Professor Jane Carlton, PhD, Director of Johns Hopkins Malaria Research Institute was introduced by Dean Ellen MacKenzie to give a Dean’s Lecture entitled “Malaria: History, current status, and the promise of ‘omics and AI.”
Prof. Carlton first gave an overview of JHMRI, which was founded in 2001. She stepped into director role in 2023. She started with the encouraging premise that AI and ‘omics can supercharge our research and pointed out the power of comparative genomics on understanding parasites and disease. Her goal is to translate discovery into real world impact through collaborations.
The talk started with a brief malaria history. Malaria was described as an ancient disease and remains one of top infectious diseases worldwide. There were 2.63 million cases and more than half a million deaths in 83 endemic countries in 2023. Today 44 countries are malaria-free.
Up until now, Prof. Carlton noted, the malaria map has been shrinking. There was a precipitous decline in malaria in India from 23 million cases to 2 million. The disease is a true humanitarian issue with a large impact on people living in resource-limited settings where housing is basic and offers no protection from mosquitoes.
The JHMRI is supported by Bloomberg philanthropies, and from that base faculty research examines, among others, better methods for controlling mosquitoes (see slide), new diagnostic tests and therapeutics, and the next generation of vaccines. Key assets to support research include mosquito insectaries and a malaria parasite core. The insectaries produce 60,000 mosquitoes per week, and with these it is possible to complete the life cycle in the laboratory.
Continuing education is another important function of JHMRI which has three conferences per year including the upcoming World Malaria Day 2025 symposium. One can also learn from the Malaria Minute podcast. The upcoming “Vector Encounter” provides sharing and learning for researchers.
JHMRI studies malaria at field sites in Africa and Asia where country collaborators are partners. Emphasis is on local capacity building in countries like Zambia, Ethiopia, Kenya, and Uganda. Researchers and the national malaria control programs in these countries work hand-in-hand.
JHMRI is involved in developing the next generation of vaccines. One approach if a human monoclonal antibody that prevents malaria infections. Another develops a vaccine that transcends’ malaria parasite strains with structure guided mimicry of an essential P. falciparum receptor-ligand complex enhances cross neutralizing antibodies. A third example asks “How many parasites does it take to cause malaria?” and assesses infection likelihood through mosquito parasite burden.
To understand the theme of her talk, Prof. Carlton reviewed the promise of ‘omics and AI in the context of her work at a center of excellence in India. Pioneering work using Malaria camps in hard-to-reach villages in Odisha, India. The main activities mobilized villagers to gather for mass screening, treatment, education, and intensified vector control. From there, Indoor Residual Spraying was planned and insecticide treated bednets were distributed. Other maternal and child health activities were incorporated. After three rounds/visits in the remote villages a great drop of malaria cases was seen. WHO lauded the camps.
In addition to lessons about the importance of surveillance, mixed strategies, and community mobilization for controlling malaria, the team learned about the growing challenge of reduced effectiveness of Rapid Diagnostic Tests. The problem arose because tests were dependent on a protein that was no longer being expressed due to Pfhrp2 gene deletions, leading to false negative test results. The team was encouraged to identify more proteins to find a more stable and central one to use in testing. Through machine learning, this work is ongoing but promising.
While we are on the verge of several research and programmatic breakthroughs, Prof. Carlton reminded the audience that we are in calamitous times. She recalled that the United States has been the top donor government to malaria efforts through Presidents Malaria Initiative and Global Fund to Fight AIDS, Tuberculosis, and Malaria. PMI was founded in 2005, and has contributed to a decline in malaria death rates of close to 50%.
With suspension of funding, an estimated increase of 12.5-17.9 million malaria cases and 71,000-166,000 malaria deaths are expected this year. Already there are serious impacts on the supply chain for major malaria commodities as estimated by the Roll Back Malaria Partnership as seen on their RBM dashboard and supply chain gap estimates where six endemic countries have less than a 3-month supply of RDTs and eleven have less than a 6-month supply.
Prof Carlton ended by saying, “I think the hope is in science, right? The hope is in research. There are definitely new initiatives, new tools which are coming to the forefront, some of which I mentioned, and several of which we’re developing here at the malaria Research Institute. I do know the World Health Organization has got together with other countries to provide additional funding and support for those countries who have lost support through PMI.”
Eyelachew Desta shares thoughts as a guest blogger in time for Mothers’ Day. Concern is expressed about ensuring increased access for low cost essential lifesaving Maternal newborn and child health supplies in Ethiopia. This posting appeared originally at Social & Cultural Basis for Community and Primary Health Programs.
Can you imagine? At this time of Mother’s Day celebration, there are thousands of women living in low income country , unlucky to be a mother to enjoy the celebration of mother’s day because of preventable birth complications due to lack of accesses to essential low cost medicines and commodities necessary for maternal, Child and New born Health. One of these low-income countries is Ethiopia where maternal and child mortality is still high.
According to an analysis published by Reproductive Health Supplies Coalition (RHSC), a quarter of all deaths between 2009 and 2013 occurred in Ethiopia are maternal mortality. This study indicated “postpartum hemorrhage (PPH)— uncontrolled bleeding after childbirth—and preeclampsia/eclampsia (PP/E)- a condition which causes high blood pressure and seizures during pregnancy”, among others, are the two leading causes of maternal deaths in Ethiopia ,could be treated by low cost and effective medicines, Oxytocin and Misoprostol.
See Photo Credit for UNICEF
The availability of accessible, reliable and low cost essential maternal health commodities is indispensable to address maternal and child mortality in Ethiopia. However according to an assessment study conducted in Ethiopia, there are gaps in the supply chain management of commodities for maternal, neonatal, and child health.
According to this study one of these gaps is “The supply chain system for MNCH commodities is inconsistent and has not been integrated into the Integrated Pharmaceutical Logistics System (IPLS)” of Ethiopia. Further the study indicated that family planning, HIV, tuberculosis, and malaria have been included in this IPLS, but not MNCH commodities. This study also identified that there is a lack of common understanding at lower level of the health system about the national policy and protocols as well as its implementation to provide MNCH services and commodities free of charge at primary health care units.
To address these gaps, there is a need of immediate actions as well as strong commitment among all stakeholders involved and engaged in the funding, monitoring, regulating and administering the logistic supply of MNCH commodities in Ethiopia. The Federal Ministry of Health (FMOH) should develop a strategy to provide continues education and training at all levels of the health system about its policy of provision of MNCH services and commodities free of charge at primary health care units , ensure policy protocols are implemented properly.
In addition to these the FMOH should strengthen its monitoring system to identify gaps in the implementation of the MNCH services and commodities policy and take measures to narrow those gaps. The Ethiopia Pharmaceuticals Fund and Supply Agency should revise its Integrated Pharmaceutical Logistics System (IPLS) to insure MNCH commodities are integrated in the system by 2020. Ultimately international donors like USAID needs to continue and strengthen their financial and technical support to the overall MNCH program of Ethiopia .
Maya Tholandi, Lolade Oseni, Anne McKenna, Herbert Onuoha, Solofo Razakamiadana, Elsa Nhantumbo, Alain Mikato, Elaine Roman of Jhpiego and the Johns Hopkins Bloomberg School of Public Health shared important Baseline Readiness Assessment Findings from Democratic Republic of the Congo, Mozambique, Madagascar, and Nigeria from the UNITAID-supported TIPTOP on Intermittent Preventive Treatment of malaria in pregnancy at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene as seen below.
Intermittent preventive treatment of malaria in pregnancy (IPTp) is unacceptably low in most of sub-Saharan Africa. A Jhpiego-led consortium is implementing the Transforming Intermittent Preventive Treatment for Optimal Pregnancy (TIPTOP) project, which supports community distribution of quality-assured sulfadoxine-pyrimethamine (SP).
TIPTOP aims to increase IPTp3 coverage from 19% to 50% of eligible pregnant women in project areas in Democratic Republic of the Congo (DRC), Madagascar, Mozambique, and Nigeria. The project, operating from 2017 to 2022, provides quality-assured SP, promotes community awareness, and supports supervision and coordination efforts between health facilities and community health workers (CHWs).
In 2017, a baseline assessment examined facility readiness for malaria in pregnancy management, antenatal care (ANC) provider knowledge, CHW characteristics and health facility linkages, and health management information system (HMIS) quality. TIPTOP assessed 140 facilities and interviewed 175 ANC providers and 67 CHW supervisors.
At project startup, the teams examined SP stock, ANC providers and CHW availability. SP Stock assessment showed a disparate stock maintenance processes and stock-out next steps indicate lack of a coherent and consistent approach to stock monitoring. In half of all cases, caregivers offer a prescription when stock is not available in the facility, with smaller numbers requesting.
Among ANC providers, 80% on average correctly reported that at least three doses of IPTp are recommended. On average, 64% correctly responded that SP should be initiated in the second trimester. Out of the 170 providers interviewed across countries, only five knew all the key signs of suspected malaria.
A low numbers of CHWs in some districts may limit their reach and capacity. Inadequate CHW education and ANC familiarity may diminish training effectiveness. In particular, low numbers of female CHWs may decrease community acceptance and pregnant women’s acceptability of receiving IPTp from CHWs.
Data Quality and Availability from the routine services would affect monitoring of interventions. Over-reporting of ANC contacts and IPTp service provision is a data quality challenge. The HMISs in Nigeria and Mozambique record IPTp3 provision, but only at the local level. Supervising facilities do not always review data before HMIS entry for accuracy.
Concerning Monitoring and Evaluation System Components, Mozambique’s HMIS is the strongest of the four countries in terms of linking to the national system, current tools and reporting forms available in the facilities, and providers reporting an understanding of indicators and data reporting processes. Nigerian facilities had limited knowledge of indicators and their definitions, despite this information being available in Federal Ministry of Health-provided registers. Madagascar struggled with indicator definitions and data management processes. DRC faced the most challenges: Tools and reporting forms were not available in health facilities, and there were limited monitoring and evaluation structures and processes.
In Conclusion, Results from the baseline assessment are Informing efforts to improve data quality and CHW facility data flow in TIPTOP implementation areas. There is need to strengthen ANC provider knowledge through TIPTOP-supported trainings. One also needs to address CHW variation by country and support health facilities to monitor their SP stock. These findings are being shared with ministries of health and key stakeholders to inform malaria implementation and data quality efforts.
Haja Andriamiharisoa, Eliane Razafimandimby, Jean Pierre Rakotovao, Jean Eugene Injerona, Zo Harifetra, Lalanirina H. Ravony, Rado Randriamboavonjy, Jocelyn Razafindrakoto, and Laurent Kapesa have been working with the USAID Maternal and Child Survival Program. At the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene they presented their experiences on “Improving Procurement and Redeployment of Malaria Commodities Using SMS and Web Mapping at a District Level in Madagascar,” and are also sharing via this posting.
Malaria is a public health problem in Madagascar. In 2016, the frequency of diseases at health center level, places malaria at the 4th cause of hospital morbidity and mortality. Out of about 30 thirty diseases, malaria accounts for 5.6% of all cases.
Health facilities often experience commodity stock-outs of products used for malaria prevention and case management. The existing logistics reporting system does not allow for macro or micro views of the monthly stock situation at the health facility level, which inhibits rapid decision-making.
On January 2018, implementation of a fast data collection system and easy-to-use data visualization began. The tool was based on the use of SMS and web mapping to map the level of monthly keys stock of commodities. The data are sent by providers at facility level via structured SMS and are published by a web server by a web mapping process. Note that sending a monthly SMS costs 9 US cents per facility. Providers at 773 health facilities in 16 regions of Madagascar sent monthly SMS (each message cost $0.09) with ART, ACT, and ITN stock levels.
Sample message: “Please send the quantity in stock at the end of month in: ART, ACT, ITN.”
Structure like: “palu csbcode year month ART ACT ITN. Thank you.”
Sample of answer received: “palu 520241031 D A 200 25 0”
Thus was created an easy-to-use tool from data received. It was free to use, and no password was needed. The SMS is simple and short (of 40 forty characters, composed of:
“palu” diminutive of malaria so that the system is ready for data collection from other cases
the health facility code : 520241031
year : here D : as project has implemented sms data collecting system since 2015 = A
month : here A that means January
stock of Injectable Artesunate (ART) : 200
stock of tablet for Artemisinin–based combination therapy (ACT) : 25
stock of Insecticide Treated Nets (ITN) : 0
Providers send SMS after completing the Monthly Activity Report. (CSB = Centre de Santé de Base, or basic health center). The received data are then displayed as web mapping on a Google map background, embedded on a web page. From this screen shot, The page displays a map of stock outs for the selected month, and monthly charts of the stock status of the three commodities. Accessing this website, is open, without restriction.
From the end of January to the end of June 2018, a hundred health facilities sent SMS each month. The data we received shows that on average:
75% Average stock-out of ITN
53% Average stock-out of ART
9% Average stock-out of ACT
The attached three-map picture provides a broad view from three screenshots of the system, showing the evolution of stock-outs at a facility level
Each point represents health facilities:
When the dot is green, this means that the 03 commodities are available in stock
When in brown, at least one of the 03 elements is unavailable
At first sight, there are more stockouts than stock availability and a tendency of the reduction of green points over the months
Appropriate decision-making would change the points of the map of the following months to green
After this broad view of the country’s overall situation and given the large number of facilities with out of stock, an emergency supply for all districts was done for some medicine since February 2018. Based on maps and stats, we could improve our interventions at a CSB level through rapid and adequate decision-making as in the supply of ITN and ART.
In conclusion, the use of SMS data collection to map stock-outs online can quickly improve input supply through simple spatial analysis. Sending SMSs to alert district-level officials about overstock in facilities at the same district level can solve many stock-out issues. All districts were restocked using this SMS and Web mapping system, but routing to the CSBs remains a challenge. Punctual stock-out reporting could significantly reduce the morbidity and mortality caused by malaria.
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A- 14-00028. The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government.
The challenges of implementing programs to control malaria in pregnancy based on experiences with US President’s Malaria Initiative Countries was presented at the Malaria World Congress in Melbourne this week. The team included Katherine Wolf, MCSP/Jhpiego, Marianne Henry, PMI/USAID, Lia Florey, PMI/USAID, Gabrielle Conecker, MCSP/Jhpiego, Betsy Hendrickson, MCSP/Jhpiego, Katherine Lilly, MCSP/Jhpiego, Nicholas
Furtado, GFATM, Maria Petro, GFATM, Susan Youll, PMI/USAID, and Julie Gutman, PMI/CDC, and their findings are shared below.
What is the danger of malaria in pregnancy (MiP)? Each year MIP is responsible for 20% of stillbirths in Sub-Saharan Africa, 100,000 Newborn deaths globally, 11% of newborn deaths in Africa and 10,000 maternal deaths globally. Four interventions are aimed at MIP, Intermittent Preventive Treatment in Pregnancy (IPTp), consistent use of insecticide treated nets, effective diagnosis and treatment and low-dose folic acid during antenatal care. IPTp with sulfadoxine-pyrimethamine reduces low birth weight by 29%, severe maternal anemia by 38% and neonatal mortality by 31%. What can be done?
Scale-up and full coverage of the WHO lifesaving interventions
Promote early and regular ANC
Preserve SP efficacy by avoiding its use for treating clinical cases of malaria
Reserve SP stocks for IPTp at ANC clinics
Methodology for MiP country review: Initial survey took place in 23 PMI countries. PMI resident advisors were surveyed, Qualitative and quantitative responses were collected and Input from NMCP/partners was obtained. Country selection resulted in 12 that were Tiptop-implementing countries, represented Geographic diversity, had varied IPTp coverage, and made clear progress or best practices to share.
Desk review including HMIS and house hold survey data, current studies and recent assessments, Selected interviews with PMI resident advisors, Jhpiego field staff and current/former NMCP staff. Analysis was a Review and clarification of qualitative and qualitative data.
The 12 countries included Angola, Benin, Burkina Faso, DRC, Ghana, Kenya, Liberia, Madagascar, Malawi, Nigeria, Senegal, and Zimbabwe (see map). The figure shows that none of these attained 80% of 2 doses of IPTp. The current recommendations are for monthly dosages from the 13th week of pregnancy. Often less that half of those receiving IPTp2 also got IPTp3.
Several health systems findings helped explain the IPT results. For Policy & Implementation, Countries reporting strong, coordinated leadership delivered
high IPTp coverage. With Community Engagement, countries reported a diversity of approaches to community health promotion and service delivery.
Concerning Service Delivery, Many countries struggle to implement MiP policies consistently and with quality in the private sector. Commodities were a challenge. Some countries continue to struggle with SP stockouts at facility level, whether ongoing or episodic. Monitoring and Evaluation processes need to catch up. Countries’ routine information systems are transitioning from tracking IPTp2 to IPTp3.
The team offered several Recommendations.
Strengthen consistency of IPTp policies across malaria and reproductive health programs
Scale up of evidence-based country appropriate
community engagement strategies
Alleviation of supply chain bottlenecks at peripheral level
Inclusion and harmonization of key MIP indicators in routine information systems
For more information please visit www.mcsprogram.org, facebook.com/MCSPglobal and twitter.com/MCSPglobal
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative AgreementAID-OAA-A-14-00028. The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government.
Testing to see if transmission of lymphatic filariasis has stopped in Burkina Faso
Two things we need to note about the list of 20 diseases that the World Health Organization and partners classify as Neglected Tropical Diseases (NTDs). First, diseases like Rabies, Snakebite/envenoming, and Leprosy, while certainly more common in the tropics now, have in the past been global in distribution. Secondly some of the diseases have not been neglected. Onchocerciasis or river blindness has been the focus of a global partnership since 1975, and transmission in the America’s and much of the Sahel in Africa has been halted. Elimination of Dracunculiasis or Guinea Worm has also been the subject of many World Health Assembly Resolutions, and concerted effort has brought the number of cases down from 3.5 million in 1986 to 30 in 2017. What is more to the point about these diseases is that they affect neglected people, the poor and vulnerable in remote rural areas or urban slums.
Still when we can compare NTD control programs with the rise of major disease control efforts like the Global Fund to fight AIDS, Tuberculosis and Malaria, the President’s Emergency Program For AIDS Relief, the President’s Malaria Initiative, World Bank Malaria Booster Program, Global A Vaccine Initiative among others, we can see that the global community has been able to focus major financial resources on a few diseases. Now with the Sustainable Development Goals, that focus expanded from infectious to Non-Communicable Diseases. It is natural therefore to fear that tropical health problems that are responsible for major loss of life and economic capacity will not be adequately addressed.
A system of rewards helped identify the last cases in many guinea worm endemic countries
Based on the World Health Organization’s 2020 Roadmap on NTDs, the London Declaration on NTDs recognized a “tremendous opportunity to control or eliminate at least 10 of these devastating diseases by the end of the decade” (i.e. by 2020). These include eradication of Guinea worm disease, and elimination by 2020 of lymphatic filariasis (LF), leprosy, sleeping sickness {human African trypanosomiasis) and blinding trachoma. In addition drug access programmes should help control by 2020 schistosomiasis, soil-transmitted helminthes (STH), Chagas disease, visceral leishmaniasis and river blindness (onchocerciasis).
Five of the diseases are notable in that they can either be controlled or eliminated through Mass Drug Administration (MDA) using Preventive Chemo-Therapy (PCT). This effort is aided by drug donation programs at the global level and community based MDA at the local level. Ten companies were signatories to the London Declaration and contributed to drug donation programs to achieve MDA. According to WHO,
Preventive chemotherapy is aimed at optimizing the largescale use of safe, single-dose medicines and offers the best means of reducing the extensive morbidity associated with four helminthiases (lymphatic filariasis, onchocerciasis, schistosomiasis and soil-transmitted helminthiases) (6). Additionally, the large-scale administration of azithromycin – a key component of the SAFE strategy for trachoma (that is, lid surgery (S), antibiotics to treat the community pool of infection (A), facial cleanliness (C) and environmental improvement (E)) – is amenable to close coordination and, in future, possibly co-administration with interventions targeted at helminthiases.
Community health workers are the cornerstone of many NTD elimination programs
Targets for the 5 PCT diseases vary. The aim is to eliminate LF and Trachoma by 2020. Although the efforts against onchocerciasis have been running the longest, the refocus from control to elimination meant increasing the geographical scope of intervention, and now elimination may not be feasible until 2025. With a focus mainly on the school aged and based populations, programs against schistosomiasis and STH talk of control, not elimination, although some endemic countries hope that elimination may be possible if the focus of these programs expands. So far, Togo is the only Sub-Saharan African country to have eliminated LF, and Ghana to have eliminated Trachoma.
Partnerships, funding and drug donations need to be strengthened if more countries are to join the ranks of Togo and Nepal.
Prakash Raj Pant and Bhim Acharya of the USAID Supported Maternal and Child Survival Program/Jhpiego (MCSP)and the Epidemiology and Disease Division, Ministry of Health, Nepal presented their case study of developing a quality assurance approach for the Global Fund supported provision of antimalarial drugs at the 7th Multilateral Initiative for Malaria Conference in Dakar. Below are their experiences.
Nepal is in the malaria elimination phase, with a target of 2026 through the Global Fund (GF) malaria grant in process for 2018–2021. The Maternal and Child Survival Program (MCSP) also supported GF HIV/AIDS, TB, and malaria grant implementation.
Quality assured antimalarials are a prerequisite for malaria elimination. This is Mandated by GF quality control policies on pharmaceuticals National Malaria Strategic Plan 2016 states: “quality assured antimalarials should be available at all points of service delivery”. Nepal National Drug Regulation Agency (NDRA) does not have a written quality assurance (QA) policy for GF pharmaceuticals
Developing and Implementing a Successful QAP requires the following Key considerations:
Effective coordination of National Malaria Control Program (NMCP) and stakeholders with NDRA
Approval of QAP by ministry of health (MOH) and GF
Presence of laboratories in the region that are prequalified by the World Health Organization or certified by ISO 17025
Advocacy among high-level MOH officials
Intersectoral collaboration among implementing partners
NDRA’s active role in scheduling inspections
Building the capacity of government entities by bilateral agencies (e.g., WHO, United States Agency for International Development) in the initial phase of QAP implementation
Budgeting for QA activities in grant funds
Next Steps in QAP Implementation start with identifying GF-approved laboratories in region for quality control testing of existing grant-funded products. Then partners must strengthen national medicine testing capacities, and seek accreditation of government laboratories by international bodies in 2–3 years. It is important to Mainstream grant-funded QA activities into the NDRA
Challenges in Resource-constrained countries like Nepal include weak pharmaceutical QA testing capacity of domestic laboratories with no accreditation from international bodies. There is inadequate attention of decision-makers in implementing QA policies.
Take-Home Messages from the experience in Nepal include the fact that QA of pharmaceuticals is a mandatory but often neglected area in many GF grant recipient countries. There is need to integrate QA measures into country’s mainstream drug regulation. Coordination with in-country stakeholders is critical.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of PMI, USAID, or the United States Government.
Njabuliso Lukhele of the Ministry of Health Swaziland shared Swaziland’s experiences in Vaccine Procurement at the recent Regional Immunization Technical Advisory Group (RITAG) Meeting, Johannesburg, South Africa, 05-08 December 2017. A summary of his presentation appears below.
As a Lower Middle Income Country (MIC), Swaziland is not and has never been eligible to receive financial support for its immunization programs through the GAVI Alliance. Therefore, 83% of the health care budget is financed through domestic sources, and only 17% comes from from WHO and UNICEF.
Swaziland has a comprehensive Multi-Year plan (cMYP) that drives investment in immunization covering the period 2017–2021. The Government of Swaziland has been fully funding 100% of vaccine costs and average 96% of routine immunization costs over the last years. The Government of Swaziland procures vaccines and distribute to all service providers (government, regional referral and mission hospitals, public as well as private sector clinics and health facilities).
The vaccine Procurement Process begins as Requisitions are sent by Expanded Program of Immunizations (EPI) unit to the procurement unit through the chief pharmacist through documented minutes. This Minute is approved by the Financial Controller (FC) acknowledging availability of funds to furnish the procurement of the vaccines. Then a Tender document is drafted by both the EPI and procurement unit. Advertisement of tender document then takes place. Tender runs for 30 days as per procurement policy. Procurement of vaccines is done through open tender.
The 5 top vaccines (PCV, IPV, OPV, Rota, Penta) in Swaziland represented 98% of the total costs in 2015-16. While this is a major internal financial obligation, Vaccine procurement for the relatively small population of Swaziland represents approximately 0.2 percent of the overall African market by volume and about 0.4 percent by value. This puts smaller countries at a disadvantage in terms of getting good pricing and negotiating with suppliers.
Swaziland was one of the first countries for the Middle Income Country (MIC) strategy mission The MIC strategy mission recommended the need on generating efficiencies in the management of the programme, in particular in the area of procurement, with a need to explore pooled procurement as well as other options with the aim of maximizing savings on the high costs of vaccines. Government desires to achieve economic efficiency in procurement and consideration of pool procurement mechanism.
The current supplier charged 81,256,196.50 Swaziland Lilangeni (SZL) or roughly $5.8 million for the total package of vaccines needed in 2016. If UNICEF were to provide the same package it would cost SZL 62,215,336.34. or $4.5 million. While commercial suppliers can be paid on delivery, UNICEF requires approval from Ministry of Finance for the advance payment with the need to make sure the funds are sufficient for full payment.
This comparative information had valuable advocacy effect. Earlier this year (2017) a MOU signed between MOH and UNICEF. A commitment letter was sent to UNICEF supply division. Now Swaziland has a more reliable supplier and a more affordable cost, enhancing the Ministry’s capacity to save lives of its citizens. Swaziland can also serve as an example for the many other MICs and countries who are ‘graduating’ from GAVI support.
The Demographic and Health Surveys has released a brief on key indicators from the Ghana Malaria Indicator Survey of 2016. While much of the malaria community is discussing the elimination framework and processes, the reality is that many high burden countries are still trying to scale up basic interventions to achieve universal coverage.
The overall prevalence across the country in children aged 6-59 months at the time of the survey was 27% using Rapid Diagnostic test and 20% using microscopy. Among children reporting fever in the previous two weeks care/advice was sought for only 72%. Although only only 30% received some sort of blood based diagnostic test, 61% of the febrile children were given the antimalarial artemisinin-based combination therapy drugs.
Children are still being treated without the benefit of parasitological testing, a key procedure highlighted in WHO case management guidelines. Presumptive treatment for malaria without testing means that a child could inappropriately receive antimalarial drugs and die of another underlying febrile illness. Appropriate testing and adherence to test results is one of the main areas of focus of Ghana’s grants from the US President’s Malaria Initiative. Improved testing is also an important element in Ghana’s current Global Fund support. Clearly more value for money is needed from these inputs.
Preventive measures as documented in the MIS fare somewhat better., but at present only 73% of households own an insecticide treated bednet. When considering the recommended 1 net for every 2 household members, the indicator drops to 50%. Concerning the typical ‘vulnerable’ populations, we see that only 52% of children below the age of 5 years slept under an ITN the night before the survey; only 50% of pregnant women did likewise.
Malaria prevention in pregnancy results reflect the fact that Ghana has promoted at least three IPTp doses for around ten years. Most pregnant women (78% ) had received the previously recommended minimum of two doses, and now 60% have received at least three doses.
One of the important issues stressed in WHO’s new malaria elimination framework is stratifying the country by prevalence to the lowest level possible in order to plan appropriate interventions. Fortunately the Ghana 217 MIS key indicator brief does stratify prevalence and intervention coverage by region. Prevalence through RDT testing ranges from nearly 5% in the urbanized greater Accra area to 44% in the Central Region. Interestingly ITN use is nearly 20% higher in Central than greater Accra.
Hopefully future planning in Ghana will build on this stratification. Better mobilization of donor, national and private sector resources will address likely issues of stock-outs and increase the likelihood of universal coverage of basic interventions that is needed to move the country along the road to malaria elimination.
The Global Fund Observer (aidspan) has provided information on the 2017-19 allocations by the Global Fund to Fight AIDS, TB and Malaria. Here we take a closer look at the malaria component.
Overall malaria grants account for $US 3.3b or 32% of total funding for the period. This includes 71 countries as follows:
41 countries in WHO’s Africa Region
6 in the Eastern Mediterranean Region
7 in the Americas
10 in Southeast Asia
7 in the Western Pacific
2017-2019 GFATM Allocation
The Global Fund Observer also noted that the GFATM board is very much aware of risks to these grants. An example comes from the management pharmaceuticals. Risks can be found along the whole supply chain process. The GFATM found that, “artemisinin-based combination therapies (ACTs) are more commonly targeted for theft or illegal diversion than are antiretrovirals (ARVs) or medicines for opportunistic infections (OIs).”
In fact the GFATM has identified 40 high or very high risk countries, most of which overlap with the list receiving current grant allocations. Therefore while we praise the provision of needed malaria funds for the upcoming three years, we also call on the Global Fund managers, country coordinating mechanisms, grant recipients and watchdogs in civil society and the media to ensure these grants continue to save lives from malaria.
Sign up for daily or weekly articles from Bill highlighting the most noteworthy developments in newspapers and scientific journals. Click here to register.






 Maya Tholandi, Lolade Oseni, Anne McKenna, Herbert Onuoha, Solofo Razakamiadana, Elsa Nhantumbo, Alain Mikato, Elaine Roman of Jhpiego and the Johns Hopkins Bloomberg School of Public Health shared important Baseline Readiness Assessment Findings from Democratic Republic of the Congo, Mozambique, Madagascar, and Nigeria from the UNITAID-supported TIPTOP on Intermittent Preventive Treatment of malaria in pregnancy at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene as seen below.
Maya Tholandi, Lolade Oseni, Anne McKenna, Herbert Onuoha, Solofo Razakamiadana, Elsa Nhantumbo, Alain Mikato, Elaine Roman of Jhpiego and the Johns Hopkins Bloomberg School of Public Health shared important Baseline Readiness Assessment Findings from Democratic Republic of the Congo, Mozambique, Madagascar, and Nigeria from the UNITAID-supported TIPTOP on Intermittent Preventive Treatment of malaria in pregnancy at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene as seen below. TIPTOP aims to increase IPTp3 coverage from 19% to 50% of eligible pregnant women in project areas in Democratic Republic of the Congo (DRC), Madagascar, Mozambique, and Nigeria. The project, operating from 2017 to 2022, provides quality-assured SP, promotes community awareness, and supports supervision and coordination efforts between health facilities and community health workers (CHWs).
TIPTOP aims to increase IPTp3 coverage from 19% to 50% of eligible pregnant women in project areas in Democratic Republic of the Congo (DRC), Madagascar, Mozambique, and Nigeria. The project, operating from 2017 to 2022, provides quality-assured SP, promotes community awareness, and supports supervision and coordination efforts between health facilities and community health workers (CHWs). At project startup, the teams examined SP stock, ANC providers and CHW availability. SP Stock assessment showed a disparate stock maintenance processes and stock-out next steps indicate lack of a coherent and consistent approach to stock monitoring. In half of all cases, caregivers offer a prescription when stock is not available in the facility, with smaller numbers requesting.
At project startup, the teams examined SP stock, ANC providers and CHW availability. SP Stock assessment showed a disparate stock maintenance processes and stock-out next steps indicate lack of a coherent and consistent approach to stock monitoring. In half of all cases, caregivers offer a prescription when stock is not available in the facility, with smaller numbers requesting.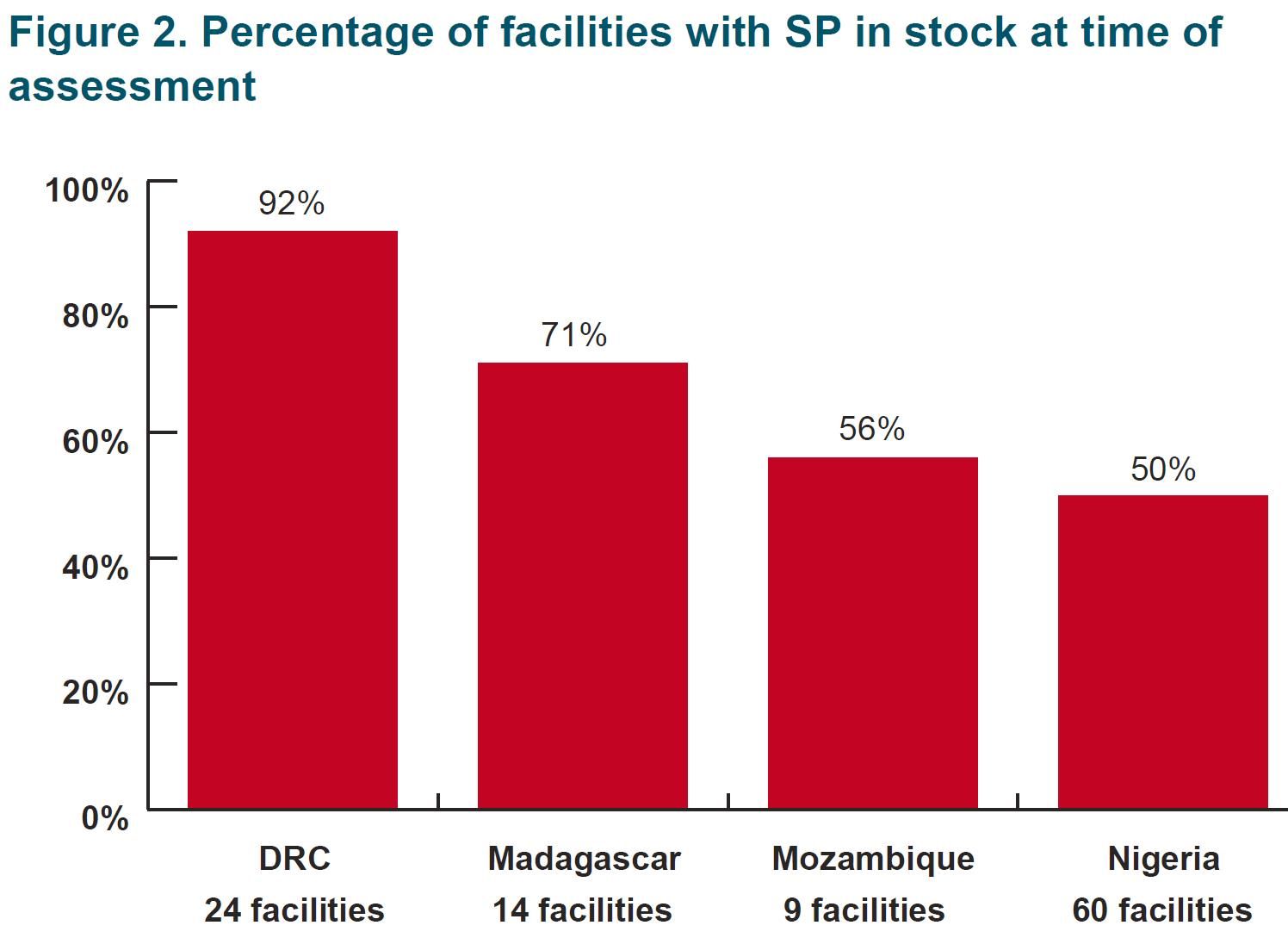 A low numbers of CHWs in some districts may limit their reach and capacity. Inadequate CHW education and ANC familiarity may diminish training effectiveness. In particular, low numbers of female CHWs may decrease community acceptance and pregnant women’s acceptability of receiving IPTp from CHWs.
A low numbers of CHWs in some districts may limit their reach and capacity. Inadequate CHW education and ANC familiarity may diminish training effectiveness. In particular, low numbers of female CHWs may decrease community acceptance and pregnant women’s acceptability of receiving IPTp from CHWs. In Conclusion, Results from the baseline assessment are Informing efforts to improve data quality and CHW facility data flow in TIPTOP implementation areas.
In Conclusion, Results from the baseline assessment are Informing efforts to improve data quality and CHW facility data flow in TIPTOP implementation areas.  There is need to strengthen ANC provider knowledge through TIPTOP-supported trainings. One also needs to address CHW variation by country and support health facilities to monitor their SP stock. These findings are being shared with ministries of health and key stakeholders to inform malaria implementation and data quality efforts.
There is need to strengthen ANC provider knowledge through TIPTOP-supported trainings. One also needs to address CHW variation by country and support health facilities to monitor their SP stock. These findings are being shared with ministries of health and key stakeholders to inform malaria implementation and data quality efforts. Haja Andriamiharisoa, Eliane Razafimandimby, Jean Pierre Rakotovao, Jean Eugene Injerona, Zo Harifetra, Lalanirina H. Ravony, Rado Randriamboavonjy, Jocelyn Razafindrakoto, and Laurent Kapesa have been working with the USAID Maternal and Child Survival Program. At the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene they presented their experiences on “Improving Procurement and Redeployment of Malaria Commodities Using SMS and Web Mapping at a District Level in Madagascar,” and are also sharing via this posting.
Haja Andriamiharisoa, Eliane Razafimandimby, Jean Pierre Rakotovao, Jean Eugene Injerona, Zo Harifetra, Lalanirina H. Ravony, Rado Randriamboavonjy, Jocelyn Razafindrakoto, and Laurent Kapesa have been working with the USAID Maternal and Child Survival Program. At the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene they presented their experiences on “Improving Procurement and Redeployment of Malaria Commodities Using SMS and Web Mapping at a District Level in Madagascar,” and are also sharing via this posting.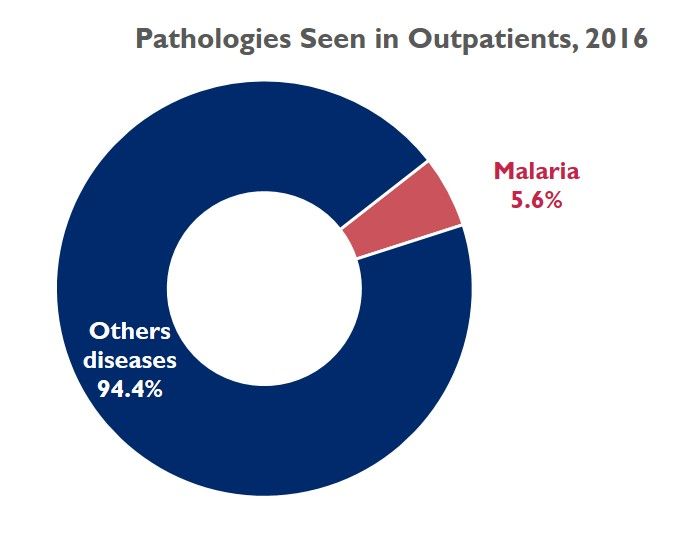 Malaria is a public health problem in Madagascar. In 2016, the frequency of diseases at health center level, places malaria at the 4th cause of hospital morbidity and mortality. Out of about 30 thirty diseases, malaria accounts for 5.6% of all cases.
Malaria is a public health problem in Madagascar. In 2016, the frequency of diseases at health center level, places malaria at the 4th cause of hospital morbidity and mortality. Out of about 30 thirty diseases, malaria accounts for 5.6% of all cases. On January 2018, implementation of a fast data collection system and easy-to-use data visualization began. The tool was based on the use of SMS and web mapping to map the level of monthly keys stock of commodities. The data are sent by providers at facility level via structured SMS and are published by a web server by a web mapping process. Note that sending a monthly SMS costs 9 US cents per facility. Providers at 773 health facilities in 16 regions of Madagascar sent monthly SMS (each message cost $0.09) with ART, ACT, and ITN stock levels.
On January 2018, implementation of a fast data collection system and easy-to-use data visualization began. The tool was based on the use of SMS and web mapping to map the level of monthly keys stock of commodities. The data are sent by providers at facility level via structured SMS and are published by a web server by a web mapping process. Note that sending a monthly SMS costs 9 US cents per facility. Providers at 773 health facilities in 16 regions of Madagascar sent monthly SMS (each message cost $0.09) with ART, ACT, and ITN stock levels.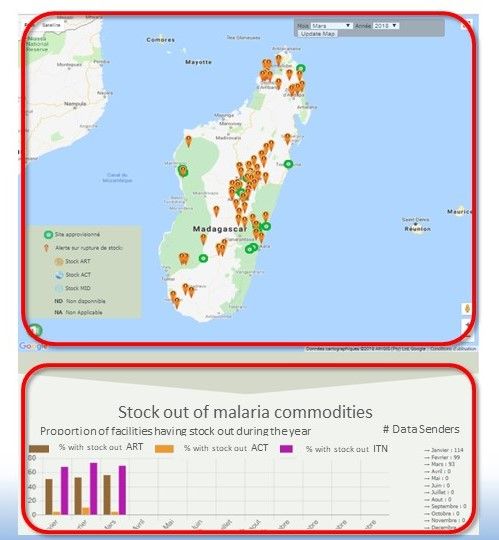 Thus was created an easy-to-use tool from data received. It was free to use, and no password was needed. The SMS is simple and short (of 40 forty characters, composed of:
Thus was created an easy-to-use tool from data received. It was free to use, and no password was needed. The SMS is simple and short (of 40 forty characters, composed of: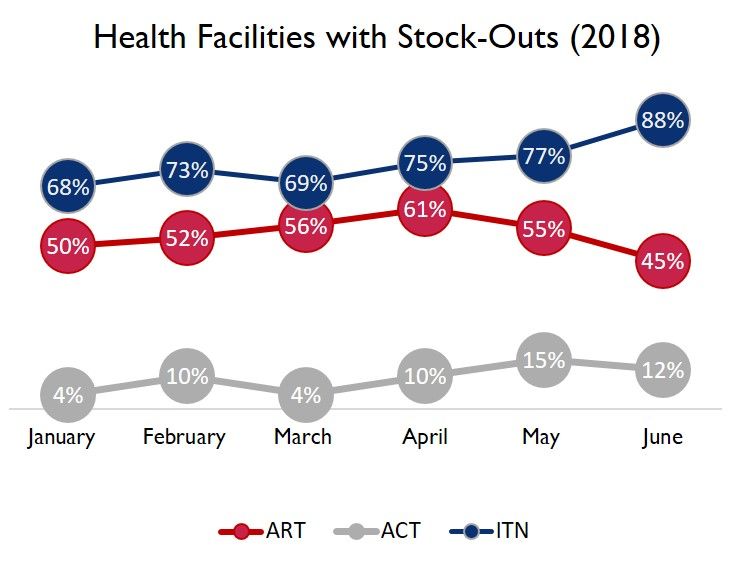 Providers send SMS after completing the Monthly Activity Report. (CSB = Centre de Santé de Base, or basic health center). The received data are then displayed as web mapping on a Google map background, embedded on a web page. From this screen shot, The page displays a map of stock outs for the selected month, and monthly charts of the stock status of the three commodities. Accessing this website, is open, without restriction.
Providers send SMS after completing the Monthly Activity Report. (CSB = Centre de Santé de Base, or basic health center). The received data are then displayed as web mapping on a Google map background, embedded on a web page. From this screen shot, The page displays a map of stock outs for the selected month, and monthly charts of the stock status of the three commodities. Accessing this website, is open, without restriction.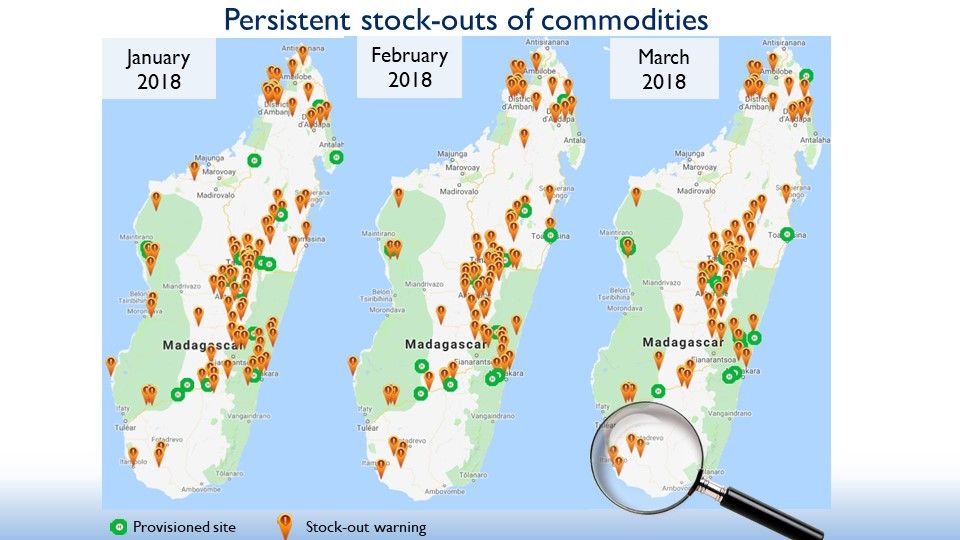 The attached three-map picture provides a broad view from three screenshots of the system, showing the evolution of stock-outs at a facility level
The attached three-map picture provides a broad view from three screenshots of the system, showing the evolution of stock-outs at a facility level After this broad view of the country’s overall situation and given the large number of facilities with out of stock, an emergency supply for all districts was done for some medicine since February 2018. Based on maps and stats, we could improve our interventions at a CSB level through rapid and adequate decision-making as in the supply of ITN and ART.
After this broad view of the country’s overall situation and given the large number of facilities with out of stock, an emergency supply for all districts was done for some medicine since February 2018. Based on maps and stats, we could improve our interventions at a CSB level through rapid and adequate decision-making as in the supply of ITN and ART. What is the danger of malaria in pregnancy (MiP)? Each year MIP is responsible for 20% of stillbirths in Sub-Saharan Africa, 100,000 Newborn deaths globally, 11% of newborn deaths in Africa and 10,000 maternal deaths globally. Four interventions are aimed at MIP, Intermittent Preventive Treatment in Pregnancy (IPTp), consistent use of insecticide treated nets, effective diagnosis and treatment and low-dose folic acid during antenatal care. IPTp with sulfadoxine-pyrimethamine reduces low birth weight by 29%, severe maternal anemia by 38% and neonatal mortality by 31%. What can be done?
What is the danger of malaria in pregnancy (MiP)? Each year MIP is responsible for 20% of stillbirths in Sub-Saharan Africa, 100,000 Newborn deaths globally, 11% of newborn deaths in Africa and 10,000 maternal deaths globally. Four interventions are aimed at MIP, Intermittent Preventive Treatment in Pregnancy (IPTp), consistent use of insecticide treated nets, effective diagnosis and treatment and low-dose folic acid during antenatal care. IPTp with sulfadoxine-pyrimethamine reduces low birth weight by 29%, severe maternal anemia by 38% and neonatal mortality by 31%. What can be done?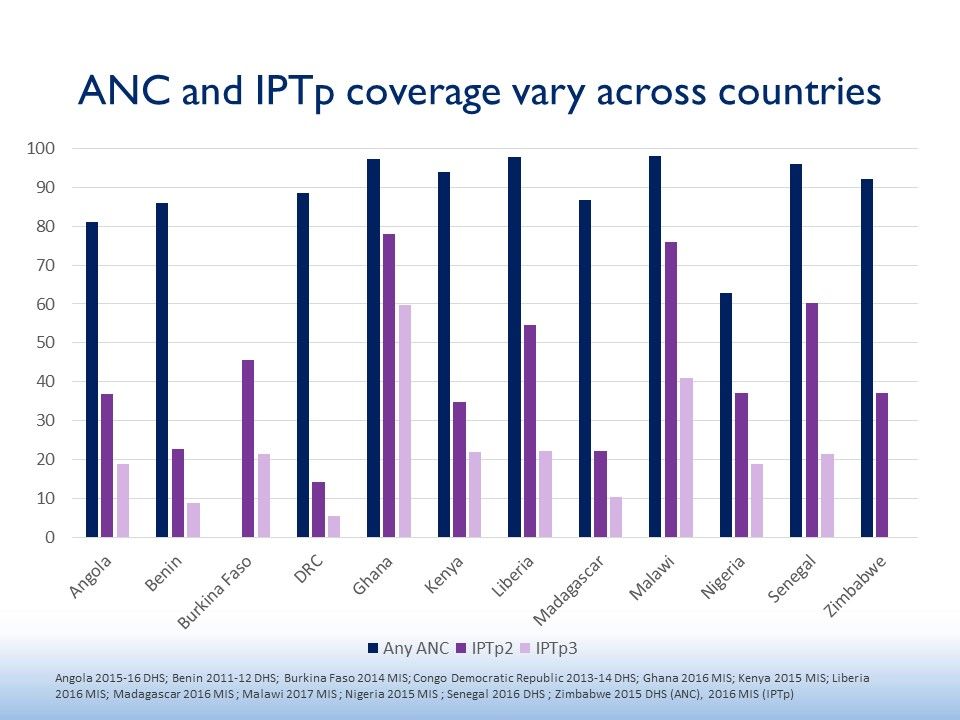 Methodology for MiP country review: Initial survey took place in 23 PMI countries. PMI resident advisors were surveyed, Qualitative and quantitative responses were collected and Input from NMCP/partners was obtained. Country selection resulted in 12 that were Tiptop-implementing countries, represented Geographic diversity, had varied IPTp coverage, and made clear progress or best practices to share.
Methodology for MiP country review: Initial survey took place in 23 PMI countries. PMI resident advisors were surveyed, Qualitative and quantitative responses were collected and Input from NMCP/partners was obtained. Country selection resulted in 12 that were Tiptop-implementing countries, represented Geographic diversity, had varied IPTp coverage, and made clear progress or best practices to share. The 12 countries included Angola, Benin, Burkina Faso, DRC, Ghana, Kenya, Liberia, Madagascar, Malawi, Nigeria, Senegal, and Zimbabwe (see map). The figure shows that none of these attained 80% of 2 doses of IPTp. The current recommendations are for monthly dosages from the 13th week of pregnancy. Often less that half of those receiving IPTp2 also got IPTp3.
The 12 countries included Angola, Benin, Burkina Faso, DRC, Ghana, Kenya, Liberia, Madagascar, Malawi, Nigeria, Senegal, and Zimbabwe (see map). The figure shows that none of these attained 80% of 2 doses of IPTp. The current recommendations are for monthly dosages from the 13th week of pregnancy. Often less that half of those receiving IPTp2 also got IPTp3.


 Nepal is in the malaria elimination phase, with a target of 2026 through the Global Fund (GF) malaria grant in process for 2018–2021. The Maternal and Child Survival Program (MCSP) also supported GF HIV/AIDS, TB, and malaria grant implementation.
Nepal is in the malaria elimination phase, with a target of 2026 through the Global Fund (GF) malaria grant in process for 2018–2021. The Maternal and Child Survival Program (MCSP) also supported GF HIV/AIDS, TB, and malaria grant implementation.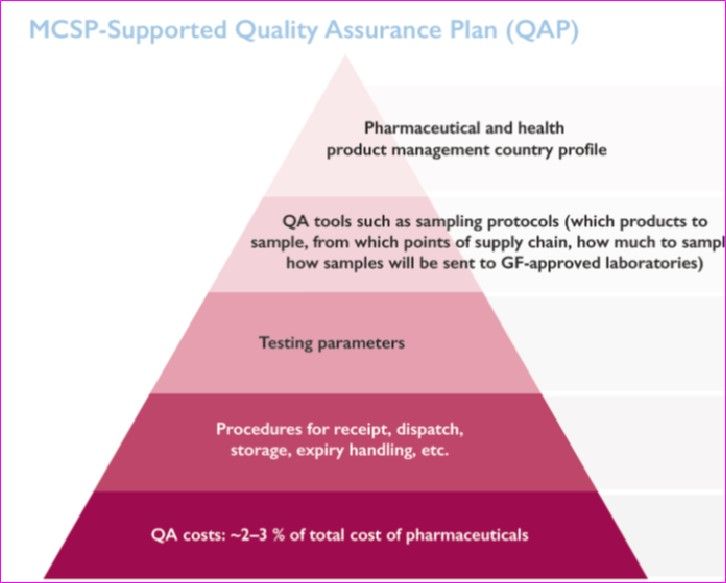 Developing and Implementing a Successful QAP requires the following Key considerations:
Developing and Implementing a Successful QAP requires the following Key considerations: Next Steps in QAP Implementation start with identifying GF-approved laboratories in region for quality control testing of existing grant-funded products. Then partners must strengthen national medicine testing capacities, and seek accreditation of government laboratories by international bodies in 2–3 years. It is important to Mainstream grant-funded QA activities into the NDRA
Next Steps in QAP Implementation start with identifying GF-approved laboratories in region for quality control testing of existing grant-funded products. Then partners must strengthen national medicine testing capacities, and seek accreditation of government laboratories by international bodies in 2–3 years. It is important to Mainstream grant-funded QA activities into the NDRA Challenges in Resource-constrained countries like Nepal include weak pharmaceutical QA testing capacity of domestic laboratories with no accreditation from international bodies. There is inadequate attention of decision-makers in implementing QA policies.
Challenges in Resource-constrained countries like Nepal include weak pharmaceutical QA testing capacity of domestic laboratories with no accreditation from international bodies. There is inadequate attention of decision-makers in implementing QA policies.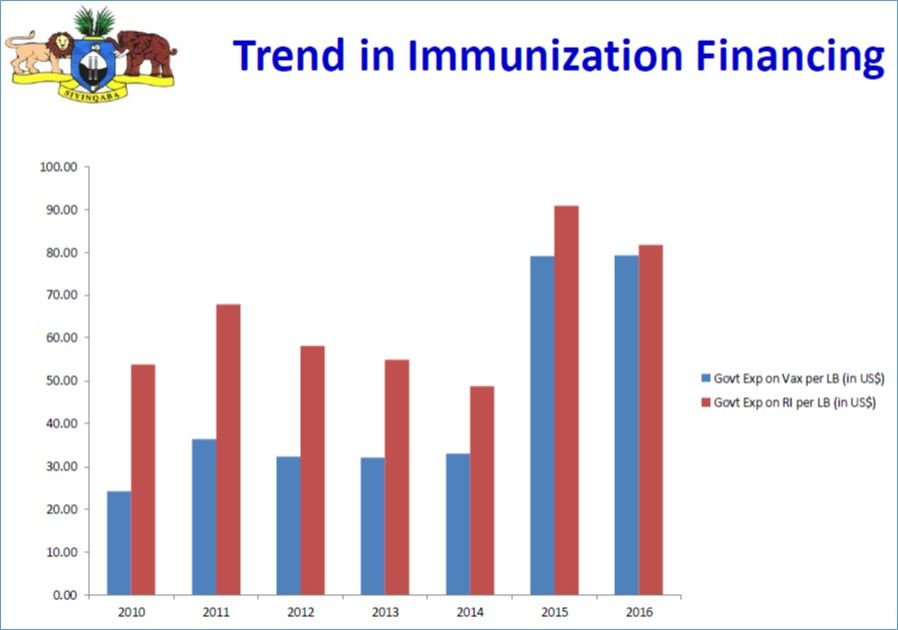 As a Lower Middle Income Country (MIC), Swaziland is not and has never been eligible to receive financial support for its immunization programs through the GAVI Alliance. Therefore, 83% of the health care budget is financed through domestic sources, and only 17% comes from from WHO and UNICEF.
As a Lower Middle Income Country (MIC), Swaziland is not and has never been eligible to receive financial support for its immunization programs through the GAVI Alliance. Therefore, 83% of the health care budget is financed through domestic sources, and only 17% comes from from WHO and UNICEF.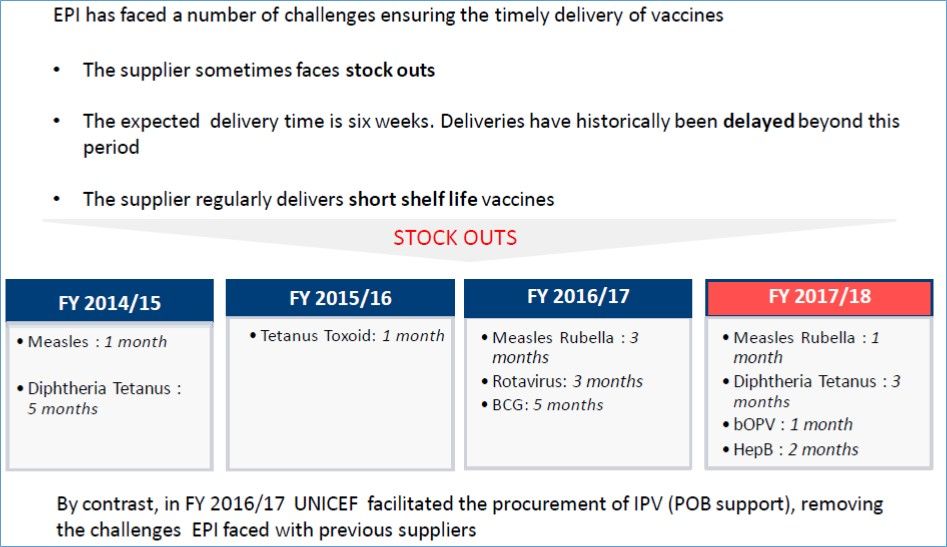 The 5 top vaccines (PCV, IPV, OPV, Rota, Penta) in Swaziland represented 98% of the total costs in 2015-16. While this is a major internal financial obligation, Vaccine procurement for the relatively small population of Swaziland represents approximately 0.2 percent of the overall African market by volume and about 0.4 percent by value. This puts smaller countries at a disadvantage in terms of getting good pricing and negotiating with suppliers.
The 5 top vaccines (PCV, IPV, OPV, Rota, Penta) in Swaziland represented 98% of the total costs in 2015-16. While this is a major internal financial obligation, Vaccine procurement for the relatively small population of Swaziland represents approximately 0.2 percent of the overall African market by volume and about 0.4 percent by value. This puts smaller countries at a disadvantage in terms of getting good pricing and negotiating with suppliers. The Demographic and Health Surveys has released a brief on key indicators from the Ghana Malaria Indicator Survey of 2016. While much of the malaria community is discussing the elimination framework and processes, the reality is that many high burden countries are still trying to scale up basic interventions to achieve universal coverage.
The Demographic and Health Surveys has released a brief on key indicators from the Ghana Malaria Indicator Survey of 2016. While much of the malaria community is discussing the elimination framework and processes, the reality is that many high burden countries are still trying to scale up basic interventions to achieve universal coverage. Children are still being treated without the benefit of parasitological testing, a key procedure highlighted in WHO case management guidelines. Presumptive treatment for malaria without testing means that a child could inappropriately receive antimalarial drugs and die of another underlying febrile illness. Appropriate testing and adherence to test results is one of the main areas of focus of Ghana’s grants from the US President’s Malaria Initiative. Improved testing is also an important element in Ghana’s current Global Fund support. Clearly more value for money is needed from these inputs.
Children are still being treated without the benefit of parasitological testing, a key procedure highlighted in WHO case management guidelines. Presumptive treatment for malaria without testing means that a child could inappropriately receive antimalarial drugs and die of another underlying febrile illness. Appropriate testing and adherence to test results is one of the main areas of focus of Ghana’s grants from the US President’s Malaria Initiative. Improved testing is also an important element in Ghana’s current Global Fund support. Clearly more value for money is needed from these inputs. Malaria prevention in pregnancy results reflect the fact that Ghana has promoted at least three IPTp doses for around ten years. Most pregnant women (78% ) had received the previously recommended minimum of two doses, and now 60% have received at least three doses.
Malaria prevention in pregnancy results reflect the fact that Ghana has promoted at least three IPTp doses for around ten years. Most pregnant women (78% ) had received the previously recommended minimum of two doses, and now 60% have received at least three doses.