coronavirus Bill Brieger | 27 Feb 2020
Policy Implications for Coronavirus
According to the World Health Organization, “Coronaviruses (CoV) are a large family of viruses that cause illness ranging from the common cold to more severe diseases such as Middle East Respiratory Syndrome (MERS-CoV) and Severe Acute Respiratory Syndrome (SARS-CoV). A novel coronavirus (nCoV) is a new strain that has not been previously identified in humans.” The current outbreak that started in Wuhan, China may have first been detected in early December 2019, hence its name COVID-19.
 From the policy perspective there are several global, regional, national and local steps and policies that must be considered. At is second meeting on the novel coronavirus, the WHO Emergencies Coronavirus Emergency Committee on 30 January 2020 recommended and the WHO Director General declared, “We would have seen many more cases outside China by now – and probably deaths – if it were not for the government’s efforts and the progress they have made to protect their own people and the people of the world… I’m declaring a Public Health Emergency of International Concern over the global outbreak of novel coronavirus.”
From the policy perspective there are several global, regional, national and local steps and policies that must be considered. At is second meeting on the novel coronavirus, the WHO Emergencies Coronavirus Emergency Committee on 30 January 2020 recommended and the WHO Director General declared, “We would have seen many more cases outside China by now – and probably deaths – if it were not for the government’s efforts and the progress they have made to protect their own people and the people of the world… I’m declaring a Public Health Emergency of International Concern over the global outbreak of novel coronavirus.”
The PHEIC was declared based on “the IHR, our main international health treaty.” This declaration and treaty enable WHO’s “leadership role for public health measures, holding countries to account concerning additional measures they may take regarding travel, trade, quarantine or screening, research efforts, global coordination, anticipation of economic impacts, support to vulnerable states,” which is where global and national policies and actions may come into concordance or conflict. Clearly some of the more draconian control measures by a few countries were perceived to be beyond the scope of these regulations, policies and treaty.
While as of this writing the spread of COVID-19 appears to slowed in China, it is picking up pace on other continents. The next policy question is whether to name the current outbreak a “pandemic.”
WHO says that, “A pandemic is the worldwide spread of a new disease.” Thus there is community level spread of the disease, not just imported cases from another country. As of today, there is still no evidence of community spread in Africa and Latin America, but a suspected community acquired case has been detected in North America.
Policy and action implications for declaring a pandemic have been spelled out in the Guardian: “a pandemic would mean travel bans would no longer be useful or make sense and would alert health authorities that they need to prepare for the next phase… This includes preparing our hospitals for a large influx of patients, stockpiling any antivirals, and advising the public that when the time comes ,they will need to think about things like staying at home if ill, social distancing, avoiding large gatherings etc.” experts said. And a big challenge for governments would be “encouraging people to change their behaviours, such as forgoing or cancelling large social events if they are sick.”
It is most likely that class members in Social and Behavioral Foundations of Primary Health Care at JHSPH will address some of these policy challenges in their blogs during the coming months.
Children &Indoor Residual Spraying &IPTp &ITNs &Malaria in Pregnancy Bill Brieger | 23 Feb 2020
Preventing Malaria in Mozambique: the 2018 Malaria Indicator Survey Summarized
 The Demographic and Health Survey Program has recently released the 2018 Malaria Indicator Survey for Mozambique. Below is a summary of some of the key findings. These focus on access and use of insecticide-treated nets, intermittent preventive treatment in pregnancy and case management
The Demographic and Health Survey Program has recently released the 2018 Malaria Indicator Survey for Mozambique. Below is a summary of some of the key findings. These focus on access and use of insecticide-treated nets, intermittent preventive treatment in pregnancy and case management
While “82% of Mozambican households have at least one ITN, and half have at least one ITN for each two people,” these achievements do not reach universal coverage targets. That said, the ownership of at least one net by a household did increase from 51% in 2011 to the recent 82%. Likewise 23% of households met the universal coverage target of one net per two people in a household in 2011 compared to 51% in 2018. The pace of progress may appear good, but this must be seen in light of lack of growth in donor funding and greater calls for countries to assume more financial responsibility for disease control.
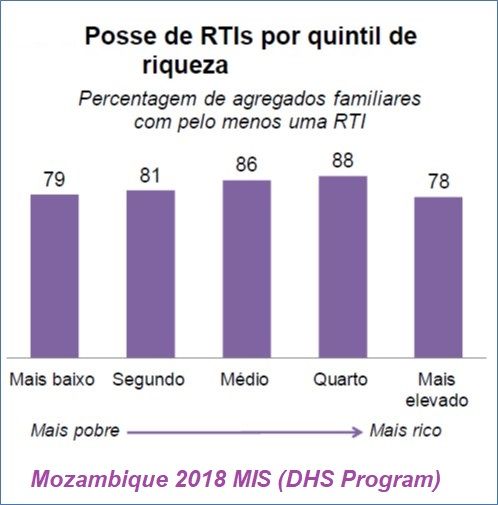 Of interest is the fact that net ownership is spread somewhat evenly over the economic class quintiles. Ideally we would want to see better ownership figures for the lower quintiles.
Of interest is the fact that net ownership is spread somewhat evenly over the economic class quintiles. Ideally we would want to see better ownership figures for the lower quintiles.
Households obtained their nets from three major sources. “Most ITNs (87%) were obtained in mass distribution campaigns, 4% in prenatal consultations (PNC) and 6% are purchased in stores or markets.” While the proportion getting their nets through PNC may roughly reflect the proportion of the population who are pregnant at a given time, the survey is not specifically a snapshot of this population in real time. Thus, one could question whether distribution of ITNs through routine health services is fully functioning.
Since it was noted that only half of households have the ideal number of ITNs to reach universal coverage of their members, it is not surprising that only, “69% of the population of households’ family members have access to an ITN. This means that 7 in every 10 people could sleep under an ITN if each ITN in a household were used by a maximum of two people.” On the positive side, this represents an approximate doubling of use of ITNs since 2011.
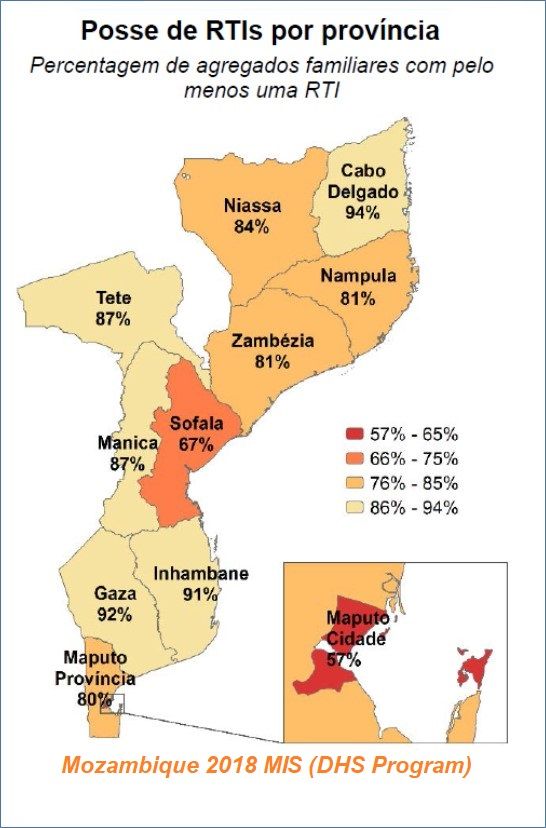 The survey further notes that those segments of the population traditionally viewed as “vulnerable” fared a bit better: “73% of children under 5 years and 76% of pregnant women slept under an ITN the night before investigation.” This too, represents a doubling from 2011. There is also geographical variation where it appears that the more rural provinces have higher rates of use.
The survey further notes that those segments of the population traditionally viewed as “vulnerable” fared a bit better: “73% of children under 5 years and 76% of pregnant women slept under an ITN the night before investigation.” This too, represents a doubling from 2011. There is also geographical variation where it appears that the more rural provinces have higher rates of use.
It would appear that IRS is not a major component of malaria control. Household coverage with indoor residual spray “decreased from 19% in 2011 to 11% in 2015, and then increased to 16% in 2018.” Urban coverage (23%) of IRS in the twelve months prior to the survey is twice as high as the percentage in rural areas (12%).
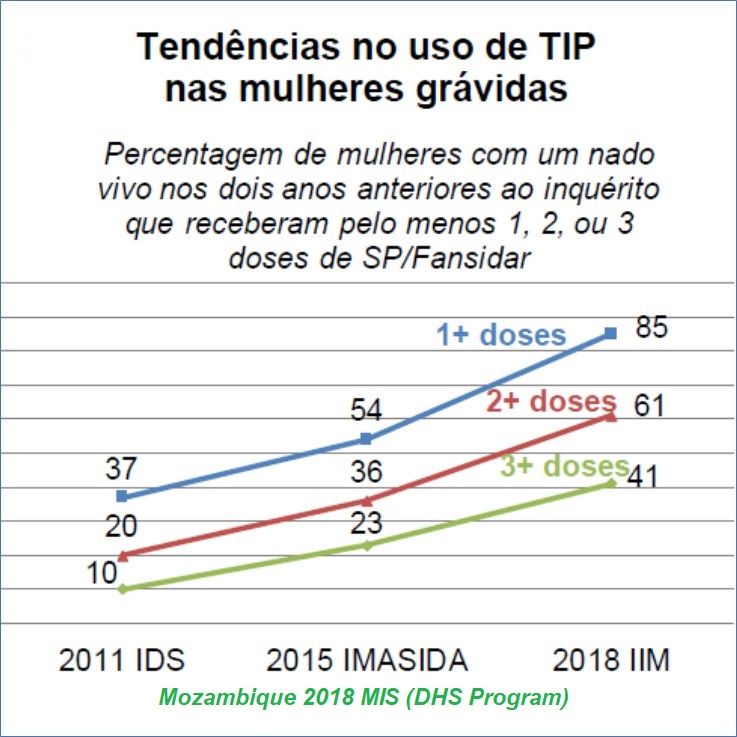 Although still not meeting targets, Mozambique has seen major progress in providing IPTp for pregnant women. Over the period from 2011 to 2018 the proportion of pregnant women receiving even one dose rose from 37% to 85%. Since WHO has set targets for at least 3 monthly doses from the 13th week of pregnancy, Mozambique’s coverage of the third dose increased from 10% to 41% with wide variation among provinces.
Although still not meeting targets, Mozambique has seen major progress in providing IPTp for pregnant women. Over the period from 2011 to 2018 the proportion of pregnant women receiving even one dose rose from 37% to 85%. Since WHO has set targets for at least 3 monthly doses from the 13th week of pregnancy, Mozambique’s coverage of the third dose increased from 10% to 41% with wide variation among provinces.
UNICEF shared data from 2015 to show that 51% of pregnant women in Mozambique attended 4 PNC/ANC visits, implying that there are missed opportunities for achieving at least 3 doses of IPTp. Also, since more women are now getting the first dose of IPTp, hopefully more can also get an ITN at PNC.
These national surveys (MIS, DHS) are invaluable for assessing progress and planning what interventions need to be strengthened where and among whom. They also show that progress is slow, reinforcing global concerns that malaria elimination will still be a challenge by 2050.