Ivermectin &Larvicide &MDA &Vaccine &Zero Malaria Bill Brieger | 25 Apr 2019
Zero Malaria Starts with Universal Coverage: Part 3 Innovations and New Interventions
Newer malaria interventions are coming on board, and whether these will be used of a large scale or targeted to certain epidemiological contexts remains to be seen. In each case, one will need to examine if in each context one can measure whether the intervention is universally accessible to and used by the intended population or subgroup.
 After 30 years of research and testing, a malaria vaccine is ready to go through implementation testing in Malawi, Ghana and Kenya. This pilot of the vaccine, known as RTS,S, will be made available to children up to 2 years of age with the Malawi launching first during the week of World Malaria Day.
After 30 years of research and testing, a malaria vaccine is ready to go through implementation testing in Malawi, Ghana and Kenya. This pilot of the vaccine, known as RTS,S, will be made available to children up to 2 years of age with the Malawi launching first during the week of World Malaria Day.
WHO explains that, “The malaria vaccine pilot aims to reach about 360,000 children per year across the three countries. Ministries of health will determine where the vaccine will be given; they will focus on areas with moderate-to-high malaria transmission, where the vaccine can have the greatest impact.” There will be a strong monitoring component to identify coverage levels as well as any implementation challenges and adverse effects that may only become visible in a larger scale intervention that the typical efficacy trials. Implementation is occurring in areas with a relatively strong existing malaria control effort, with an intent to learn how a vaccine can complement a total control package.
 Mass Drug Administration (MDA, also known as preventive chemotherapy) has been a successful strategy for controlling and eliminating neglected tropical diseases with special reference to onchocerciasis, lymphatic filariasis, trachoma, soil transmitted helminths and schistosomiasis. MDA use in malaria has been limited due to a number of financial and logistical challenges, not the least of which is the need to achieve high coverage over several periods of distribution. This is why WHO recommends, “Use of MDA for the elimination of P. falciparum malaria can be considered in areas approaching interruption of transmission where there is good access to treatment, effective implementation of vector control and surveillance, and a minimal risk of re-introduction of infection.”
Mass Drug Administration (MDA, also known as preventive chemotherapy) has been a successful strategy for controlling and eliminating neglected tropical diseases with special reference to onchocerciasis, lymphatic filariasis, trachoma, soil transmitted helminths and schistosomiasis. MDA use in malaria has been limited due to a number of financial and logistical challenges, not the least of which is the need to achieve high coverage over several periods of distribution. This is why WHO recommends, “Use of MDA for the elimination of P. falciparum malaria can be considered in areas approaching interruption of transmission where there is good access to treatment, effective implementation of vector control and surveillance, and a minimal risk of re-introduction of infection.”
Another link with MDA for a different disease, onchocerciasis, has pointed to a potential new malaria intervention. Around ten years ago it was observed that after ivermectin treatment for onchocerciasis in Senegal survivorship of malaria vectors was reduced. Subsequently the potential effect of ivermectin has been intentionally researched with the outcome that, “Frequently repeated mass administrations of ivermectin during the malaria transmission season can reduce malaria episodes among children without significantly increasing harms in the populace.” Mathematical models for onchocerciasis control have predicted the need to achieve annual coverage targets below what could be called universal levels. Using ivermectin for mosquito control would require more frequent dosing and higher coverage.
Although not defined as ‘new’ it is important to include mention of additional vector interventions like larviciding and indoor residual spraying, as these present technical and coverage challenges. For example, larviciding interventions either chemical or biological, do not cover individuals. These focus on breeding sites in communities. This may require better use of the concept of geographical coverage as has been used in onchocerciasis control wherein the proportion of endemic villages reached is monitored.
For example, in Mali the NTD program aimed to achieve 80% program coverage of individuals eligible for preventive chemotherapy and 100% geographical coverage yearly. This means all villages should be reached. In reality, the program achieved 85% geographical coverage for lymphatic filariasis and over 90% for onchocerciasis.
In conclusion, we have seen that defining as well as achieving universal coverage of malaria interventions is a challenging prospect. For example, do we base our monitoring on households, villages, or populations? Do we have the funds and technical capacity to implement and sustain the level of coverage required to have an impact on malaria transmission and move toward elimination? Are we able to introduce new, complimentary and appropriate interventions as a country moves closer to elimination?
Asymptomatic &Case Management &Diagnosis &Elimination &Ivermectin &Surveillance &Uncategorized Bill Brieger | 30 Jan 2019
Asymptomatic Malaria – we need to eliminate what we can’t see
After the World’s first attempt at eradicating the complicated disease malaria mainly through a single tool, a period of control set in where the aim was to reduce mortality through prompt and presumptive treatment of fevers with anti-malarials, particularly in young children. During this period in the 1980s and 1990s it was recognized that parasite-based diagnostic capabilities in the form of microscopy were limited, so in malaria endemic areas, it was worth providing inexpensive medicines like chloroquine (CQ) and sulfadoxine-pyrimethamine (SP) to febrile children in order to save lives. When the fevers did not resolve, other illnesses explored.
The difficulty arose in identifying cases that did not offer clinical clues that they might be malaria. Today countries approaching malaria elimination face challenges, such as seen in Zanzibar where, “outdoor transmission, a large asymptomatic parasite reservoir and imported infections, require novel tools and reoriented strategies to prevent a rebound effect and achieve elimination.”[i] Here we examine the challenge of asymptomatic malaria infections.

Background
By 1998 when the Roll Back Malaria partnership formed, there had been enough research done so that the malaria community had a better arsenal of interventions including insecticide-treated bed nets, artemisinin-based combination therapy (ACT) and intermittent preventive treatment with SP during pregnancy. The Abuja Declaration of 2000 set a target of 80% coverage of these interventions by the year 2010.
While ACTs overcame the challenges of parasite resistance that had developed for the single drugs, CQ and SP, it cost several times more than those medicines. The need for easy-to-use, inexpensive, point-of-care diagnostics was recognized so that not only would ACTs be targeted only to parasitologically confirmed malaria cases, but also in the process, overuse and misuse would not contribute to parasite resistance of these new drugs.[ii] Unfortunately, the development and dissemination of antigen-based rapid diagnostic tests (RDTs), lagged behind the availability of ACTs meaning that health workers unfortunately continued their business as usual with presumptive treatment using ACTs.
The benefits of RDTs were generally two-fold. First, they could be used by front-line, auxiliary and community-based health workers. Secondly, they tended to identify more cases than microscopy. The big challenge was convincing health workers to use them and trust the results, because the era of presumptive treatment had given these staff a false sense of confidence in their own clinical diagnostic abilities.

Although reaching the 2010 coverage targets has remained illusive for most endemic countries, there has been enough progress for major reductions in incidence (despite a recent upsurge).[iii] As the proportion of actual malaria cases among febrile illness patients declines, concern has risen that transmission might continue among people with subclinical or asymptomatic malaria. Here we explore the extent of this problem and new directions in parasitological testing needed to ensure continued progress toward elimination in each endemic country.
Understanding the Risk of Asymptomatic Malaria
Risk can relate to geographical, epidemiological, and socio-demographic factors as well as history of malaria interventions. Kenya has stratified the country by higher and lower malaria transmission areas. Even the higher areas are comparatively low compared to its higher transmission neighbors. Studying the prevalence of asymptomatic malaria in some of these higher transmission areas in the west of the country was seen as a way to better identify people at risk and learn about intervention effectiveness. An examination of apparently healthy children (no symptoms) revealed a Plasmodium falciparum malaria prevalence 36.0% (27.5%, 44.5%) by RDT and 22.3% (16.0%, 28.6%) by thick film microscopy.[iv] Living in a household with electricity was protective but the adjusted odds ratio of prevalence comparing households with and without indoor residual spray showed only borderline benefit. Unfortunately, in Zanzibar, asymptomatic malaria infection was not associated “with use of any vector control.”1
A major challenge in detecting cases through routine health care systems is care seeking patterns of care seeking for fever. The 2018 World Malaria Report acknowledges that there are major equity challenges in care seeking wherein families with higher incomes, better education and living in urban areas are more likely to seek help for their febrile children that rural, poor and less educated families who would be more at risk. Care seeking without the signs of fever is more challenging. A dual strategy of enabling better service utilization as well as outreach to detect cases will be necessary to detect asymptomatic cases.3
In Burkina Faso, the prevalence of asymptomatic malaria infection in children under 5 years of age was estimated at 38.2% in 24 of its 70 health districts. Those at most risk for asymptomatic malaria infection included the following:[v]
- older children (48–59 vs < 6 months: OR: 6.79 [5.62, 8.22])
- children from very poor households (Richest vs poorest: OR: 0.85 [0.74–0.96])
- households located more than 5 km from a health facility (< 5 km vs ? 5 km: OR: 1.14 [1.04–1.25])
- localities with inadequate number of nurses (< 3 vs ? 3: 0.72 [0.62, 0.82]
- rural areas (OR: 1.67 [1.39–2.01])
Nine districts reported significantly higher risks (Batié, Boromo, Dano, Diébougou, Gaoua, Ouahigouya, Ouargaye, Sapouy and Toma. The researchers concluded that, “Such national spatial analysis should help to prioritize areas for increased malaria control activities.”
A study in Ghana found that, “children and pregnant women had higher prevalence of submicroscopic gametocytes (39.5% and 29.7%, respectively) compared to adults
(17.4%).”[vi]

An additional concern is emerging in terms of sharing of malaria parasite species between humans and primates, especially as urbanization and deforestation push these two populations into closer contact. For example Mapua and colleagues working in Central Africa Republic, “found the human malaria parasite P. ovale wallikeri in both asymptomatic humans and western lowland gorillas in Dzanga Sangha Protected Areas. Molecular analysis revealed that the genotype of the P. ovale wallikeri DNA found in a gorilla was genetically identical to that of a human isolate within the mt cytb and mt cox 1 genes, indicating potential human–ape transmission.”[vii] They noted similar sharing of parasites in the region between humans and chimpanzees.
Detecting and Responding to Asymptomatic Cases
WHO’s Framework for Malaria Elimination[viii] recognizes the important role of case detection and subsequent treatment as well as broader community level preventive responses around detected cases. In the context of elimination WHO notes that case detection “requires use of a diagnostic test to identify asymptomatic malaria infections.” WHO stresses that a case is a case, regardless of whether it is symptomatic or asymptomatic, as long as the diagnostic process confirms presence of malaria infection.
It is important to monitor Plasmodium parasitemia in areas where malaria transmission has declined and efforts to achieve malaria elimination are underway, such as Zambia, where 3,863 household members were tested.[ix] Only 2.6% were positive by either microscopy, RDT, or PCR. Of these, 48 (47%) had subpatent parasitemia, and 85% of those with subpatent parasitemia were asymptomatic. “Compared with individuals without parasitemia, individuals with subpatent parasitemia were significantly more likely to be aged 5–25 years.” The authors suggested that their findings pointed to the need for active or reactive case detection to identify asymptomatic individuals and thus better target individuals with subpatent parasitemia with appropriate malaria interventions.
WHO explains that active case detection (ACD) takes place in areas of limited or under-utilization of health care services.4 It may start with initial screening for symptoms, followed by appropriate parasitological laboratory confirmation. In low-transmission settings or as part of a focus investigation, “ACD may consist of testing of a defined population group without prior symptom screening (population-wide or mass testing) in order to identify asymptomatic infections.” Elimination cannot be achieved until even asymptomatic infections have stopped. The challenge is the expense of community-wide screening.
Reactive Case Detection (RCD), according to WHO, takes place in settings low transmission intensity where the few “occurring malaria cases are highly aggregated.”4 When a case is identified, usually through identification of an actual infected patient at a local clinic, the community where the patient comes from is visited and a “net is cast around the index case” where household members and neighbors within a selected radius are tested. In this process asymptomatic cases are also identified.

Our existing diagnostic tools may be inadequate. McCreesh and colleagues reported on subpatent malaria in Namibia that, “fever history and standard RDTs are not useful to address this burden. Achievement of malaria elimination may require active case detection using more sensitive point-of-care diagnostics or presumptive treatment and targeted to high-risk groups.” This includes loop-mediated isothermal amplification (LAMP) using dried blood spots, which they tested.[x] Likewise from experience in a Zambian study, Kobayashi and co-researchers suggest, “more sensitive diagnostic tests or focal drug administration may be necessary to target individuals with subpatent parasitemia to achieve malaria elimination.”[xi]
Responses to detecting asymptomatic cases start at the individual level with prompt treatment of those found through RCD to be infected. Then focused preventive interventions such as distribution of insecticide treated bednets can be provided to those in the cluster or village. Follow-up would be needed for such ‘hot spots.’

On a broader basis we have Seasonal Malaria Chemoprevention (SMC) as practiced in Sahelian countries where during the peak transmission (rainy) season intermittent preventive treatment is given to children monthly by community health workers and volunteers. Of course, many of these children would be asymptomatic carriers and SMC could benefit the reduction of parasites in circulation. At present SMC focuses on pre-school aged children, but Thera and co-researchers stress the importance of reaching school aged children who are also often asymptomatic carriers.[xii]
Another intervention being tested for mass drug administration (MDA) use providing the community with ivermectin, a drug that has been highly effective in controlling filarial diseases and also found to kill mosquitoes who take a blood meal from a person who has recently taken it.[xiii] This strategy is still being tested, but again MDA means all community members, especially those with asymptomatic infection, would be reached.
A major question requires further research. To what extent
do asymptomatic, submicroscopic and subpatent parasitemia contribute to
continued malaria transmission? Another question is how can we address malaria
infection in other primates? We know that scientists recommend targeting of
malaria elimination interventions based on mapping of these infections.5
We therefore need to study the actual transmission potential of this
phenomenon.
[i] Björkman A, Shakely D, Ali AS, Morris U, Mkali H, Abbas AK, Al-Mafazy A-W, Haji KA, Mcha J, Omar R, Cook J, Elfving K, Petzold M, Sachs MC, Aydin-Schmidt B, Drakeley V, Msellem M and Mårtensson A. From high to low malaria transmission in Zanzibar—challenges and opportunities to achieve elimination. BMC Medicine (2019) 17:14, https://doi.org/10.1186/s12916-018-1243-z
[ii] Global Malaria Programme. Universal access to malaria diagnostic testing – An operational manual. World Health Organization. November 2011 (rev. February 2013). https://www.who.int/malaria/publications/atoz/9789241502092/en/
[iii] Global Malaria Programme. World malaria report 2018. World Health Organization. 19 November 2018. https://www.who.int/malaria/publications/world-malaria-report-2018/en/
[iv] Peprah S, Tenge C, Genga IO, Mumia M, Were PA, Kuremu RT, Wekes WN, Sumba PO, Kinyera T, Otim T, Legason ID, Biddle J, Reynolds SJ, Talisuna AO, Biggar1 RJ, Bhatia K, Goedert JJ, Pfeiffer RM, Mbulaiteye SM. A Cross-Sectional Population Study of Geographic, Age-Specific, and Household Risk Factors for Asymptomatic Plasmodium falciparum Malaria Infection in Western Kenya. The American Journal of Tropical Medicine and Hygiene, Volume 100, Issue 1, Jan 2019, p.54-65. DOI: https://doi.org/10.4269/ajtmh.18-0481.
[v] Ouédraogo M, Samadoulougou S, Rouamba T, Hien H, Sawadogo JEM Tinto H, Alegana VA, Speybroeck N and Kirakoya?Samadoulougou F. Spatial distribution and determinants of asymptomatic malaria risk among children under 5 years in 24 districts in Burkina Faso. Malaria Journal 2018; 17:460 https://doi.org/10.1186/s12936-018-2606-9
[vi] Lamptey H, Ofori MF, Kusi KA, Adu B, Owusu-Yeboa E, Kyei-Baafour E, Arku AT, Bosomprah S, Alifrangis M, Quakyi IA. The prevalence of submicroscopic Plasmodium falciparum gametocyte carriage and multiplicity of infection in children, pregnant women and adults in a low malaria transmission area in Southern Ghana. Malar J. 2018 Sep 17;17(1):331. doi: 10.1186/s12936-018-2479-y.
[vii] Mapua MI, Hans-Peter Fuehrer HP, Petrželková KJ, Todd A, Noedl H, Qablan MA, and Modrý D. Plasmodium ovale wallikeri in Western Lowland Gorillas and Humans Central African Republic. Emerging Infectious Disease journal. Volume 24, Number 8—August 2018. https://wwwnc.cdc.gov/eid/article/24/8/18-0010_article
[viii] Global Malaria Programme. A framework for malaria elimination. ISBN 978-92-4-151198-8. World Health Organization 2017, http://www.who.int/malaria/publications/atoz/9789241511988/en/
[ix] Kobayashi T, Kanyangarara M, Laban NM, Phiri M, Hamapumbu H, Searle KM, Stevenson JC, Thuma PE, Moss WJ and the Southern Africa International Centers of Excellence for Malaria Research. Characteristics of Subpatent Malaria in a Pre-Elimination Setting in Southern Zambia. The American Journal of Tropical Medicine and Hygiene, 10 December 2018, DOI: https://doi.org/10.4269/ajtmh.18-0399
[x] McCreesh P, Mumbengegwi D, Roberts K, Tambo M, Smith J, Whittemore B, Kelly G, Moe C, Murphy M, Chisenga M, Greenhouse B, Ntuku H, Kleinschmidt I, Sturrock H, Uusiku P, Gosling R, Bennett A, Hsiang MS. Subpatent malaria in a low transmission African setting: a cross-sectional study using rapid diagnostic testing (RDT) and loop-mediated isothermal amplification (LAMP) from Zambezi region, Namibia. Malar J. 2018 Dec 19;17(1):480. doi: 10.1186/s12936-018-2626-5.
[xi] Kobayashi T, Kanyangarara M, Laban NM, Phiri M, Hamapumbu H, Searle KM, Stevenson JC, Thuma PE, Moss WJ, For The Southern Africa International Centers Of Excellence For Malaria Research.Characteristics of Subpatent Malaria in a Pre-Elimination Setting in Southern Zambia. Am J Trop Med Hyg. 2018 Dec 10. doi: 10.4269/ajtmh.18-0399. [Epub ahead of print]
[xii] Thera MA, Konea AK, Tangaraa B, Diarraa E, Niarea A, Dembeleb A, Sissokoa MS, Doumboa OK. School-aged children based seasonal malaria chemoprevention using artesunate-amodiaquine in Mali. Parasite Epidemiology and Control 3 (2018) 96–105. https://doi.org/10.1016/j.parepi.2018.02.001
[xiii] Smit MR, Ochomo EO, Aljayyoussi G, Kwambai TK, Abong’o BO, Chen T, Bousema T, Slater HC, Waterhouse D, Bayoh NM, Gimnig JE, Samuels AM, Desai MR, Phillips-Howard PA, Kariuki SK, Wang D, Ward SA, ter Kuile FO. Safety and mosquitocidal efficacy of high-dose ivermectin when co-administered with dihydroartemisinin-piperaquine. www.thelancet.com/infection Published online March 27, 2018 http://dx.doi.org/10.1016/S1473-3099(18)30163-4
CHW &Community &ITNs &Ivermectin &Mapping &MDA &Seasonal Malaria Chemoprevention Bill Brieger | 04 Jul 2018
Mapping to Integrate Filariasis and Onchocerciasis Control with Malaria Interventions
 William R Brieger (wbriege1@jhu.edu) and Gilbert Burnham (gburnha1@jhu.edu) of The Johns Hopkins Bloomberg School of Public Health, Department of International Health presented ideas about mapping and integration of neglected tropical diseases and malaria interventions at the Malaria World Congress, Melbourne, Australia, July 2018
William R Brieger (wbriege1@jhu.edu) and Gilbert Burnham (gburnha1@jhu.edu) of The Johns Hopkins Bloomberg School of Public Health, Department of International Health presented ideas about mapping and integration of neglected tropical diseases and malaria interventions at the Malaria World Congress, Melbourne, Australia, July 2018
Overview: Lymphatic Filariasis (LF) and Malaria share a common vector in sub-Saharan Africa. Mass Drug Administration (MDA) is a strategy that is common to both diseases. Where the diseases overlap there is the potential opportunity to coordinate both vector control and MDA to achieve synergy in program results. The example of Burkina Faso, supplemented with information from Ghana, serves as an example of what could be integrated and what actually happens.
 Background: Thirty years ago then veterinary drug, ivermectin, was found effective in controlling neglected tropical diseases (NTDs), specifically two human filarial diseases: onchocerciasis and lymphatic filariasis (LF). The drug manufacturer donates 300 million treatments annually to eliminate both diseases. Since then, annual community based mass drug administration (MDA) efforts have resulted in millions of treatments in endemic countries and great progress has been made toward elimination of transmission. Through observation and experimentation, ivermectin was found to kill malaria carrying mosquitoes when they bite people who have taken ivermectin making it a useful tool for vector control.
Background: Thirty years ago then veterinary drug, ivermectin, was found effective in controlling neglected tropical diseases (NTDs), specifically two human filarial diseases: onchocerciasis and lymphatic filariasis (LF). The drug manufacturer donates 300 million treatments annually to eliminate both diseases. Since then, annual community based mass drug administration (MDA) efforts have resulted in millions of treatments in endemic countries and great progress has been made toward elimination of transmission. Through observation and experimentation, ivermectin was found to kill malaria carrying mosquitoes when they bite people who have taken ivermectin making it a useful tool for vector control.

CHWs in Burkina Faso demonstrating how to measure height to determine ivermectin dosage
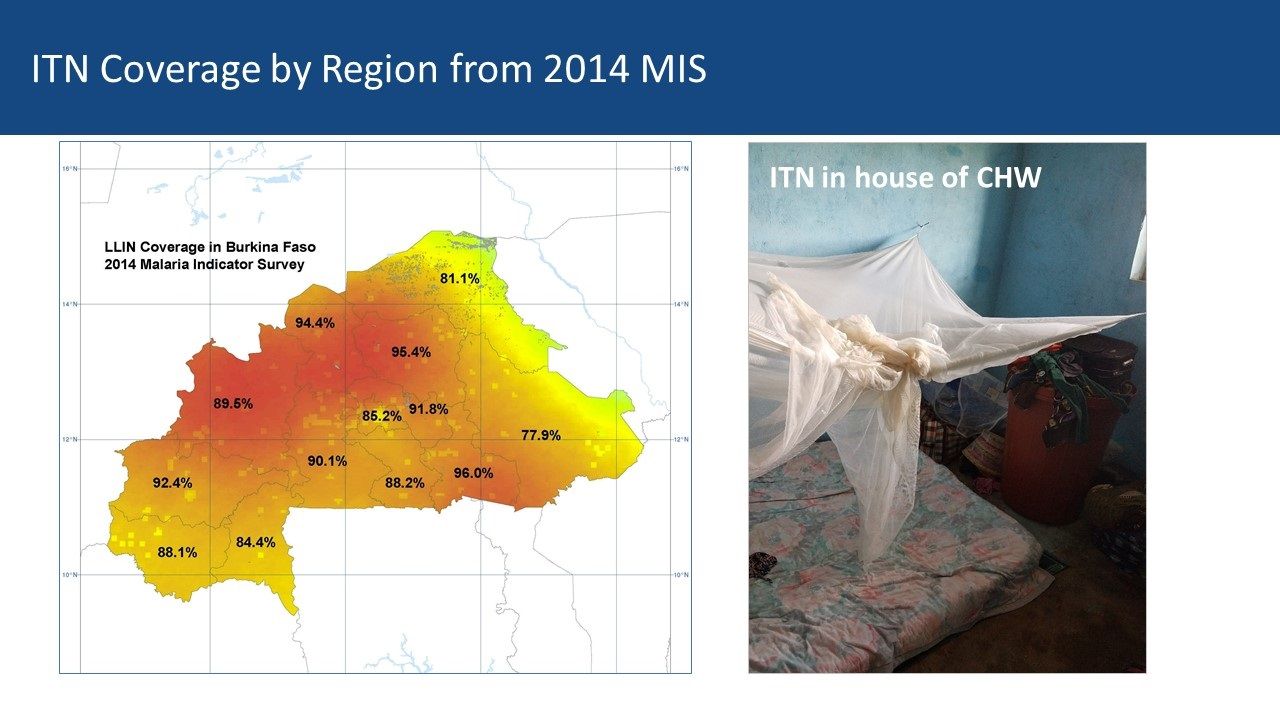
Community Health Workers’ Role: Current research is examining how dosing and timing of treatments may impact national malaria vector control efforts. Comparing maps between malaria and LF can be a starting point for adapting ivermectin MDAs for malaria vector control. Burkina Faso MDAs are operationalized by community health workers (CHWs) who are part of a national program that provides treatment for common illnesses and also conducts village level onchocerciasis and LF MDAs. Vector Control with Long Lasting Insecticide Treated Nets In most of rural Africa, malaria and lymphatic Filariasis are co-endemic and share the same anopheles mosquito vector.
However, that does not mean that there is a coordinated effort to plan distribution of LLINs despite the fact that the intervention meets the needs of both disease control efforts. The current NTD programs in Burkina Faso and Ghana focus on Preventive Chemotherapy (PCT) delivered through Mass Drug Administration (MDA). Vector Control is seen as essential in areas co-endemic with LF, Loa loa and Malaria – mapping helps identify priority areas for vector control.
 Vector Control by Chance: In Ghana, the NTD/LF elimination program was unaware of the LLIN coverage data available in the NMCP housed in an adjacent building. This illustrates the lack of collaboration between the two programs. Thus where — and if — vector control benefits the reduction of both diseases, it is often by chance where LF is concerned. The International NGO, The Carter Center, may be the only one that includes vector control as part of its programming for both malaria and LF in Nigeria. This practice should be replicated by other partners and country programs where possible.
Vector Control by Chance: In Ghana, the NTD/LF elimination program was unaware of the LLIN coverage data available in the NMCP housed in an adjacent building. This illustrates the lack of collaboration between the two programs. Thus where — and if — vector control benefits the reduction of both diseases, it is often by chance where LF is concerned. The International NGO, The Carter Center, may be the only one that includes vector control as part of its programming for both malaria and LF in Nigeria. This practice should be replicated by other partners and country programs where possible.
 Mass Drug Administration: MDA is the major strategy for control of five PCT diseases in the NTD program, and LF is one of those. Currently MDA anti-malarial drugs has been considered in limited situations in countries where there are areas that have very low transmission In the future countries may consider research that shows mosquitocidal effects of Onchocerciasis and LF MDAs with ivermectin. Otherwise for malaria, a special intervention called Seasonal Malaria Chemoprevention (SMC) is used in an MDA-like approach to reach young children in the African Sahel during high transmission months. In both cases, existing cadres of (usually volunteer) community health workers are the front line providers of MDA.
Mass Drug Administration: MDA is the major strategy for control of five PCT diseases in the NTD program, and LF is one of those. Currently MDA anti-malarial drugs has been considered in limited situations in countries where there are areas that have very low transmission In the future countries may consider research that shows mosquitocidal effects of Onchocerciasis and LF MDAs with ivermectin. Otherwise for malaria, a special intervention called Seasonal Malaria Chemoprevention (SMC) is used in an MDA-like approach to reach young children in the African Sahel during high transmission months. In both cases, existing cadres of (usually volunteer) community health workers are the front line providers of MDA.
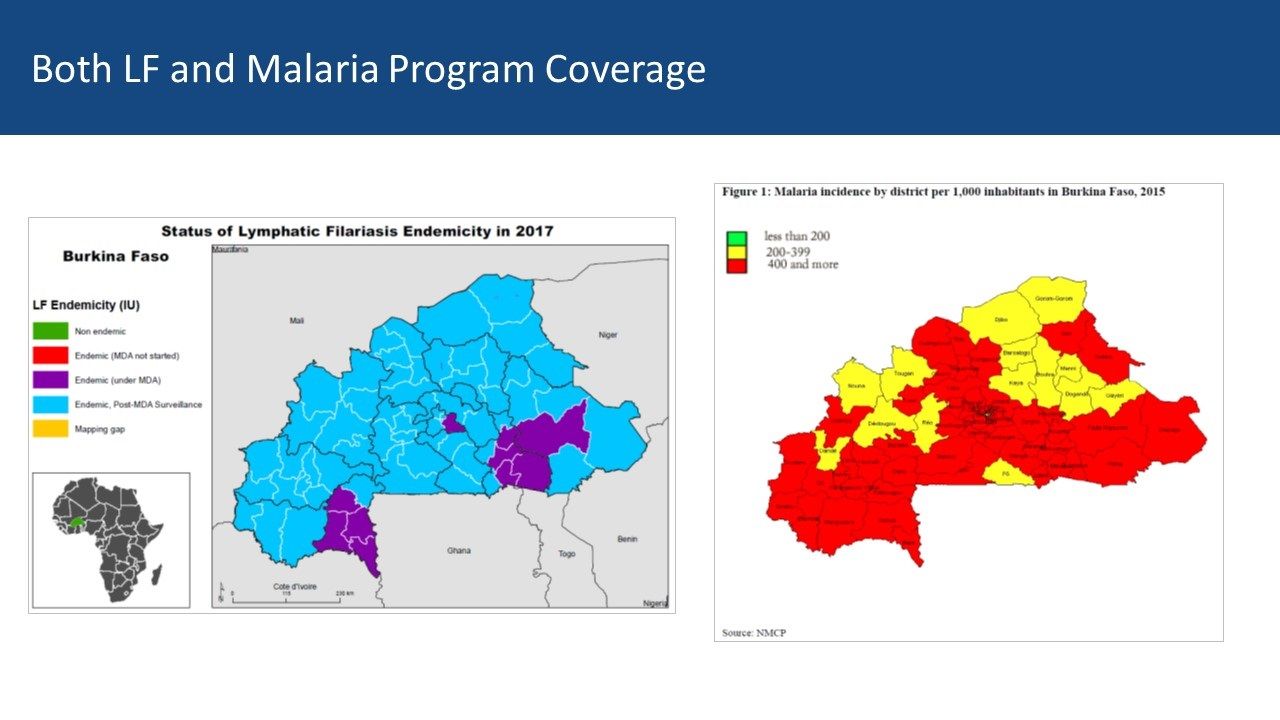
Burkina Faso LF Map from ESPEN: Mapping shows 10 of 70 health districts are currently doing LF MDA, though all have done it. Thus CHWs in all districts are experienced in ivermectin MDA. The malaria map shows that two-thirds of districts have a malaria incidence of 400/1000 or more while 14 have lower incidence. There is an overlap between current LF MDA districts and higher incidence malaria districts Both LF and Malaria Program Coverage can be seen to overlap in [program maps.

Ghana CHWs explain how they conduct MDA
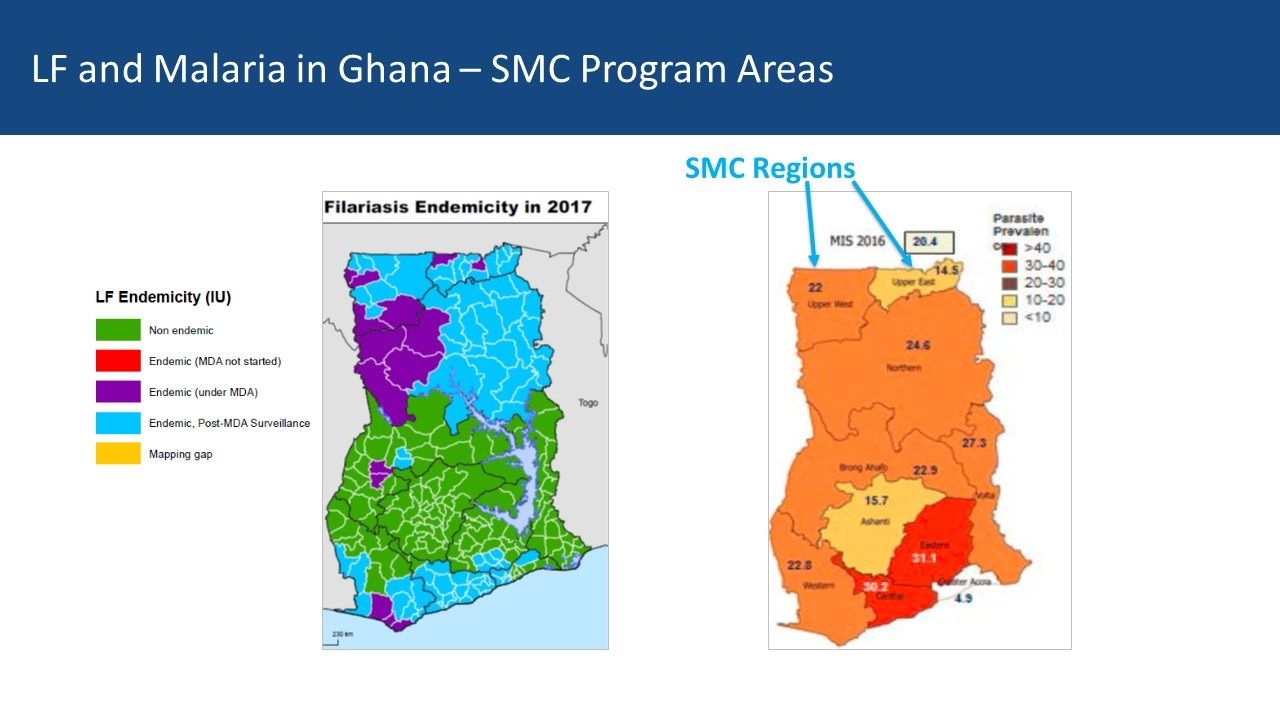
Ghana Experiences: Ghana provides a contrasting example. There five regions in central Ghana that are mostly non-endemic for LF but do have moderate malaria transmission In the south two regions with former LF MDA activity overlap with higher malaria endemicity While four northern regions have lower malaria parasite prevalence, they do have current and recent LF MDAs Community Directed Distributors work with LF MDA in Ghana
Conclusions: Malaria elimination will need a mix of strategies to be successful. Therefore, it is not too early for malaria and NTD program managers, as well as their respective donors, to begin comparing maps to identify possibilities for adapting ivermectin MDAs for malaria vector control. Even though one endemic disease is nearing control or elimination, the infrastructure put in place to accomplish this can be mobilized for other disease control efforts – as long as we map where interventions and resources have been targeted.
Elimination &Ivermectin &MDA &NTDs &Procurement Supply Management Bill Brieger | 16 Jun 2018
Many Neglected Tropical Diseases: What About Eliminating Them?

Testing to see if transmission of lymphatic filariasis has stopped in Burkina Faso
Two things we need to note about the list of 20 diseases that the World Health Organization and partners classify as Neglected Tropical Diseases (NTDs). First, diseases like Rabies, Snakebite/envenoming, and Leprosy, while certainly more common in the tropics now, have in the past been global in distribution. Secondly some of the diseases have not been neglected. Onchocerciasis or river blindness has been the focus of a global partnership since 1975, and transmission in the America’s and much of the Sahel in Africa has been halted. Elimination of Dracunculiasis or Guinea Worm has also been the subject of many World Health Assembly Resolutions, and concerted effort has brought the number of cases down from 3.5 million in 1986 to 30 in 2017. What is more to the point about these diseases is that they affect neglected people, the poor and vulnerable in remote rural areas or urban slums.
Still when we can compare NTD control programs with the rise of major disease control efforts like the Global Fund to fight AIDS, Tuberculosis and Malaria, the President’s Emergency Program For AIDS Relief, the President’s Malaria Initiative, World Bank Malaria Booster Program, Global A Vaccine Initiative among others, we can see that the global community has been able to focus major financial resources on a few diseases. Now with the Sustainable Development Goals, that focus expanded from infectious to Non-Communicable Diseases. It is natural therefore to fear that tropical health problems that are responsible for major loss of life and economic capacity will not be adequately addressed.

A system of rewards helped identify the last cases in many guinea worm endemic countries
Based on the World Health Organization’s 2020 Roadmap on NTDs, the London Declaration on NTDs recognized a “tremendous opportunity to control or eliminate at least 10 of these devastating diseases by the end of the decade” (i.e. by 2020). These include eradication of Guinea worm disease, and elimination by 2020 of lymphatic filariasis (LF), leprosy, sleeping sickness {human African trypanosomiasis) and blinding trachoma. In addition drug access programmes should help control by 2020 schistosomiasis, soil-transmitted helminthes (STH), Chagas disease, visceral leishmaniasis and river blindness (onchocerciasis).
Five of the diseases are notable in that they can either be controlled or eliminated through Mass Drug Administration (MDA) using Preventive Chemo-Therapy (PCT). This effort is aided by drug donation programs at the global level and community based MDA at the local level. Ten companies were signatories to the London Declaration and contributed to drug donation programs to achieve MDA. According to WHO,
Preventive chemotherapy is aimed at optimizing the largescale use of safe, single-dose medicines and offers the best means of reducing the extensive morbidity associated with four helminthiases (lymphatic filariasis, onchocerciasis, schistosomiasis and soil-transmitted helminthiases) (6). Additionally, the large-scale administration of azithromycin – a key component of the SAFE strategy for trachoma (that is, lid surgery (S), antibiotics to treat the community pool of infection (A), facial cleanliness (C) and environmental improvement (E)) – is amenable to close coordination and, in future, possibly co-administration with interventions targeted at helminthiases.

Community health workers are the cornerstone of many NTD elimination programs
Targets for the 5 PCT diseases vary. The aim is to eliminate LF and Trachoma by 2020. Although the efforts against onchocerciasis have been running the longest, the refocus from control to elimination meant increasing the geographical scope of intervention, and now elimination may not be feasible until 2025. With a focus mainly on the school aged and based populations, programs against schistosomiasis and STH talk of control, not elimination, although some endemic countries hope that elimination may be possible if the focus of these programs expands. So far, Togo is the only Sub-Saharan African country to have eliminated LF, and Ghana to have eliminated Trachoma.
Partnerships, funding and drug donations need to be strengthened if more countries are to join the ranks of Togo and Nepal.
Diagnosis &Elimination &Ivermectin &MDA &Treatment Bill Brieger | 20 Nov 2016
Leadership and Support for Malaria Pre-Elimination in Nepal
Emmanuel Le Perru, Jhpiego field staff in Nepal, shared his experiences in aiding the malaria pre-elimination efforts in the country during a retreat that preceded the 65th Annual Meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. Here are some highlights of his talk.
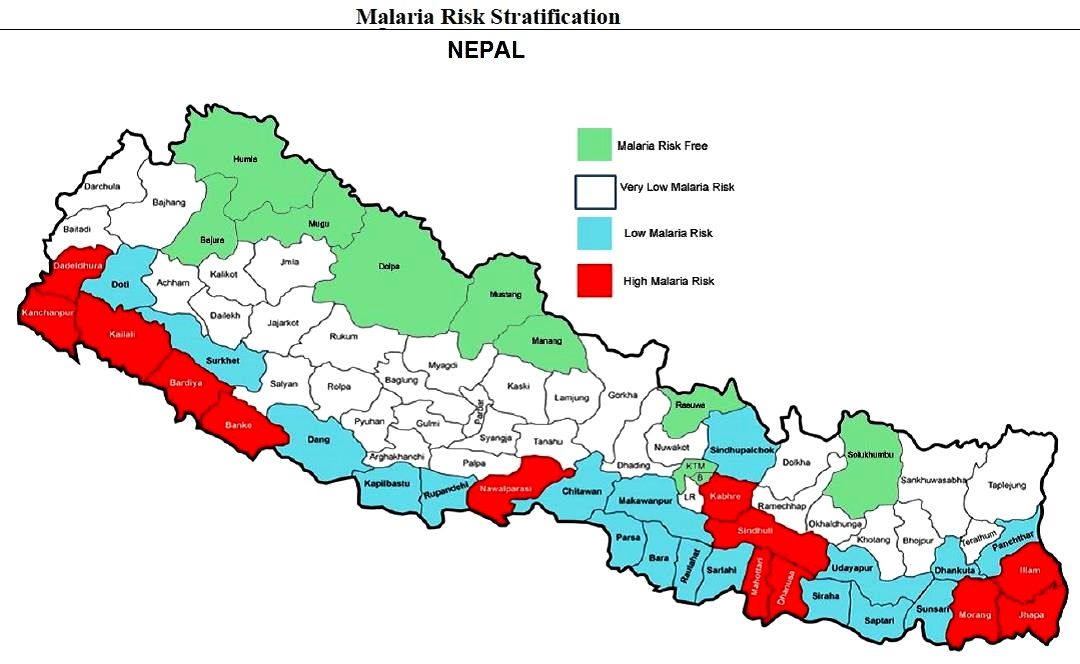 Malaria Pre-Elimination efforts are targeting 0 deaths as well as investigation of 100% of confirmed cases in Nepal. Systematic entomology investigation/interventions are required. Glucose-6-Phosphate Dehydrogenase deficiency (enzyme genetic defect causing hemolysis with primaquine) testing for Plasmodium vivax in high G6PDd prevalence communities is required. Cases should receive treatment within 72 hours of symptoms for Pf (to quickly prevent transmission and gametocyte reservoir). There is also a need to distinguish between indigenous and imported cases.
Malaria Pre-Elimination efforts are targeting 0 deaths as well as investigation of 100% of confirmed cases in Nepal. Systematic entomology investigation/interventions are required. Glucose-6-Phosphate Dehydrogenase deficiency (enzyme genetic defect causing hemolysis with primaquine) testing for Plasmodium vivax in high G6PDd prevalence communities is required. Cases should receive treatment within 72 hours of symptoms for Pf (to quickly prevent transmission and gametocyte reservoir). There is also a need to distinguish between indigenous and imported cases.
Jhpiego is providing technical assistance and capacity building for Nepal’s Ministry of Health pre-elimination efforts as follows:
- Integrated Vector Management
- Micro-stratification
- Entomology curriculum to be conducted in medical college (need new positions)
- Case-based Surveillance guidelines
- Private-sector engagement (for increased reporting and product quality control/procurement such as Antigen RDTs)
- Capacity Assessments in 9 health systems strengthening components at central and district levels (Jhpiego Malaria Implementation Guide)
- Human resources: clear job descriptions and performance goals
- Leadership & Management development program
 Program highlights include the fact that the Global Fund malaria grant rating improved from B2 (inadequate but demonstrating potential) in January 2016, but now A2 (meeting expectations) in November 2016. Concept note for operational research at 2 or 3 border check points has been developed in order to determine whether such intervention (communication & voluntary screening) is cost-effective and relevant to catch/target imported cases, raise awareness on malaria available services, detect/prevent sources of potential outbreaks. This will inform GFATM on the relevance to fund such intervention. A similar approach was done at the China-Myanmar border but was not recognized by not WHO.
Program highlights include the fact that the Global Fund malaria grant rating improved from B2 (inadequate but demonstrating potential) in January 2016, but now A2 (meeting expectations) in November 2016. Concept note for operational research at 2 or 3 border check points has been developed in order to determine whether such intervention (communication & voluntary screening) is cost-effective and relevant to catch/target imported cases, raise awareness on malaria available services, detect/prevent sources of potential outbreaks. This will inform GFATM on the relevance to fund such intervention. A similar approach was done at the China-Myanmar border but was not recognized by not WHO.
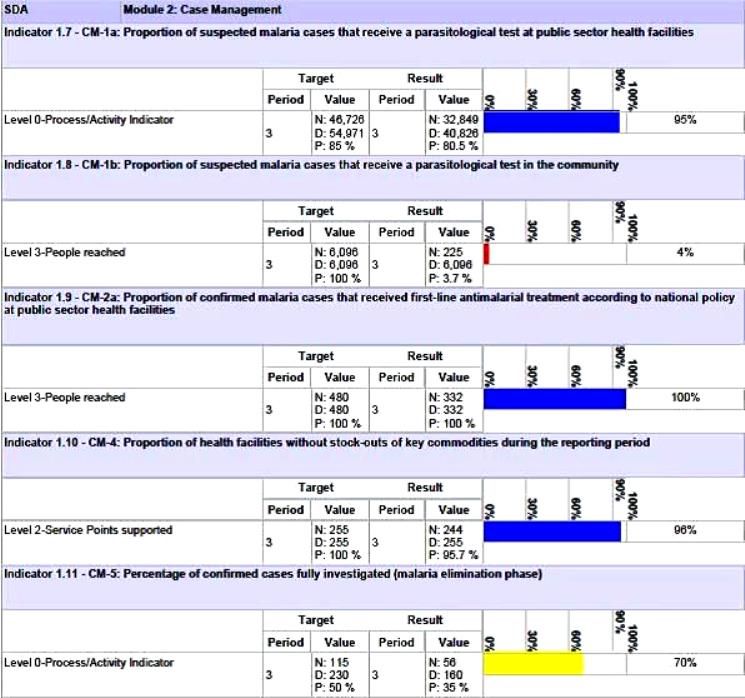
Nepal’s Global Fund Grant Indicators for Malaria Case Management
Although the National Malaria Strategic Plan refers to high risk groups (forest workers, national parks security personnel, refugees, prisoners, etc.) evidence is needed to back this up. A study or improved investigation forms are needed to identify such groups and use this information to design appropriate behavior change communications and other interventions.
Special Programming Highlights include proposing a focus on Closed/Isolated Settings/Foci (limited migration, duration and population) to WHO and GFATM. Considering a targeted mass drug administration (MDA) Plasmodium vivax (not yes recommended by WHO) with Primaquine/G6PD testing. Consideration is being given to new drugs in the pipeline such as Ivermectin. Molecular Testing using Polymerase Chain Reaction (PCR) to detect low parasitemia, asymptomatic or re-infection cases (Pv includes inactive/dormant sporozoites known as hypnozoites) is being proposed.
Community based testing as proposed in the Global Fund grant needs strengthening. Therefore RDT use by Female Community Health Volunteer is being considered. Active case detection is another possibility for those areas moving toward pre-elimination. As mentioned, there is also need for studies of asymptomatic infection.
Lessons learned so far for best practices for efforts in identifying specific pre-elimination interventions include the value of getting consensus at national level through the Malaria Technical Working Group. There is also need to challenge WHO recommendations and engage dialogue to get creative. At present there is a risk of a Catch 22 situation wherein the GFATM asks for innovative interventions but at the same time tries to adhere strictly WHO to existing guidance.
The Nepalese malaria program is in constant dialogue with the GFATM Fund Portfolio Manager and team on the local context and technical challenges in order to get them involved in looking for innovative solutions.
Challenges arise in malaria diagnostics. While systematic microscopy is the gold standard, quality can be poor because of low stain/re-agent quality, constant staff turnover and donor reluctance to fund additional training. Also microscopy confirmation and slide quality control are time consuming, and often this process is not clear or well followed. PCR require specific equipment, training and qualifications. Takes time to be operational.
There are opportunities moving forward. Progress could be made if there were more “elimination experts” to position to influencer to WHO to seek and propose new interventions for the pre-elimination stage. Nepal provides an ideal opportunity to test new ideas. It will also be necessary for the national malaria program staff to receive regular technical updates on program issues such as new drugs (Ivermectin?) and on-going pilots of MDA.
Integrated Vector Management &ITNs &Ivermectin &NTDs Bill Brieger | 11 Oct 2016
Malaria, Lymphatic Filariasis and Insecticide-treated Nets

?
Throughout Africa one of the main vectors that carry Lymphatic Filariasis (LF) is the Anopheles mosquito, which also carries the malaria parasite. The Carter Center has been promoting use of insecticide treated nets (ITNs) for many years as part of its LF control efforts, but others may not have gotten the message.
The global community is targeting LF for elimination in 2020. The primary strategy is mass drug administration annually with ivermectin and albendazole. The plan is that up to seven annual rounds of drug distribution in endemic communities where 90% of population coverage is achieved is necessary to stop LF transmission. The Carter Center explains that distribution of long-lasting insecticidal bed nets (LLINs) protects pregnant women and children who cannot take drug treatment.
The LF strategy often builds on and integrates with onchocerciasis control efforts where these diseases overlap. The community directed treatment with ivermectin (CDTI) model pioneered by the African Program for Onchocerciasis Control (APOC), wherein communities or villages plan together the distribution process including selecting their own community directed distributors (CDDs). This model has also been used to distribute ITNs.
 A second component of the LF strategy is morbidity management which focuses on enhanced personal hygiene or cleaning of the parts of the body that experience lymphedema. Another aspect uses surgery to address some of the worst effects, hydrocele. While this component does not ‘control’ LF, it is a necessary effort to reduce suffering and the negative stigma from the disease.
A second component of the LF strategy is morbidity management which focuses on enhanced personal hygiene or cleaning of the parts of the body that experience lymphedema. Another aspect uses surgery to address some of the worst effects, hydrocele. While this component does not ‘control’ LF, it is a necessary effort to reduce suffering and the negative stigma from the disease.
To judge whether transmission has stopped and elimination has been achieved Transmission Assessment Surveys (TAS) are conducted with rapid diagnostic tests on young children after at least 5 years of MDA in a community. Specifically WHO recommends an implementation unit must have completed five effective rounds of annual MDA defined as achieving rates of drug coverage exceeding 65% in the total population.
For example the Carter Center in Support of the Nigerian Federal Ministry of Health worked in Plateau and Nasarawa States through community health education, delivery of long lasting insecticide-treated nets (LLINs) and 33 million drug treatments for lymphatic filariasis and river blindness between 2000 and 2011. “In 2012, it was confirmed (through TAS) that lymphatic filariasis transmission had stopped. Post-treatment surveillance is currently underway to assure that the parasite is not reintroduced into the area.”
Another component of the assessment process is yet to be fully realized. That is the testing of mosquitoes for the presence of microfilariae. This indirectly implies an important role in preventing human-vector contact as would be achieved through the use of ITNs as well as indoor residual spray (IRS).
Vector control can benefit more than one disease. Integrated vector management is seen as a key tool to prevent reintroduction of LF in areas where anopheles mosquitoes carry the disease and where ITN campaigns are successful.
Ultimately the key to benefiting from the disease control synergies provided by insecticide-treated nets is an understanding what if any effect nets have on transmission. This poses a challenge in terms of separating it from the effect of MDAs as well as the fact that MDAs are time-limited. As MDAs are still underway in many places it is incumbent on program managers to monitor and evaluate the impact of all activities, treatment and vector control, over the next decade to determine the success of eliminating LF and hopefully malaria, too.
Drug Development &Ivermectin &NTDs Bill Brieger | 09 Oct 2016
Malaria, Onchocerciasis and Ivermectin – Possibility of Eliminating Two Diseases
Many tropical diseases are co-endemic in a given country and environment. Therefore, it only makes sense to learn whether there can be common strategies and synergies in disease control and elimination efforts. Onchocerciasis or River Blindness is carried by the black fly (simulium damnosum) that breeds along the banks of fast flowing rivers and malaria are examples.
Onchocerciasis was eliminated in many settings in the Sahel through the process or aerial spraying of these riverbanks to kill the black fly larvae. Though the insecticide used was often the same as used for malaria larviciding, the habitats differed and no synergies were achieved then.

Merck donates ivermectin to achieve control and elimination of onchocerciasis
Through subsequent programs using community directed treatment with ivermectin (Mectizan ®) interventions sponsored by the African Program for Onchocerciasis Control (APOC) it was learned that ivermectin also had beneficial effects on malaria transmission.
Ivermectin had been used in agriculture not only for internal parasites of animals. The agricultural community has long known that ivermectin kills both internal parasites (worms) but is also effective against some external parasites (lice and ticks).
Around 2010 scientists began to consider the anti-mosquito effects ivermectin might have when humans consumed it. It turns out that after a mass distribution in a community of ivermectin for onchocerciasis that mosquitoes feeding on people who had recently swallowed ivermectin would die. This was demonstrated when mosquitoes bit volunteers who took ivermectin of the first few days after consumption died there was no effect in the group not taking the drug.

Ivermectin distribution sessions in a Cameroonian village
Of particular interest was the fact that people who had consumed ivermectin would contribute to mosquito mortality even when they were outdoors. While the effect was not long lasting, the onchocerciasis control programs in the Americas have shown that it is safe to administer the drug two or four times a year.
Research that looks at the malaria parasite concluded that, “it is likely that ivermectin treatment is arresting parasite growth.” The researchers note that, “given the prior use of ivermectin and its safety record in humans and animals, it can be considered in combination therapy with other antimalarials.” The issue of dosage would need to be tested further. Ivermectin at sub-lethal concentrations even inhibits the sporogony of P. falciparum in An. Gambiae.
Because of the need to find new and complementary tools to eliminate malaria the Malaria Policy Advisory Committee (MPAC) of the World Health Organization’s Global Malaria Program considered at its recent meeting the role of endectocides including ivermectin in the future of malaria control and elimination and the importance of further research.
The future of malaria elimination requires finding new tools to integrate with and the strengthening of existing tools. If these efforts also benefit the control and elimination of other diseases, the public’s health will benefit.