coronavirus &COVID-19 &Ebola &Elimination &iCCM &IPTi &IPTp &IRS &ITNs &Research Bill Brieger | 25 Apr 2020
Zero Malaria Starts after Lockdown?
 The novel 2019 coronavirus, also known as COVID-19 and SARS-COV2, is casting a heavy shadow over the 2020 World Malaria Day. People are trying to remain upbeat declaring the tagline “zero malaria starts with me,” but nothing can hide the fear that the current pandemic will both disrupt the current delivery of essential malaria preventive and treatment services, but will have longer term impacts on malaria funding and our capacity to learn new ways to reach malaria elimination goals. As we can see in the graphic to the right, accessible, lifesaving, community-based services may be especially hard hit.
The novel 2019 coronavirus, also known as COVID-19 and SARS-COV2, is casting a heavy shadow over the 2020 World Malaria Day. People are trying to remain upbeat declaring the tagline “zero malaria starts with me,” but nothing can hide the fear that the current pandemic will both disrupt the current delivery of essential malaria preventive and treatment services, but will have longer term impacts on malaria funding and our capacity to learn new ways to reach malaria elimination goals. As we can see in the graphic to the right, accessible, lifesaving, community-based services may be especially hard hit.
 Another ironic image is the indoor residual spray (IRS) team member with a face mask needed for protection from the insecticides being sprayed. When will such teams be able to go back into homes? When can household members actually pack out their belongings so that spraying can commence? When will such masks not be needed for intensive care COVID-19 case management instead?
Another ironic image is the indoor residual spray (IRS) team member with a face mask needed for protection from the insecticides being sprayed. When will such teams be able to go back into homes? When can household members actually pack out their belongings so that spraying can commence? When will such masks not be needed for intensive care COVID-19 case management instead?
WHO is urging “countries to move quickly to save lives from malaria in sub-Saharan Africa” because “New analysis supports the WHO call to minimize disruptions to malaria prevention and treatment services during the COVID-19 pandemic.” This will be difficult in high burden countries like Nigeria that are already on lockdown with over 1,000 coronavirus cases detected already. Modeling by WHO and partners has projected, “Severe disruptions to insecticide-treated net campaigns and in access to antimalarial medicines could lead to a doubling in the number of malaria deaths in sub-Saharan Africa this year compared to 2018.”
 The Global Malaria Program offers guidance for tailoring malaria interventions to the present circumstances. Great concern is drawn from previous epidemic situations when observing that, “it is essential that other killer diseases, such as malaria, are not ignored. We know from the recent Ebola outbreak in west Africa that a sudden increased demand on fragile health services can lead to substantial increases in morbidity and mortality from other diseases, including malaria. The COVID-19 pandemic could be devastating on its own – but this devastation will be substantially amplified if the response undermines the provision of life-saving services for other diseases.”
The Global Malaria Program offers guidance for tailoring malaria interventions to the present circumstances. Great concern is drawn from previous epidemic situations when observing that, “it is essential that other killer diseases, such as malaria, are not ignored. We know from the recent Ebola outbreak in west Africa that a sudden increased demand on fragile health services can lead to substantial increases in morbidity and mortality from other diseases, including malaria. The COVID-19 pandemic could be devastating on its own – but this devastation will be substantially amplified if the response undermines the provision of life-saving services for other diseases.”
Specifically, GMP recommends that national malaria programs should ensure the following:
- a focal point for malaria is a member of the National COVID-19 Incident Management Team.
- continued engagement with all relevant national COVID-19 stakeholders and partners.
- continued access to and use of recommended insecticide-treated mosquito nets (ITNs)
- continuation of planned targeted indoor residual spraying (IRS)
- early care-seeking for fever and suspected malaria by the general population to prevent a spike in severe malaria
- access to case management services in health facilities and communities with diagnostic confirmation through rapid diagnostic tests [RDTs]
- treatment of confirmed malaria cases with approved protocols
- continued delivery of planned preventive services normally provided to specific target populations (SMC, IPTi, IPTp)
- the safety of all malaria personnel and their clients in the process of carrying out the above interventions
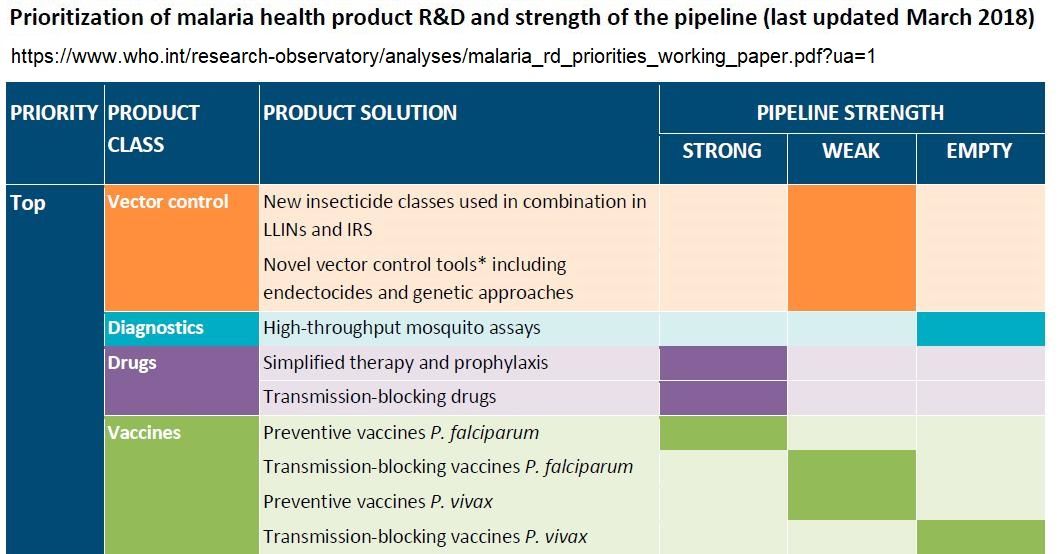 In editorial in the American Journal of Tropical Medicine and Hygiene by Yanow and Good address the damaging longer term impact of the present shutdown. “The impacts of research shutdowns will be felt long after the pandemic. Many scientists study diseases that do not share the same obvious urgency as COVID-19 and yet take a shocking toll on human life. For example, malaria infects more than 200 million people and takes the lives of nearly half a million people, mostly young children, each year.1 During laboratory closures and without clinical studies, there will be no progress toward treating and preventing malaria: no progress toward new drugs, vaccines, or diagnostics.”
In editorial in the American Journal of Tropical Medicine and Hygiene by Yanow and Good address the damaging longer term impact of the present shutdown. “The impacts of research shutdowns will be felt long after the pandemic. Many scientists study diseases that do not share the same obvious urgency as COVID-19 and yet take a shocking toll on human life. For example, malaria infects more than 200 million people and takes the lives of nearly half a million people, mostly young children, each year.1 During laboratory closures and without clinical studies, there will be no progress toward treating and preventing malaria: no progress toward new drugs, vaccines, or diagnostics.”
The case for continuing malaria services to save hundreds of thousands of lives is not difficult to make. The actual implementation during lockdowns and quarantines is a management challenge. The importance of malaria testing to provide patients with appropriate care for the right disease is crucial. The question is whether in resource strapped endemic countries these decisions and management arrangements can be made in a timely fashion and for the long term whether the next generation of research can proceed with much needed new medicines and technologies.
Case Management &CHW &Community &iCCM Bill Brieger | 29 Oct 2018
Performance of Community Health Workers in Providing Integrated Community Case Management (iCCM) Services in Eight Districts of Rwanda

During the first poster session at the 2018 Annual Meeting fo the American Society of Tropical Medicine and Hygiene, Noella Umulisa, Aline Uwimana, Cathy Mugeni, Beata Mukarugwiro, Stephen Mutwiwa, and Aimable Mbituyumuremyi of the Maternal and Child Survival Project (USAID)/Jhpiego and the Ministry of Health, Rwanda, presented findings from a review of community health workers in malaria case management. Their findings follow:
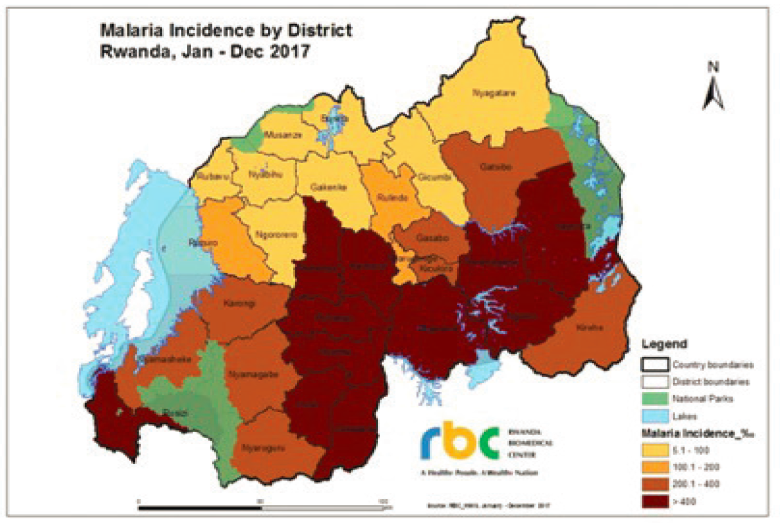 Rwanda has achieved near universal coverage of long-lasting insecticide nets, artemisinin-based combination therapy (ACT) and diagnosis, and targeted indoor residual spraying. Even so, there was an unprecedented increase in malaria cases from 2012-2017 despite optimal coverage of preventive and curative key interventions. The increase was caused by higher temperature, more rainfall, and increased resistance to insecticides.
Rwanda has achieved near universal coverage of long-lasting insecticide nets, artemisinin-based combination therapy (ACT) and diagnosis, and targeted indoor residual spraying. Even so, there was an unprecedented increase in malaria cases from 2012-2017 despite optimal coverage of preventive and curative key interventions. The increase was caused by higher temperature, more rainfall, and increased resistance to insecticides.
With more cases, the need for community case management (CCM) is crucial. Rwanda therefore trains, equips and supports community health providers to deliver high- impact treatment interventions and aims to supplement facility-based case management. Rwanda introduced integrated CCM 2008. Trained community health workers (CHWs) provide iCCM based on empirical diagnosis and treatment of pneumonia, diarrhea, and malaria. They also conduct malnutrition surveillance, comprehensive reporting and referral services.
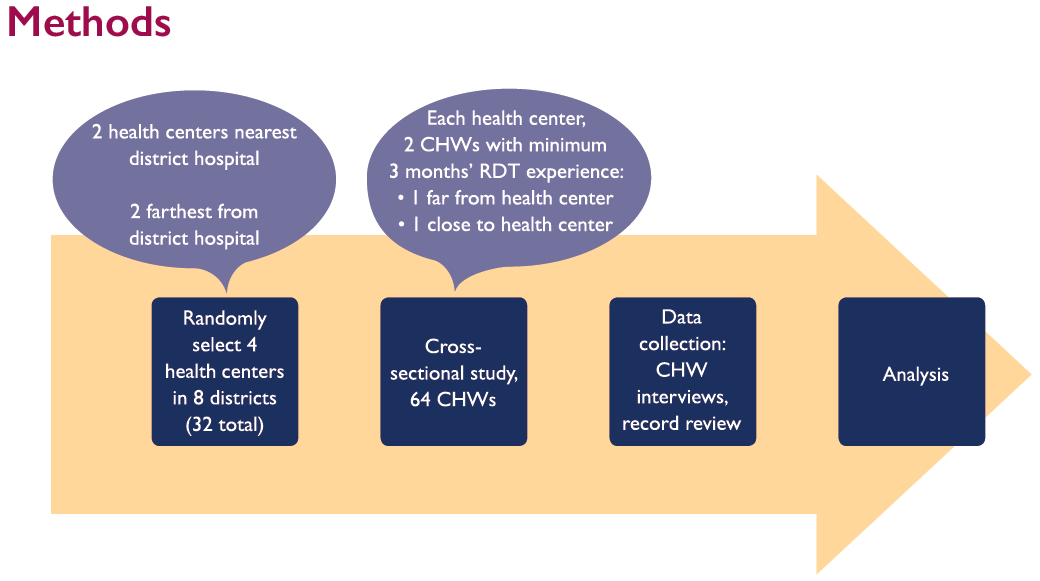 Given the changing status of malaria in the country, it was necessary to evaluate the performance of the CHWs. The evaluation aimed 1) to evaluate CHW performance in managing malaria, pneumonia and diarrhea in 8 districts of Rwanda based on national guidelines, and 2) to identify areas to reinforce and empower community health interventions. Using proximity (near/far) to hospitals and health centers, CHWs who had a minimum of 3 months experience using malaria rapid diagnostic tests (RDTs) were selected for interview. Slightly over half of CHWs were Males (56.2%). Most were over 40 years of age and nearly one-third were 50 years and older. Only 2% were between 25-29 years old.
Given the changing status of malaria in the country, it was necessary to evaluate the performance of the CHWs. The evaluation aimed 1) to evaluate CHW performance in managing malaria, pneumonia and diarrhea in 8 districts of Rwanda based on national guidelines, and 2) to identify areas to reinforce and empower community health interventions. Using proximity (near/far) to hospitals and health centers, CHWs who had a minimum of 3 months experience using malaria rapid diagnostic tests (RDTs) were selected for interview. Slightly over half of CHWs were Males (56.2%). Most were over 40 years of age and nearly one-third were 50 years and older. Only 2% were between 25-29 years old.
 Based on National Guidelines, CHWs were judged to have provided “adequate” treatment more frequently than “correct” treatment. Overall, 90% of cases were adequately treated; only 70% correctly treated. Among the three main conditions, malaria was most often adequately and correctly treated. Incorrect treatment was due to lack of adherence to guidelines. For malaria incorrect treatment often meant using the wrong does for age packet for treatment when the correct packet was not in stock.
Based on National Guidelines, CHWs were judged to have provided “adequate” treatment more frequently than “correct” treatment. Overall, 90% of cases were adequately treated; only 70% correctly treated. Among the three main conditions, malaria was most often adequately and correctly treated. Incorrect treatment was due to lack of adherence to guidelines. For malaria incorrect treatment often meant using the wrong does for age packet for treatment when the correct packet was not in stock.
 In conclusion, CHWs correctly treat 70% of children for all IMCI pathologies according to national guidelines. Malaria was the most seen/treated pathology; cases increased during study period. Overall, cases more often treated adequately than correctly. CHWs use complex tools thus lack adequate time to follow all steps correctly when providing services.
In conclusion, CHWs correctly treat 70% of children for all IMCI pathologies according to national guidelines. Malaria was the most seen/treated pathology; cases increased during study period. Overall, cases more often treated adequately than correctly. CHWs use complex tools thus lack adequate time to follow all steps correctly when providing services.
The study team recommends the need to strengthen iCCM commodities supply chain, especially at community level through supervision and mentorship conducted at health centers, district hospitals and central level. Also it is necessary to revise and simplify iCCM tools used by CHWs to decrease burden and improve quality of services.
 This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Advocacy &Case Management &Children &CHW &Community &Elimination &Funding &iCCM &Invest in Malaria Control &IPTp &ITNs Bill Brieger | 25 Apr 2018
On World Malaria Day the realities of resurgence should energize the call to ‘Beat Malaria’
 Dr Pedro Alonso who directed the World Health Organization’s Global Malaria Program, has had several opportunities in the past two weeks to remind the global community that complacency on malaria control and elimination must not take hold as there are still over 400,000 deaths globally from malaria each year. At the Seventh Multilateral Initiative for Malaria Conference (MIM) in Dakar, Dr Alonso drew attention to the challenges revealed in the most recent World Malaria Report (WMR). While there have been decreases in deaths, there are places where the number of actual cases is increasing.
Dr Pedro Alonso who directed the World Health Organization’s Global Malaria Program, has had several opportunities in the past two weeks to remind the global community that complacency on malaria control and elimination must not take hold as there are still over 400,000 deaths globally from malaria each year. At the Seventh Multilateral Initiative for Malaria Conference (MIM) in Dakar, Dr Alonso drew attention to the challenges revealed in the most recent World Malaria Report (WMR). While there have been decreases in deaths, there are places where the number of actual cases is increasing.
 Around twenty years ago the course of malaria changed with the holding of the first MIM, also in Dakar and the establishment of the Roll Bank Malaria (RBM) Partnership. These were followed in short order by the Abuja Declaration that set targets for 2010 and embodied political in endemic countries, as well as major funding mechanisms such as the Global Fund to fight AIDS, TB and Malaria. This spurred what has been termed a ‘Golden Decade’ of increasing investment and intervention coverage, leading to decreasing malaria morbidity and mortality. The Millennium Development Goals provided additional impetus to reduce the toll of malaria by 2015.
Around twenty years ago the course of malaria changed with the holding of the first MIM, also in Dakar and the establishment of the Roll Bank Malaria (RBM) Partnership. These were followed in short order by the Abuja Declaration that set targets for 2010 and embodied political in endemic countries, as well as major funding mechanisms such as the Global Fund to fight AIDS, TB and Malaria. This spurred what has been termed a ‘Golden Decade’ of increasing investment and intervention coverage, leading to decreasing malaria morbidity and mortality. The Millennium Development Goals provided additional impetus to reduce the toll of malaria by 2015.
 On Facebook Live yesterday Dr Alonso talked about that ‘Golden Decade.’ There was a 60% decrease in mortality and a 40% decreases in malaria cases. But progress slowing down and we may be stalled at a crossroads. He noted that history show unless accelerate efforts, malaria will come back with a vengeance. Not only is renewed political leadership and funding, particularly from affected countries needed, but we also need new tools. Dr Alonso explained that the existing tools allowed 7m deaths be diverted in that golden decade, but these tools are not perfect. We are reaching limits on these tools such that we need R&D for tools to enable quantum leap forward. Even old tools like nets are threatened by insecticide resistance, and research on alternative safe insecticides is crucial.
On Facebook Live yesterday Dr Alonso talked about that ‘Golden Decade.’ There was a 60% decrease in mortality and a 40% decreases in malaria cases. But progress slowing down and we may be stalled at a crossroads. He noted that history show unless accelerate efforts, malaria will come back with a vengeance. Not only is renewed political leadership and funding, particularly from affected countries needed, but we also need new tools. Dr Alonso explained that the existing tools allowed 7m deaths be diverted in that golden decade, but these tools are not perfect. We are reaching limits on these tools such that we need R&D for tools to enable quantum leap forward. Even old tools like nets are threatened by insecticide resistance, and research on alternative safe insecticides is crucial.
 Dr Alonso at MIM pointed to the worrying fact that investment in malaria overall peaked in 2013. Investment by endemic countries themselves has remained stable throughout and never gone reached $1 billion despite advocacy and leadership groups like the Africa Leaders Malaria Alliance. The 2017 WMR shows that while 16 countries achieved a greater that 20% reduction in malaria cases, 25 saw a greater that 20% increase in cases. The outnumbering of decreasing countries by increasing was 4 to 8 in Africa, the region with the highest burden of the disease. Overall 24 African countries saw increases in cases between 2015 and 2016 versus 5 that saw a decrease. A review of the Demographic and Health and the Malaria Information Surveys in recent years show that most countries continue to have difficulty coming close to the Abuja 2010 targets for Insecticide treated net (ITN) use, prompt and appropriate malaria case management and intermittent preventive treatment of malaria in pregnancy (IPTp).
Dr Alonso at MIM pointed to the worrying fact that investment in malaria overall peaked in 2013. Investment by endemic countries themselves has remained stable throughout and never gone reached $1 billion despite advocacy and leadership groups like the Africa Leaders Malaria Alliance. The 2017 WMR shows that while 16 countries achieved a greater that 20% reduction in malaria cases, 25 saw a greater that 20% increase in cases. The outnumbering of decreasing countries by increasing was 4 to 8 in Africa, the region with the highest burden of the disease. Overall 24 African countries saw increases in cases between 2015 and 2016 versus 5 that saw a decrease. A review of the Demographic and Health and the Malaria Information Surveys in recent years show that most countries continue to have difficulty coming close to the Abuja 2010 targets for Insecticide treated net (ITN) use, prompt and appropriate malaria case management and intermittent preventive treatment of malaria in pregnancy (IPTp).
 The coverage gap is real. The WMR shows that while there have been small but steady increase in 3 doses of IPTp, coverage of the first dose has leveled off. Also while ownership of a net by households has increased, less than half of households have at least one net for every two residents.
The coverage gap is real. The WMR shows that while there have been small but steady increase in 3 doses of IPTp, coverage of the first dose has leveled off. Also while ownership of a net by households has increased, less than half of households have at least one net for every two residents.
In contrast a new form of IPT – seasonal malaria chemoprevention (SMC) for children in the Sahel countries has taken off with over 90% of children receiving at least one of the monthly doses during the high transmission season. Community case management is taking off as is increased use of rapid diagnostic testing. Increased access to care may explain how in spite of increased cases, deaths can be reduced. This situation could change rapidly if drug resistance spreads.
 While some international partners are stepping up, we are far short of the investment needed. The Gates Foundation is pledging more for research and development to address the need for new tools as mentioned by Dr Alonso. A big challenge is adequate funding to sustain the implementation of both existing tools and the new ones when they come online. Even in the context of a malaria elimination framework, WHO stresses the need to maintain appropriate levels of intervention with case management, ITNs and other measures regardless of the stage of elimination at which a country or sub-strata of a country is focused.
While some international partners are stepping up, we are far short of the investment needed. The Gates Foundation is pledging more for research and development to address the need for new tools as mentioned by Dr Alonso. A big challenge is adequate funding to sustain the implementation of both existing tools and the new ones when they come online. Even in the context of a malaria elimination framework, WHO stresses the need to maintain appropriate levels of intervention with case management, ITNs and other measures regardless of the stage of elimination at which a country or sub-strata of a country is focused.
Twenty years after the formation of RBM and 70 years after the foundation of WHO, the children, families and communities of endemic countries are certainly ready to beat malaria. The question is whether the national and global partners are equally ready.
CHW &Diagnosis &iCCM &Treatment Bill Brieger | 14 Nov 2016
A Pilot to Use Malaria RDTs at the Community Level in Burkina Faso
A poster entitled “The Improving Malaria Care (IMC) Project’s Contribution to follow up a Pilot to Use Rapid Diagnostic Tests (RDTs) at the Community Level in Burkina Faso” was presented by members of Jhpiego’s Burkina Faso Team: Ousmane Badolo, Stanislas P. Nebie, Moumouni Bonkoungou, Mathurin Dodo, Rachel Waxman, Danielle Burke, William Brieger at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
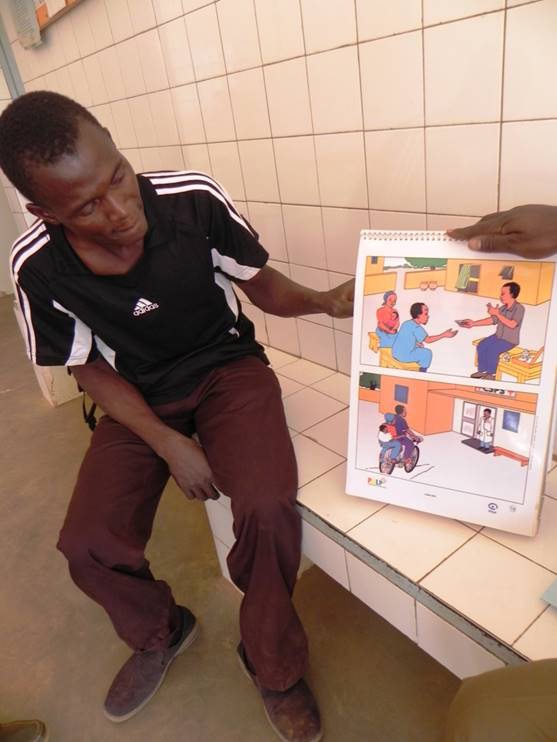
CHWs provide malaria testing, treatment and health education
Early and correct case management of malaria in health facilities and at the community level is among the priorities of Burkina Faso’s National Malaria Control Program (NMCP). In line with this initiative, the NMCP piloted use of Rapid Diagnostic Tests (RDTs) by Community Health Workers (CHWs) to confirm malaria cases in the three health districts of Kaya, Saponé and Nouna between 2013 and 2015. With PMI support, follow-up visits were organized to document best practices, as well as challenges, on RDT use by CHWs that could serve as lessons learned for scale-up.
During follow-up visits, malaria commodities management (supply, storage and use) at the community level was examined, use of RDTs was assessed, and implementation at the community 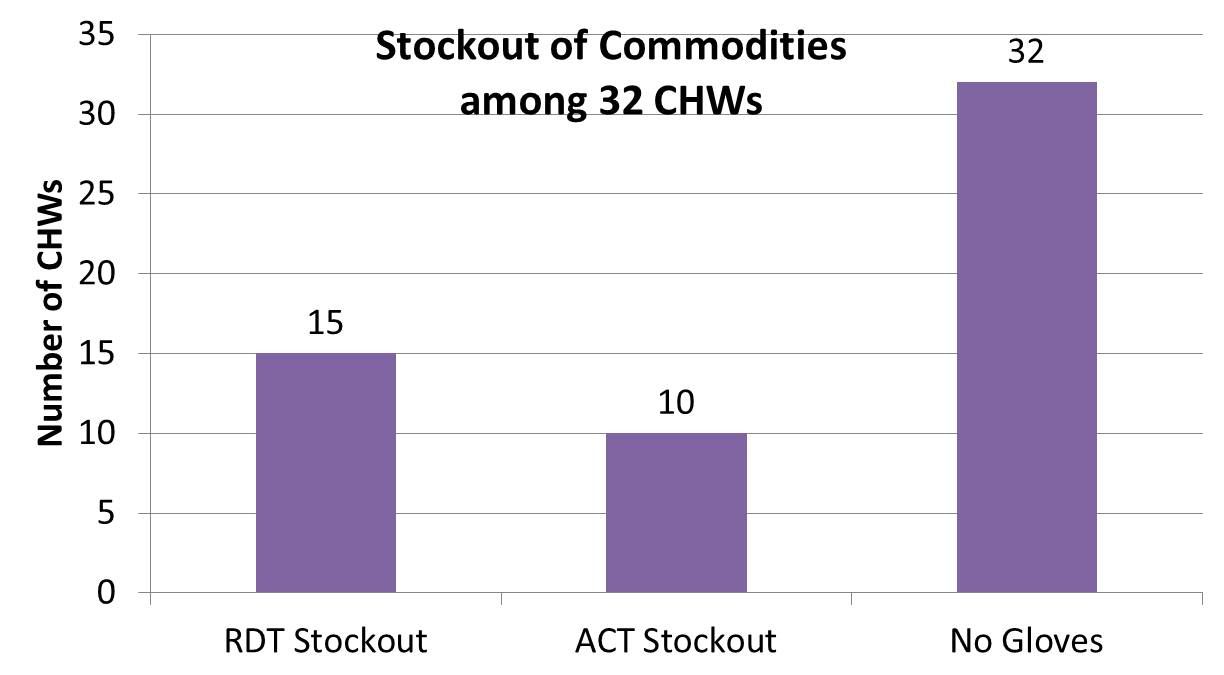 level was discussed with all actors at regional, district, health facilities, and community levels. The team examined the monitoring/supervision processes at all levels, used a check list on malaria commodities management, and employed a questionnaire for each type of actor. Both qualitative and quantitative data have been collected. A total of 108 persons were contacted including 32 CHWs, 42 community leaders and 34 health care providers and managers.
level was discussed with all actors at regional, district, health facilities, and community levels. The team examined the monitoring/supervision processes at all levels, used a check list on malaria commodities management, and employed a questionnaire for each type of actor. Both qualitative and quantitative data have been collected. A total of 108 persons were contacted including 32 CHWs, 42 community leaders and 34 health care providers and managers.
 Findings revealed frequent stock-outs of RDTs and artemisinin-based combination therapies, non-payment of stipends to CHWs (a demotivator) and insufficient supervision of CHW by health teams. From the community perspective, 66% of community leaders were satisfied with their CHW’s work (diagnosis and treatment of uncomplicated malaria
Findings revealed frequent stock-outs of RDTs and artemisinin-based combination therapies, non-payment of stipends to CHWs (a demotivator) and insufficient supervision of CHW by health teams. From the community perspective, 66% of community leaders were satisfied with their CHW’s work (diagnosis and treatment of uncomplicated malaria  and referral of severe cases to health facilities). However, 46% of community leaders complained of frequent stock-outs and unanimously agreed on the importance of regular payment of premiums to CHW.
and referral of severe cases to health facilities). However, 46% of community leaders complained of frequent stock-outs and unanimously agreed on the importance of regular payment of premiums to CHW.
Follow up of the pilot was valuable in obtaining community, CHW and health worker perspectives for improving the program. While the community finds the program acceptable, its sustainability will require that solutions be found for stock-outs, non-payment, and insufficient supervision before scale up takes place.
CHW &Diagnosis &iCCM Bill Brieger | 30 Oct 2016
Community health workers provide integrated community case management using malaria rapid diagnostic test kits
Please find below the abstract of the above named article that is first appearing as an accepted paper in the journal Research in Social and Administrative Pharmacy. The authors – Bright C. Orji, Namratha Rao, Elizabeth Thompson, William R. Brieger, Emmanuel
‘Dipo Otolorin – conducted this work as part of Jhpiego’s commitment to fighting malaria in Nigeria.
ABSTRACT
Background: Throughout Nigeria malaria is an endemic disease. Efforts to treat malaria can also be combined with other illnesses including pneumonia and diarrhea, which are killing children under five years of age. The use of Rapid Diagnostic Test (RDT) aids early diagnosis of malaria and informs when other illnesses should be considered. Those with positive RDT results should be treated with Artemisinin-based Combination Therapy (ACTs), while those with negative RDTs results are further investigated for pneumonia and diarrhea.

Community Directed Distributor performs malaria rapid diagnostic test of febrile child
Critical health systems challenges such as human resource constraints mean that community case management (CCM) and community health workers such as volunteers called Community Directed Distributors (CDDs) can therefore play an important role in diagnosing and treating malaria. This report described an effort to monitor and document the performance of trained CDDs in providing quality management of febrile illnesses including the use of RDTs.
Method: The program trained one hundred and fifty-two (152) CDDs on the use of RDTs to test for malaria and give ACTs for positive RDTs results, cotrimoxazole for the treatment of pneumonia and Oral rehydration solution and zinc for diarrhea They were also taught to counsel on compliance medicine, identify adverse reactions, and keep accurate records. The CDDs worked for 12 Calendar months. Their registers were retrieved and audited using a checklist to document client complaints, tests done, test results and treatment provided. No client identifying information was collected.
Results: There were 32 (21%) male CDDs and 120 (79%) females. The overall mean age of the CDDs was 36.8 (±8.7) years old. 89% of the male CDDs provided correct treatment based on RDT results compared to 97.6% of the female CDDs, a statistically significant difference. Likewise CDDs younger than 36 years of age provided 92.7% correct case management compared to those 36 years and older (98.4%). The difference between the age groups was also significant. There was a strong association between CDDs dispensing ACTs with positive RDT results. In RDT negative cases, the most common course of action was dispensing antibiotics (43.2%), followed by referring the patients (30.34%) and the providing ORS (24.1%).
Conclusion: Volunteer CDDs who are community members can adhere to treatment protocols and guidelines and comply with performance standards. The next step is scaling this approach to a state-wide level.
Accepted Date: 26 September 2016. Please cite this article as: Orji BC, Rao N, Thompson E, Brieger WR, ‘Dipo Otolorin E, Community health workers provide integrated community case management using malaria rapid diagnostic test kits, Research in Social & Administrative Pharmacy (2016), doi: 10.1016/j.sapharm.2016.09.006.
Case Management &Community &Diagnosis &Drug Development &iCCM &Vaccine Bill Brieger | 12 Nov 2015
Pneumonia and Malaria – similar challenges and pathways to success
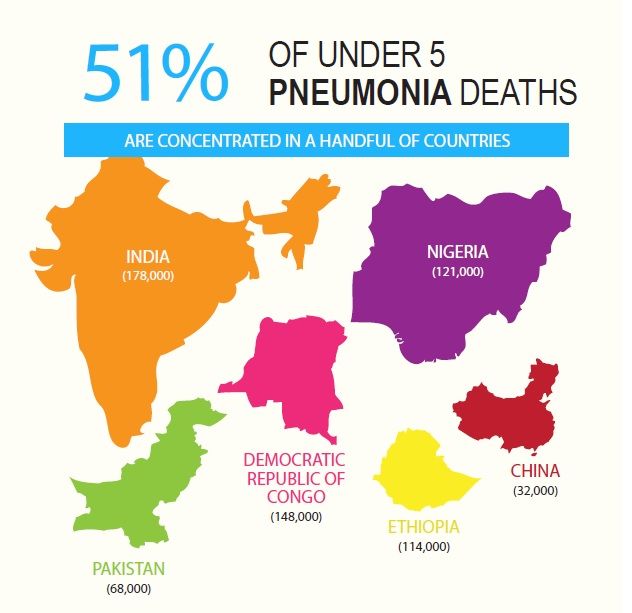 World Pneumonia Day (WPD) helps us focus on the major killers of children globally. While Pneumonia is responsible for more child mortality across the world, in tropical malaria endemic areas both create nearly equal damage (see WPD graphic showing Nigeria and DRC which are both have the highest burden for pneumonia, but also malaria). Of particular concern is case management at the clinic and community level where there is great need to differentiate between these two forms of febrile illness so that the right care is given and lives are saved.
World Pneumonia Day (WPD) helps us focus on the major killers of children globally. While Pneumonia is responsible for more child mortality across the world, in tropical malaria endemic areas both create nearly equal damage (see WPD graphic showing Nigeria and DRC which are both have the highest burden for pneumonia, but also malaria). Of particular concern is case management at the clinic and community level where there is great need to differentiate between these two forms of febrile illness so that the right care is given and lives are saved.
![]() Diagnostics are a particular challenge. While we now have malaria rapid diagnostic test kits that can be used at the community level, we must rely on breath counting for malaria. The Pneumonia Diagnostics Project (see video) “is working to identify the most accurate and acceptable devices for use by frontline health workers in remote settings in Cambodia, Ethiopia, South Sudan and Uganda.”
Diagnostics are a particular challenge. While we now have malaria rapid diagnostic test kits that can be used at the community level, we must rely on breath counting for malaria. The Pneumonia Diagnostics Project (see video) “is working to identify the most accurate and acceptable devices for use by frontline health workers in remote settings in Cambodia, Ethiopia, South Sudan and Uganda.”
Ease of use at low cost must be achieved. One approach to solve the pneumonia diagnostics challenge at community and front line clinic level is to find “mobile phone applications or alternative energy for pulse oximetry,” to test low oxygen levels.
 Vaccine development for both diseases is underway. The challenge for malaria results from the different stages of the parasites life-cycle. Lack of affordable vaccines for pneumonia limits at present widespread preventive action, though public-private partnerships offer hope.
Vaccine development for both diseases is underway. The challenge for malaria results from the different stages of the parasites life-cycle. Lack of affordable vaccines for pneumonia limits at present widespread preventive action, though public-private partnerships offer hope.
Dispersable and correct dose for age prepackaged malaria drugs are already available. Now more child-friendly medicines for pneumonia are being developed. In low resource settings, “amoxicillin dispersible tablets are a better option, particularly for children who can’t swallow pills. They have a longer shelf-life, are cost-effective, don’t need refrigeration, and are easy to administer.”
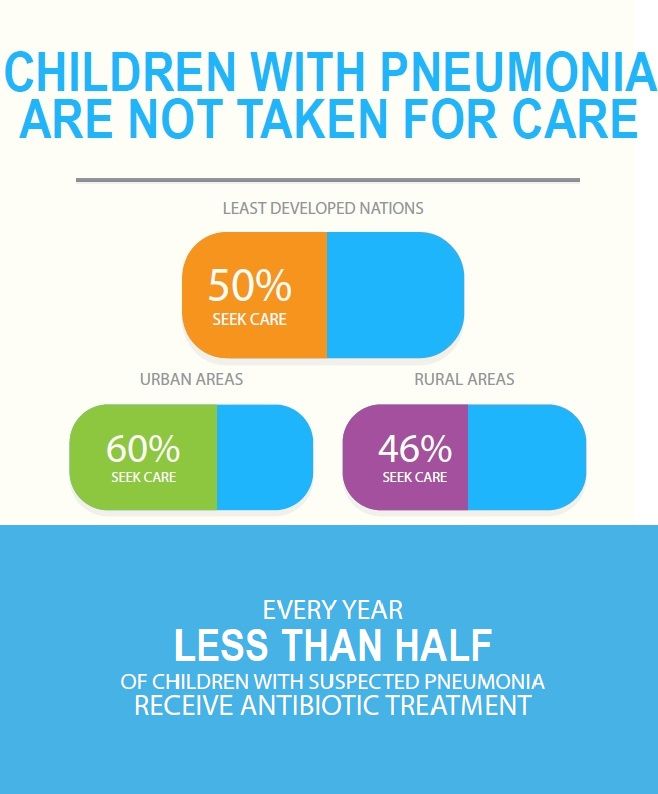
Similarities in the problems and solutions to control these two diseases require that interventions must continue to be developed and implemented jointly in order to benefit children the most. As can be seen again from the WPD graphics (right), many children do not get needed treatment. Integrated case management at all levels is the answer.
CHW &iCCM Bill Brieger | 28 Oct 2015
Use of community health volunteers to increase coverage for integrated community case management in Bondo, Kenya
Colleagues[1] from John Snow, Inc. and Jhpiego are presenting presenting a poster at the American Society of Tropical Medicine 64th Annual Meeting Wednesday 28 October 2015. Visit Poster 1330. Below is a summary of their findings.
 Bondo County is located in the Western region of Kenya. It has an IMR of 110 and an U5MR of 208 per 1,000 live births which is thrice the national U5MR of 74/1000. There continues to be limited access to and use of health services in some rural areas that are underserved by health facilities. This provided the impetus for advocating for the implementation of integrated Community Case Management (iCCM) as a way to address these health disparities.
Bondo County is located in the Western region of Kenya. It has an IMR of 110 and an U5MR of 208 per 1,000 live births which is thrice the national U5MR of 74/1000. There continues to be limited access to and use of health services in some rural areas that are underserved by health facilities. This provided the impetus for advocating for the implementation of integrated Community Case Management (iCCM) as a way to address these health disparities.
An 18-month study is underway in Bondo to test whether community health volunteers (CHVs) can effectively deliver an iCCM package in the context of the existing community health strategy platform. The study is a quasi-experimental design with intervention and comparison groups of four community units each. Fifty-eight intervention group CHVs were trained on iCCM and health promotion, provided with iCCM commodities, and a monthly stipend of $23.
 In the comparison group CHVs were only trained in health promotion and receive a similar stipend. Baseline survey was done in October 2013 and midline in July 2014; the latter was limited to the intervention group only.
In the comparison group CHVs were only trained in health promotion and receive a similar stipend. Baseline survey was done in October 2013 and midline in July 2014; the latter was limited to the intervention group only.
An endline survey is planned for June 2015. Overall introduction of iCCM resulted in over 100% increase in iCCM cases managed from baseline compared to midline (2,367 vs. 4,868), with the CHVs’ share being 56%.
In terms of performance, the CHVs demonstrated good ability to follow the iCCM algorithm from the identification of signs to the classification of illness, and deciding whether to treat at home or refer to the health facility. The greatest improvement was in the ability to examine or “look” for signs of illness (average of 3% at baseline vs. 74% at midline), p <0.05.
Key stakeholders reported that there were various benefits of iCCM in Bondo such as improved access to health services, improved health behaviors at individual and community level, community empowerment, and increased trust of the CHVs by the community. Based on these results so far, CHVs can effectively provide iCCM services and thus contribute to reducing childhood morbidity deaths in Bondo, Kenya
[1] Savitha Subramanian, Mark Kabue, Dyness Kasungami, Makeba Shiroya-Wadambwa, Dan James Otieno, Charles Waka
Community &iCCM &Procurement Supply Management &Treatment Bill Brieger | 06 Aug 2015
RSAP Themed Issue on Pharmaceutical Logistics for integrated Community Case Management (iCCM) – Call for Papers
 A themed issue for Research in Social and Administrative Pharmacy (RSAP at http://www.journals.elsevier.com/research-in-social-and-administrative-pharmacy/) will feature the challenges of guaranteeing regular and adequate pharmaceutical supplies and commodities for integrated Community Case Management (iCCM). iCCM can be described as a comprehensive approach to providing essential health services in and by the community. iCCM relies on having basic commodities like Rapid Diagnostic Tests (RDTs) and artemisinin-based combination therapy (ACT) medicines for malaria, oral rehydration solution (ORS) packets and zinc for diarrhea, in addition to appropriate antibiotics like amoxicillin and cotrimoxazole for pneumonia available in the community.
A themed issue for Research in Social and Administrative Pharmacy (RSAP at http://www.journals.elsevier.com/research-in-social-and-administrative-pharmacy/) will feature the challenges of guaranteeing regular and adequate pharmaceutical supplies and commodities for integrated Community Case Management (iCCM). iCCM can be described as a comprehensive approach to providing essential health services in and by the community. iCCM relies on having basic commodities like Rapid Diagnostic Tests (RDTs) and artemisinin-based combination therapy (ACT) medicines for malaria, oral rehydration solution (ORS) packets and zinc for diarrhea, in addition to appropriate antibiotics like amoxicillin and cotrimoxazole for pneumonia available in the community.
Early successes describing the documentation of need and initial procurement of these essential therapies in developing nations have been published; however, this themed issue will share original research, models, and expert commentaries on ensuing stages in procurement and supply chain management (PSM) that will sustain iCCM.
PSM/logistical success for iCCM can occur in countries that have a department or unit that focuses on community health promotion and supports standardized training and equipping of Community Health Workers (CHWs) even in small villages. Unfortunately, most programs lack adequate procurement and supply management systems, especially planning and forecasting. Front-line health center staff who train and supervise village-based iCCM volunteers express concern about the difficulty in acquiring enough medicines for their own clinical needs, let alone supplies for volunteer community health workers.
 Other programs reserve iCCM only for selected communities in a catchment area based on distance or availability of community health extension/auxiliary workers. There are also examples of iCCM that are narrowly focused on one or two health problems, while others take a more comprehensive approach. Clearly each has different logistical concerns such as the generic issues of forecasting, procurement, shipping and storage, while others experience the difficulty obtaining funding support when many disease control programs have vertical financial streams.
Other programs reserve iCCM only for selected communities in a catchment area based on distance or availability of community health extension/auxiliary workers. There are also examples of iCCM that are narrowly focused on one or two health problems, while others take a more comprehensive approach. Clearly each has different logistical concerns such as the generic issues of forecasting, procurement, shipping and storage, while others experience the difficulty obtaining funding support when many disease control programs have vertical financial streams.
There are various models for providing medicines at the community level. One is the pioneering work of the World Health Organization’s (WHO’s) Tropical Disease Research (TDR) program in promoting Community-Directed Treatment with Ivermectin (CDTI) for River Blindness Control, which evolved into the Community Directed Intervention (CDI) approach for delivering basic health commodities by the community, itself.[1] …
Policymakers, health organizations, and front-line clinicians often say, “no product, no program.” This themed issue will share the experiences and lessons of iCCM, both successes and challenges, to help the global health community see the need for more systematic planning of PSM for iCCM. International agencies and donors clearly recognize that alternative forms of essential health service delivery are needed to achieve coverage targets and save lives. The community as a source of care has a solid foundation as established at the International Conference on Primary Health Care, which produced global guidance through the Alma Ata Primary Health Care Declaration of 1978,[2] but in all those years, actualization of this ideal has been difficult for logistical reasons. This RSAP themed issue should not only help us understand the present challenges, but map a way forward to better access to essential health commodities in communities throughout the developing world.
The themed issue will include various contributions such as:
- Commentary/Overview from the World Health Organization staff who have spearheaded the iCCM movement
- Implementation/intervention research on:
- The link between front-line clinics and community health workers/distributors in guaranteeing iCCM commodities
- The challenge of providing iCCM commodities for use by nomadic populations
- Provision of iCCM commodities by different types community workers
- Successes and challenges in maintaining supplies and commodities for large-scale and national community primary health care programs
- Comparative lessons from other community based programs such as family planning commodity distribution and home-based care for people living with HIV
- Documented program experiences including:
- The challenges of maintaining iCCM supplies and logistics in emergency situations, as with disaster refugee and outbreak situations
- The role of donors and non-governmental organizations (NGOs) in providing commodities.
We are still seeking additional contributions. If you have a paper or idea for one or more, please contact the guest editors. Papers must be submitted on the Elsevier RSAP platform at http://ees.elsevier.com/rsap/ by February 1, 2016 for publication in fall of 2016.
Guest Editors:
- William R Brieger, MPH, DrPH, Professor, Department of International Health, Bloomberg School of Public health, The Johns Hopkins University; Senior Malaria Specialist, Jhpiego; RSAP Editorial Board Member. <bbbrieger@yahoo.com>
- Maria KL Eng, MPH, PhD, Departmental Associate, Department of International Health, Bloomberg School of Public health, The Johns Hopkins University; Instructor for “Pharmaceuticals Management for Under-Served Populations” <meng@jhu.edu>
[1] http://www.who.int/bulletin/volumes/88/7/09-069203/en/
[2] http://www.who.int/dg/20080915/en/