Out-of-hospital cardiac arrest (OHCA) is estimated to have an average global incidence of 55 adults per 100,000 person-years. However, despite advances in medical care and technology, survival to hospital discharge remains abysmally low at 8-10%. In low to middle income countries like Nigeria, where cardiovascular disease is rising but emergency response systems are poor, the rate of survival after OHCA is lower.
Interventions such as bystander cardiopulmonary resuscitation (CPR) training and automated external defibrillator (AED) use are effective, scalable, and low-cost interventions that can reduce the OHCA mortality. Training schoolchildren to perform Hands-only CPR has been shown to increase bystander CPR.
Cardiopulmonary Resuscitation Peer Educator’s Program (CPEP) is a community-based program in Ibadan, Nigeria, designed enhance understanding of CPR in secondary school students. The American Heart Association’s school health module was adapted. The training was run jointly by staff of the four pilot schools, a Nigerian NGO, and the Revolving Hearts Foundation, Atlanta.
The training had both in-person and virtual components due to COVID-19 travel restrictions on Atlanta based partners. Here we present the results of training on knowledge, comfort level and perceived barriers of performing hands-only CPR.
A pre-training survey was conducted in February 2021 using convenience sampling that also was used to recruit participants. Pre- and post- training responses were matched by participants to assess the changes. Data were analyzed using Stata 16.1 software. A paired t-test analysis was conducted. The primary outcome was a percentage change in mean knowledge scores and secondary outcome was a change in comfort level and perceived barriers pre- and post- training.
A total of 45 secondary school students from 4 schools completed the tests. Females comprised 31.1% of students and the average age was 15.02 + 0.18 years. Paired t-test showed a significant change of 44.6% (p <0.0001) in the mean knowledge score. There was also an increase in comfort level in performing hands-only CPR, and a decrease in perceived barriers.
Trainees have started sharing what they learned through skits at school assemblies. Planning is underway to follow-up on training and to expand to other schools and states.
PS: as a followup another training session with a new group of 45 students and 15 teachers was conducted. The students made videos of their understanding of CPR from the program so it could be used for peer education, and most of them were pretty good and creative.
Inside the first grade class of a Malaria Smart School
Uganda suffers from one of the highest burdens of malaria in Sub-Saharan Africa and in the world. Many Ugandans are familiar with bed nets and many have visited health clinics for malaria treatment. But still, malaria affects a high percentage of the country’s population.
In 2019, I traveled to outside of Kampala, Uganda to visit a malaria education and prevention program run by the National Malaria Controlle Program within the Ugandan Ministry of Health and USAID’S President’s Malaria Initiative (PMI). The program is referred to a Malaria Smart School where education about malaria is incorporated into the curriculum of each grade.
A “malaria corner” in a Malaria Smart School classroom
Each classroom has what is called a “malaria corner” where students’ projects on the anatomy of mosquitos, malaria parasite life cycle, the spread of malaria, and artistic expressions about malaria are featured.
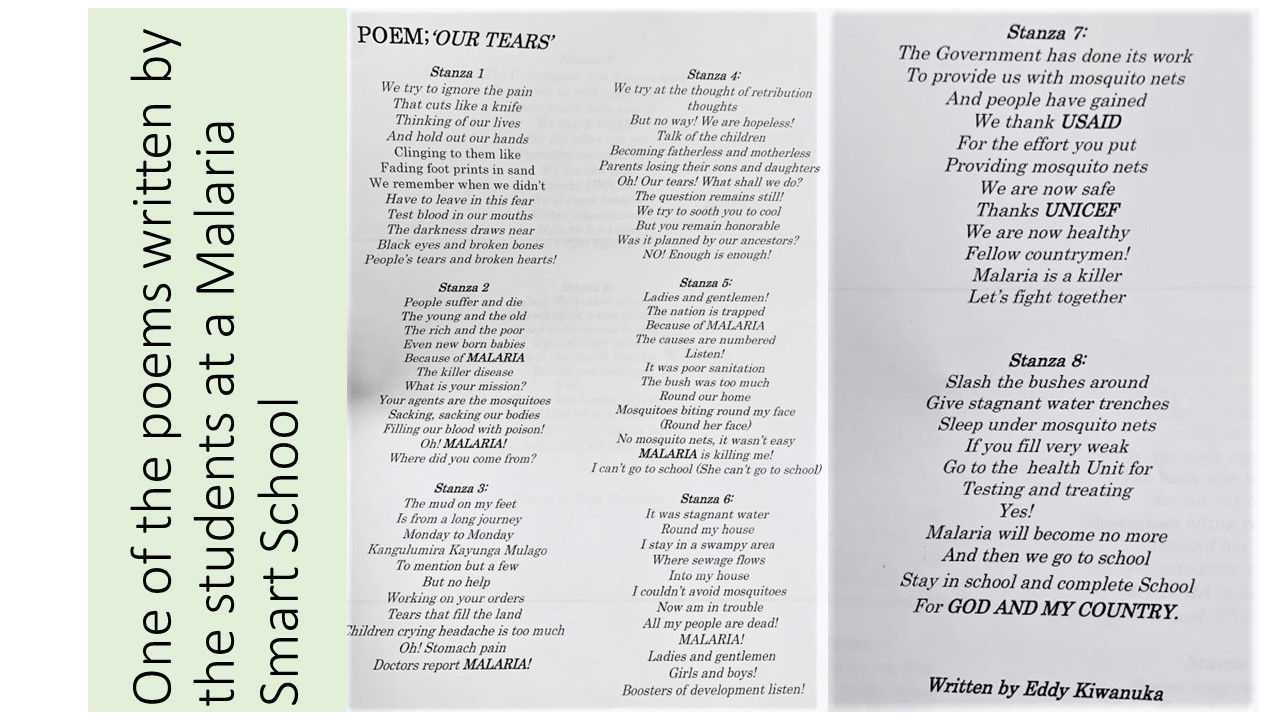
The Malaria Smart School also incorporates education on malaria into song, dance, and art. In this way, students are learning more about how malaria is spread than any generation before them, which is also an important factor considering their population is so large! Pictured below is a poem written by the malaria smart school students. The poem was recited along with dance and acting.
The Ugandan Ministry of Health and PMI have been pleased with the Malaria Smart School program. It was evident during my visit that the students have gained a comprehensive knowledge of malaria and a knowledge they share and are passing onto their families and people they live with. In fact, one of the primary goals of this program was to break behavior cycles in the community regarding malaria through the students’ learning. The result of this program is that children are able to teach older generations proper preventative strategies about malaria, treatment options, and even basic scientific epidemiology of malaria.
This is already disrupting behaviors, leading older generations to seek proper care and follow proper mitigation efforts to combat malaria. If these programs were to expand to other regions in Uganda, within even a generation, there would be a significant decline in malaria cases because of the knowledge learned and passed on by these children. The Malaria Smart School program is one many countries should model in their national malaria control programs, and with outside support from partnering organizations like PMI, this model could really impact the global burden of malaria.
Recent publications in Malaria Journal, The Lancet and eLife tackle several challenges to saving lives and malaria elimination. Problems include low access to bednets for children in Ethiopia, high prevalence of asymptomatic malaria in Ghanaian adults, risk of co-infection with other infectious diseases, and gaps in current interventions to prevent malaria in pregnancy and children. On the hopeful side, new targets for drug therapy are being identified. Read more on each by following the links below.
Long-lasting insecticide-treated bed net ownership, utilization and associated factors among school-age children in Southern Ethiopia
Dara Mallo and Uba Debretsehay districts because malaria is one of the major causes of morbidity and mortality among school-age children (SAC) in sub-Saharan Africa. This study was part of a baseline assessment in a cluster-randomized controlled trial.
The ownership of at least one LLIN by households of school-aged children (SAC) was about 19.3% (95% CI 17.7–21.0%) but only 10.3% % (95% CI 7.7–13.7%) of these households had adequate access of bed nets to the household members. Ownership of bed net was lower than universal coverage of at least one bed net for two individuals. It is important to monitor replacement needs and educate mothers with low education level with their SAC on the benefit of consistent utilization of bed nets.
Prevalence of and risk factors for Plasmodium spp. co-infection with hepatitis B virus: a systematic review and meta-analysis
Kotepui and Kotepui observed that Plasmodium spp. and hepatitis B virus (HBV) are among the most common infectious diseases in underdeveloped countries. Therefore they examined co-infection in people living in endemic areas of both diseases. The PubMed, Web of Science, and Scopus databases were searched. Observational cross-sectional studies and retrospective studies assessing the prevalence of Plasmodium species and HBV co-infection were examined. and found 22 studies to include in a systematic review and meta-analysis. Overall, the pooled prevalence estimate of Plasmodium spp. and HBV co-infection was 6% (95% CI 4–7%, Cochran’s Q statistic?<?0.001, I2: 95.8%).
No difference in age or gender and risk of Plasmodium spp. and HBV co-infection group was found. The present study revealed the prevalence of Plasmodium spp. and HBV co-infection, which will help in understanding co-infection and designing treatment strategies. Future studies assessing the interaction between Plasmodium spp. and HBV are recommended.
High prevalence of asymptomatic malaria infections in adults, Ashanti Region, Ghana, 2018
Melina Heinemann and co-researchers noted that Ghana is among the high-burden countries for malaria infections and recently reported a notable increase in malaria cases. While asymptomatic parasitaemia is increasingly recognized as a hurdle for malaria elimination, studies on asymptomatic malaria are scarce, and usually focus on children and on non-falciparum species. Therefore asymptomatic adult residents from five villages in the Ashanti Region, Ghana, were screened for Plasmodium species by rapid diagnostic test (RDT) and polymerase chain reaction (PCR) during the rainy season. Samples tested positive were subtyped using species-specific real-time PCR.
Molecular prevalence of asymptomatic Plasmodium infection was 284/391 (73%); only 126 (32%) infections were detected by RDT. While 266 (68%) participants were infected with Plasmodium falciparum, 33 (8%) were infected with Plasmodium malariae and 34 (9%) with P. ovale. The sub-species P. ovale curtisi and P. ovale wallikeri were identified to similar proportions. Non-falciparum infections usually presented as mixed infections with P. falciparum.
Most adult residents in the Ghanaian forest zone are asymptomatic Plasmodium carriers. The high Plasmodium prevalence not detected by RDT in adults highlights that malaria eradication efforts must target all members of the population. Beneath Plasmodium falciparum, screening and treatment must also include infections with P. malariae, P. o. curtisi and P. o. wallikeri.
Scientists shed new light on mechanisms of malaria parasite motility
eLife reports a new insight on the molecular mechanisms that allow malaria parasites to move and spread disease within their hosts has just been published. The first X-ray structures of the molecular complex that allows malaria parasites to spread disease highlight a novel target for antimalarial treatments.
The movement and infectivity of the parasite Plasmodium falciparum, and ultimately its ability to spread malaria among humans, rely on a large molecular complex called the glideosome. The new findings provide a blueprint for the design of future antimalarial treatments that target both the glideosome motor and the elements that regulate it.
New Lancet Series: Malaria in early life
Malaria infections are harmful to both the pregnant mother and the developing fetus. Malaria is associated with a 3–4 times increased risk of miscarriage and a substantially increased risk of stillbirth, and it disproportionately affects children younger than 5 years. Falciparum malaria is responsible for more than 200 000 child deaths per year in Africa and vivax malaria causes excess mortality in children in Asia and Oceania. In a duet of papers, we review 1) the deleterious effects of malaria in pregnancy on the developing fetus and 2) the current strategies for prevention and treatment of malaria in children.
Paper 1 is “Deleterious effects of malaria in pregnancy on the developing fetus: a review on prevention and treatment with antimalarial drugs” by Makoto Saito, Valérie Briand, Aung Myat Min, and Rose McGready. The authors are concerned that one in ten maternal deaths in malaria endemic countries may result from Plasmodium falciparum infection, that malaria is associated with a 3–4 times increased risk of miscarriage and a substantially increased risk of stillbirth. While current treatment and prevention strategies reduce, but do not eliminate, malaria’s damaging effects on pregnancy outcomes. They conclude that there is a need for alternative strategies to prevent malaria in pregnancy.
Paper 2 is “Treatment and prevention of malaria in children” by Elizabeth A Ashley and Jeanne Rini Poespoprodjo. They examine the following interventions: Triple antimalarial combination therapies, the RTS,S/AS01 vaccine, seasonal malaria chemoprevention and preventing relapse in Plasmodium vivax infection with primaquine.
If all it took to eradicate a disease was a well proven drug, vaccine or technology, we would not be still reporting on polio, measles and guinea worm, to name a few. In the past week Afghanistan reported 2 wild poliovirus type 1 (WPV1) cases, and Pakistan had 3 WPV1 cases. Circulating vaccine-derived poliovirus type 2 (cVDPV2) was reported in Nigeria (1), DRC (4) and Ethiopia (3) from healthy community contacts.
Continued Ebola Challenges
In the seven days from Saturday to Friday (June 28) there were 71 newly confirmed Ebola Cases and 56 deaths reported by the Democratic Republic of Congo’s Ministry of Health. As Ebola cases continue to pile up in the Democratic Republic of the Congo (DRC), with 12 more confirmed Thursday and 7 more Friday, a USAID official said four major donors have jump-started a new strategic plan for coordinating response efforts. To underscore the heavy toll the outbreak has caused, among its 2,284 cases, as noted on the World Health Organization Ebola dashboard today, are 125 infected healthcare workers, including 2 new ones, DRC officials said.
Pacific Standard explained the differences in Ebola outbreaks between DRC today and the West Africa outbreak of 2014-16. On the positive side are new drugs used in organized trials for the current outbreak. The most important factor is safe, effective vaccine that has been tested in 2014-16, but is now a standard intervention in the DRC. While both Liberia and Sierra Leone had health systems and political weaknesses as post-conflict countries, DRC’s North Kivu and Ituri provinces are currently a war zone, effectively so for the past generation. Ebola treatment centers and response teams are being attacked. There are even cultural complications, a refusal to believe that Ebola exists. So even with widespread availability of improved technologies, teams may not be able to reach those in need.
To further complicate matters in the DRC, Doctors Without Borders (MSF) “highlighted ‘unprecedented’ multiple crises in the outbreak region in northeastern DRC. Ebola is coursing through a region that is also seeing the forced migration of thousands of people fleeing regional violence and is dealing with another epidemic. Moussa Ousman, MSF head of mission in the DRC, said, ‘This time we are seeing not only mass displacement due to violence but also a rapidly spreading measles outbreak and an Ebola epidemic that shows no signs of slowing down, all at the same time.’”
NIPAH and Bats
Like Ebola, NIPAH is zoonotic, and also involves bats, but the viruses differ. CDC explains that, “Nipah virus (NiV) is a member of the family Paramyxoviridae, genus Henipavirus. NiV was initially isolated and identified in 1999 during an outbreak of encephalitis and respiratory illness among pig farmers and people with close contact with pigs in Malaysia and Singapore. Its name originated from Sungai Nipah, a village in the Malaysian Peninsula where pig farmers became ill with encephalitis.
A recent human outbreak in southern India has been followed up with a study of local bats. In a report shared by ProMED, out of 36 Pteropus species bats tested for Nipah, 12 (33%) were found to be positive for anti-Nipah bat IgG antibodies. Unlike Ebola there are currently no experimental drugs or vaccines.
Climate Change and Dengue
Climate change is expected to heighten the threat of many neglected tropical diseases, especially arboviral infections. For example, the New York Times reports that increases in the geographical spread of dengue fever. Annually “there are 100 million cases of dengue infections severe enough to cause symptoms, which may include fever, debilitating joint pain and internal bleeding,” and an estimated 10,000 deaths. Dengue is transmitted by Aedes mosquitoes that also spread Zika and chikungunya. A study, published Monday in the journal Nature Microbiology, found that in a warming world there is a strong likelihood for significant expansion of dengue in the southeastern United States, coastal areas of China and Japan, as well as to inland regions of Australia. “Globally, the study estimated that more than two billion additional people could be at risk for dengue in 2080 compared with 2015 under a warming scenario.”
Schistosomiasis – MDA Is Not Enough, and Neither Are Supplementary Interventions
Schistosomiasis is one of the five neglected tropical diseases (NTDs) that are being controlled and potentially eliminated through mass drug administration (MDA) of preventive chemotherapy (PCT), in this case praziquantel. In The Lancet Knopp et al. reported that biannual MDA substantially reduced Schistosomiasis haematobium prevalence and infection intensity but was insufficient to interrupt transmission in Zanzibar. In addition, neither supplementary snail control or behaviour change activities did not significantly boost the effect of MDA. Most MDA programs focus on school aged children, and so other groups in the community who have regular water contact would not be reached. Water and sanitation activities also have limitations. This raises the question about whether control is acceptable for public health, or if there needs to be a broader intervention to reach elimination?
Trachoma on the Way to Elimination
Speaking of elimination, WHO has announced major “sustained progress” on trachoma efforts. “The number of people at risk of trachoma – the world’s leading infectious cause of blindness – has fallen from 1.5 billion in 2002 to just over 142 million in 2019, a reduction of 91%.” Trachoma is another NTD that uses the MDA strategy.
The news about NTDs from Dengue to Schistosomiasis to Trachoma is complicated and demonstrates that putting diseases together in a category does not result in an easy choice of strategies. Do we control or eliminate or simply manage illness? Can our health systems handle the needs for disease elimination? Is the public ready to get on board?
Malaria Updates
And concerning being complicated, malaria this week again shows many facets of challenges ranging from how to recognize and deal with asymptomatic infection to preventing reintroduction of the disease once elimination has been achieved. Several reports this week showed the particular needs for malaria intervention ranging from high burden areas to low transmission verging on elimination to preventing re-introduction in areas declared free from the disease.
In South West, Nigeria Dokunmu et al. studied 535 individuals aged from 6 months were screened during the epidemiological survey evaluating asymptomatic transmission. Parasite prevalence was determined by histidine-rich protein II rapid detection kit (RDT) in healthy individuals. They found that, “malaria parasites were detected by RDT in 204 (38.1%) individuals. Asymptomatic infection was detected in 117 (57.3%) and symptomatic malaria confirmed in 87 individuals (42.6%).
Overall, detectable malaria by RDT was significantly higher in individuals with symptoms (87 of 197/44.2%), than asymptomatic persons (117 of 338/34.6%)., p = 0.02. In a sub-set of 75 isolates, 18(24%) and 14 (18.6%) individuals had Pfmdr1 86Y and 1246Y mutations. Presence of mutations on Pfmdr1 did not differ by group. It would be useful for future study to look at the effect of interventions such as bednet coverage. While Southwest Nigeria is a high burden area, the problem of asymptomatic malaria will become an even bigger challenge as prevalence reduces and elimination is in sight.
Sri Lanka provides a completely different challenge from high burden areas. There has been no local transmission of malaria in Sri Lanka for 6 years following elimination of the disease in 2012. Karunasena et al. report the first case of introduced vivax malaria in the country by diagnosing malaria based on microscopy and rapid diagnostic tests. “The imported vivax malaria case was detected in a foreign migrant followed by a Plasmodium vivax infection in a Sri Lankan national who visited the residence of the former. The link between the two cases was established by tracing the occurrence of events and by demonstrating genetic identity between the parasite isolates. Effective surveillance was conducted, and a prompt response was mounted by the Anti Malaria Campaign. No further transmission occurred as a result.”
Bangladesh has few but focused areas of malaria transmission and hopes to achieve elimination of local transmission by 2030. A particular group for targeting interventions is the population of slash and burn cultivators in the Rangamati District. Respondents in this area had general knowledge about malaria transmission and modes of prevention and treatment was good according to Saha and the other authors. “However, there were some gaps regarding knowledge about specific aspects of malaria transmission and in particular about the increased risk associated with their occupation. Despite a much-reduced incidence of malaria in the study area, the respondents perceived the disease as life-threatening and knew that it needs rapid attention from a health worker. Moreover, the specific services offered by the local community health workers for malaria diagnosis and treatment were highly appreciated. Finally, the use of insecticide-treated mosquito nets (ITN) was considered as important and this intervention was uniformly stated as the main malaria prevention method.”
Kenya offers some lessons about low transmission areas but also areas where transmission may increase due to climate change. A matched case–control study undertaken in the Western Kenya highlands. Essendi et al. recruited clinical malaria cases from health facilities and matched to asymptomatic individuals from the community who served as controls in order to identify epidemiological risk factors for clinical malaria infection in the highlands of Western Kenya.
“A greater percentage of people in the control group without malaria (64.6%) used insecticide-treated bed nets (ITNs) compared to the families of malaria cases (48.3%). Low income was the most important factor associated with higher malaria infections (adj. OR 4.70). Houses with open eaves was an important malaria risk factor (adj OR 1.72).” Other socio-demographic factors were examined. The authors stress the need to use local malaria epidemiology to more effectively targeted use of malaria control measures.
The key lesson arising from the forgoing studies and news is that disease control needs strong global partnerships but also local community investment and adaptation of strategies to community characteristics and culture.
Ramatsobane Johanna Ledwaba provides us with a guest blog to address the need to reach more school aged girls with vaccines for human papilloma (HPV) virus in South Africa and in the process prevent cervical cancer. Her blog originally appeared in Social, Cultural & Behavioral Issues in PHC & Global Health.
Cervical cancer is the first most common cancer in women and the first leading cancer related-deaths among South African women, aged 15-44 years. More that 12,000 women are diagnosed with cervical cancer annually, of which 5,500 die from cancer— age-specific incidence rate (15-44 years) of 41.8 per 100,000 women per year and age-specific mortality rate (15-44 years) of 11,7 per 100,000 women per year. Reasons for such a high mortality rate include, low screening coverage of 19.3%, and late presentation with an advanced stage compounded by the high HIV epidemic. The World Health Organization recommends a 2-dose HPV vaccination among girls of 9-13 years.
In 2014, the South African National Department of Health introduced a school-based HPV vaccination policy— using 2-dose Cervarix vaccine, as prevention for cervical cancer among girls aged 9 and above in grade 4 attending public schools. The policy aimed to vaccinate 500, 000 young girls from 18,000 public schools before their sexual debut.
HPV vaccine campaign poster distributed by the Department of Health. Source: Government Communication and Information SystemPreliminary data showed that 91% of schools were reached and 87% age eligible grade 4 girls were vaccinated, however there is a high dropout rate in the second dose.
Although the programme seems a success thus far, there is a need for expanded coverage of the vaccine to include higher grades that could potentially house girls of ages 11-13 years. In addition, the vaccine must be widely available at public health facilities for girls who were missed at school because they changed schools or dropped out.
Girls attending private schools are presumed to access HPV vaccine through the private health sector, however the HPV vaccine coverage in the private health sector remains low due to high costs and lack of awareness— which suggest that there is low coverage in private schools. Therefore, the vaccine must be expanded to include private schools. This gap may lead to poor coverage of HPV vaccination and may also increase perceptions or hesitancy against the vaccine because it is not widely available for all girls of targeted age. No girl must be left behind.
Sign up for daily or weekly articles from Bill highlighting the most noteworthy developments in newspapers and scientific journals. Click here to register.
 Out-of-hospital cardiac arrest (OHCA) is estimated to have an average global incidence of 55 adults per 100,000 person-years. However, despite advances in medical care and technology, survival to hospital discharge remains abysmally low at 8-10%. In low to middle income countries like Nigeria, where cardiovascular disease is rising but emergency response systems are poor, the rate of survival after OHCA is lower.
Out-of-hospital cardiac arrest (OHCA) is estimated to have an average global incidence of 55 adults per 100,000 person-years. However, despite advances in medical care and technology, survival to hospital discharge remains abysmally low at 8-10%. In low to middle income countries like Nigeria, where cardiovascular disease is rising but emergency response systems are poor, the rate of survival after OHCA is lower.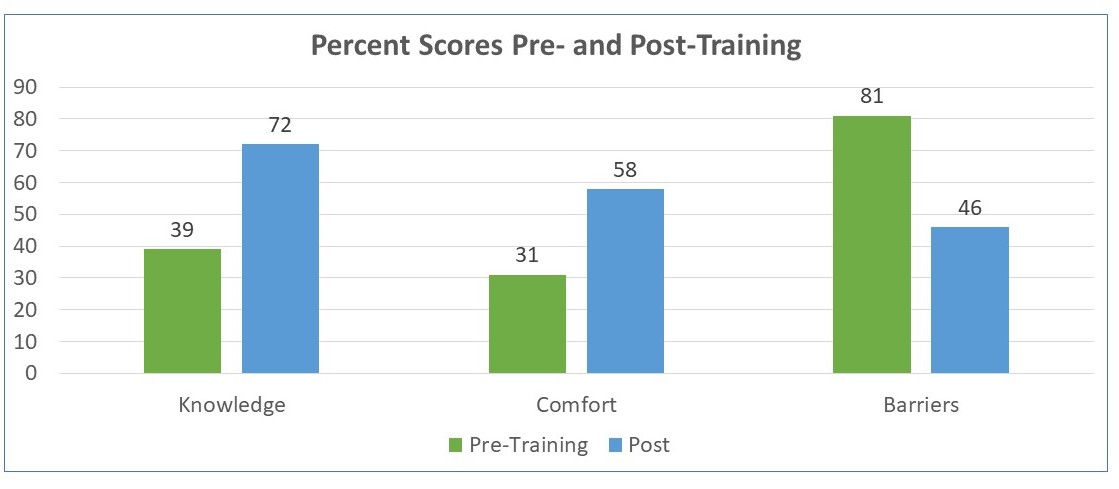 Interventions such as bystander cardiopulmonary resuscitation (CPR) training and automated external defibrillator (AED) use are effective, scalable, and low-cost interventions that can reduce the OHCA mortality. Training schoolchildren to perform Hands-only CPR has been shown to increase bystander CPR.
Interventions such as bystander cardiopulmonary resuscitation (CPR) training and automated external defibrillator (AED) use are effective, scalable, and low-cost interventions that can reduce the OHCA mortality. Training schoolchildren to perform Hands-only CPR has been shown to increase bystander CPR. The training had both in-person and virtual components due to COVID-19 travel restrictions on Atlanta based partners. Here we present the results of training on knowledge, comfort level and perceived barriers of performing hands-only CPR.
The training had both in-person and virtual components due to COVID-19 travel restrictions on Atlanta based partners. Here we present the results of training on knowledge, comfort level and perceived barriers of performing hands-only CPR. Trainees have started sharing what they learned through skits at school assemblies. Planning is underway to follow-up on training and to expand to other schools and states.
Trainees have started sharing what they learned through skits at school assemblies. Planning is underway to follow-up on training and to expand to other schools and states.

 This is already disrupting behaviors, leading older generations to seek proper care and follow proper mitigation efforts to combat malaria. If these programs were to expand to other regions in Uganda, within even a generation, there would be a significant decline in malaria cases because of the knowledge learned and passed on by these children. The Malaria Smart School program is one many countries should model in their national malaria control programs, and with outside support from partnering organizations like PMI, this model could really impact the global burden of malaria.
This is already disrupting behaviors, leading older generations to seek proper care and follow proper mitigation efforts to combat malaria. If these programs were to expand to other regions in Uganda, within even a generation, there would be a significant decline in malaria cases because of the knowledge learned and passed on by these children. The Malaria Smart School program is one many countries should model in their national malaria control programs, and with outside support from partnering organizations like PMI, this model could really impact the global burden of malaria.
 Molecular prevalence of asymptomatic Plasmodium infection was 284/391 (73%); only 126 (32%) infections were detected by RDT. While 266 (68%) participants were infected with Plasmodium falciparum, 33 (8%) were infected with Plasmodium malariae and 34 (9%) with P. ovale. The sub-species P. ovale curtisi and P. ovale wallikeri were identified to similar proportions. Non-falciparum infections usually presented as mixed infections with P. falciparum.
Molecular prevalence of asymptomatic Plasmodium infection was 284/391 (73%); only 126 (32%) infections were detected by RDT. While 266 (68%) participants were infected with Plasmodium falciparum, 33 (8%) were infected with Plasmodium malariae and 34 (9%) with P. ovale. The sub-species P. ovale curtisi and P. ovale wallikeri were identified to similar proportions. Non-falciparum infections usually presented as mixed infections with P. falciparum.