Equity &ITNs Bill Brieger | 28 Feb 2019
Equity in Malaria Programming, the example of bednets
The WHO defines Equity as “the absence of avoidable, unfair, or remediable differences among groups of people, whether those groups are defined socially, economically, demographically or geographically or by other means of stratification. ‘Health equity’ or ‘equity in health’ implies that ideally everyone should have a fair opportunity to attain their full health potential and that no one should be disadvantaged from achieving this potential.”
WHO goes on to say that, “Countries and programs need to disaggregate selected health indicators by key stratifiers including demographic characteristics (gender, age), place of residence (urban/rural, subnational), socioeconomic status (wealth, education), as well as other characteristics (migrant/minority status etc.).”
 Writing for the Tropical Disease Research Program, H. Kristian Heggenhougen, Veronica Hackethal, and Pramila Vivek in the publication, The behavioural and social aspects of malaria and its control, say that …
Writing for the Tropical Disease Research Program, H. Kristian Heggenhougen, Veronica Hackethal, and Pramila Vivek in the publication, The behavioural and social aspects of malaria and its control, say that …
“What must now be clear is our conviction that any review of factors for world-wide malaria control must give specific attention to issues of socio-economic inequity and disease epidemiology.” Malaria is not an equal opportunity killer, but disproportionately affects certain segments of the population. Heggenhougen et al. continue that, “while we argue for a focused attack on malaria, we cannot avoid noting that without attention to these larger matters – inequity and marginalization – any improvement in health, including malaria, may be short-lived.”
 The Demographic and Health Survey (DHS) and its Malaria Indicator Survey (MIS) provide an important snapshot on equity issues in the rollout and coverage of major malaria. In particular, we look at the issue of long lasting insecticide-treated nets in two countries, Ghana (2016 MIS) and Liberia (2016 MIS), to demonstrate how equity issues can be seen. Two three measures are considered, wealth quintile, location (urban/rural) and gender/sex.
The Demographic and Health Survey (DHS) and its Malaria Indicator Survey (MIS) provide an important snapshot on equity issues in the rollout and coverage of major malaria. In particular, we look at the issue of long lasting insecticide-treated nets in two countries, Ghana (2016 MIS) and Liberia (2016 MIS), to demonstrate how equity issues can be seen. Two three measures are considered, wealth quintile, location (urban/rural) and gender/sex.
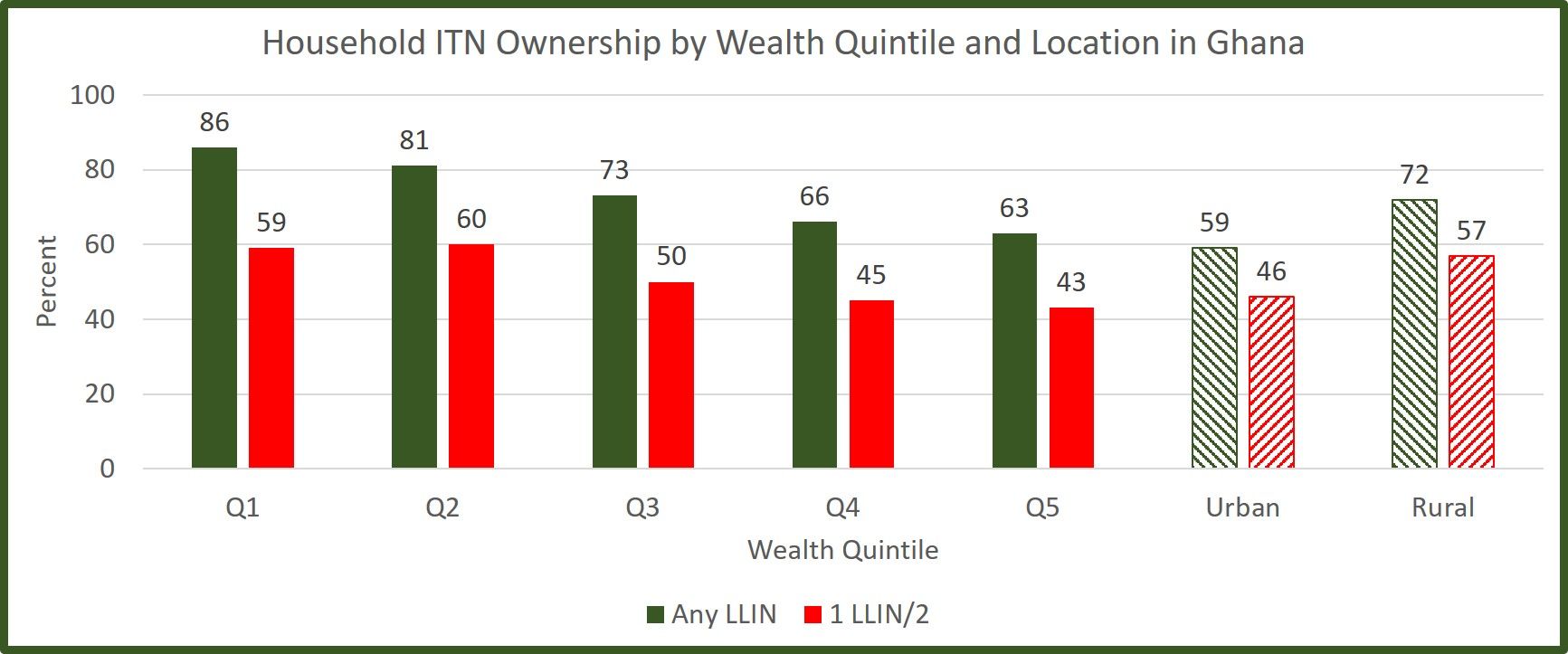
 In Ghana we see that having at least one net for the household is more common in lower income groups. These groups are more vulnerable. Although not specifically shown in the MIS, one might assume that people in the higher income groups have better quality housing that provides less opportunity for mosquito entry. Likewise households in rural areas, where anopheles are more likely to breed, have a higher proportion of nets. So while nets are not ‘equally distributed by these characteristics, they are more favorably available in those households that may be more vulnerable to malaria.
In Ghana we see that having at least one net for the household is more common in lower income groups. These groups are more vulnerable. Although not specifically shown in the MIS, one might assume that people in the higher income groups have better quality housing that provides less opportunity for mosquito entry. Likewise households in rural areas, where anopheles are more likely to breed, have a higher proportion of nets. So while nets are not ‘equally distributed by these characteristics, they are more favorably available in those households that may be more vulnerable to malaria.
When we look at the indicator of universal coverage where it is expected that there should be one net for every two household members, the proportion meeting that goal is much lower than simply having a net in the household for all groups. That said the pattern of higher proportions among rural and lower income groups remains. Within households, the Ghana MIS a nearly equal proportion of female (43%) and male (41%) had slept under a net the night prior to the survey.
 Overall, Liberia has much lower LLIN coverage than Ghana. The pattern for location is similar to that of Ghana, but for wealth, the poorest group (Q1) have lower coverage that wealth quintile groups 2-4. Also as in Ghana the Female (40%) and male (38%) are very similar.
Overall, Liberia has much lower LLIN coverage than Ghana. The pattern for location is similar to that of Ghana, but for wealth, the poorest group (Q1) have lower coverage that wealth quintile groups 2-4. Also as in Ghana the Female (40%) and male (38%) are very similar.
We encourage readers to review the recent MIS and/or DHS reports from the countries where they work and look for differences in net availability as well as uptake of other malaria control interventions to determine the level of equity in intervention access and use, but also as one sees in Liberia, take action to ensure that strategies are in place to reach the poorest and most vulnerable segment of society.
Capacity Building &Case Management &Funding &Health Systems &IPTp &ITNs &Leadership Bill Brieger | 09 Feb 2019
Guinea: The Challenge of Malaria Control in a Post-Ebola Context
The preliminary 2018 Demographic and Health Survey (DHS) data have been released for Guinea (Conakry). Since the last DHS in 2012, Guinea and its neighbors experienced the largest Ebola outbreak in history, an event that damaged already weak health systems.
 The previous DHS showed very weak malaria indicators. Only 47% of households had at least one ITN, which averages to 0.8 ITNs per person (compared to the universal coverage of 2.0). Among vulnerable groups only 26% of children below the age of 5 years slept under an ITN, as did 28% of pregnant women. Very few, 18%, pregnant women got two doses of IPTp, and only 5% of febrile children received ACTs (testing was not reported then).
The previous DHS showed very weak malaria indicators. Only 47% of households had at least one ITN, which averages to 0.8 ITNs per person (compared to the universal coverage of 2.0). Among vulnerable groups only 26% of children below the age of 5 years slept under an ITN, as did 28% of pregnant women. Very few, 18%, pregnant women got two doses of IPTp, and only 5% of febrile children received ACTs (testing was not reported then).
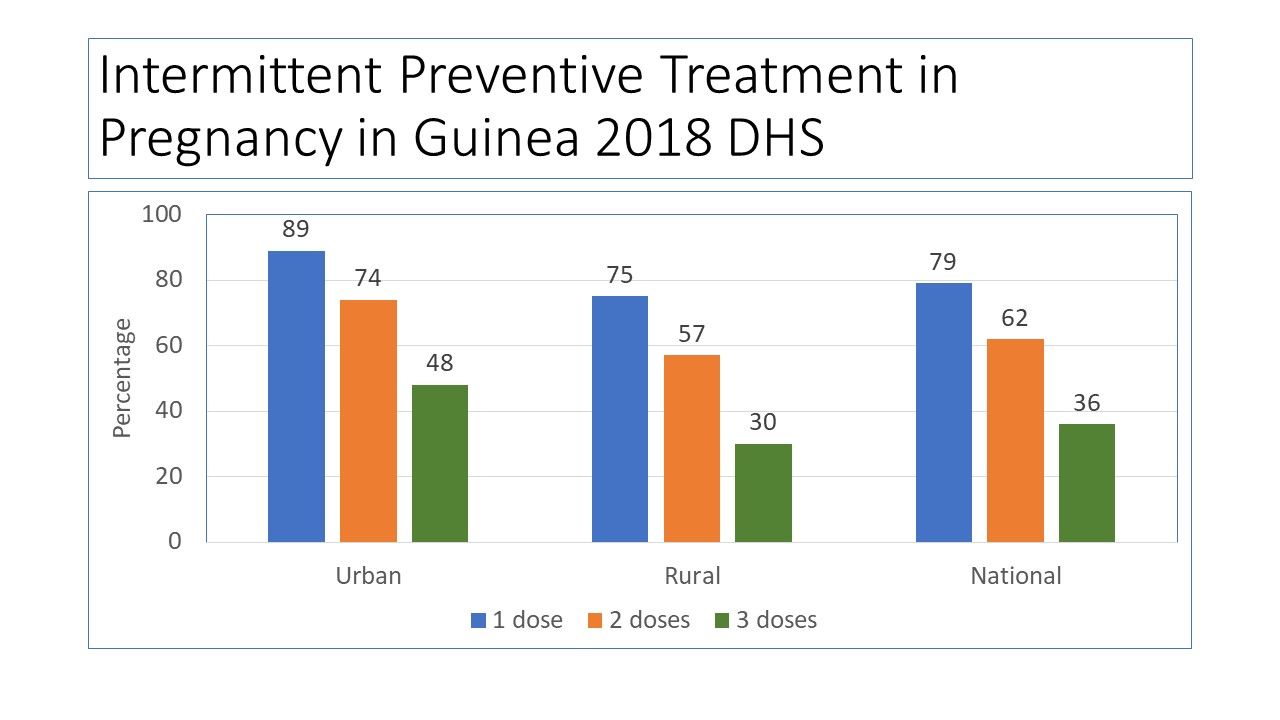
 Not much has changed concerning ITN coverage as reported in 2018. Slight improvements are seen in IPTp (which now requires 3 or more doses) and malaria testing and treatment for children. Ironically none of the indicators has passed the original 2006 Roll Back Malaria target of 60%, let alone 80% for 2010 and not of course the drive for universal coverage.
Not much has changed concerning ITN coverage as reported in 2018. Slight improvements are seen in IPTp (which now requires 3 or more doses) and malaria testing and treatment for children. Ironically none of the indicators has passed the original 2006 Roll Back Malaria target of 60%, let alone 80% for 2010 and not of course the drive for universal coverage.
 DHS has released a preliminary report for 2018 and the malaria component is summarized in the charts posted here. The national coverage for ITNs is 44%, slightly lower than 2012, but the average per household member is slightly higher at 1.1. Again, these numbers do not mark significant progress. Looking at wealth and ITN ownership there is a slight benefit in terms of equity in net possession among those with lower income, but this must be seen in the overall context of very low basic coverage.
DHS has released a preliminary report for 2018 and the malaria component is summarized in the charts posted here. The national coverage for ITNs is 44%, slightly lower than 2012, but the average per household member is slightly higher at 1.1. Again, these numbers do not mark significant progress. Looking at wealth and ITN ownership there is a slight benefit in terms of equity in net possession among those with lower income, but this must be seen in the overall context of very low basic coverage.
 Having a net in the household and using it are different challenges as seen in the reports of sleeping under the net on the night prior to the survey among children under 5 years of age and pregnant women. The sad finding is that even in households that own a net, the coverage of these two groups remains very low. This is reflected in the low net per person ratio nationally (1.1).
Having a net in the household and using it are different challenges as seen in the reports of sleeping under the net on the night prior to the survey among children under 5 years of age and pregnant women. The sad finding is that even in households that own a net, the coverage of these two groups remains very low. This is reflected in the low net per person ratio nationally (1.1).
 One would almost wonder if malaria is a neglected disease in Guinea. The reality is that since 2003, Guinea has received around $172 million US dollars in malaria project funding from the Global Fund. Its most recent annual funding from the US President’s Malaria Initiative (PMI) is around $14 million. Of that PMI funding 24% was designated for nets and related activities, while 52% was to be spent on medicines, diagnostics and pharmaceutical management. These investments include systems strengthening and capacity building in addition to commodities.
One would almost wonder if malaria is a neglected disease in Guinea. The reality is that since 2003, Guinea has received around $172 million US dollars in malaria project funding from the Global Fund. Its most recent annual funding from the US President’s Malaria Initiative (PMI) is around $14 million. Of that PMI funding 24% was designated for nets and related activities, while 52% was to be spent on medicines, diagnostics and pharmaceutical management. These investments include systems strengthening and capacity building in addition to commodities.
PMI provides the needed context: “Since the country was declared Ebola-free in in June of 2016, Guinea continues to make positive advances towards building a strong health system in line with the health recovery plan. The government continues to mobilize internal and external resources for rolling out the health system recovery plan, but much remains to be done if this plan is to yield the intended results.” Areas in particular need of strengthening within the National Malaria Control Program include coordination, health information systems, leadership, supervision and logistics.
Three years have passed since the last Ebola case in Guinea. Hopefully the country can stave off another outbreak and at the same time strengthen its health system. Guinea may not yet be targeted for malaria elimination, but until systems are strengthened, the resources going into malaria control will not be able to push malaria indicators toward saving more lives.
Advocacy &Case Management &Children &Education &Seasonal Malaria Chemoprevention Bill Brieger | 02 Feb 2019
A child’s personal experiences with malaria lead to a life career fighting the disease
Gbenga Jokodola tells his story of growing up to fight malaria in Nigeria. Gbenga has a MPH in Field Epidemiology from the University of Ibadan, and a BPharm from Ahmadu Bello University. He is currently working with Malaria Consortium as a Zonal Project Manager on the Seasonal Malaria Chemoprevention (SMC) Project, delivering preventive care to over 400,000 children between the ages of 3 – 59 months in Jigawa and Katsina States of Nigeria. He has worked on several malaria projects over the years sponsored by Unicef, the Global Fund, Catholic Relief Services and the Bill & Melinda Gates Foundation. As he narrates below, his early experiences with malaria were formative of his present focus in life.

At 3 months of age Gbenga was probably still protected from malaria by maternal antibodies and did not realize what malaria held in store for his future
Growing up in Zaria, northern Nigeria in the 70s and 80s was one of the best experience any child could ask for. I lived with my parents in two rented rooms in a compound on one of the streets in Sabon Gari Zaria – a community that had virtually all the tribes in Nigeria and of course, with all the love and communal living you can ever get from a true Nigerian community.
In such loving setting we enjoyed as children, I imagined that mosquito communities also lived around our pit latrine and backyard. I imagined that parent-mosquitoes trained their off-springs very well on how to bite and fly away tactfully, how to dodge the usual clap-like manner we use in killing mosquitoes, which homes to avoid visiting, and so on.
I was reputed to be a strong boy then, one of the few kids who were “strong”; I was a “tough” boy who rarely fell ill to malaria. Then, it was common to hear, “Gbenga is a strong boy”. I ate and slept in any room in our compound – with or without covering from mosquito and was hailed for doing so by my friends who often fall ill to malaria.
Life lesson as a Primary School pupil: There is no immunity against malaria
One day, the “malaria forces” (mosquitoes) taught me a life lesson: Indeed, there is no immunity against malaria.
My local Government primary school rotated school attendance between morning and afternoon every week. As an 8-year-old, while preparing for my afternoon school I suddenly felt very cold and sleepy at the same time and decided to lie down briefly on my senior brother’s 6-spring bed in our sitting room. Shortly after, I was shivering and sweating profusely under 3 of my mother’s wrappers.
Help was not immediately near as most people were out. My head was pounding like I was a piece of yam being pounded with a pestle in my mother’s mortar. My stomach was churning. All the while, I kept saying “I am a strong boy, I will not be sick”! I was in that state for over an hour. I began to wonder if I was strong after all and will not end up dying. I could no longer talk but my teeth were chattering.

Gbenga second from left at about 7 years old in company of Sisters and friends in the compound
Sweating profusely, yet I was cold! I was helpless. It was in this state that one of our neighbor’s daughters walked into our sitting room, wondering if there was any food to eat. Immediately she saw the “strong man” shivering under 3 wrappers, she raised an alarm. Her shout saved me as neighbors immediately rushed into our sitting room. Among them was a relation of the landlord, a beautiful “Aunty” Esther, who was visiting from the Ahmadu Bello University school of Nursing. As soon as she came over, she said: “this is malaria!”.
Aunty Esther immediately organized and rescued me that day; she saved the life of the “strong man”! She quickly sought iced-cold water and toweled my body with my father’s “untouchable” towel hanging on the door of the inner room. Ah, what a good feel it was! She then gave me a sweet syrup which I later found out to be Paracetamol syrup. After about 30 minutes, she returned with a plate of hot rice and stew, encouraging me to eat before treatment with anti-malarial medication. I struggled to eat the rice, angry that I had lost my ever-available appetite! I only took few spoons, amidst the encouragement I received from all present.
I was then given an injection by Aunty Nurse Esther, tucked back into the bed and told to prepare to sleep. She then said, “Gbenga, no school for you today, okay? You even need to get well before you resume school”. Everyone knew I loved school. I had to lose a precious school day (and three more days) to malaria! So, I simply focused on staying alive, wondering which “wicked” mosquito bit me. That was the day I dramatically lost my title of “strong man” to malaria, painfully realizing that I was not immune to malaria at all!
My treatment against malaria was continued with further jabs of the needle (twice a day) over the course of the next 3 days at the Dispensary/Primary Health Unit “Aunty” Esther directed my parents to. I got well and resumed school after the third day. Later, I researched and found out I was treated with a sedative, Chloroquine and Paracetamol.
Gbenga with classmates at First Baptist Church, Benin Street, Sabon Gari Zaria
My parents later introduced “Sunday-Sunday Medicine” (one Sweetened pyrimethamine tablet weekly) against Malaria to our diet on Sundays. With this painful encounter with Malaria, I resolved to fight mosquitoes; I was determined to regain my “strong man” title. I made up my mind to be a community health worker, saving communities from diseases like malaria.
Fast-forward to Year 2007: My new twist in combating Malaria
By the year 2007, my personal malaria episodes had lessened with greater knowledge of the disease. In addition, the application of the preventive, diagnostic and treatment procedures reduced my malaria episodes to about 1 in 3 years. With each episode, I normally use laboratory test (microscopy) to confirm if severity is +, ++, or even +++. Thereafter, I get a prescription from a Physician on appropriate medication to use.
However, while practicing in Abuja, I encountered a tearful case of death from malaria, of an 8-year old beautiful daughter of a colleague. Three days prior to her death, a Community Pharmacist had dispensed anti-malarial medication to her, based on prescription tendered by the father from a Government hospital he had earlier taken her to. The news of her death brought back memories of how I would have died as

ACCESS-SMC Project: Scaling up access to seasonal malaria chemoprevention in the Sahel
an 8-year old from this same Malaria. Yes, this same Malaria! That death of the 8-year old triggered a fresh resolve in me to step up my fight with mosquitoes and combat malaria squarely at community, state, National and global levels.
Still at War with Malaria in 2018
Now armed with post-graduate training in Public Health/Epidemiology and field-based experience, my Malaria diagnosis strategy has now changed. I now use Rapid Diagnostic Test Kits (RDT). If confirmed positive, I receive prescription on the most applicable Artemisinin-based combination Therapy (ACT) to use.
My malaria story continues and will only end when mosquitoes are defeated – when children and adults no longer fall ill nor die from mosquito bites that cause malaria.
You can follow Gbenga on Twitter.