Environment &Epidemiology &Health Systems &Indigenous Medicine &Lassa Fever &NTDs &poverty &Zoonoses Bill Brieger | 30 Apr 2024
Challenges of Lassa Fever in the 21st century: the need for health system accountability
Anthony AHUMIBE is a staff member of Nigeria CDC and presently a doctoral student at the Institute of Tropical Medicine, Nagasaki University, Nagasaki, Japan. Herein he examines the challenges posed by Lassa Fever to the West African region.
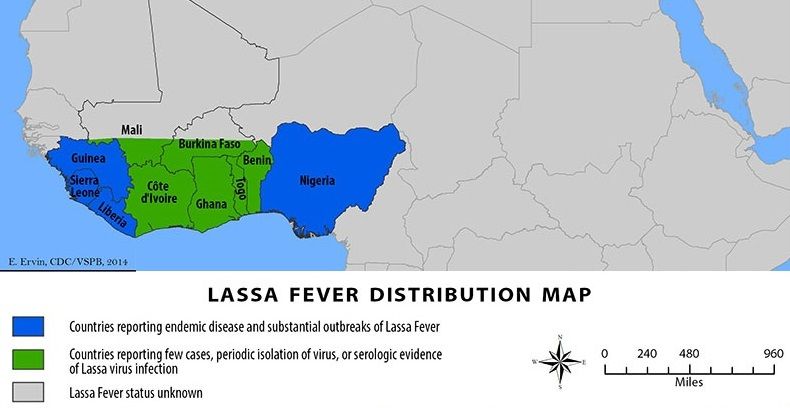
Following the West Africa Ebola epidemic of 2014, the global community has been preoccupied with Lassa fever, a zoonotic viral infection that has caused sickness and death in some communities in Nigeria, Liberia, Sierra Leone, and Guinea. Familiar challenges like absence of vaccine and point of care diagnostics are being handled through investments in research and development. There are, however, some imperceptible yet weighty challenges along the path of Lassa fever control.
The recent finding by Happi and colleagues shows that several species of household rodents, nonspecific to the familiar multimammate rats and other peri-urban small animals carry the Lassa virus and demonstrate that the virus is adapting. Conversely the economic turn of events in the endemic countries indicates that more people are moving into poverty and are unable to make proper hygiene choices. Furthermore, the expansion of city slums, and poor structured housing increases the opportunity for human contact with these rodents, thereby increasing rodents to human virus transmission.
 The table derives from weekly reports published by NCDC. Nigeria Lassa fever data summary for Epi week 15, 2024 is compared with Epi Week 15 cumulative data in 2023 and 2024 (Courtesy: Nigeria CDC Situation report).
The table derives from weekly reports published by NCDC. Nigeria Lassa fever data summary for Epi week 15, 2024 is compared with Epi Week 15 cumulative data in 2023 and 2024 (Courtesy: Nigeria CDC Situation report).
Related to the issue of homestead hygiene is the ineffective management of hospital waste in most of these communities. Many cases of Lassa fever slip through the cracks as malaria fever in health centres with limited capacity for molecular diagnosis. After treatment, body fluid-stained dressings and disposables as well as serum and other body fluids are disposed as waste. The ineffectual medical waste management, so unsupervised, promotes fomite-rodent transmission and genetic spill-over to other species of household animals.
Citizens in the endemic countries share the same burden of poor health infrastructure and limited access to healthcare. For instance, only about 3% of adults aged 15-49 years have a form of health insurance. The high out-of-pocket expenditure required has caused increased hesitance in visiting hospital. As an alternative, many persons become victims of charlatans while genuine traditional healers who approach medical care blindly and without protective equipment become targets of infection and sources of transmission.
 The photo (by author) shows the traditional sun drying of grated cassava for fufu meal. This exposure increases potential for Lassa fever transmission through contamination with rodent excreta.
The photo (by author) shows the traditional sun drying of grated cassava for fufu meal. This exposure increases potential for Lassa fever transmission through contamination with rodent excreta.
The large trust deficit between the citizens and the political leaders owing to the several years of perceived economic and social mismanagement is also a great source of concern. Trust in the system by the people has been affirmed as necessary in advancing the cause of public health. Marcia McNutt and Michael Crow wrote in their op-ed, published in Issues in Science and Technology magazine that scientists and elected leaders need to earn citizens’ trust to win the war against misinformation and disinformation. Hesitancy in uptake of available countermeasures, appropriate risk perception and required behavioural change, seem imperiled in these communities due to the lack of trust in government and government institutions.
Finally, it is often assumed that every new infection cycle is initiated by human contact with rodent or rodent fluid. This does not consider however that the reinfection cycle could have started from a lab leak. Pathogen escape pathways are preponderant with many vials of remnant serum held unaccounted for in many public and private care institutions, some in community hospitals. This can only change if these countries develop a national system for accountability and repository of high-consequence pathogens.
Ebola &Hearing Loss &Lassa Fever &Zika Bill Brieger | 03 Mar 2018
World Hearing Day and the Problem of Infectious and Tropical Diseases
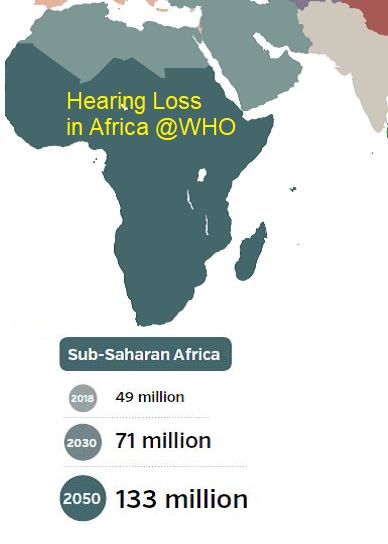
 March 3rd marks the annual World Health Day. The World Health Organization explains that the purpose of this day is to raise awareness on how to prevent deafness and hearing loss and promote ear and hearing care across the world. WHO notes that, “Unless action is taken, by 2030 there will be nearly 630 million people with disabling hearing loss.”
March 3rd marks the annual World Health Day. The World Health Organization explains that the purpose of this day is to raise awareness on how to prevent deafness and hearing loss and promote ear and hearing care across the world. WHO notes that, “Unless action is taken, by 2030 there will be nearly 630 million people with disabling hearing loss.”
Factors associated with health loss and disability include ageing of the population, environmental noise exposure, certain medications, and infectious diseases. It is the latter that we address here.
 Globally there are several infectious diseases associated with hearing loss. In children these include congenital rubella infections a direct result of bacterial meningitis infections, although with improved immunization rates these are less of a problem. In contrast Congenital cytomegalovirus infection has been on the increase.
Globally there are several infectious diseases associated with hearing loss. In children these include congenital rubella infections a direct result of bacterial meningitis infections, although with improved immunization rates these are less of a problem. In contrast Congenital cytomegalovirus infection has been on the increase.
Continuing study of Ebola, Lassa Fever and Zika point to infectious tropical diseases as another serious concern. The large scale of infection and survisorship in Ebola outbreak in West Africa made it possible to study on a large scale reported symptoms of “post-Ebolavirus disease syndrome” (PEVDS) that include, “chronic joint and muscle pain, fatigue, anorexia, hearing loss, blurred vision, headache, sleep disturbances, low mood and short-term memory problems.” A study of 277 Ebola Survivors in one Sierra Leone community found the following clinical sequelae were common: arthralgias (76%), new ocular symptoms (60%), uveitis (18%), and auditory symptoms (24%).
 Lassa Fever has unfortunately made a strong showing in West Africa this dry season. Mateer and colleagues noted an association between Lassa fever (LF) and sudden-onset sensorineural hearing loss (SHNL) was confirmed clinically in 1990. Their literature review found that, “Although LF-induced SNHL has been documented, the prevalence and economic impact in endemic regions may be underestimated.”
Lassa Fever has unfortunately made a strong showing in West Africa this dry season. Mateer and colleagues noted an association between Lassa fever (LF) and sudden-onset sensorineural hearing loss (SHNL) was confirmed clinically in 1990. Their literature review found that, “Although LF-induced SNHL has been documented, the prevalence and economic impact in endemic regions may be underestimated.”
Finally, while much of the focus on the complications of Zika have focused on microcephaly, other problems occur. Zare Mehrjardi et al. documented that Zika Virus may cause “other central nervous system abnormalities such as brain parenchymal atrophy with secondary ventriculomegaly, intracranial calcification, malformations of cortical development (such as polymicrogyria, and lissencephaly-pachygyria), agenesis/hypoplasia of the corpus callosum, cerebellar and brainstem hypoplasia, sensorineural hearing-loss, and ocular abnormalities as well as arthrogryposis in the infected fetuses.”

The benefits of vaccines for rubella and meningitis should spur on immunization research for Ebola, Zika and Lassa Fever. In the meantime there are some preventive measures. One would not have thought that using personal protective equipment by health workers would protect hearing, but it is a practice that should be enabled and encouraged for multiple reasons. Household and community control of Aedes aegypti and rodent breeding to prevent Zika and Lassa, respectively, can also help. By protecting our communities from infection we can also protect their hearing.
Ebola &Infection Prevention &Lassa Fever Bill Brieger | 04 Jun 2016
Poorly Managed Lassa Fever Outbreak in Nigeria
Dr. Obinna O E Oleribe, Chief Executive Officer, E&F Management Care Centre, Abuja Nigeria (Twitter: @OleribeO) shares with readers his view and experiences concerning the August 2015 – May 2016 Lassa Fever outbreak in Nigeria and sees its handling as a strong indicator of weak and failing National Health System.
 On February 6th, 2016, the Vanguard Newspaper reported the growing Lassa Fever outbreak that had killed over 101 persons out of 175 suspected and confirmed cases since August 2015 when the outbreak began in Nigeria. More recently, the World Health Organization (WHO) announced that it had been notified of 273 cases of Lassa fever, including 149 deaths in Nigeria between August 2015 and May 17, 2016. Of the 273, 165 cases and 89 deaths were confirmed through laboratory investigation from 23 states of Nigeria. These deaths include two health care workers out of 10 infected with Lassa fever virus. As at the time of the WHO report (May 17, 2016), eight states were still reporting Lassa fever cases (suspected, probable, and confirmed), deaths and following 248 contacts for the maximum 21-day incubation period.
On February 6th, 2016, the Vanguard Newspaper reported the growing Lassa Fever outbreak that had killed over 101 persons out of 175 suspected and confirmed cases since August 2015 when the outbreak began in Nigeria. More recently, the World Health Organization (WHO) announced that it had been notified of 273 cases of Lassa fever, including 149 deaths in Nigeria between August 2015 and May 17, 2016. Of the 273, 165 cases and 89 deaths were confirmed through laboratory investigation from 23 states of Nigeria. These deaths include two health care workers out of 10 infected with Lassa fever virus. As at the time of the WHO report (May 17, 2016), eight states were still reporting Lassa fever cases (suspected, probable, and confirmed), deaths and following 248 contacts for the maximum 21-day incubation period.
First diagnosed in Nigeria in 1969, Lassa fever (LF) is an acute viral illness caused by Lassa virus, a zoonotic, rodent-borne (multimammate rat), single-stranded ribonucleic acid (RNA) virus from the Arenaviridae, virus family. Since it first isolation in 1969 from a missionary nurse working in Lassa town of Borno State in North-Eastern Nigeria, Lassa Fever has become almost endemic in not only Nigeria, but the West African sub-region as it has continued to be a major public health concern in Nigeria, Liberia, Sierra Leone and Guinea with over 70 million people at risk of the disease. Annually, there are over 3 million cases and about 67,000 deaths from Lassa Fever globally. High association with nosocomial outbreaks, healthcare workers are at increased risk of infection and death. Also, the disease is fast spreading beyond the shores of West Africa into Europe and America from viremic travelers.
A look at the WHO website revealed that Lassa Fever has gained the importance it demanded and was rightly cited on its first page as a disease of public health importance (disease outbreak news). Also, as it is further decreasing the already very limited human resources for health in Nigeria and the rest of West Africa, one would have thought that healthcare managers across the world would have given it the attention it needed.
 In July 2014, Ebola was identified in Nigeria (Lagos State) after Patrick Sawyer imported the disease from Liberia (where there was already an ongoing epidemic). The Lagos State Government, the National Center for Disease Control (NCDC), the Nigerian Field Epidemiology and Laboratory Training Program (NFELTP) and Federal Ministry of Health (FMOH) with the support of well-meaning Nigerian volunteers and some international organizations rose to the occasion and within four months (July 20 – October 20, 2014) kicked Ebola out of Nigeria. They achieved this unbelievable feat through decisive actions, interdisciplinary collaboration, intensive case management, detailed contact tracing, and active port health services. Using isolation, quarantine and supportive management of the infected, case fatality rate was kept at 40% as eight out of the 20 infected individuals succumbed to the virus including several health workers. What was more interesting was the immediate response of government and all relevant stakeholders. The success recorded was to the amazement of the entire world, and completely against all epidemic projects and statistical reasoning.
In July 2014, Ebola was identified in Nigeria (Lagos State) after Patrick Sawyer imported the disease from Liberia (where there was already an ongoing epidemic). The Lagos State Government, the National Center for Disease Control (NCDC), the Nigerian Field Epidemiology and Laboratory Training Program (NFELTP) and Federal Ministry of Health (FMOH) with the support of well-meaning Nigerian volunteers and some international organizations rose to the occasion and within four months (July 20 – October 20, 2014) kicked Ebola out of Nigeria. They achieved this unbelievable feat through decisive actions, interdisciplinary collaboration, intensive case management, detailed contact tracing, and active port health services. Using isolation, quarantine and supportive management of the infected, case fatality rate was kept at 40% as eight out of the 20 infected individuals succumbed to the virus including several health workers. What was more interesting was the immediate response of government and all relevant stakeholders. The success recorded was to the amazement of the entire world, and completely against all epidemic projects and statistical reasoning.
However, few months later, there is another epidemic of another viral hemorrhagic fever. This time around, by a virus that is not as deadly or virulent as Ebola. It has lasted for ten months, killed more people (over 1100% of those killed by Ebola), affected over 800% more cases and with higher case fatality rate of 54%. One, cannot but wonder why Nigeria is finding it difficult to mobilize the same strategies that ended Ebola in Nigeria in 2014 to end Lassa Fever? Or are the structures and personnel not available for this particular outbreak? Or is the will to stop the outbreak lacking among policy makers and healthcare managers?
I believe that there is a need to focus on developing sustainable public health systems that can be mobilized to manage outbreaks across nation; have ready and equipped field workers and foot soldiers who will track, isolate and manage suspected, probable and confirmed cased of any outbreak; and maintain strong surveillance systems able to identify and contain any new, emerging or re-emerging outbreaks.
Nigeria and her leaders should value the lives of the Nigerian people. The government should take health issues more seriously. The citizens of Nigeria need a government that cares. Healthcare workers have a right to live – and not die while working to save other people’s lives. Every hand should be on deck right now to end this outbreak – and as much as possible ensure a delay of its re-emergence.
The time to end Lassa Fever outbreak is NOW. Let us all work towards stopping it once and for all.
Diagnosis &Lassa Fever Bill Brieger | 17 Jan 2016
Lassa Fever in Nigeria
Fever brings to mind ‘malaria’ for most health workers often resulting in dangerous nmis-diagnoses. Not all fevers are alike, and when health workers do not practice infection procedures in examining a febrile patient, they put themselves, their families and all people at their clinic at risk.
 Witness the Ebola outbreak in Guinea, Liberia and Sierra Leone where health workers disproportionately died. And just as happened with Ebola, the Guardian reported that, “A medical doctor in Rivers State has been confirmed dead after being diagnosed of See WHO’s Lassa fever fact sheetin the state’s apex hospital, the Brewaithe Memorial Specialist Hospital (BMH), Port Harcourt.”
Witness the Ebola outbreak in Guinea, Liberia and Sierra Leone where health workers disproportionately died. And just as happened with Ebola, the Guardian reported that, “A medical doctor in Rivers State has been confirmed dead after being diagnosed of See WHO’s Lassa fever fact sheetin the state’s apex hospital, the Brewaithe Memorial Specialist Hospital (BMH), Port Harcourt.”
As of 9th January the death toll rose to 35 with 81 cases. The Guardian Newspaper noted that “Non-Specific Symptoms Of Ailment Threaten Interruption Efforts, ” and that at the rate the current Lassa Fever outbreak is ravaging in the country, the federal government may soon have no option but to declare an emergency to hasten containment.”
By January 16th the number of deaths had risen to 44 as reported by MENAFN.com. They also explained that Lassa is “transmitted through the faeces, urine and blood of rats (and subsequently) human bodily fluids,” of those infected via rats. Rats closely inhabit spaces with humans, while fruit bats that carry Ebola are more confined to forests (which unfortunately have been pushed back through human activity).
Lassa is endemic in Nigeria and West Africa across to Liberia, Sierra Leone and Guinea where some suspected the initial Ebola cases might have been Lassa. The first cases were CDC: documented in Nigeria in 1969, and as the AllAfrica.Com, Guardian: Ministry of Health noted, “Lassa fever which has over the years registered its presence in the country, supposed not to have taken us by surprise.”
The US Centers for Disease Control and Prevention/CDC provides the following useful information showing that while infectious, Lassa may not be as dangerous as Ebola:
- “Signs and symptoms of Lassa fever typically occur 1-3 weeks after the patient comes into contact with the virus. For the majority of Lassa fever virus infections (approximately 80%), symptoms are mild and are undiagnosed. Mild symptoms include slight fever, general malaise and weakness, and headache. In 20% of infected individuals, however, disease may progress to more serious symptoms including hemorrhaging (in gums, eyes, or nose, as examples), respiratory distress, repeated vomiting, facial swelling, pain in the chest, back, and abdomen, and shock. Neurological problems have also been described, including hearing loss, tremors, and encephalitis. Death may occur within two weeks after symptom onset due to multi-organ failure.”
 Finally CDC cautions health workers to protect themselves and not assume every fever is malaria. “When caring for patients with Lassa fever, further transmission of the disease through person-to-person contact or nosocomial routes can be avoided by taking preventive precautions against contact with patient secretions (called VHF isolation precautions or barrier nursing methods). Such precautions include wearing protective clothing, such as masks, gloves, gowns, and goggles; using infection control measures, such as complete equipment sterilization; and isolating infected patients from contact with unprotected persons until the disease has run its course.”
Finally CDC cautions health workers to protect themselves and not assume every fever is malaria. “When caring for patients with Lassa fever, further transmission of the disease through person-to-person contact or nosocomial routes can be avoided by taking preventive precautions against contact with patient secretions (called VHF isolation precautions or barrier nursing methods). Such precautions include wearing protective clothing, such as masks, gloves, gowns, and goggles; using infection control measures, such as complete equipment sterilization; and isolating infected patients from contact with unprotected persons until the disease has run its course.”
While health workers at the front line are encouraged to use malaria Rapid Diagnostic Tests to determine or exclude a diagnosis of malaria, they must remember that RDTs involve blood. Protective materials are always required, even for ‘simple’ malaria. Health systems – public and private – need to ensure health workers have these life saving materials.