Ebola &Health Rights Bill Brieger | 30 Oct 2014
Louisiana: High Rhetoric on Ebola, Low Concern for Public Health
The 63rd Annual Meeting of the American Society for Tropical Medicine and Hygiene begins in a couple days in New Orleans Louisiana. In preparation for this event the Governor of Louisiana through the Department of Health and Hospitals dis-invited any conference participant who has been to an Ebola-affected country (Liberia, Guinea, Sierra Leone) with the following information:
 NOTICE TO TRAVELERS: From a medical perspective, asymptomatic individuals are not at risk of exposing others; however, the State is committed to preventing any unnecessary exposure of Ebola to the general public. As part of that commitment, we have requested that any individuals that will be traveling to Louisiana following a trip to the West African countries of Guinea, Liberia, and Sierra Leone or have had contact with an EVD-infected individual remain in a self-quarantine for the 21 days following their relevant travel history. In Louisiana, we love to welcome visitors, but we must balance that hospitality with the protection of Louisiana residents and other visitors.
NOTICE TO TRAVELERS: From a medical perspective, asymptomatic individuals are not at risk of exposing others; however, the State is committed to preventing any unnecessary exposure of Ebola to the general public. As part of that commitment, we have requested that any individuals that will be traveling to Louisiana following a trip to the West African countries of Guinea, Liberia, and Sierra Leone or have had contact with an EVD-infected individual remain in a self-quarantine for the 21 days following their relevant travel history. In Louisiana, we love to welcome visitors, but we must balance that hospitality with the protection of Louisiana residents and other visitors.
Not only does this decision, which bars many people who had no contact with patients or infected people, lack scientific backing, it is also unlikely to do much for health of Louisiana. These citizens actually need more that fearful proclamations to protect them. Louisiana needs to step up its public health efforts to show it really cares about its residents instead of political grandstanding.
 America’s Health Rankings from the United Health Foundation presents some interesting information on each US state – not just its ranking overall, but factors that contribute to this ranking. Overall, Louisiana ranked 48th in 2013. While there are 30 key indicators, ranks on individual vary with 24 being negative and 6 having a positive influence in the Louisiana’s overall 2013 rankings. Some problem areas are noted below:
America’s Health Rankings from the United Health Foundation presents some interesting information on each US state – not just its ranking overall, but factors that contribute to this ranking. Overall, Louisiana ranked 48th in 2013. While there are 30 key indicators, ranks on individual vary with 24 being negative and 6 having a positive influence in the Louisiana’s overall 2013 rankings. Some problem areas are noted below:
- Obesity 50th
- Smoking 46th
- High School Graduation 46th
- Low Birth Weight 49th
- Infant Mortality 48th
- Infectious Disease 48th
- Preventable Hospitalizations 48th
Of particular interest is public expenditure to address health problems. Here Louisiana ranks 19th at $87 per capita, below the national average. “After 4 years of increases, public health funding (in Louisiana) declined in the past year,” according to America’s Health rankings.
Nationally, “Public health funding ranges from more than $200 per person in Alaska and Hawaii to $37 per person in Nevada. The average funding in the United States is $92 per person, unchanged from last year’s edition (2012).” Louisiana, while not the lowest spender, could certainly do more to bring itself up in the rankings and help its people.
We would understand Louisiana’s concern if it had done more to correct these low rankings. The State’s neglect of its citizens is more of a threat to public health than a visiting conference attender who may have tried to improve public health in Africa.
Communication &Ebola &Epidemic Bill Brieger | 26 Oct 2014
What the Press Tells Us about the Early Days of Liberia’s Ebola Outbreak
The mass media are assumed to play an important role in the national response to a crisis, and Ebola should be no exception. The first cases of the disease in Liberia appeared in March 2014 after victims crossed the border from its point of origin In Guinea. A search for Ebola-related articles from the early period, March to May, was undertaken in The Liberian Observer.
 While to date over 1,000 articles and references on Ebola were found in The Liberian Observer, most of the news coverage has appeared from August to October. In particular there were few articles in March, a surge in April and then a tapering off in May and June, before Ebola gained more prominence in print from July onwards.
While to date over 1,000 articles and references on Ebola were found in The Liberian Observer, most of the news coverage has appeared from August to October. In particular there were few articles in March, a surge in April and then a tapering off in May and June, before Ebola gained more prominence in print from July onwards.
Generally the early news articles in the Observer report events and opinions surrounding Ebola rather than serve as direct avenues for behavior change communication (BCC). Articles on politics, science, religion, economics, social commentary and even cartoons focused indirectly or directly on key events in the development of the national response.
 Because of upcoming elections politicians used the outbreak to criticize each other’s response to the problem. In the early days the economic concerns focused primarily on reduced revenues across national borders in the region. Religious leaders either tried to rally support for control through prayer and fasting or blamed the epidemic on sin.
Because of upcoming elections politicians used the outbreak to criticize each other’s response to the problem. In the early days the economic concerns focused primarily on reduced revenues across national borders in the region. Religious leaders either tried to rally support for control through prayer and fasting or blamed the epidemic on sin.
A couple opinion pieces in April acknowledged that BCC was going on through the radio. Special events such as sporting and athletics adopted an Ebola prevention theme, and several local NGOs pledged support for community outreach and awareness creation. Senators even had a retreat to learn more about the disease so they could educate their constituents.
 On March 23rd Marday L Peters wrote in the Observer, As Deadly Virus Threatens Liberia, Where is the Outcry?” At least from the communications point of view, the situation improved in April.
On March 23rd Marday L Peters wrote in the Observer, As Deadly Virus Threatens Liberia, Where is the Outcry?” At least from the communications point of view, the situation improved in April.
A.M. Johnson, The Health Correspondent for the Observer reported about Health Promoters Network, Liberia (HPNL) on April 3rd, quite early in the outbreak. HPNL in expressing its support for Ministry of Health and Social Welfare efforts “urged everyone within our borders to adhere to those preventive measures such as do not eat animals that are found dead in the bush, and avoid contacts with fruit bats, monkeys, chimpanzees, antelopes and porcupines. Limit as much as possible direct contact with body fluids of infected persons or dead persons. Wash your hands with soap and water as frequently as possible.” HPNL called on other Liberian NGOs to join the cause of educating the public.
On April 20th, S. Vaanii Passewe, II mentioned in a commentary that, “… the airwaves were laden with the news of an outbreak of the deadly Ebola outbreak… Subsequent warnings from the Ministry of Health notably said that the populace should report suspected cases, refrain from coming into body contact with suspected Ebola patients, avoid shaking hands, do not have casual sex with strangers, etc. These weird precautionary measures heightened fear.”
Some actionable information was provided in regular news articles in April. For example in an article on April 25th The Observer talked about “Ending Ebola in Liberia, A Collective Approach Needed,” readers were told about the symptoms, the potential spread through fruit bats and the fact that there was no specific cure, but supportive care is needed.
Further study of more mass media outlets concerning Liberia’s Ebola control efforts is needed. We know that although an early start to educate the public was undertaken, a relative dearth of coverage in the Observer might also indicate a reduction in enthusiasm by the press, NGOs and government to sustain Ebola communication and action. For whatever reason, the epidemic spiked. Fortunately efforts are now back on track, but there is a long road ahead.
Diagnosis Bill Brieger | 23 Oct 2014
Marketing approval for UMT from the Nigeria NAFDAC
 Fyodor Biotechnologies Inc. has sponsored a study to evaluate the clinical performance of the one-step Fyodor Urine Malaria Test (UMT), to determine its accuracy (sensitivity and specificity) for the diagnosis of Plasmodium falciparum malaria in febrile patients.
Fyodor Biotechnologies Inc. has sponsored a study to evaluate the clinical performance of the one-step Fyodor Urine Malaria Test (UMT), to determine its accuracy (sensitivity and specificity) for the diagnosis of Plasmodium falciparum malaria in febrile patients.
A total of 1500 properly consented children and adults presenting with fever (axillary temperature ?37.5°C) or history of fever in the last 48 hours (Group 1), 250 apparently “healthy” individuals (Control, Group 2), and 50 patients with Schistosoma hematobium and Rheumatoid arthritis (Group 3), were recruited.
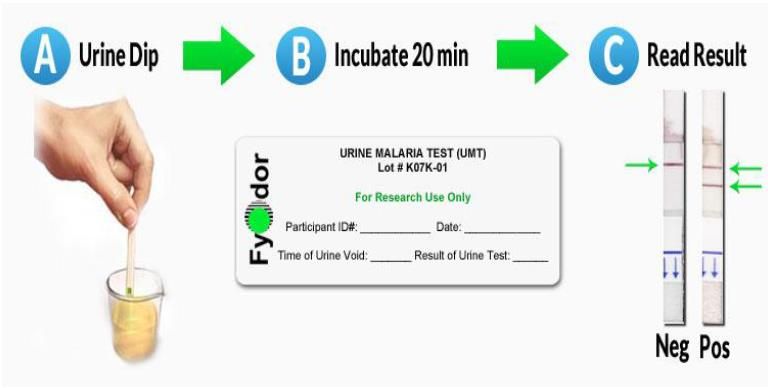 Matched urine and fingerprick (capillary) blood samples were collected and tested using the UMT and, Binax NOW® malaria rapid diagnostic test (blood test) and thick smear microscopy, respectively. The overall agreement of the UMT results to the Binax NOW analysis and thick smear microscopy was used to establish UMT sensitivity and specificity.
Matched urine and fingerprick (capillary) blood samples were collected and tested using the UMT and, Binax NOW® malaria rapid diagnostic test (blood test) and thick smear microscopy, respectively. The overall agreement of the UMT results to the Binax NOW analysis and thick smear microscopy was used to establish UMT sensitivity and specificity.
The UMT showed comparable performance with blood-based tests. The UMT has the potential of expanding access to parasitological confirmation of malaria in both the public and private health sector as well as the community
As a result, Fyodor has now received marketing approval for the UMT from the Nigeria NAFDAC (food and drug agency).
According to the Principal Investigator, Wellington Oyinbo of the University of Lagos, “This is a defining moment for malaria case management and hopefully, countries will be able to meet their set national targets for parasitological confirmation of malaria. Important as well is the fact that a strip of nitrocellulose paper is able to fast-track malaria diagnosis in an otherwise weak health/diagnostic system.”
Community Bill Brieger | 14 Oct 2014
The reception of village malaria workers in rural Cambodia: knowledge, perceptions, and preferences in user communities
The recently concluded Global Health Systems Research Symposium in Cape Town featured a number of abstracts that touched directly or indirectly on malaria. Malaria services and movement toward malaria elimination cannot be achieved in a country without a strong health system that involves both communities, program staff and policy makers.
 Below is an abstract by Marco Liverani, Ra Sok, Daro Kim, Panarith Nou, Sokhan Nguon, Chea Nguon, Shunmay Yeung of the London School of Hygiene and Tropical Medicine, UK, Partners for Development, Cambodia and Ministry of Health, Cambodia on malaria village health workers in Cambodia.
Below is an abstract by Marco Liverani, Ra Sok, Daro Kim, Panarith Nou, Sokhan Nguon, Chea Nguon, Shunmay Yeung of the London School of Hygiene and Tropical Medicine, UK, Partners for Development, Cambodia and Ministry of Health, Cambodia on malaria village health workers in Cambodia.
“Despite sustained efforts to strengthen the health system and significant progress, Cambodia still suffers from critical shortages of health professionals and inequities in the distribution of health services. This problem is particularly acute in remote areas, where the incidence of infectious diseases such as malaria and typhoid fever is higher, where access to health facilities may be limited by environmental barriers, and where poor communities bear the greatest economic burden of illness.

Village Malaria Worker courtesy of WHO: http://who.int/malaria/areas/greater_mekong/cambodia-frontline-heroes/en/
“Over the past decade, the deployment of lay members of the community to provide basic medical services amongst the most vulnerable populations has been one of the key interventions to address this problem.
“We conducted a qualitative study to examine the reception and impact of the Village Malaria Workers (VMW) programme in Cambodia, a community-based intervention to support the management of malaria cases and childhood illnesses.
“Methods included observations and in-depth interviews (n=80) in user communities. A thematic question guide with open-ended questions was used for the interviews. Thematic content analysis was then conducted to explore factors that may promote or discourage service utilisation.
“Many respondents thought that VMWs can deliver appropriate medical care and services, but some expressed a preference for private providers as these were seen to offer more comprehensive and qualified health care. Many respondents had inadequate awareness of VMWs and the range of services they provide.”
“Findings from our study point to the need for innovative communication strategies to increase the utilisation of VMWs. We argue that investment in symbols and visual communication tools are required to promote the visibility, status, and identity of health volunteers in user communities, also given current policy trends – in and outside Cambodia – towards an increasing use of community workers to perform roles and tasks that are conventionally associated with health professionals.
Community &Integration &Treatment Bill Brieger | 11 Oct 2014
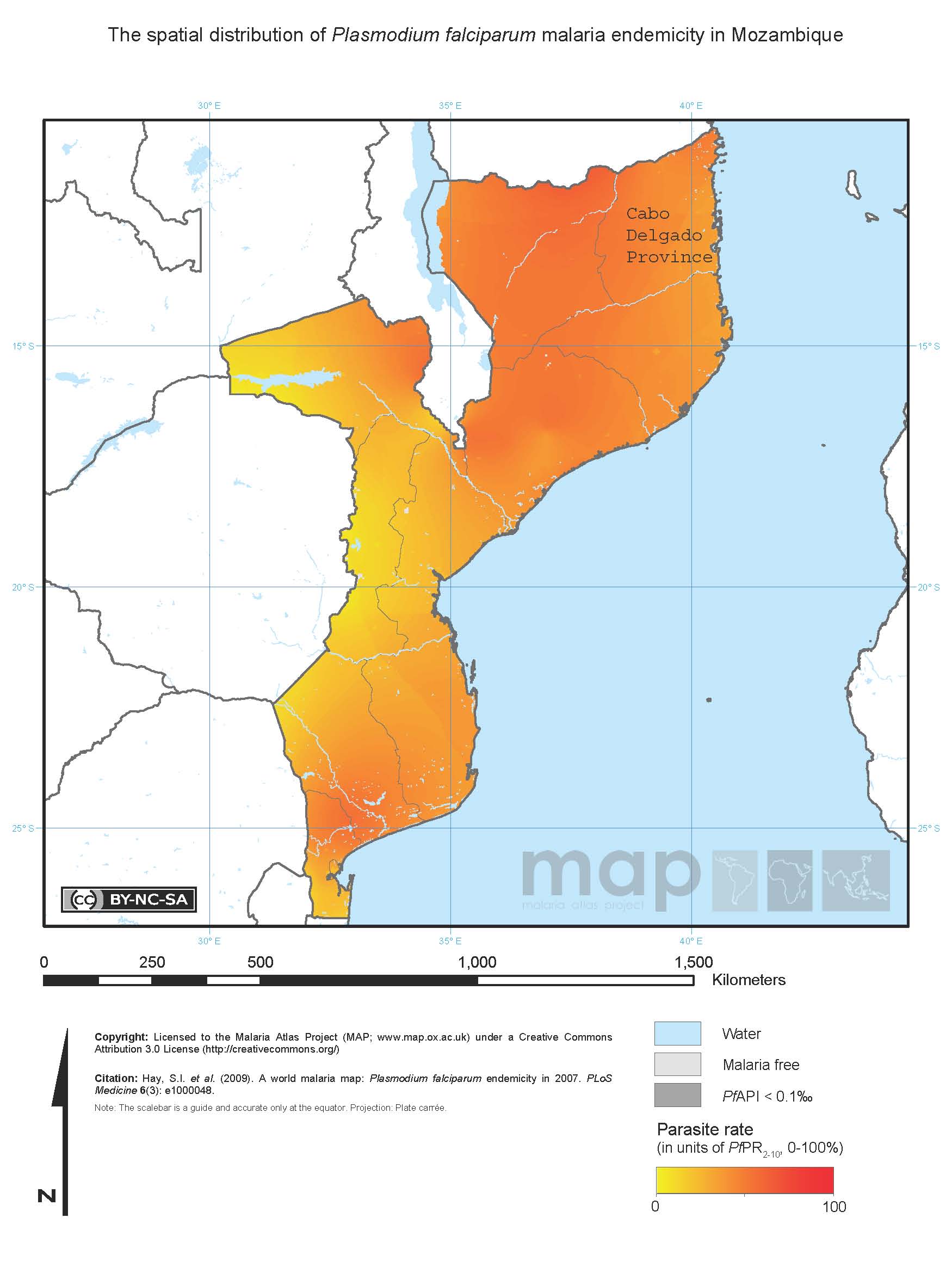
Is community case management sustainable in Mozambique? A qualitative policy analysis
The recently concluded Global Health Systems Research Symposium in Cape Town featured a number of abstracts that touched directly or indirectly on malaria. Malaria services and movement toward malaria elimination cannot be achieved in a country without a strong health system that involves both communities, program staff and policy makers.
Below is an abstract by Baltazar Chilundo, Julie Cliff, Alda Mariano, Daniela Rodrigues, and Asha George of the University Eduardo Mondlane, Mozambique and the Johns Hopkins School of Public Health on the sustainability of community case management, building on longstanding community health worker programs. They stress the importance of community commitment, an often missing factor when CHW and CCM programs are organized by national agencies.
“In Mozambique, community case management (CCM) of diarrhoea, malaria and pneumonia is embedded in the national community health worker (CHW) programme. Since 1978 this programme functioned fitfully and was relaunched in 2010, with a target to train and retrain over 6000 CHWs.
 “Considering the checkered history of the CHW program, sustainability lies at the heart of concerns related to the design and implementation of CCM in CHW programs at scale in Mozambique and in people centred health systems more broadly.
“Considering the checkered history of the CHW program, sustainability lies at the heart of concerns related to the design and implementation of CCM in CHW programs at scale in Mozambique and in people centred health systems more broadly.
“Using qualitative retrospective case study methodology, we reviewed 54 national documents and interviewed 21 key national informants for a policy analysis of CCM in Mozambique. The data were analysed thematically according to a sustainability framework and validated though a national debriefing workshop.
“The sustainability of CCM was facilitated by embedding it in the national CHW programme, which was relaunched after wide consultation within government and with supportive donors and non-governmental organizations (NGOs).
“Although communities were not widely consulted, they were eager for CHWs to provide curative services. The new CHW program aimed to improve CHW retention, by paying them a salary and giving priority to females. However, salary costs come from partners and in practice most CHWs are male.
“The poor capacity of the health system to adequately supervise CHWs and guarantee drug supplies for CCM, the dependence on external partners for funding, and on NGOs for implementation and the lack of mobilization of communities and top policy makers remain critical concerns.
“Embedding CCM in the national CHW programme favoured sustainability, however this made CCM susceptible to the same factors that undermine sustainability of the CHW programme. Moving forward, these policy concerns need to be addressed to ensure a national CHW program, responsive to community needs, supportive of CHW themselves and owned by national governments.”
Community &Drug Quality &Private Sector &Treatment Bill Brieger | 08 Oct 2014
Registered drug shops are preferred for treating acute febrile illness in rural Uganda
The recently concluded Global Health Systems Research Symposium in Cape Town featured a number of abstracts that touched directly or indirectly on malaria. Malaria services and movement toward malaria elimination cannot be achieved in a country without a strong health system that involves both communities, program staff and policy makers.
Below is an abstract by Freddy Kitutu, Chrispus Mayora, Phyllis Awor, Forsberg Birger, Stefan Peterson, and Henry Wamani of Makerere University and the Karolinska Institute on use of medicine shops in Uganda.
“Under-five child mortality in Uganda is still high and majority is caused by easily treatable pneumonia, malaria and diarrhoeal diseases among the poorest people. One of the reasons for these deaths is the lack of timely access to proven life saving medicines. This hinders progress towards attainment of MDG 4 target by 2015.
“To increase access to quality medicines and diagnostics for child febrile illnesses, Makerere University School of Public Health (MakSPH) in collaboration with WHO Alliance for Health Policy and Systems Research, is doing a project to assess the potential to deliver quality integrated care for malaria, pneumonia and diarrhoea using integrated community case management (iCCM) strategies and tools. Hence, an assessment was conducted to determine baseline care seeking preferences.
“A baseline household survey interviewed caregivers of children under-five years. The study protocol and data collection tools had been reviewed and approved by Research and Ethics Committees at WHO, MakSPH and Uganda National Council of Science and Technology.
“A total of 2606 households were surveyed. The main childhood diseases reported included fever (70%), cough (77%), and diarrhoea (40%) convulsions (16%) Most households use private drug shops to purchase medicines to manage these illnesses. Use of drug shops was attributed to long distances to public health facilities, availability and reliability of drug stocks at drug shops, perceived high quality of services, and options for credit.
“Interventions that target public health facilities are likely to miss many healthcare seekers especially the poor in rural distant areas. Conclusion: Drug shops are the convenient and preferred outlets for rural poor communities, and therefore need to be included in interventions such as iCCM strategy.
“Significance for the selected field-building dimension: This abstract presents findings from the baseline assessment prior to introducing a health system intervention in drug shops to improve access to and quality of care for under-five children.”
Uncategorized Bill Brieger | 05 Oct 2014
Unwilling or unable? understanding healthcare providers’ perspectives on guideline compliance for malaria testing in Ghana
The recently concluded Global Health Systems Research Symposium in Cape Town featured a number of abstracts that touched directly or indirectly on malaria. Malaria services and movement toward malaria elimination cannot be achieved in a country without a strong health system that involves both communities, program staff and policy makers.
Below is an abstract by Nana Yaa Boadu (IDRC), John Amuasi (University of Minnesota), Daniel Ansong KATH Kumasi), Edna Einsedel (University of Calgary), and Stephanie Yanow, (University of Alberta) on malaria/febrile illness testing in Ghana. Other abstracts will appear subsequently.
“The test-based malaria management guideline in Ghana reflects a 2009 recommendation by the World Health Organization, to confirm suspected cases before providing treatment. The guideline aims to limit inappropriate antimalarial use, which contributes to emerging drug resistance. Rapid diagnostic tests (RDTs) enable confirmatory malaria diagnosis in peripheral settings without microscopy.
“Yet healthcare providers frequently prescribe antimalarials without a test, or despite negative test results. This study investigated poor providers’ compliance with the malaria testing guideline. The findings are useful to streamline antimalarial prescribing practices, to improve malaria management, and to limit drug resistance development in Ghana.
“A focused ethnography conducted between November 2011 and October 2012 involved 50 providers at six different primary healthcare settings in the Atwima-Nwabiagya district. Observations, semi-structured interviews and focus groups involving providers revealed reasons for poor compliance. Consultations with local and national policy representatives identified system-wide factors affecting providers’ compliance, including national health insurance.
“Poor availability and quality of RDTs, heavy workloads, and insufficient guideline knowledge limited providers’ readiness to test before treating suspected malaria. Knowing the risks and consequences of delayed treatment, providers were unwilling to withhold antimalarials from suspected cases. Due to frequent RDT stock outs testing was sporadic, often conducted after treated patients returned with unyielding signs and symptoms.
“Limited healthcare delivery capacity created tension for providers between recommended and achievable practice standards, which restricted effective guideline implementation. Perceived patient risk and poor RDT quality undermined providers’ willingness to test, leading to precautionary treatment practices. These factors interdependently influenced guideline compliance.
“Training should enhance providers’ knowledge of policy, practice, and technology for diagnosing malaria. However, health system capacity-building is critical to bolster providers’ confidence in RDT and guideline utility for managing malaria.”
Private Sector &Procurement Supply Management &Treatment Bill Brieger | 05 Oct 2014
Licensed chemical sellers and antimalarial prices in northern Ghana under the affordable medicines facility
The recently concluded Global Health Systems Research Symposium in Cape Town featured a number of abstracts that touched directly or indirectly on malaria. Malaria services and movement toward malaria elimination cannot be achieved in a country without a strong health system that involves both communities, program staff and policy makers.
Below is an abstract by Heather Lanthorn of the Harvard School of Public Health on the AMFm program testing in Ghana. Other abstracts will appear subsequently.
“The Affordable Medicines Facility – malaria (AMFm) represents an important experiment in using private retail chains to improve access to medicines in low- and middle-income countries. AMFm aimed to make quality-assured artemisinin-based combination therapies (QA.ACTs) accessible at the variety of outlets where citizens treat fevers. In Ghana, where ACTs are legally sold over the counter, Licensed Chemical Sellers (LCS) are a key antimalarial provider.
“I use a framework adapted from industrial organization to study a unique, geo-coded data set of 250 LCSs in and around Tamale, Ghana collected explicitly for this study. Through well-integrated quantitative (multiple logistic regression) and qualitative (open thematic analysis) approaches, I analyze: the experiences of LCSs with AMFm; LCS reported compliance with recommended retail prices (RRPs); LCS economic and social explanations for compliance; and associations between LCS objective characteristics – including geo-location – and RRP compliance.
“We find high stocking of subsidized QA.ACTs and high RRP compliance. 18% of LCSs report selling above the RRP. The majority of non-compliers cite rising prices from their supplier as the major determinant of their own pricing. The majority of non-compliers sold at USD 1.5 rather than the RRP, USD 1.0. Indeed, in the quantitative analysis, RRP compliance is most clearly associated with the distributor prices and with LCS reputation (years in business).
 “A driving motivation for experimentally piloting AMFm was to learn whether the QA.ACT subsidy would be passed on to end-line private retailers and, in turn, to consumers. We find that, largely, it is. By considering LCSs both as economic agents and community members, the present analyses accord with, complement and innovate on the large, independent evaluation of AMFm, which focused on prices but neither objective nor perceptual explanations for price-compliance.”
“A driving motivation for experimentally piloting AMFm was to learn whether the QA.ACT subsidy would be passed on to end-line private retailers and, in turn, to consumers. We find that, largely, it is. By considering LCSs both as economic agents and community members, the present analyses accord with, complement and innovate on the large, independent evaluation of AMFm, which focused on prices but neither objective nor perceptual explanations for price-compliance.”