ITNs Bill Brieger | 29 Apr 2017
Insecticide Treated Nets in Malawi: Lessons from the 2015-16 Demographic and Health Survey
In 2000 the Abuja Declaration set a target of 80% coverage for people in endemic countries owning AND sleeping under nets by the year 2010. The United Nations came along in 2009 and upped the ante making the target “Universal Coverage.” Such targets were assumed to help countries meet the 2015 Millennium Development Goals for reducing malaria morbidity and mortality. So what happens when these dates pass and countries still have neither achieved nor maintained ITN coverage?
 An example of the remaining challenges can be seen in the 2015-16 malaria section of the Malawi Demographic and Health Survey. The MDHS notes that while household ownership of nets increased from 27% in 2004 to 57% in 2010, it did not change between 2010 and 2015-16. This is despite efforts by the Ministry of health, The US President’s Malaria Initiative and the Global Fund, not to mention peer pressure from the members of the Southern African Development Community who are pushing a malaria elimination agenda.
An example of the remaining challenges can be seen in the 2015-16 malaria section of the Malawi Demographic and Health Survey. The MDHS notes that while household ownership of nets increased from 27% in 2004 to 57% in 2010, it did not change between 2010 and 2015-16. This is despite efforts by the Ministry of health, The US President’s Malaria Initiative and the Global Fund, not to mention peer pressure from the members of the Southern African Development Community who are pushing a malaria elimination agenda.
Even though the actual availability of nets in the households did not increase recently, use or those available improved slightly. The MDHS explains that, “The ITN use among children under age 5 has increased over the years, from 15% in 2004 to 39% in 2010, and 43% in 2015-16. Among pregnant women, ITN use increased from 15% in 2004 to 35% in 2010, and 44% in 2015-16.” This shows some improvement in health education activities, but people cannot use the net that is not available.
Where do the nets come from? Among the nets found in surveyed households newly a third (32%) were acquired through a mass distribution campaign. Nearly half (47%) were acquired through a routine clinic visit such as antenatal care, child birth, immunization clinic and other clinic visits. The remainder were bought from shops or other places. This shows a good mix of distribution strategies. It is therefore, the volume of nets made available that is of concern, possibly more than the process, but further analysis by the national malaria program should examine all of these avenues to ensure efficiency.
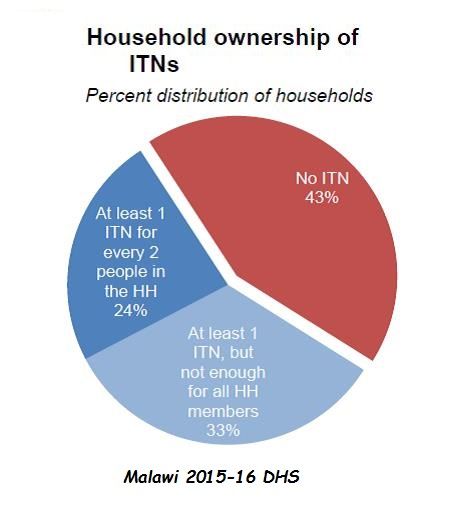
 An irony appears in the pie chart on net availability in households. While 43% did not have any nets, another 33% did not have enough nets to meet coverage targets of one net per two people. This again poses serious access issues. Thus, it is not surprising that 13% of people who in theory have access to nets did not sleep under them.
An irony appears in the pie chart on net availability in households. While 43% did not have any nets, another 33% did not have enough nets to meet coverage targets of one net per two people. This again poses serious access issues. Thus, it is not surprising that 13% of people who in theory have access to nets did not sleep under them.
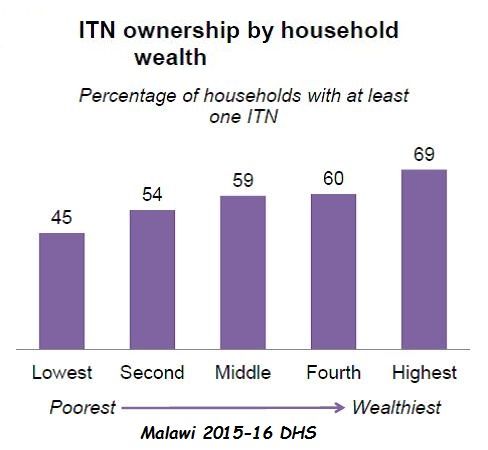
Several other challenges were documented. Only 45% of the poorest segment of the population lived in households with nets, compared to 69% of the wealthiest. Similarly rural populations were less likely to sleep under ITNs (32%) than urban (42%). It would appear that more attention to equity in ITN programs is needed. Interestingly, urban households are more likely to purchase their nets from shops and markets than rural dwellers.
Good news is that the US President’s Malaria Initiative plans to help maintain coverage of pregnant women and children in the coming year through the procurement and distribution of ITNs through routine service channels with 1.2 million ITNs. In addition the Global Fund reports that over 7.7 million ITNs were distributed in Malawi in 2016 with it’s support. Maybe these efforts will reflect in the next iteration of the DHS or MIS, but fluctuations in ITN availability do impact on disease transmission, and concerns about equity will remain.
The DHS and its sister survey, the Malaria Information Surveys are crucial tools for identifying challenges and planning ways to improve coverage of malaria interventions. Hopefully Malawi will be able to use this information to save lives.
CHW &Community &IRS &Treatment Bill Brieger | 27 Apr 2017
Rwanda Celebrates World Malaria Day 2017 – community is a major focus
Dr. Noella Umulisa, the Malaria Team Lead or the USAID Maternal and Child Survival Program in Kigali Rwanda shares with us experiences from Rwanda’s recent observance of World Malaria Day 2017.
The Malaria Day celebration took place in Huye districts in the southern Province. Why the southern province? – because among the 10 high endemic districts, 6 are the southern province. Why Huye district? – because IRS has been launched in Huye district yesterday and in another district Nyanza in Southern province.
 The ceremony was attended by USAID and WHO representative, local leaders, MOH staff, partners, population of Simbi sector and the guest of honour was Dr Jeannine Condo the Director General of Rwanda Biomedical Center (which houses malaria activities).
The ceremony was attended by USAID and WHO representative, local leaders, MOH staff, partners, population of Simbi sector and the guest of honour was Dr Jeannine Condo the Director General of Rwanda Biomedical Center (which houses malaria activities).
A special recognition was given to community health workers (CHWs) who are playing a key role and are on the front line of fighting Malaria through sensitization of the population, testing and treating the population through community case management (iCMM and HBM) of Malaria, and now when a big number of CHWs will be involved in spraying households in their community.
 The World Malaria Day celebration in Rwanda is marked by different activities for Malaria prevention conducted at community level from 24th to 29th April 2017. Also, Malaria prevention and control messages are being disseminated using different communication tools and approaches such as radio and TV programs, community outreach activities, educating communities on proper use of bed nets.
The World Malaria Day celebration in Rwanda is marked by different activities for Malaria prevention conducted at community level from 24th to 29th April 2017. Also, Malaria prevention and control messages are being disseminated using different communication tools and approaches such as radio and TV programs, community outreach activities, educating communities on proper use of bed nets.
Door to door mobilization is being conducted about the Indoor Residual Spraying (IRS) in high malaria burden districts of Huye and Nyanza. MCSP, with support from the US President’s Malaria Initiative, has participated actively in this event by supporting Community outreaches though theatre skits in the first 10 high endemic district.
 The Director General made the following statement:
The Director General made the following statement:
In January 2016, the Government of Rwanda and partners developed a Malaria Contingency Plan in response to the increase in malaria cases. The following interventions were implemented to address malaria rise in Rwanda: A Home Based Management of fever for adults at community level was set up countywide to reduce the malaria burden and prevent severe malaria and death. From Nov 2016 up to March 2017, the country distributed more than 6 million nets in 30 districts ensuring universal coverage of the entire population.
The country has increased access to health services for all through Community Based Health Insurance (CBHI). The Government of Rwanda provides free treatment of malaria to the most vulnerable population (Ubudehe 1&2 categories) to ensure that all financial barriers are no more to hinder the health service delivery for the community. Extension of Indoor residual spraying (IRS) in districts with high malaria burden where 5 out of 8 were sprayed (Nyagatare, Kirehe, Bugesera, Gisagara and Gatsibo).
We hope that this commitment will keep Rwanda on track to control and eventually eliminate malaria.
IPTp &Malaria in Pregnancy Bill Brieger | 27 Apr 2017
Preventing Malaria in Pregnancy – fill the coverage gaps
In a press release for World Malaria Day 2017, the World Health Organization called for the global community to “Prevent malaria – save lives” as part of the WHO push for prevention on World Malaria Day, 25th April. WHO recommended that, “Together with diagnosis and treatment, WHO recommends a package of proven prevention approaches, including insecticide treated nets, spraying indoor walls with insecticides, and preventive medicines for the most vulnerable groups: pregnant women, under-fives and infants.” This package has averted 663 million cases have been averted since 2001.
That said, WHO also identified gaps.
- Approximately 69% of pregnant women in 20 African countries did not have access to the recommended 3 or more doses of preventive treatment.
- An estimated 43% of people at risk (including pregnant Women) of malaria in the region were not protected by either a net or indoor insecticide spraying in 2015
This gap became evident on a recent visit to Ouargaye Health District in Burkina Faso where National Malaria Control Program and Jhpiego, with support from US President’s Malaria Initiative and USAID’s Mother and Child Survival Project, are setting up a pilot program to test community delivery of IPTp through the existing network of community health workers.
 Normally IPTp is delivered as part of antenatal/prenatal care and the new project will use the ANC clinic as a base for training and supervising the CHWs. Health Statistics from the District from 2016 show the challenge that the community approach hopes to address.
Normally IPTp is delivered as part of antenatal/prenatal care and the new project will use the ANC clinic as a base for training and supervising the CHWs. Health Statistics from the District from 2016 show the challenge that the community approach hopes to address.
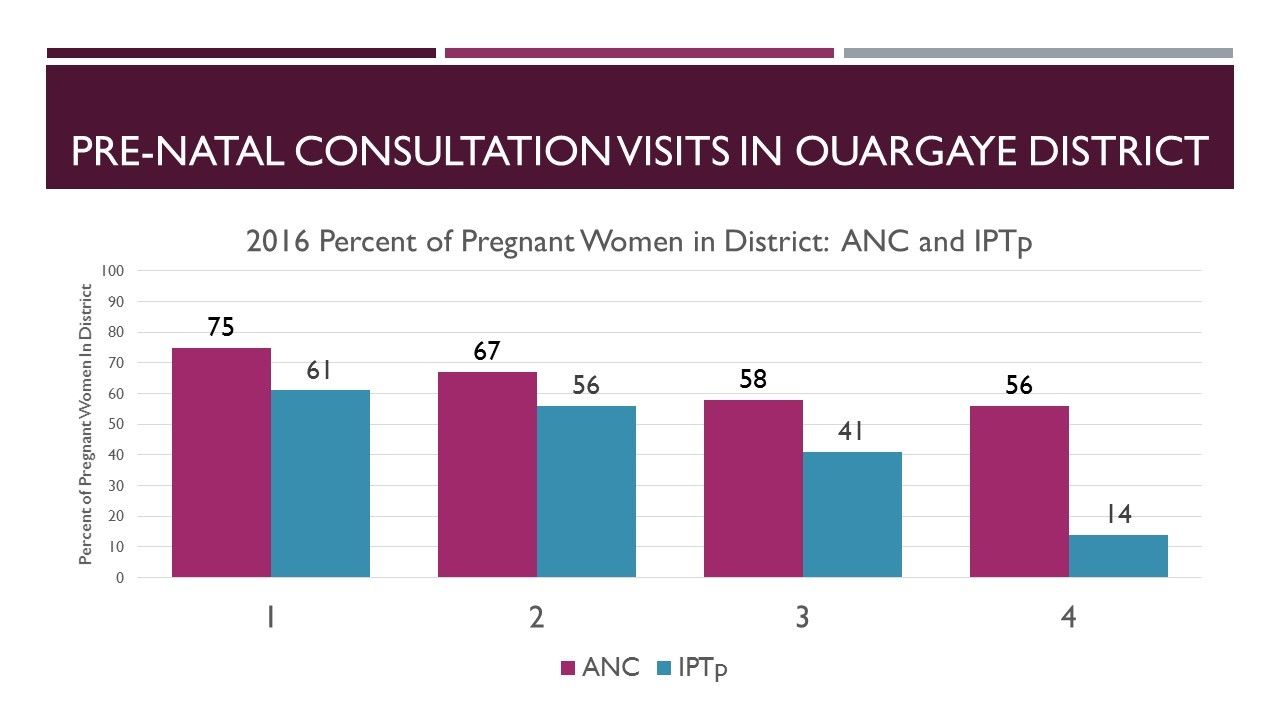
Among the approximately 20408 pregnant women in the District, 75% attended ANC once, 67% twice, 58% more than thrice and 56% four or more times. At present IPTp coverage is lower than ANC attendance: 61% received one dose, 56% got 2, 41% received 3, 14% got 4 and only 3% received 5 or more doses.
The pilot project intends to use CHWs mobilize more women to register for ANC and get their first IPTp dose. Then the CHWs, under supervision of the health center staff will deliver additional doses at the appropriate monthly interval.
More and more health interventions, including integrated community case management, are moving into the community. Universal health coverage requires that the health system meet people where they are – let the health system adapt to the clients, not the clients adjust to the convenience of health workers. With this approach the gap in ANC attendance and IPTp coverage will hopefully close, saving more women’s lives through prevention.
Advocacy &Elimination &Invest in Malaria Control &Universal Coverage Bill Brieger | 23 Apr 2017
Malaria Day 17 Years Later: Documenting and Investing to End Malaria
The first time the global community observed a day devoted to tackling the problem of malaria was April 25th 2001. This was agreed upon at the African Summit on Roll Back Malaria held in Abuja, Nigeria in 2000. The first seven annual observances were titled “Africa Malaria Day,” and recognized that the largest global burden of the disease affects people on the African continent. As thoughts moved toward elimination, the importance of addressing all endemic communities resulted in the first “World Malaria Day” in 2008.
 Thus on April 25th 2017 we are observing the 17th Malaria Day overall and the 10th anniversary of World Malaria Day. This observance has been complimented over the years with a malaria day for the Southern African Development Community and for countries in the Americas.
Thus on April 25th 2017 we are observing the 17th Malaria Day overall and the 10th anniversary of World Malaria Day. This observance has been complimented over the years with a malaria day for the Southern African Development Community and for countries in the Americas.
Each year Malaria Day has had a theme or themes to help focus education and advocacy. Regardless of the theme, the special day has been a time to mark progress and rally partners from the global to community level to continue the fight against the disease. The list below shows some of the issues/themes raised on the past Malaria Days. As noted, in some years advocacy efforts dealt with more than one key idea, though all are not presented.
- 2001 – Africa Malaria Day 2001: The First Africa Malaria Day; Malaria – A Crisis With Solutions; A Malaria Free-World
- 2002 – Mobilizing Communities to Roll Back Malaria
- 2003 – Insecticide Treated Nets and effective malaria treatment for pregnant
- women and young children
- 2004 – A Malaria-Free Future: Children for Children to Roll Back Malaria
- 2005 – Unite against malaria: Together we can beat malaria
- 2006 – Get Your ACT Together: Universal Access to Effective Malaria Treatment is a Human Right
- 2007 – Leadership and Partnership for Results
- 2008 – Malaria, A Disease without Borders
- 2009 – Counting Malaria Out
- 2010 – Counting Malaria Out; (and in the Africa Region) Communities engage to conquer malaria!
- 2011 – Achieving Progress and Impact
- 2012 – Sustain Gains. Save Lives. Invest in Malaria
- 2013-15 – Invest in the Future: Defeat Malaria
- 2016-17 – End Malaria for Good
 In sum these themes emphasize the importance of access to malaria interventions, documenting that access, using the data to stimulate more investment ultimately leading to an end (elimination) of malaria. The most recent World Malaria Report (2016) provides several important examples of the progress so far.
In sum these themes emphasize the importance of access to malaria interventions, documenting that access, using the data to stimulate more investment ultimately leading to an end (elimination) of malaria. The most recent World Malaria Report (2016) provides several important examples of the progress so far.
- Households with least one ITN increased to 79% in 2015
- 53% of the population at risk slept under an ITN in 2015 in Africa increasing from 30% in 2010
- The proportion of suspected malaria cases receiving a parasitological test in the public sector increased from 40% in the WHO African Region in 2010 to 76% in 2015
- In 2015, 31% of eligible pregnant women received three or more doses of intermittent preventive treatment in pregnancy (IPTp) among 20 countries with sufficient data, a major increase from 6% in 2010
In addition to noting progress, the report also points out gaps in appropriate care seeking for malaria, attendance at antenatal care clinics, and adequate numbers of nets for a household. As implied in the IPTp data, there is the additional problem of obtaining timely and accurate date to document progress and/or gaps. Looking at the Malaria Day themes around investing, we know that unless one can show investors results, it will be difficult to “End Malaria for Good.”
Climate &Environment &Mosquitoes &Zoonoses Bill Brieger | 22 Apr 2017
Earth Day, Climate, Environment and Malaria
![]() The Earth Day website notes that, “Our planet is currently losing over 15 billion trees each year—that’s 56 acres of forest every minute. We’re working hard to reverse that trend by supporting global reforestation projects. Earth Day Network’s Reforestation Campaign benefits local communities, increases habitat for species, and combats climate change.”
The Earth Day website notes that, “Our planet is currently losing over 15 billion trees each year—that’s 56 acres of forest every minute. We’re working hard to reverse that trend by supporting global reforestation projects. Earth Day Network’s Reforestation Campaign benefits local communities, increases habitat for species, and combats climate change.”
This habitat change if often conducive to the spread of malaria in areas and among populations that may not have been affected before. Specifically, “More risks associated with El Niño are: flooding and landslides in the Americas, drought in Southeast Asia and Australia, scrambled fisheries, and malaria, cholera, and dengue outbreaks.”
Terry Devitt reported that the incidence of malaria jumps when Amazon forests are cut, establishing a firm link between environmental change and human disease. The report, which combines detailed information on the incidence of malaria in 54 Brazilian health districts and high-resolution satellite imagery of the extent of logging in the Amazon forest, shows that clearing tropical forest landscapes boosts the incidence of malaria by nearly 50 percent (according to Olson and colleagues).
Moyes et al. Predicted the geographical distributions of the macaque hosts and mosquito vectors of Plasmodium knowlesi malaria in forested and non-forested areas of Southeast Asia. When urbanization and deforestation bring people into habitats they never lived in, zoonotic transmission of malaria results. Fornace et al. similarly observed that, “Marked spatial heterogeneity in P. knowlesi incidence was observed, and village-level numbers of P. knowlesi cases were positively associated with forest cover and historical forest loss in surrounding areas. These results suggest the likelihood that deforestation and associated environmental changes are key drivers in P. knowlesi transmission in these areas” of Malaysia.
Back to Brazil, de  Alvarenga and co-researchers reported in the transmission of Plasmodium simian malaria in the Brazilian Atlantic forest as a natural infection of capuchin monkeys (Cebinae subfamily). Because of human movement into forest areas, cases among people have now been documented.
Alvarenga and co-researchers reported in the transmission of Plasmodium simian malaria in the Brazilian Atlantic forest as a natural infection of capuchin monkeys (Cebinae subfamily). Because of human movement into forest areas, cases among people have now been documented.
The zoonotic transmission of malaria to humans due to changes in climate, environment and habitat pose another unwanted challenge to global efforts to eliminate malaria. On Earth Day it is imperative for malaria control and elimination workers to collaborate closely with colleagues in environmental health and protection.
Community &ITNs &Urban Bill Brieger | 19 Apr 2017
Challenges and Recommendations in Distribution of LLINs in Urban Contexts
by Brooke Farrenkopf

With the malaria team made up of public health nurses and an infectious disease specialist in Kumasi
I participated in a study on urban distribution of long lasting insecticide treated bednets (LLINs) as part of the USAID/PMI VectorWorks Project of the Johns Hopkins University Center for Communication Programs aided by a JHU Global Health Field Placement Scholarship. I conducted qualitative interviews to support a programmatic study on the challenges associated with mass distributions in urban contexts and helped develop report recommendations for developing the guidelines for future campaigns in urban areas. I am sharing my findings here.
As noted VectorWorks is funded by the US President’s Malaria Initiative and works to improve access to long-lasting insecticide treated nets (LLINs) in 12 countries in Asia and Africa. VectorWorks Ghana, through collaboration with the National Malaria Control Program (NMCP) and partners, supports the following distribution campaigns:
- School-based distribution, occurring every May for grades 2 and 6
- Continuous facility-based distribution at ANC and EPI visits
- Point mass distribution campaigns, occurring every 3 years
 In Kumasi, Takoradi, and Tamale, a point mass distribution campaign had already occurred. The campaign in Accra occurred while I was in Ghana, and I was able to visit the distribution sites and the health facilities where a portion of the LLINs were stored. Here, I was able to see some of the logistical challenges associated with the urban context.
In Kumasi, Takoradi, and Tamale, a point mass distribution campaign had already occurred. The campaign in Accra occurred while I was in Ghana, and I was able to visit the distribution sites and the health facilities where a portion of the LLINs were stored. Here, I was able to see some of the logistical challenges associated with the urban context.
I was also able to see the solutions put in place by the local malaria teams. One solution to improve program delivery was the development of a coupon coding system. As each community member attended the distribution site to receive a LLIN, Ghana Health Service (GHS) staff had to match their registration coupon with the coded coupon in the book. The coding system organized the coupons and identified members who had not attended distribution.
Mass distribution campaigns are the most effective method to rapidly increase long-lasting insecticidal net (LLIN) coverage. Mass distribution in urban areas with characteristically large and heterogeneous populations of high population density comes with higher costs and difficult logistics. Many inhabitants are not indigenous to the area and are of varied religious, occupational, and socioeconomic backgrounds. Urban areas commonly have large mobile working class populations that are difficult to access. These characteristics are unique to urban areas and introduces the need for improved guidelines in urban areas.

VectorWorks Ghana Team
To date, the National malaria Control Program (NMCP) guidelines for point mass distribution in Ghana have made no distinction between urban and rural areas and have therefore not addressed these differences. This study intended to provide information to refine these guidelines.
Most interviews were conducted in hospitals and health facilities where the members of the malaria teams were located. The interviews were conducted in-person in the four largest metropolitan areas in Ghana: Kumasi, Greater Accra, Takoradi, and Tamale. I helped develop and follow a question guide that covered each phase of the distribution focusing on the challenges, solutions, and recommendations associated with each phase of distribution.
Most common challenges with implementation in urban communities:
- Reaching community members during registration
- Completing registration within the period of days provided and the volunteers allocated, because the population was too dense to reach all of the households and many community members were not at home during registration
- Beneficiary dissatisfaction with universal health coverage definition of sufficient LLIN coverage {one net per two people in each household}
Most common recommendations for future distributions:
- Greater inclusion of sub-metro teams in development of the micro plan
- Increase the resources to recruit and remunerate more volunteers and supervisors to enable more distribution sites, help control crowds, and allow fewer days for each phase
- Intensify social mobilization and allow sub-metros to help develop this plan to utilize local resources, especially to improve understanding of universal health coverage definition of one net per two people and to inform about logistics
- Increase the number of registration days
- Conduct a utilization study to understand coverage of LLIN use and barriers to consistent use.
I was able to speak with public health nurses, malaria experts, and district health directors, and hear their insight on how to improve future campaigns. My favorite anecdotes included examples of how teams developed innovative solutions to improve campaign efficiency or strategically access hard to reach populations.
The observations and recommendations by the respondents themselves should guide future LLIN campaigns in urban settings in Ghana.
References
- VectorWorks (2017) Johns Hopkins center for Communication Programs. http://ccp.jhu.edu/projects/malaria-vector-control/
- de Beyl CZ, Koenker H, Acosta A, Onyefunafoa EO, Adegbe E, McCartney-Melstad A, Killian A (2016) Multi-country comparison of delivery strategues for mass campaigns to achieve universal coverage with insecticide-treated nets: what works best? Malaria Journal, 15(1): 1.
- Stakeholder Review of Experiences in urban Long-Lasting Insecticidal Net (LLIN) campaign distributions (2012). Malaria Consortium Africa.
CHW &Community Bill Brieger | 12 Apr 2017
Success Stories in Community Health in Africa
 The African Public Health Network of the Johns Hopkins Bloomberg School of Public Health held a panel discussion about community health successes in Africa on Monday 10th of April as the first in a series of events for the annual “Faces of Africa Week”.
The African Public Health Network of the Johns Hopkins Bloomberg School of Public Health held a panel discussion about community health successes in Africa on Monday 10th of April as the first in a series of events for the annual “Faces of Africa Week”.
Africa evokes different reactions to different people. For many, it’s the pictures of starving children, wars, poverty and disease that they find in various print and electronic media. But there has been a lot of achievement in Africa!
The Johns Hopkins Bloomberg School of Public Health – an institution that has invested a lot of time and resources in saving millions of lives at a time- has a huge footprint on the continent and other parts of the developing world through the work done and being done by experienced faculty members. Here is a summary of there thoughts as presented at Monday’s panel.
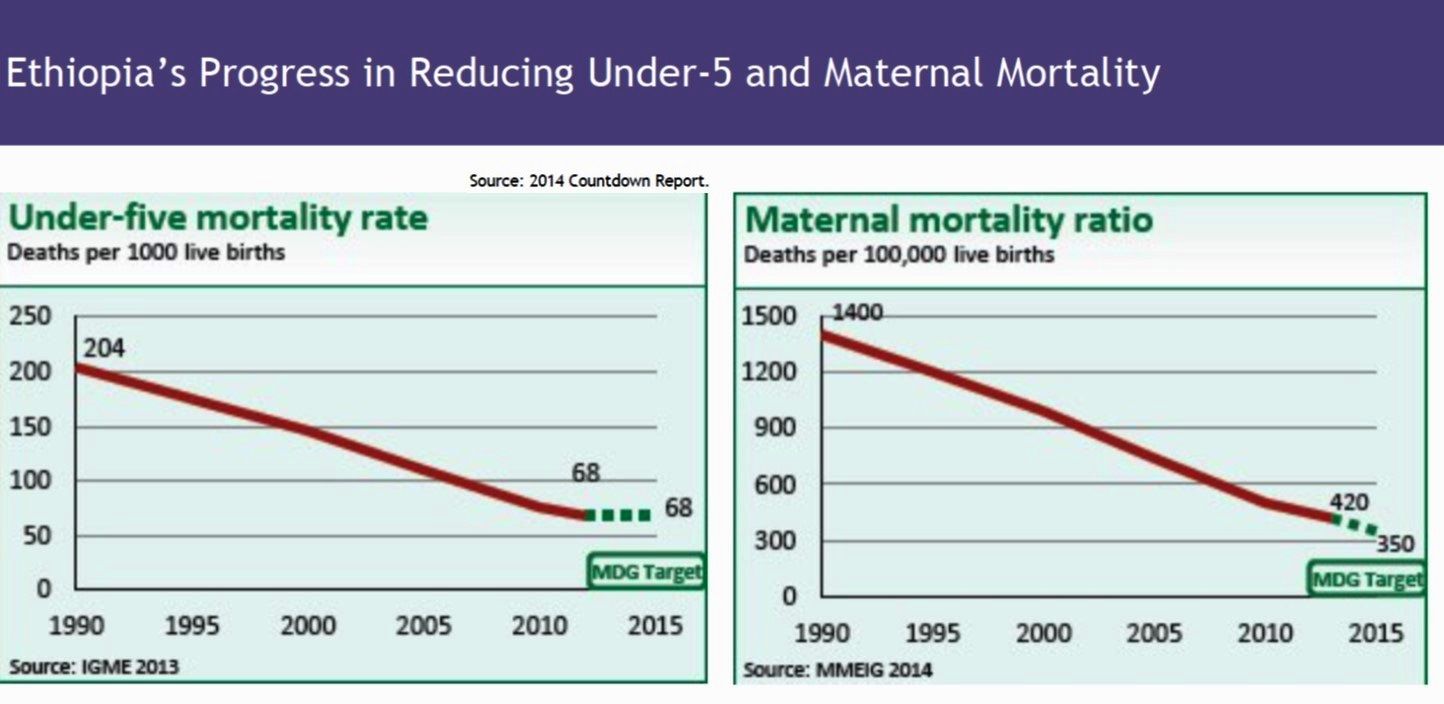 Dr. Henry Perry led the panel discussion on ‘The success stories in Public Health in Africa in the context of the role of Community Based Health Care’. He provided insights from the experiences of Rwanda and Ethiopia. He stressed the achievements of both countries in establishing and scaling up community health worker programs and in achieving Millennium Development Goals with reduced child mortality.
Dr. Henry Perry led the panel discussion on ‘The success stories in Public Health in Africa in the context of the role of Community Based Health Care’. He provided insights from the experiences of Rwanda and Ethiopia. He stressed the achievements of both countries in establishing and scaling up community health worker programs and in achieving Millennium Development Goals with reduced child mortality.
 Dr. William Brieger shared his experience from having lived and worked in Nigeria for over 27 years. He shared the progress in working with volunteer health workers and helping to shape community directed interventions. This history ranged from volunteer CHW programs by local NGOs, FBOs and universities in the 1970s to the development of a standardized set of CHW guidance and training materials by the Federal Ministry of Health in 2012. In the 1990s Nigeria took part in WHO’s African Program for Onchocerciasis Control and established a system of community directed treatment with ivermectin (CDTI) and community directed distributors to enable communities to take charge of annual ivermectin delivery. Then in the 2000s efforts build on the CDTI model to create the community directed intervention approach that included delivery of malaria
Dr. William Brieger shared his experience from having lived and worked in Nigeria for over 27 years. He shared the progress in working with volunteer health workers and helping to shape community directed interventions. This history ranged from volunteer CHW programs by local NGOs, FBOs and universities in the 1970s to the development of a standardized set of CHW guidance and training materials by the Federal Ministry of Health in 2012. In the 1990s Nigeria took part in WHO’s African Program for Onchocerciasis Control and established a system of community directed treatment with ivermectin (CDTI) and community directed distributors to enable communities to take charge of annual ivermectin delivery. Then in the 2000s efforts build on the CDTI model to create the community directed intervention approach that included delivery of malaria  services (ITNs, Case management and intermittent preventive treatment), vitamin A and DOTS for TB through community effort.
services (ITNs, Case management and intermittent preventive treatment), vitamin A and DOTS for TB through community effort.
Dr. Anbrasi Edward shared the Mozambique experience highlighting the Vurhonga projects and the impact of the care group model in improving maternal and child health. She described how the Care Group model was developed by an NGO that involved community volunteers providing education and services to small groups of community members. This model has spread throughout Africa.
 Mr. Bonny Musefano from the Embassy of The Republic of Rwanda provide perspectives on how Rwanda rebuilt its health system after the 1994 genocide ultimately leading to good community health. He stress the importance of Rwanda’s innovative system of community health insurance called Mutuelles de Santé. Very high coverage means that almost all Rwandans have access to health care. He also stressed the country’s interest in innovative technology and how drones are being used to deliver medical supplies to remote areas.
Mr. Bonny Musefano from the Embassy of The Republic of Rwanda provide perspectives on how Rwanda rebuilt its health system after the 1994 genocide ultimately leading to good community health. He stress the importance of Rwanda’s innovative system of community health insurance called Mutuelles de Santé. Very high coverage means that almost all Rwandans have access to health care. He also stressed the country’s interest in innovative technology and how drones are being used to deliver medical supplies to remote areas.
The APHN is grateful to members of the panel and to Prof. David Peters who helped fund the event via the Department of International Health.
For APHN: Joseph Uwazota, Jean Olivier Twahirwa Rwema, Zyleen Kassamali, Eve-Marie Benson, and Massah Massaquoi
Elimination &Surveillance &Vector Control Bill Brieger | 11 Apr 2017
A malaria elimination framework that includes high prevalence countries, too
When the Nigeria Malaria Control Program changes its name to Nigeria Malaria Elimination Program (NMEP) a few years ago, people wondered whether this was getting too far ahead of the situation in one of the highest burden malaria countries in the world. The recently released Framework for Malaria Elimination by the Global Malaria Program of WHO shows that all endemic countries can fit into the elimination process.

Recent Webinar by WHO’s Global Malaria Program stressed that all countries have a role in malaria elimination
The Framework stresses that, “Every country can accelerate progress towards elimination through evidence-based strategies, regardless of the current intensity of transmission and the malaria burden they may carry.” The Three pillars of the malaria elimination framework have room for high burden countries. Pillar 1 states that, “Ensure universal access to malaria prevention, diagnosis and treatment.”
First it is important to understand that the Framework defines malaria elimination as the cessation of indigenous mosquito-borne transmission of malaria throughout a country. The Framework also observes that even within countries there are diverse transmission areas. Some are not amenable to malaria transmission, while others may be amenable but do not experience transmission.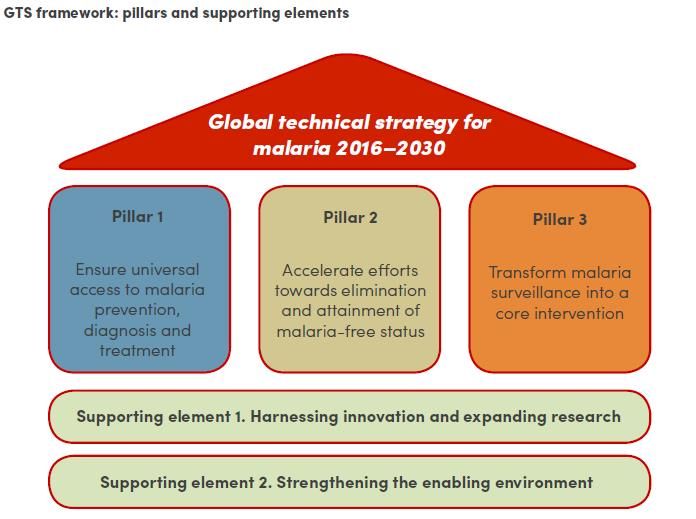
It is important to realize that malaria transmission in most countries is characterized by diversity and complexity. Areas where transmission is occurring range from very low transmission zones where hotspots erupt to high levels of ongoing transmission. Thus even high burden countries may have variation that require development of intervention packages tailored to the specific transmission setting.
This stratifi cation and development of appropriate intervention packages requires, “Excellent surveillance and response are the keys to achieving and maintaining malaria elimination; information systems must become increasingly ‘granular’ to allow identification, tracking, classification and response for all malaria cases (e.g. imported, introduced, indigenous).” This should lead to “subnational elimination targets as internal milestones.”
cation and development of appropriate intervention packages requires, “Excellent surveillance and response are the keys to achieving and maintaining malaria elimination; information systems must become increasingly ‘granular’ to allow identification, tracking, classification and response for all malaria cases (e.g. imported, introduced, indigenous).” This should lead to “subnational elimination targets as internal milestones.”
 For high burden countries key components of Pillar 1 is, “Vector control strategies, such as use of insecticide-treated mosquito nets (ITNs/LLINs) and indoor residual spraying (IRS), together with case management (prompt access to diagnosis and effective treatment) are critical for reducing malaria morbidity and mortality, and reducing malaria transmission.”
For high burden countries key components of Pillar 1 is, “Vector control strategies, such as use of insecticide-treated mosquito nets (ITNs/LLINs) and indoor residual spraying (IRS), together with case management (prompt access to diagnosis and effective treatment) are critical for reducing malaria morbidity and mortality, and reducing malaria transmission.”
Recommendations like ensuring political commitment, private sector involvement and establishment of an independent advisory committee are valuable at all stages of elimination. A challenge for high burden countries will be maintaining political commitment over many years. Early involvement of the private sector will boost coverage of major interventions. An independent advisory/monitoring group will help track data and progress.
It is important to put in place good monitoring systems to ensure that program coverage is well targeted, achieved and maintained. “Systematic tracking of programme actions over time, including budget allocations and adherence to standard operating procedures.” This enables accountability and enhances political commitment.
 Finally the Malaria Atlas Project has mapped most recent data, and as we can see Nigeria does have a variety of transmission settings. We know now that the decision of Nigeria’s malaria program to update its name was appropriate. Hopefully not only the NMEP but also the various state malaria programs will look at their malaria transmission strata and plan according toward elimination.
Finally the Malaria Atlas Project has mapped most recent data, and as we can see Nigeria does have a variety of transmission settings. We know now that the decision of Nigeria’s malaria program to update its name was appropriate. Hopefully not only the NMEP but also the various state malaria programs will look at their malaria transmission strata and plan according toward elimination.
CHW &Diagnosis &Health Workers &Performance &Training &Treatment Bill Brieger | 06 Apr 2017
World Health Workers Week, a Time to Recognize Health Worker Contributions to Malaria Care
 Since the beginning of the Roll Back malaria Partnership in 1998 there has been strong awareness that malaria control success is inextricably tied to the quality of health systems. Achieving coverage of malaria interventions involves all aspects of the health system but most particularly the human resources who plan, deliver and assess these services. World Health Worker Week is a good opportunity to recognize health worker contributions to ridding the world of malaria.
Since the beginning of the Roll Back malaria Partnership in 1998 there has been strong awareness that malaria control success is inextricably tied to the quality of health systems. Achieving coverage of malaria interventions involves all aspects of the health system but most particularly the human resources who plan, deliver and assess these services. World Health Worker Week is a good opportunity to recognize health worker contributions to ridding the world of malaria.
We can start with community health workers who may be informal but trained volunteers or front line formal health staff. According to the Frontline Health Workers Coalition, “Frontline health workers provide immunizations and treat common infections. They are on the frontlines of battling deadly diseases like Ebola and HIV/AIDS, and many families rely on them as trusted sources of information for preventing, treating and managing a variety of leading killers including diarrhea, pneumonia, malaria and tuberculosis.”
 The presence of CHWs exemplifies the ideal of a partnership between communities and the health system. With appropriate training and supervision CHWs ensure that malaria cases are diagnosed and treated promptly and appropriately, malaria prevention activities like long lasting insecticide-treated nets are implemented and pregnant women are protected from the dangers of the disease. CHWs save lives according to Nkonki and colleagues who “found evidence of cost-effectiveness of community health worker (CHW) interventions in reducing malaria and asthma, decreasing mortality of neonates and children, improving maternal health, increasing exclusive breastfeeding and improving malnutrition, and positively impacting physical health and psychomotor development amongst children.”
The presence of CHWs exemplifies the ideal of a partnership between communities and the health system. With appropriate training and supervision CHWs ensure that malaria cases are diagnosed and treated promptly and appropriately, malaria prevention activities like long lasting insecticide-treated nets are implemented and pregnant women are protected from the dangers of the disease. CHWs save lives according to Nkonki and colleagues who “found evidence of cost-effectiveness of community health worker (CHW) interventions in reducing malaria and asthma, decreasing mortality of neonates and children, improving maternal health, increasing exclusive breastfeeding and improving malnutrition, and positively impacting physical health and psychomotor development amongst children.”
 CHWs do not act in isolation but depend on health workers at the facility and district levels for training, supervision and maintenance of supplies and inventories. These health staff benefit from capacity building – when they are capable of performing malaria tasks, they can better help others learn and practice.
CHWs do not act in isolation but depend on health workers at the facility and district levels for training, supervision and maintenance of supplies and inventories. These health staff benefit from capacity building – when they are capable of performing malaria tasks, they can better help others learn and practice.
A good example of this capacity building is the Improving Malaria Care (IMC) project in Burkina Faso, implemented by Jhpiego and supported by USAID and the US President’s malaria Initiative. IMC builds capacity of health workers at facility and district level to improve malaria prevention service delivery and enhance accuracy in malaria diagnosis and treatment. Additionally capacity building is provided to health staff in the National Malaria Control Program to plan, design, manage and coordinate a comprehensive malaria control program. As a result of capacity building there has been a large increase in malaria cases diagnosed using parasitological techniques and in the number of women getting more doses of intermittent preventive treatment to prevent malaria during pregnancy.
Malaria care is much more than drugs, tests and nets. Health worker capacity is required to get the job done and move us forward on the pathway to eliminate malaria.
ITNs &Partnership &Private Sector &Vector Control Bill Brieger | 05 Apr 2017
The Business Case for Malaria Prevention: Employer Perceptions of Workplace LLIN Distribution in Southern Ghana
Kate Klein as part of her Master of Science in Public Health program in Social and Behavioral Interventions at the Johns Hopkins Bloomberg School of Public Health undertook a study of the potential for private sector involvement in malaria prevention in Ghana. She shares a summary of her work here. During her practicum in Ghana she was hosted by JHU’s Center for Communications Programs and its USAID supported VectorWorks Program. Her practicum she was also supported by the JHU Center for Global Health, and she presented her findings in a poster at the CGH’s Global Health Day on 30th March 2017. Her essay readers/advisers were Dr. Elli Leontsini (Department of International Health) and Kathryn Bertram (Center for Communication Programs).
Malaria is endemic in all parts of Ghana and significantly burdens families, communities, and economies. Malaria remains a leading cause of morbidity and mortality in Ghana; it accounts for eight percent of deaths in the country (The Global Fund, Ghana). It was also responsible for about 38% of outpatient visits, 27.3% of admissions in health facilities, and 48.5% of under-five deaths in 2015 (Nonvignon et al., 2016). In Ghana, the estimated cost of malaria to businesses in 2014 alone was estimated to be US$6.58 million, and 90% of these were direct costs (Nonvignon et al., 2016). Malaria leads to reduced productivity due to increased worker absenteeism and increased health care spending, which negatively impact business returns and tax revenue to the state (Nabyonga et al., 2011).
Although long-lasting insecticidal treated nets (LLINs) are a well-documented strategy to prevent disease in developing countries, most governments, including Ghana, lack the resources needed to comprehensively control malaria. The Global Fund (GF), USAID/President’s Malaria Initiative (PMI Ghana), and the United Kingdom Department for International Development (DfID Ghana) are the main donors for the national malaria control strategy and have worked primarily with the public sector (World Malaria Report, 2015). As government funding remains unable to close the funding gap for malaria, there is an increasing need to revitalize the private sector in sales and distribution of this life-saving technology.
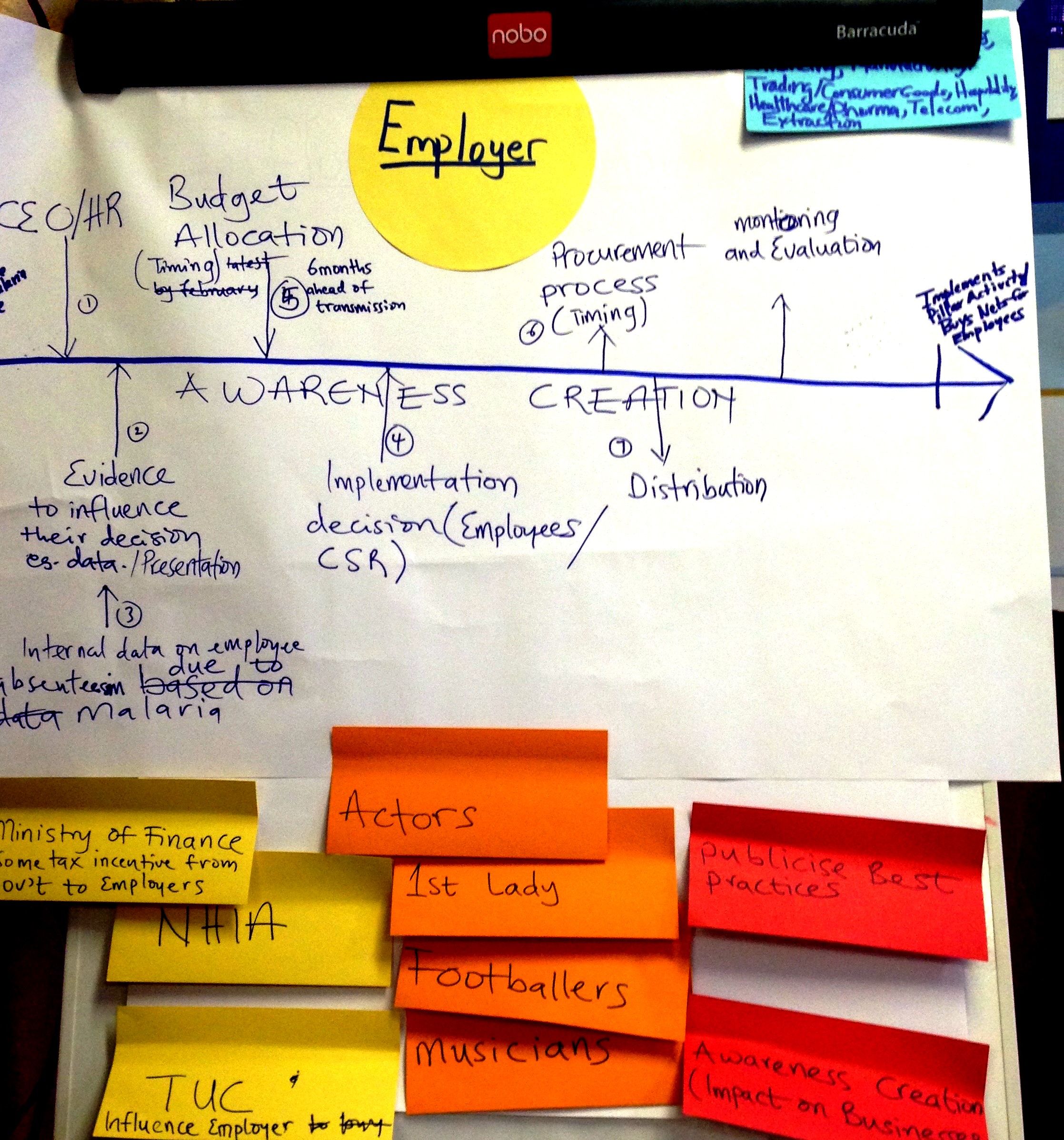
A “Journey mapping” exercise to consider the process of employers buying and distributing nets to employees, created during a PSMP advocacy workshop in December 2016
Ghana is looking to the private sector to encourage a departure from previous dependence on donor-funded free bed nets. The Private Sector Malaria Prevention (PSMP at JHU) project is being implemented in Southern Ghana to increase commercial sector distribution of LLINs. Three case studies served as a situation analysis and exemplified the potential for the PSMP: a rubber producing company, a mining company and a brewery.
All three had experience in malaria control and prevention but only one had specific experience with LLINs (which dovetailed well with its own corporate strengths in logistics management as exemplified by other bottling companies in Africa). Another supported the idea of adding LLINs to its existing indoor residual spraying and community health education efforts, but needed to consider how to develop the flexibility to engage in multiple malaria interventions.
The third had had the right climate and leadership to be able to partner with PSMP, but recently underwent a takeover by a large multinational brewing company and the resulting period of transition could potentially complicate their participation in LLIN distribution efforts from a budgetary standpoint. Generally these companies had the understanding of the potential benefits to the company of situating malaria control within their structure, and thus being early candidates for adoption of the PSMP.
 While the three case study companies recognized the business case for malaria, this was not a unanimous opinion among other five companies interviewed. Their concerns ranged from a preference toward treatment interventions to concerns expressed by employees about the difficulty of achieving high levels of net usage due to an array of complaints surrounding sleeping under LLINs. Some of these others had financial constraints.
While the three case study companies recognized the business case for malaria, this was not a unanimous opinion among other five companies interviewed. Their concerns ranged from a preference toward treatment interventions to concerns expressed by employees about the difficulty of achieving high levels of net usage due to an array of complaints surrounding sleeping under LLINs. Some of these others had financial constraints.
Through case studies and interviews PSMP was able to identify various challenges moving forward as well as areas where further clarity must be sought. PSMP learned that several companies are pouring their resources into strong treatment and case management programs, and one challenge will be determining how to push for preventative action, such as LLIN distribution, when treatment mechanisms are so established and bias exists.
For those companies who are making tremendous strides in malaria prevention, bringing recognition to these successes through advocacy will be necessary for encouraging future participation and convincing other similar employers of the benefits of starting their own LLIN distribution programs. Finally, PSMP needs to prioritize clarifying viewpoints on LLIN efficacy and use, with a focus on understanding why employers may hold unfavorable views and what it would take to overturn them.
In the future it will be necessary to move beyond the occupational considerations specific to mining and agro-industrial operations and consider how the work has changed the environment into a malaria habitat and the non-traditional work hours that may create more significant Anopheles mosquito exposures. PSMP should gather specific information on lifestyle, housing, and work environments during future visits with employers so that companies that have the most to gain through LLIN distribution are identified and targeted.