Case Management &Quality of Services &Training Bill Brieger | 27 Nov 2019
Improving the Quality of Malaria Case Management and Malaria Prevention During Pregnancy in Public Health Facilities in Burkina Faso
 Thierry D. A. Ouedraogo, Ousmane Badolo, Mathurin Dodo, Bonkoungou Moumouni, Youssouf Sawadogo, Dao Blami, and Stanislas Nébié presented a poster entitled “Improving the Quality of Malaria Case Management and Malaria Prevention During Pregnancy in Public Health Facilities in Burkina Faso” at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings are shared below.
Thierry D. A. Ouedraogo, Ousmane Badolo, Mathurin Dodo, Bonkoungou Moumouni, Youssouf Sawadogo, Dao Blami, and Stanislas Nébié presented a poster entitled “Improving the Quality of Malaria Case Management and Malaria Prevention During Pregnancy in Public Health Facilities in Burkina Faso” at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings are shared below.
Background: In 2017, malaria was the leading cause of medical consultation (43.34%), of hospitalization (44.05%) and of death (16.13%) in Burkina Faso. The disease mostly kills children under five years and pregnant women. One objective of the National Malaria Control Program (NMCP) is to contribute to improving the health of the population by reducing malaria mortality rate by at least 40% compared to 2015 in Burkina Faso by the end of 2020.
 In order to achieve that, the NMCP revised the malaria treatment guidelines in 2014 to take into account WHO guidelines on malaria case management and conducted training in primary health care facilities. NMCP implemented a one-day orientation training in district and regional hospitals since 2015, with the support of the PMI Improving Malaria Care Project.
In order to achieve that, the NMCP revised the malaria treatment guidelines in 2014 to take into account WHO guidelines on malaria case management and conducted training in primary health care facilities. NMCP implemented a one-day orientation training in district and regional hospitals since 2015, with the support of the PMI Improving Malaria Care Project.
Health Care Providers Training: The training of health care providers was carried out in several 5-days sessions at health districts level. It was aimed at strengthening their skills in the prevention and management of malaria cases in Primary health centers (CSPSs) according to the revised guidelines. 1,819 providers (633 females, 1,186 males) have been trained on the updated malaria prevention and control guidelines in 53 districts during this period.
 The training covered the definition and epidemiology of malaria, malaria drug prevention, biological diagnosis of malaria, of uncomplicated malaria cases management, severe malaria case management, healing assessment and health education, monitoring and evaluation. Clinical learning sessions on uncomplicated and severe malaria case management have allowed providers to practice treatment themselves.
The training covered the definition and epidemiology of malaria, malaria drug prevention, biological diagnosis of malaria, of uncomplicated malaria cases management, severe malaria case management, healing assessment and health education, monitoring and evaluation. Clinical learning sessions on uncomplicated and severe malaria case management have allowed providers to practice treatment themselves.
The goal of the project was To assess the diagnosis and case management of uncomplicated and severe malaria according malaria guideline in the various health facilities in Burkina Faso in 2017. A cross-sectional study was conducted in 2017 to assess the quality of malaria treatment and prevention during pregnancy in public health facilities.
 Submission of protocol Ethics Committee included Information of the surveyed structures and Information to respondents & verbal agreement. The team also worked to provide Quality assurance, Investigator training, Supervision of data collection and Development of guidelines for data collection.
Submission of protocol Ethics Committee included Information of the surveyed structures and Information to respondents & verbal agreement. The team also worked to provide Quality assurance, Investigator training, Supervision of data collection and Development of guidelines for data collection.
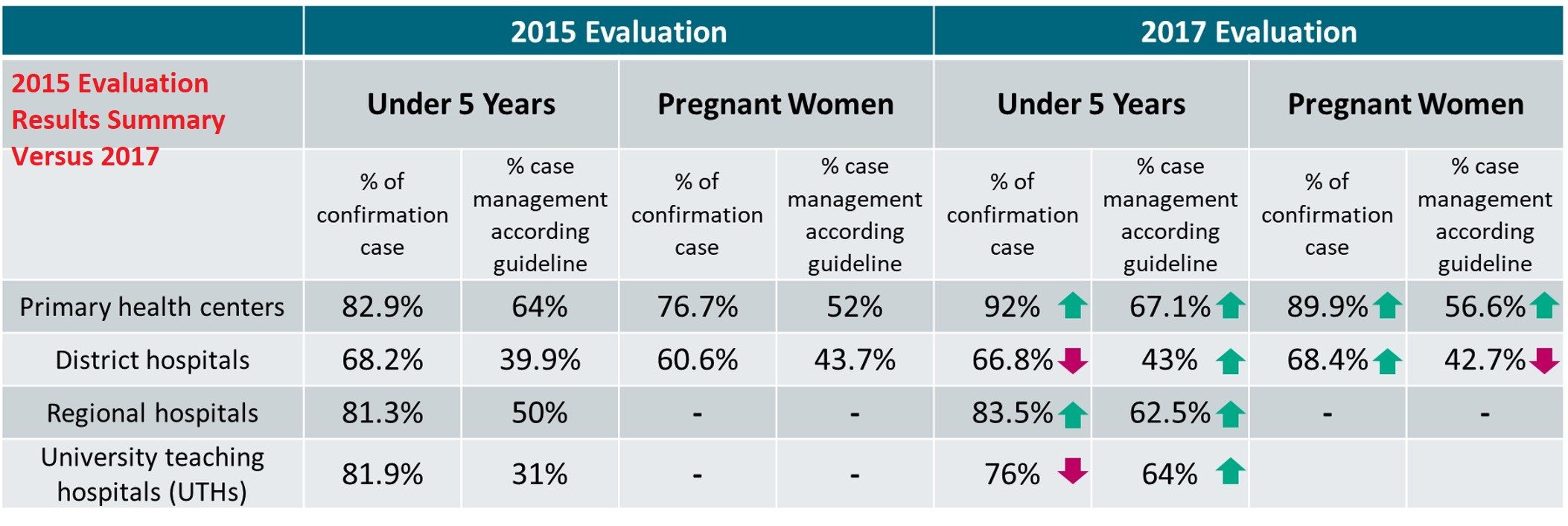
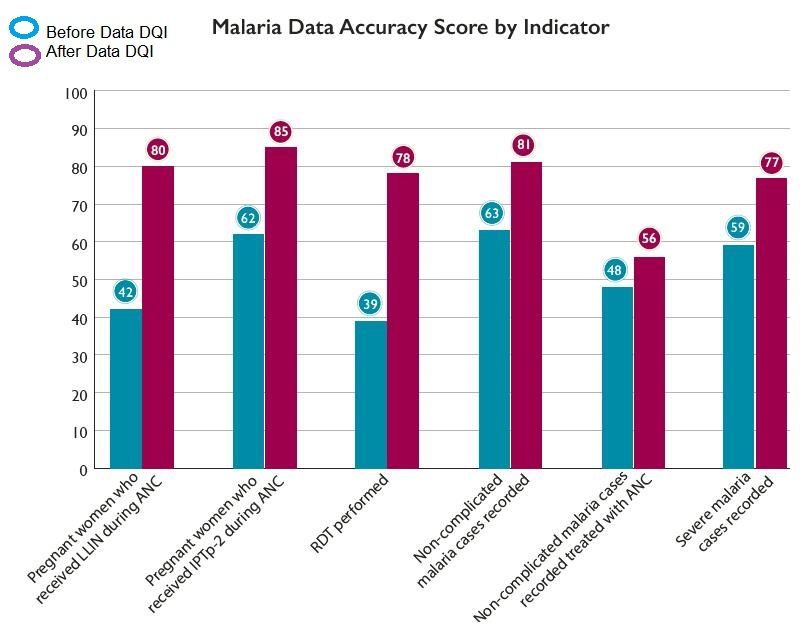
Data processing began with Data review. Data entry used Epi Info input 7.2.2.6. The Data collection period ran from 17-30 September 2018. The assessment focused on the malaria diagnosis and treatment. A comparative analysis of 2015 and 2017 data was done to understand trends.
Challenges included The lack of regional and district regular supervision and
The treatment of presumptive cases without confirmation. The non-application of the treatment protocol for severe malaria occurred in some case and as were variations in doses and duration of treatment. There was some stock-out of drugs for the treatment of uncomplicated and severe malaria.
 Overall there was an increase in correct procedures, and IMC project has strongly contributed to this success by training health care providers since 2015, by regularly monitoring the implementation of malaria control guidelines during supervision, and by ensuring the availability of supplies at all levels
Overall there was an increase in correct procedures, and IMC project has strongly contributed to this success by training health care providers since 2015, by regularly monitoring the implementation of malaria control guidelines during supervision, and by ensuring the availability of supplies at all levels
Recommendations include Ensuring the effective implementation of national guidelines for malaria management according to levels of care and the availability of supplies for the diagnosis, treatment and prevention of malaria during pregnancy at all levels.
In Conclusion, The results of the evaluation show that all health centres surveyed (50/50) have the capacity to diagnose (confirm cases) and treat malaria cases. At the end of the study, the results indicate that progress has been made in the diagnosis and treatment of malaria from 2015 to 2017.
*Affiliation: PMI Improving Malaria Care Project; Jhpiego Burkina Faso. This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID) under Cooperative Agreement No. AID-624-A-13-00010 and the President’s Malaria Initiative (PMI). The contents are the responsibility of the authors and do not necessarily reflect the views of USAID, PMI or the United States Government.
Case Management &Diagnosis &IPTp &ITNs &Quality of Services Bill Brieger | 26 Nov 2019
Use of Malaria Service and Data Quality Improvement in Mwanza Tanzania
 Emmanuel Lesilwa, Goodluck Tesha, Jasmine Chadewa, Agnes Kosia, Zahra Mkomwa, Bayoum Awadhi, Gaudiosa Tibaijuka, Rita Noronha, Dunstan Bishanga, Lusekelo Njonge, Frank Chacky, Abdallah Lusasi, Ally Mohamed, Chonge Kitojo, and Erik Reaves presented a poster entitled “Use of Malaria Service and Data Quality Improvement (MSDQI) Tool in Cascaded Supervision Approach Improved Quality of Malaria Services – Experience from Mwanza, Tanzania” at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings are shared below.
Emmanuel Lesilwa, Goodluck Tesha, Jasmine Chadewa, Agnes Kosia, Zahra Mkomwa, Bayoum Awadhi, Gaudiosa Tibaijuka, Rita Noronha, Dunstan Bishanga, Lusekelo Njonge, Frank Chacky, Abdallah Lusasi, Ally Mohamed, Chonge Kitojo, and Erik Reaves presented a poster entitled “Use of Malaria Service and Data Quality Improvement (MSDQI) Tool in Cascaded Supervision Approach Improved Quality of Malaria Services – Experience from Mwanza, Tanzania” at the 68th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings are shared below.
 Inadequate quality of malaria service and data has been one of the problems in Mwanza region due to high malaria prevalence, inadequate knowledge of supervisors and standardized supervision tool. In 2017, NMCP and stakeholders developed malaria services and data quality improvement (MSDQI) tool to guide supervisors. The tool comprises of seven modules addressing performance of Malaria Case Management with indicators weighted against a standard score. Any facility scoring below 50% of the overall score is deemed poorly performing, 50%-75% moderate and above 75% good performance.
Inadequate quality of malaria service and data has been one of the problems in Mwanza region due to high malaria prevalence, inadequate knowledge of supervisors and standardized supervision tool. In 2017, NMCP and stakeholders developed malaria services and data quality improvement (MSDQI) tool to guide supervisors. The tool comprises of seven modules addressing performance of Malaria Case Management with indicators weighted against a standard score. Any facility scoring below 50% of the overall score is deemed poorly performing, 50%-75% moderate and above 75% good performance.
 What is Malaria Service and Data Quality Improvement (MSDQI)? It is a checklist to guide supportive supervision teams in evaluating the quality of malaria services at the health facility level. MSDQI helps with the:-
What is Malaria Service and Data Quality Improvement (MSDQI)? It is a checklist to guide supportive supervision teams in evaluating the quality of malaria services at the health facility level. MSDQI helps with the:-
- Monitoring and evaluation
- Facility-based malaria performance indicators
- Provision of timely, accurate information and data for decision-making at district, regional, and national levels
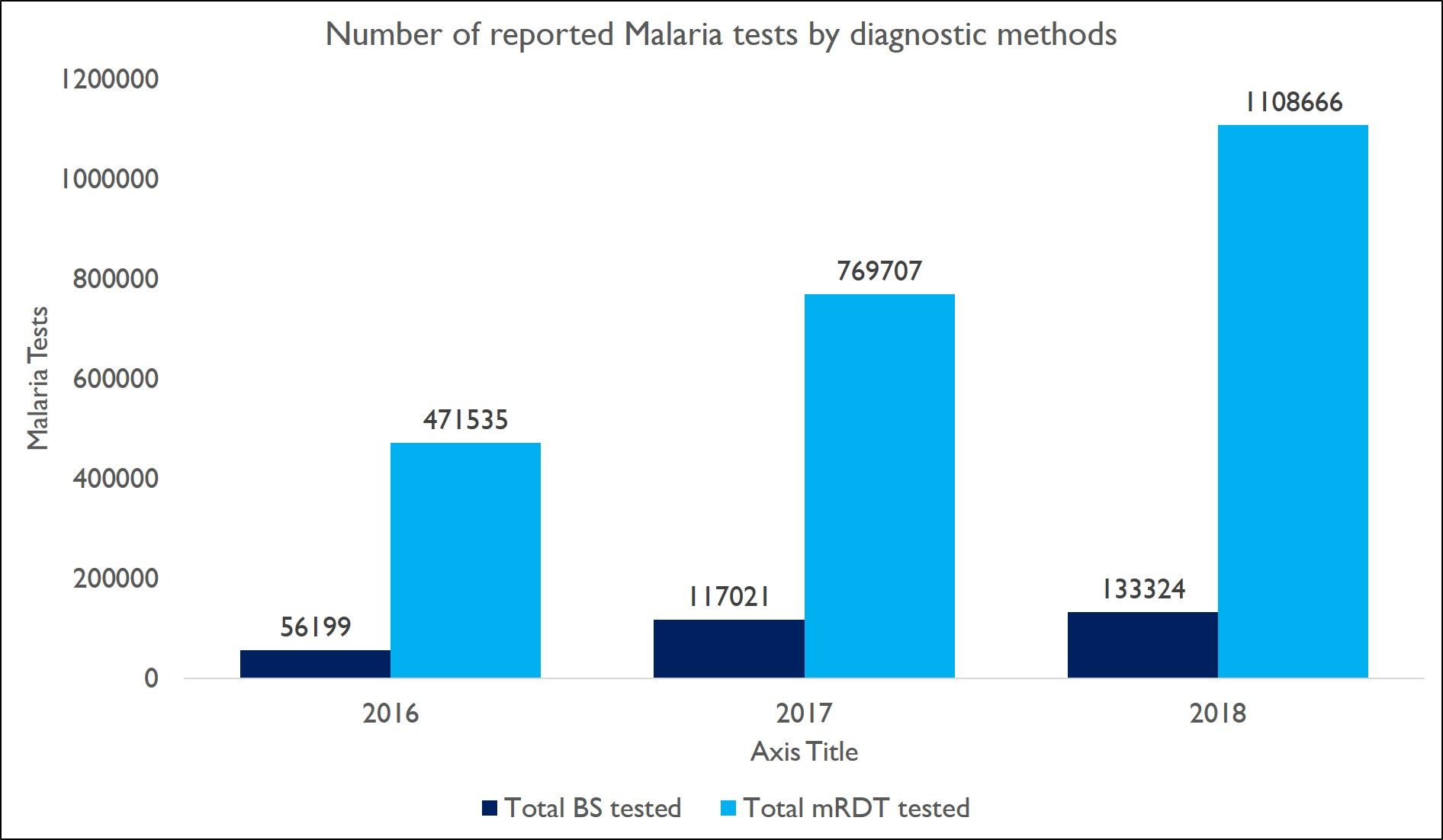
 In the attached graphs we present the Number of malaria test among OPD cases and the Number of malaria test among OPD cases which increased from 527,734 in 2016 to 1,241,990 in 2018 in Mwanza region. This resulted to the decrease of patients treated without malaria confirmatory test.
In the attached graphs we present the Number of malaria test among OPD cases and the Number of malaria test among OPD cases which increased from 527,734 in 2016 to 1,241,990 in 2018 in Mwanza region. This resulted to the decrease of patients treated without malaria confirmatory test.
 After intervention with MSDQI, there was a Decline in proportion of malaria cases clinically diagnosed and treated in Mwanza Regions reduced from 6.5% cases in 2016 to 0.1% cases in 2018
After intervention with MSDQI, there was a Decline in proportion of malaria cases clinically diagnosed and treated in Mwanza Regions reduced from 6.5% cases in 2016 to 0.1% cases in 2018
Good progress in IPTp2 and IPTp3 Coverage in Mwanza region was also 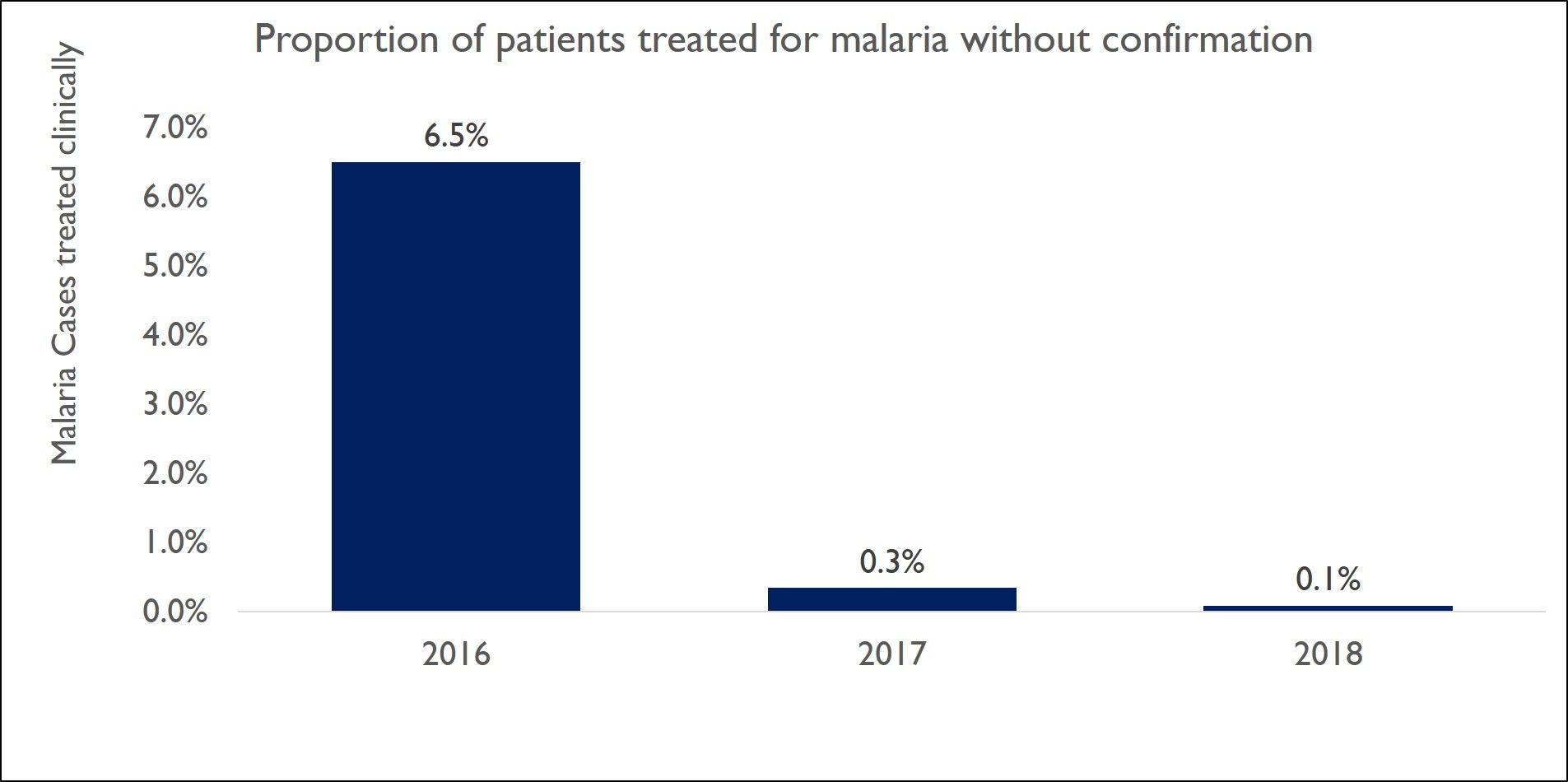 documented. IPTp2 increased from 37.6% in 2016 to 72.3%, while PITp3 increased from 1.2% in 2016 to 48.5% in 2018.
documented. IPTp2 increased from 37.6% in 2016 to 72.3%, while PITp3 increased from 1.2% in 2016 to 48.5% in 2018.
There was Increased coverage of LLINs in pregnant women and infants.
Increased coverage of LLINs in Pregnant women went from 4.9% 2016 to 75.6% in 2018. Likewise that for Infants increased from 2.9% 2016 to 65% in 2018.
 Several Lessons were Learned. Cascaded supervision approaches contribute to improved quality of malaria service provision and hence improved malaria indicators. The Way forward is to Continue using cascaded supervisors to improve quality of data and malaria services through MSDQI
Several Lessons were Learned. Cascaded supervision approaches contribute to improved quality of malaria service provision and hence improved malaria indicators. The Way forward is to Continue using cascaded supervisors to improve quality of data and malaria services through MSDQI
 *Affiliation: : USAID Boresha Afya Lake and Western Zone – PATH; USAID Boresha Afya Lake and Western Zone –Jhpiego; National Malaria Control Programme-Tanzania Ministry of Health, Community Development, Gender, Elderly and Children, Tanzania; US President’s Malaria Initiative-United States Agency for International Development
*Affiliation: : USAID Boresha Afya Lake and Western Zone – PATH; USAID Boresha Afya Lake and Western Zone –Jhpiego; National Malaria Control Programme-Tanzania Ministry of Health, Community Development, Gender, Elderly and Children, Tanzania; US President’s Malaria Initiative-United States Agency for International Development
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of the USAID Boresha Afya and do not necessarily reflect the views of USAID or the United States government
Case Management &Children &Health Workers &IPTp &Malaria in Pregnancy &Quality of Services Bill Brieger | 04 Nov 2018
Improving Malaria through National Rollout of Malaria Service and Data Quality Improvement: A Case Study from Tanzania
Jasmine Chadewa, Chonge Kitojo, Goodluck Tesha, Naomi Kaspar, Lusekelo Njoge, Zahra Mkomwa, Dunstan Bishanga, George Greer, Abdallah Lusasi, and Sigsbert Mkude of the USAID Boresha Afya Project, the US President’s Malaria Initiative, the National Malaria Control Program, and the Community Development, Gender, Elderly and Children (Tanzanian Ministry of Health) shared how malaria data quality could be improved at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. Below are their findings.
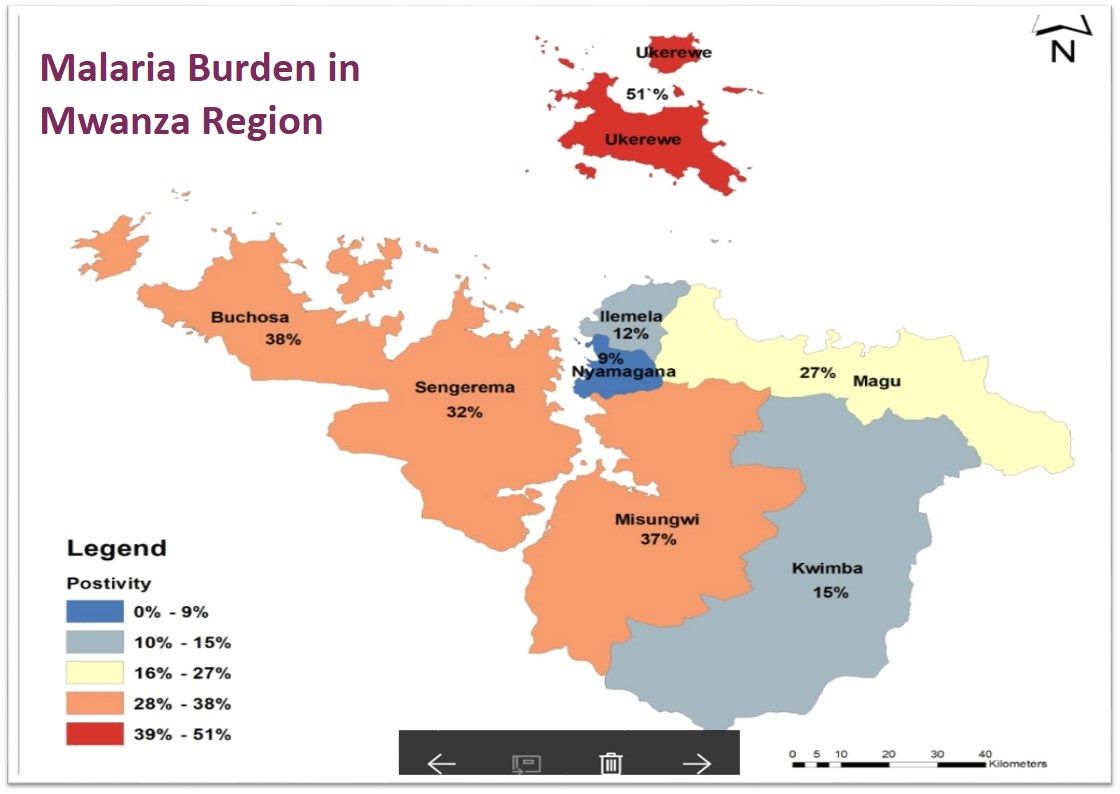
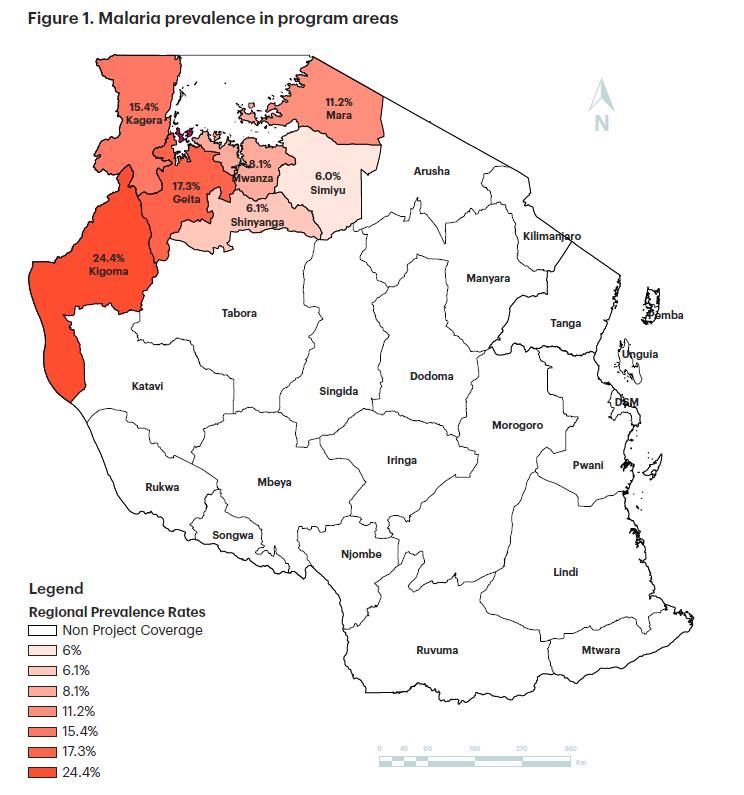 Tanzania has a high malaria burden (see Figure 1) and is facing an increased demand for health services. The Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) developed the Malaria Service and Data Quality Improvement (MSDQI) checklist to guide supportive supervision teams in evaluating the quality of malaria case management (MCM) services at facility level. MSDQI helps with the collection, monitoring, and evaluation of facility-based malaria performance indicators at all levels of service delivery that provide timely, accurate information and data for decision-making at district, regional, and national levels.
Tanzania has a high malaria burden (see Figure 1) and is facing an increased demand for health services. The Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) developed the Malaria Service and Data Quality Improvement (MSDQI) checklist to guide supportive supervision teams in evaluating the quality of malaria case management (MCM) services at facility level. MSDQI helps with the collection, monitoring, and evaluation of facility-based malaria performance indicators at all levels of service delivery that provide timely, accurate information and data for decision-making at district, regional, and national levels.
 USAID Boresha Afya conducted MSDQI assessments in 1,222 health facilities in the Lake and Western zones in outpatient departments (OPDs) and during antenatal care (ANC). The program disseminates malaria and ANC guidelines, tablets, job aids, and standard operating procedures. It also continues to facilitate supportive
USAID Boresha Afya conducted MSDQI assessments in 1,222 health facilities in the Lake and Western zones in outpatient departments (OPDs) and during antenatal care (ANC). The program disseminates malaria and ANC guidelines, tablets, job aids, and standard operating procedures. It also continues to facilitate supportive  supervision and mentorship through the MSDQI tool to build providers’ capacity in identified areas.
supervision and mentorship through the MSDQI tool to build providers’ capacity in identified areas.
Among the challenges reported, Supervisors need to be trained in more than one module to reduce cost. There is turnover of MSDQI supervisors. Cases that come back positive for diseases other than malaria are not investigated further. The use of Android smartphones sometimes  interfered with data collection and the reporting system. • Regions/districts depend on donor support to implement MSDQI activities.
interfered with data collection and the reporting system. • Regions/districts depend on donor support to implement MSDQI activities.
In conclusion, effective implementation of the MSDQI tool requires regions, districts, and facilities to be well informed and given clear instruction so they can form supportive supervision teams. This should be done by:
- Orienting teams on roles and responsibilities
- Training teams on relevant competencies, resource allocation, and tablet
use for data collection
The team learned that MCM improved in OPDs and during ANC as a result of the MSDQI assessment. Improved access to quality MCM (diagnosis) nationwide. Frequency of malaria testing increased during the first ANC contact. Testing increased from 87% in April–June 2017 to 96% April–June 2018, a 9% change (see Figure 3). Second doses of intermittent preventive treatment of malaria in pregnancy (IPTp2) coverage increased by 15% on average in Boresha Afya-supported regions between October 2016 and June 2018 (see Figure 4).
![]() This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of USAID Boresha Afya and do not necessarily reflect the views of USAID or the United States government.
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of USAID Boresha Afya and do not necessarily reflect the views of USAID or the United States government.
Case Management &Health Information &Quality of Services Bill Brieger | 02 Nov 2018
Using the collaborative quality improvement approach to increase adherence to the test, treat, and track malaria case management framework: Experiences from 10 health facilities in Uganda
Thomson Ngabirano, Espilidon Tumukurate, Innocent Atukunda, Emily Katarikawe, Jimmy Opigo, Martin Muhire, Emily Goodwin, Sam Gudoi, Kassahun Belay, Peter Thomas, James Tibenderana have been working with the following partners in Uganda to improve malaria  case management: Jhpiego, United States Agency for International Development’s (USAID) Malaria Action Program for Districts (MAPD) Project, Uganda National Malaria Control Program, Ministry of Health, University Research Co., the USAID ASSIST Project, Malaria Consortium, US President’s Malaria Initiative, and the US Centers for Disease Control and Prevention, Uganda. Their work, seen below, was presented at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene.
case management: Jhpiego, United States Agency for International Development’s (USAID) Malaria Action Program for Districts (MAPD) Project, Uganda National Malaria Control Program, Ministry of Health, University Research Co., the USAID ASSIST Project, Malaria Consortium, US President’s Malaria Initiative, and the US Centers for Disease Control and Prevention, Uganda. Their work, seen below, was presented at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Malaria has a 19 percent parasite prevalence in Uganda and is a leading cause of morbidity and mortality in Uganda and in 2014 was responsible for:
- 30-50 percent of outpatient visits
- 15-20 percent of hospital admissions
- 20 percent of inpatient deaths.[1]
 In an effort to reduce its malaria burden, in 2016 the Ministry of Health in Uganda incorporated a number of World Health Organization recommendations into its National Malaria Policy Guidelines. The main elements in these guidelines implemented by health workers were:
In an effort to reduce its malaria burden, in 2016 the Ministry of Health in Uganda incorporated a number of World Health Organization recommendations into its National Malaria Policy Guidelines. The main elements in these guidelines implemented by health workers were:
- testing all suspected malaria cases with malaria rapid diagnostic tests (mRDT) or microscopy before treatment
- using artemisinin-based combination therapy (ACT) to treat only positive malaria cases
- providing at least three doses of intermittent preventive treatment in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP).
However, a number of challenges for malaria service delivery were encountered during
implementation, including incomplete, inaccurate, and inconsistent malaria records and reports; health workers not adhering to the malaria test, treat, and track policy; and malaria causing high caseloads at outpatient and inpatient service points.
To overcome these issues, and in particular to improve adherence to the malaria test, treat and track policy and strengthen the quality of data collection and recording, USAID’s Malaria Action Program for Districts (MAPD) implemented a collaborative quality improvement approach (CQI).
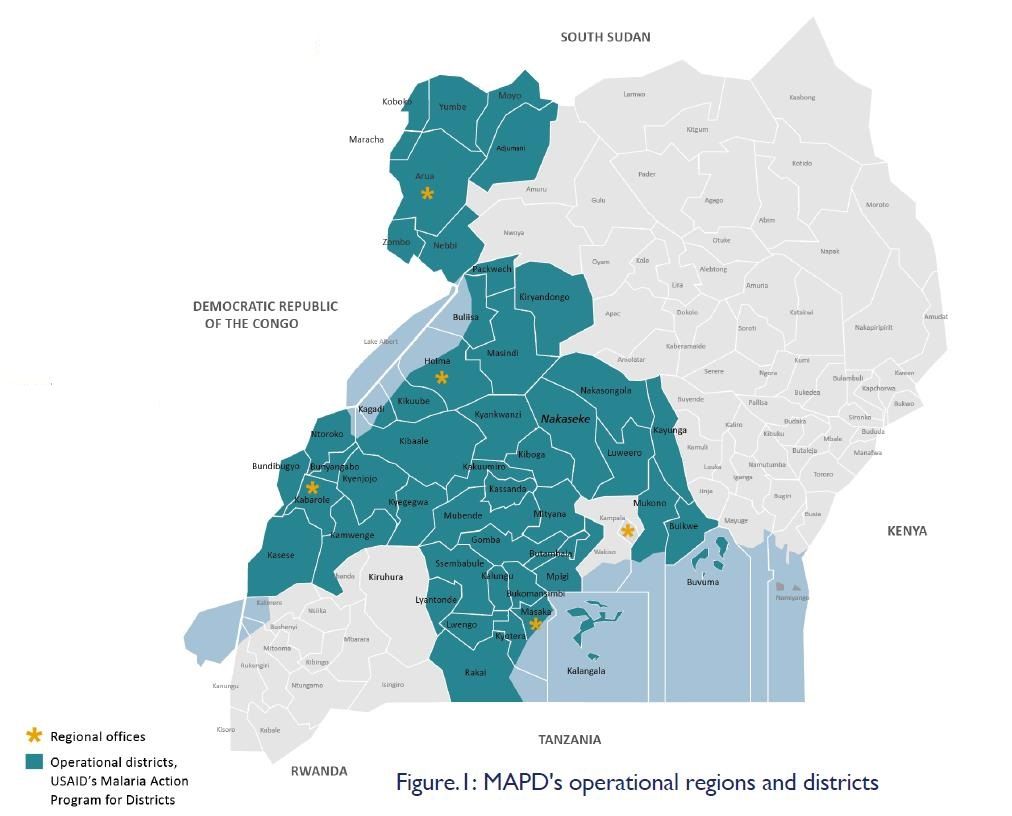
 A CQI approach was introduced to MAPD in November 2017 and implemented using both qualitative and quantitative methods. These included reviewing malaria indicators on the District Health Information System, identifying 10 high-volume facilities across MAPD’s five operational regions with poor malaria indicators (see Figure 1), holding entry meetings with the district health teams, conducting collaborative data reviews and problem analysis with health facility staff, and presenting the results of data reviews to health facility staff to identify inaccurate reporting and non-compliance with the test, treat and track policy. Interventions also included working with health facility staff to identify potential solutions and interventions, implementing agreed interventions and reviewing indicators, monitoring progress using documentation journals, holding learning sessions led by a CQI coach, agreeing on new actions.
A CQI approach was introduced to MAPD in November 2017 and implemented using both qualitative and quantitative methods. These included reviewing malaria indicators on the District Health Information System, identifying 10 high-volume facilities across MAPD’s five operational regions with poor malaria indicators (see Figure 1), holding entry meetings with the district health teams, conducting collaborative data reviews and problem analysis with health facility staff, and presenting the results of data reviews to health facility staff to identify inaccurate reporting and non-compliance with the test, treat and track policy. Interventions also included working with health facility staff to identify potential solutions and interventions, implementing agreed interventions and reviewing indicators, monitoring progress using documentation journals, holding learning sessions led by a CQI coach, agreeing on new actions.
Malaria data indicators reviewed include accuracy and completeness of cases in lab register and OPD, number of fever cases tested for malaria using mRDT or microscopy, number of malaria-negative cases treated with ACTs, number of malaria-positive cases treated with ACTs, and number of pregnant women receiving three or more doses of IPTp-SP.
In a sample of 300 cases from a June 2018 lab register, taken eight months after the CQI approach was introduced, all 300 (100 percent) were recorded in the respective OPD register. This represents a 108 percent increase from when an equivalent sample was first reviewed in November 2017. In a sample of 300 patients that were treated using ACTs in June 2018, all patients were tested for malaria using mRDTs or microscopy and no patients were treated that had tested negative. This represents an 89 percent decrease from November 2017 when 27 (nine percent) malaria-negative cases were incorrectly treated using ACTs.
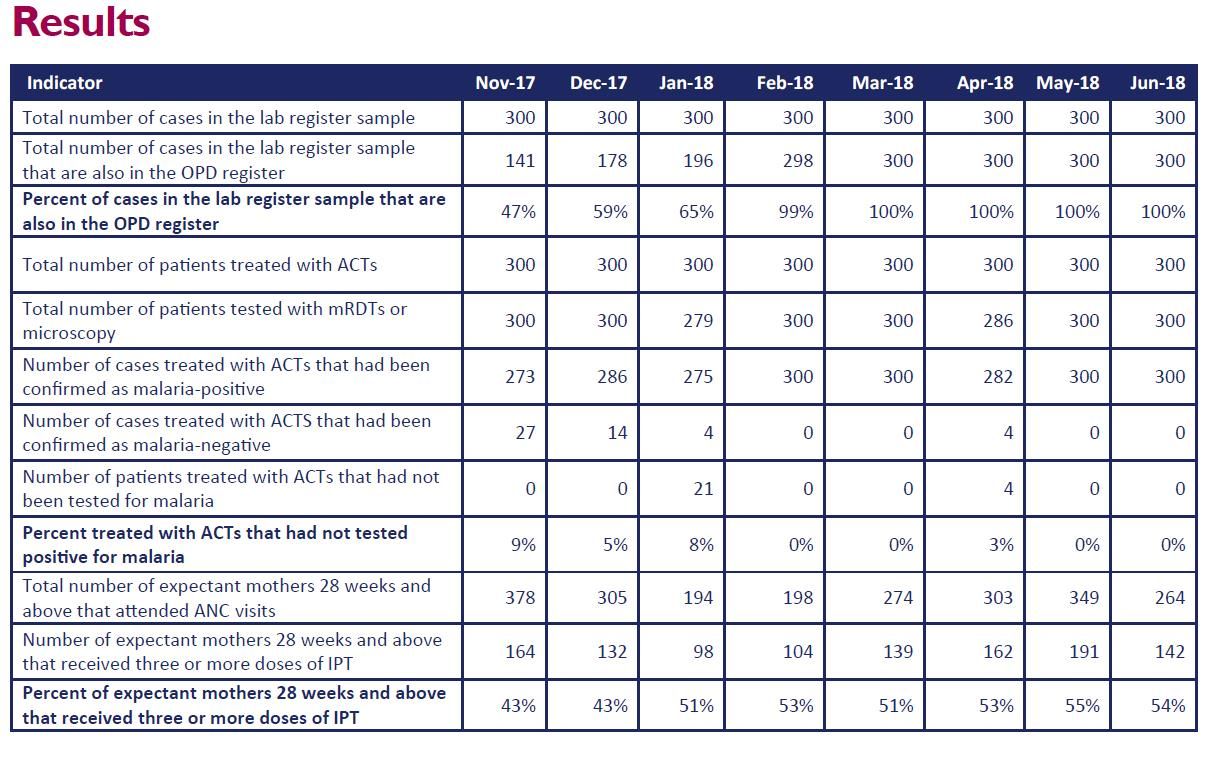
Of the total 264 expectant mothers (who were 28 weeks pregnant and above) that attended ANC visits in July 2018, 142 (54 percent) received three or more doses of IPTp-SP. This is a marked increase on the 43 percent of pregnant women who received three or more doses in November 2017.
Feedback from discussions with health workers in facility meetings and regional learning sessions showed that health teams now accept that there is a need for accurate and complete data and understand the importance of adhering to the National Malaria Policy Guidelines. In conclusion … The CQI approach was found to promote accurate data collection and improve adherence to the malaria test, treat, and track policy among health workers at 10 health facilities in five regions of Uganda.
[1] Reference: Uganda Bureau of Statistics (UBOS) and ICF International. Uganda Malaria Indicator Survey 2014-15. Kampala, Uganda and Rockville, Maryland, USA: UBOS and ICF International; 2015. Available at https://dhsprogram.com/pubs/pdf/mis21/mis21.pdf
MAPD is a project (running from 2016-2021), funded by the US President’s Malaria Initiative, USAID, UK aid, and the government of Uganda, which aims to improve the health status of the Ugandan population by reducing malaria-related morbidity and mortality among children and pregnant women. This poster was made possible by the support of the American and British People through the United States Agency for International Development and UK aid from the UK government. The contents of this poster are the sole responsibility of USAID Malaria Action Program for Districts and do not necessarily reflect the views of USAID or the United States Government and do not necessarily reflect the UK government’s official policies. For more information, please contact; 1. Dr Thomson Ngabirano, Malaria in Pregnancy Specialist Thomson.Ngabirano@Jhpiego.org 2. Dr Sam Siduda Gudoi, Chief of Party s.gudoi@malariaconsortium.org
Case Management &Health Information &IPTp &Mortality &Quality of Services Bill Brieger | 31 Oct 2018
Improving Malaria Care Project Contribution in Transforming Malaria Control for Vulnerable Populations in Burkina Faso
![]() Mathurin Dodo, Ousmane Badolo, Stanislas Nebie, Youssouf Sawadogo, Thierry Ouedraogo, Moumouni Bonkoungou, Youssouf Zongo, Maria Gouem, Danielle Burke, Gladys Tetteh, Lolade Oseni, Linda Fogarty, and William Brieger of Jhpiego and the USAID Improving malaria Care Project in Burkina Faso shared the status of malaria control efforts at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. The focus on vulnerable populations is shared below.
Mathurin Dodo, Ousmane Badolo, Stanislas Nebie, Youssouf Sawadogo, Thierry Ouedraogo, Moumouni Bonkoungou, Youssouf Zongo, Maria Gouem, Danielle Burke, Gladys Tetteh, Lolade Oseni, Linda Fogarty, and William Brieger of Jhpiego and the USAID Improving malaria Care Project in Burkina Faso shared the status of malaria control efforts at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. The focus on vulnerable populations is shared below.
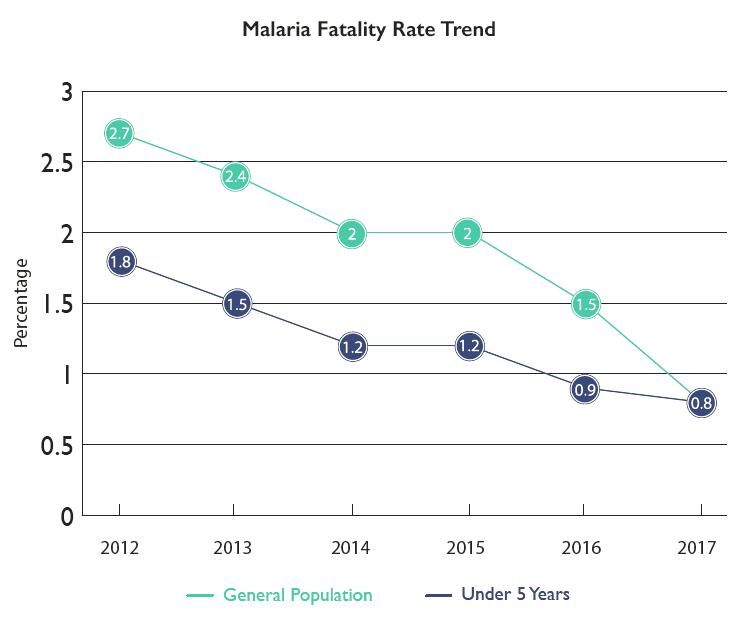
Burkina Faso in 2010-2012 experienced poor capacity in malaria prevention and control, Malaria fatality rate was high:
- Pregnant women: 0.71% in 2010 and 0.66% in 2012
- Children under 5: 2.8% in 2010 and 2.7% in 2012
Improving Malaria Care (IMC) Project funded by USAID/President’s Malaria Initiative, began in 2013. IMC supports National Malaria Control Program to improve prevention and case
Management. IMC’s Strategies include the following:
- Update national malaria prevention and case management guidelines
- Strengthen health care provider capacity
- Align malaria training package with revised guidelines
- Strengthen national malaria health management information system (HMIS)
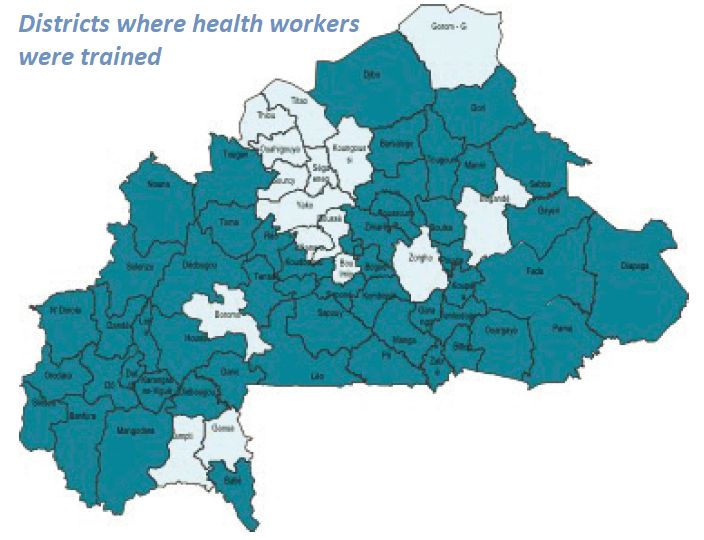 IMC together with the National Malaria Control Program has been strengthening Health Care Provider Capacity. 54 health districts have been covered by IMC direct support where 1819 providers were trained. Training reached 185 trainers/supervisors on revised training Modules who then trained 1,819 health care providers from 1,349 health facilities in 54 districts on new guidelines
IMC together with the National Malaria Control Program has been strengthening Health Care Provider Capacity. 54 health districts have been covered by IMC direct support where 1819 providers were trained. Training reached 185 trainers/supervisors on revised training Modules who then trained 1,819 health care providers from 1,349 health facilities in 54 districts on new guidelines
 After training 58 supervisors rolled out quality improvement (QI) systems. They oriented 897 providers from referral hospitals on new severe case management guidelines. Formative Supervision, Performance and Quality Improvement efforts were based on an improved malaria supervision guide and tools. Post-training supervision reached each provider. Specifically, malaria supervisions occurred twice a year.
After training 58 supervisors rolled out quality improvement (QI) systems. They oriented 897 providers from referral hospitals on new severe case management guidelines. Formative Supervision, Performance and Quality Improvement efforts were based on an improved malaria supervision guide and tools. Post-training supervision reached each provider. Specifically, malaria supervisions occurred twice a year.
The quality improvement approach, SBM-R® (Standards-Based Management and Recognition) approach, was implemented in 6 regions, 28 districts. Organized data review and validation workshop in 67 districts were another aspect of quality improvement. To sustain quality improvement, IMC conducted 2-day quality assessments and guided developed DQI implementation plans.
 Social Behavior Change Communication was a central component of IMC. IMC conducted 13 regional advocacy workshops on malaria issues. The project developed and broadcast 2 malaria spots through 27 media, revised 5 diagnostic and case management job aids, distributed 7,440 job aids to health facilities, and reached 792,660 people through community activities and sensitization sessions
Social Behavior Change Communication was a central component of IMC. IMC conducted 13 regional advocacy workshops on malaria issues. The project developed and broadcast 2 malaria spots through 27 media, revised 5 diagnostic and case management job aids, distributed 7,440 job aids to health facilities, and reached 792,660 people through community activities and sensitization sessions
 IMC Strengthened National Malaria HMIS. This included training 1,300 (72%) health workers to enter data into monthly reporting forms. Also trained were 326 data managers on HMIS and data use for decisionmakers. The malaria data collection system was integrated into national HMIS using DHIS2. To facilitate this the national HMIS manual was revised and distributed. Data Quality was improved through malaria data review and validation at district levelUltimately these interventions resulted in Improved Malaria Services. More confirmed simple malaria cases received artemisinin-based combination therapy (65% in 2013 to 90% in 2017). More women received three doses of IPTp3 (14% in 2014 to 51% in June 2018). More suspected cases tested for malaria (65% in 2013 to 96% 2017). More women received insecticide-treated nets at antenatal care. There was Better accuracy in reporting of malaria key indicators.
IMC Strengthened National Malaria HMIS. This included training 1,300 (72%) health workers to enter data into monthly reporting forms. Also trained were 326 data managers on HMIS and data use for decisionmakers. The malaria data collection system was integrated into national HMIS using DHIS2. To facilitate this the national HMIS manual was revised and distributed. Data Quality was improved through malaria data review and validation at district levelUltimately these interventions resulted in Improved Malaria Services. More confirmed simple malaria cases received artemisinin-based combination therapy (65% in 2013 to 90% in 2017). More women received three doses of IPTp3 (14% in 2014 to 51% in June 2018). More suspected cases tested for malaria (65% in 2013 to 96% 2017). More women received insecticide-treated nets at antenatal care. There was Better accuracy in reporting of malaria key indicators.
 Improved services led to decreased national malaria fatality rate. In the General population there was a decrease in malaria deaths of 34% and a decrease in overall fatality rate by 47%. Among pregnant women there was a decrease in malaria deaths by 91% and a decrease in malaria fatality rate by 93%. For Children under 5 years of age, there was a decrease in malaria deaths by 34% and a decrease in fatality rate 48%
Improved services led to decreased national malaria fatality rate. In the General population there was a decrease in malaria deaths of 34% and a decrease in overall fatality rate by 47%. Among pregnant women there was a decrease in malaria deaths by 91% and a decrease in malaria fatality rate by 93%. For Children under 5 years of age, there was a decrease in malaria deaths by 34% and a decrease in fatality rate 48%
 In conclusion the IMC Project Contributed to Lives Saved in Burkina Faso. IMC supported health delivery sites in Burkina Faso (Jan 2014 -Sep 2017). As a result the health system was able to Distribute 33,566,671 courses of artemisinin-based combination therapy. IMC provided 2,175,648 pregnant women with intermittent preventive treatment 2nd dose and distributed 1,146,185 nets to pregnant women during antenatal care visit. These interventions averted estimated 150,390 malaria deaths and 12,866,271 DALYs (Disability-Adjusted Life Years calculated using PSI Impact calculator. 1 DALY=1 lost year of “healthy” life.)
In conclusion the IMC Project Contributed to Lives Saved in Burkina Faso. IMC supported health delivery sites in Burkina Faso (Jan 2014 -Sep 2017). As a result the health system was able to Distribute 33,566,671 courses of artemisinin-based combination therapy. IMC provided 2,175,648 pregnant women with intermittent preventive treatment 2nd dose and distributed 1,146,185 nets to pregnant women during antenatal care visit. These interventions averted estimated 150,390 malaria deaths and 12,866,271 DALYs (Disability-Adjusted Life Years calculated using PSI Impact calculator. 1 DALY=1 lost year of “healthy” life.)
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID) under Cooperative Agreement No. AID-624-A-13-00010 and the President’s Malaria Initiative (PMI). The contents are the responsibility of the authors and do not necessarily reflect the views of USAID, PMI or the United States Government.
Announcement &Case Management &CHW &Community &Ebola &Infection Prevention &IPTp &Malaria in Pregnancy &Quality of Services Bill Brieger | 29 Oct 2018
Malaria Featured in Jhpiego Sessions at ASTMH 2018

Below is a list of Jhpiego Sessions at this week’s American Society of Tropical Medicine Annual Meeting in New Orleans (28 October-1 November). Please attend if you are at the conference:
![]() Poster Session A, Monday, October 29 (Posters in Marriott Grand Ballroom – 3rd Floor )
Poster Session A, Monday, October 29 (Posters in Marriott Grand Ballroom – 3rd Floor )
- Poster Number 098: Performance of community health workers in providing integrated community case management services (iCCM) in 8 districts of Rwanda
- Poster 380: Contribution of quarterly malaria data review and validation to data quality and malaria services Improvement
- Poster LB-5117: Community based health workers can enhance coverage of intermittent preventive treatment of malaria in pregnancy and promote antenatal attendance
Poster Session B, Tuesday 30 October
- Poster 1088: Assessing organizational capacity to deliver quality malaria services in rural Liberia
- Poster 1092: Contribution of IMC project in transforming the face of malaria control for vulnerable populations in Burkina Faso
- Poster 1093: Malaria response plan in times of high transmission: An approach to improving the quality of hospital malaria management
- Poster 1111: Setting the stage to introduce a ground breaking approach to prevent malaria in pregnancy in Sub-Saharan Africa: baseline-readiness assessment findings from Democratic Republic of Congo, Mozambique, Madagascar, and Nigeria
- Poster 1337: Institutionalizing infection prevention and control practices in health facilities in Liberia following the Ebola epidemic
 Scientific Session 87, Tuesday, 1:45 – 3:30 p.m. Marriott – La Galerie 1 & 2 – 2nd Floor: Improving procurement and redeployment of district level malaria commodities using SMS and web mapping in Madagascar
Scientific Session 87, Tuesday, 1:45 – 3:30 p.m. Marriott – La Galerie 1 & 2 – 2nd Floor: Improving procurement and redeployment of district level malaria commodities using SMS and web mapping in Madagascar
Poster Session C, Wednesday 31 October
- Poster 1816: Experiences and perceptions of care seeking for febrile illness among caregivers and providers in 8 districts of Madagascar
- Poster 1818: Improving adherence to national malaria treatment guidelines by village health workers in selected townships through a low-dose, high-frequency training approach
- Poster 1819: Improving malaria case management through national roll-out of Malaria Service and Data Quality Improvement (MSDQI): A Case study from Tanzania
- Poster 1820: Collaborative quality improvement framework to support data quality improvement, experience from 10 collaborative facilities in Uganda
- Poster 1821: Using malaria death audits to improve malaria case management and prevent future malaria related preventable deaths
- Poster 1833: Multiple approaches for malaria case management in the struggle to reach pre-elimination of malaria.
Scientific Session 182, Thursday, November 1, 10:15 am – 12:00 p.m. Marriott – Balcony I,J,K – 3rd Floor: Seasonal malaria chemoprevention, an effective intervention for reducing malaria morbidity and mortality
Community &Health Workers &Quality of Services Bill Brieger | 17 Apr 2018
Application d’un audit de la qualité des données (DQA) du paludisme dans le district sanitaire de Kribi, Cameroun
 Kodjo Morgah, Naibei Mbaïbardoum, Mathurin Dodo, et Eric Tchinda from Jhpiego share their experiences in improving malaria data quality in Kribi District, Cameroon. The project was funded by the ExxonMobil Foundation. Their findings are presented below.
Kodjo Morgah, Naibei Mbaïbardoum, Mathurin Dodo, et Eric Tchinda from Jhpiego share their experiences in improving malaria data quality in Kribi District, Cameroon. The project was funded by the ExxonMobil Foundation. Their findings are presented below.
Les indicateurs clés du paludisme En 2015 dans le district sanitaire de Kribi, Cameroun, le mortalité palustre était 19% et le morbidité palustre était 29%. En outre, le couverture du premier traitement de TPI était 76% et 55% pour le deuxième.
 Les interventions du projet Amélioration de la qualité des services de contrôle du paludisme au Tchad et au Cameroun sont montrés dans le diagramme ci-joint.
Les interventions du projet Amélioration de la qualité des services de contrôle du paludisme au Tchad et au Cameroun sont montrés dans le diagramme ci-joint.
Les activités DQA ont commencé en 2012. Au début du projet, les formations sanitaires de Kribi ne disposaient pas d’une gestion des données suffisante en termes de fiabilité, de complétude et de promptitude des registres des formations sanitaires et des rapports soumis. En 2013 nous avons formé des prestataires de Kribi en prévention et traitement du paludisme, y compris la collecte et la gestion des données, et collaboration avec l’équipe cadre de district (ECD) du Ministère de la Santé Publique (MSP) pour institutionnaliser les réunions mensuelles de vérification et de validation des données. Puis en 2015 nous avons développé et diffusé d’affiches de suivi des données pour aider les formations sanitaires à suivre les indicateurs clés du paludisme afin de soutenir une prise de décision efficace. L’année passe, en 2017, le DQA est réalisé.
 Objectifs du DQA sont d’améliorer la qualité des données du paludisme dans le district de Kribi; identifier les erreurs systématiques; apprécier les sous-déclarations et/ou sur-déclarations; mesurer la concordance des données rapportées; apprécier la précision, la validité, la fiabilité, et la complétude des données collectées; et renforcer les capacités des ECD et du PNLP.
Objectifs du DQA sont d’améliorer la qualité des données du paludisme dans le district de Kribi; identifier les erreurs systématiques; apprécier les sous-déclarations et/ou sur-déclarations; mesurer la concordance des données rapportées; apprécier la précision, la validité, la fiabilité, et la complétude des données collectées; et renforcer les capacités des ECD et du PNLP.
Pour mettre en œuvre du DQA, nous avons sélectionné huit indicateurs du paludisme et un indicateur général. Le projet a adapté des outils de collecte des données développés par le projet MEASURE Evaluation financé par l’USAID. Puis, il a facilité le constitution et orientation des équipes d’évaluateurs des données composées du personnel de Jhpiego et des membres de l’ECD. Apres ça, les équipes commencent le réalisation du DQA dans des sites sélectionnés
Modalités :
- Aucun problème de qualité des données, si la mDA est comprise entre 100% et 90%
- Problèmes mineurs de qualité des données, si la mDA est comprise entre 89% et 70%
- Problèmes majeurs de qualité des données, si la mDA est inférieure à 70%
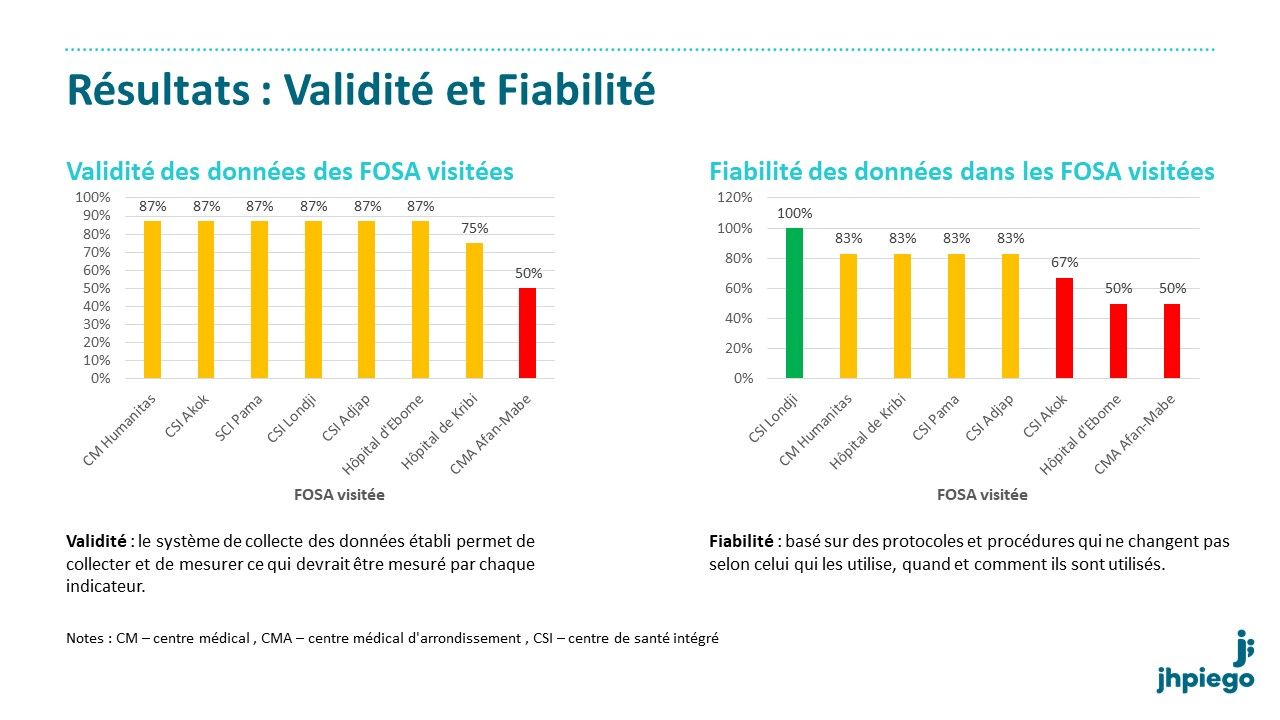
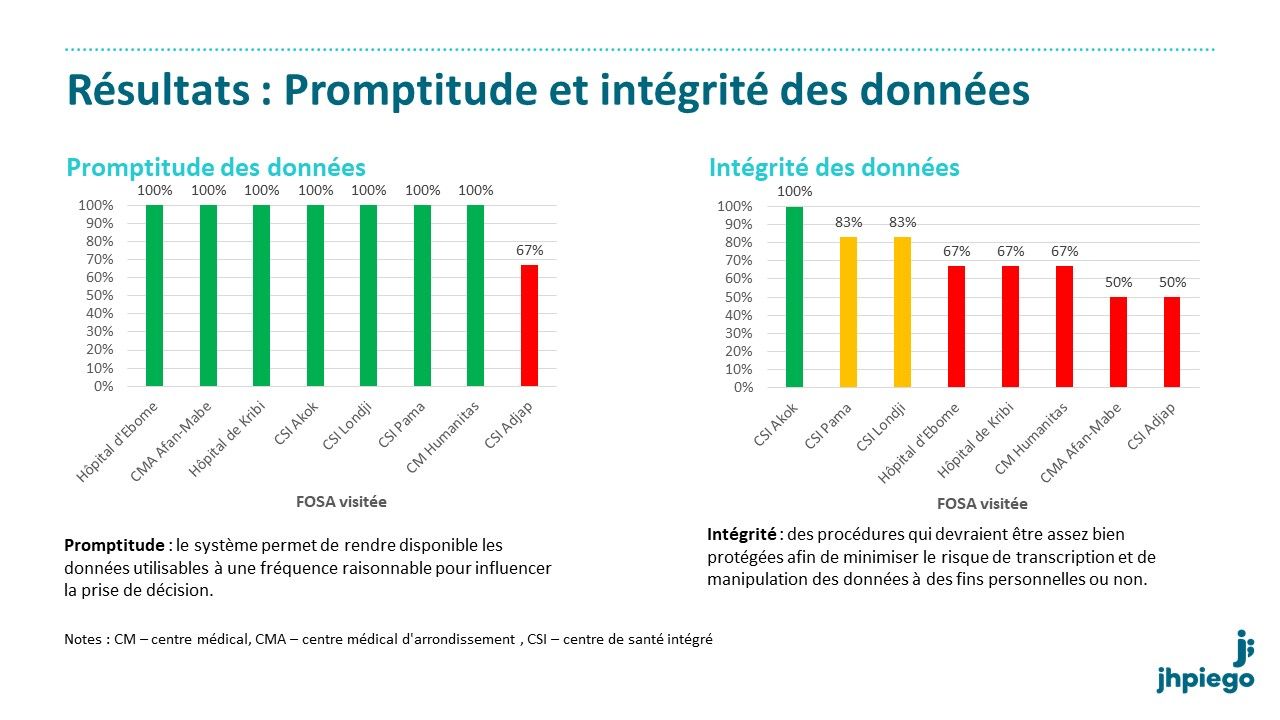


Conclusions: Le DQA a réussi à identifier les problèmes qui ont affecté la qualité des données dans les formations sanitaires de Kribi. Il a aussi révélé une meilleure qualité des données dans les formations sanitaires rurales que dans les formations sanitaires urbaines. Dans l’ensemble, la qualité des données du paludisme est acceptable dans la majorité des formations sanitaires soutenues par le projet.
 L’équipe de projet doit soutenir le personnel et les formations sanitaires du MS du district dans l’intégration des recommandations du DQA pour continuer à améliorer la qualité des données.
L’équipe de projet doit soutenir le personnel et les formations sanitaires du MS du district dans l’intégration des recommandations du DQA pour continuer à améliorer la qualité des données.
Recommendations: Il est necessaire de renforcer les capacités des prestataires dans la collecte des données à travers la supervision formative. Dans l’outil de supervision de district, il est utile d’intégrer la vérification et le contrôle des données. Une Aide-mémoire sur la vérification, le contrôle et la validation des données du paludisme devrait être disponible.
IPTp &Malaria in Pregnancy &Quality of Services Bill Brieger | 15 Apr 2018
Improved IPTp Uptake: MCSP Restoration of Health Services Experience in Liberia
Nyapu D.Taylor, Birhanu Getahun,Topian Zikeh, Anne Fiedler, and Allyson Nelson of the USAID supported Maternal and Child Survival Program/Jhpiego in Liberia are presenting their project aimed at strengthening health services in Liberia to improve uptake of Intermittent preventive treatment of malaria in pregnancy at the 7th Multilateral Initiative for Malaria in Dakar this week. Below are a description of their work and their main findings.

Mother and baby in Liberian Government Hospital, Grand Bassa County, Liberia. Photo by Kate Holt, Jhpiego.
In Liberia more than 170,000 pregnancies occur each year. Provision of two or more doses of SP for IPTp (IPTp2+) merely increased from 50% 2016. Provision of the three or more doses of
IPTp (IPTp3+) remains at 22%.Liberia adopted WHO’s IPTp3+ guideline but it is not practiced all over the country. There is a gap in the competency of the health care workforce. There are recurring stock-outs of SP.The Maternal and Child Survival Program (MCSP) Restoration of Health Services (RHS) intended to address these challenges. Project
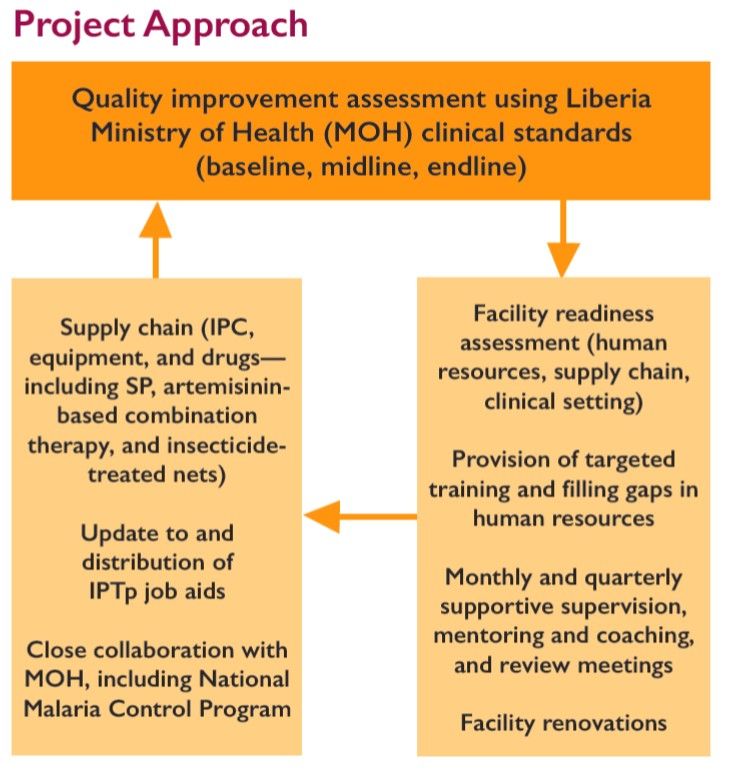
Objectives included Prevention at facilities by strengthening infection prevention and control (IPC) practices at 77 health facilities through training, intensive supportive supervision, triage, improvement of waste management, and provision of essential IPC commodities and supplies. Also the project aimed to Increase utilization of and demand for maternal and child health services bu restoring delivery of quality primary health care services through implementation of integrated reproductive, maternal, newborn, child, and adolescent health as part of the Essential Package of Health Services in 77 facilities.
 MCSP RHS supported health facilities in three counties:
MCSP RHS supported health facilities in three counties:
- Grand Bassa: 30 (91% of health facilities in county)
- Lofa: 17 (27% of health facilities in county)
- Nimba: 30 (46% of health facilities in county)
Population coverage was 900,000 or 20% of population. This included 45,000 pregnancies per year. The Project timeline is September 2015–June 2018. The quality improvement process used in the project is seen in the attached diagram.
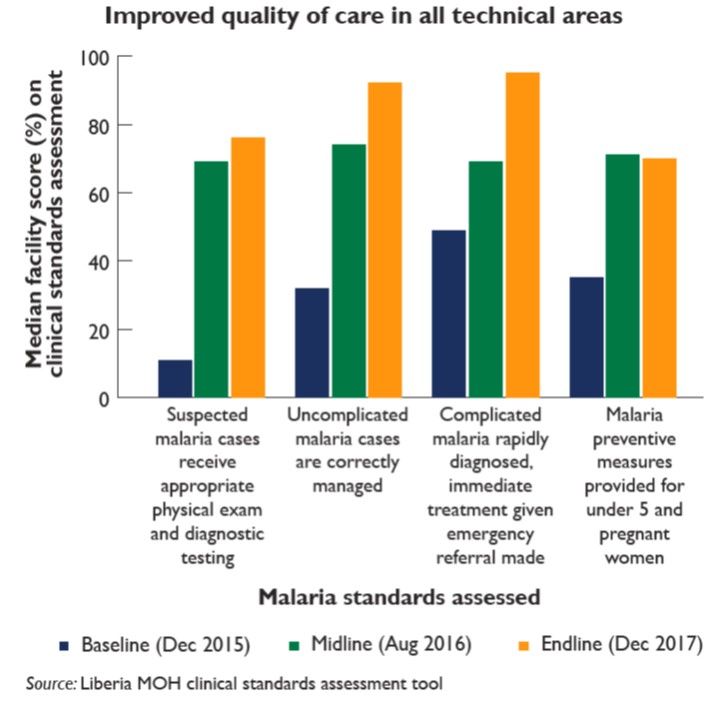
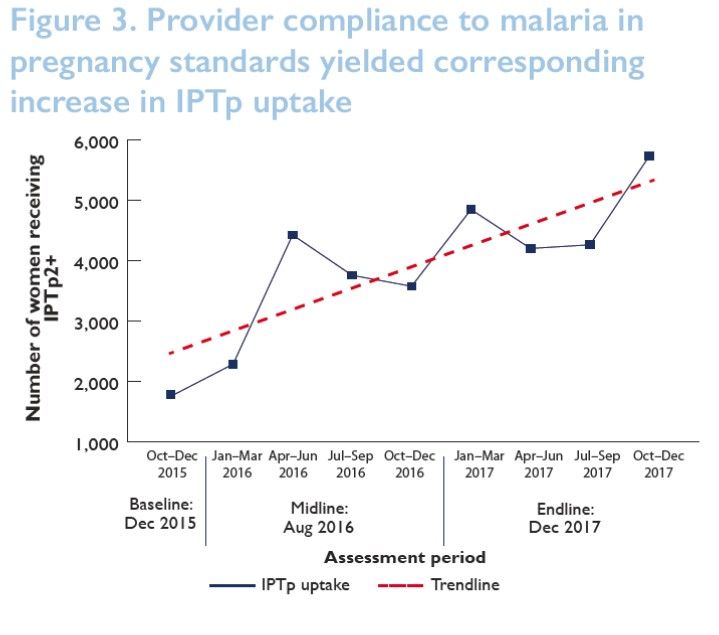
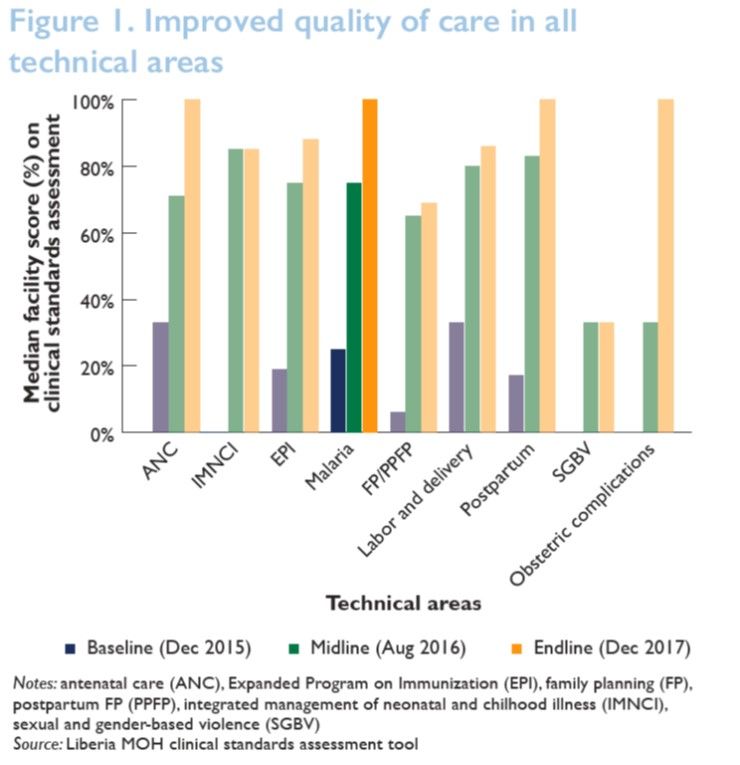 Several achievements were documented. Adherence to malaria clinical standards improved from 25% at baseline to 100% at endline in 39 MCSP-supported facilities—sampled at endline (see Figure 1). Adherence to malaria clinical standards improved substantially from baseline to endline in 39 MCSP-supported facilities—sampled at endline (see Figure 2). Increasing uptake of IPT2+ in the 77 RHS facilities has been observed since the inception of the project (see Figure 3).
Several achievements were documented. Adherence to malaria clinical standards improved from 25% at baseline to 100% at endline in 39 MCSP-supported facilities—sampled at endline (see Figure 1). Adherence to malaria clinical standards improved substantially from baseline to endline in 39 MCSP-supported facilities—sampled at endline (see Figure 2). Increasing uptake of IPT2+ in the 77 RHS facilities has been observed since the inception of the project (see Figure 3).
 The project met and dealt with several challenges. Health facilities were sporadically stocked with SP and mosquito nets (another component of malaria in pregnancy services). Bad roads prevented travel to field during rainy seasons. This affected distribution of malaria supplies and provision of mentorship and supervision for quality service. Clients had huge difficulty accessing health facilities.
The project met and dealt with several challenges. Health facilities were sporadically stocked with SP and mosquito nets (another component of malaria in pregnancy services). Bad roads prevented travel to field during rainy seasons. This affected distribution of malaria supplies and provision of mentorship and supervision for quality service. Clients had huge difficulty accessing health facilities.
 Among the lessons learned were that close collaboration and involvement of key actors, especially MOH (National Malaria Control Program) and country health team at all levels, is an effective and efficient approach for project implementation. Regular mentorship and coaching during supportive supervision improves the quality of care provided for malaria in pregnancy. Ensuring availability of IPTp drugs and long-lasting insecticidal nets at health facilities are key to preventing malaria in pregnancy.
Among the lessons learned were that close collaboration and involvement of key actors, especially MOH (National Malaria Control Program) and country health team at all levels, is an effective and efficient approach for project implementation. Regular mentorship and coaching during supportive supervision improves the quality of care provided for malaria in pregnancy. Ensuring availability of IPTp drugs and long-lasting insecticidal nets at health facilities are key to preventing malaria in pregnancy.
In conclusion the project met IPC objectives and achieved 80% Safe, Quality, Health Services score. Thus there was improved service delivery utilization.
The poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Health Workers &IPTp &Malaria in Pregnancy &Performance &Quality of Services Bill Brieger | 09 Nov 2017
Results of an evaluation of the Toolkit to Improve Early and Sustained Intermittent Preventive Treatment in Pregnancy (IPTp) Uptake in Mozambique and Madagascar
 Lalanirina Ravony, Elana Fiekowsky, Lisa Noguchi, Patricia P. Gomez, Jean Pierre Rakotovao, Eliane Razafimandimby, Armindo Tiago, Kathryn Smock, Arsene Ratsimbarisoa, Kristen Vibbert, and Robert Sellke shared their efforts to apply a toolkit to enable health providers to ensure better uptake of intermittent preventive treatment for malaria during antenatal clinics. As seen below, they presented their findings at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
Lalanirina Ravony, Elana Fiekowsky, Lisa Noguchi, Patricia P. Gomez, Jean Pierre Rakotovao, Eliane Razafimandimby, Armindo Tiago, Kathryn Smock, Arsene Ratsimbarisoa, Kristen Vibbert, and Robert Sellke shared their efforts to apply a toolkit to enable health providers to ensure better uptake of intermittent preventive treatment for malaria during antenatal clinics. As seen below, they presented their findings at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene.
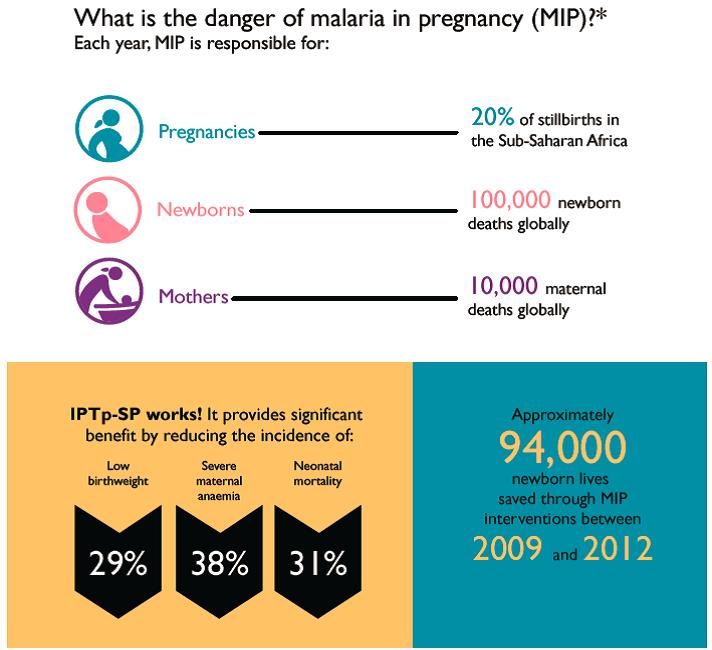
Malaria in pregnancy (MIP) is a leading cause of maternal and newborn morbidity and mortality; however uptake of intermittent preventive treatment in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP), an effective prevention tool, remains alarmingly low across sub-Saharan Africa, including Mozambique and Madagascar.
 The WHO 2012 policy recommendations to prevent MIP include early enrollment into antenatal care (ANC), accurate estimation of gestational age (GA) and administration of IPTp-SP during ANC visits beginning early in the second trimester, spaced at least one month apart. Preventing MIP remains a challenge in settings with inconsistent application of these recommendations and inadequate provider training in estimating GA.
The WHO 2012 policy recommendations to prevent MIP include early enrollment into antenatal care (ANC), accurate estimation of gestational age (GA) and administration of IPTp-SP during ANC visits beginning early in the second trimester, spaced at least one month apart. Preventing MIP remains a challenge in settings with inconsistent application of these recommendations and inadequate provider training in estimating GA.
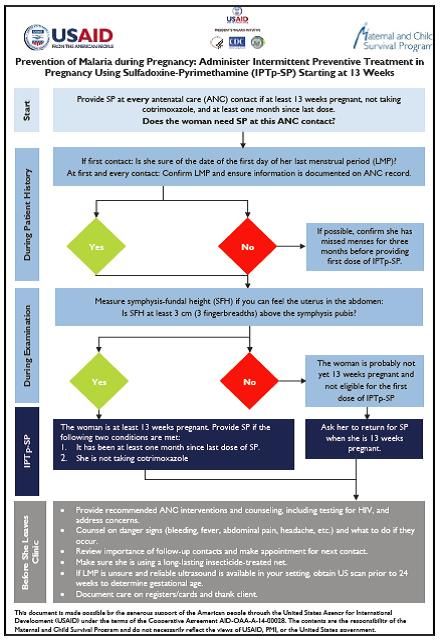 To improve adherence to these recommendations, a toolkit was designed which includes a job aid with an algorithm to guide providers during ANC visits to determine IPTp-SP eligibility. Twenty-four providers from 24 facilities in Madagascar and 29 providers from seven facilities in Mozambique were trained on use of the job aid and interviewed three months later about their experience.
To improve adherence to these recommendations, a toolkit was designed which includes a job aid with an algorithm to guide providers during ANC visits to determine IPTp-SP eligibility. Twenty-four providers from 24 facilities in Madagascar and 29 providers from seven facilities in Mozambique were trained on use of the job aid and interviewed three months later about their experience.
Individual providers were interviewed using a questionnaire to assess the clarity and utility to the job aid, and their opinions of the practicality of the orientation. Interviewers also gathered information on years of experience and clinical certification. All providers reported that the job aid reminded them to estimate GA and measure fundal height, which is particularly helpful since few women remember the date of their last menstrual period (LMP).
 Health workers also reported that the job helped them encourage the use of long-lasted insecticide treated nets, and reminded them of the proper timing to start IPTp-SP. We conclude that the toolkit is useful to prompt providers to calculate GA and offer IPTp as early as possible in the second trimester.
Health workers also reported that the job helped them encourage the use of long-lasted insecticide treated nets, and reminded them of the proper timing to start IPTp-SP. We conclude that the toolkit is useful to prompt providers to calculate GA and offer IPTp as early as possible in the second trimester.
Future potential directions include revision of all Toolkit components to reflect input from this evaluation, including development of a wall poster version to enhance readability, and inclusion of a pregnancy wheel to facilitate calculation of GA and estimated date of delivery.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Malaria in Pregnancy &Quality of Services Bill Brieger | 09 Nov 2017
Using the Antenatal Care Quality Improvement Tool and targeted training to strengthen ANC Services including MiP in Tanzania
 Malaria prevention in pregnancy (MIP) is a major component of antenatal services in endemic countries. Jasmine Chadewa, Dunstan Bishanga, Elaine Roman, Godlisten Martin, Kristen Vibbert, Lauren Borsa, Agrey Mbilinyi, Jeremie Zoungrana, and Hussein Kidanto describe how they applied a quality improvement tool to strengthen ANC and MIP services at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings follow:
Malaria prevention in pregnancy (MIP) is a major component of antenatal services in endemic countries. Jasmine Chadewa, Dunstan Bishanga, Elaine Roman, Godlisten Martin, Kristen Vibbert, Lauren Borsa, Agrey Mbilinyi, Jeremie Zoungrana, and Hussein Kidanto describe how they applied a quality improvement tool to strengthen ANC and MIP services at the 66th Annual Meeting of the American Society of Tropical Medicine and Hygiene. Their findings follow:
Malaria in Pregnancy (MiP) is a major, preventable cause of maternal morbidity and poor birth outcomes. In collaborations with partners, Tanzania’s National Malaria Control Program (NMCP) and the Reproductive and Child Health Unit has been working to promote the World Health Organization’s three-pronged approach to address the burden of MiP.
 A malaria training for 180 supervisors and 360 ANC providers from 221 health facilities was conducted in the Kagera and Mara regions. Updates included an orientation on MiP as well as malaria case management, screening, data management and ITN promotion.
A malaria training for 180 supervisors and 360 ANC providers from 221 health facilities was conducted in the Kagera and Mara regions. Updates included an orientation on MiP as well as malaria case management, screening, data management and ITN promotion.
Prior to the training, facility baseline assessments were conducted using the Ministry of Health, Community Development, Gender, Elderly and Children (MOHCDGEC) antenatal care quality improvement (ANC QI) tool to identify gaps in knowledge and skills of health providers to better target trainings to improving the quality of ANC services.
A second assessment took place six months post training. Both assessments included hospital, health facility and dispensary levels and included observation, interviews, record reviews and skills assessments.
 Results demonstrated that over 90% of the facilities scored below 30% across all categories in the overall baseline assessment with a high score of 35 %, while the 2nd assessment showed a large improvement with 40% of the facilities scoring below 30% and a high score of 70%.
Results demonstrated that over 90% of the facilities scored below 30% across all categories in the overall baseline assessment with a high score of 35 %, while the 2nd assessment showed a large improvement with 40% of the facilities scoring below 30% and a high score of 70%.
The ANC QI tool is effective in determining the impact of ANC health provider’s knowledge and skills to target training to improve ANC service quality.
The presentation was made possible through support provided to the USAID Boresha Afya Project, under the terms of the Cooperative Agreement AID-621-A-16-00003 by the President’s Malaria Initiative via the United States Agency for International Development (USAID), an inter-agency agreement with Centers for Disease Control and Prevention (CDC). The opinions expressed herein are those of the author(s) and do not necessarily reflect the views of the President’s Malaria Initiative via the US Agency for International Development.