Capacity Building &Climate &Elimination &Malaria &Migration &PAHO &Refugee &Treatment &Urban Bill Brieger | 17 May 2025
Malaria in the Americas: Colombia and the Challenge of Refugees
Malaria is one of the more than 30 diseases and conditions included in the Elimination Initiative and targeted for elimination in the Region of the Americas by 2030. Colombia provides a useful example of the progress and challenges. Of the over 72,000 reported malaria cases in 2022, About 61% were caused by P. vivax, 38% by P. falciparum, and 1% were mixed. The Ministry of Health explains that unlike other South American countries, the most malaria endemic regions are not in the Amazonian forest but lie in the northwest of the country in the Pacific coastal forests, populated by Afro-Colombian and indigenous communities.

The Ministry also notes that malaria transmission is characterized by the presence of epidemic cycles that occur every 2 to 7 years, related to the occurrence of the Niño-Southern Oscillation phenomenon. Malaria control is particularly challenging in provinces where illegal mining, logging and the growing of illicit crops are conducted. The World Malaria Report of 2023 traced annual malaria trends in Colombia and showed a peak in 2018-19 with a reduction in subsequent years that points toward efforts at elimination
The International Rescue Committee identifies a particular challenge for Colombia. At least 4 million Venezuelans have crossed the border to seek refuge, and that number continues to rise. Venezuela continues to be plagued by malnutrition, lack of medical supplies, high homicide rates and the spread of diseases such as malaria and measles. Since outbreaks of measles, diphtheria and malaria have been reported across Venezuela, it would be surprising that refugees would enter Colombia with malaria infections.

A study of malaria among migrants in a university hospital in Colombia during 2018 found that imported malaria has increased in Colombia since 2015 and has been attributed to migrants coming from Venezuela. To address the challenge, we need to know where are the refugees? Regular migration is usually located in the main cities and in places where tourism or the mining industry are active. Many of the destinations are in areas where malaria is not endemic, onward transmission would be less likely. Unfortunately, the following migration destinations overlap with malaria transmission: Nariño, Antioquia, Cundinamarca, Cauca, and Chocó, such that those migrants can acquire new infections.
The challenge is that as Colombia makes progress toward eliminating malaria, it still must maintain high capacity to tackle imported cases as well as new cases among a particularly vulnerable refugee population.
Hepatitis &HIV &Training &Treatment Bill Brieger | 26 Aug 2024
Expanding Access to Hepatitis C Treatment in Tshwane, South Africa
On August 20, 2024, esaayman posted this blog about Hepatitis C in the class blog of the course, Social and Behavioral Foundations of Primary Health Care at the Johns Hopkins Bloomberg School of Public Health.
Hepatitis C remains a significant public health burden in South Africa, disproportionately affecting people who inject drugs, with the highest prevalences, monitored by the South African Community Epidemiological Network on Drug Use and the National Institute for Communicable Diseases, ranging from 68% to 94% in Tshwane. Despite national guidelines and an action plan for viral hepatitis recommending direct acting antiviral therapy and point-of-care technology use for hepatitis c management in people who inject drugs since 2019, with treatment registration by SAHPRA since 2020, access remains limited. The essential medicines list restricts treatment to tertiary level liver clinics. These clinics are often inaccessible to people who inject drugs due stigma, and stringent abstinence-based criteria for treatment.
 Community hepatitis C screening at Sediba Hope Medical Centre (Source: SHMC, 2024)
Community hepatitis C screening at Sediba Hope Medical Centre (Source: SHMC, 2024)
While community-based HIV-focused harm reduction services, such as opioid agonist therapy, exist, they are primarily managed by donor-funded civil society organizations, with limited integration into public healthcare systems. The City of Tshwane’s health department in partnership with the University of Pretoria initiated opioid agonist therapy services at primary care level in 2016, however with limited resources allocated, hepatitis c screening and treatment remains sporadic. A local pilot study, offered by Sediba Hope Medical Centre, a public-private partnership-based clinic for marginalized communities, has demonstrated successful community-based hepatitis c treatment integration, signalling for sustained access to care at the appropriate level.
 HIV and viral hepatitis prevalence in South Africa (Source: INHSU, 2021)
HIV and viral hepatitis prevalence in South Africa (Source: INHSU, 2021)
Improved access to treatment within the city would require purposeful implementation of hepatitis c treatment guidelines alongside best practices from harm reduction guidelines and national action plans. This includes training of primary care providers to manage uncomplicated cases, further supported by specialist through existing mentoring platforms. To strengthen clear referral pathways, collaboration between liver clinics and community-based harm reduction and primary care facilities is required, building on the use of existing inter-facility referral applications and decentralized medication delivery options. Additionally, dedicated funds for adequate diagnostic tools, care coordination staff, and medication procurement should be considered on a national level, with the same urgency as with the HIV response. By implementing these strategies, Tshwane can expand access to hepatitis c treatment for people who inject drugs, thereby aiming to become the first South African city to achieve micro-elimination, averting adverse health outcomes for people who inject drugs. Implementation strategies and outcomes should be documented to inform increased treatment coverage nationally, further advocating for the consideration of direct acting antivirals for inclusion in the primary care essential medicines list.
Children &COVID-19 &Diagnosis &IPTp &ITNs &Malaria in Pregnancy &Treatment Bill Brieger | 06 Oct 2022
2021 DHS and MIS Findings from Six Malaria Endemic Countries
The Demographic and Health Survey Program has released final and summary reports for both DHS and Malaria Indicator Surveys (MIS) for 2021 from several malaria endemic African countries. Below is a brief summary of some of the findings from Madagascar, Nigeria, Burkina Faso, Mali, Côte d’Ivoire, and Senegal. Click the link on each country to download a copy for yourself.
The proportion of the population who slept under an insecticide treated bednet the night before the survey varied. In Madagascar it was 49%, While in Nigeria it was 59%. Mali achieved the highest coverage at 73%, while Burkina Faso had the lowest previous night coverage at 41%.
 Senegal showed a worrying decrease from 63% in 2016 to 46% in 2021. Côte d’Ivoire did not report total household use, but indicated that 72% of homes had at least one net, with 58% of children below 5 years of age and 64% of pregnant women sleeping under them.
Senegal showed a worrying decrease from 63% in 2016 to 46% in 2021. Côte d’Ivoire did not report total household use, but indicated that 72% of homes had at least one net, with 58% of children below 5 years of age and 64% of pregnant women sleeping under them.
At least three doses of sulfadoxine-pyremethamine is recommended for Intermittent preventive treatment of malaria in pregnant women. The national average was 38% for at least 3 doses in Senegal, although ironically 92% had been reached with the first dose. In Mali only 35% received at least a third dose. Burkina Faso started out with 92% for the first dose, but reached 57% with three or more. Côte d’Ivoire started with 80% receiving their first dose and concluded with only 35% receiving a third. Both Madagascar and Nigeria had the lowest 3-dose coverage at 31%.
Malaria testing and treatment using rapid diagnostic tests and artemisinin-based combination therapy (ACT) was reported. Nigeria demonstrates the challenges of following guidelines. Although 63% of children under 5 years of age were reported to have had a fever in the two weeks preceding the survey, only 24% of those received a diagnostic test. The summary results report that 74% of those with fever “who took any anti-malaria medicine” used the recommended ACT. The implication is that many received medicine without confirmatory testing such that some may have gotten ACT who needed another medicine and some who actually had malaria may have missed the correct treatment.
 A similar low level of testing was seen in Senegal (22%), Mali (23%), and Madagascar (20%). Côte d’Ivoire reported 38% of febrile children having been tested. Burkina Faso performed better for testing with 65%.
A similar low level of testing was seen in Senegal (22%), Mali (23%), and Madagascar (20%). Côte d’Ivoire reported 38% of febrile children having been tested. Burkina Faso performed better for testing with 65%.
These brief findings indicate that implementation of Malaria interventions are far from ideal. We know that some of the blame can be placed on health service disruptions due to demands of COVID-19 activities by health ministries and partners. Still, with 8 years remaining until 2030, Reinvigorated efforts are needed in all endemic countries if these six examples are indicative of the challenges we face.
Community &Diagnosis &Guidelines &Health Workers &IPTp &Malaria in Pregnancy &Monitoring &Treatment Bill Brieger | 02 Nov 2021
Updating Malaria Guidelines and Tools: The Kenya Example
 Kenya Division of National Malaria Program (DNMP) with support from PMI Impact Malaria (IM) and in collaboration with other stakeholders reviewed/developed/updated nine key program documents. Agustine Ngindu and the Impact Malaria/PMI team stress the importance of keeping key malaria technical guidance and tools up-to-date.
Kenya Division of National Malaria Program (DNMP) with support from PMI Impact Malaria (IM) and in collaboration with other stakeholders reviewed/developed/updated nine key program documents. Agustine Ngindu and the Impact Malaria/PMI team stress the importance of keeping key malaria technical guidance and tools up-to-date.
 Guidelines for the Diagnosis, Treatment, and Prevention of Malaria in Kenya was revised to indicate the start of IPTp at 13 weeks from the prior recommendation of 16 weeks of gestation and updated the IPTp schedule in line with WHO guidance. The program also updated dosing charts for artemether lumefantrine, dihydroartemisinin-piperaquine, and injectable artesunate to include both weight and age range particulars. This update will enhance adherence to treatment guidelines among healthcare workers
Guidelines for the Diagnosis, Treatment, and Prevention of Malaria in Kenya was revised to indicate the start of IPTp at 13 weeks from the prior recommendation of 16 weeks of gestation and updated the IPTp schedule in line with WHO guidance. The program also updated dosing charts for artemether lumefantrine, dihydroartemisinin-piperaquine, and injectable artesunate to include both weight and age range particulars. This update will enhance adherence to treatment guidelines among healthcare workers
 The Kenya Quality Assurance Guidelines for Parasitological Diagnosis of Malaria was in draft form for nearly 10 years. Revisions were motivated by the lack of a functional quality assurance (QA)/quality control (QC) system for malaria diagnosis. Sections were added to guide implementation of internal quality control and external quality assurance programs. Updates also provided guidance on surveys to determine the extent of gene deletion and its effect on routine RDT-based malaria diagnosis.
The Kenya Quality Assurance Guidelines for Parasitological Diagnosis of Malaria was in draft form for nearly 10 years. Revisions were motivated by the lack of a functional quality assurance (QA)/quality control (QC) system for malaria diagnosis. Sections were added to guide implementation of internal quality control and external quality assurance programs. Updates also provided guidance on surveys to determine the extent of gene deletion and its effect on routine RDT-based malaria diagnosis.
 Implementation Framework for Malaria Rapid Diagnostic Tests was developed to facilitate rollout of malaria diagnostics QA/QC in line with Kenya Malaria Strategy (KMS) of 2019-2023. As p[art of this effort, the M&E framework was expanded to include the performance matrix. A costed implementation matrix to provide guidance was developed on costing of activities in line with KMS 2019-2023.
Implementation Framework for Malaria Rapid Diagnostic Tests was developed to facilitate rollout of malaria diagnostics QA/QC in line with Kenya Malaria Strategy (KMS) of 2019-2023. As p[art of this effort, the M&E framework was expanded to include the performance matrix. A costed implementation matrix to provide guidance was developed on costing of activities in line with KMS 2019-2023.
 Biosafety Guidelines for Malaria Rapid Diagnostic Testing at Community Level was highlighted in new guidelines developed to address emerging QA and biosafety concerns at community level. This was a response to requirements by the Kenya Medical Laboratory Technicians and Technologists Board to allow for a new waiver for community health volunteers (CHVs) to conduct testing using mRDTs.
Biosafety Guidelines for Malaria Rapid Diagnostic Testing at Community Level was highlighted in new guidelines developed to address emerging QA and biosafety concerns at community level. This was a response to requirements by the Kenya Medical Laboratory Technicians and Technologists Board to allow for a new waiver for community health volunteers (CHVs) to conduct testing using mRDTs.
 The Guidelines on Community Case Management of malaria and its implementation plan were strengthened as was the Implementation framework for Rapid Diagnostic Testing. Updated job aids included dosing schedules for artemether lumefantrine (AL) and injectable artesunate for use at service delivery points by Health Care Workers in line with the revised guidelines.
The Guidelines on Community Case Management of malaria and its implementation plan were strengthened as was the Implementation framework for Rapid Diagnostic Testing. Updated job aids included dosing schedules for artemether lumefantrine (AL) and injectable artesunate for use at service delivery points by Health Care Workers in line with the revised guidelines.
 Hopefully all national malaria programs will take the Kenya experience as an example of the need to update regularly all the tools needed for front line staff to achieve malaria elimination.
Hopefully all national malaria programs will take the Kenya experience as an example of the need to update regularly all the tools needed for front line staff to achieve malaria elimination.
Elimination &Eradication &Health Systems &Helminths/Worms &ITNs &Journalists/Media &Leishmaniasis &NGOs &Nigeria &NTDs &Partnership &Repellent &Research &Schistosomiasis &Technical Assistance &Treatment Bill Brieger | 29 Sep 2020
Malaria News Today 2020-09-28/29: media involvement, NGOs, monitoring and research
A variety of malaria and related issues have arisen over the past two days. A media coalition for malaria elimination formed in Ghana. A Nigerian NGO stresses the importance of addressing malaria on Nigeria’s 60th Independence Day (October 1). An innovative technology foundation is supporting various malaria and NTD treatment and diagnostic research efforts. Click on links below to read the details.
Media Coalition for malaria control and elimination launched
A Media Coalition comprising of selected journalists and editors, has been launched in Ghana under the umbrella of the “Zero Malaria Starts with Me” campaign to eliminate malaria by 2030. The Coalition, which aimed to enhance the quality and quantity of malaria coverage, and support broader advocacy efforts, was launched at a workshop in Accra organized by the National Malaria Control Programme (NMCP), in collaboration with the African Media and Malaria Research Network and Speak Up Africa, an advocacy and communication Organisation based in Senegal.
The workshop brought together media personnel from across the regions, who nominated their Regional Executives, with two National Co-Chairpersons coming from Greater Accra. The Members of the Coalition, made a firm declaration of their commitment towards the elimination of malaria in Ghana by the year 2030, by championing the fight, taking responsibility for their roles through proactive, regular, accurate, and high-quality media output of news on malaria.
Chinwe Chibuike Foundation Set To Flag-off Full Scale Malaria Eradication Program On Independence Day
![]() A Nigeria indigenous and international non-governmental organization, envisioned to create a conducive environment towards the accessibility of healthcare facilities and improved educational opportunities, has joined the fight against the bizzare challenges of Malaria. The renowned Nigeria-USA humanitarian organization, Chinwe Chibuike Foundation is collaborating with other organizations to flagoff a full scale malaria eradication exercise tagged “Nigeria at 60 Malaria Eradication Project”, on the 1st of October 2020.
A Nigeria indigenous and international non-governmental organization, envisioned to create a conducive environment towards the accessibility of healthcare facilities and improved educational opportunities, has joined the fight against the bizzare challenges of Malaria. The renowned Nigeria-USA humanitarian organization, Chinwe Chibuike Foundation is collaborating with other organizations to flagoff a full scale malaria eradication exercise tagged “Nigeria at 60 Malaria Eradication Project”, on the 1st of October 2020.
According to the founder and President of Chinwe Chibuike Foundation, Ms Gloria Chibuike, during an interview session with Pulse TV few days ago, she noted the forthcoming Nigeria At 60 Malaria Eradication Program will be different and of more impact, especially with the full scale approach and introduction a new Malaria repellant Band.
While emphasizing on the extensive features of the project, Ms Gloria described Malaria as one of the biggest problems in Africa at the moment, considering the increased number of recorded deaths and infection. She narrated that the discovery of the new malaria repellent band was timely and off-course very efficient, especially with testimonies from few persons who have already tried the brand.
Drugs and Diagnostics: Malaria and NTDs
The Global Health Innovative Technology (GHIT) Fund announced today a total of 1.37 billion yen (US$13 million*) to invest in seven partnerships to develop new lifesaving drugs and diagnostics for malaria, Buruli ulcer, Chagas disease, leishmaniasis, schistosomiasis, and soil-transmitted helminths (STH). This includes three newly funded projects and four that will receive continued funding. The RBM Partnership is planning on how to monitor and provide technical support for ITN programs. Click the links within each section to read details.
As of September 29, GHIT’s portfolio includes 50 ongoing projects: 26 discovery projects, 16 preclinical projects and eight clinical trials (Appendix 3). The total amount of investments since 2013 is 22.3 billion yen (US$211 million).
Support the Improvement of Operational Efficiency of ITN Campaigns
The Alliance for Malaria Prevention (AMP) is a workstream within the RBM Partnership to End Malaria. With malaria indicators stagnating and intense pressure to improve access and use of effective ITNs, WHO has renewed focus on stratifying vector control strategies in countries. Along with the introduction of new, more expensive ITNs, countries are now challenged to determine where they should deploy different ITN types to manage insecticide resistance within limited funding envelopes, as well as to identify more efficient ways to implement mass ITN distribution.
 Countries that have accessed AMP technical assistance have significantly improved their capacity to modify and update strategies and tools to increase ITN access, use and accountability. They have also continued to identify further gaps and look for effective ways to address them. Now AMP planning to support update and finalization of ITN tracking tool, aligned with priorities across major partners (GF, PMI, RBM).
Countries that have accessed AMP technical assistance have significantly improved their capacity to modify and update strategies and tools to increase ITN access, use and accountability. They have also continued to identify further gaps and look for effective ways to address them. Now AMP planning to support update and finalization of ITN tracking tool, aligned with priorities across major partners (GF, PMI, RBM).
Artesunate &Referral &Treatment Bill Brieger | 25 Nov 2019
Reduction in malaria-attributable deaths following a rectal artesunate pre-referral treatment pilot in Burkina Faso, 2018
 Ousmane Badolo,* Stanislas Nébié, Youssouf Sawadogo, Thierry Ouedraogo, Bonkoungou Moumouni, Mathurin Dodo, Lolade Oseni, Gladys Teteh, and William Brieger, presented a poster entitled, “Reduction in malaria-attributable deaths following a rectal artesunate pre-referral treatment pilot in Burkina Faso, 2018,” at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Ousmane Badolo,* Stanislas Nébié, Youssouf Sawadogo, Thierry Ouedraogo, Bonkoungou Moumouni, Mathurin Dodo, Lolade Oseni, Gladys Teteh, and William Brieger, presented a poster entitled, “Reduction in malaria-attributable deaths following a rectal artesunate pre-referral treatment pilot in Burkina Faso, 2018,” at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
 Background: In 2017, 4.32 percent of malaria cases were documented as severe malaria in Burkina Faso. The National Case Management Guidelines (August 2017) recommends that the First line treatment for severe malaria be injectable artesunate except in pregnancy where injectable quinine is used for the 1st trimester and injectable artesunate used for the 2nd and 3rd trimesters.
Background: In 2017, 4.32 percent of malaria cases were documented as severe malaria in Burkina Faso. The National Case Management Guidelines (August 2017) recommends that the First line treatment for severe malaria be injectable artesunate except in pregnancy where injectable quinine is used for the 1st trimester and injectable artesunate used for the 2nd and 3rd trimesters.
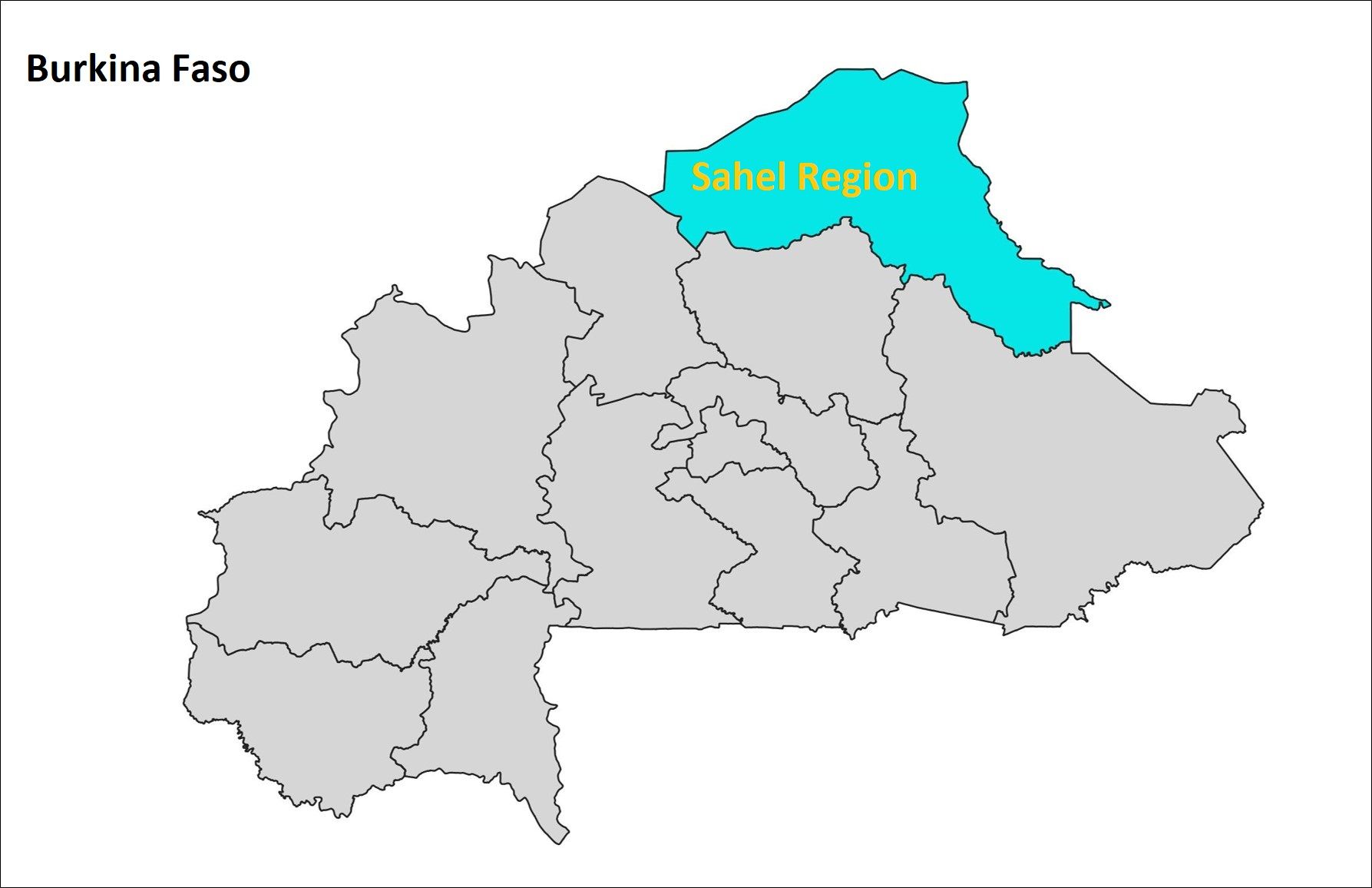
The guidelines recommend pre-referral treatment of severe disease at peripheral health facilities using rectal artesunate for children under 5, parenteral artesunate, artemether, or quinine for older children and adults. The guidelines also recommend pre-referral 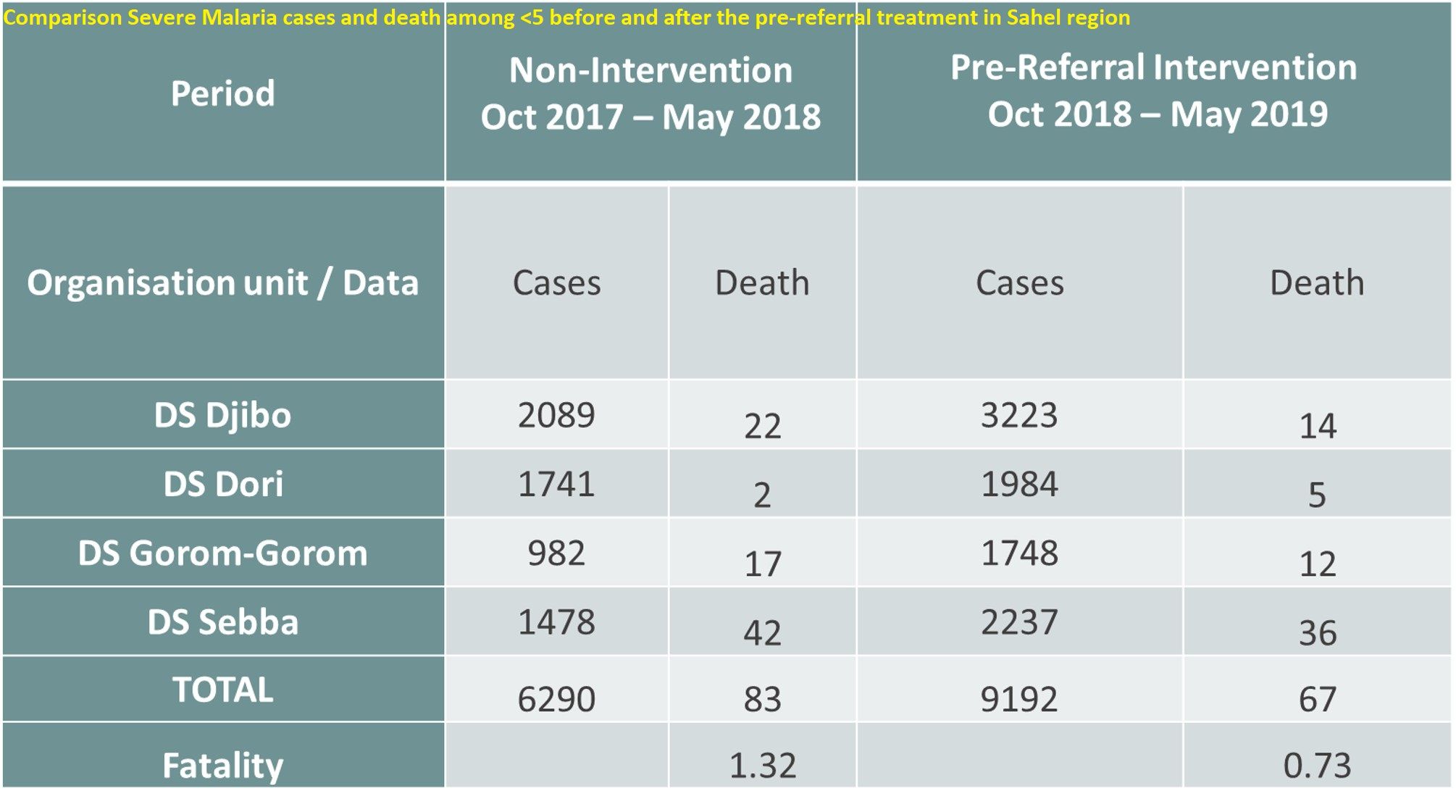 treatment of severe disease by community health workers with rectal artesunate for children under 5 only. The National Malaria Control Program is currently piloting pre-referral rectal artesunate for children under five years of age by CHWs in three districts in North and Sahel regions, where malaria mortality is the highest.
treatment of severe disease by community health workers with rectal artesunate for children under 5 only. The National Malaria Control Program is currently piloting pre-referral rectal artesunate for children under five years of age by CHWs in three districts in North and Sahel regions, where malaria mortality is the highest.
Results: Comparison Severe Malaria cases and death among <5 before and after the pre-referral treatment in Sahel region is seen in the Table. Pre-referral treatment was able to  reduce fatality by 45%.
reduce fatality by 45%.
Comparison of monthly fatality of severe malaria among <5 year (October 16 to April 17; October 17 to April 18 and October 18 to April 19) in the Sahel region is seen in the Graph. This shows a substantial decline in severe malaria following introduction ofthe pre-referral rectal artesunate pilot.
Several Lessons were Learned based on the Encouraging preliminary results. The involvement of the community in health activities allows good visibility of the intervention resulting in good acceptability and adherence. The community can take charge of its own health if it is well supervised. Good functionality of the “canary fridge” device when used in hot areas. Ability to use other meeting and supervisory opportunities to implement the strategy. Challenges identified can be corrected by close monitoring.
 Insecurity in Northern Burkina Faso is a major constraint, but pre-referral treatment of severe malaria is needed to decrease mortality from malaria. Despite implementation difficulties, this experience has contributed to a reduction in deaths due to severe malaria in the Sahel region, which is also facing increasing insecurity.
Insecurity in Northern Burkina Faso is a major constraint, but pre-referral treatment of severe malaria is needed to decrease mortality from malaria. Despite implementation difficulties, this experience has contributed to a reduction in deaths due to severe malaria in the Sahel region, which is also facing increasing insecurity.
An evaluation of the implementation with data collection for a one-year implementation period will provide lessons for the national scale up of pre-referral artesunate implementation.
*Affiliations: PMI Improving Malaria Care Project, Jhpiego Baltimore, MD, United States, Johns Hopkins University, Baltimore, MD, United States
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID) under Cooperative Agreement No. AID-624-A-13-00010 and the President’s Malaria Initiative (PMI). The contents are the responsibility of the authors and do not necessarily reflect the views of USAID, PMI or the United States Government.
Children &Equity &IPTp &ITNs &Nigeria &Treatment Bill Brieger | 02 Jul 2019
Nigeria’s 2018 Demographic and Health Survey: Malaria Situation
 The Demographic and Health Survey for 2018 in Nigeria has released preliminary findings. These cover insecticide Treated Nets (ITNs), Intermittent Preventive Treatment of malaria in pregnancy (IPTp), and treatment of children with Artemisinin-Based Combination Therapy (ACT).
The Demographic and Health Survey for 2018 in Nigeria has released preliminary findings. These cover insecticide Treated Nets (ITNs), Intermittent Preventive Treatment of malaria in pregnancy (IPTp), and treatment of children with Artemisinin-Based Combination Therapy (ACT).
The key findings have been converted into graphs. We can see that ITN ownership by a household (HH) is greater in rural areas, but overall reaches only a national average of 60% of households having at least one net. People may recall that the 2010 target by the Roll Back malaria Partnership was 80% for all key indicators with the hope that by attaining and then maintaining 80% coverage or more, malaria incidence would drop and elimination would be on the horizon.
Nigeria is not among WHO’s Elimination by 2020 (E2020) countries, and it is not clear when transmission will move i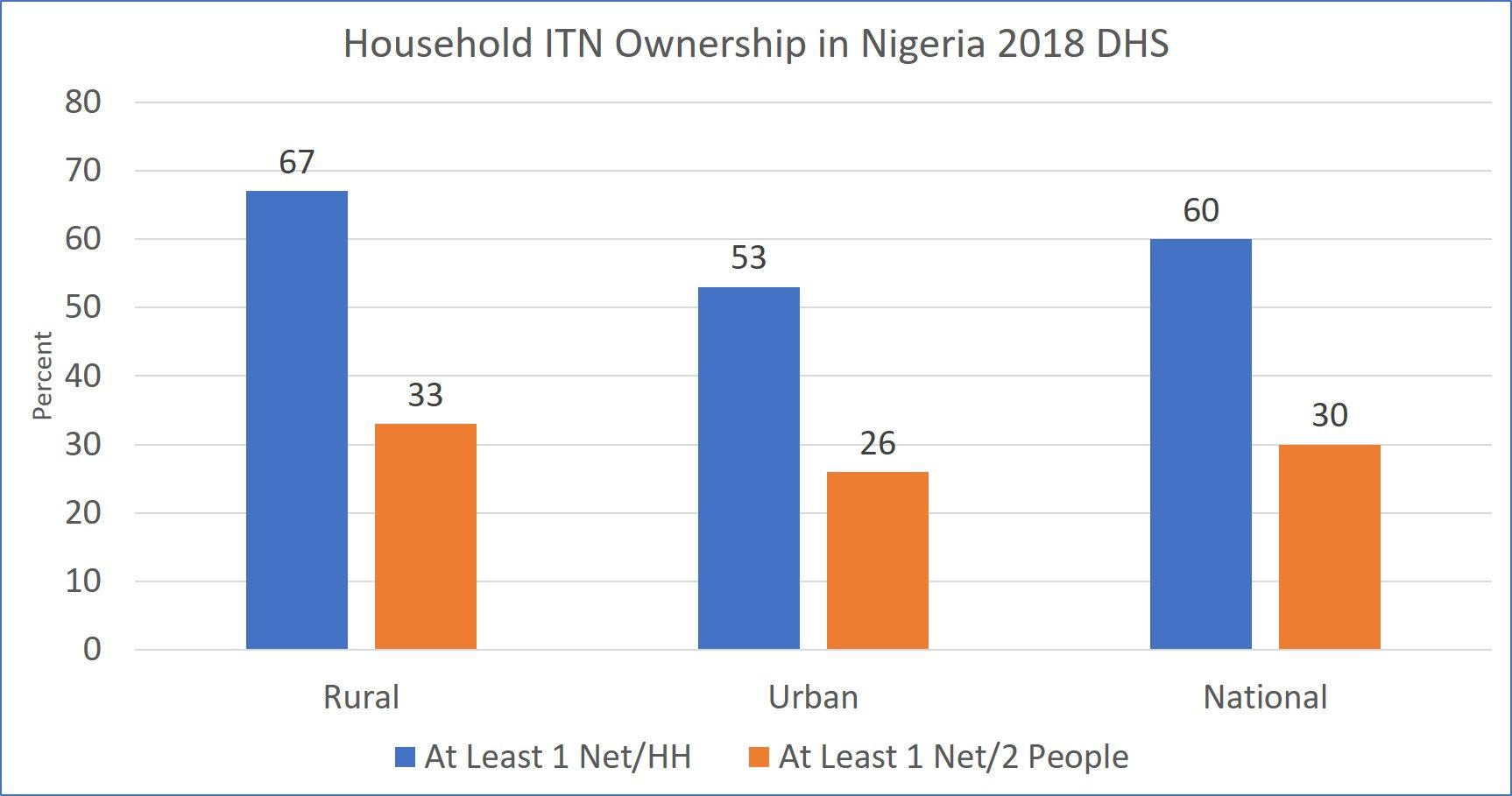 n that direction when key interventions are still not reaching targets. This is due also to the fact that 60% of households covered does not mean that residents are protected. In fact only 30% meet the goal of universal net coverage with at least one net for every two household members.
n that direction when key interventions are still not reaching targets. This is due also to the fact that 60% of households covered does not mean that residents are protected. In fact only 30% meet the goal of universal net coverage with at least one net for every two household members.
On the positive side, comparison of household net ownership and we alth status appears to favor the poorer households. 72% of the poorest households have at least one net compared to 48% of the highest income quintile. Unfortunately the gap between rich and poor narrows when it comes to the target of 1 net for 2 people.
alth status appears to favor the poorer households. 72% of the poorest households have at least one net compared to 48% of the highest income quintile. Unfortunately the gap between rich and poor narrows when it comes to the target of 1 net for 2 people.
Although these days we stress universal coverage of all household members, DHS still collects data on what are often termed ‘vulnerable’ groups, children below the age of 5 years and pregnant women. Just over half of each group slept under an ITN the night before the survey. It is obvious that access plays a role, so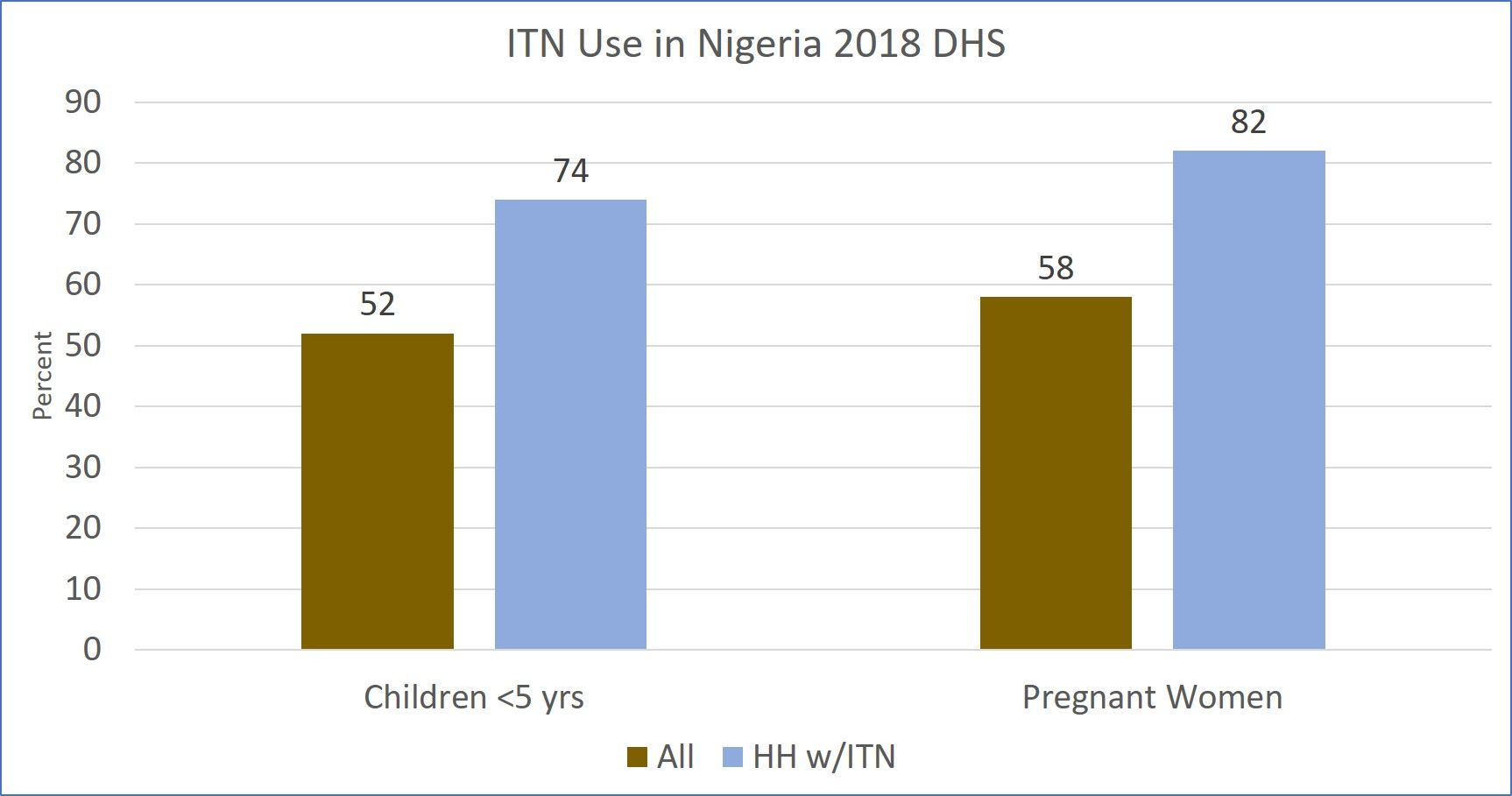 in those households that actually own at least one net 74% of children and 82% of pregnant women slept under an ITN. These figures might even be higher if the target of 1 net per two people were met.
in those households that actually own at least one net 74% of children and 82% of pregnant women slept under an ITN. These figures might even be higher if the target of 1 net per two people were met.
Nigeria is a huge and diverse country in terms of geography, epidemiology and ethncity. The country has 6 regions that are used for planning and analysis pur poses. The map attached shows that there are major regional variations in households owning at least one net and households having at least one net for every 2 people residing there.
poses. The map attached shows that there are major regional variations in households owning at least one net and households having at least one net for every 2 people residing there.
There is better coverage of at least one net per household in the northern zones than the southern, with the Northwest achieving 86% and then 42% for covering two people with one net. When it comes to that latter measure, the remaining 5 regions are all in the 20% level, meaning that for most of the country, there is a long way to go to achieve universal net coverage.
 Intermittent preventive treatment of pregnant women with sulphadoxine-pyrimethamine (SP) has been a long standing intervention to protect women and their unborn children from the devastating effects of malaria. For at least six years now, WHO has recommended that pregnant women take three or more monthly doses of IPTp from the 13th week of pregnancy, onward.
Intermittent preventive treatment of pregnant women with sulphadoxine-pyrimethamine (SP) has been a long standing intervention to protect women and their unborn children from the devastating effects of malaria. For at least six years now, WHO has recommended that pregnant women take three or more monthly doses of IPTp from the 13th week of pregnancy, onward.
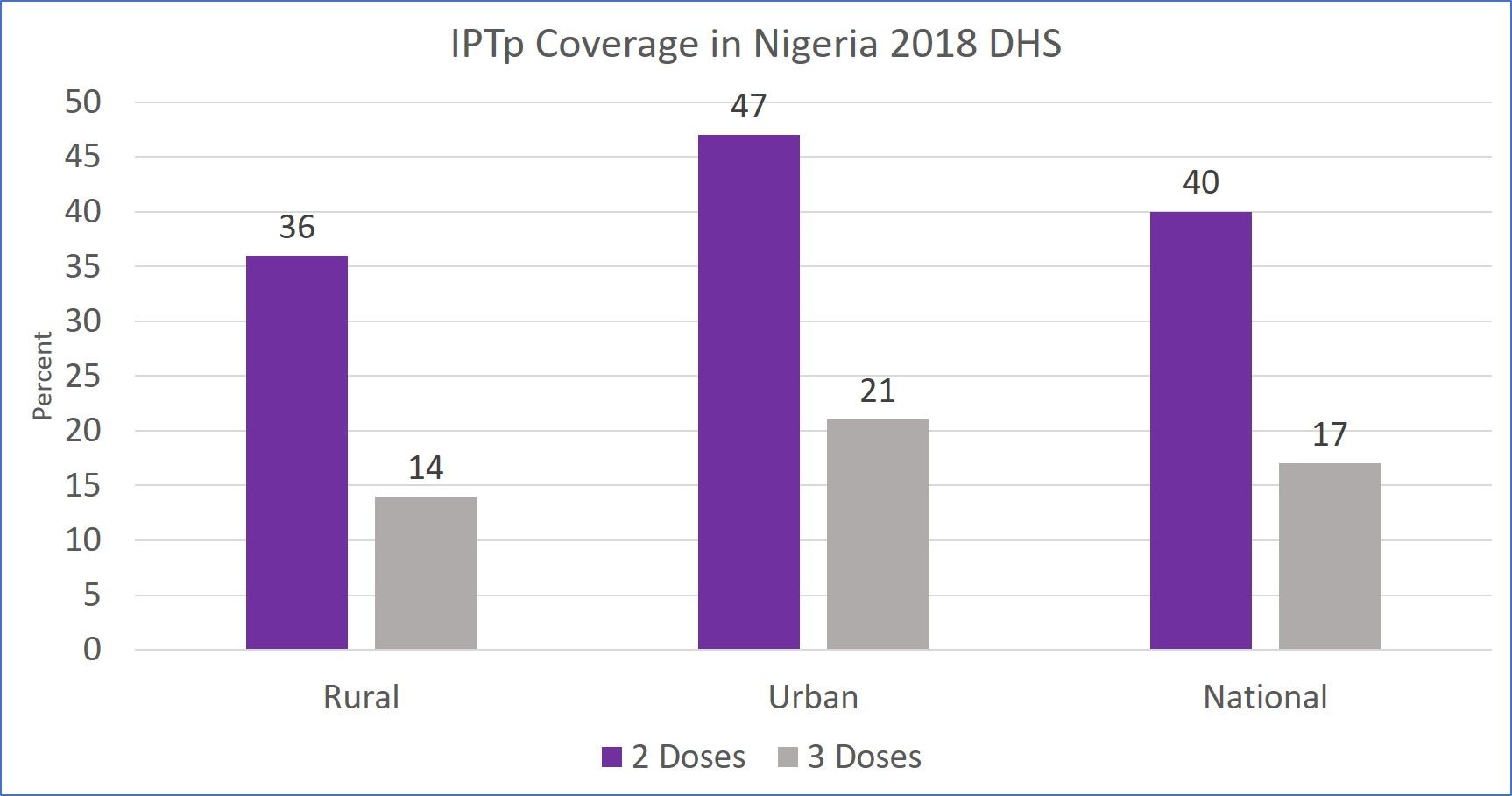
A challenge to getting IPTp is contact with antenatal care services, and only 67% of women who delivered a child in the 5 year preceding the survey attended ANC even once. Not surprisingly, only 40% of those pregnant women received two doses of IPTp and only 17% got three doses.
Finally, only 28% of children with fever in the two weeks prior to the survey took ACT, although we are not certain about the proportion who had been tested. It is difficult to interpret this finding since we do not know what proportion of those with fever might have been tested and found to harbor malaria parasites. ACTs should only be given to those with positive parasitological tests.
DHS and its sister survey, the Malaria Indicator Survey are performed at approximately three-year intervals. These data sources are valuable for evaluating past interventions and planning new. Clearly some serious planning is needed to address the shortfalls in malaria intervention coverage and save more lives.
Diagnosis &Essential Medicines &IPTi &Malaria in Pregnancy &Seasonal Malaria Chemoprevention &Treatment &Zero Malaria Bill Brieger | 25 Apr 2019
Zero Malaria Starts with Universal Coverage: Part 2 Preventive and Curative Treatments
April hosts several important global health days or observances. On World Health Day 2019 WHO stressed that, “Universal health coverage (UHC) is WHO’s number one goal. Key to achieving it is ensuring that everyone can obtain the care they need, when they need it, right in the heart of the community.” Nationwide monitoring through the Demographic and Health Surveys (DHS), the Malaria Indicator Surveys (MIS) and the Multi-Indicator Cluster Surveys (MICS) can document the status of appropriate malaria treatment and intermittent preventive treatment in pregnant women (IPTp).
 Definitions of indicators have evolved for treatment-related malaria interventions. When Intermittent Preventive Treatment for pregnant women (IPTp) began in the early 2000s, the recommended dosing was twice during pregnancy after the first trimester one month apart in high and/or stable transmission areas. Due to lessening efficacy of sulfadoxine-pyrimethamine (SP), the dosage recommendation has changed to at least three times, still a month apart from the beginning of the second trimester.
Definitions of indicators have evolved for treatment-related malaria interventions. When Intermittent Preventive Treatment for pregnant women (IPTp) began in the early 2000s, the recommended dosing was twice during pregnancy after the first trimester one month apart in high and/or stable transmission areas. Due to lessening efficacy of sulfadoxine-pyrimethamine (SP), the dosage recommendation has changed to at least three times, still a month apart from the beginning of the second trimester.
This updated policy was broadcast widely between 2012 and 2013, but it took countries some time to build capacity and scale up for the expanded coverage goals. UNICEF Data5 again show that between 2014 and 2017 coverage was far below either 80% of pregnant women, let alone reaching them universally (Figure 2). Most countries achieved 30% or less coverage. Zambia at 50% was the highest. Low coverage leaves both pregnant women and the unborn child at risk for anemia and death in the former and low birth weight, still birth or miscarriage for the latter. The World Malaria Report of 2018 estimates that three doses of IPTp were received by only 22% of pregnant women in the target countries in 2017.
The concept of IPT was investigated for infants and children during by a consortium of researchers in several African Countries. It was found that IPTi with SP could have a positive effect on preventing malaria. To operationalize this concept, the World Health Organization developed what is known as Seasonal Malaria Chemoprevention (SMC) that would be delivered in the Sahel region of West Africa where malaria transmission itself is seasonal and where there are some countries with very low transmission with implications for malaria elimination.
 The SMC delivery process was not linked to immunization but provided by community health workers and volunteers. SP and Amodiaquine (SP-AQ) were used in combination and provided monthly, three or four times during the rainy/high transmission season. Coverage was targeted at children below school age. It is only recently that SMC has been scaled up to reach all eligible countries or states and regions within designated countries.
The SMC delivery process was not linked to immunization but provided by community health workers and volunteers. SP and Amodiaquine (SP-AQ) were used in combination and provided monthly, three or four times during the rainy/high transmission season. Coverage was targeted at children below school age. It is only recently that SMC has been scaled up to reach all eligible countries or states and regions within designated countries.
WHO states that SMC focuses on, “children aged 3–59 months (and) reduces the incidence of clinical attacks and severe malaria by about 75%.” In some countries the coverage is extended to primary school aged children, making comparisons and calculations of coverage (universal por otherwise) challenging.
 The World Malaria Report of 2018 notes that, “In 2017, 15.7 million children in 12 countries in Africa’s Sahel subregion were protected through seasonal malaria chemoprevention (SMC) programs. However, about 13.6 million children who could have benefited from this intervention were not covered, mainly due to a lack of funding.” This implies that 54% of eligible children were reached. Coverage of SMC can refer to receiving any of the doses or as having received all the monthly doses offered by a nation’s malaria control program. Specifically, the World Malaria Report 2018 drew on surveys in 7 countries that provided 4 monthly doses to determine that 53% of children received all doses.
The World Malaria Report of 2018 notes that, “In 2017, 15.7 million children in 12 countries in Africa’s Sahel subregion were protected through seasonal malaria chemoprevention (SMC) programs. However, about 13.6 million children who could have benefited from this intervention were not covered, mainly due to a lack of funding.” This implies that 54% of eligible children were reached. Coverage of SMC can refer to receiving any of the doses or as having received all the monthly doses offered by a nation’s malaria control program. Specifically, the World Malaria Report 2018 drew on surveys in 7 countries that provided 4 monthly doses to determine that 53% of children received all doses.
 Determining coverage for malaria treatment for sick people is not as straightforward as finding out the numbers who slept under an ITN or swallowed IPTp doses, and even those are not simple. As defined, correct treatment first consists of parasitological diagnosis, which at the primary care level could be by microscopy or rapid diagnostic test (RDT). The next issue is treating only those with positive tests. Finally, the treatment must consist of age- or weight-specific doses of an approved artemisinin-based combination therapy (ACT) drug. Very few clinic records or surveys document whether the treatment given is ‘correct’ by these standards.
Determining coverage for malaria treatment for sick people is not as straightforward as finding out the numbers who slept under an ITN or swallowed IPTp doses, and even those are not simple. As defined, correct treatment first consists of parasitological diagnosis, which at the primary care level could be by microscopy or rapid diagnostic test (RDT). The next issue is treating only those with positive tests. Finally, the treatment must consist of age- or weight-specific doses of an approved artemisinin-based combination therapy (ACT) drug. Very few clinic records or surveys document whether the treatment given is ‘correct’ by these standards.
WHO addresses the need for achieving universal access to malaria diagnostic testing and notes this will not be easy. They provide a successful example of Senegal, where following the introduction of malaria RDTs in 2007, malaria diagnostic testing rates rose rapidly from 4% to 86% (by 2009). Logistics, funding, training and supportive supervision complicate implementation.
UNICEF Data report that performance of malaria diagnostics in febrile children in surveys 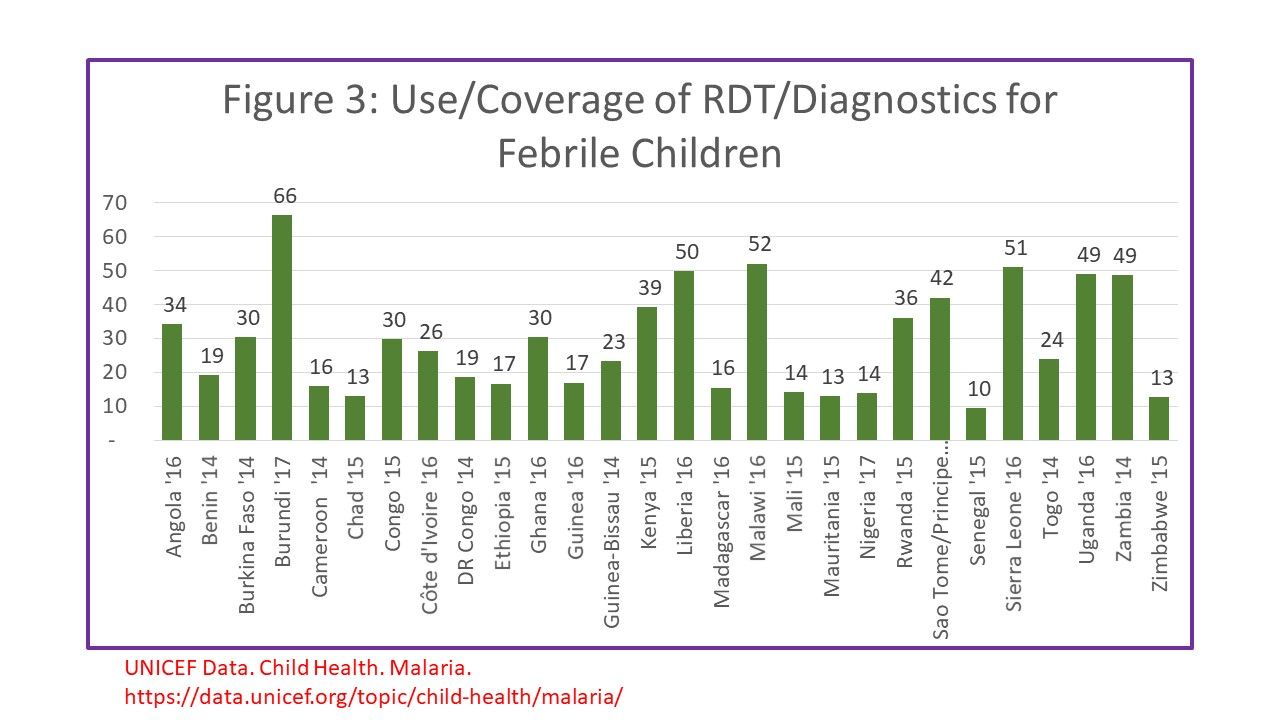 between 2014-17 was approximately 30% on average for countries with national surveys within that time frame (Figure 3). Only 4 countries achieved 50% or better. Most surveys then go on to report the number of febrile children who received ACTs, but do not necessary indicate how many who were correctly diagnoses were given ACTs vs those who received ACT but did not receive a test or tested negative.
between 2014-17 was approximately 30% on average for countries with national surveys within that time frame (Figure 3). Only 4 countries achieved 50% or better. Most surveys then go on to report the number of febrile children who received ACTs, but do not necessary indicate how many who were correctly diagnoses were given ACTs vs those who received ACT but did not receive a test or tested negative.
The Nigeria 2015 Malaria Indicator Survey Illustrates this dilemma. Among 2600 children who reported having a fever in the two weeks preceding the survey, 66.1% sought advice (or care). Overall, 12.6% of febrile children received a diagnostic test as defined in the question as to whether the child was stuck on the finger or heel to obtain blood. Among the febrile children 37.6% reportedly were given some type of antimalarial drug. Overall 15.5% of febrile children were given an ACT. Even if ACTs were given only to tested children, not all tests would have been positive.
The overall implication of measuring treatment without a link to testing is that if more children receive any, let alone the correct drugs, is that evidence for actual presence of disease. We have a long way to go to measure malaria treatment coverage correctly, not to mention achieving universal coverage with appropriate treatment. Different malaria treatment-related interventions with different steps and different target groups in different regions of Africa and the World make defining, no less achieving UHC, a huge challenge.
Capacity Building &Costs &Research &Seasonal Malaria Chemoprevention &Surveillance &Treatment Bill Brieger | 04 May 2018
Multilateral Initiative for Malaria: Posters Range from Prevention to Cost to E-Learning and Beyond
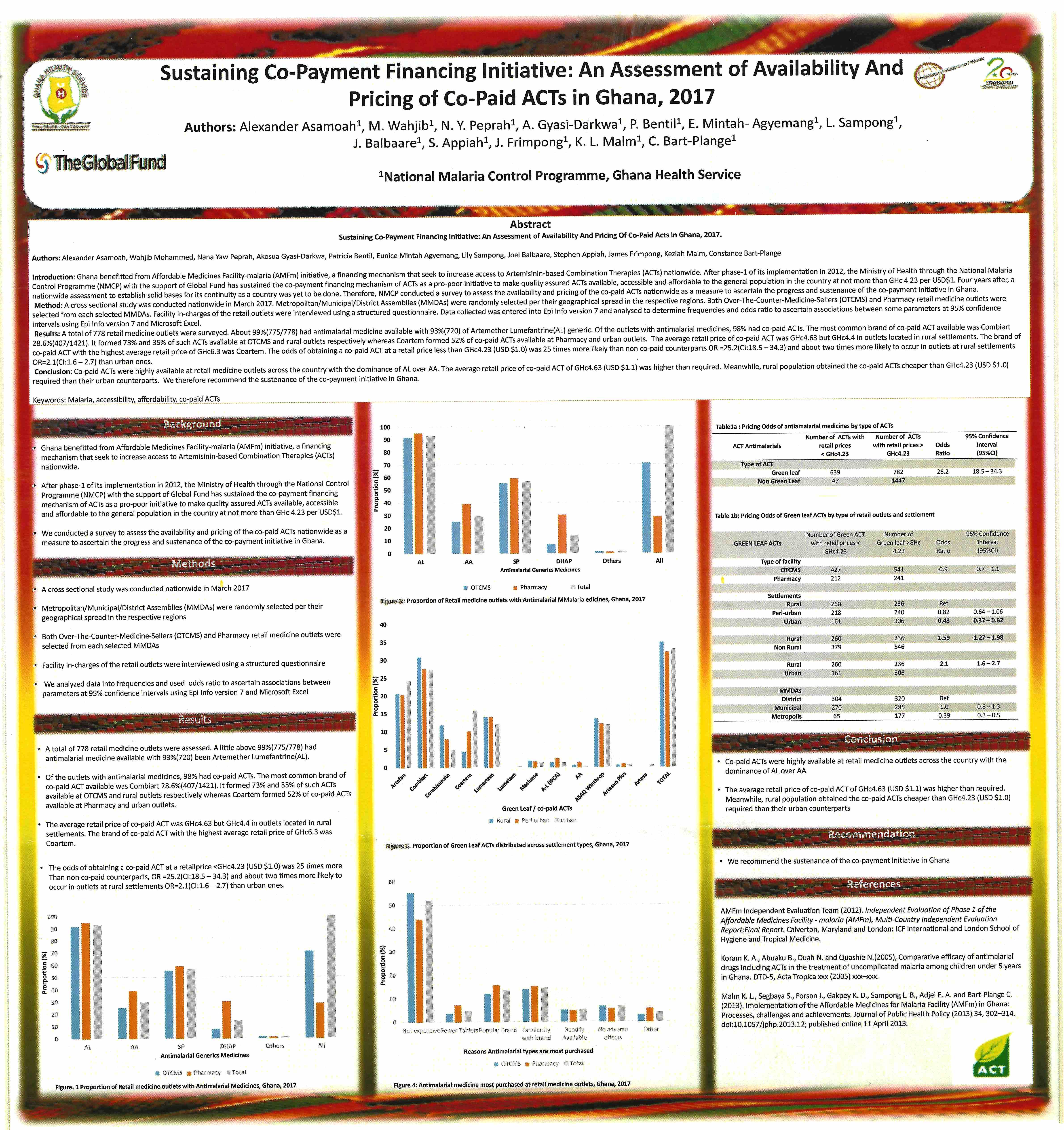
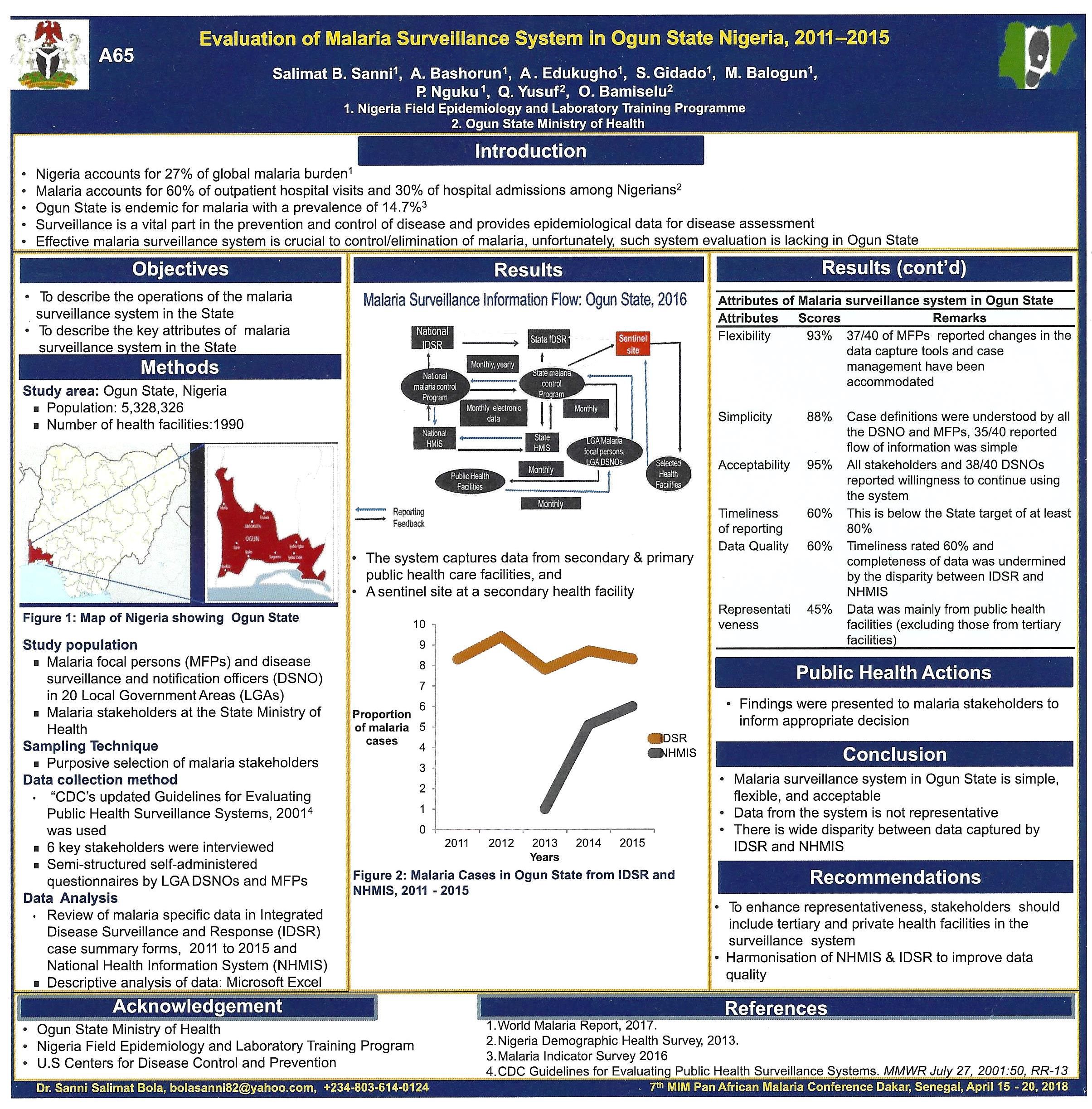
A major feature of all conferences are the poster sessions. These are often overlooked due to timing and placement. Fortunately at the recent 7th Multilateral Initiative for Malaria Conference in Dakar, tea breaks and lunch were made available in the poster tent ensuring more people came to view. Even so some people may have missed the valuable knowledge shared through this medium. We tweeted many of the posters during the event, but below are six posters in more detail.
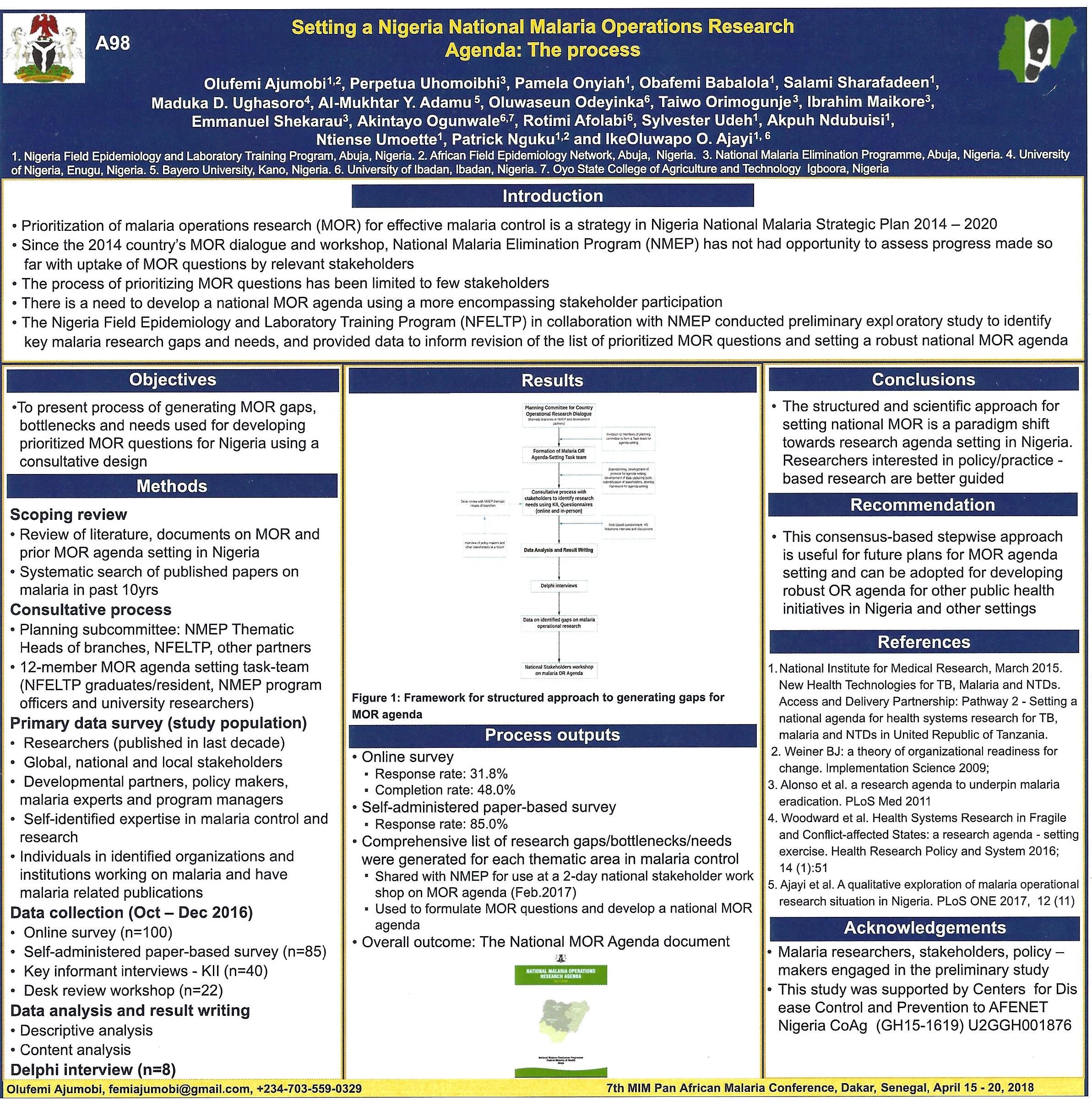
These range from evaluating a malaria surveillance system to financing systems to sustain malaria drug supplies, including through community pharmacies. The potential of E-Learning for malaria capacity building was explored, and the process pf establishing a national malaria operations research agenda was presented. Several posters examined the seasonal malaria chemoprevention (SMC) program in the Sahel of West Africa including one from Mali as seen below.
Please contact the authors for additional information and updates. Readers who presented a poster at MIM are welcome to share their findings with us.



Treatment &Universal Coverage &Women Bill Brieger | 07 Apr 2018
Health Insurance, Malaria and Universal Coverage
World Health Day 2018 is promoting universal health coverage. National Health Insurance Schemes (NHIS) are seen as a way to foster universal health coverage by improving access to basic, life-saving care. In malaria-endemic countries, NHIS hopefully play a role in reducing malaria mortality. For example in Nepal, malaria was among the chronic and communicable illnesses that showed increased catastrophic health expenditure over time leading to impoverishment. Health insurance was seen as a way to counteract this problem.
Although health insurance coverage in Tanzania was quite low, “a higher proportion of women with health insurance had a proper timing of 1st ANC attendance compared to their counterparts.” This enables them to access malaria prevention services and interventions.
 Ghana has been operating a NHIS since 2003. Overall national coverage has been estimated at around 40%, with a greater proportion of women covered than men. The 2014 Demographic and Health and 2016 Malaria Indicator Surveys (DHS, MIS) show that around 60% of women of reproductive age have NHIS coverage. How does this translate into malaria service coverage?
Ghana has been operating a NHIS since 2003. Overall national coverage has been estimated at around 40%, with a greater proportion of women covered than men. The 2014 Demographic and Health and 2016 Malaria Indicator Surveys (DHS, MIS) show that around 60% of women of reproductive age have NHIS coverage. How does this translate into malaria service coverage?
 In Ghana a decrease in malaria deaths was seen against a backdrop of increased admissions owing to free access to hospitalization through the NHIS, but hospital admission is not an option for all. Community case management is aimed at increasing access to and coverage of timely management of malaria and other child illnesses, but such services may not be covered by a NHIS. Since iCCM is effective in reaching children, Ghana is questioning how community based health workers can be brought into the health insurance arena.
In Ghana a decrease in malaria deaths was seen against a backdrop of increased admissions owing to free access to hospitalization through the NHIS, but hospital admission is not an option for all. Community case management is aimed at increasing access to and coverage of timely management of malaria and other child illnesses, but such services may not be covered by a NHIS. Since iCCM is effective in reaching children, Ghana is questioning how community based health workers can be brought into the health insurance arena.
Rwanda started its community based health insurance scheme in 2003 also and by 2013 had achieved 74% coverage. In Rwanda community malaria action teams (CMATs) were initiated in mid-2014 as platforms to deliver malaria preventive messages at village level. Among other benefits of the CMATs, an increase in community-based health insurance membership occurred,

Mutuelle (community health insurance) kiosk outside a clinic in Burkina Faso
which was also considered as a predictor of prompt and adequate care. Another study in Rwanda showed that head of household having health insurance (among other factors) was significantly associated with prompt and adequate care for presumed malaria illness.
NHIS have their own challenges in terms of affordability, community understanding of payment of premiums and availability of points of care that accept insurance or are accredited. And not all endemic countries have achieved even the modest successes of NHIS in Ghana and Rwanda. Thus health insurance offers hope for expanding universal coverage of malaria services, but health systems and community understanding and participation need to be improved for this to happen.