Case Management &CHW &Training Bill Brieger | 31 Oct 2018
Improving Adherence to National Malaria Treatment Guidelines through a Low-Dose, High-Frequency Approach Targeting Village Malaria Workers in Selected Townships in Myanmar
 Ni Ni Aye, May Aung Lin, Saw Lwin, Khin Than Win, Kyan Khaing, Nu Nu Khin, Kyaw Myint Tun who are colleagues from Jhpiego, PMI Defeat Malaria Project, University Research Co., Myanmar Nurses and Midwives Association; and the USAID/US President’s Malaria Initiative, Myanmar
Ni Ni Aye, May Aung Lin, Saw Lwin, Khin Than Win, Kyan Khaing, Nu Nu Khin, Kyaw Myint Tun who are colleagues from Jhpiego, PMI Defeat Malaria Project, University Research Co., Myanmar Nurses and Midwives Association; and the USAID/US President’s Malaria Initiative, Myanmar  presented their experiences training village malaria workers on national malaria treatment guidelines at the 2018 Annual Meeting of the American Society of Tropical Medicine an Hygiene. Below are their findings.
presented their experiences training village malaria workers on national malaria treatment guidelines at the 2018 Annual Meeting of the American Society of Tropical Medicine an Hygiene. Below are their findings.
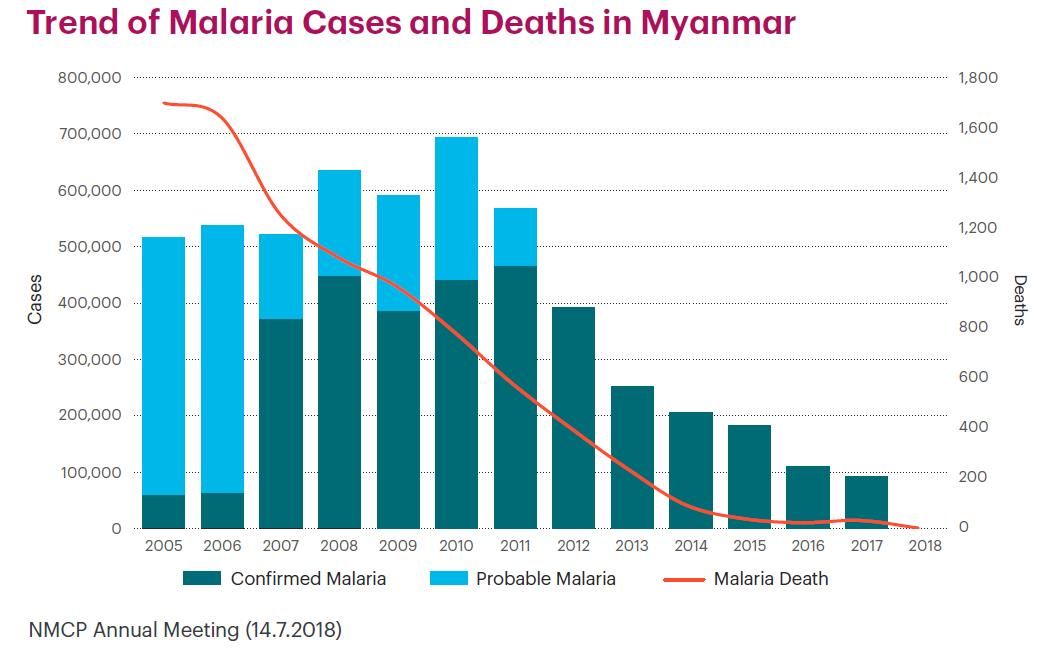
The Trend of Malaria Cases and Deaths in Myanmar has been steadily decreasing. PMI Defeat Malaria Project (October 2016–September 2021) wants to ensure that this trend continues.
 Project goals include reduce malaria burden, control artemisinin-resistant malaria in target area, and eliminate malaria in Myanmar. Specific Objectives are:
Project goals include reduce malaria burden, control artemisinin-resistant malaria in target area, and eliminate malaria in Myanmar. Specific Objectives are:
- Achieve universal coverage of at-risk populations
- Strengthen malaria surveillance system
- Enhance provider technical capacity
- Promote community and public and private-sector involvement in malaria control and elimination
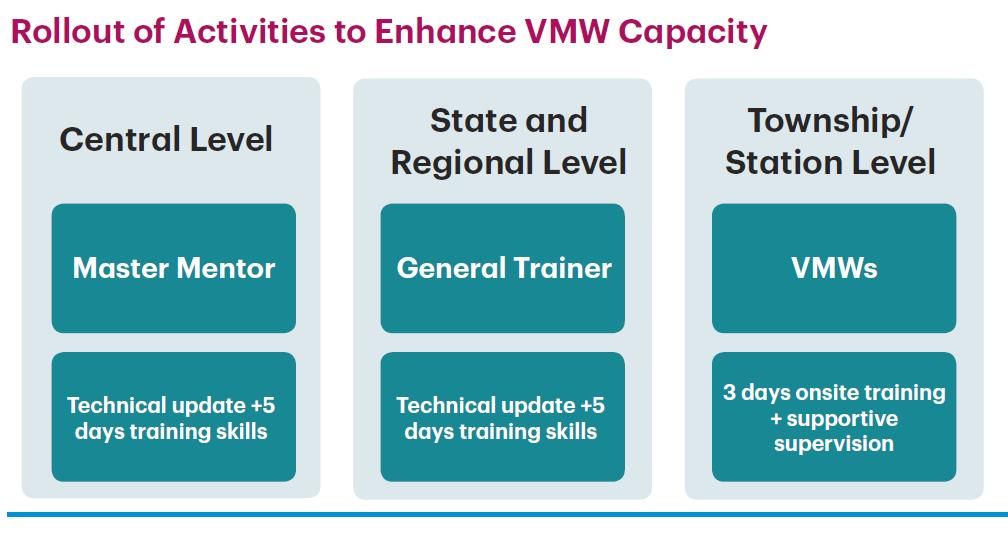 Capacity Development Strategy for Village Malaria Workers (VMWs) focused on Two townships with low adherence to National Malaria Treatment Guidelines (NTGs): Palaw Township with 38 Village Malaria Workers (VMWs) and Gwa Township with 39 VMWs. The project used a Competency-based low-dose, high-frequency (LDHF) training approach. There were Three sessions, one day/month during June, July, and August 2017.
Capacity Development Strategy for Village Malaria Workers (VMWs) focused on Two townships with low adherence to National Malaria Treatment Guidelines (NTGs): Palaw Township with 38 Village Malaria Workers (VMWs) and Gwa Township with 39 VMWs. The project used a Competency-based low-dose, high-frequency (LDHF) training approach. There were Three sessions, one day/month during June, July, and August 2017.
 Post-training follow-up used a Clinical audit result review during supportive supervision and monitoring visits. Data quality assessment and verification was performed by field teams and monthly reports examined.
Post-training follow-up used a Clinical audit result review during supportive supervision and monitoring visits. Data quality assessment and verification was performed by field teams and monthly reports examined.
The project also Conducted refresher training using LDHF approach for at least two doses followed by on-the-job training and regular supervision and monitoring. They Formulated culturally appropriate materials for areas like Palaw Township where different languages are spoken. A Job Aid on Benefits of Adherence to Antimalarial Drug was developed.
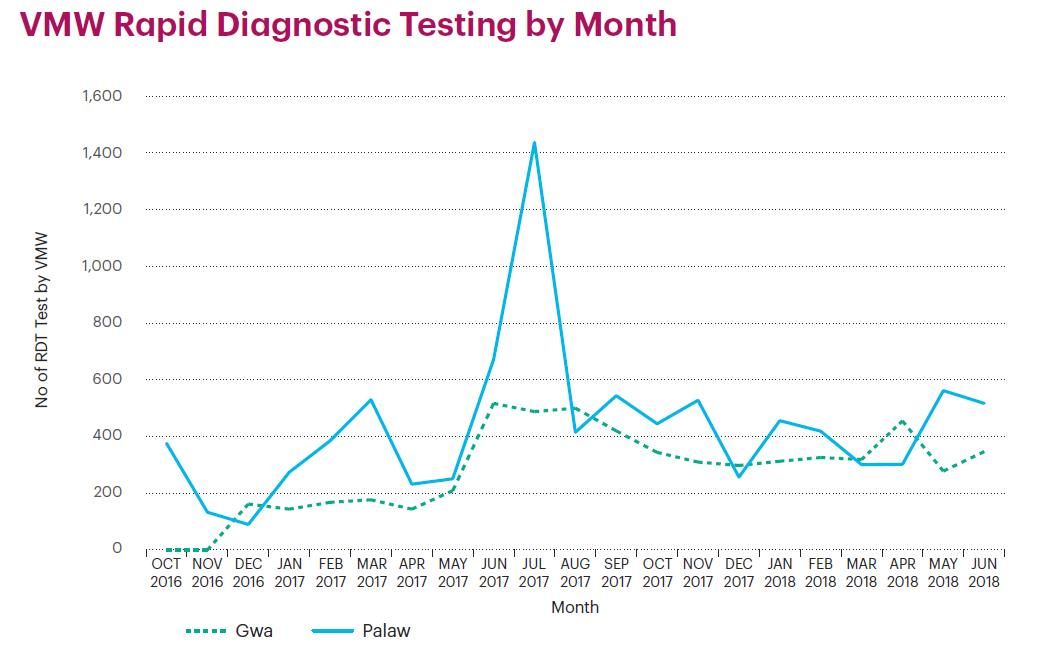 VMW Rapid Diagnostic Testing was observed by Month. There was an Improvement in VMW Knowledge Assessment Scores with a positive Post-training Assessment Knowledge of Malaria.
VMW Rapid Diagnostic Testing was observed by Month. There was an Improvement in VMW Knowledge Assessment Scores with a positive Post-training Assessment Knowledge of Malaria.
Post-training Assessment for RDT Competency also took place. 85-90% of 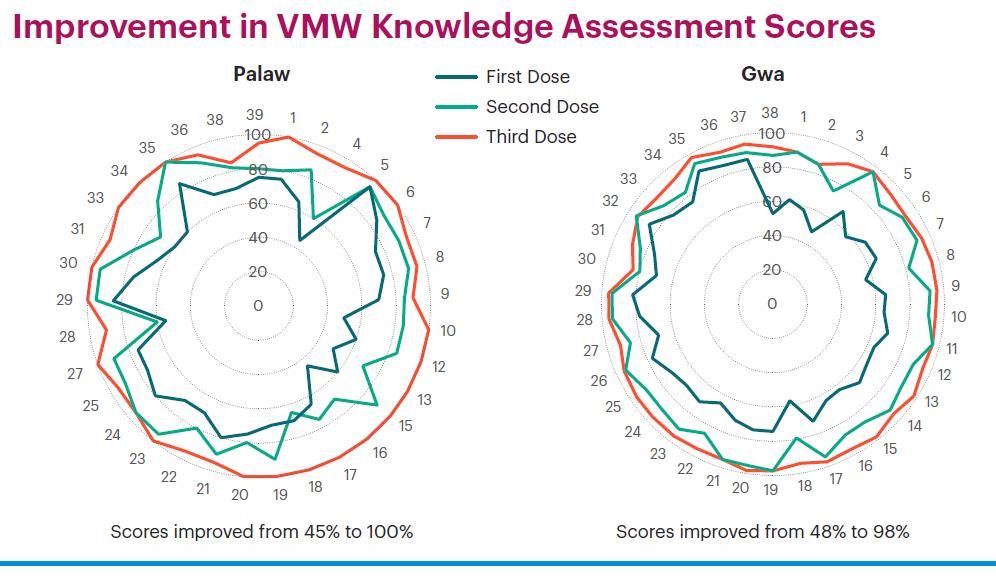 VMWs Told clients about blood testing and provided emotional support. 70-80% of VMWs Conducted RDT testing according to standards. 95-98% of VMWs Performed hand hygiene before and after rapid diagnostic test. 80-90% of VMWs Disposed used lancet immediately into safety box after use. 85-90% of VMWs Gave health education. Finally 80-90% Disposed of contaminated items appropriately and recorded test in malaria register, and 80% Used job aids/manual and provided correct treatment according to National Training Guidelines (NTGs).
VMWs Told clients about blood testing and provided emotional support. 70-80% of VMWs Conducted RDT testing according to standards. 95-98% of VMWs Performed hand hygiene before and after rapid diagnostic test. 80-90% of VMWs Disposed used lancet immediately into safety box after use. 85-90% of VMWs Gave health education. Finally 80-90% Disposed of contaminated items appropriately and recorded test in malaria register, and 80% Used job aids/manual and provided correct treatment according to National Training Guidelines (NTGs).
 In Conclusion, Improvement was seen in adherence to NTGs assessed as percent of uncomplicated malaria cases that received correct antimalarial treatment. VMWs Adhered to NTGs. In Gwa thus Increased from 72% to 100% and remained high. In Palaw this Stayed at 91% – 92% after training period. Therefore, the LDHF approach was appropriate for
In Conclusion, Improvement was seen in adherence to NTGs assessed as percent of uncomplicated malaria cases that received correct antimalarial treatment. VMWs Adhered to NTGs. In Gwa thus Increased from 72% to 100% and remained high. In Palaw this Stayed at 91% – 92% after training period. Therefore, the LDHF approach was appropriate for 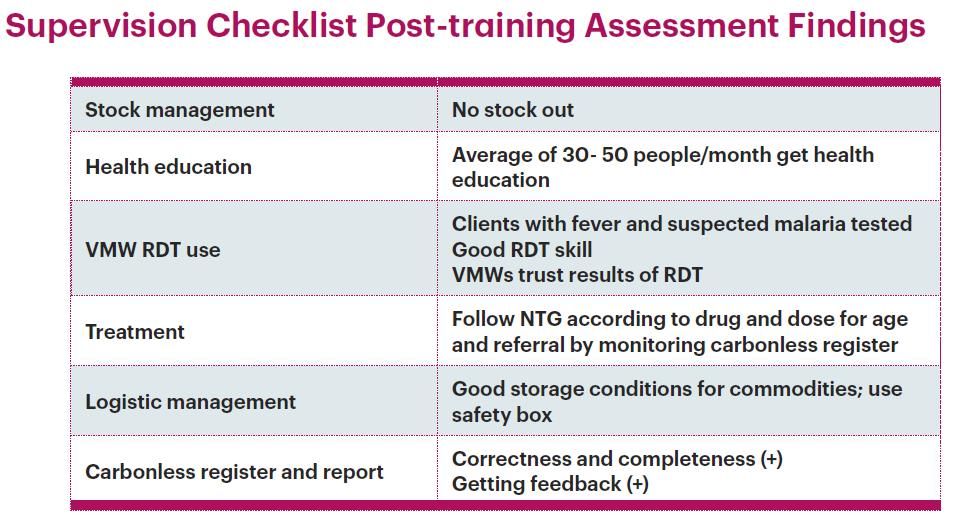 VMW capacity-building on protocol adherence in Gwa Township where there was no language barrier.
VMW capacity-building on protocol adherence in Gwa Township where there was no language barrier.
Next Steps include Conducting refresher training using LDHF approach for at least two doses followed by on-the-job training and regular supervision and monitoring. The project will Formulate culturally appropriate materials for areas like Palaw Township where different languages are spoken.
Community &Sahel &Seasonal Malaria Chemoprevention Bill Brieger | 31 Oct 2018
Seasonal Malaria Chemoprevention: An Effective Intervention for Reducing Malaria Morbidity and Mortality
![]() Moumouni Bonkoungou, Ousmane Badolo, Stanislas Nébié, Justin Tiendrebeogo, Mathurin Dodo, Thierry Ouedraogo, Youssouf Sawadogo, Danielle Burke, Bethany Arnold, William Brieger, and Gladys Tetteh of the USAID/Jhpiego Improving Malaria care Project and the Burkina Faso National Malaria Control Program presented implementation of the SMC program at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene as seen below.
Moumouni Bonkoungou, Ousmane Badolo, Stanislas Nébié, Justin Tiendrebeogo, Mathurin Dodo, Thierry Ouedraogo, Youssouf Sawadogo, Danielle Burke, Bethany Arnold, William Brieger, and Gladys Tetteh of the USAID/Jhpiego Improving Malaria care Project and the Burkina Faso National Malaria Control Program presented implementation of the SMC program at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene as seen below.
 Malaria remains a serious problem in Burkina Faso, a high burden country. Data from the 2016 Health Management Information System reports 9,852,097 malaria cases, and 4,440 malaria Deaths. Malaria accounts for 43.38% of Outpatient department visits, 44.63% of Hospitalizations and 21.84% Deaths. The burden of Malaria is highest during the months of July– October. During these months, malaria transmission is intense due to heavy rainfall and intensive biting behavior
Malaria remains a serious problem in Burkina Faso, a high burden country. Data from the 2016 Health Management Information System reports 9,852,097 malaria cases, and 4,440 malaria Deaths. Malaria accounts for 43.38% of Outpatient department visits, 44.63% of Hospitalizations and 21.84% Deaths. The burden of Malaria is highest during the months of July– October. During these months, malaria transmission is intense due to heavy rainfall and intensive biting behavior
 Seasonal Malaria Chemoprevention (SMC) is the Intermittent administration of full treatment of antimalarial medicines to children under 5 (age 3-59 months) in areas of high seasonal transmission. It is an important malaria elimination strategy in the West African Sahel. Effective prevention intervention takes place where Malaria transmission is concentrated within a high transmission season. The bulk of clinical malaria cases (> 60%) occur during short rainy season over 4 months.
Seasonal Malaria Chemoprevention (SMC) is the Intermittent administration of full treatment of antimalarial medicines to children under 5 (age 3-59 months) in areas of high seasonal transmission. It is an important malaria elimination strategy in the West African Sahel. Effective prevention intervention takes place where Malaria transmission is concentrated within a high transmission season. The bulk of clinical malaria cases (> 60%) occur during short rainy season over 4 months.
 SMC Implementation started when Burkina Faso adopted SMC in 2013 as key part of National Malaria control strategy. SMC uses Sulfadoxine-pyrimethamine plus amodiaquine (SP+AQ). Four monthly doses are given to children 3?59 months old from July to October by community health workers and other volunteers.
SMC Implementation started when Burkina Faso adopted SMC in 2013 as key part of National Malaria control strategy. SMC uses Sulfadoxine-pyrimethamine plus amodiaquine (SP+AQ). Four monthly doses are given to children 3?59 months old from July to October by community health workers and other volunteers.
The Improving Malaria Care (IMC) project is implemented by Jhpiego and funded by the U.S. President’s Malaria Initiative (PMI). IMC supports National Malaria Control Program (NMCP) to improve quality of malaria prevention, diagnosis and treatment. NMCP expanded SMC implementation to 7 districts in 2014 and then 59 districts in 2017.
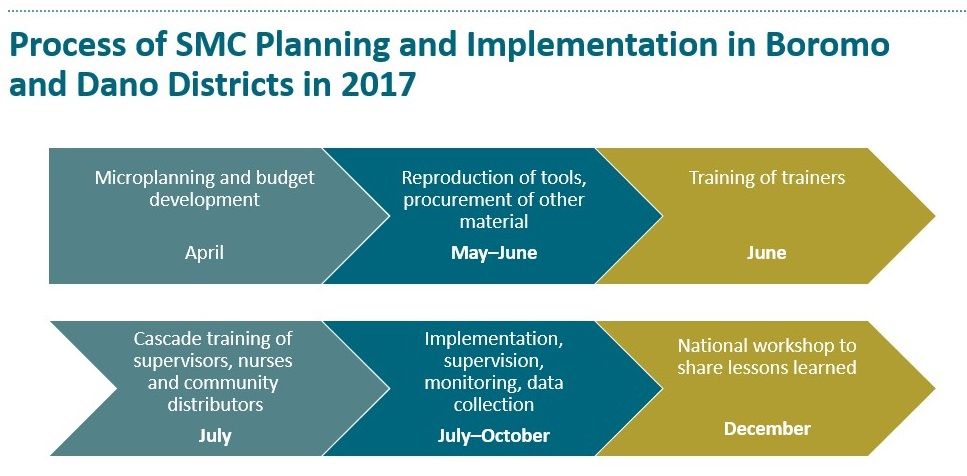 Process of SMC Planning and Implementation in Boromo and Dano Districts in 2017 provides an example of how the program works. Treatment Coverage during the 2017 campaign treated 58,246 children in Boromo District and 50,007 children in Dano, or 97.3% of target population. The attached flow chart shows the Process of SMC Planning and Implementation in Boromo and Dano Districts in 2017. Microplanning is an important component. Reviewing lessons learned
Process of SMC Planning and Implementation in Boromo and Dano Districts in 2017 provides an example of how the program works. Treatment Coverage during the 2017 campaign treated 58,246 children in Boromo District and 50,007 children in Dano, or 97.3% of target population. The attached flow chart shows the Process of SMC Planning and Implementation in Boromo and Dano Districts in 2017. Microplanning is an important component. Reviewing lessons learned 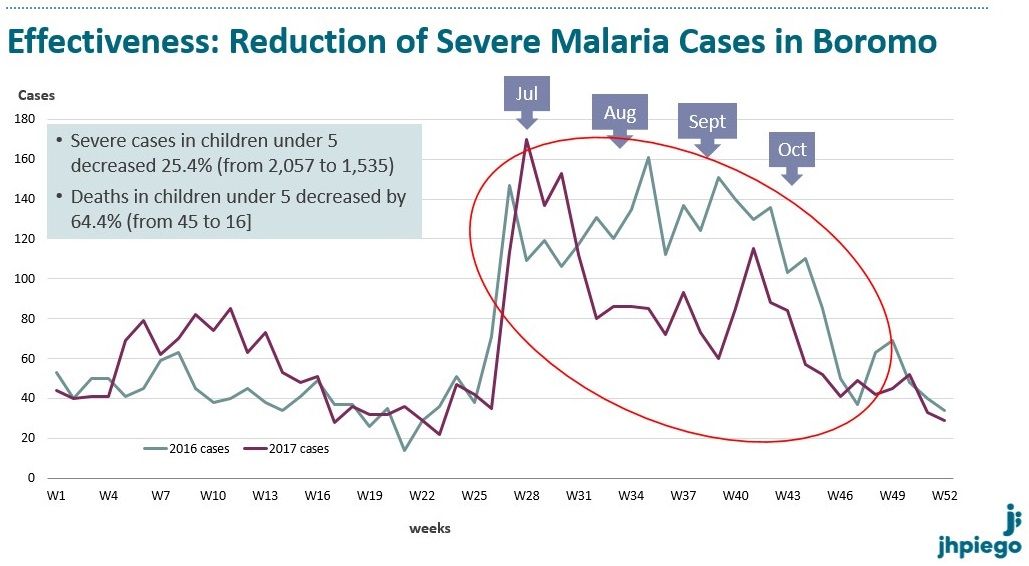 was crucial for planning SMC in 2018. The attached charts show a Reduction of Severe Malaria Cases in Boromo over the implementation period of SMC as well as a Reduction of Severe Malaria Cases in Dano.
was crucial for planning SMC in 2018. The attached charts show a Reduction of Severe Malaria Cases in Boromo over the implementation period of SMC as well as a Reduction of Severe Malaria Cases in Dano.
These successes were or without challenges to SMC Scale-up in Burkina Faso. It is difficult access to some villages during the 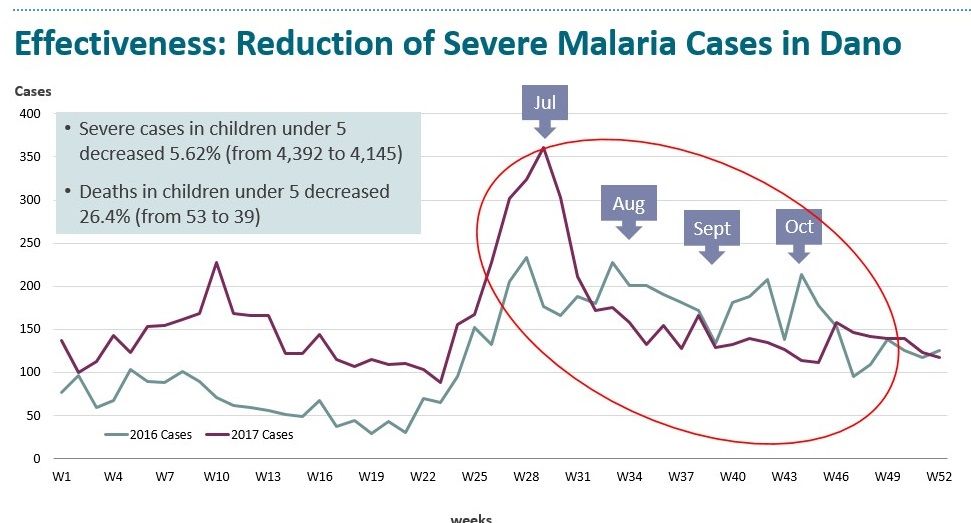 rainy season. Limiting SMC administration to children below 5 years of age makes some parents with older children unhappy, and they also demand the service. As of 2017 there was lack of resources to cover all districts.
rainy season. Limiting SMC administration to children below 5 years of age makes some parents with older children unhappy, and they also demand the service. As of 2017 there was lack of resources to cover all districts.
 In conclusion, the NMCP continues to scale up SMC to reach all eligible children with support of implementing partners/projects like IMC. Moving forward, the NMCP aims to increase efficiency of SMC campaigns, achieve effectiveness of intervention, mitigate known challenges, and anticipate new challenges.
In conclusion, the NMCP continues to scale up SMC to reach all eligible children with support of implementing partners/projects like IMC. Moving forward, the NMCP aims to increase efficiency of SMC campaigns, achieve effectiveness of intervention, mitigate known challenges, and anticipate new challenges.
 Our partners recommend that to improve coverage, safety, efficacy and health impact we should strengthen interpersonal communication with communities, conduct independent monitoring, optimize coordination of partners’ interventions, and synchronize with neighboring countries.
Our partners recommend that to improve coverage, safety, efficacy and health impact we should strengthen interpersonal communication with communities, conduct independent monitoring, optimize coordination of partners’ interventions, and synchronize with neighboring countries.
Acknowledgments: US President’s Malaria Initiative, United States Agency for International Development, Burkina Faso Ministry of Health, National Malaria Control Program
Case Management &Health Information &IPTp &Mortality &Quality of Services Bill Brieger | 31 Oct 2018
Improving Malaria Care Project Contribution in Transforming Malaria Control for Vulnerable Populations in Burkina Faso
![]() Mathurin Dodo, Ousmane Badolo, Stanislas Nebie, Youssouf Sawadogo, Thierry Ouedraogo, Moumouni Bonkoungou, Youssouf Zongo, Maria Gouem, Danielle Burke, Gladys Tetteh, Lolade Oseni, Linda Fogarty, and William Brieger of Jhpiego and the USAID Improving malaria Care Project in Burkina Faso shared the status of malaria control efforts at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. The focus on vulnerable populations is shared below.
Mathurin Dodo, Ousmane Badolo, Stanislas Nebie, Youssouf Sawadogo, Thierry Ouedraogo, Moumouni Bonkoungou, Youssouf Zongo, Maria Gouem, Danielle Burke, Gladys Tetteh, Lolade Oseni, Linda Fogarty, and William Brieger of Jhpiego and the USAID Improving malaria Care Project in Burkina Faso shared the status of malaria control efforts at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. The focus on vulnerable populations is shared below.
Burkina Faso in 2010-2012 experienced poor capacity in malaria prevention and control, Malaria fatality rate was high:
- Pregnant women: 0.71% in 2010 and 0.66% in 2012
- Children under 5: 2.8% in 2010 and 2.7% in 2012
Improving Malaria Care (IMC) Project funded by USAID/President’s Malaria Initiative, began in 2013. IMC supports National Malaria Control Program to improve prevention and case
Management. IMC’s Strategies include the following:
- Update national malaria prevention and case management guidelines
- Strengthen health care provider capacity
- Align malaria training package with revised guidelines
- Strengthen national malaria health management information system (HMIS)
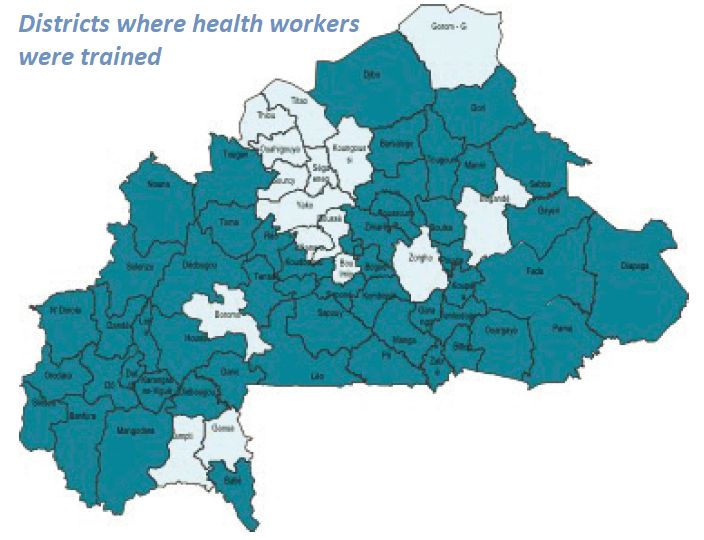 IMC together with the National Malaria Control Program has been strengthening Health Care Provider Capacity. 54 health districts have been covered by IMC direct support where 1819 providers were trained. Training reached 185 trainers/supervisors on revised training Modules who then trained 1,819 health care providers from 1,349 health facilities in 54 districts on new guidelines
IMC together with the National Malaria Control Program has been strengthening Health Care Provider Capacity. 54 health districts have been covered by IMC direct support where 1819 providers were trained. Training reached 185 trainers/supervisors on revised training Modules who then trained 1,819 health care providers from 1,349 health facilities in 54 districts on new guidelines
 After training 58 supervisors rolled out quality improvement (QI) systems. They oriented 897 providers from referral hospitals on new severe case management guidelines. Formative Supervision, Performance and Quality Improvement efforts were based on an improved malaria supervision guide and tools. Post-training supervision reached each provider. Specifically, malaria supervisions occurred twice a year.
After training 58 supervisors rolled out quality improvement (QI) systems. They oriented 897 providers from referral hospitals on new severe case management guidelines. Formative Supervision, Performance and Quality Improvement efforts were based on an improved malaria supervision guide and tools. Post-training supervision reached each provider. Specifically, malaria supervisions occurred twice a year.
The quality improvement approach, SBM-R® (Standards-Based Management and Recognition) approach, was implemented in 6 regions, 28 districts. Organized data review and validation workshop in 67 districts were another aspect of quality improvement. To sustain quality improvement, IMC conducted 2-day quality assessments and guided developed DQI implementation plans.
 Social Behavior Change Communication was a central component of IMC. IMC conducted 13 regional advocacy workshops on malaria issues. The project developed and broadcast 2 malaria spots through 27 media, revised 5 diagnostic and case management job aids, distributed 7,440 job aids to health facilities, and reached 792,660 people through community activities and sensitization sessions
Social Behavior Change Communication was a central component of IMC. IMC conducted 13 regional advocacy workshops on malaria issues. The project developed and broadcast 2 malaria spots through 27 media, revised 5 diagnostic and case management job aids, distributed 7,440 job aids to health facilities, and reached 792,660 people through community activities and sensitization sessions
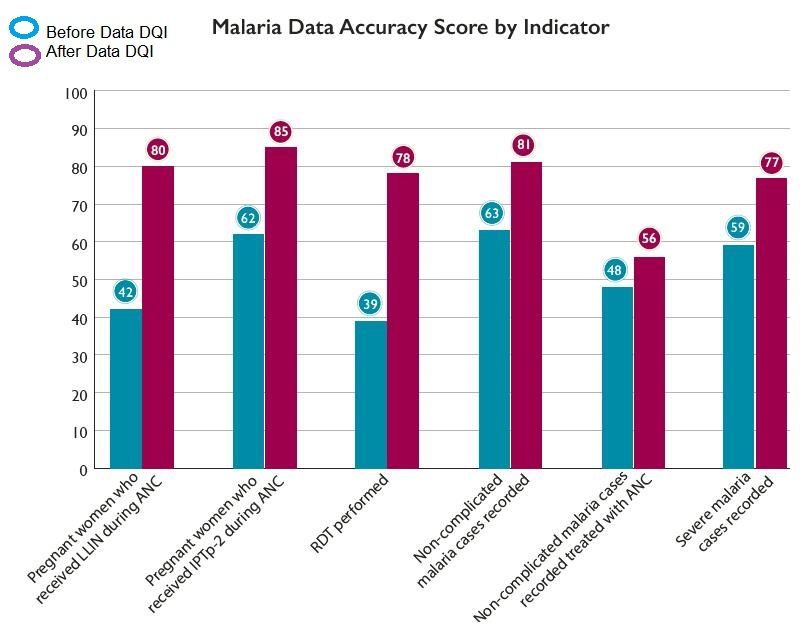
 IMC Strengthened National Malaria HMIS. This included training 1,300 (72%) health workers to enter data into monthly reporting forms. Also trained were 326 data managers on HMIS and data use for decisionmakers. The malaria data collection system was integrated into national HMIS using DHIS2. To facilitate this the national HMIS manual was revised and distributed. Data Quality was improved through malaria data review and validation at district levelUltimately these interventions resulted in Improved Malaria Services. More confirmed simple malaria cases received artemisinin-based combination therapy (65% in 2013 to 90% in 2017). More women received three doses of IPTp3 (14% in 2014 to 51% in June 2018). More suspected cases tested for malaria (65% in 2013 to 96% 2017). More women received insecticide-treated nets at antenatal care. There was Better accuracy in reporting of malaria key indicators.
IMC Strengthened National Malaria HMIS. This included training 1,300 (72%) health workers to enter data into monthly reporting forms. Also trained were 326 data managers on HMIS and data use for decisionmakers. The malaria data collection system was integrated into national HMIS using DHIS2. To facilitate this the national HMIS manual was revised and distributed. Data Quality was improved through malaria data review and validation at district levelUltimately these interventions resulted in Improved Malaria Services. More confirmed simple malaria cases received artemisinin-based combination therapy (65% in 2013 to 90% in 2017). More women received three doses of IPTp3 (14% in 2014 to 51% in June 2018). More suspected cases tested for malaria (65% in 2013 to 96% 2017). More women received insecticide-treated nets at antenatal care. There was Better accuracy in reporting of malaria key indicators.
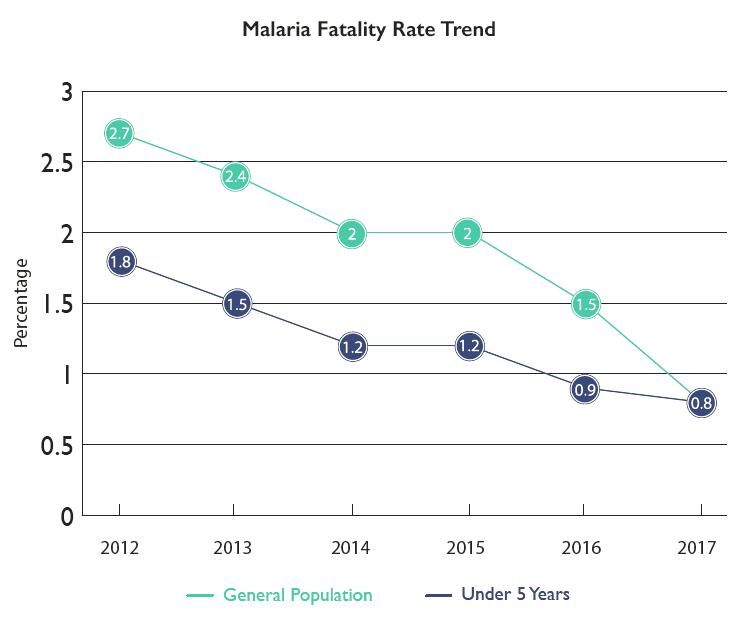
 Improved services led to decreased national malaria fatality rate. In the General population there was a decrease in malaria deaths of 34% and a decrease in overall fatality rate by 47%. Among pregnant women there was a decrease in malaria deaths by 91% and a decrease in malaria fatality rate by 93%. For Children under 5 years of age, there was a decrease in malaria deaths by 34% and a decrease in fatality rate 48%
Improved services led to decreased national malaria fatality rate. In the General population there was a decrease in malaria deaths of 34% and a decrease in overall fatality rate by 47%. Among pregnant women there was a decrease in malaria deaths by 91% and a decrease in malaria fatality rate by 93%. For Children under 5 years of age, there was a decrease in malaria deaths by 34% and a decrease in fatality rate 48%
 In conclusion the IMC Project Contributed to Lives Saved in Burkina Faso. IMC supported health delivery sites in Burkina Faso (Jan 2014 -Sep 2017). As a result the health system was able to Distribute 33,566,671 courses of artemisinin-based combination therapy. IMC provided 2,175,648 pregnant women with intermittent preventive treatment 2nd dose and distributed 1,146,185 nets to pregnant women during antenatal care visit. These interventions averted estimated 150,390 malaria deaths and 12,866,271 DALYs (Disability-Adjusted Life Years calculated using PSI Impact calculator. 1 DALY=1 lost year of “healthy” life.)
In conclusion the IMC Project Contributed to Lives Saved in Burkina Faso. IMC supported health delivery sites in Burkina Faso (Jan 2014 -Sep 2017). As a result the health system was able to Distribute 33,566,671 courses of artemisinin-based combination therapy. IMC provided 2,175,648 pregnant women with intermittent preventive treatment 2nd dose and distributed 1,146,185 nets to pregnant women during antenatal care visit. These interventions averted estimated 150,390 malaria deaths and 12,866,271 DALYs (Disability-Adjusted Life Years calculated using PSI Impact calculator. 1 DALY=1 lost year of “healthy” life.)
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID) under Cooperative Agreement No. AID-624-A-13-00010 and the President’s Malaria Initiative (PMI). The contents are the responsibility of the authors and do not necessarily reflect the views of USAID, PMI or the United States Government.
Ebola &Infection Prevention Bill Brieger | 30 Oct 2018
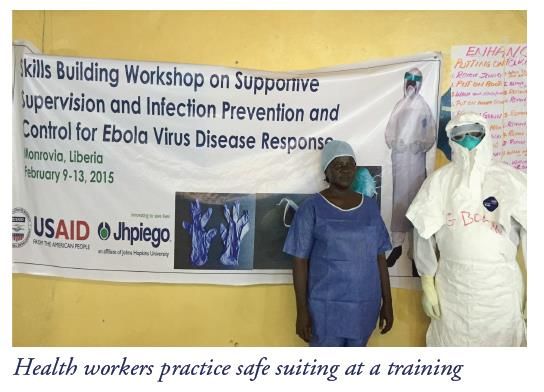
Institutionalizing Infection Prevention and Control: Post-Ebola Experience in Liberian Health Facilities
 Allyson R. Nelson, Anne Fiedler,Topian Zikeh, Nancy Moses, Chandrakant Ruparelia, Lolade Oseni, Mantue Reeves, and Birhanu Getahun presented the work of the Maternal and Child Survival Project in preventing infection among health workers during Ebola and other infectious disease outbreaks. Their efforts are shared below.
Allyson R. Nelson, Anne Fiedler,Topian Zikeh, Nancy Moses, Chandrakant Ruparelia, Lolade Oseni, Mantue Reeves, and Birhanu Getahun presented the work of the Maternal and Child Survival Project in preventing infection among health workers during Ebola and other infectious disease outbreaks. Their efforts are shared below.
 Ebola virus disease (EVD) outbreak in 2014–2015 affected an estimated 4% of the Liberian health workforce. 372 health workers contracted EVD, and 184 died. EVD outbreak and transmission between health care workers and clients highlighted critical gaps in health facilities, especially infection prevention (IPC) practices including waste, water, and triage infrastructure.
Ebola virus disease (EVD) outbreak in 2014–2015 affected an estimated 4% of the Liberian health workforce. 372 health workers contracted EVD, and 184 died. EVD outbreak and transmission between health care workers and clients highlighted critical gaps in health facilities, especially infection prevention (IPC) practices including waste, water, and triage infrastructure.
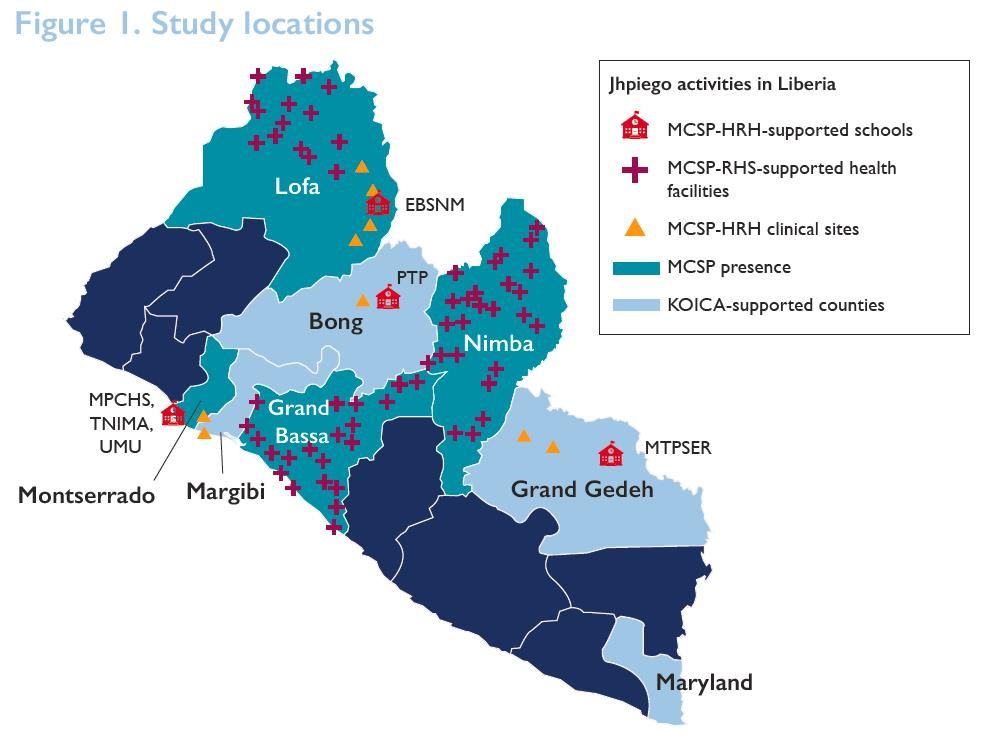
 Liberia’s ministry of health (MOH), with support from Jhpiego and other partners, developed and introduced IPC standards in 2015. Through funding from the Office of U.S. Foreign Disaster Assistance (OFDA), Korea International Cooperation Agency (KOICA), and the United States Agency for International Development’s Maternal and Child Survival Program (MCSP), Jhpiego worked with the MOH to achieve and maintain adherence to IPC standards in over 200 health facilities from 2015 to 2017.
Liberia’s ministry of health (MOH), with support from Jhpiego and other partners, developed and introduced IPC standards in 2015. Through funding from the Office of U.S. Foreign Disaster Assistance (OFDA), Korea International Cooperation Agency (KOICA), and the United States Agency for International Development’s Maternal and Child Survival Program (MCSP), Jhpiego worked with the MOH to achieve and maintain adherence to IPC standards in over 200 health facilities from 2015 to 2017.
 Capacity-building was central to addressing the problem. The team identified critical gaps in skills, infrastructure, supplies hindering adherence to IPC standards. They developed and rolled out standard operating procedures for clinical and nonclinical settings.
Capacity-building was central to addressing the problem. The team identified critical gaps in skills, infrastructure, supplies hindering adherence to IPC standards. They developed and rolled out standard operating procedures for clinical and nonclinical settings.
Partners provided IPC supplies including personal protective equipment (PPE), 90 hand hygiene buckets, Soap, Gloves, 50 waste containers, Rain boots, and Sharps containers.
 Capacity building included Training (clinical and support personnel). 278 existing health facility staff members as IPC focus points for daily monitoring (OFDA) were trained. Additionally 1,065 health facility staff were trained in Keep Safe Keep Serving IPC and emergency response training (OFDA). Onsite IPC management teams were established in 210 facilities (KOICA and MCSP). Also health workers were offered onsite refresher trainings.
Capacity building included Training (clinical and support personnel). 278 existing health facility staff members as IPC focus points for daily monitoring (OFDA) were trained. Additionally 1,065 health facility staff were trained in Keep Safe Keep Serving IPC and emergency response training (OFDA). Onsite IPC management teams were established in 210 facilities (KOICA and MCSP). Also health workers were offered onsite refresher trainings.
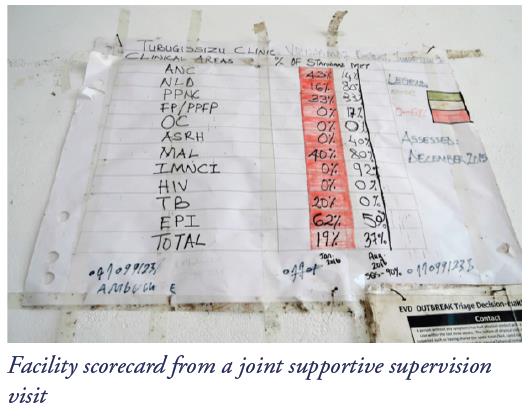 Supportive supervision, mentoring, and coaching were capacity building interventions. 50 district health officers and supervisors were trained in eight counties in supportive supervision, mentoring, and coaching (OFDA). They co-conducted, with district and county health staff, 7,980 weekly and 2,280 monthly supportive supervision visits (OFDA). IPC practices were monitored against the MOH’s IPC minimum standards tool monthly, with scoring, feedback to clinicians and supervisors, and development of action plans for improvement of gaps. Onsite mentoring and coaching was provided on adherence using IPC minimum standards tool at least four times yearly (KOICA and MCSP).
Supportive supervision, mentoring, and coaching were capacity building interventions. 50 district health officers and supervisors were trained in eight counties in supportive supervision, mentoring, and coaching (OFDA). They co-conducted, with district and county health staff, 7,980 weekly and 2,280 monthly supportive supervision visits (OFDA). IPC practices were monitored against the MOH’s IPC minimum standards tool monthly, with scoring, feedback to clinicians and supervisors, and development of action plans for improvement of gaps. Onsite mentoring and coaching was provided on adherence using IPC minimum standards tool at least four times yearly (KOICA and MCSP).
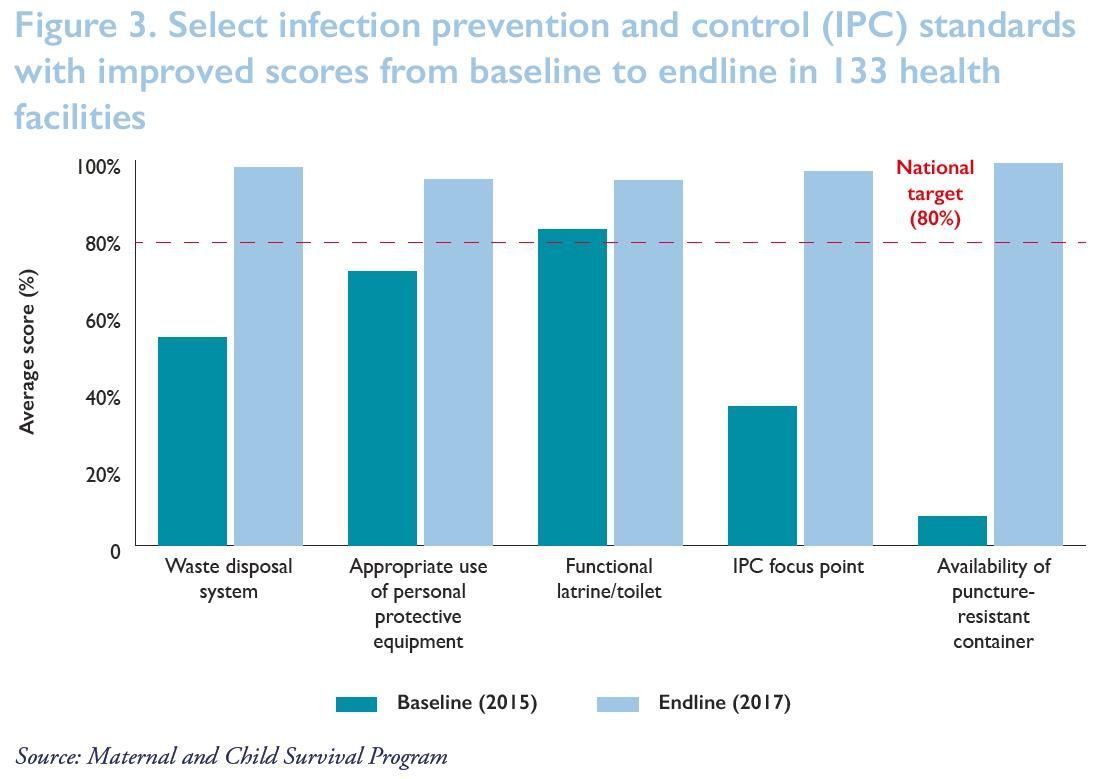
 As a result of the intervention Clinicians and support personnel at program-supported health care facilities adopted, adhered to, and maintained proper IPC practices. This enabled them to provide safe services and evidenced by IPC scores from the Safe, Quality Health Services IPC standards tool. Out of 131 health facilities at endline 99% improved their waste disposal, particularly the availability and use of puncture-resistant sharps containers for the safety of cleaning staff. All (100%) had in place and were using a clear protocol for management and disposal of waste. 98% were segregating waste for safe disposal and management to avoid contamination and spread of infectious disease. 94% had a functional latrine/toilet. All (100%) had operational IPC focus points ensuring adherence to IPC practices. In 95%, staff were regularly using risk-appropriate personal protective equipment during routine care.
As a result of the intervention Clinicians and support personnel at program-supported health care facilities adopted, adhered to, and maintained proper IPC practices. This enabled them to provide safe services and evidenced by IPC scores from the Safe, Quality Health Services IPC standards tool. Out of 131 health facilities at endline 99% improved their waste disposal, particularly the availability and use of puncture-resistant sharps containers for the safety of cleaning staff. All (100%) had in place and were using a clear protocol for management and disposal of waste. 98% were segregating waste for safe disposal and management to avoid contamination and spread of infectious disease. 94% had a functional latrine/toilet. All (100%) had operational IPC focus points ensuring adherence to IPC practices. In 95%, staff were regularly using risk-appropriate personal protective equipment during routine care.
Lessons learned from the intervention showed the importance of the following efforts:
- Comprehensive support is needed to improve adherence to infection prevention and control (IPC) standard practices:
- Capacity-building among health facility staff
- Infrastructure upgrades
- Provision/availability of IPC supplies
- To maintain that adherence after the immediate threat has passed and thus mitigate potential future outbreaks, health facilities need:
- Continuous hands-on mentoring
- Upgraded IPC infrastructure for reproductive, maternal, newborn, child, and adolescent health services
- Changes in behavior and attitudes of health facility staff
- Regular and rigorous data collection and feedback
 This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Abbreviations: EBSNM, Esther Bacon School of Nursing and Midwifery; HRH, Human Resources for Health; KOICA, Korea International Cooperation Agency; MCSP, Maternal and Child Survival Program; MPCHS, Mother Patern College of Health Sciences; MTPSER, Midwifery Training Program-Southeastern Region; PTP, Phebe Paramedical Training Program; RHS, Restoration of Health Services; TNIMA, Tubman National Institute of Medical Arts; UMU, United Methodist University
Case Management &Health Information &Procurement Supply Management Bill Brieger | 30 Oct 2018
One SMS Saves Lives in Madagascar
Haja Andriamiharisoa, Eliane Razafimandimby, Jean Pierre Rakotovao, Jean Eugene Injerona, Zo Harifetra, Lalanirina H. Ravony, Rado Randriamboavonjy, Jocelyn Razafindrakoto, and Laurent Kapesa have been working with the USAID Maternal and Child Survival Program. At the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene they presented their experiences on “Improving Procurement and Redeployment of Malaria Commodities Using SMS and Web Mapping at a District Level in Madagascar,” and are also sharing via this posting.
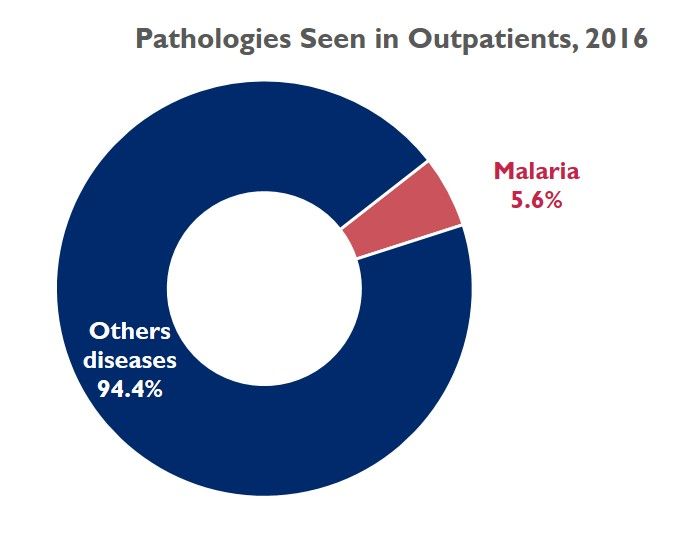 Malaria is a public health problem in Madagascar. In 2016, the frequency of diseases at health center level, places malaria at the 4th cause of hospital morbidity and mortality. Out of about 30 thirty diseases, malaria accounts for 5.6% of all cases.
Malaria is a public health problem in Madagascar. In 2016, the frequency of diseases at health center level, places malaria at the 4th cause of hospital morbidity and mortality. Out of about 30 thirty diseases, malaria accounts for 5.6% of all cases.
Health facilities often experience commodity stock-outs of products used for malaria prevention and case management. The existing logistics reporting system does not allow for macro or micro views of the monthly stock situation at the health facility level, which inhibits rapid decision-making.
 On January 2018, implementation of a fast data collection system and easy-to-use data visualization began. The tool was based on the use of SMS and web mapping to map the level of monthly keys stock of commodities. The data are sent by providers at facility level via structured SMS and are published by a web server by a web mapping process. Note that sending a monthly SMS costs 9 US cents per facility. Providers at 773 health facilities in 16 regions of Madagascar sent monthly SMS (each message cost $0.09) with ART, ACT, and ITN stock levels.
On January 2018, implementation of a fast data collection system and easy-to-use data visualization began. The tool was based on the use of SMS and web mapping to map the level of monthly keys stock of commodities. The data are sent by providers at facility level via structured SMS and are published by a web server by a web mapping process. Note that sending a monthly SMS costs 9 US cents per facility. Providers at 773 health facilities in 16 regions of Madagascar sent monthly SMS (each message cost $0.09) with ART, ACT, and ITN stock levels.
- Sample message: “Please send the quantity in stock at the end of month in: ART, ACT, ITN.”
- Structure like: “palu csbcode year month ART ACT ITN. Thank you.”
- Sample of answer received: “palu 520241031 D A 200 25 0”
 Thus was created an easy-to-use tool from data received. It was free to use, and no password was needed. The SMS is simple and short (of 40 forty characters, composed of:
Thus was created an easy-to-use tool from data received. It was free to use, and no password was needed. The SMS is simple and short (of 40 forty characters, composed of:
- “palu” diminutive of malaria so that the system is ready for data collection from other cases
- the health facility code : 520241031
- year : here D : as project has implemented sms data collecting system since 2015 = A
- month : here A that means January
- stock of Injectable Artesunate (ART) : 200
- stock of tablet for Artemisinin–based combination therapy (ACT) : 25
- stock of Insecticide Treated Nets (ITN) : 0
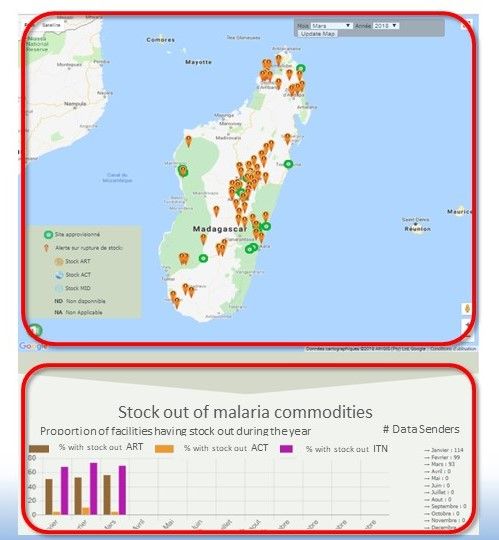
 Providers send SMS after completing the Monthly Activity Report. (CSB = Centre de Santé de Base, or basic health center). The received data are then displayed as web mapping on a Google map background, embedded on a web page. From this screen shot, The page displays a map of stock outs for the selected month, and monthly charts of the stock status of the three commodities. Accessing this website, is open, without restriction.
Providers send SMS after completing the Monthly Activity Report. (CSB = Centre de Santé de Base, or basic health center). The received data are then displayed as web mapping on a Google map background, embedded on a web page. From this screen shot, The page displays a map of stock outs for the selected month, and monthly charts of the stock status of the three commodities. Accessing this website, is open, without restriction.
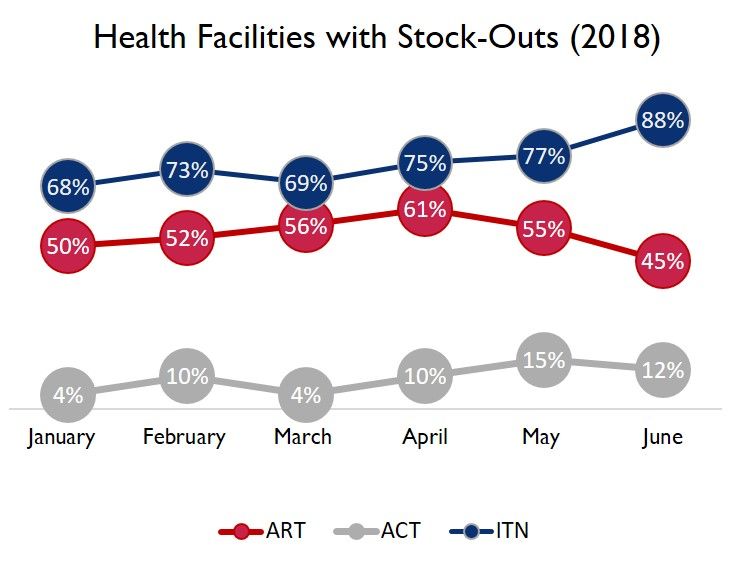
From the end of January to the end of June 2018, a hundred health facilities sent SMS each month. The data we received shows that on average:
- 75% Average stock-out of ITN
- 53% Average stock-out of ART
- 9% Average stock-out of ACT
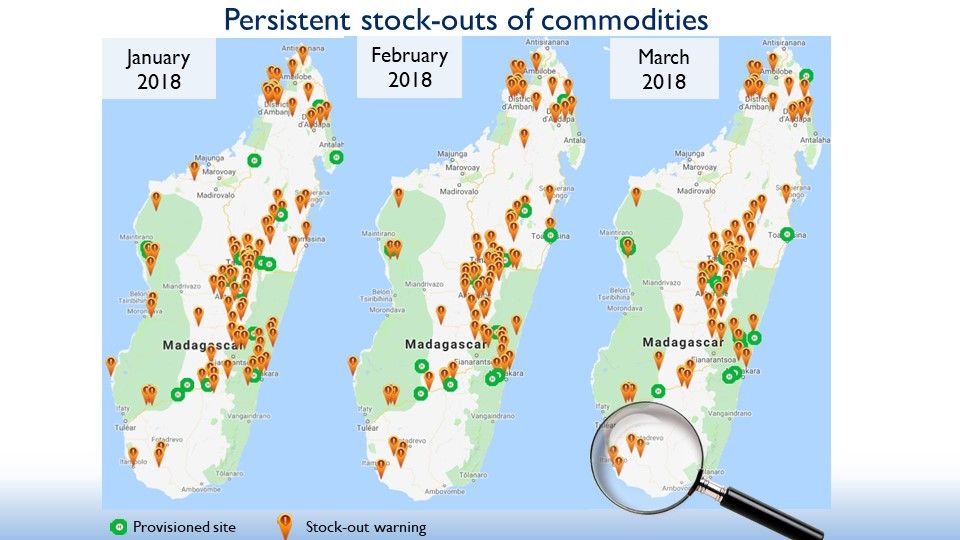 The attached three-map picture provides a broad view from three screenshots of the system, showing the evolution of stock-outs at a facility level
The attached three-map picture provides a broad view from three screenshots of the system, showing the evolution of stock-outs at a facility level
- Each point represents health facilities:
- When the dot is green, this means that the 03 commodities are available in stock
- When in brown, at least one of the 03 elements is unavailable
- At first sight, there are more stockouts than stock availability and a tendency of the reduction of green points over the months
- Appropriate decision-making would change the points of the map of the following months to green
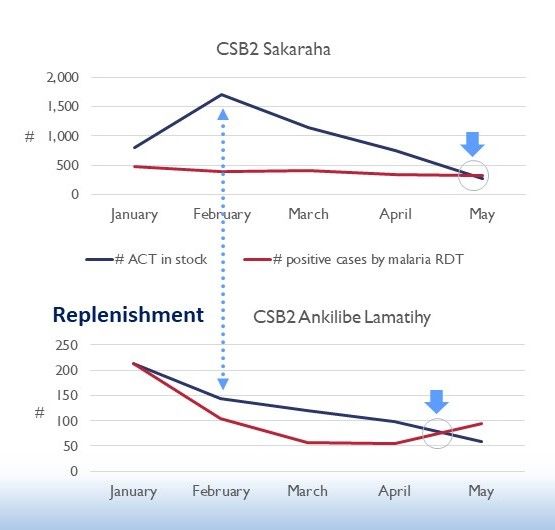 After this broad view of the country’s overall situation and given the large number of facilities with out of stock, an emergency supply for all districts was done for some medicine since February 2018. Based on maps and stats, we could improve our interventions at a CSB level through rapid and adequate decision-making as in the supply of ITN and ART.
After this broad view of the country’s overall situation and given the large number of facilities with out of stock, an emergency supply for all districts was done for some medicine since February 2018. Based on maps and stats, we could improve our interventions at a CSB level through rapid and adequate decision-making as in the supply of ITN and ART.
In conclusion, the use of SMS data collection to map stock-outs online can quickly improve input supply through simple spatial analysis. Sending SMSs to alert district-level officials about overstock in facilities at the same district level can solve many stock-out issues. All districts were restocked using this SMS and Web mapping system, but routing to the CSBs remains a challenge. Punctual stock-out reporting could significantly reduce the morbidity and mortality caused by malaria.
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A- 14-00028. The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government.
Health Information &Health Systems &Health Workers &Leadership Bill Brieger | 30 Oct 2018
Assessing Organizational Capacity to Deliver Malaria Services in Rural Liberia
Swaliho F. Kamara, Wede Tate, Allyson R. Nelson, Lauretta N. Se, Lolade Oseni, Gladys Tetteh of MCSP/Jhpiego are presenting a poster at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene on Malaria Service delivery in rural Liberia. Their findings are shared below:
 In Liberia Malaria prevalence in children under 5 is 45% nationally and higher in rural counties (NMCP et al. 2017). The National Malaria Control Program (NMCP) leads the rollout of malaria prevention and control activities to county health teams (CHTs), per the National Malaria Strategic Plan (2016–2020). A key donor supporting malaria prevention and control, the President’s Malaria Initiative (PMI), has been committed to the Ministry of Health and Social Welfare (MOHSW) strategy since 2008, when it began working in three out of 15 malaria-affected counties. PMI supports CHTs in their management of local health systems and service delivery oversight. As part of an expansion program to five additional rural, neglected, high-burden counties in 2017, the United States Agency for International Development (USAID)/ PMI-funded Maternal and Child Survival Program (MCSP) assessed CHTs’ organizational capacity to identify ways to improve the quality of malaria health services.
In Liberia Malaria prevalence in children under 5 is 45% nationally and higher in rural counties (NMCP et al. 2017). The National Malaria Control Program (NMCP) leads the rollout of malaria prevention and control activities to county health teams (CHTs), per the National Malaria Strategic Plan (2016–2020). A key donor supporting malaria prevention and control, the President’s Malaria Initiative (PMI), has been committed to the Ministry of Health and Social Welfare (MOHSW) strategy since 2008, when it began working in three out of 15 malaria-affected counties. PMI supports CHTs in their management of local health systems and service delivery oversight. As part of an expansion program to five additional rural, neglected, high-burden counties in 2017, the United States Agency for International Development (USAID)/ PMI-funded Maternal and Child Survival Program (MCSP) assessed CHTs’ organizational capacity to identify ways to improve the quality of malaria health services.
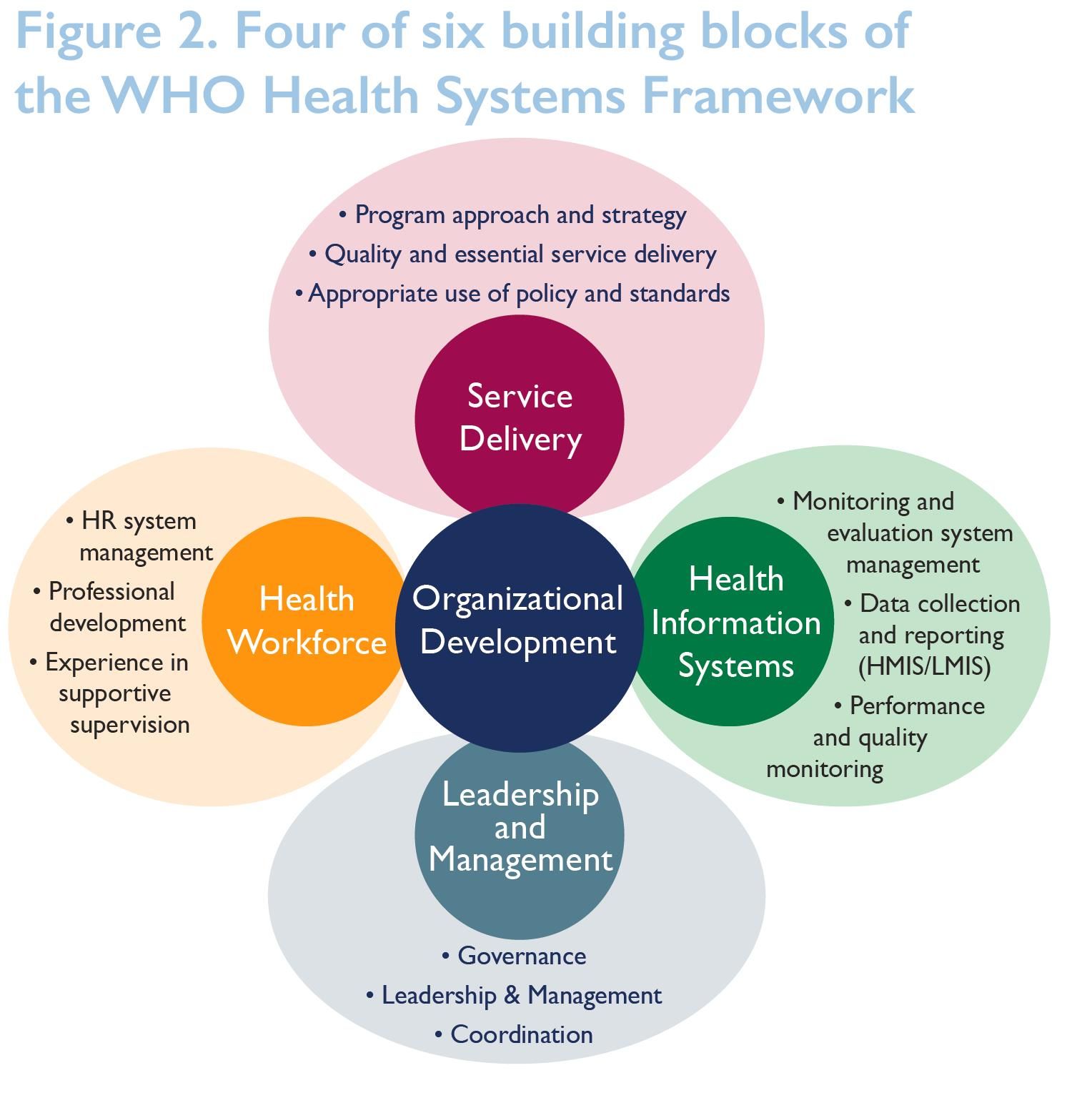 We assessed CHTs’ capacity using a modified organizational capacity assessment (OCA) tool that was used by the USAID’s Rebuilding Basic Health Services (RBHS) project to assess the capacity of the MOHSW, CHTs, and district health teams (DHTs), capturing four of the six World Health Organization (WHO) building blocks of the Health Systems Framework. We also assessed all 30 districts in five counties. Performed desk review, review of self- evaluations, and face- to-face validation interviews. The assessment focused on processes, not physical systems, so the capacity and knowledge of the respondents may have influenced results in some of counties.
We assessed CHTs’ capacity using a modified organizational capacity assessment (OCA) tool that was used by the USAID’s Rebuilding Basic Health Services (RBHS) project to assess the capacity of the MOHSW, CHTs, and district health teams (DHTs), capturing four of the six World Health Organization (WHO) building blocks of the Health Systems Framework. We also assessed all 30 districts in five counties. Performed desk review, review of self- evaluations, and face- to-face validation interviews. The assessment focused on processes, not physical systems, so the capacity and knowledge of the respondents may have influenced results in some of counties.
 Scoring Structure of the OCA Tool: Following each assessment, MCSP used a detailed summary sheet (Figure 3) to display the aggregate scores for each subarea under all key domains, then generated an overall score for each domain. The total score was then expressed as a percentage for each key domain. The majority of the assessment involved asking specific questions about performing malaria interventions per the project scope.
Scoring Structure of the OCA Tool: Following each assessment, MCSP used a detailed summary sheet (Figure 3) to display the aggregate scores for each subarea under all key domains, then generated an overall score for each domain. The total score was then expressed as a percentage for each key domain. The majority of the assessment involved asking specific questions about performing malaria interventions per the project scope.
Effective Interventions were determined:
- Health Workforce Interventions …
- Trained health care workers.
- Trained supervisors on revised supervision tool.
- Performed quarterly supervision and mentoring.
- Leadership and Governance
- Identified a malaria focal point.
- Activated functional health-sector coordination committees.
- Held quarterly review meetings.
- Health Information System
- Provided health management information systems (HMIS) forms to health facilities.
- Facilitated in-service training on onsite data verification.
 Results showed that CHTs’ overall average score was 87% in service delivery, 65% in health information systems, 78% in health workforce, and 70% in leadership/management. Interventions addressing gaps identified in health workforce, leadership and governance, and health information systems resulted in improved service delivery (see Figure 4).
Results showed that CHTs’ overall average score was 87% in service delivery, 65% in health information systems, 78% in health workforce, and 70% in leadership/management. Interventions addressing gaps identified in health workforce, leadership and governance, and health information systems resulted in improved service delivery (see Figure 4).
 In conclusion, The OCA tool helps to identify common challenges, assist with systemwide improvements across CHTs or DHTs, evaluate progress, and meet specific needs. Future efforts are needed to improve the tool’s specificity, the weighting attached to different sections and issues, and its relevance to different types of organizations. Training is an important component to capacity-building, but it is just one part of the picture. Need to improve the way organizations and CHTs/DHTs coordinate with partners to improve all health interventions. Need to focus on application and results of capacity-building, not on capacity as an end in itself.
In conclusion, The OCA tool helps to identify common challenges, assist with systemwide improvements across CHTs or DHTs, evaluate progress, and meet specific needs. Future efforts are needed to improve the tool’s specificity, the weighting attached to different sections and issues, and its relevance to different types of organizations. Training is an important component to capacity-building, but it is just one part of the picture. Need to improve the way organizations and CHTs/DHTs coordinate with partners to improve all health interventions. Need to focus on application and results of capacity-building, not on capacity as an end in itself.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Health Information Bill Brieger | 29 Oct 2018
Contribution of Quarterly Malaria Data Review and Validation to Data Quality and Malaria Services Improvement
Without quality service delivery data, we can never confidently say what progress we are making in improving access and uptake to malaria services. Mathurin Dodo, Ousmane Badolo, Stanislas Nebie, Youssouf Sawadogo, Thierry Ouedraogo, Moumouni Bonkoungou,  Youssouf Zongo, Maria Gouem, Danielle Burke, William Brieger, and Gladys Tetteh of the USAID/Jhpiego Improving Malaria Care Project and Burkina Faso Ministry of Health have implemented procedures to review malaria data quality. They share their findings at the 2018 American Society of Tropical Medicine and Hygiene as well as in the text that follows:
Youssouf Zongo, Maria Gouem, Danielle Burke, William Brieger, and Gladys Tetteh of the USAID/Jhpiego Improving Malaria Care Project and Burkina Faso Ministry of Health have implemented procedures to review malaria data quality. They share their findings at the 2018 American Society of Tropical Medicine and Hygiene as well as in the text that follows:
In Burkina Faso, malaria seriously affects pregnant women and children under 5 years of age . The malaria fatality rate for children under 5 was 2.8% in 2010, 2.10% in 2011, and 2.7% in 2012. For pregnant women, it was 0.71% in 2011 and 0.66% in 2013. Since October 2013, the United States Agency for International Development/ President’s Malaria Initiative has funded the 6-year Improving Malaria Care (IMC) project to improve malaria prevention and case management in support of the National Malaria Control Program (NMCP). The Ministry of Health and IMC staff conducted two malaria data quality audits (DQAs) in September 2014 and February 2017 that confirmed the poor quality of malaria data. The accuracy of malaria key indicators ranged from 56% to 76%.
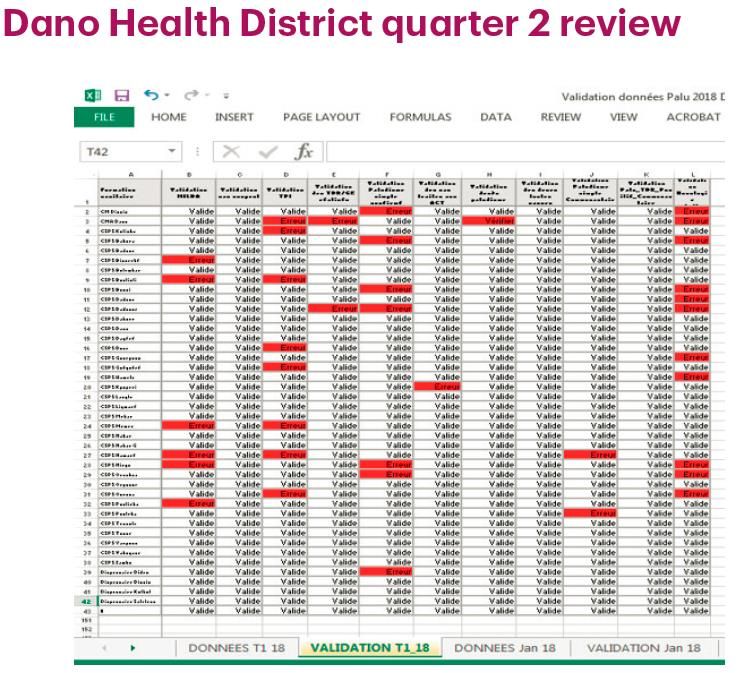 A Pre-Data Review Workshop begins the process. IMC supported the NMCP and health management information system to develop a manual of procedures for malaria data review and validation at health district level. IMC assisted in developing a malaria data review sheet based on data validation rules in manual. Each quarter, the district data manager entered data from monthly reports sent by the health facilities in the three health district project areas—Boromo, Dano, and Koupela—into DHIS2.
A Pre-Data Review Workshop begins the process. IMC supported the NMCP and health management information system to develop a manual of procedures for malaria data review and validation at health district level. IMC assisted in developing a malaria data review sheet based on data validation rules in manual. Each quarter, the district data manager entered data from monthly reports sent by the health facilities in the three health district project areas—Boromo, Dano, and Koupela—into DHIS2.
 During the Data Review Workshop the regional data manager asked each health facility manager to verify reports. When correcting each error, the regional data manager and head of the district management team explained to providers the indicator definitions and malaria prevention and treatment guidelines. The district data manager corrected the data in DHIS2.
During the Data Review Workshop the regional data manager asked each health facility manager to verify reports. When correcting each error, the regional data manager and head of the district management team explained to providers the indicator definitions and malaria prevention and treatment guidelines. The district data manager corrected the data in DHIS2.
After three rounds of quarterly reviews, all three health districts saw an overall decrease in the number of reporting errors. After two rounds of quarterly data review workshops, there were no errors due to understanding detected.
Quarterly data review workshops can be used to reinforce the technical capacity of providers. Involving providers who are responsible for malaria prevention, diagnosis, and treatment gives them a better understanding of indicator definitions and linkages between indicators and the services they provide. Working with health care providers to improve data quality at the district level helps providers build capacity in health management information systems and in data collection, verification, and control at facility level. It also improves the quality of malaria services. The malaria data review contributes to malaria data quality improvement. All opportunities should be used to reinforce the capacity of health care providers and improve the quality of malaria prevention and case management services.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID) under Cooperative Agreement No. AID-624-A-13-00010 and the President’s Malaria Initiative (PMI). The contents are the responsibility of the authors and do not necessarily reflect the views of USAID, PMI or the United States Government.
Case Management &CHW &Community &iCCM Bill Brieger | 29 Oct 2018
Performance of Community Health Workers in Providing Integrated Community Case Management (iCCM) Services in Eight Districts of Rwanda

During the first poster session at the 2018 Annual Meeting fo the American Society of Tropical Medicine and Hygiene, Noella Umulisa, Aline Uwimana, Cathy Mugeni, Beata Mukarugwiro, Stephen Mutwiwa, and Aimable Mbituyumuremyi of the Maternal and Child Survival Project (USAID)/Jhpiego and the Ministry of Health, Rwanda, presented findings from a review of community health workers in malaria case management. Their findings follow:
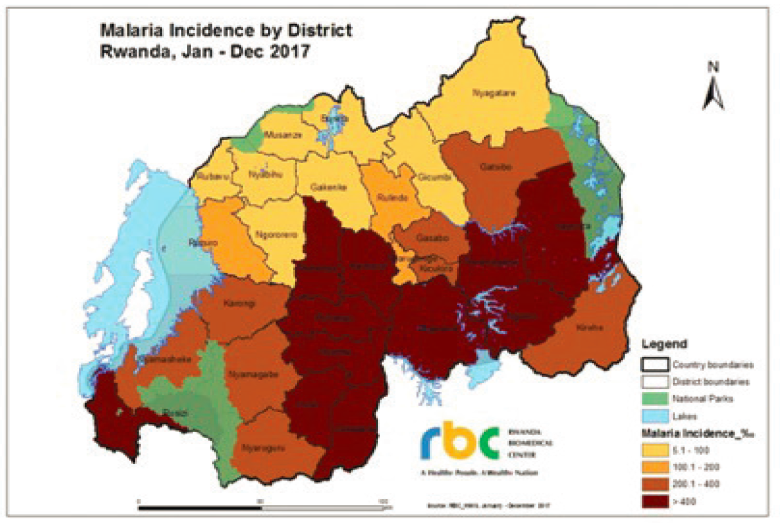 Rwanda has achieved near universal coverage of long-lasting insecticide nets, artemisinin-based combination therapy (ACT) and diagnosis, and targeted indoor residual spraying. Even so, there was an unprecedented increase in malaria cases from 2012-2017 despite optimal coverage of preventive and curative key interventions. The increase was caused by higher temperature, more rainfall, and increased resistance to insecticides.
Rwanda has achieved near universal coverage of long-lasting insecticide nets, artemisinin-based combination therapy (ACT) and diagnosis, and targeted indoor residual spraying. Even so, there was an unprecedented increase in malaria cases from 2012-2017 despite optimal coverage of preventive and curative key interventions. The increase was caused by higher temperature, more rainfall, and increased resistance to insecticides.
With more cases, the need for community case management (CCM) is crucial. Rwanda therefore trains, equips and supports community health providers to deliver high- impact treatment interventions and aims to supplement facility-based case management. Rwanda introduced integrated CCM 2008. Trained community health workers (CHWs) provide iCCM based on empirical diagnosis and treatment of pneumonia, diarrhea, and malaria. They also conduct malnutrition surveillance, comprehensive reporting and referral services.
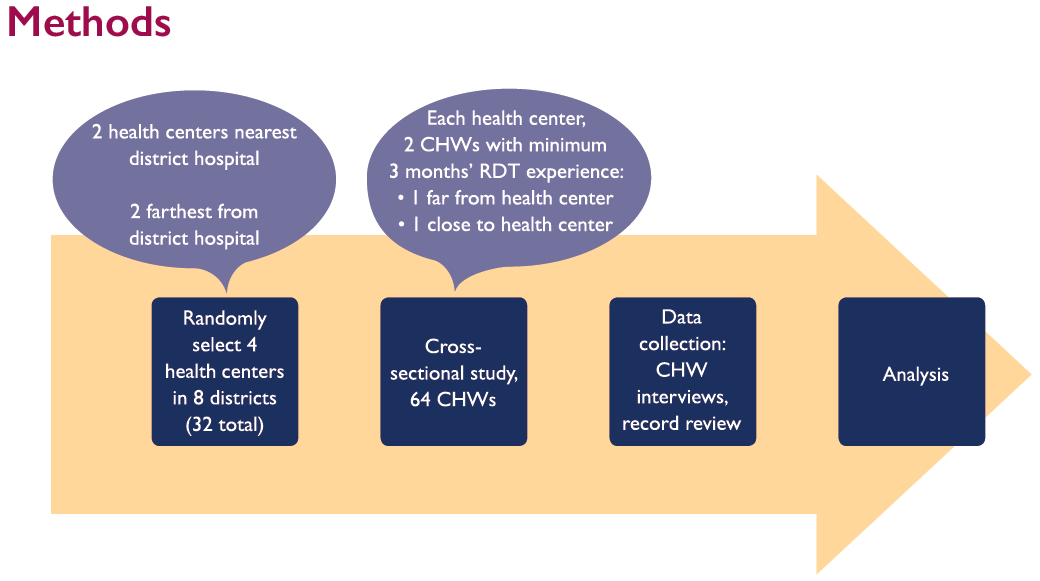 Given the changing status of malaria in the country, it was necessary to evaluate the performance of the CHWs. The evaluation aimed 1) to evaluate CHW performance in managing malaria, pneumonia and diarrhea in 8 districts of Rwanda based on national guidelines, and 2) to identify areas to reinforce and empower community health interventions. Using proximity (near/far) to hospitals and health centers, CHWs who had a minimum of 3 months experience using malaria rapid diagnostic tests (RDTs) were selected for interview. Slightly over half of CHWs were Males (56.2%). Most were over 40 years of age and nearly one-third were 50 years and older. Only 2% were between 25-29 years old.
Given the changing status of malaria in the country, it was necessary to evaluate the performance of the CHWs. The evaluation aimed 1) to evaluate CHW performance in managing malaria, pneumonia and diarrhea in 8 districts of Rwanda based on national guidelines, and 2) to identify areas to reinforce and empower community health interventions. Using proximity (near/far) to hospitals and health centers, CHWs who had a minimum of 3 months experience using malaria rapid diagnostic tests (RDTs) were selected for interview. Slightly over half of CHWs were Males (56.2%). Most were over 40 years of age and nearly one-third were 50 years and older. Only 2% were between 25-29 years old.
 Based on National Guidelines, CHWs were judged to have provided “adequate” treatment more frequently than “correct” treatment. Overall, 90% of cases were adequately treated; only 70% correctly treated. Among the three main conditions, malaria was most often adequately and correctly treated. Incorrect treatment was due to lack of adherence to guidelines. For malaria incorrect treatment often meant using the wrong does for age packet for treatment when the correct packet was not in stock.
Based on National Guidelines, CHWs were judged to have provided “adequate” treatment more frequently than “correct” treatment. Overall, 90% of cases were adequately treated; only 70% correctly treated. Among the three main conditions, malaria was most often adequately and correctly treated. Incorrect treatment was due to lack of adherence to guidelines. For malaria incorrect treatment often meant using the wrong does for age packet for treatment when the correct packet was not in stock.
 In conclusion, CHWs correctly treat 70% of children for all IMCI pathologies according to national guidelines. Malaria was the most seen/treated pathology; cases increased during study period. Overall, cases more often treated adequately than correctly. CHWs use complex tools thus lack adequate time to follow all steps correctly when providing services.
In conclusion, CHWs correctly treat 70% of children for all IMCI pathologies according to national guidelines. Malaria was the most seen/treated pathology; cases increased during study period. Overall, cases more often treated adequately than correctly. CHWs use complex tools thus lack adequate time to follow all steps correctly when providing services.
The study team recommends the need to strengthen iCCM commodities supply chain, especially at community level through supervision and mentorship conducted at health centers, district hospitals and central level. Also it is necessary to revise and simplify iCCM tools used by CHWs to decrease burden and improve quality of services.
 This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
CHW &Community &IPTp &Malaria in Pregnancy Bill Brieger | 29 Oct 2018
Community Health Workers Can Enhance Coverage of Intermittent Preventive Treatment of Malaria in Pregnancy and Promote Antenatal Attendance
Among the poster presentations on malaria from Jhpiego, the President’s Malaria Initiative and partners at the 2018 ASTMH Annual Meeting, WR Brieger, J Tiendrebeogo, O Badolo, M Dodo, D Burke, K Vibbert, SJ Youll, and JR Gutman shared the findings from a 15-month intervention that tested the ability of community health workers to deliver intermittent preventive treatment of malaria in pregnancy in 3 districts in Burkina Faso. Please check out the poster and talk to one of the co-investigators at Poster Session A on Monday 29 October. Their results are found below.
Malaria in pregnancy is responsible for a substantial proportion of low-birthweight and stillborn infants in sub-Saharan Africa. To prevent this, the World Health Organizatio n (WHO) recommends that pregnant women receive intermittent preventive treatment of malaria in pregnancy (IPTp) using sulfadoxine-pyrimethamine. Specifically, WHO recommends an optimal three or more doses (e.g., IPTp3, IPTp4).
n (WHO) recommends that pregnant women receive intermittent preventive treatment of malaria in pregnancy (IPTp) using sulfadoxine-pyrimethamine. Specifically, WHO recommends an optimal three or more doses (e.g., IPTp3, IPTp4).
In stable malaria endemic countries, IPTp coverage remains unacceptably low, at around 19% for IPTp3. Community IPTp might provide an answer. Community delivery can improve coverage as seen in previous study in Nigeria and Malawi, but its effects on antenatal care (ANC) attendance have been mixed. Additional data are needed to determine whether delivery of IPTp-SP by community health workers (CHWs) is effective and does not detract from ANC attendance. Hence the Burkina Faso intervention was designed and implemented
The study piloted community delivery of IPTp (c-IPTp) in three districts of Burkina Faso  with high malaria transmission: Po, Ouargaye, and Batie. Four health facilities per district were randomly selected to participate (two intervention and two control).
with high malaria transmission: Po, Ouargaye, and Batie. Four health facilities per district were randomly selected to participate (two intervention and two control).
In 2017, following a baseline household survey of women who recently became pregnant, implementation of c-IPTp began in intervention areas by existing CHWs trained and supervised by health staff. At Baseline in each of the three study districts, four health centers (CSPSs) and the villages in their catchment areas were selected—two as intervention and two as control. A random sample of 374 women who had been pregnant within the last 9 months were interviewed in CSPS catchment villages. There were no significant differences in ANC attendance (ANC1=90%, ANC4=62%) or IPTp coverage between intervention and control areas:
- IPTp3 was 81% (intervention) and 86% (control).
- IPTp4 was 22% (intervention) and 16% (control).
 The Intervention consisted of building on Burkina Faso’s existing CHWs. They were trained and monitored by clinic staff. The CHWs encouraged women to attend the first ANC visit to obtain IPTp1. Then the CHWs provided monthly doses of IPTp, submitted monthly reports, and continued to promote ANC. ANC attendance and IPTp uptake were monitored through monthly clinic and CHW reports. The catchment area populations were roughly the same, and monitoring showed that the additional provision of IPTp by CHWs resulted in more women being reached while at the same time ANC attendance remained high.
The Intervention consisted of building on Burkina Faso’s existing CHWs. They were trained and monitored by clinic staff. The CHWs encouraged women to attend the first ANC visit to obtain IPTp1. Then the CHWs provided monthly doses of IPTp, submitted monthly reports, and continued to promote ANC. ANC attendance and IPTp uptake were monitored through monthly clinic and CHW reports. The catchment area populations were roughly the same, and monitoring showed that the additional provision of IPTp by CHWs resulted in more women being reached while at the same time ANC attendance remained high.
An endline su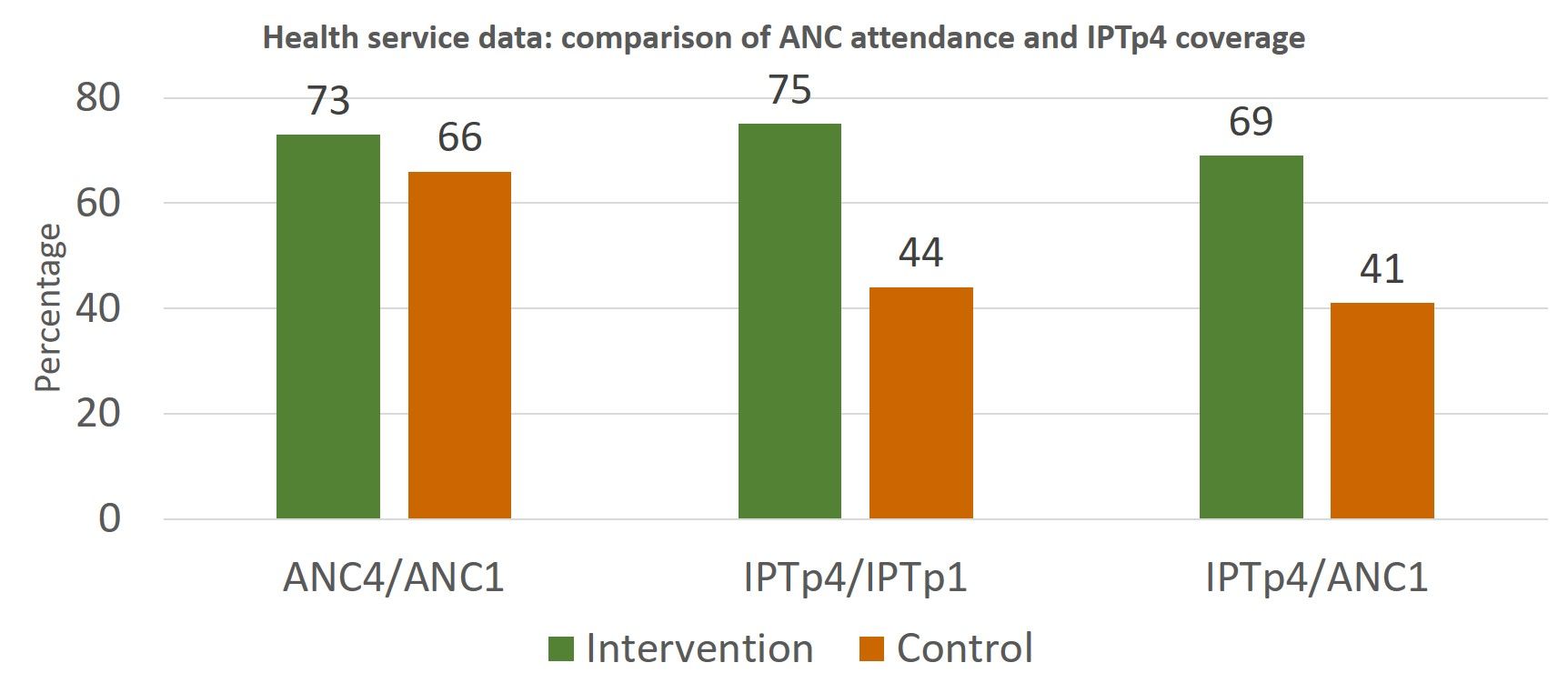 rvey was conducted after 18 months of implementation. Changes over time were compared between baseline and endline in intervention versus control villages. Attendance at ANC1 and ANC4 increased in both groups between baseline and endline but was significantly better for the intervention group. Likewise, coverage of IPTp3 and IPTp4 increased between baseline and endline for intervention and control women, but the difference was significant only in the intervention areas.
rvey was conducted after 18 months of implementation. Changes over time were compared between baseline and endline in intervention versus control villages. Attendance at ANC1 and ANC4 increased in both groups between baseline and endline but was significantly better for the intervention group. Likewise, coverage of IPTp3 and IPTp4 increased between baseline and endline for intervention and control women, but the difference was significant only in the intervention areas.
 Monthly monitoring of CHW and ANC registers and the household surveys both documented that community delivery of IPTp resulted in the desired increased uptake of services without detracting from ANC attendance. Community IPTp may be a promising strategy to improve coverage of IPTp.
Monthly monitoring of CHW and ANC registers and the household surveys both documented that community delivery of IPTp resulted in the desired increased uptake of services without detracting from ANC attendance. Community IPTp may be a promising strategy to improve coverage of IPTp.
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Announcement &Case Management &CHW &Community &Ebola &Infection Prevention &IPTp &Malaria in Pregnancy &Quality of Services Bill Brieger | 29 Oct 2018
Malaria Featured in Jhpiego Sessions at ASTMH 2018

Below is a list of Jhpiego Sessions at this week’s American Society of Tropical Medicine Annual Meeting in New Orleans (28 October-1 November). Please attend if you are at the conference:
![]() Poster Session A, Monday, October 29 (Posters in Marriott Grand Ballroom – 3rd Floor )
Poster Session A, Monday, October 29 (Posters in Marriott Grand Ballroom – 3rd Floor )
- Poster Number 098: Performance of community health workers in providing integrated community case management services (iCCM) in 8 districts of Rwanda
- Poster 380: Contribution of quarterly malaria data review and validation to data quality and malaria services Improvement
- Poster LB-5117: Community based health workers can enhance coverage of intermittent preventive treatment of malaria in pregnancy and promote antenatal attendance
Poster Session B, Tuesday 30 October
- Poster 1088: Assessing organizational capacity to deliver quality malaria services in rural Liberia
- Poster 1092: Contribution of IMC project in transforming the face of malaria control for vulnerable populations in Burkina Faso
- Poster 1093: Malaria response plan in times of high transmission: An approach to improving the quality of hospital malaria management
- Poster 1111: Setting the stage to introduce a ground breaking approach to prevent malaria in pregnancy in Sub-Saharan Africa: baseline-readiness assessment findings from Democratic Republic of Congo, Mozambique, Madagascar, and Nigeria
- Poster 1337: Institutionalizing infection prevention and control practices in health facilities in Liberia following the Ebola epidemic
 Scientific Session 87, Tuesday, 1:45 – 3:30 p.m. Marriott – La Galerie 1 & 2 – 2nd Floor: Improving procurement and redeployment of district level malaria commodities using SMS and web mapping in Madagascar
Scientific Session 87, Tuesday, 1:45 – 3:30 p.m. Marriott – La Galerie 1 & 2 – 2nd Floor: Improving procurement and redeployment of district level malaria commodities using SMS and web mapping in Madagascar
Poster Session C, Wednesday 31 October
- Poster 1816: Experiences and perceptions of care seeking for febrile illness among caregivers and providers in 8 districts of Madagascar
- Poster 1818: Improving adherence to national malaria treatment guidelines by village health workers in selected townships through a low-dose, high-frequency training approach
- Poster 1819: Improving malaria case management through national roll-out of Malaria Service and Data Quality Improvement (MSDQI): A Case study from Tanzania
- Poster 1820: Collaborative quality improvement framework to support data quality improvement, experience from 10 collaborative facilities in Uganda
- Poster 1821: Using malaria death audits to improve malaria case management and prevent future malaria related preventable deaths
- Poster 1833: Multiple approaches for malaria case management in the struggle to reach pre-elimination of malaria.
Scientific Session 182, Thursday, November 1, 10:15 am – 12:00 p.m. Marriott – Balcony I,J,K – 3rd Floor: Seasonal malaria chemoprevention, an effective intervention for reducing malaria morbidity and mortality