Impact Malaria (IM) and in collaboration with other stakeholders reviewed/developed/updated nine key program documents. Agustine Ngindu and the Impact Malaria/PMI team stress the importance of keeping key malaria technical guidance and tools up-to-date.
Kenya Division of National Malaria Program (DNMP) with support from PMI Impact Malaria (IM) and in collaboration with other stakeholders reviewed/developed/updated nine key program documents. Agustine Ngindu and the Impact Malaria/PMI team stress the importance of keeping key malaria technical guidance and tools up-to-date.
 Guidelines for the Diagnosis, Treatment, and Prevention of Malaria in Kenya was revised to indicate the start of IPTp at 13 weeks from the prior recommendation of 16 weeks of gestation and updated the IPTp schedule in line with WHO guidance. The program also updated dosing charts for artemether lumefantrine, dihydroartemisinin-piperaquine, and injectable artesunate to include both weight and age range particulars. This update will enhance adherence to treatment guidelines among healthcare workers
Guidelines for the Diagnosis, Treatment, and Prevention of Malaria in Kenya was revised to indicate the start of IPTp at 13 weeks from the prior recommendation of 16 weeks of gestation and updated the IPTp schedule in line with WHO guidance. The program also updated dosing charts for artemether lumefantrine, dihydroartemisinin-piperaquine, and injectable artesunate to include both weight and age range particulars. This update will enhance adherence to treatment guidelines among healthcare workers
 The Kenya Quality Assurance Guidelines for Parasitological Diagnosis of Malaria was in draft form for nearly 10 years. Revisions were motivated by the lack of a functional quality assurance (QA)/quality control (QC) system for malaria diagnosis. Sections were added to guide implementation of internal quality control and external quality assurance programs. Updates also provided guidance on surveys to determine the extent of gene deletion and its effect on routine RDT-based malaria diagnosis.
The Kenya Quality Assurance Guidelines for Parasitological Diagnosis of Malaria was in draft form for nearly 10 years. Revisions were motivated by the lack of a functional quality assurance (QA)/quality control (QC) system for malaria diagnosis. Sections were added to guide implementation of internal quality control and external quality assurance programs. Updates also provided guidance on surveys to determine the extent of gene deletion and its effect on routine RDT-based malaria diagnosis.
 Implementation Framework for Malaria Rapid Diagnostic Tests was developed to facilitate rollout of malaria diagnostics QA/QC in line with Kenya Malaria Strategy (KMS) of 2019-2023. As p[art of this effort, the M&E framework was expanded to include the performance matrix. A costed implementation matrix to provide guidance was developed on costing of activities in line with KMS 2019-2023.
Implementation Framework for Malaria Rapid Diagnostic Tests was developed to facilitate rollout of malaria diagnostics QA/QC in line with Kenya Malaria Strategy (KMS) of 2019-2023. As p[art of this effort, the M&E framework was expanded to include the performance matrix. A costed implementation matrix to provide guidance was developed on costing of activities in line with KMS 2019-2023.
 Biosafety Guidelines for Malaria Rapid Diagnostic Testing at Community Level was highlighted in new guidelines developed to address emerging QA and biosafety concerns at community level. This was a response to requirements by the Kenya Medical Laboratory Technicians and Technologists Board to allow for a new waiver for community health volunteers (CHVs) to conduct testing using mRDTs.
Biosafety Guidelines for Malaria Rapid Diagnostic Testing at Community Level was highlighted in new guidelines developed to address emerging QA and biosafety concerns at community level. This was a response to requirements by the Kenya Medical Laboratory Technicians and Technologists Board to allow for a new waiver for community health volunteers (CHVs) to conduct testing using mRDTs.
 The Guidelines on Community Case Management of malaria and its implementation plan were strengthened as was the Implementation framework for Rapid Diagnostic Testing. Updated job aids included dosing schedules for artemether lumefantrine (AL) and injectable artesunate for use at service delivery points by Health Care Workers in line with the revised guidelines.
The Guidelines on Community Case Management of malaria and its implementation plan were strengthened as was the Implementation framework for Rapid Diagnostic Testing. Updated job aids included dosing schedules for artemether lumefantrine (AL) and injectable artesunate for use at service delivery points by Health Care Workers in line with the revised guidelines.
 Hopefully all national malaria programs will take the Kenya experience as an example of the need to update regularly all the tools needed for front line staff to achieve malaria elimination.
Hopefully all national malaria programs will take the Kenya experience as an example of the need to update regularly all the tools needed for front line staff to achieve malaria elimination.
Capacity Building &CHW &Community &Elimination &Health Education &Indoor Residual Spraying &IPTp &ITNs &Malaria in Pregnancy &World Malaria Day &Zero Malaria Bill Brieger | 25 Apr 2021
Twenty Years of Malaria Day Observances: Jhpiego at the Forefront
 In 2001 the first Africa Malaria Day (AMD) was observed. The opportunity to mark progress and exhort increased efforts for the continent continued through 2007. Then in 2008, the concept of World Malaria Day (WMD) took over, though it could not be denied that the bulk of malaria morbidity, mortality and intervention still was focused on African countries. Other countries have made progress such as the recent certification of malaria elimination in Argentina and El Salvador, but twenty years after the first AMD/WMD, Africa is still leading the way for creative, sustained intervention against the disease, despite threats to resources from economic downturns and new pandemic diseases.
In 2001 the first Africa Malaria Day (AMD) was observed. The opportunity to mark progress and exhort increased efforts for the continent continued through 2007. Then in 2008, the concept of World Malaria Day (WMD) took over, though it could not be denied that the bulk of malaria morbidity, mortality and intervention still was focused on African countries. Other countries have made progress such as the recent certification of malaria elimination in Argentina and El Salvador, but twenty years after the first AMD/WMD, Africa is still leading the way for creative, sustained intervention against the disease, despite threats to resources from economic downturns and new pandemic diseases.
Below we go straight to Africa to share activities and observances of WMD 2021 from Jhpiego’s African Malaria Technical Officers. After reading through, please watch “Jhpiego Leaves No One Behind | World Malaria Day, 2021″ on YouTube.
 “Saramed” from Guinea reports that Guinea, like other countries in the world, celebrates World Malaria Day under the theme: ” Zero Malaria, Draw a Line on Malaria “. We are currently conducting the following activities:
“Saramed” from Guinea reports that Guinea, like other countries in the world, celebrates World Malaria Day under the theme: ” Zero Malaria, Draw a Line on Malaria “. We are currently conducting the following activities:
- Lectures and debates on malaria in medical faculties and health schools;
- Animation of debate programs on malaria in public and private radios and televisions of the country,
- Advocacy and sensitization of religious and other influential people
- Carrying out a package of activities (administration of IPT to pregnant women who have missed their ANC appointment, community distribution of LLINs, screening and treatment of confirmed cases, awareness raising on malaria) in high incidence localities.
These activities is in line with the WHO approach of “high burden, high impact”.
 Noella Umulisa reports that the WMD celebration took place in Eastern Province, in Bugesera district in the Mareba sector. Due to COVID-19 pandemic ,only 100 persons were invited to the event.This year’s the national theme is “Zero Malaria starts with me”.
Noella Umulisa reports that the WMD celebration took place in Eastern Province, in Bugesera district in the Mareba sector. Due to COVID-19 pandemic ,only 100 persons were invited to the event.This year’s the national theme is “Zero Malaria starts with me”.
Key activities during the event included …
- Visit of breeding sites under sentinel surveillance
- Visit of indoor residual spraying (IRS) sites
- Launching of the Awareness of the population using drones on the ongoing IRS campaign in this time of COVID-19
- Song by CHWs
- Certificate to Integrated Vector Management (IVM) Training of Trainers who will train others up to village level
- Speech of the Director General ,the guest of honor.
 From Burkina Faso, Yousseff Sawadogo and Moumouni Bonkoungou shared photos of the celebration that featured a giant Insecticide-Treated Net, a speech by the US Ambassador, a malaria song composed by a nurse, an official speech by the President of the National Assembly, and national recognition given to one of the current Jhpiego staff members, Thiery Ouedraogo, who at one time also served as director of the national malaria control program. He was decorated by the country’s authorities as a knight of the order of merit.
From Burkina Faso, Yousseff Sawadogo and Moumouni Bonkoungou shared photos of the celebration that featured a giant Insecticide-Treated Net, a speech by the US Ambassador, a malaria song composed by a nurse, an official speech by the President of the National Assembly, and national recognition given to one of the current Jhpiego staff members, Thiery Ouedraogo, who at one time also served as director of the national malaria control program. He was decorated by the country’s authorities as a knight of the order of merit.
 Bright Orgi from Jhpiego’s TiPToP malaria in pregnancy project in Nigeria ?? shared photos from a series of compound meetings in the community to mark WMD 2021. The meetings focused on malaria prevention and treatment. Provided opportunities to rural communities to ask questions on malaria issues. Here we can see that observance of WMD must be taken to the people who actually suffer from malaria and need to be actively involved in its solution. Deo Cibinda from the Democratic Republic of the Congo share photos of a national celebration, seen to the left.
Bright Orgi from Jhpiego’s TiPToP malaria in pregnancy project in Nigeria ?? shared photos from a series of compound meetings in the community to mark WMD 2021. The meetings focused on malaria prevention and treatment. Provided opportunities to rural communities to ask questions on malaria issues. Here we can see that observance of WMD must be taken to the people who actually suffer from malaria and need to be actively involved in its solution. Deo Cibinda from the Democratic Republic of the Congo share photos of a national celebration, seen to the left.
 Finally, As Kristen Vibbert noted, “These are such amazing World Malaria Day stories. I’m so heartened to see all of these great country efforts to remind everyone of how the fight against malaria must continue despite the Covid-19 pandemic.” Charles Wanga tweeted, “We know how to defeat #malaria. But that’s not enough. We must do more to save pregnant women and children from the deadly scourge. This #WorldMalariaDay and everyday, because@Jhpiego leaves no one behind in our fight to #EndMalaria for good in Africa, and everywhere”
Finally, As Kristen Vibbert noted, “These are such amazing World Malaria Day stories. I’m so heartened to see all of these great country efforts to remind everyone of how the fight against malaria must continue despite the Covid-19 pandemic.” Charles Wanga tweeted, “We know how to defeat #malaria. But that’s not enough. We must do more to save pregnant women and children from the deadly scourge. This #WorldMalariaDay and everyday, because@Jhpiego leaves no one behind in our fight to #EndMalaria for good in Africa, and everywhere”