Funding &HIV Bill Brieger | 18 Apr 2025
Securing the Future of HIV/AIDS Treatment in South Africa
As part of the work for the Johns Hopkins University course on Social and Behavioral Foundations of Primary Health Care, Skylar Chapdelaine posted in the class blog about HIV/AIDS Treatment in South Africa.
South Africa has the highest global burden of HIV with over 7.7 million people living with the virus. While over 5 million people are on antiretroviral therapy (ART), the decline of international funding especially from the U.S. President’s Emergency Plan for AIDS Relief challenges the sustainability of this.
For years the United States has played an important role in financing South Africa’s HIV response; however, as this money is expected to be lost, South Africa must seek alternative funding mechanisms to sustain programming.
Initiatives and Challenges
Despite financial uncertainties, South Africa has announced a goal of putting an additional 1.1 million people on treatment by the end of 2025 as a step towards their ending AIDS as a threat by 2030.

However, challenges persist. The loss of funding has already affected healthcare personnel, drug supply chains, and monitoring systems. Community organizations such as the Treatment Action Campaign (TAC) have previously been instrumental in expanding ART access, but the financial constraints are limiting their availability to help advocate for patients.
Additionally, international pharmaceutical companies dominate the ART market. Intellectual property restrictions limit local production making ART expensive and difficult to scale up. Without affordable alternatives, millions with HIV could face interruptions in treatment.
Strategies for Engaging Stakeholders
To influence policymakers to secure a sustainable future for HIV treatment, stakeholders need to be strategically engaged.
One of the most crucial stakeholders in this, the South African National AIDS Council (SANAC), plays an important role in coordinating the national HIV response through uniting multiple sectors. SANAC can lead by organizing regular policy roundtables and cross sector forums that bring government officials, civil society leaders, and private sector representatives together. By facilitating these conversations, SANAC can guide the development of policy briefs that offer evidence based solutions, such as strategies to boost local ART production and sustainable financing models and engage policymakers.
Without urgent action from policymakers to begin securing sustainable funding, millions of South Africans are at risk of disruptions in their treatment.
CHW &Community &Funding &Human Resources &Maternal Health Bill Brieger | 17 Apr 2025
Expanding the Boma Health Initiative (BHI) in South Sudan
As part of the work for the Johns Hopkins University course on Social and Behavioral Foundations of Primary Health Care, posted in the class blog about a community-based health initiative in South Sudan as seen below.
 South Sudan continues to experience high maternal and child mortality rates, limited healthcare access, and a shortage of trained professionals. The Boma Health Initiative (BHI) is a community-based healthcare program that trains and deploys Community Health Workers (CHWs) to deliver maternal care, immunizations, and disease management in underserved areas. While promising, BHI faces funding instability, supply shortages, and a lack of standardized training and supervision. To ensure sustainable impact, I strongly advocate for increased financial investment in CHW’s training as a priority policy goal.
South Sudan continues to experience high maternal and child mortality rates, limited healthcare access, and a shortage of trained professionals. The Boma Health Initiative (BHI) is a community-based healthcare program that trains and deploys Community Health Workers (CHWs) to deliver maternal care, immunizations, and disease management in underserved areas. While promising, BHI faces funding instability, supply shortages, and a lack of standardized training and supervision. To ensure sustainable impact, I strongly advocate for increased financial investment in CHW’s training as a priority policy goal.
For this policy to succeed, we must engage key stakeholders strategically. World Health Organization (WHO) – Department of Health Systems Governance & Financing. WHO supports community-based health models and can provide technical and financial resources. Advocacy Approach: Partner with WHO to champion CHW training through reports, policy dialogues, and media engagement.
 South Sudan’s Ministry of Health (MoH) – Directorate of Community Health Services. As the lead health agency, MoH oversees BHI implementation and CHW workforce management. The advocacy approach should push for MoH to allocate domestic funding for CHW training, ensuring sustainability beyond donor reliance.
South Sudan’s Ministry of Health (MoH) – Directorate of Community Health Services. As the lead health agency, MoH oversees BHI implementation and CHW workforce management. The advocacy approach should push for MoH to allocate domestic funding for CHW training, ensuring sustainability beyond donor reliance.
The World Bank’s Human Development Practice Group funds health initiatives but has not directly committed to BHI. Advocacy approaches include presenting cost-effectiveness evidence to secure investment in CHW training programs.
Some physicians from the South Sudan Doctor’s Association (SSDA) fear CHWs will replace trained professionals, while others support task-sharing. Advocacy approaches include collaborating with SSDA to define CHW roles, ensuring they complement rather than replace professional healthcare providers.
In order to expand BHI and improve CHW training, I urge the South Sudanese government to commit long-term funding. Partners, including WHO and World Bank need to invest in capacity-building initiatives. Finally the SSDA must support CHWs as a critical part of the healthcare system.
Funding &Vector Control &World Malaria Day Bill Brieger | 10 Apr 2025
Global State of Malaria: New Research, Evolving Risks, and Silver Linings
In the lead up to World Malaria Day 2025, the Johns Hopkins Malaria Research Institute held an Expert Briefing for the Media to discuss the Global State of Malaria: New Research, Evolving Risks, and Silver Linings. The session was moderated by Ellen Wilson.
The two experts included Jane M. Carlton, PhD, director of the Johns Hopkins Malaria Research Institute at the Johns Hopkins Bloomberg School of Public Health and a Bloomberg Distinguished Professor in the Department of Molecular Microbiology and Immunology at the School and George Dimopoulos, PhD, MBA, also a professor in the Department of Molecular Microbiology and Immunology.
 The speakers discussed and responded to questions regarding the current state of malaria, the need for global commitment to malaria prevention, control, and research, advancing diagnostics and therapeutics, current mosquito vector control methods and their limitations, and the need for an integrated approach to malaria control. As an overview, attendees were told that malaria is a mosquito-borne disease that in 2023 took nearly 600,000 lives in 83 countries, the majority being children under age 5 years in the WHO African Region. In the U.S., the risk of contracting malaria remains low; however, continued vigilance is needed to prevent increases in both domestic cases from foreign travel and as occurred in 2023 for the first time in 20 years, locally transmitted cases.
The speakers discussed and responded to questions regarding the current state of malaria, the need for global commitment to malaria prevention, control, and research, advancing diagnostics and therapeutics, current mosquito vector control methods and their limitations, and the need for an integrated approach to malaria control. As an overview, attendees were told that malaria is a mosquito-borne disease that in 2023 took nearly 600,000 lives in 83 countries, the majority being children under age 5 years in the WHO African Region. In the U.S., the risk of contracting malaria remains low; however, continued vigilance is needed to prevent increases in both domestic cases from foreign travel and as occurred in 2023 for the first time in 20 years, locally transmitted cases.
Jane Carlton expressed concern that malaria cases had increased from 2022 to 2023, but was hopeful because of innovations such as vaccines, and genetically modified mosquitoes. One could also draw hope from efforts to establish local manufacturing capabilities in endemic countries, including partnerships for African vaccine development and production. And in fact, she noted, in 2022, “one company in Kenya became the first African-based manufacturer to receive WHO pre-qualification for a malaria drug. There is a second Nigerian manufacturer that is making progress.” There are several research organizations and universities in African countries that are working towards new drug and intervention development. Studies are ongoing perhaps to use some local plants as anti-larval treatments.
Prof. Carlton explained that the burden of malaria in India has reduced dramatically. “There’s been about a 70% reduction in cases from just over 6 million in 2017 to 2 million in 2023,” although two million cases is still quite a large number.
Prof. Carlton was also asked about the effect climate change on malaria transmission and the potentially expanding the geographic range of malaria. How are researchers adapting? She observed that, “Yes, that’s a very interesting question. In fact, it goes against intuition in a way but increasing the temperature doesn’t always increase the number of malaria cases. The malaria parasite and the mosquito that carries operate within quite a tight temperature range.
In reality, it can get too hot, but as some areas get wetter and formerly cool areas become warmer due to climate change, malaria transmission can move to new locations. “So, there is an increasing shift and an increasing understanding that surveillance of this particular issue is important,” especially needing to monitor climate contexts. For example, scientists have looking at the invasive Anopheles stephensi, which is severely disrupting activities of National Malaria control programs.
There’s been an analysis from the Oxford Malaria Atlas Project, or MAP, and they have projected that with a freeze for one year of PMI activities, this would result in up to 18 million additional malaria cases and up to 107,000 additional malaria deaths. This represents an increase in morbidity of 13%. This would occur in PMI’s focus geographies across 27 African countries. This analysis doesn’t account for the additional impact of PMI supported diagnostics.
Prof. Carlton observed that “globally, total investments in malaria control reached an estimated $4 billion in 2023, but this already fell short of the $8 billion funding target” of the World Health Organization Roll Back Malaria Partnership.
George Dimopoulos stressed e importance of community engagement in vector control activities. He explained that malaria is one of the diseases of poverty where the poor are disproportionately at risk and impacted. He then responded to a question about gene-drive technology based on the
CRISPR-Cas9 system that can spread mosquito genes in natural populations. “This has advanced very significantly in mosquitoes over the past roughly 10 years.”

Prof. Dimopoulos explained that gene-drive “can also work in all malaria vector species. In this way it becomes a malaria control strategy that could work in all malaria endemic areas.” Prof. Dimopoulos’ team has also done research on the effects of sugars and micro-organisms on the mosquito gut and malaria transmission. “We have shown through our research that the health of the mosquito gut depends on a protein quality control system. With appropriate control interventions, “The mosquitoes become very sick and a large proportion of them will actually die.”
In conclusion, the “Silver Linings” mentioned in the session’s title include advances in both parasite and vector control. Deployment of two malaria vaccines offers one ray of hope. New vector control technologies such as gene-drive, offer another. The speakers encouraged people to attend the upcoming JHU-MRI Malaria Day conference to learn more.
Community &Funding &HIV Bill Brieger | 19 Mar 2024
Resources for HIV Financing in Nigeria: Empowering Local HIV Control Organizations
has posted an important perspective on local and community action in HIV control on the blog for the course Social and Behavioral Foundations of Primary Health Care. See the key issues from that posting below.
Nigeria grapples with one of the highest burdens of HIV/AIDS globally, with an estimated 1.9 million people living with the virus. Despite significant international assistance, the country heavily relies on external financing to combat the epidemic. This dependency on foreign aid is unsustainable in the long term and undermines Nigeria’s ability to address the epidemic effectively, perpetuating health disparities and social inequalities. Marginalized populations, such as women, youth, face heightened vulnerability to HIV infection due to limited access to prevention, treatment, and care services. To confront this pressing issue, empowering local HIV control organizations through increased domestic funding not only enhances their capacity to deliver targeted interventions but also fosters community ownership and sustainability.
 (Photo source: The guardian)
(Photo source: The guardian)
Funding &Vaccine Bill Brieger | 04 Aug 2021
GAVI Press Release: Financing for Malaria Vaccine
Geneva/London, 4 August 2021 – Gavi, the Vaccine Alliance, GlaxoSmithKline (GSK) and MedAccess today announced an innovative financing agreement to guarantee continued production of the antigen for the RTS,S/AS01e malaria vaccine in advance of key decisions regarding its roll-out.
 The RTS,S/AS01e vaccine – the first malaria vaccine to be proven safe and effective in a large Phase 3 clinical trial – is currently being piloted in routine immunisation programmes in Ghana, Kenya and Malawi, through the Malaria Vaccine Implementation Programme (MVIP). The World Health Organization (WHO) is expected to decide later this year whether to recommend the vaccine for broader use based on data emerging from the MVIP. The Gavi Board will then decide whether to finance a new malaria vaccination programme for countries in sub-Saharan Africa. Following its investment of around US$ 700 million in the development of RTS,S,GSK has donated up to 10 million doses for the ongoing pilot programme.
The RTS,S/AS01e vaccine – the first malaria vaccine to be proven safe and effective in a large Phase 3 clinical trial – is currently being piloted in routine immunisation programmes in Ghana, Kenya and Malawi, through the Malaria Vaccine Implementation Programme (MVIP). The World Health Organization (WHO) is expected to decide later this year whether to recommend the vaccine for broader use based on data emerging from the MVIP. The Gavi Board will then decide whether to finance a new malaria vaccination programme for countries in sub-Saharan Africa. Following its investment of around US$ 700 million in the development of RTS,S,GSK has donated up to 10 million doses for the ongoing pilot programme.
In advance of the key decisions from WHO and Gavi and to address the associated uncertainty around future demand, Gavi, GSK and MedAccess have developed an innovative financing solution to ensure continued manufacturing of the vaccine antigen so that it will be immediately available should there be a positive decision to move forward.
Gavi will fund GSK’s continued manufacturing of the RTS,S antigen for a period of up to three years. If the Gavi Board decides to approve a malaria vaccination programme (following a positive WHO recommendation), GSK will credit the value of the Gavi-funded costs towards procurement of finished doses for the Gavi-supported programme. If the Gavi Board decides not to open a funding window for a malaria vaccination programme, MedAccess will replenish Gavi for the majority of costs incurred to that point.
This arrangement will ensure that vaccine doses made from the production of Gavi-funded bulk antigen can be supplied rapidly after a potential WHO vaccine recommendation and Gavi financing decisions. This will help accelerate vaccine access, if a programme is approved, by avoiding the long production ramp-up phase that would occur if GSK had to restart the dedicated antigen production facility.
A MedAccess analysis estimates that this continuous manufacture agreement could catalyse the vaccine reaching up to 7.5 million more children than would otherwise have been possible if there was a production delay.
“Malaria kills over a quarter of a million children every year; this vaccine has the potential to have a real impact on this toll,” said Dr Seth Berkley, CEO of Gavi, the Vaccine Alliance. “That’s why it is vital that we keep production lines running while waiting for important decisions around its use in African populations. This is innovative financing at its best: tackling risk and uncertainty to ensure access to what could be an important additional tool in the battle against malaria.”
“In 2020 we saw that risk-taking finance can accelerate the journey of new vaccines to market,” said Michael Anderson, CEO of MedAccess. “The same idea is at work in this agreement, where smart finance can unlock and secure access to an important product at faster pace. This unique partnership is a prime example of how science, public health expertise and innovative finance can combine to save lives.”
Thomas Breuer, Chief Global Health Officer, GSK, said: “Reaching an agreement to support continuous production of RTS,S bulk antigen is a significant achievement built on a unique funding solution and I congratulate all of the partners involved. Continuity of RTS,S manufacturing now will be crucial in how quickly we can offer malaria protection once WHO, Gavi and implementing countries agree to scale up demand.”
Separate to this agreement, GSK and Bharat Biotech of India will continue activities related to the antigen tech transfer to Bharat Biotech, which will become the sole supplier of the vaccine in 2029, an agreement announced by GSK, Bharat, and PATH earlier this year. GSK will ensure the continuous production of the adjuvant (AS01e).
A Phase 3 trial conducted over 5 years from 2009 to 2014 found that among children aged 5–17 months who received four doses of RTS,S/AS01e, the vaccine prevented approximately 4 in 10 (39%) cases of malaria over 4 years of follow-up and about 3 in 10 (29%) cases of severe malaria, with significant reductions also seen in overall hospital admissions as well as in admissions due to malaria or severe anaemia. The vaccine also reduced the need for blood transfusions, which are required to treat life-threatening malaria anaemia, by 29%.
RTS,S/AS01e is currently being piloted in three African countries (Ghana, Kenya, Malawi) and, despite COVID-19, has achieved and maintained high coverage levels. As of July 2021, two years after the start of vaccinations, more than 2 million RTS,S/AS01e doses have been administered across the three countries and more than 740,000 children have been reached with at least one dose of vaccine.
Ministries of Health are leading the implementation of the vaccine, which is being delivered through routine immunisation programmes, with WHO playing a coordinating role, working in collaboration with GSK, PATH, Unicef and a range of other partners. The programme is funded by Gavi, the Global Fund and Unitaid, with doses donated by GSK, and was designed to address several outstanding questions related to the public health use of the vaccine following the Phase 3 trial.
Diagnosis &Elimination &Funding &IPTp &ITNs &Journalists/Media &Malaria in Pregnancy &Migration &Zero Malaria Bill Brieger | 26 Sep 2020
Malaria News Today 2020-09-26: supporting and strengthening malaria programs
Today’s selection of abstracts and news looks at the role of the media in supporting malaria programs, mass treatment to prevent Imported malaria, problems managing malaria in pregnancy services, malaria research in Mali and health systems strengthening to support malaria control in Guinea. Follow links to read mor details.
GHS calls for media support to eradicate malaria

The media has a role in supporting malaria programs
The Ghana Health Service (GHS) has called on journalists to support the Service to deliver integrated health package through accurate messages towards malaria eradication in the country.“Also, we need your support to set malaria as a national development agenda. This will drive advocacy for political will, increase partnership, availability and accessibility of effective tool for prevention, diagnoses and treatment of malaria in all the vulnerable populations.”
Dr Anthony Adofo Ofosu, the Deputy Director General, GHS, said this at the launch of “Zero malaria starts with me” campaign in Accra. The launch coincided with a sensitisation programme by the African Media and Malaria Research Network (AMMRN), the National Malaria Control Programme and the Speak Up African Organisation. The Deputy Director General said “It is the belief of the GHS that with effective engagement…we will be able to eradicate malaria from the country in the near future.”
Mass radical treatment of a group of foreign workers to mitigate the risk of re-establishment of malaria in Sri Lanka
Following malaria elimination, Sri Lanka was free from indigenous transmission for six consecutive years, until the first introduced case was reported in December 2018. The source of transmission (index case) was a member of a group of 32 migrant workers from India and the location of transmission was their residence reporting a high prevalence of the primary vector for malaria. Despite extensive vector control the situation was highly susceptible to onward transmission if another of the group developed malaria. Therefore, Mass Radical Treatment (MRT) of the group of workers for Plasmodium vivax malaria was undertaken to mitigate this risk.
The workers were screened for malaria by microscopy and RDT, their haemoglobin level assessed, and tested for Glucose 6 phosphate dehydrogenase deficiency (G6PD) using the Care Start RDT and Brewers test prior to treatment with chloroquine (CQ) 25 mg/kg body weight (over three days) and primaquine (PQ, based on G6PD test results) (0.25 mg/kg/day bodyweight for 14 days) following informed consent. All were monitored for adverse events. None of the foreign workers were parasitaemic at baseline screening.
Mass treatment may be an option in prevention of reintroduction settings for groups of migrants who are likely to be carrying latent malaria infections, and resident in areas of high receptivity. However, in the case of Plasmodium vivax and Plasmodium ovale, a more reliable and affordable point-of-care test for G6PD activity would be required. Most countries which are eliminating malaria now are in the tropical zone and face considerable and similar risks of malaria re-introduction due to massive labour migration between them and neighbouring countries. Regional elimination of malaria should be the focus of global strategy if malaria elimination from countries is to be worthwhile and sustainable.
Managing intermittent preventive treatment of malaria in pregnancy challenges: an ethnographic study of two Ghanaian administrative regions
Malaria in pregnancy (MiP) is an important public health problem across sub-Saharan Africa. The package of measures for its control in Ghana in the last 20 years include regular use of long-lasting insecticide-treated bed nets (LLINs), directly-observed administration (DOT) of intermittent preventive treatment with sulfadoxine-pyrimethamine (IPTp-SP) and prompt and effective case management of MiP. Unfortunately, Ghana like other sub-Saharan African countries did not achieve the reset Abuja targets of 100% of pregnant women having access to IPTp and 100% using LLINs by 2015.
This ethnographic study explored how healthcare managers dealt with existing MiP policy implementation challenges and the consequences on IPTp-SP uptake and access to maternal healthcare. Healthcare managers addressed frequent stock-outs of malaria programme drugs and supplies from the National Malaria Control Programme and delayed reimbursement from the NHIS, by instituting co-payment, rationing and prescribing drugs for women to buy from private pharmacies.
 Some clients did not receive the recommended 5?+?doses of SP, others did not obtain LLINs early and some did not obtain treatment for MiP. Healthcare providers felt frustrated whenever they could not provide comprehensive care to women who could not afford comprehensive maternal and MiP care. For Ghana to achieve her goal of controlling MiP, the Ministry of Health and other supporting institutions need to ensure prompt reimbursement of funds, regular supply of programme drugs and medical supplies to public, faith-based and private health facilities.
Some clients did not receive the recommended 5?+?doses of SP, others did not obtain LLINs early and some did not obtain treatment for MiP. Healthcare providers felt frustrated whenever they could not provide comprehensive care to women who could not afford comprehensive maternal and MiP care. For Ghana to achieve her goal of controlling MiP, the Ministry of Health and other supporting institutions need to ensure prompt reimbursement of funds, regular supply of programme drugs and medical supplies to public, faith-based and private health facilities.
Malaria prevention program continuation in Guinea
CRS Guinea is the Principal Recipient (PR) in Malaria prevention program continuation grant by the Global Fund for the new cycle of funding (NFM) (January 2021-December 2023). Community health is a top priority of the Ministry of Health as a primary strategy to increase accessibility and coverage to basic health services. Under the new Global Fund grant, the community health component will be expanded to six districts, in addition to two pilot districts, Kindia and Telimele. CRS will also support coordination with other donors, including World Bank, UNICEF, Gavi, European Union and the Guinea Ministry of Health to implement the national community health strategy in 12 health districts supported by Global Fund malaria project.
The United States and Mali Celebrate 60 Years of Friendship and Partnership
Thirty years ago, our National Institutes of Health created a Malaria Research and Training Center, which is now a component of the International Center for Excellence in Research in Mali. Until today, it serves as a reference center with over 700 Malian scientists and support staff who work on malaria and other infectious diseases. Together, we have dropped malaria prevalence rates in Mali by an astounding 60 percent since 2012.
COVID-19 &Drug Development &Elimination &Funding &Plasmodium/Parasite &Resistance &Vaccine Bill Brieger | 17 Sep 2020
Malaria News Today 2020-09-17
 Leading off our news update are findings from eastern Kenya about a genetic blood grouping that may help prevent malaria. While government leaders in the Asia-Pacific region committed to eliminating malaria, a report from the Gates Foundation explains how COVID-19 has set progress back and without new tools it may take more than 25 years to rid the world of the disease. In that light, Novartis is staking its finances on being able to make medicines that will be accessible and fight malaria. More details and the Gates video can be seen by clicking the links below.
Leading off our news update are findings from eastern Kenya about a genetic blood grouping that may help prevent malaria. While government leaders in the Asia-Pacific region committed to eliminating malaria, a report from the Gates Foundation explains how COVID-19 has set progress back and without new tools it may take more than 25 years to rid the world of the disease. In that light, Novartis is staking its finances on being able to make medicines that will be accessible and fight malaria. More details and the Gates video can be seen by clicking the links below.
How Dantu Blood Group protects against malaria
The secret of how the Dantu genetic blood variant helps to protect against malaria has been revealed for the first time by scientists at the Wellcome Sanger Institute, the University of Cambridge and the KEMRI-Wellcome Trust Research Programme, Kenya. The team found that red blood cells in people with the rare Dantu blood variant have a higher surface tension that prevents them from being invaded by the world’s deadliest malaria parasite, Plasmodium falciparum. The findings were published in Nature and could be significant in the wider battle against malaria.
In 2017, researchers discovered that the rare Dantu blood variant, which is found regularly only in parts of East Africa, provides some degree of protection against severe malaria. The intention behind this new study was to explain why. Red blood cell samples were collected from 42 healthy children in Kilifi, Kenya, who had either one, two or zero copies of the Dantu gene. The Dantu variant created cells with a higher surface tension—like a drum with a tighter skin. At a certain tension, malaria parasites were no longer able to enter the cell.
Novartis ties bond sale to malaria treatment access in sustainability push
Novartis raised 1.85 billion euros on Wednesday from the sale of a bond on which interest payments will rise if the drugmaker fails to expand access to medicines and programmes to combat malaria and leprosy in a number of developing countries.
Investors are increasingly pushing companies to improve their track record on environmental, social and governance (ESG) issues while sustainable investing grows in popularity, spurring an increase in sustainable debt issuance year after year. Novartis’ bond is only the third issue to date to link payments to creditors to company-wide sustainable development targets. By Yoruk Bahceli
Commitment to make Asia Pacific a malaria free region
Government officials from across Asia Pacific have come together during virtual Malaria Week 2020, to reaffirm their commitment to eliminating malaria and strengthening health systems to keep the region safe from health threats. Embracing the theme of “Inclusion. Integration. Innovation.”, officials called for increased collaboration and action to accelerate towards the goal of ending malaria in the region by 2030, at a time when major gains and regional progress are under threat due to disruptions caused by Covid-19.
It could take up to 25 years to eradicate malaria from Africa – Bill Gates
Bill Gates said: “Moving to malaria which is a very awful disease not just to the kids it kills but many kids whose brains are permanently damaged, the economic effects you have with malaria. If we don’t have new tools like vaccines or new ways of killing mosquitoes, it would probably take more than 25 years to get rid of malaria. If we get the new tools and they work, we think it can be done in under 20 years. So the malaria field is both trying to keep the number of deaths down, and we have to deal with the resistance that comes up, that the mosquitoes develop.”
Gates Foundation Report notes that, “We’ve been set back about 25 years in about 25 weeks.” Extreme poverty increased 7% because of COVID-19. In a video included in the Foundation’s report, Bill Gates explains how COVID-19 disrupts the fight against malaria.
Agriculture &Artesunate &Case Management &Children &Drug Development &Elimination &Funding &NTDs &Resistance Bill Brieger | 16 Sep 2020
Malaria News Today 2020-09-15
Malaria Journal released three articles ranging from the relation between malaria and agricultural irrigation, artemisinin resistance on the Myanmar-China border, and efforts at costing malaria elimination interventions. PLoS Medicine examined the quality of malaria clinical management in children. Finally, Frontiers in Cellular and Infection Microbiology reported on a new drug against malaria and toxoplasmosis. Click on links to read more details.
Minimal tillage and intermittent flooding farming systems show a potential reduction in the proliferation of Anopheles mosquito larvae in a rice field in Malanville, Northern Benin
Irrigation systems have been identified as one of the factors promoting malaria disease around agricultural farms in sub-Saharan Africa. However, if improved water management strategy is adopted during rice cultivation, it may help to reduce malaria cases among human population living around rice fields.
A clear reduction of larva density was observed with both intermittent flooding systems applied to minimal tillage (MT?+?IF?+?NL) and intermittent flooding applied to deep tillage (DT?+?IF?+?AL), showing that intermittent flooding could reduce the abundance of malaria vector in rice fields. Recommending intermittent flooding technology for rice cultivation may not only be useful for water management but could also be an intentional strategy to control mosquitoes vector-borne diseases around rice farms.
No evidence of amplified Plasmodium falciparum plasmepsin II gene copy number in an area with artemisinin-resistant malaria along the China–Myanmar border
The emergence and spread of artemisinin resistance in Plasmodium falciparum poses a threat to malaria eradication, including China’s plan to eliminate malaria by 2020. Piperaquine (PPQ) resistance has emerged in Cambodia, compromising an important partner drug that is widely used in China in the form of dihydroartemisinin (DHA)-PPQ. Several mutations in a P. falciparum gene encoding a kelch protein on chromosome 13 (k13) are associated with artemisinin resistance and have arisen spread in the Great Mekong subregion, including the China–Myanmar border. Multiple copies of the plasmepsin II/III (pm2/3) genes, located on chromosome 14, have been shown to be associated with PPQ resistance.
DHA-PPQ for uncomplicated P. falciparum infection still showed efficacy in an area with artemisinin-resistant malaria along the China–Myanmar border. There was no evidence to show PPQ resistance by clinical study and molecular markers survey. Continued monitoring of the parasite population using molecular markers will be important to track emergence and spread of resistance in this region.
Costing malaria interventions from pilots to elimination programmes
Malaria programmes in countries with low transmission levels require evidence to optimize deployment of current and new tools to reach elimination with limited resources. Recent pilots of elimination strategies in Ethiopia, Senegal, and Zambia produced evidence of their epidemiological impacts and costs. There is a need to generalize these findings to different epidemiological and health systems contexts. Drawing on experience of implementing partners, operational documents and costing studies from these pilots, reference scenarios were defined for rapid reporting (RR), reactive case detection (RACD), mass drug administration (MDA), and in-door residual spraying (IRS). These generalized interventions from their trial implementation to one typical of programmatic delivery. In doing so, resource use due to interventions was isolated from research activities and was related to the pilot setting. Costing models developed around this reference implementation, standardized the scope of resources costed, the valuation of resource use, and the setting in which interventions were evaluated. Sensitivity analyses were used to inform generalizability of the estimates and model assumptions.
Populated with local prices and resource use from the pilots, the models yielded an average annual economic cost per capita of $0.18 for RR, $0.75 for RACD, $4.28 for MDA (two rounds), and $1.79 for IRS (one round, 50% households). Intervention design and resource use at service delivery were key drivers of variation in costs of RR, MDA, and RACD. Scale was the most important parameter for IRS. Overall price level was a minor contributor, except for MDA where drugs accounted for 70% of the cost. The analyses showed that at implementation scales comparable to health facility catchment area, systematic correlations between model inputs characterizing implementation and setting produce large gradients in costs. Prospective costing models are powerful tools to explore resource and cost implications of policy alternatives. By formalizing translation of operational data into an estimate of intervention cost, these models provide the methodological infrastructure to strengthen capacity gap for economic evaluation in endemic countries. The value of this approach for decision-making is enhanced when primary cost data collection is designed to enable analysis of the efficiency of operational inputs in relation to features of the trial or the setting, thus facilitating transferability.
Quality of clinical management of children diagnosed with malaria: A cross-sectional assessment in 9 sub-Saharan African countries between 2007–2018
Appropriate clinical management of malaria in children is critical for preventing progression to severe disease and for reducing the continued high burden of malaria mortality. This study aimed to assess the quality of care provided to children under 5 diagnosed with malaria across 9 sub-Saharan African countries. We used data from the Service Provision Assessment (SPA) survey. SPAs are nationally representative facility surveys capturing quality of sick-child care, facility readiness, and provider and patient characteristics across 9 countries, including Uganda (2007), Rwanda (2007), Namibia (2009), Kenya (2010), Malawi (2013), Senegal (2013–2017), Ethiopia (2014), Tanzania (2015), and Democratic Republic of the Congo (2018).
In this study, we found that a majority of children diagnosed with malaria across the 9 surveyed sub-Saharan African countries did not receive recommended care. Clinical management is positively correlated with the stocking of essential commodities and is somewhat improved in more recent years, but important quality gaps remain in the countries studied. Continued reductions in malaria mortality will require a bigger push toward quality improvements in clinical care. Despite increases in the distribution of malaria tests and effective antimalarial medications, significant gaps in the quality of care for pediatric malaria are present in these 9 countries. Further improvements in quality of malaria care may require a better understanding of remaining barriers and facilitators to appropriate management.
Novel drug could be a powerful weapon in the fight against malaria and toxoplasmosis
Princeton researchers are making key contributions toward developing a promising new treatment for the widespread and devastating diseases toxoplasmosis and malaria.
The Princeton scientists specialize in preparing the drug compound into a medicine that is both safe and effective for humans and able to reach its intended sites of action in the body in sufficient doses. An international team of scientists found the new drug—designated JAG21—to be highly effective against parasites in cell-based studies in the lab. After the discovery, team representatives contacted Princeton’s Robert Prud’homme for help in translating the JAG21 compound into a deliverable medication. Prud’homme is a co-author of a study, published in June 2020 in Frontiers in Cellular and Infection Microbiology, that describes the compound and its excellent preliminary results in mice.
Funding &Partnership Bill Brieger | 01 Mar 2019
Malaria: Global Funding, Not Just the Global Fund
The Global Fund sixth Replenishment Conference will take place in October 2019 to raise new funds and mobilize partners toward ending AIDS, TB and malaria by 2030 in alignment with the Sustainable Development Goals. The target is to raise at least US$14 billion “to help save 16 million lives, avert 234 million infections and help the world get back on track to end these diseases.”
 It is not exactly clear how much of this US$14 billion would be pegged for malaria, especially since there are cross-cutting health systems strengthening components to many grants. That said, the total seems to pale in light of the 2018 World Malaria Report estimated investment needs of US$6.6 billion alone for malaria from 2020 onward.
It is not exactly clear how much of this US$14 billion would be pegged for malaria, especially since there are cross-cutting health systems strengthening components to many grants. That said, the total seems to pale in light of the 2018 World Malaria Report estimated investment needs of US$6.6 billion alone for malaria from 2020 onward.
Of course the Global Fund is calling on the private sector to “mobilize at least US$1 billion to step up the fight.” It is not clear whether this should be included in the US14 billion or in addition.
The RBM Partnership notes that “Accounting for more than half of all external resources and 44% of total malaria funds available, the Global Fund represents the leading source of funding for malaria prevention and treatment.” Such non-Global Fund external resources have come from partners like the World Bank, the US President’s Malaria Initiative, DfID and a host of other bilateral, NGO and corporate sources. The implication is that at most 15-20% of current financial investment in malaria has been borne endemic countries.
 RBM also highlights that at the recent African Union meeting, “African Heads of State and Government adopted the 2018 African Union Malaria Progress Report which was prepared by malaria experts from countries in Africa…” This means that the leaders acknowledged that malaria investments and significant achievements already made “are under threat and accelerated action is needed now to get countries back on track.” This led the current chair of the Africa Malaria Leaders Alliance, His Majesty King Mswati III of the Kingdom of Eswatini, to say, “It will take significant resources to achieve malaria elimination. Now, more than ever, we must boost our domestic resources from both the public and private sectors.”
RBM also highlights that at the recent African Union meeting, “African Heads of State and Government adopted the 2018 African Union Malaria Progress Report which was prepared by malaria experts from countries in Africa…” This means that the leaders acknowledged that malaria investments and significant achievements already made “are under threat and accelerated action is needed now to get countries back on track.” This led the current chair of the Africa Malaria Leaders Alliance, His Majesty King Mswati III of the Kingdom of Eswatini, to say, “It will take significant resources to achieve malaria elimination. Now, more than ever, we must boost our domestic resources from both the public and private sectors.”
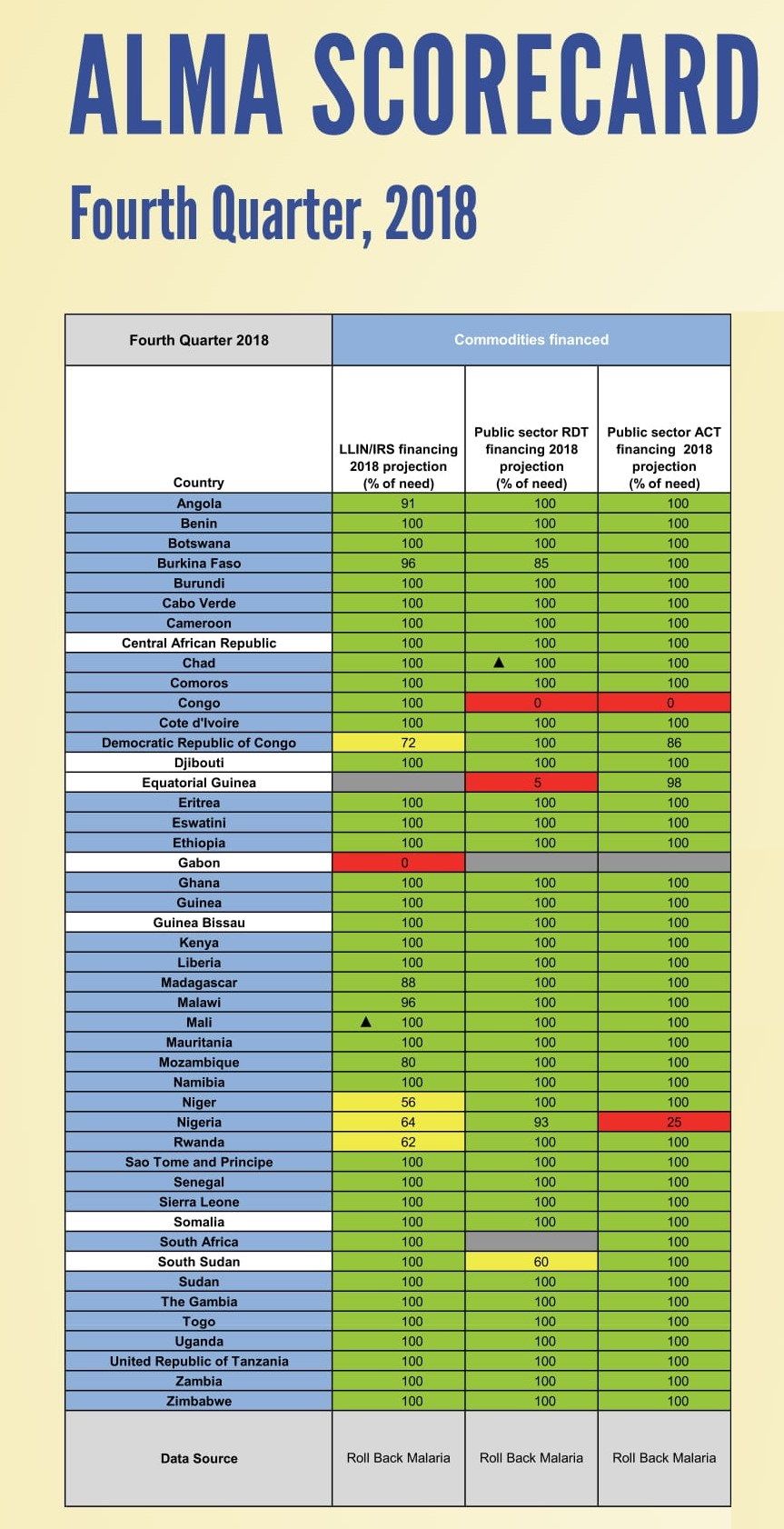
Analysis in the ALMA Scorecard shows in the fourth quarter of 2018 most countries have acquired the needed funds to finance malaria commodities. The analysis does not point out the source of these funds. The 2030 target is only 11 years away. Serious national planning, political will and advocacy are needed not only to prevent resurgence of malaria to pre-RBM days, but also to reduce and eliminate a disease responsible for so much economic loss and loss of life.
Capacity Building &Case Management &Funding &Health Systems &IPTp &ITNs &Leadership Bill Brieger | 09 Feb 2019
Guinea: The Challenge of Malaria Control in a Post-Ebola Context
The preliminary 2018 Demographic and Health Survey (DHS) data have been released for Guinea (Conakry). Since the last DHS in 2012, Guinea and its neighbors experienced the largest Ebola outbreak in history, an event that damaged already weak health systems.
 The previous DHS showed very weak malaria indicators. Only 47% of households had at least one ITN, which averages to 0.8 ITNs per person (compared to the universal coverage of 2.0). Among vulnerable groups only 26% of children below the age of 5 years slept under an ITN, as did 28% of pregnant women. Very few, 18%, pregnant women got two doses of IPTp, and only 5% of febrile children received ACTs (testing was not reported then).
The previous DHS showed very weak malaria indicators. Only 47% of households had at least one ITN, which averages to 0.8 ITNs per person (compared to the universal coverage of 2.0). Among vulnerable groups only 26% of children below the age of 5 years slept under an ITN, as did 28% of pregnant women. Very few, 18%, pregnant women got two doses of IPTp, and only 5% of febrile children received ACTs (testing was not reported then).
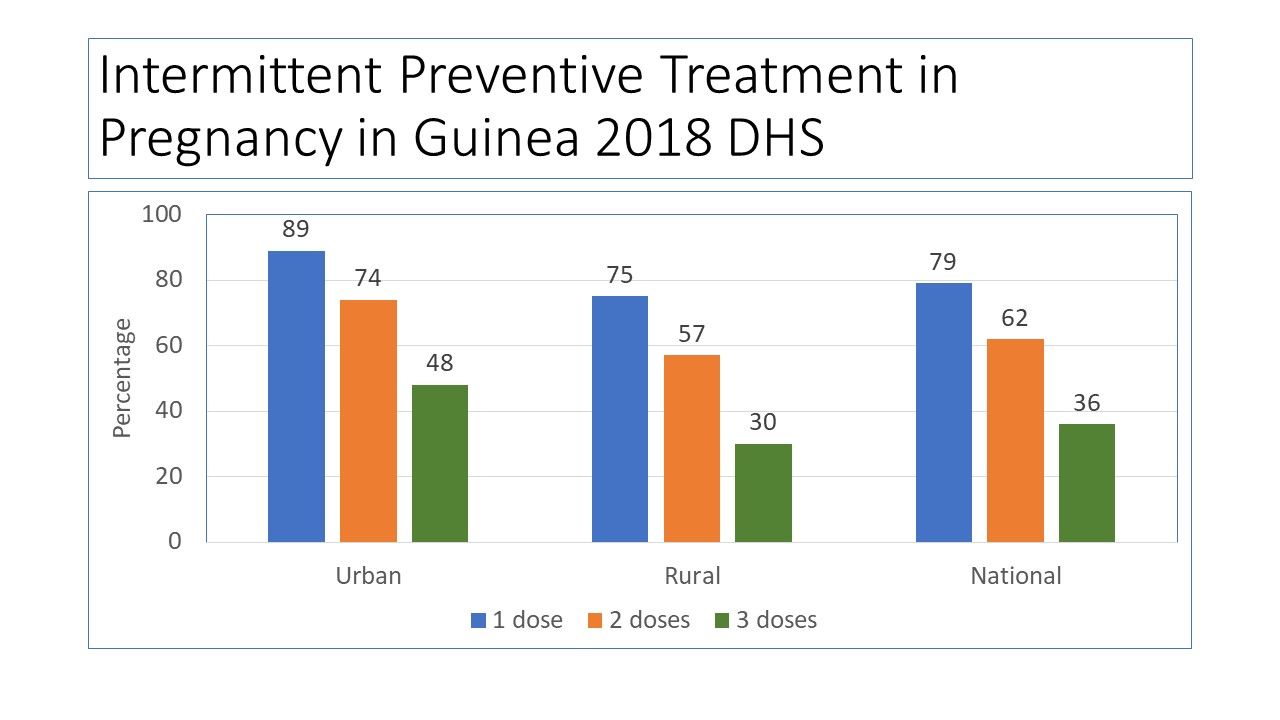
 Not much has changed concerning ITN coverage as reported in 2018. Slight improvements are seen in IPTp (which now requires 3 or more doses) and malaria testing and treatment for children. Ironically none of the indicators has passed the original 2006 Roll Back Malaria target of 60%, let alone 80% for 2010 and not of course the drive for universal coverage.
Not much has changed concerning ITN coverage as reported in 2018. Slight improvements are seen in IPTp (which now requires 3 or more doses) and malaria testing and treatment for children. Ironically none of the indicators has passed the original 2006 Roll Back Malaria target of 60%, let alone 80% for 2010 and not of course the drive for universal coverage.
 DHS has released a preliminary report for 2018 and the malaria component is summarized in the charts posted here. The national coverage for ITNs is 44%, slightly lower than 2012, but the average per household member is slightly higher at 1.1. Again, these numbers do not mark significant progress. Looking at wealth and ITN ownership there is a slight benefit in terms of equity in net possession among those with lower income, but this must be seen in the overall context of very low basic coverage.
DHS has released a preliminary report for 2018 and the malaria component is summarized in the charts posted here. The national coverage for ITNs is 44%, slightly lower than 2012, but the average per household member is slightly higher at 1.1. Again, these numbers do not mark significant progress. Looking at wealth and ITN ownership there is a slight benefit in terms of equity in net possession among those with lower income, but this must be seen in the overall context of very low basic coverage.
 Having a net in the household and using it are different challenges as seen in the reports of sleeping under the net on the night prior to the survey among children under 5 years of age and pregnant women. The sad finding is that even in households that own a net, the coverage of these two groups remains very low. This is reflected in the low net per person ratio nationally (1.1).
Having a net in the household and using it are different challenges as seen in the reports of sleeping under the net on the night prior to the survey among children under 5 years of age and pregnant women. The sad finding is that even in households that own a net, the coverage of these two groups remains very low. This is reflected in the low net per person ratio nationally (1.1).
 One would almost wonder if malaria is a neglected disease in Guinea. The reality is that since 2003, Guinea has received around $172 million US dollars in malaria project funding from the Global Fund. Its most recent annual funding from the US President’s Malaria Initiative (PMI) is around $14 million. Of that PMI funding 24% was designated for nets and related activities, while 52% was to be spent on medicines, diagnostics and pharmaceutical management. These investments include systems strengthening and capacity building in addition to commodities.
One would almost wonder if malaria is a neglected disease in Guinea. The reality is that since 2003, Guinea has received around $172 million US dollars in malaria project funding from the Global Fund. Its most recent annual funding from the US President’s Malaria Initiative (PMI) is around $14 million. Of that PMI funding 24% was designated for nets and related activities, while 52% was to be spent on medicines, diagnostics and pharmaceutical management. These investments include systems strengthening and capacity building in addition to commodities.
PMI provides the needed context: “Since the country was declared Ebola-free in in June of 2016, Guinea continues to make positive advances towards building a strong health system in line with the health recovery plan. The government continues to mobilize internal and external resources for rolling out the health system recovery plan, but much remains to be done if this plan is to yield the intended results.” Areas in particular need of strengthening within the National Malaria Control Program include coordination, health information systems, leadership, supervision and logistics.
Three years have passed since the last Ebola case in Guinea. Hopefully the country can stave off another outbreak and at the same time strengthen its health system. Guinea may not yet be targeted for malaria elimination, but until systems are strengthened, the resources going into malaria control will not be able to push malaria indicators toward saving more lives.