Eyelachew Desta shares thoughts as a guest blogger in time for Mothers’ Day. Concern is expressed about ensuring increased access for low cost essential lifesaving Maternal newborn and child health supplies in Ethiopia. This posting appeared originally at Social & Cultural Basis for Community and Primary Health Programs.
Can you imagine? At this time of Mother’s Day celebration, there are thousands of women living in low income country , unlucky to be a mother to enjoy the celebration of mother’s day because of preventable birth complications due to lack of accesses to essential low cost medicines and commodities necessary for maternal, Child and New born Health. One of these low-income countries is Ethiopia where maternal and child mortality is still high.
According to an analysis published by Reproductive Health Supplies Coalition (RHSC), a quarter of all deaths between 2009 and 2013 occurred in Ethiopia are maternal mortality. This study indicated “postpartum hemorrhage (PPH)— uncontrolled bleeding after childbirth—and preeclampsia/eclampsia (PP/E)- a condition which causes high blood pressure and seizures during pregnancy”, among others, are the two leading causes of maternal deaths in Ethiopia ,could be treated by low cost and effective medicines, Oxytocin and Misoprostol.
See Photo Credit for UNICEF
The availability of accessible, reliable and low cost essential maternal health commodities is indispensable to address maternal and child mortality in Ethiopia. However according to an assessment study conducted in Ethiopia, there are gaps in the supply chain management of commodities for maternal, neonatal, and child health.
According to this study one of these gaps is “The supply chain system for MNCH commodities is inconsistent and has not been integrated into the Integrated Pharmaceutical Logistics System (IPLS)” of Ethiopia. Further the study indicated that family planning, HIV, tuberculosis, and malaria have been included in this IPLS, but not MNCH commodities. This study also identified that there is a lack of common understanding at lower level of the health system about the national policy and protocols as well as its implementation to provide MNCH services and commodities free of charge at primary health care units.
To address these gaps, there is a need of immediate actions as well as strong commitment among all stakeholders involved and engaged in the funding, monitoring, regulating and administering the logistic supply of MNCH commodities in Ethiopia. The Federal Ministry of Health (FMOH) should develop a strategy to provide continues education and training at all levels of the health system about its policy of provision of MNCH services and commodities free of charge at primary health care units , ensure policy protocols are implemented properly.
In addition to these the FMOH should strengthen its monitoring system to identify gaps in the implementation of the MNCH services and commodities policy and take measures to narrow those gaps. The Ethiopia Pharmaceuticals Fund and Supply Agency should revise its Integrated Pharmaceutical Logistics System (IPLS) to insure MNCH commodities are integrated in the system by 2020. Ultimately international donors like USAID needs to continue and strengthen their financial and technical support to the overall MNCH program of Ethiopia .
CS4ME was created during the Global Malaria Civil Society Strategising and Advocacy Pre-Meeting jointly convened by the Global Fund Advocates Network Asia-Pacific (GFAN AP) and APCASO held on 29th and 30th June 2018, prior to the First Malaria Wor1d Congress in Melbourne, Australia, with the support of the Malaria World Congress, Global Fund to Fight AIDS, Tuberculosis and Malaria, and the Burnet Institute. An interim working group mode up of individuals that attended the Pre-Meeting was established to coordinate, recommend processes and mechanisms, identify resources and support necessary for CS4ME going forward. For more Information please contact Ms Olivia Ngou Zongue <ngouolivia@gmail.com> of the Interim Working Group of CS4ME for further information. The Declaration arising from their meeting if provided below.
GLOBAL CIVIL SOCIETY FOR MALARIA ELIMINATION (CS4ME) DECLARATION MALARIA WORLD CONGRESS 1ST-5TH JULY 2018 MELBOURNE, AUSTRALIA
Firm in the belief that empowered community and civil society are game-changers in health responses, we, representatives of national, regional and global malaria communities and civil society attending the First Malaria World Congress, have come together and formed the Global Civil Society for Malaria Elimination (CS4ME) as part of our commitment to joint advocacy for more effective, sustainable, people-centred, rights-based, equitable, and inclusive malaria programmes and Interventions.
At a time when the world has the resources and tools to prevent and treat malaria, it is unconscionable how people – mainly from impoverished, vulnerable and underserved communities – continue to die from the disease. While we commend the efforts of governments and the international community that brought the world closer to malaria elimination, we call for greater accountability, political will and action, resource investments, and sense of urgency to eliminate the disease.
CS4ME makes the following call to the governments of implementing countries, donor countries and other duty bearers:
FRAME MALARIA RESPONSES IN THE CONTEXT Of SOCIAL JUSTICE AND HUMAN RIGHTS, AND WITHIN UNIVERSAL HEALTH COVERAGE
Significant progress has been attained during the past 10 years to reduce the burden of malaria throughout the world and in working towards achieving malaria elimination. As countries enter into the elimination phase, we see again and again the epidemic concentrating among the most marginalised, remote, and disenfranchised communities. In South East Asia, the concentration of malaria among communities barred from accessing quality and affordable health services has accelerated the emergence of drug resistance that now threatens the wor1d at large. Everywhere, the last mile of elimination becomes a matter of access to health for impoverished and marginalised communities, in particular, refugees, ethnic minorities, indigenous communities, migrant and mobile populations – with many of the risks faced by these groups compounded further amongst women and girls.
Including the most local, represents a strategic investment contributing to appropriate, effective service delivery and people-driven surveillance and response.
We call on national governments, international institutions, bilateral and multilateral donors to prioritise and increase funding allocations for community-driven community and civil society initiatives. We request that specific funding streams be made available to community groups, and their access supported through peer-to-peer technical assistance.
Furthermore, we request that key performance indicators that enable accountability for bringing malaria services to the underserved be developed and implemented.
PARTNER WITH CIVIL SOCIETY AND COMMUNITY ACTORS FOR AN EFFECTIVE MALARIA SURVEILLANCE AND RESPONSE
As surveillance becomes an essential pillar for malaria elimination, the need for timely and robust data is increasingly critical. Essential evidence includes routine data, qualitative and quantitative research, as well as experience, lessons learned and the voices from affected communities. Support is required to build the ability of civil society to generate evidence, as well as to communicate it effectively to ensure that community-generated evidence will be able to influence decisions and result in sustained change.
To eliminate malaria, surveillance requires a response. Communities and civil society are the first responders, and will have the clearest insight Into what responses are effective in their context or on behalf of their constituents.
We demand that communities and civil society organisations be given equitable access to data and other information that can inform field-level response. We call for transparent information systems and multi-directional information flows in order to enable dialogue, and inform decisions at all levels. We urge the building up of surveillance systems that involve communities as analysts, advisors, decision-makers and responders.
We, malaria communities and civil society, offer our support, expertise, and lived experiences In contributing towards our shared vision of malaria elimination. We are fully committed to working alongside other stakeholders to build stronger, more inclusive and effective partnerships and sustainable responses towards elimination of malaria in this lifetime.
World Health Day 2018 is promoting universal health coverage. National Health Insurance Schemes (NHIS) are seen as a way to foster universal health coverage by improving access to basic, life-saving care. In malaria-endemic countries, NHIS hopefully play a role in reducing malaria mortality. For example in Nepal, malaria was among the chronic and communicable illnesses that showed increased catastrophic health expenditure over time leading to impoverishment. Health insurance was seen as a way to counteract this problem.
Although health insurance coverage in Tanzania was quite low, “a higher proportion of women with health insurance had a proper timing of 1st ANC attendance compared to their counterparts.” This enables them to access malaria prevention services and interventions.
In Ghana a decrease in malaria deaths was seen against a backdrop of increased admissions owing to free access to hospitalization through the NHIS, but hospital admission is not an option for all. Community case management is aimed at increasing access to and coverage of timely management of malaria and other child illnesses, but such services may not be covered by a NHIS. Since iCCM is effective in reaching children, Ghana is questioning how community based health workers can be brought into the health insurance arena.
Rwanda started its community based health insurance scheme in 2003 also and by 2013 had achieved 74% coverage. In Rwanda community malaria action teams (CMATs) were initiated in mid-2014 as platforms to deliver malaria preventive messages at village level. Among other benefits of the CMATs, an increase in community-based health insurance membership occurred,
Mutuelle (community health insurance) kiosk outside a clinic in Burkina Faso
which was also considered as a predictor of prompt and adequate care. Another study in Rwanda showed that head of household having health insurance (among other factors) was significantly associated with prompt and adequate care for presumed malaria illness.
NHIS have their own challenges in terms of affordability, community understanding of payment of premiums and availability of points of care that accept insurance or are accredited. And not all endemic countries have achieved even the modest successes of NHIS in Ghana and Rwanda. Thus health insurance offers hope for expanding universal coverage of malaria services, but health systems and community understanding and participation need to be improved for this to happen.
March is Women’s History Month and thus a time to examine the role of women in bringing an end to malaria. For many years studies at the household level have told us that women often lack the financial independence or social support to make important decisions about malaria treatment and prevention for themselves and their children. Furthermore, as WHO notes, “Gender norms and values … influence the division of labour, leisure patterns, and sleeping arrangements may lead to different patterns of exposure to mosquitoes for men and women.” As part of the solution to these problems, it is important to look at women role models in the fight against the disease – at women making malaria history.
One of these role models is Tu Youyou who became one of three scientists to win the 2015 Nobel Prize for medicine. Her work of over 40 years was virtually unknown to the outside world until then, but her study of artemisinin medicinal compounds has saved the lives of millions.
Moving from the lab to the community one can find role models who have broken role stereotypes. A few years ago President’s Malaria Initiative-funded Africa Indoor Residual Spraying (AIRS) project drew out attention to Maimouna Sanogo as a woman making a difference. She helped protect people in her country from malaria through her work as a supervisor on AIRS indoor residual spraying project in Mali. The AIRS project reported that, “As a woman in a leadership role, Maimouna is a trailblazer. In Mali, only 37% of women participate in the labor force, while participation is nearly double among Malian men (70%).”
Women have played crucial leadership roles in national malaria programs. Dr TO Sofola as Director of Nigeria’s National Malaria Control Program (NMCP, now National Malaria Elimination Program) guided the transition of case management policy to the use of artemisinin-based combination therapy, oversaw planning for the first massive national LLIN campaign, guided development of the World Bank Booster Program support, helped strengthen Nigeria’s first Global Fund Malaria Grants, and brought state level malaria control programs into the national strategy process. Women have also led NMCPs in Malawi, Kenya and other countries.
Dr Rose Leke, Emeritus Professor of Immunology and Parasitology, Faculty of Medicine and Biomedical Sciences, University of Yaounde, Cameroon, was one of six people to be given the Kwame Nkrumah Scientific Award for Women in 2011. Dr Leke explained the challenges facing women, “Science is still a challenging field for women to enter, and even more so in which to progress. At the university, I have seen many promising young women finish their studies and start jobs as assistants only to either get stuck in that position indefinitely or eventually leave to take care of their families. There just wasn’t the mentorship or financial support for research needed for them to be able to progress. It was an issue I really took to heart.” Therefore, Dr Leke and colleagues started the HIGHER Women Consortium in Cameroon. We provided training and mentorship to young women researchers.
Women in academics, research, government and front line programs have and continue to make history in the efforts to eliminate malaria. As Dr Leke’s example shows, these women leaders can make sure no one stands in the way of ensuring that the next generation of women scientists, managers and field workers make malaria history.
The time is ripe for a revitalization of the primary health care (PHC) movement. “Health for All through Primary Health Care” (HFA) was first envisioned at the 1978 International Conference on Primary Health Care (World Health Organization and UNICEF), and was enshrined in the Declaration of Alma-Ata. The HFA goal of bringing essential, affordable, scientifically sound, socially acceptable health care provided by health workers who are trained to work as a health team and who are responsive to the health needs of the community, guided by strong community engagement by the year 2000 but has not been fully met. Fortunately the vision of Alma-Ata has taken root, sprouted and flourished in a number of locations.
Thanks to the vision and intellectual and political leadership of Dr. Tedros Adhanom Ghebreyesus, the then Minister of Health of Ethiopia and recently elected Director General of the World Health Organization, Ethiopia is an outstanding example of the Alma-Ata legacy. Access to PHC services was greatly expanded through the training of 40,000 Health Extension Workers (women from the local area with one year of training, each of whom serve 2,500 people and receive a government salary), recruitment of 3 million community female health volunteers (called the Health Development Army), and engagement with communities to enable them to take responsibility for improving their health.
This expansion of PHC enabled Ethiopia to achieve its health-related MDGs. Child mortality (those younger than 5 years of age) declined from 166 deaths per 1,000 live births in 1990 to 67 in 2016 (MDG 4). Significant progress was achieved in reducing levels of childhood malnutrition (MDG 1). MDG 5 was almost reached, with a decline in maternal morality of 72%, versus the goal of 75%, and the percentage of mothers obtaining a delivery by a skilled provider increased 6-fold between 1995 and 2016. The prevalence rate of modern contraceptive use increased from 6% in 2000 to 35% in 2016. MDG 6 (for HIV, malaria and tuberculosis) was also reached. The number of new HIV infections declined by 90%, and the number of AIDS-related deaths by 53%. Between 1990 and 2015, the tuberculosis incidence and mortality rate declined by 48% and 72%, respectively. The malaria incidence rate declined by 50% and malaria mortality by 60%. Ethiopia’s PHC system is acknowledged as the major factor leading to these impressive health gains.
Representatives from more than half of sub-Saharan Africa countries have come to Ethiopia to see its PHC system in action. Because of this interest, in 2016 the Federal Ministry of Health of Ethiopia established the International Institute for Primary Health Care – Ethiopia, with seed funding from the Bill & Melinda Gates Foundation and technical support from the Johns Hopkins Bloomberg School of Public Health. Our goal is for the Institute to become a global center of excellence for training, knowledge dissemination and research in primary health care, supported by multiple donors.
The Institute has begun to provide formalized short-term training to high-level policy makers and officials, program planners and managers, as well as to those engaged in service delivery, to see first-hand how an effective national PHC system functions. Trainees come from within Ethiopia and around the world. Trainees also visit communities, meet their leaders, and observe primary health care providers at work. Trainees will return to their home country with renewed energy and new vision and skills to revitalize their own primary health care system.
The Institute will also conduct and support research that yields evidence to guide ongoing strengthening of the Health Extension Program, and will rapidly disseminate open access information about recent advances in PHC. The Institute marks a significant step forward on the road to achieving the Alma-Ata vision of Health for All.
A website for IIfPHC-E is being built to provide further information about these programs and will be available at: www.iifphc.org.
This posting was prepared by: Kesetebirhan Admasu1, Michael J. Klag2, Yifru Berhan Mitke3, Amir Aman4, Mengesha Admassu5, Solomon Zewdu6, Jose Rimon7, Henry B. Perry8
1Chief Executive Officer, Rollback Malaria Partnership, Geneva, Switzerland and Chair, Advisory Board, International Institute for Primary Health Care — Ethiopia
2Dean, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA
3Minister, Federal Ministry of Health, Government of Ethiopia, Addis Ababa, Ethiopia
4State Minister, Federal Ministry of Health, Government of Ethiopia, Addis Ababa, Ethiopia and Co-Chair, Advisory Board, International Institute for Primary Health Care – Ethiopia
5Executive Director, International Institute for Primary Health Care – Ethiopia, Addis Ababa, Ethiopia
6Health and Nutrition Development Lead – Ethiopia, Integrated Programs, Global Policy & Advocacy – Global Development, Bill& Melinda Gates Foundation, Addis Ababa, Ethiopia
7Director, Bill & Melinda Gates Institute for Population and Reproductive Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA
8Coordinator for Johns Hopkins University Support of the International Institute for Primary Health Care – Ethiopia, Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA
In the 1960s, the Brazilian government adopted a laissez-faire attitude, which lead to the predominance of private organizations in the provision of family planning services. Since then, Brazil has witnessed one of the most dramatic reductions in family size in modern history in part due to increased access to family planning services. (Photo New York Times: Members of the Union of Mothers of Angels.)
However, in early 2015, the widespread epidemic of the Zika fever caused by the Zika virus in Brazil caused persisting gaps in access to contraception to resurface. Since it was first detected it has instilled fear and uncertainty in pregnant women whose fetuses could be at risk of Zika-related birth defects like microcephaly should the virus be contracted during pregnancy. This makes access to comprehensive reproductive health services and education a critical need for women who are pregnant or considering becoming pregnant.
While contraceptive use is fairly high in Brazil with 75.2% of women using modern forms of contraception, barriers to access remain. Some women face challenges, some of which include but are not limited to incomplete insurance coverage or lack of reimbursement for long-acting reversible contraceptives (LARCs), high up-front costs, low number of contraceptive service sites, and/or a lack of supply of the implants in the public sector . This may be one driver behind why LARCs only make up 0.5% of all contraceptive sales. Furthermore, 55% of all pregnancies in Brazil estimated to be unplanned and 20% of all lives births are attributed to teenage girls, indicating that there may be substantial reproductive knowledge gaps in how to effectively prevent pregnancy.
Amid the spread of a virus that poses unique health risks to pregnant women and their fetuses, there is an urgent need to address these gaps in reproductive health access and education. First, the Brazilian National Health System, which laudably provides most contraceptives free of charge to about 74% of the population, needs to reevaluate existing policies that may be still limiting access to contraceptive services. Secondly, organizations like the Brazilian Society for Family Welfare (BENFAM), which provides reproductive health services and education to underserved Brazilian communities, need greater financial and political support from policymakers, civil society, and even organizations traditionally opposed to such services like the Catholic Archdiocese.
Despite Brazil’s great strides to improve access to contraception and reproductive health education in recent years, Zika’s arrival highlighted gaps in the existing system that must be addressed through policy reform and greater political and financial support. Especially in the time of Zika, Brazilian women deserve no less.
The potential impact of mass malaria drug administration (MDA) on pregnant women was the focus of Symposium 146 at the recent 65th Annual Meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The symposium was co-chaired by Clara Menéndez and Larry Slutsker who opened the session with an overview.
As malaria control interventions are scaled up and sustained and malaria transmission levels decline and prevalence falls, an increasing number of countries are starting to see elimination on the horizon. For pregnant women, the antimalarial antibodies that have provided some level of protection in moderate to high malaria transmission settings are reduced as malaria transmission declines.
Current evidence shows that as transmission levels decline, the consequences from P. falciparum malaria are even greater for pregnant women. As countries enter pre-elimination stage and move towards eventual elimination, it will be important to address the needs of pregnant women given their increased vulnerability.
To help achieve elimination, countries are exploring strategies involving widespread distribution of anti-malarials, primarily artemisinin-combination therapies (ACTs), to asymptomatic individuals, including both mass drug administration (MDA) and mass screen and treat (MSaT).
Animal studies have suggested potential embryo toxicity and teratogenic effects of artemisinin drugs in the first trimester of pregnancy.
Given the limited human data, ACTs are currently contraindicated in first trimester, except in documented cases of clinical malaria illness where quinine is unavailable. This poses a challenge in mass campaigns, as it requires the identification of women in early pregnancy who are not yet obviously pregnant. Screening including offering pregnancy tests and/or interview to ask a woman her pregnancy status directly may not work as many may not wish to reveal their pregnancy status.
Final Algorithm for Screening Prior to MDA in Mozambique
While only about 5% of the population is pregnant at any given time, and only 1/3 of those are in the first trimester, approximately 20% of the population is comprised of women of reproductive age who may be pregnant. Thus, the number of women who need to be screened for pregnancy is substantial across countries. In addition to privacy issues, costs of screening processes are another barrier.
During the symposium Francisco Saúte from Mozambique and Samuel J. Smith from Sierra Leone shared experiences. Clara Menéndez addressed ethical issues involved in the potential risk of MDA with the ACT Dihydroartemisinin-Piperaquine (DHA-P). These two countries have addressed pregnant women in MDAs in two widely different contexts.
Mozambique is learning whether MDA is a valuable component to malaria elimination in the low transmission areas in the southern part of the country. In Sierra Leone MDA was seen as a lifesaving tool to prevent malaria deaths during the Ebola epidemic when taking blood samples for diagnosis was a major risk.
Over several rounds of MDA, Mozambique refined its pregnancy screening procedures over several rounds of MDA as seen in the attached slide. Costs, confidentiality, convenience and efficiency entered into the equation that saw a greater focus on communicating with women rather that testing. Lessons learned from MDA in Mozambique included –
Screening for early pregnancy in the context of MDA is challenging, particularly among teenage girls where disclosing pregnancy can be problematic
Need to train field workers (preferably women) about the need to ensure confidentiality of pregnancy testing/results
Confidentiality is also crucial to ensure adherence to t
MDA Rationale in Sierra Leone during Ebola Outbreak
he pregnancy testing
Women not accepting pregnancy test must be warned on risks/ benefits of ACTs in 1st trimester
Health authorities must understand that IPTp and MDA are not mutually exclusive
The Ebola epidemic in Sierra Leone and its neighbors, Liberia and Guinea, devastated the health workforce, and the availability of any sort of testing supplies was low. The country experienced a major drop in utilization of clinic based MCH services including those for malaria during the period.
MDA Goals in Sierra Leone
Because of initial similarities in presenting symptoms between Ebola and malaria, people were often fearful of going to the health center in case they were detained for Ebola care or were exposed to other patients who had Ebola. Community MDA seemed to be one way to protect the population from malaria in this emergency situation. The attached slide offers a rational for the MDA. A second slide explains Sierra Leone’s goal for MDA with Artesunate-Amodiaquine in the context of Ebola. Though not completely, the Sierra Leone MDAs were able to exclude pregnancy women in their first trimester.
Pregnant women excluded from MDA in Sierra Leone
In conclusion MDA is a tool conceived primarily for countries and areas of countries as part of the pre-elimination strategy. It presents a variety of logistical challenges, but a major concern should also be the ethical issues of giving a potentially toxic drug to women in their first trimester of pregnancy. Alternative strategies to protect these women, including insecticide treated nets, must be explored.
Yacine Djibo, Founder & President of Speak Up Africa is helping focus International Women’s Day (March 8th) on efforts to protect women from malaria in Senegal. She is highlighting the commitments of 8 strong and beautiful women, in Senegal, that are dedicated to eliminating malaria in their country. These commitments are part of an inclusive mass communication campaign that aims to launch a national movement in favor of malaria elimination in Senegal: the “Zero Malaria! Count Me In” campaign
International Women’s Day, represents an opportunity to celebrate the achievements of women all around the world. This year’s theme is “Empowering Women – Empowering Humanity: Picture it” envisions a world where each woman and girl can exercise her choices, such as participating in politics, getting an education or fighting malaria. Below is the second feature on women fighting malaria.
Pr. Awa Marie Coll Seck, the former Executive Secretary of the Roll Back Malaria Partnership pursues her fight against malaria in her own country, Senegal, as Minister of Health. Known for her smooth diplomatic skills and experience in policy formulation, she leads an aggressive reform striving to eliminate all deaths due to malaria in Senegal.
Pr. Awa Marie Coll Seck, Minister of Health and Social Action, Senegal
As global leadership increasingly realizes that the international strategy demands a strong local response and the most active engagement of beneficiaries, Senegal’s Minister of Health walks the talk. The Zero Malaria! Count Me In! campaign aims at creating a movement around the importance of accountability and individual responsibility when it comes to putting an end to this preventable disease. Malaria elimination demands the coordinated efforts of all sectors of society.
As the Minister of Health pledges to build capacity within health facilities so that they are able to properly manage simple and severe cases of malaria, the Zero Malaria! Count Me In! campaign insists on the necessary parallel commitment that Senegalese people need to make in order for the country to reach its malaria elimination objective.
Since the past decade, the country has made tremendous progress and reduced malaria mortality by 62%. Over 6.5 million of insecticide treated mosquito nets were distributed throughout the country and lifesaving medicines are now available in public health facilities free of charge.
Women being the primary caretakers of their families, International Women Day is the perfect occasion to celebrate the leadership of Senegalese women throughout the country, without whom, malaria elimination could never become a reality.
Thank you Minister for leading by example and proving that actions speak louder than words.
Happy International Women Day to all!
*****
Headquartered in Dakar, Senegal, Speak Up Africa is a creative health communications and advocacy organization dedicated to catalyzing African leadership, enabling policy change, securing resources and inspiring individual action for the most pressing issue affecting Africa’s future: child health.
Yacine Djibo, Founder & President of Speak Up Africa is helping focus International Women’s Day (March 8th) on efforts to protect women from malaria in Senegal. She is highlighting the commitments of 8 strong and beautiful women, in Senegal, that are dedicated to eliminating malaria in their country. These commitments are part of an inclusive mass communication campaign that aims to launch a national movement in favor of malaria elimination in Senegal: the “Zero Malaria! Count Me In” campaign
International Women’s Day, represents an opportunity to celebrate the achievements of women all around the world. This year’s theme is “Empowering Women – Empowering Humanity: Picture it” envisions a world where each woman and girl can exercise her choices, such as participating in politics, getting an education or fighting malaria. Below is the first feature on women fighting malaria.
Amy Niambo Ndao Fall, President of the Association of Women Doctors
Dr. Amy Ndao Fall is the President of the Association of Women Doctors of Senegal (AFEMS). This Association, composed of 400 members across the country, aims to undertake sustainable activities for the health of the Senegalese populations.
On the eve of Women International Day, in partnership with the Ministry of health and UN women, AFEMS organized in Dakar on March 7, a conference on the theme “women’s health for an emergent Senegal”.
The conference started with Dr. Ndao signing a pledge, on behalf of AFEMS to support the “Zero Malaria, Count me In” campaign and the National Malaria Control Program in their elimination efforts.
Dr. Ndao stated the association’s commitment to support all efforts toward malaria elimination in Senegal and abroad and concluded with the following words:
“It is a pleasure and an honour for me, to sign this engagement on behalf of AFEMS, to mobilize all our efforts to eliminate malaria in Senegal. We need to keep in mind that women are particularly vulnerable to this disease and that they can be change agents in their families for more efficient vector control in particular by promoting the systematic use of long lasting insecticide-treated mosquito nets for all their family members.”
On this International Women Day, we celebrate and thank Dr. Ndao and all the women Doctors of Senegal for their leadership and commitment to eliminate malaria and are proud to see such amazing partners joining efforts to make Zero Malaria a reality in Senegal.
*****
Headquartered in Dakar, Senegal, Speak Up Africa is a creative health communications and advocacy organization dedicated to catalyzing African leadership, enabling policy change, securing resources and inspiring individual action for the most pressing issue affecting Africa’s future: child health.
Sign up for daily or weekly articles from Bill highlighting the most noteworthy developments in newspapers and scientific journals. Click here to register.

 CS4ME was created during the Global Malaria Civil Society Strategising and Advocacy Pre-Meeting jointly convened by the Global Fund Advocates Network Asia-Pacific (GFAN AP) and APCASO held on 29th and 30th June 2018, prior to the First Malaria Wor1d Congress in Melbourne, Australia, with the support of the Malaria World
CS4ME was created during the Global Malaria Civil Society Strategising and Advocacy Pre-Meeting jointly convened by the Global Fund Advocates Network Asia-Pacific (GFAN AP) and APCASO held on 29th and 30th June 2018, prior to the First Malaria Wor1d Congress in Melbourne, Australia, with the support of the Malaria World  Congress, Global Fund to Fight AIDS, Tuberculosis and Malaria, and the Burnet Institute. An interim working group mode up of individuals that attended the Pre-Meeting was established to coordinate, recommend processes and mechanisms, identify resources and support necessary for CS4ME going forward. For more Information please contact Ms Olivia Ngou Zongue <ngouolivia@gmail.com> of the Interim Working Group of CS4ME for further information. The Declaration arising from their meeting if provided below.
Congress, Global Fund to Fight AIDS, Tuberculosis and Malaria, and the Burnet Institute. An interim working group mode up of individuals that attended the Pre-Meeting was established to coordinate, recommend processes and mechanisms, identify resources and support necessary for CS4ME going forward. For more Information please contact Ms Olivia Ngou Zongue <ngouolivia@gmail.com> of the Interim Working Group of CS4ME for further information. The Declaration arising from their meeting if provided below. Ghana has been operating a NHIS since 2003. Overall national coverage has been estimated at around 40%, with a greater proportion of women covered than men. The 2014 Demographic and Health and 2016 Malaria Indicator Surveys (DHS, MIS) show that around 60% of women of reproductive age have NHIS coverage. How does this translate into malaria service coverage?
Ghana has been operating a NHIS since 2003. Overall national coverage has been estimated at around 40%, with a greater proportion of women covered than men. The 2014 Demographic and Health and 2016 Malaria Indicator Surveys (DHS, MIS) show that around 60% of women of reproductive age have NHIS coverage. How does this translate into malaria service coverage? In Ghana a decrease in malaria deaths was seen against a backdrop of increased admissions owing to free access to hospitalization through the NHIS, but hospital admission is not an option for all. Community case management is aimed at increasing access to and coverage of timely management of malaria and other child illnesses, but such services may not be covered by a NHIS. Since iCCM is effective in reaching children, Ghana is questioning how community based health workers can be brought into the health insurance arena.
In Ghana a decrease in malaria deaths was seen against a backdrop of increased admissions owing to free access to hospitalization through the NHIS, but hospital admission is not an option for all. Community case management is aimed at increasing access to and coverage of timely management of malaria and other child illnesses, but such services may not be covered by a NHIS. Since iCCM is effective in reaching children, Ghana is questioning how community based health workers can be brought into the health insurance arena.
 One of these role models is Tu Youyou who became one of three scientists to win the 2015 Nobel Prize for medicine. Her work of over 40 years was virtually unknown to the outside world until then, but her study of artemisinin medicinal compounds has saved the lives of millions.
One of these role models is Tu Youyou who became one of three scientists to win the 2015 Nobel Prize for medicine. Her work of over 40 years was virtually unknown to the outside world until then, but her study of artemisinin medicinal compounds has saved the lives of millions. Moving from the lab to the community one can find role models who have broken role stereotypes. A few years ago President’s Malaria Initiative-funded Africa Indoor Residual Spraying (AIRS) project drew out attention to Maimouna Sanogo as a woman making a difference. She helped protect people in her country from malaria through her work as a supervisor on AIRS indoor residual spraying project in Mali. The AIRS project reported that, “As a woman in a leadership role, Maimouna is a trailblazer. In Mali, only 37% of women participate in the labor force, while participation is nearly double among Malian men (70%).”
Moving from the lab to the community one can find role models who have broken role stereotypes. A few years ago President’s Malaria Initiative-funded Africa Indoor Residual Spraying (AIRS) project drew out attention to Maimouna Sanogo as a woman making a difference. She helped protect people in her country from malaria through her work as a supervisor on AIRS indoor residual spraying project in Mali. The AIRS project reported that, “As a woman in a leadership role, Maimouna is a trailblazer. In Mali, only 37% of women participate in the labor force, while participation is nearly double among Malian men (70%).” Dr Rose Leke, Emeritus Professor of Immunology and Parasitology, Faculty of Medicine and Biomedical Sciences, University of Yaounde, Cameroon, was one of six people to be given the Kwame Nkrumah Scientific Award for Women in 2011. Dr Leke explained the challenges facing women, “Science is still a challenging field for women to enter, and even more so in which to progress. At the university, I have seen many promising young women finish their studies and start jobs as assistants only to either get stuck in that position indefinitely or eventually leave to take care of their families. There just wasn’t the mentorship or financial support for research needed for them to be able to progress. It was an issue I really took to heart.” Therefore, Dr Leke and colleagues started the HIGHER Women Consortium in Cameroon. We provided training and mentorship to young women researchers.
Dr Rose Leke, Emeritus Professor of Immunology and Parasitology, Faculty of Medicine and Biomedical Sciences, University of Yaounde, Cameroon, was one of six people to be given the Kwame Nkrumah Scientific Award for Women in 2011. Dr Leke explained the challenges facing women, “Science is still a challenging field for women to enter, and even more so in which to progress. At the university, I have seen many promising young women finish their studies and start jobs as assistants only to either get stuck in that position indefinitely or eventually leave to take care of their families. There just wasn’t the mentorship or financial support for research needed for them to be able to progress. It was an issue I really took to heart.” Therefore, Dr Leke and colleagues started the HIGHER Women Consortium in Cameroon. We provided training and mentorship to young women researchers. The time is ripe for a revitalization of the primary health care (PHC) movement. “Health for All through Primary Health Care” (HFA) was first envisioned at the 1978 International Conference on Primary Health Care (World Health Organization and UNICEF), and was enshrined in the Declaration of Alma-Ata. The HFA goal of bringing essential, affordable, scientifically sound, socially acceptable health care provided by health workers who are trained to work as a health team and who are responsive to the health needs of the community, guided by strong community engagement by the year 2000 but has not been fully met. Fortunately the vision of Alma-Ata has taken root, sprouted and flourished in a number of locations.
The time is ripe for a revitalization of the primary health care (PHC) movement. “Health for All through Primary Health Care” (HFA) was first envisioned at the 1978 International Conference on Primary Health Care (World Health Organization and UNICEF), and was enshrined in the Declaration of Alma-Ata. The HFA goal of bringing essential, affordable, scientifically sound, socially acceptable health care provided by health workers who are trained to work as a health team and who are responsive to the health needs of the community, guided by strong community engagement by the year 2000 but has not been fully met. Fortunately the vision of Alma-Ata has taken root, sprouted and flourished in a number of locations. Thanks to the vision and intellectual and political leadership of Dr. Tedros Adhanom Ghebreyesus, the then Minister of Health of Ethiopia and recently elected Director General of the World Health Organization, Ethiopia is an outstanding example of the Alma-Ata legacy. Access to PHC services was greatly expanded through the training of 40,000 Health Extension Workers (women from the local area with one year of training, each of whom serve 2,500 people and receive a government salary), recruitment of 3 million community female health volunteers (called the Health Development Army), and engagement with communities to enable them to take responsibility for improving their health.
Thanks to the vision and intellectual and political leadership of Dr. Tedros Adhanom Ghebreyesus, the then Minister of Health of Ethiopia and recently elected Director General of the World Health Organization, Ethiopia is an outstanding example of the Alma-Ata legacy. Access to PHC services was greatly expanded through the training of 40,000 Health Extension Workers (women from the local area with one year of training, each of whom serve 2,500 people and receive a government salary), recruitment of 3 million community female health volunteers (called the Health Development Army), and engagement with communities to enable them to take responsibility for improving their health. This expansion of PHC enabled Ethiopia to achieve its health-related MDGs. Child mortality (those younger than 5 years of age) declined from 166 deaths per 1,000 live births in 1990 to 67 in 2016 (MDG 4). Significant progress was achieved in reducing levels of childhood malnutrition (MDG 1). MDG 5 was almost reached, with a decline in maternal morality of 72%, versus the goal of 75%, and the percentage of mothers obtaining a delivery by a skilled provider increased 6-fold between 1995 and 2016. The prevalence rate of modern contraceptive use increased from 6% in 2000 to 35% in 2016. MDG 6 (for HIV, malaria and tuberculosis) was also reached. The number of new HIV infections declined by 90%, and the number of AIDS-related deaths by 53%. Between 1990 and 2015, the tuberculosis incidence and mortality rate declined by 48% and 72%, respectively. The malaria incidence rate declined by 50% and malaria mortality by 60%. Ethiopia’s PHC system is acknowledged as the major factor leading to these impressive health gains.
This expansion of PHC enabled Ethiopia to achieve its health-related MDGs. Child mortality (those younger than 5 years of age) declined from 166 deaths per 1,000 live births in 1990 to 67 in 2016 (MDG 4). Significant progress was achieved in reducing levels of childhood malnutrition (MDG 1). MDG 5 was almost reached, with a decline in maternal morality of 72%, versus the goal of 75%, and the percentage of mothers obtaining a delivery by a skilled provider increased 6-fold between 1995 and 2016. The prevalence rate of modern contraceptive use increased from 6% in 2000 to 35% in 2016. MDG 6 (for HIV, malaria and tuberculosis) was also reached. The number of new HIV infections declined by 90%, and the number of AIDS-related deaths by 53%. Between 1990 and 2015, the tuberculosis incidence and mortality rate declined by 48% and 72%, respectively. The malaria incidence rate declined by 50% and malaria mortality by 60%. Ethiopia’s PHC system is acknowledged as the major factor leading to these impressive health gains. Representatives from more than half of sub-Saharan Africa countries have come to Ethiopia to see its PHC system in action. Because of this interest, in 2016 the Federal Ministry of Health of Ethiopia established the International Institute for Primary Health Care – Ethiopia, with seed funding from the Bill & Melinda Gates Foundation and technical support from the Johns Hopkins Bloomberg School of Public Health. Our goal is for the Institute to become a global center of excellence for training, knowledge dissemination and research in primary health care, supported by multiple donors.
Representatives from more than half of sub-Saharan Africa countries have come to Ethiopia to see its PHC system in action. Because of this interest, in 2016 the Federal Ministry of Health of Ethiopia established the International Institute for Primary Health Care – Ethiopia, with seed funding from the Bill & Melinda Gates Foundation and technical support from the Johns Hopkins Bloomberg School of Public Health. Our goal is for the Institute to become a global center of excellence for training, knowledge dissemination and research in primary health care, supported by multiple donors. In the 1960s, the Brazilian government adopted a laissez-faire attitude, which lead to the predominance of private organizations in the provision of family planning services. Since then, Brazil has witnessed one of the most dramatic reductions in family size in modern history in part due to increased access to family planning services. (Photo New York Times: Members of the Union of Mothers of Angels.)
In the 1960s, the Brazilian government adopted a laissez-faire attitude, which lead to the predominance of private organizations in the provision of family planning services. Since then, Brazil has witnessed one of the most dramatic reductions in family size in modern history in part due to increased access to family planning services. (Photo New York Times: Members of the Union of Mothers of Angels.) As malaria control interventions are scaled up and sustained and malaria transmission levels decline and prevalence falls, an increasing number of countries are starting to see elimination on the horizon. For pregnant women, the antimalarial antibodies that have provided some level of protection in moderate to high malaria transmission settings are reduced as malaria transmission declines.
As malaria control interventions are scaled up and sustained and malaria transmission levels decline and prevalence falls, an increasing number of countries are starting to see elimination on the horizon. For pregnant women, the antimalarial antibodies that have provided some level of protection in moderate to high malaria transmission settings are reduced as malaria transmission declines.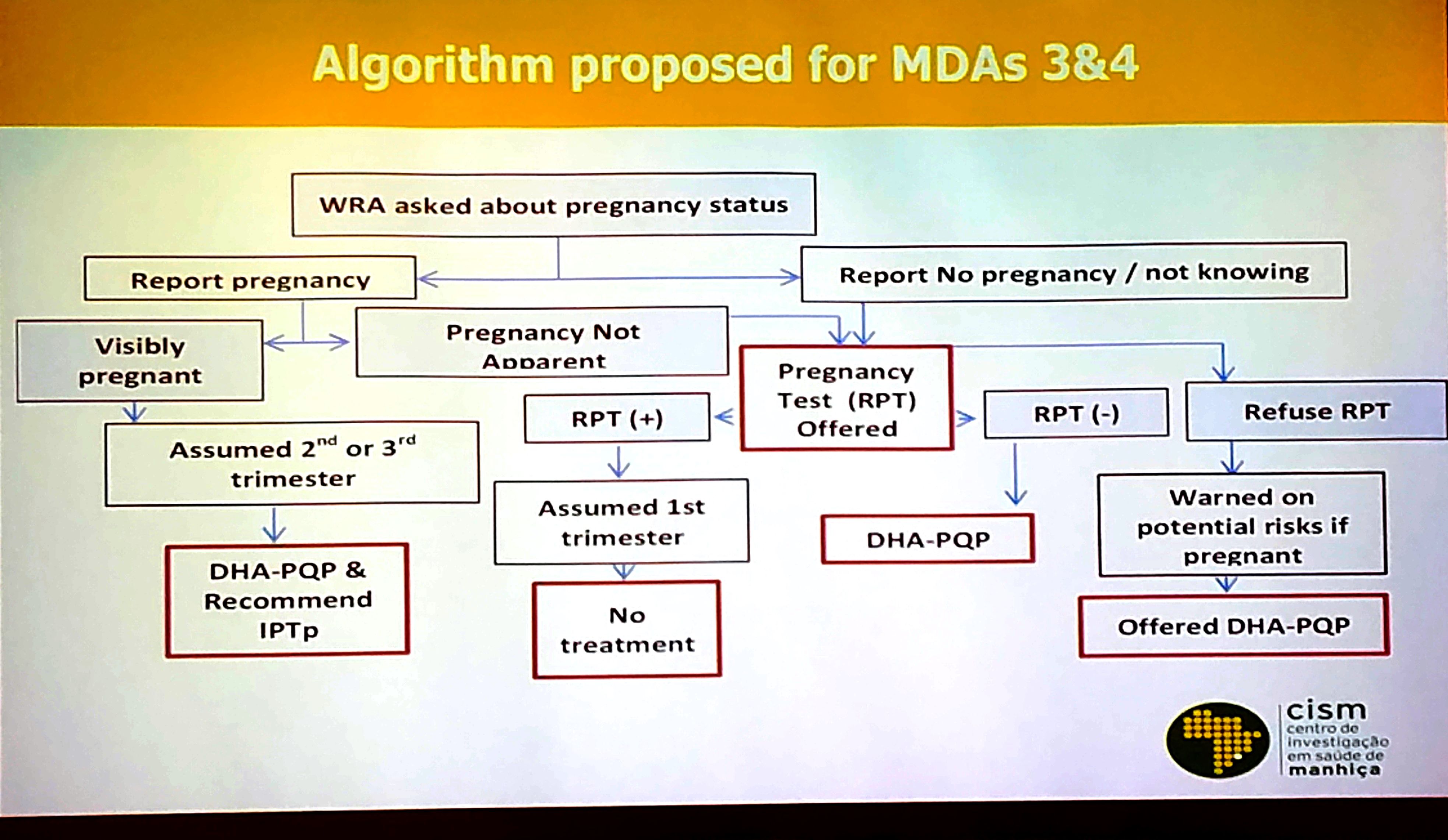




 International Women’s Day, represents an opportunity to celebrate the achievements of women all around the world. This year’s theme is “Empowering Women – Empowering Humanity: Picture it” envisions a world where each woman and girl can exercise her choices, such as participating in politics, getting an education or fighting malaria. Below is the second feature on women fighting malaria.
International Women’s Day, represents an opportunity to celebrate the achievements of women all around the world. This year’s theme is “Empowering Women – Empowering Humanity: Picture it” envisions a world where each woman and girl can exercise her choices, such as participating in politics, getting an education or fighting malaria. Below is the second feature on women fighting malaria.

 “It is a pleasure and an honour for me, to sign this engagement on behalf of AFEMS, to mobilize all our efforts to eliminate malaria in Senegal. We need to keep in mind that women are particularly vulnerable to this disease and that they can be change agents in their families for more efficient vector control in particular by promoting the systematic use of long lasting insecticide-treated mosquito nets for all their family members.”
“It is a pleasure and an honour for me, to sign this engagement on behalf of AFEMS, to mobilize all our efforts to eliminate malaria in Senegal. We need to keep in mind that women are particularly vulnerable to this disease and that they can be change agents in their families for more efficient vector control in particular by promoting the systematic use of long lasting insecticide-treated mosquito nets for all their family members.”