Polio &Vaccine Bill Brieger | 30 Mar 2026
From Campaigns to Community Trust: Rethinking Polio Strategy in Southern KP, Pakistan
Originally published on 21 March 2026 by Nosheen Khan for the JHU/BSPH course “Social and Behavioral Foundations of Primary Health Care.”
Pakistan remains one of only two countries where wild poliovirus still circulates. In southern Khyber Pakhtunkhwa—districts like Bannu, North and South Waziristan, Tank, Lakki Marwat, and Dera Ismail Khan—vaccine refusals and low routine immunization coverage continue to fuel transmission. In some areas, routine coverage is critically low, leaving large numbers of “zero-dose” children.

For years, the response has relied on repeated mass campaigns. While these efforts have saved millions of children globally, in southern KP they are no longer enough. Communities face fatigue, misinformation, and deep-rooted distrust. Many families ask a simple question: “Why only polio drops, but no other health services?”
Evidence from the Global Polio Eradication Initiative and World Health Organization shows that access, trust, and behavior change are as critical as vaccines themselves. Similarly, UNICEF Pakistan highlights the importance of community engagement and social mobilization in addressing refusals.
A Needed Shift: From Campaigns to Communities
Southern KP needs a programmatic shift, not a new law. The provincial government—through the Khyber Pakhtunkhwa Department of Health and the Pakistan Polio Eradication Programme—should transition toward a community-centered, integrated service model:
- Combine polio vaccination with routine immunization, nutrition, and maternal-child health services
- Engage Jirga councils and religious networks to counter misinformation
- Invest in female frontline workers to improve access in conservative areas
- Strengthen routine immunization systems to rebuild trust
This approach addresses the root causes of refusal, not just the symptoms.

Why This Matters Now
With ongoing transmission and persistent immunity gaps, the cost of inaction is high—not just for Pakistan, but globally. A child missed today is a risk tomorrow.
Call to Action
The Khyber Pakhtunkhwa Department of Health and Pakistan Polio Eradication Programme must revise implementation guidelines within the next 6–12 months to integrate polio efforts with broader health services in southern KP. Development partners should align funding and technical support to accelerate this shift.
Ending polio in Pakistan will not come from more campaigns alone—it will come from building trust, delivering services, and putting communities at the center.
Advocacy &Community &Diagnosis &Education &Elimination &Epidemiology &India &IRS &ITNs &Malaria &Plasmodium/Parasite &Procurement Supply Management &Research &Strategy &Surveys &Vaccine &Vector Control &World Malaria Day Bill Brieger | 24 Apr 2025
The Johns Hopkins Bloomberg School of Public Health Dean’s Lecture on Malaria
Professor Jane Carlton, PhD, Director of Johns Hopkins Malaria Research Institute was introduced by Dean Ellen MacKenzie to give a Dean’s Lecture entitled “Malaria: History, current status, and the promise of ‘omics and AI.”

Prof. Carlton first gave an overview of JHMRI, which was founded in 2001. She stepped into director role in 2023. She started with the encouraging premise that AI and ‘omics can supercharge our research and pointed out the power of comparative genomics on understanding parasites and disease. Her goal is to translate discovery into real world impact through collaborations.
The talk started with a brief malaria history. Malaria was described as an ancient disease and remains one of top infectious diseases worldwide. There were 2.63 million cases and more than half a million deaths in 83 endemic countries in 2023. Today 44 countries are malaria-free.
Up until now, Prof. Carlton noted, the malaria map has been shrinking. There was a precipitous decline in malaria in India from 23 million cases to 2 million. The disease is a true humanitarian issue with a large impact on people living in resource-limited settings where housing is basic and offers no protection from mosquitoes.

The JHMRI is supported by Bloomberg philanthropies, and from that base faculty research examines, among others, better methods for controlling mosquitoes (see slide), new diagnostic tests and therapeutics, and the next generation of vaccines. Key assets to support research include mosquito insectaries and a malaria parasite core. The insectaries produce 60,000 mosquitoes per week, and with these it is possible to complete the life cycle in the laboratory.
Continuing education is another important function of JHMRI which has three conferences per year including the upcoming World Malaria Day 2025 symposium. One can also learn from the Malaria Minute podcast. The upcoming “Vector Encounter” provides sharing and learning for researchers.

JHMRI studies malaria at field sites in Africa and Asia where country collaborators are partners. Emphasis is on local capacity building in countries like Zambia, Ethiopia, Kenya, and Uganda. Researchers and the national malaria control programs in these countries work hand-in-hand.
JHMRI is involved in developing the next generation of vaccines. One approach if a human monoclonal antibody that prevents malaria infections. Another develops a vaccine that transcends’ malaria parasite strains with structure guided mimicry of an essential P. falciparum receptor-ligand complex enhances cross neutralizing antibodies. A third example asks “How many parasites does it take to cause malaria?” and assesses infection likelihood through mosquito parasite burden.
To understand the theme of her talk, Prof. Carlton reviewed the promise of ‘omics and AI in the context of her work at a center of excellence in India. Pioneering work using Malaria camps in hard-to-reach villages in Odisha, India. The main activities mobilized villagers to gather for mass screening, treatment, education, and intensified vector control. From there, Indoor Residual Spraying was planned and insecticide treated bednets were distributed. Other maternal and child health activities were incorporated. After three rounds/visits in the remote villages a great drop of malaria cases was seen. WHO lauded the camps.

In addition to lessons about the importance of surveillance, mixed strategies, and community mobilization for controlling malaria, the team learned about the growing challenge of reduced effectiveness of Rapid Diagnostic Tests. The problem arose because tests were dependent on a protein that was no longer being expressed due to Pfhrp2 gene deletions, leading to false negative test results. The team was encouraged to identify more proteins to find a more stable and central one to use in testing. Through machine learning, this work is ongoing but promising.
While we are on the verge of several research and programmatic breakthroughs, Prof. Carlton reminded the audience that we are in calamitous times. She recalled that the United States has been the top donor government to malaria efforts through Presidents Malaria Initiative and Global Fund to Fight AIDS, Tuberculosis, and Malaria. PMI was founded in 2005, and has contributed to a decline in malaria death rates of close to 50%.

With suspension of funding, an estimated increase of 12.5-17.9 million malaria cases and 71,000-166,000 malaria deaths are expected this year. Already there are serious impacts on the supply chain for major malaria commodities as estimated by the Roll Back Malaria Partnership as seen on their RBM dashboard and supply chain gap estimates where six endemic countries have less than a 3-month supply of RDTs and eleven have less than a 6-month supply.
Prof Carlton ended by saying, “I think the hope is in science, right? The hope is in research. There are definitely new initiatives, new tools which are coming to the forefront, some of which I mentioned, and several of which we’re developing here at the malaria Research Institute. I do know the World Health Organization has got together with other countries to provide additional funding and support for those countries who have lost support through PMI.”
Polio &Refugee &Vaccine Bill Brieger | 24 Aug 2024
Rise of polio cases amid Afghan Refugee Crisis
According to MinahHAli, polio is still with us as seen in this posting about polio challenges in the class blog of the course, Social and Behavioral Foundations of Primary Health Care at the Johns Hopkins Bloomberg School of Public Health
 Image Source: UNHCR
Image Source: UNHCR
After a much-desired decrease of polio cases in Pakistan, the recent increase in cases reported has been alarming. This latest surge coincided with the Afghan Refugee Crisis in Pakistan, showcasing the impact of government policies in the success of polio eradication.
What is Polio? Polio, also known as poliomyelitis, is a viral disease which affects nerves in the spinal cord or brain stem leading to paralysis and death in some cases. Poliovirus rapidly spreads either via feces or droplets from coughing/sneezing. Polio mainly affects unvaccinated children.
Why are Polio vaccination initiatives focused on Pakistan and Afghanistan? Are all polio cases the same? Pakistan and Afghanistan are the last two countries in the world which consistently report polio cases. Despite spending $9.3 billion over the course of 10 years (2013-2023) polio cases remain present in Pakistan. According to WHO, Polio cases in Afghanistan can be traced back to one variant: YB3A. However, recently polio cases in Pakistan are now also from YB3A variant.
 Image Source: CNN
Image Source: CNN
What is the Afghan Refugee Crisis and how is it fueling the spread of polio? Pakistan is the largest host country for Afghan refugees since 1979 post-Soviet invasion. In 2019, Ministry of National Health Services, Regulation and Coordination in Pakistan, along with UNHCR, promised healthcare which included polio vaccination to Afghan refugees. However, due to increased security threats recently near the Pak-Afghan border these efforts have stopped.
Due to attacks on Pakistani soil which have been linked to Afghan terrorist groups, the Federal Government of Pakistan is currently forcibly relocated Afghan refugees back to Afghanistan. Due to this, many Afghans refugees refuse to seek healthcare in the fear of being reported and deported.
Why are the polio eradication programs failing? The political climate in Pakistan, especially in the Khyber Pakhtunkhwa province which borders Afghanistan, is tense; heightened insecurity, fueled with tribal conflicts amongst Pakistanis and Afghanis residing in the area is making polio vaccination programs “almost impossible”, according to polio eradication lead at Bill and Melinda Gates foundation.
By neglecting the on-going polio spread amongst Afghan refugees, Poliovirus is making its way into Pakistani citizens/communities. It is imperative that the Ministry of National Health Services, Regulation and Coordination, as well as the provincial Khyber Pakhtunkhwa Government increase their efforts for polio vaccination- regardless of immigration status.
Polio &Vaccine Bill Brieger | 23 Aug 2024
Polio Eradication in Pakistan, an Update
On August 20, 2024, Yasir Ahmed Posted this blog about polio challenges in the class blog of the course, Social and Behavioral Foundations of Primary Health Care at the Johns Hopkins Bloomberg School of Public Health
Pakistan and Afghanistan are the only countries in the world reporting wild type polio virus cases. Polio is a crippling disease that does not have any cure but it is preventable through immunization. The detection of wild-type virus in wastewater suggests 2024 target of ending all wild virus transmission will be missed. 6 cases were reported in 2023 and 14 have been reported this year so far. According to a report by IMB, an estimated 300,000 children have been consistently missed in vaccination activities in Pakistan and in the East region of Afghanistan. Disinformation, false beliefs and mistrust on the government and administration, refusal, not understanding the importance of vaccines, and low general literacy and health literacy etc. are among the important factors contributing to these missed opportunities.
In addition to the above-mentioned factors, insecurity, movement across the porous 2400 kilometers long Pakistan-Afghan border, and poor water and sanitation and waste management are the contributing factors. I believe that the missed opportunities to reach and vaccinate these children has a major role in the spread of poliovirus along with poor water and sanitation in these areas.
 The program uses four distinct risk tiers to classify areas according to the risk they present and to devise risk appropriate strategies. Core reservoir districts (or Tier 1 districts), high-risk districts (or Tier 2 districts), vulnerable districts (or Tier 3 districts), and low-risk districts (or Tier 4 districts). Most of the tier 1 and tier 2 areas are located on the western border aka Pakistan-Afghan border (upper parts on the map).
The program uses four distinct risk tiers to classify areas according to the risk they present and to devise risk appropriate strategies. Core reservoir districts (or Tier 1 districts), high-risk districts (or Tier 2 districts), vulnerable districts (or Tier 3 districts), and low-risk districts (or Tier 4 districts). Most of the tier 1 and tier 2 areas are located on the western border aka Pakistan-Afghan border (upper parts on the map).
Pakistan Polio Eradication Program is an initiative that is driven by the largest surveillance network in the world (up to 339,521 trained and dedicated polio workers), quality data collection and analysis, behavioral change communication, laboratories, and epidemiologists and public health experts in Pakistan, working with experts and local and international stakeholders. The government started National Emergency Action Plan for Polio Eradication in 2010, which runs supplemental immunization activities on regular basis to reach every child in Pakistan. As a result, a huge decline in the number of polio cases is seen since the 90’s. The World Health Organization (WHO) and UNICEF along with other key partners of the Global Polio Eradication Initiative, has been a very supportive to the Government of Pakistan in polio eradication. Gavi the vaccine alliance, the Center of Disease Control (CDC), Rotary International, and Bill and Melinda Gates Foundation are important stakeholders that provides major financial, technical and field support.
 A Polio-worker is pictured giving an oral polio vaccine during an immunization campaign.
A Polio-worker is pictured giving an oral polio vaccine during an immunization campaign.
Innovative approaches are required to reach the children missing vaccinations including:
- Expanding the network and improving data collection and surveillance, targeting the areas of high density with polio cases e.g., the tribal areas along the porous Pak-Afghan border.
- Mandatory vaccination at border crossing.
- Increased security for the polio workers.
- Taking local religious and community leaders and scholars on-board to counter disinformation and false beliefs.
- Continuation and strengthening of National Emergency Action Plan for Polio Eradication by the government of Pakistan.
Continued efforts and support from the local and international stakeholders as we are getting very close global polio eradication.
Vaccine Bill Brieger | 16 May 2024
Expanding Access of Malaria Vaccinations in Vihiga County Benefits All of Kenya
The class blog for Social and Behavioral Foundations of PHC features a posting by Alice Calhoun on the importance of pilot implementation of the new malaria vaccine in Kenya. Her comments are found below.
 Since 2019, significant improvements in death rates and hospitalizations from malaria in young children have been made in Kenya after initiating the pilot malaria vaccine trial, Malaria Vaccine Implementation Programme (MVIP) involving children under 2 years old. Under the leadership and support from WHO, GAVI, and PATH and many other stakeholders, Kenya was able to benefit from the RTS,S vaccine that was developed for over 35 years by GlaxoSmithKline Pharmaceuticals. As the vaccination program continues in Western Kenya, parents in Vihiga County have noted that their children who have been vaccinated are less sick than their older siblings. The 4 part vaccination series typically begins at age 6 months with its completion at 24 months.
Since 2019, significant improvements in death rates and hospitalizations from malaria in young children have been made in Kenya after initiating the pilot malaria vaccine trial, Malaria Vaccine Implementation Programme (MVIP) involving children under 2 years old. Under the leadership and support from WHO, GAVI, and PATH and many other stakeholders, Kenya was able to benefit from the RTS,S vaccine that was developed for over 35 years by GlaxoSmithKline Pharmaceuticals. As the vaccination program continues in Western Kenya, parents in Vihiga County have noted that their children who have been vaccinated are less sick than their older siblings. The 4 part vaccination series typically begins at age 6 months with its completion at 24 months.
Malaria prevention must have a multi-faceted approach to be successful in eradicating this terrible disease from the community. This includes using insecticide treated bednets, indoor spraying, rapid diagnosis and treatment of active malaria, and malaria prevention during pregnancy. By using education and collaboration with groups such as the Kenya Malaria Youth Army, community health workers (CHW) are the key to disseminating information to the villages and encouraging mothers to complete the series for their children. CHW are also providing catch up vaccinations for other diseases while supporting the malaria campaign in Kenya by handing out bednets.
 Now is the time for the Ministry of Health (MOH) to expand the vaccine program to all children under 5 years of age, some of whom missed out on the initial set of vaccines due to vaccine hesitancy during the COVID pandemic. The benefits have been seen by the community in Vihiga County and the attitudes of the mothers are now overwhelmingly positive. Due to the dedication of the CHW and the Immunization Coordinator, nurse Edith Anjere, Vihiga County has the highest rate of childhood immunization coverage in Kenya: up to 96% of children as surveyed in 2022.
Now is the time for the Ministry of Health (MOH) to expand the vaccine program to all children under 5 years of age, some of whom missed out on the initial set of vaccines due to vaccine hesitancy during the COVID pandemic. The benefits have been seen by the community in Vihiga County and the attitudes of the mothers are now overwhelmingly positive. Due to the dedication of the CHW and the Immunization Coordinator, nurse Edith Anjere, Vihiga County has the highest rate of childhood immunization coverage in Kenya: up to 96% of children as surveyed in 2022.
Vihiga County is the perfect community to capture more children in the vaccination program since the health infrastructure is already in place as well as an openness in the community to continue vaccinating our children. The MOH can support this nationwide campaign against malaria by allowing other vulnerable children access to RTS,S in Vihiga County, serving as a model program for other counties. Kenya has been at the forefront of the malaria vaccination program and will continue to inspire other countries in Africa to work toward this goal of keeping our most vulnerable citizens healthier.
Vaccine Bill Brieger | 13 May 2024
Vaccine Hesitancy and Malaria
The term “vaccine hesitancy” is relatively new jargon that is defined in Wikipedia as, “… a delay in acceptance, or refusal, of vaccines despite the availability of vaccine services and supporting evidence.” The World Health Organization considers Vaccine Hesitancy among the top 10 threats to global public health. Vaccine hesitancy is primarily a matter of trust in institutions, technology, government, and health workers among others, according to Unfried and Priebe. Thus, hesitancy has social and political dimensions. This public health concern now extends into the realm of malaria control and elimination.
 After many years of testing for efficacy and implementability, we now have two malaria vaccines. Therefore, it is not surprising that the issue of hesitancy has been identified as a potential challenge. Hussein et al. studied parents in Ghana and found that “About one-third (34.5%) of the parents were hesitant to give their children the R21/Matrix-M malaria vaccine,” even though “showed a high safety and efficacy level, and Ghana is the first country to approve this new vaccine.” It seems that parents who had not been getting routine vaccinations for their children were among those who were more hesitant.
After many years of testing for efficacy and implementability, we now have two malaria vaccines. Therefore, it is not surprising that the issue of hesitancy has been identified as a potential challenge. Hussein et al. studied parents in Ghana and found that “About one-third (34.5%) of the parents were hesitant to give their children the R21/Matrix-M malaria vaccine,” even though “showed a high safety and efficacy level, and Ghana is the first country to approve this new vaccine.” It seems that parents who had not been getting routine vaccinations for their children were among those who were more hesitant.
The experience with door-to-door oral polio vaccine outreach campaigns from twenty plus years ago, shows that the general problem of avoidance or reluctance is nothing new, but often rooted in political and cultural factors, according to Jegede. Covid-19 has shed new light on the problem as explained in the Lancet: “COVID-19 vaccines to low-income and middle-income countries (LMICs) is threatened by vaccine hesitancy. In Africa in particular, the low vaccine coverage and the ubiquitous vaccine hesitancy in a concerning proportion of the population undermine efforts to fight the COVID-19 pandemic.”
It should be noted that the term ‘hesitancy’ puts the blame for not vaccinating children and others on community members and health care consumers. When the expanded program on immunization started 50 years ago, there was recognition that reasons for seeking or not obtaining vaccines were multifaceted and included much more than consumer knowledge and attitudes. Health system factors and economic barriers were of equal concern. We need to return to those days when we took a holistic view on how to promote vaccine uptake.
 Low levels of vaccine overage go beyond trust. When the Wikipedia definition mentions “despite the availability” there is the assumption that in fact vaccines are available, which is a major logistics, economics, and systems challenge. Fortunately, Mutombo et al. in the Lancet stress the other factors for low vaccine coverage including “historical, structural, and other systemic dynamics that underpin vaccine hesitancy.” They address serious supply problems wherein the global community has not made a “firm commitment to expedite vaccine deployment to the African continent.” It is not surprising that Nigeria has the highest level of unmet demand for COVID-19 vaccines in the world. Wollburg et al. also note that “Many who are willing to get vaccinated are deterred by a lack of easy access to vaccines at the local level.”
Low levels of vaccine overage go beyond trust. When the Wikipedia definition mentions “despite the availability” there is the assumption that in fact vaccines are available, which is a major logistics, economics, and systems challenge. Fortunately, Mutombo et al. in the Lancet stress the other factors for low vaccine coverage including “historical, structural, and other systemic dynamics that underpin vaccine hesitancy.” They address serious supply problems wherein the global community has not made a “firm commitment to expedite vaccine deployment to the African continent.” It is not surprising that Nigeria has the highest level of unmet demand for COVID-19 vaccines in the world. Wollburg et al. also note that “Many who are willing to get vaccinated are deterred by a lack of easy access to vaccines at the local level.”
Concerning the two malaria vaccines, UNICEF notes that “It is clear that the demand is very high and far surpasses the supply that is expected to become available.” Concerns revolve around production capacity, supply chain management, integration within the health system’s existing immunization programs, pricing, and partnerships. While it is useful to plan ways to counteract hesitancy, such efforts will not be relevant is there is inadequate supply to meet current and projected demand and needs. As Gavi explains, “partners will also work with countries to provide orientation and technical assistance to ensure quality planning and country readiness.”
Vaccine Bill Brieger | 14 May 2023
Tanzania needs malaria vaccines to reduce malaria burden
David Kanamugire has published a blog on the need to add the malaria vaccine to Tanzania’s arsenal of malaria elimination strategies. The original posting is found in the class blog for the Social & Cultural Basis for Community and Primary Health Programs class at the Johns Hopkins Bloomberg School of Public Health. Below is his perspectives on the issue.
Malaria is still a major public health problem. In 2021, malaria killed an estimated 619,000 people – 95 percent of them in Africa. Children under the age of 5 accounted for 80 percent of Africa malaria deaths. Tanzania is among 4 countries that account for just over half of all global malaria deaths.
The country has significantly reduced malaria cases, from a prevalence of 18% in 2008 to 8.1% in 2022. This reduction is attributed to intervention such as Insecticide Treated bed Nets, Indoor Residual Spray, effective drugs and Malaria Rapid Diagnostic tests.
But recently the global progress on malaria has stalled and this could be due to emerging drug resistance, insecticide resistance and the spreading of invasive species Anopheles stephensi. For the past 3 years, the global malaria death remains above 600,000. Therefore there is need for new approaches to help in efforts to prevent and control malaria. 
Photo: Gavi, the Vaccine Alliance
Vaccines are safe and cost-effective way combat communicable diseases and improve health outcomes. One of malaria vaccine that have been approved by the WHO is R21. It was developed by Oxford and is produced at a large scale by the Serum Institute of India.
The R21 vaccine is cheap and can be easily produced thus making it ideal for Africa countries. The R21 is also effective against malaria as three initial doses followed by a booster give up to 80 percent protection against malaria.
Innovation &Invest in Malaria Control &Vaccine &World Malaria Day &Zero Malaria Bill Brieger | 25 Apr 2023
World Malaria Day: Investing in Malaria Vaccines
 World Malaria Day 2023 is focusing on three key themes, Investment, Innovation, and Implementation, the 3 I’s. The recently approved malaria vaccines and those still under development embody these themes fully. They all represent decades of investment in innovation, research, and now implementation.
World Malaria Day 2023 is focusing on three key themes, Investment, Innovation, and Implementation, the 3 I’s. The recently approved malaria vaccines and those still under development embody these themes fully. They all represent decades of investment in innovation, research, and now implementation.
After extensive several decades of clinical research and three years of field implementation in Ghana, Malawi, and Kenya by the World Health Organization and National Malaria and Immunization Programs, the RTS,S/AS01 malaria vaccine is being rolled out with assistance of GAVI, the Global Vaccine Alliance. During the malaria vaccine implementation program (MVIP) and also based on GAVI’s philosophy for vaccine programs generally, a key strategy was to provide RTS,S as routine immunization services alongside other essential services including a comprehensive package of malaria control and elimination interventions. RTS,S is not only being made available to the three MVIP countries, but as supplies come on board, other falciparum malaria endemic countries have started to apply for supplies and funding through GAVI.
 It was well known from the beginning that although RTS,s might be first out the gate, other vaccines would be following closely on its heels. The benefits as well as the efficacy limitations of RTS,S were well known. Therefore, talk was common for new products being available by 2026. Now in 2023, countries have started to move ahead on another vaccine candidate.
It was well known from the beginning that although RTS,s might be first out the gate, other vaccines would be following closely on its heels. The benefits as well as the efficacy limitations of RTS,S were well known. Therefore, talk was common for new products being available by 2026. Now in 2023, countries have started to move ahead on another vaccine candidate.
BBC reported that “Ghana is the first country to approve a(nother) new malaria vaccine that has been described as a ‘world-changer’ by the scientists who developed it.” R21 appears to be more effective than its predecessor, so Ghana’s drug regulators moved ahead quickly using final trial data on the vaccine’s safety and effectiveness, which is not even public, to approve it. Interestingly, this move is in parallel to the World Health Organization’s consideration of approving the vaccine. Shortly thereafter, Nigerian medicine regulators also approved R21. Reuters noted that these “approvals are unusual as they have come before the publication of final-stage trial data for the vaccine.” The actual roll out will ultimately depend on official publication of the safety data and sourcing of funds.
 As mentioned above, these malaria vaccines represented considerable investment of time and resources, embody the kind of innovation that is needed to tackle malaria as drug and insecticide resistance threaten progress toward elimination, and require detailed planning right down to the grassroots levels to ensure that a malaria vaccine delivery is part of a comprehensive package of malaria and child health services.
As mentioned above, these malaria vaccines represented considerable investment of time and resources, embody the kind of innovation that is needed to tackle malaria as drug and insecticide resistance threaten progress toward elimination, and require detailed planning right down to the grassroots levels to ensure that a malaria vaccine delivery is part of a comprehensive package of malaria and child health services.
We need to return to the theme of investment. While international organizations, universities, ministries of health, and of course pharmaceutical companies have been investing in developing a safe, effective, and feasible product, these innovative products will not save lives until funds are invested for both purchase and service delivery are guaranteed. GAVI and Partners have put together over $200 million in support for RTS,S implementation for three years. The first window was open in September 2022 for the initial three MVIP countries, and a second window for others, depending on available supplies was open in December 2022.
Investment FOR implementation is a challenging subject because GAVI and collaborating agencies are not a bottomless well of money. What level of national investment by a country to protect its own children is feasible? Is there the national political will to contribute and invest in children in endemic countries, and not continue depending heavily on donors?
Malaria vaccines are a perfect example of what the 3 I’s can achieve. But beyond celebrating this addition to the malaria elimination toolkit, will we also be celebrating commitments by endemic countries of local funds to make zero malaria a reality?
HPV &Vaccine Bill Brieger | 15 Mar 2023
Malawi Experiences HPV vaccination Shortages as Registration Increases Among Adolescents Girls
By Jordan Kerr and originally posted in the Social and Behavioral Foundations of Primary Health Care Blog.
 Malawi is making strides in increasing HPV vaccinations among adolescent girls across the nation. Since the official implementation of the HPV vaccine program in 2019, 20 out of the 29 districts in Malawi have begun administering the vaccine to adolescent girls between the age of 9 and 14. Despite this success, Malawi continues to be one of the leading countries worldwide in cervical cancer-related mortality. New cases of cervical cancer in Malawi are reported at a rate five times higher than the global average.
Malawi is making strides in increasing HPV vaccinations among adolescent girls across the nation. Since the official implementation of the HPV vaccine program in 2019, 20 out of the 29 districts in Malawi have begun administering the vaccine to adolescent girls between the age of 9 and 14. Despite this success, Malawi continues to be one of the leading countries worldwide in cervical cancer-related mortality. New cases of cervical cancer in Malawi are reported at a rate five times higher than the global average.
 This highly preventable disease places a more significant burden on low-income countries like Malawi due to poor access to healthcare services and resources. International agencies are improving their outreach efforts to reach girls not enrolled in school and address vaccine hesitancy in districts with higher vaccine refusal rates. Due to this outreach vaccine registration is improving however healthcare facilities are experiencing stockouts. In some districts, healthcare facilities are reporting that the main reason individuals are not receiving vaccinations is that they are running out of vaccine stocks.
This highly preventable disease places a more significant burden on low-income countries like Malawi due to poor access to healthcare services and resources. International agencies are improving their outreach efforts to reach girls not enrolled in school and address vaccine hesitancy in districts with higher vaccine refusal rates. Due to this outreach vaccine registration is improving however healthcare facilities are experiencing stockouts. In some districts, healthcare facilities are reporting that the main reason individuals are not receiving vaccinations is that they are running out of vaccine stocks.
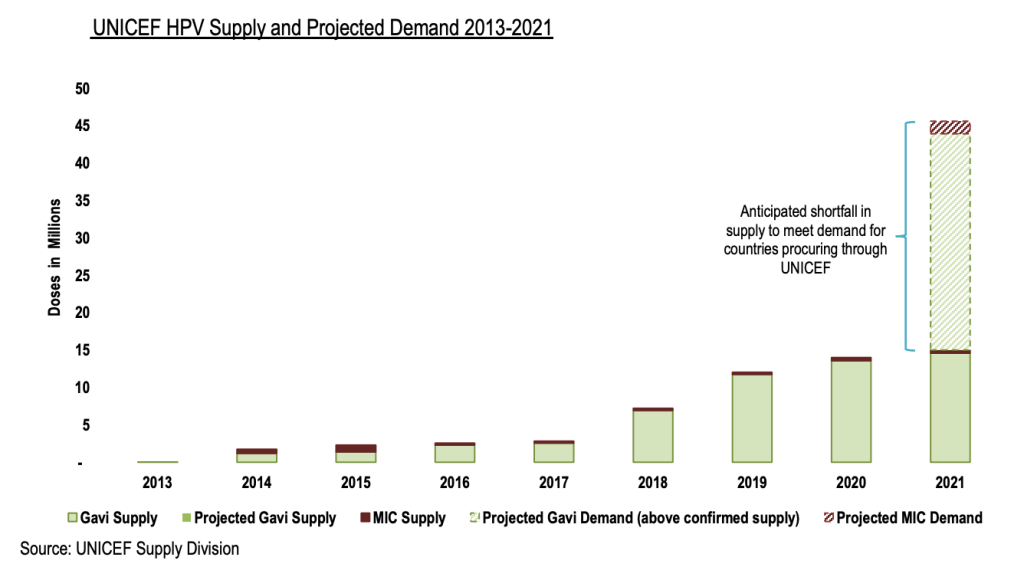
The World Health Organization (WHO) set a goal in 2018 to eliminate cervical cancer by increasing HPV vaccination uptake globally. This initiative has shown to be successful in addressing disparities in low- and middle-income countries however, in 2020 an HPV vaccination shortage began and is expected to continue through 2025.
The Center for Strategic and International Studies (CSIS) presents several strategies that can be used to address this shortage to keep on track with the goal to eliminate cervical cancer. Efforts must be taken to support facilities developing the HPV vaccine to ensure stockouts do not continue. We need policymakers to lobby for policies that increase funding for vaccination development and establish priority vaccination allocations to countries like Malawi that are experiencing high mortality rates from cervical cancer
Children &Mortality &Vaccine Bill Brieger | 14 Mar 2023
THE RTS,S MALARIA VACCINE: A Solution to Nigeria’s Constant Public Health Crisis
By Blessing George & Chino Nduaka and originally posted in the Social and Behavioral Foundations of Primary Health Care Blog.
 More than 50% of deaths from malaria are from four African countries, and Nigeria heads the list, contributing a significant part at more than 30%. Nigeria faces a major public health burden, with an estimated 65 million cases and over 100,000 deaths in 2021, representing over 50% of malaria cases in West Africa. With most outpatient visits in Nigeria being caused by malaria, this disease has taken a toll on the economy.
Malaria is among the top five causes of under-five mortality in Nigeria. Over the years, various organizations have joined hands in the fight against this deadly disease. However, Nigeria remains at the top of the list contributing significantly to the mortality rate. Insecticide-treated nets (ITNs), indoor residual spraying, and free sharing of anti-malaria drugs for prophylaxis and treatment constitute ways the country has tackled the disease burden. With the funding allocation repeatedly given by international organizations such as the WHO, the World Bank, and the Global Fund channeled to these interventions that have proved somewhat ineffective, we are at crossroads that begs the question, what next?
In 2016, the world’s pioneer malaria vaccine, RTS, S, sold with the brand name, Mosquirix, was introduced for pilot implementation in three malaria-endemic countries. It has been administered to over a million children with positive results on its effectiveness. In 2022, the Nigerian government officially applied to receive the vaccine through GAVI but was hit back with the response that currently, there is an insufficient supply of vaccines.
More than 50% of deaths from malaria are from four African countries, and Nigeria heads the list, contributing a significant part at more than 30%. Nigeria faces a major public health burden, with an estimated 65 million cases and over 100,000 deaths in 2021, representing over 50% of malaria cases in West Africa. With most outpatient visits in Nigeria being caused by malaria, this disease has taken a toll on the economy.
Malaria is among the top five causes of under-five mortality in Nigeria. Over the years, various organizations have joined hands in the fight against this deadly disease. However, Nigeria remains at the top of the list contributing significantly to the mortality rate. Insecticide-treated nets (ITNs), indoor residual spraying, and free sharing of anti-malaria drugs for prophylaxis and treatment constitute ways the country has tackled the disease burden. With the funding allocation repeatedly given by international organizations such as the WHO, the World Bank, and the Global Fund channeled to these interventions that have proved somewhat ineffective, we are at crossroads that begs the question, what next?
In 2016, the world’s pioneer malaria vaccine, RTS, S, sold with the brand name, Mosquirix, was introduced for pilot implementation in three malaria-endemic countries. It has been administered to over a million children with positive results on its effectiveness. In 2022, the Nigerian government officially applied to receive the vaccine through GAVI but was hit back with the response that currently, there is an insufficient supply of vaccines.
 Nigeria tops the list of the global malaria mortality rate and should be prioritized. The Nigerian Ministry of Health, in collaboration with the Nigerian Primary Healthcare agency, needs to fight for the health of its citizens, respond to GAVI, and state the concrete reasons why the country should be prioritized. The goal is to ensure that these vaccines are made available for the under-5 population in Nigeria by 2025 such that in the malaria world report of 2030, Nigeria should not be named a major contributing country to malaria mortality.
Nigeria tops the list of the global malaria mortality rate and should be prioritized. The Nigerian Ministry of Health, in collaboration with the Nigerian Primary Healthcare agency, needs to fight for the health of its citizens, respond to GAVI, and state the concrete reasons why the country should be prioritized. The goal is to ensure that these vaccines are made available for the under-5 population in Nigeria by 2025 such that in the malaria world report of 2030, Nigeria should not be named a major contributing country to malaria mortality.

https://www.everydayhealth.com/malaria/world-health-organization-approves-first-malaria-vaccine/
 Nigeria tops the list of the global malaria mortality rate and should be prioritized. The Nigerian Ministry of Health, in collaboration with the Nigerian Primary Healthcare agency, needs to fight for the health of its citizens, respond to GAVI, and state the concrete reasons why the country should be prioritized. The goal is to ensure that these vaccines are made available for the under-5 population in Nigeria by 2025 such that in the malaria world report of 2030, Nigeria should not be named a major contributing country to malaria mortality.
Nigeria tops the list of the global malaria mortality rate and should be prioritized. The Nigerian Ministry of Health, in collaboration with the Nigerian Primary Healthcare agency, needs to fight for the health of its citizens, respond to GAVI, and state the concrete reasons why the country should be prioritized. The goal is to ensure that these vaccines are made available for the under-5 population in Nigeria by 2025 such that in the malaria world report of 2030, Nigeria should not be named a major contributing country to malaria mortality.