CHW &Integration &IPTi &IPTp &Malaria in Pregnancy &Maternal Health &Seasonal Malaria Chemoprevention Bill Brieger | 12 Dec 2022
Malaria Chemoprevention in 2021 as Seen in The World Malaria Report of 2022
 Dr Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization, reminds us in this year’s edition of the World Malaria Report (WMR 2022) that, “Although hard hit, most countries held the line and were able to maintain services to prevent, detect and treat malaria – a remarkable feat in the midst of a pandemic. Nonetheless, more than 600 000 people still die of malaria every year – most of them children. Even with the heroic efforts to maintain services during the pandemic, malaria control efforts face many hurdles in addition to the already significant COVID-related disruptions and other health system challenges.”
Dr Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization, reminds us in this year’s edition of the World Malaria Report (WMR 2022) that, “Although hard hit, most countries held the line and were able to maintain services to prevent, detect and treat malaria – a remarkable feat in the midst of a pandemic. Nonetheless, more than 600 000 people still die of malaria every year – most of them children. Even with the heroic efforts to maintain services during the pandemic, malaria control efforts face many hurdles in addition to the already significant COVID-related disruptions and other health system challenges.”
Even though there was an increase in cases between 2020 and 2021, there are now more strategies in the malaria control and elimination toolkit than ever before. One in particular is an updated take on an old concept of chemoprophylaxis, which fell out of use due to mounting drug resistance. Years of research with pregnant women and young children led to the development over time of using regularly scheduled treatment doses of malaria medicines as chemoprevention. Intermittent Preventive Treatment for pregnant women (IPTp) and Seasonal Malaria Chemoprevention for young children, both targeted to appropriate epidemiological settings, are now common. Countries are also exploring IPT for children in other settings.
 We were, therefore, curious what the current WMR shares on chemoprevention initiatives. Specifically, the WMR summarized WHO recommendations as follows: “Updated guidelines provide recommendations on intermittent preventive treatment of malaria in pregnancy (IPTp), perennial malaria chemoprevention (PMC) and seasonal malaria chemoprevention (SMC), intermittent preventive treatment of malaria in school-aged children (IPTsc), post-discharge malaria chemoprevention (PDMC), mass drug administration (MDA) and elimination.”
We were, therefore, curious what the current WMR shares on chemoprevention initiatives. Specifically, the WMR summarized WHO recommendations as follows: “Updated guidelines provide recommendations on intermittent preventive treatment of malaria in pregnancy (IPTp), perennial malaria chemoprevention (PMC) and seasonal malaria chemoprevention (SMC), intermittent preventive treatment of malaria in school-aged children (IPTsc), post-discharge malaria chemoprevention (PDMC), mass drug administration (MDA) and elimination.”
In summary, WMR 2022 notes that, “The average number of children treated per cycle of SMC increased from about 0.2 million in 2012 to almost 45 million in 2021,” and “Using data from 33 countries in the WHO African Region, the percentage of IPTp use by dose was computed. In 2021, 72% of pregnant women used ANC services at least once during their pregnancy. About 55% of pregnant women received one dose of IPTp, 45% received two doses and 35% received three doses.” This is not just progress over time, but also represents an expansion targets and work required for success. For pregnant women the increase represented a change in target from only two doses during pregnancy to a minimum of three. Starting with pilot efforts, SMC now covers children in 15 countries.
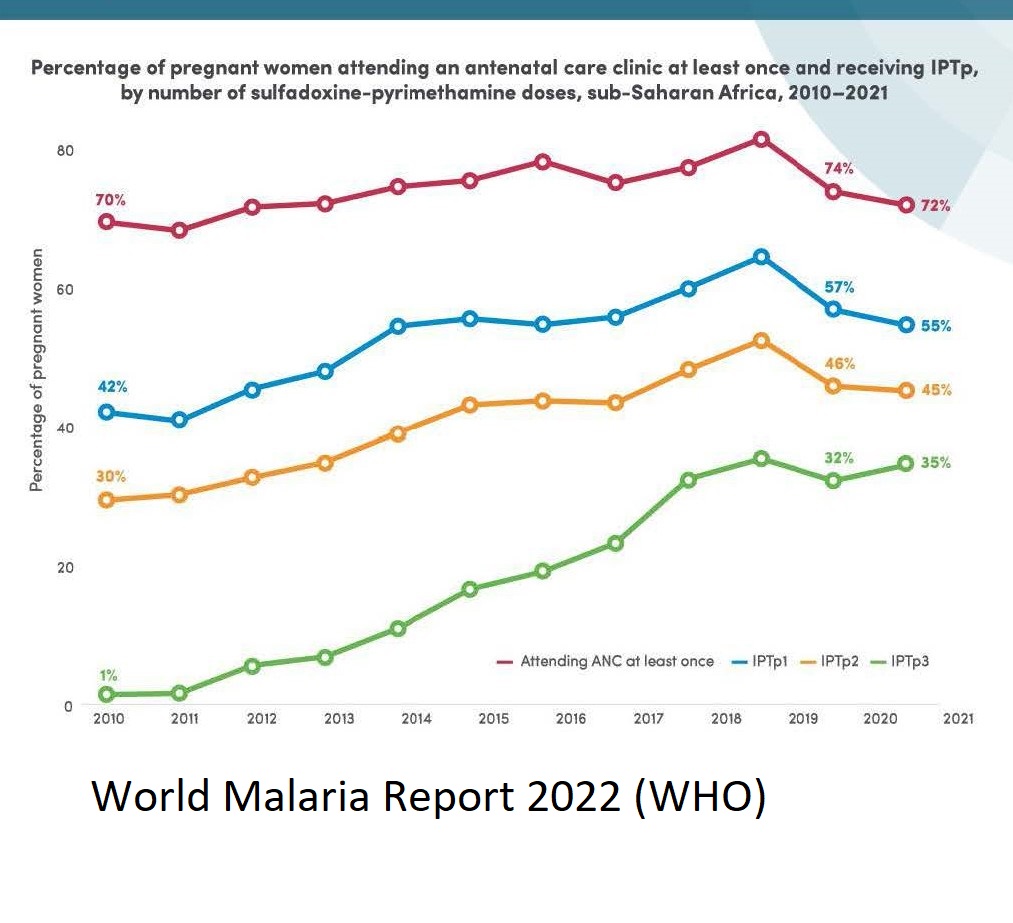 The targeted three doses for IPTp shows that two thirds of women who register for antenatal (prenatal) care (ANC), fail to achieve full coverage. Stronger collaboration is needed between malaria control and maternal health programs to ensure that pregnant women actually attend ANC and do so early and often enough to receive 3 monthly doses minimum in their second and third trimesters. More emphasis is needed on community IPTp distribution, since we know that community health workers have been crucial in achieving SMC as well as integrated community case management efforts.
The targeted three doses for IPTp shows that two thirds of women who register for antenatal (prenatal) care (ANC), fail to achieve full coverage. Stronger collaboration is needed between malaria control and maternal health programs to ensure that pregnant women actually attend ANC and do so early and often enough to receive 3 monthly doses minimum in their second and third trimesters. More emphasis is needed on community IPTp distribution, since we know that community health workers have been crucial in achieving SMC as well as integrated community case management efforts.
Similar challenges exist for SMC as research looks into whether additional doses are needed based on mosquito breeding and malaria transmission season factors in endemic countries. Adding extra months to the program will tax resources, but also save lives.
Both maternal and child efforts at chemoprevention will need to address research that first shows increasing resistance to the common medicines used, and the potential for introducing new drug combinations in light of that resistance. Challenges here reflect another aspect of SMC, the need for CHWs to guarantee that on any given distribution round, three doses on medicine are required. Recent reports show that within any given round, community adherence to SMC has been good. We need to apply those lessons to IPTp when the regimen changes.
Ultimately, chemoprevention has proven to be an important life saving tool. The challenges of multiple contacts and doses that lead to success rely not only on having effective medicines, but also on culturally appropriate behavior change strategies and well-funded efforts to strengthen the health systems that deliver preventive treatments.
coronavirus &COVID-19 &Ebola &Elimination &iCCM &IPTi &IPTp &IRS &ITNs &Research Bill Brieger | 25 Apr 2020
Zero Malaria Starts after Lockdown?
 The novel 2019 coronavirus, also known as COVID-19 and SARS-COV2, is casting a heavy shadow over the 2020 World Malaria Day. People are trying to remain upbeat declaring the tagline “zero malaria starts with me,” but nothing can hide the fear that the current pandemic will both disrupt the current delivery of essential malaria preventive and treatment services, but will have longer term impacts on malaria funding and our capacity to learn new ways to reach malaria elimination goals. As we can see in the graphic to the right, accessible, lifesaving, community-based services may be especially hard hit.
The novel 2019 coronavirus, also known as COVID-19 and SARS-COV2, is casting a heavy shadow over the 2020 World Malaria Day. People are trying to remain upbeat declaring the tagline “zero malaria starts with me,” but nothing can hide the fear that the current pandemic will both disrupt the current delivery of essential malaria preventive and treatment services, but will have longer term impacts on malaria funding and our capacity to learn new ways to reach malaria elimination goals. As we can see in the graphic to the right, accessible, lifesaving, community-based services may be especially hard hit.
 Another ironic image is the indoor residual spray (IRS) team member with a face mask needed for protection from the insecticides being sprayed. When will such teams be able to go back into homes? When can household members actually pack out their belongings so that spraying can commence? When will such masks not be needed for intensive care COVID-19 case management instead?
Another ironic image is the indoor residual spray (IRS) team member with a face mask needed for protection from the insecticides being sprayed. When will such teams be able to go back into homes? When can household members actually pack out their belongings so that spraying can commence? When will such masks not be needed for intensive care COVID-19 case management instead?
WHO is urging “countries to move quickly to save lives from malaria in sub-Saharan Africa” because “New analysis supports the WHO call to minimize disruptions to malaria prevention and treatment services during the COVID-19 pandemic.” This will be difficult in high burden countries like Nigeria that are already on lockdown with over 1,000 coronavirus cases detected already. Modeling by WHO and partners has projected, “Severe disruptions to insecticide-treated net campaigns and in access to antimalarial medicines could lead to a doubling in the number of malaria deaths in sub-Saharan Africa this year compared to 2018.”
 The Global Malaria Program offers guidance for tailoring malaria interventions to the present circumstances. Great concern is drawn from previous epidemic situations when observing that, “it is essential that other killer diseases, such as malaria, are not ignored. We know from the recent Ebola outbreak in west Africa that a sudden increased demand on fragile health services can lead to substantial increases in morbidity and mortality from other diseases, including malaria. The COVID-19 pandemic could be devastating on its own – but this devastation will be substantially amplified if the response undermines the provision of life-saving services for other diseases.”
The Global Malaria Program offers guidance for tailoring malaria interventions to the present circumstances. Great concern is drawn from previous epidemic situations when observing that, “it is essential that other killer diseases, such as malaria, are not ignored. We know from the recent Ebola outbreak in west Africa that a sudden increased demand on fragile health services can lead to substantial increases in morbidity and mortality from other diseases, including malaria. The COVID-19 pandemic could be devastating on its own – but this devastation will be substantially amplified if the response undermines the provision of life-saving services for other diseases.”
Specifically, GMP recommends that national malaria programs should ensure the following:
- a focal point for malaria is a member of the National COVID-19 Incident Management Team.
- continued engagement with all relevant national COVID-19 stakeholders and partners.
- continued access to and use of recommended insecticide-treated mosquito nets (ITNs)
- continuation of planned targeted indoor residual spraying (IRS)
- early care-seeking for fever and suspected malaria by the general population to prevent a spike in severe malaria
- access to case management services in health facilities and communities with diagnostic confirmation through rapid diagnostic tests [RDTs]
- treatment of confirmed malaria cases with approved protocols
- continued delivery of planned preventive services normally provided to specific target populations (SMC, IPTi, IPTp)
- the safety of all malaria personnel and their clients in the process of carrying out the above interventions
 In editorial in the American Journal of Tropical Medicine and Hygiene by Yanow and Good address the damaging longer term impact of the present shutdown. “The impacts of research shutdowns will be felt long after the pandemic. Many scientists study diseases that do not share the same obvious urgency as COVID-19 and yet take a shocking toll on human life. For example, malaria infects more than 200 million people and takes the lives of nearly half a million people, mostly young children, each year.1 During laboratory closures and without clinical studies, there will be no progress toward treating and preventing malaria: no progress toward new drugs, vaccines, or diagnostics.”
In editorial in the American Journal of Tropical Medicine and Hygiene by Yanow and Good address the damaging longer term impact of the present shutdown. “The impacts of research shutdowns will be felt long after the pandemic. Many scientists study diseases that do not share the same obvious urgency as COVID-19 and yet take a shocking toll on human life. For example, malaria infects more than 200 million people and takes the lives of nearly half a million people, mostly young children, each year.1 During laboratory closures and without clinical studies, there will be no progress toward treating and preventing malaria: no progress toward new drugs, vaccines, or diagnostics.”
The case for continuing malaria services to save hundreds of thousands of lives is not difficult to make. The actual implementation during lockdowns and quarantines is a management challenge. The importance of malaria testing to provide patients with appropriate care for the right disease is crucial. The question is whether in resource strapped endemic countries these decisions and management arrangements can be made in a timely fashion and for the long term whether the next generation of research can proceed with much needed new medicines and technologies.
Diagnosis &Essential Medicines &IPTi &Malaria in Pregnancy &Seasonal Malaria Chemoprevention &Treatment &Zero Malaria Bill Brieger | 25 Apr 2019
Zero Malaria Starts with Universal Coverage: Part 2 Preventive and Curative Treatments
April hosts several important global health days or observances. On World Health Day 2019 WHO stressed that, “Universal health coverage (UHC) is WHO’s number one goal. Key to achieving it is ensuring that everyone can obtain the care they need, when they need it, right in the heart of the community.” Nationwide monitoring through the Demographic and Health Surveys (DHS), the Malaria Indicator Surveys (MIS) and the Multi-Indicator Cluster Surveys (MICS) can document the status of appropriate malaria treatment and intermittent preventive treatment in pregnant women (IPTp).
 Definitions of indicators have evolved for treatment-related malaria interventions. When Intermittent Preventive Treatment for pregnant women (IPTp) began in the early 2000s, the recommended dosing was twice during pregnancy after the first trimester one month apart in high and/or stable transmission areas. Due to lessening efficacy of sulfadoxine-pyrimethamine (SP), the dosage recommendation has changed to at least three times, still a month apart from the beginning of the second trimester.
Definitions of indicators have evolved for treatment-related malaria interventions. When Intermittent Preventive Treatment for pregnant women (IPTp) began in the early 2000s, the recommended dosing was twice during pregnancy after the first trimester one month apart in high and/or stable transmission areas. Due to lessening efficacy of sulfadoxine-pyrimethamine (SP), the dosage recommendation has changed to at least three times, still a month apart from the beginning of the second trimester.
This updated policy was broadcast widely between 2012 and 2013, but it took countries some time to build capacity and scale up for the expanded coverage goals. UNICEF Data5 again show that between 2014 and 2017 coverage was far below either 80% of pregnant women, let alone reaching them universally (Figure 2). Most countries achieved 30% or less coverage. Zambia at 50% was the highest. Low coverage leaves both pregnant women and the unborn child at risk for anemia and death in the former and low birth weight, still birth or miscarriage for the latter. The World Malaria Report of 2018 estimates that three doses of IPTp were received by only 22% of pregnant women in the target countries in 2017.
The concept of IPT was investigated for infants and children during by a consortium of researchers in several African Countries. It was found that IPTi with SP could have a positive effect on preventing malaria. To operationalize this concept, the World Health Organization developed what is known as Seasonal Malaria Chemoprevention (SMC) that would be delivered in the Sahel region of West Africa where malaria transmission itself is seasonal and where there are some countries with very low transmission with implications for malaria elimination.
 The SMC delivery process was not linked to immunization but provided by community health workers and volunteers. SP and Amodiaquine (SP-AQ) were used in combination and provided monthly, three or four times during the rainy/high transmission season. Coverage was targeted at children below school age. It is only recently that SMC has been scaled up to reach all eligible countries or states and regions within designated countries.
The SMC delivery process was not linked to immunization but provided by community health workers and volunteers. SP and Amodiaquine (SP-AQ) were used in combination and provided monthly, three or four times during the rainy/high transmission season. Coverage was targeted at children below school age. It is only recently that SMC has been scaled up to reach all eligible countries or states and regions within designated countries.
WHO states that SMC focuses on, “children aged 3–59 months (and) reduces the incidence of clinical attacks and severe malaria by about 75%.” In some countries the coverage is extended to primary school aged children, making comparisons and calculations of coverage (universal por otherwise) challenging.
 The World Malaria Report of 2018 notes that, “In 2017, 15.7 million children in 12 countries in Africa’s Sahel subregion were protected through seasonal malaria chemoprevention (SMC) programs. However, about 13.6 million children who could have benefited from this intervention were not covered, mainly due to a lack of funding.” This implies that 54% of eligible children were reached. Coverage of SMC can refer to receiving any of the doses or as having received all the monthly doses offered by a nation’s malaria control program. Specifically, the World Malaria Report 2018 drew on surveys in 7 countries that provided 4 monthly doses to determine that 53% of children received all doses.
The World Malaria Report of 2018 notes that, “In 2017, 15.7 million children in 12 countries in Africa’s Sahel subregion were protected through seasonal malaria chemoprevention (SMC) programs. However, about 13.6 million children who could have benefited from this intervention were not covered, mainly due to a lack of funding.” This implies that 54% of eligible children were reached. Coverage of SMC can refer to receiving any of the doses or as having received all the monthly doses offered by a nation’s malaria control program. Specifically, the World Malaria Report 2018 drew on surveys in 7 countries that provided 4 monthly doses to determine that 53% of children received all doses.
 Determining coverage for malaria treatment for sick people is not as straightforward as finding out the numbers who slept under an ITN or swallowed IPTp doses, and even those are not simple. As defined, correct treatment first consists of parasitological diagnosis, which at the primary care level could be by microscopy or rapid diagnostic test (RDT). The next issue is treating only those with positive tests. Finally, the treatment must consist of age- or weight-specific doses of an approved artemisinin-based combination therapy (ACT) drug. Very few clinic records or surveys document whether the treatment given is ‘correct’ by these standards.
Determining coverage for malaria treatment for sick people is not as straightforward as finding out the numbers who slept under an ITN or swallowed IPTp doses, and even those are not simple. As defined, correct treatment first consists of parasitological diagnosis, which at the primary care level could be by microscopy or rapid diagnostic test (RDT). The next issue is treating only those with positive tests. Finally, the treatment must consist of age- or weight-specific doses of an approved artemisinin-based combination therapy (ACT) drug. Very few clinic records or surveys document whether the treatment given is ‘correct’ by these standards.
WHO addresses the need for achieving universal access to malaria diagnostic testing and notes this will not be easy. They provide a successful example of Senegal, where following the introduction of malaria RDTs in 2007, malaria diagnostic testing rates rose rapidly from 4% to 86% (by 2009). Logistics, funding, training and supportive supervision complicate implementation.
UNICEF Data report that performance of malaria diagnostics in febrile children in surveys 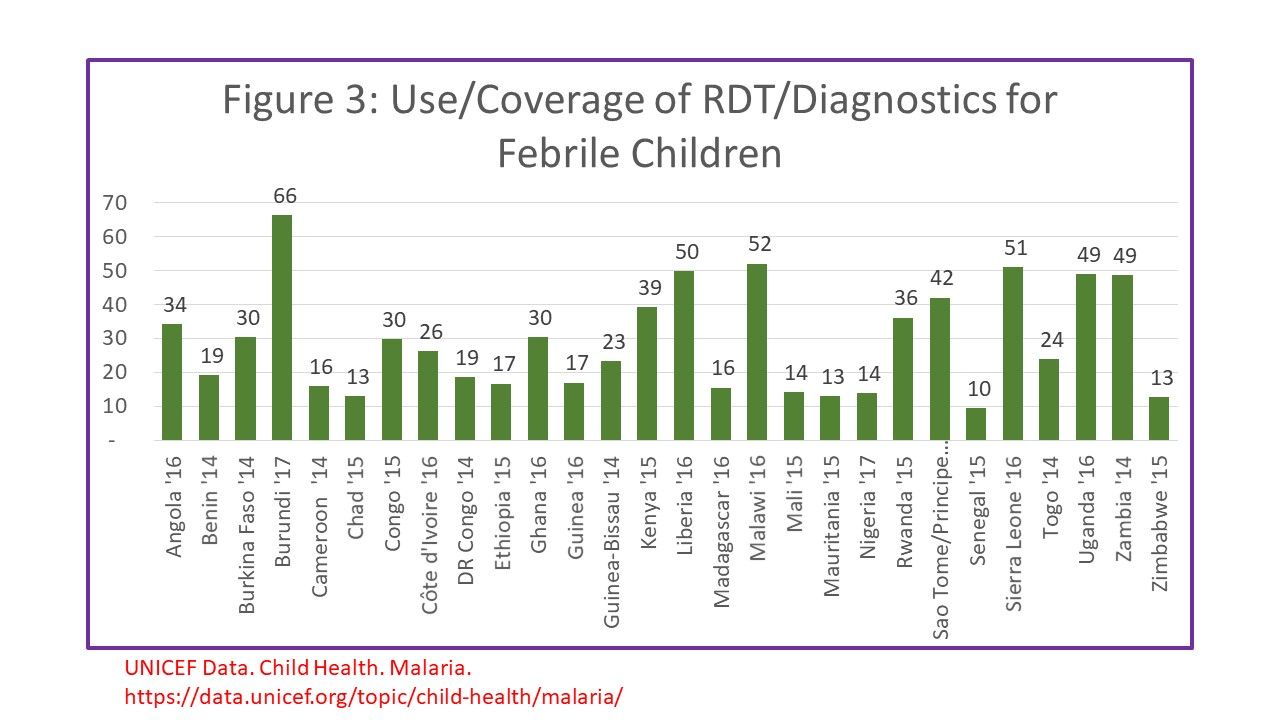 between 2014-17 was approximately 30% on average for countries with national surveys within that time frame (Figure 3). Only 4 countries achieved 50% or better. Most surveys then go on to report the number of febrile children who received ACTs, but do not necessary indicate how many who were correctly diagnoses were given ACTs vs those who received ACT but did not receive a test or tested negative.
between 2014-17 was approximately 30% on average for countries with national surveys within that time frame (Figure 3). Only 4 countries achieved 50% or better. Most surveys then go on to report the number of febrile children who received ACTs, but do not necessary indicate how many who were correctly diagnoses were given ACTs vs those who received ACT but did not receive a test or tested negative.
The Nigeria 2015 Malaria Indicator Survey Illustrates this dilemma. Among 2600 children who reported having a fever in the two weeks preceding the survey, 66.1% sought advice (or care). Overall, 12.6% of febrile children received a diagnostic test as defined in the question as to whether the child was stuck on the finger or heel to obtain blood. Among the febrile children 37.6% reportedly were given some type of antimalarial drug. Overall 15.5% of febrile children were given an ACT. Even if ACTs were given only to tested children, not all tests would have been positive.
The overall implication of measuring treatment without a link to testing is that if more children receive any, let alone the correct drugs, is that evidence for actual presence of disease. We have a long way to go to measure malaria treatment coverage correctly, not to mention achieving universal coverage with appropriate treatment. Different malaria treatment-related interventions with different steps and different target groups in different regions of Africa and the World make defining, no less achieving UHC, a huge challenge.
Borders &CHW &Climate &Elimination &IPTi &Sahel &Surveillance &Vector Control Bill Brieger | 26 Sep 2018
Hopefully Malaria Elimination will not be the SaME
The Sahel Malaria Elimination Initiative (SaME) has been launched, but builds on a long history of cooperation in the region. Efforts by eight Sahelian countries to share lessons and strategies mirrors the Elimination Eight group on the opposite end of the continent.

The few rainy season months in the Sahel offer optimum malaria transmission, which SaME is tackling
The Roll Back Malaria (RBM) Partnership to End Malaria announced that in Dakar on 31st August 2018, the health “ministers from Burkina Faso, Cabo Verde, Chad, Mali, Mauritania, Niger, Senegal and The Gambia established a new regional platform to combine efforts on scaling up and sustaining universal coverage of anti-malarials and mobilizing financing for elimination.” The group plans a fast-track introduction of “innovative technologies to combat malaria and develop a sub-regional scorecard that will track progress towards the goal of eliminating malaria by 2030.” This will build on the existing country scorecard that has been developed and implemented by AMLA2030 for all countries in the region and tracks roll out of key malaria and health interventions. The Sahel Malaria Elimination Initiative will be hosted by the West African Health Organization, a specialised agency of the Economic Community of West African States (ECOWAS).
RBM explains that while the eight countries will work together, they do not have a homogenous epidemiological picture or experience with malaria programming. The Sahel experiences 20 million annual malaria cases, according to RBM, and “the Sahel region has seen both achievements and setbacks in the fight against the disease in recent years.” These eight have a highly variable malaria experience. Burkina Faso and Niger continue to be among the countries with high malaria burdens. Cabo Verde is on target for malaria free status by 2020. The Gambia, Mauritania and Senegal are reorienting their national malaria program towards malaria elimination. A benefit of this epidemiological and programmatic diversity is that countries can learn important lessons from each other.
The SaME Initiative will use the following main approaches to accelerate the combined efforts towards the attainment of malaria elimination in the sub-region:3
- Regional coordination
- Advocacy to keep malaria elimination high on the development and political agenda
- Sustainable financing mechanisms
- Cross-border collaboration and ensuring accountability
- Fast-track the introduction of innovative and progressive technologies
- Re-enforcing the Regional regulatory mechanism for quality of malaria commodities and introduction of new tools.
- Establish malaria observatory, regional surveillance, and best practice sharing
Collaboration across borders on vector control is an example of needed regional coordination. According to Thomson et al., climate variations have the potential to significantly impact vector-borne disease dynamics at multiple space and time scales. Another challenge to vector control in the region is the issue of how mosquitoes repopulate areas after an extended dry season. Huestis et al. examined the response of Anopheles coluzzii and Anopheles gambiae to environmental cues in season change in the Sahel.

Seasonal Malaria Chemoprevention Round 3 of 2018 in Burkina Faso
In addition to a history of cooperation, Sahelian countries share a unique malaria intervention, Seasonal Malaria Chemoprevention (SMC) that as the name implies, built on the reality of highly seasonal transmission in the region. SMC grew out of over five years of research in several African settings to test the effect of what was originally termed Intermittent Preventive Treatment for Infants (and later children) or IPTi.
Like IPT for pregnant women, SMC would be given monthly for at least 3-4 months, but unlike IPTp, SMC would consist of a combination two medicines, amodiaquine plus sulfadoxine-pyrimethamine (AQ+SP), which required a three daily doses (SP alone as used in IPTp consists on one dose). SMC could not therefore, be delivered effectively as a clinic-based intervention, but “should be integrated into existing programmes, such as Community Case Management and other Community Health Workers schemes.” Access to SMC by pre-school aged children as delivered by CHWs was found to be more equitable than sleeping under an LLIN. SMC has been recommended for school-age children, a neglected group that bears a substantial burden of malaria.
Closely linked to surveillance is modeling the spatial and temporal variability of climate parameters, which is crucial to tackling malaria in the Sahel. This requires reliable observations of malaria outbreaks over a long time period. To date efforts are mainly linked to climate variables such as rainfall and temperature as well as specific landscape characteristics. Other environmental and socio-economic factors that are not included in this mechanistic malaria model.
The Sahel Malaria Elimination initiative offers a unique collaborative opportunity for countries to improve on the quality of proven interventions like SMC and test and take to scale new strategies like school-based malaria programs. Regional coordination can produce better, timelier and longer-term surveillance and better understanding of and actions against malaria vectors. Readers will surely be anticipating the publishing of the regular progress malaria elimination scorecards as promised by SaME leadership.
Advocacy &IPTi &Malaria in Pregnancy Bill Brieger | 16 Nov 2016
Country Updates on Global Call to Action to Increase Coverage of Intermittent Preventive Treatment in Pregnancy
Symposium 87 at the 65th Annual Meeting of the American Society of Tropical Medicine and Hygiene focused on the Global Call to Action to Increase Coverage of Intermittent Preventive Treatment in Pregnancy: Progress and Lessons Learned. The original Global Call was initiated at a previous ASTMH meeting. Elaine Roman of Jhpiego chaired the session. Panelists included Julie Gutman of the US CDC, Frank Chacky of the NMCP in Tanzania, Yacouba Savadogo of the NMCP in Burkina Faso and Fannie Kachale of the Reproductive Health Directorate in the Malawi MOH.
 The symposium speakers reviewed country progress in sub-Saharan Africa (SSA) in increasing intermittent preventative treatment in pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP). They described how Ministries of Health and donors and partners are working to increase IPTp-SP coverage to address malaria in pregnancy (MiP).
The symposium speakers reviewed country progress in sub-Saharan Africa (SSA) in increasing intermittent preventative treatment in pregnancy (IPTp) with sulfadoxine-pyrimethamine (SP). They described how Ministries of Health and donors and partners are working to increase IPTp-SP coverage to address malaria in pregnancy (MiP).
Following the release of the World Health Organization’s (WHO) 2012 updated policy on IPTp-SP, a number of global stakeholders came together through the Roll Back Malaria-Malaria in Pregnancy Working Group, to elaborate the Global Call to Action: To Increase National Coverage with IPTp of MiP for Immediate Impact. The Call to Action calls upon countries and partners to immediately scale up IPTp-SP to improve health outcomes for mothers and their newborns. Scaling up IPTp-SP across most countries in sub-Saharan Africa remains a critical weapon to prevent the devastating consequences of MiP.
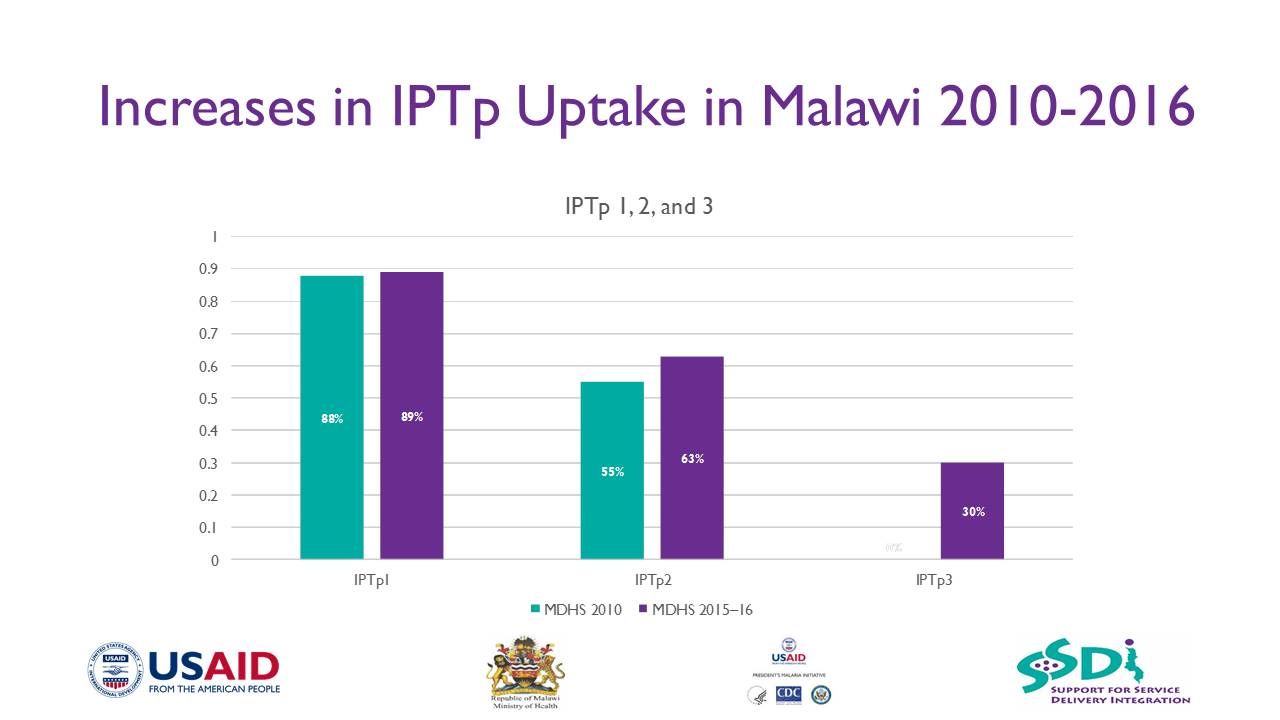
IPTp3+ has been started in Malawi following WHO recommendations
However, the low proportion of eligible pregnant women receiving at least one dose of IPTp-SP (52%) and IPTp3-SP (17%) in 2014 is unacceptable. Despite growing parasite resistance to SP in some areas, IPTp-SP remains Tuesday a highly cost-effective, life-saving strategy to prevent the adverse effects of MiP in the vast majority of SSA.
Completion of the recommended three or more doses of IPTp-SP decreases the incidence of low birthweight (LBW) by 27%, severe maternal anemia by 40% and neonatal mortality by 38%. This symposium will feature presentations from WHO and the President’s Malaria Initiative on how they are prioritizing support to scale up MiP interventions including IPTp-SP across SSA.
Panelists from Burkina Faso, Malawi and Tanzania discussed how they were able to dramatically scale up IPTp-SP through a health systems approach that addresses MiP from community to district to national level.
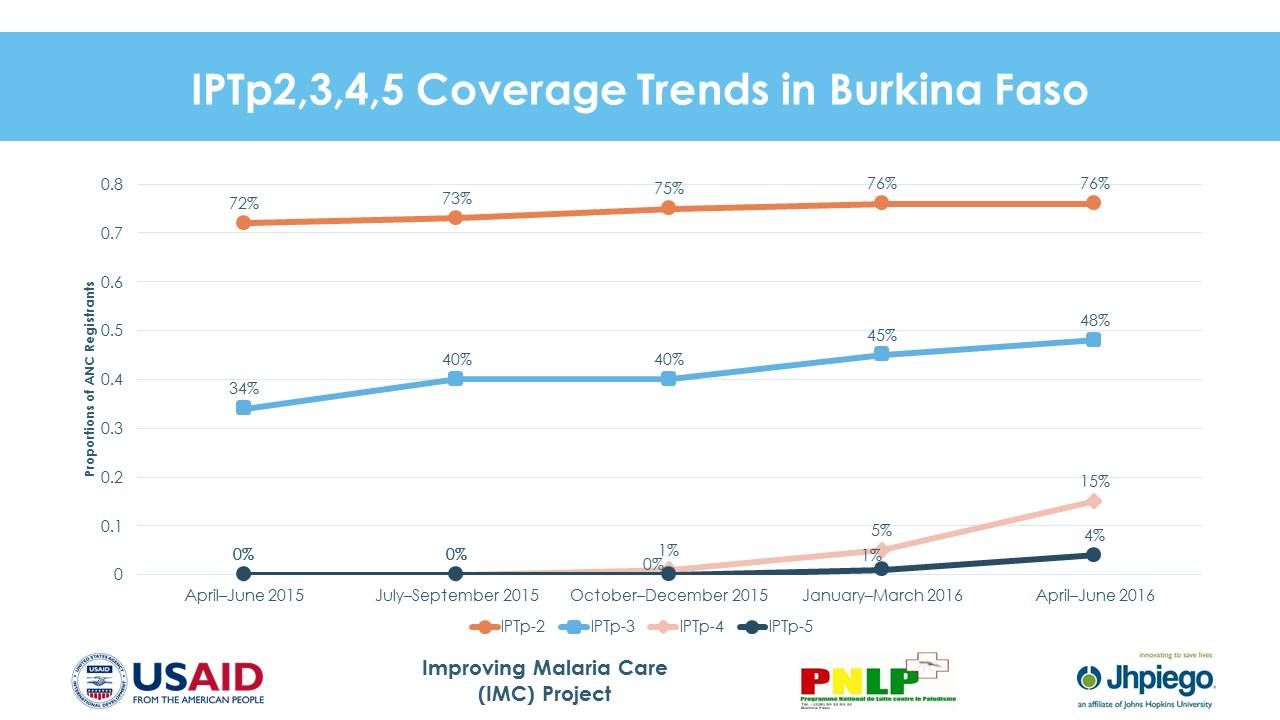 In Burkina Faso, IPTp2-SP increased from 54.8% in 2013 to 82.3% nationally in 2015 and IPTp3-SP increased from 13.5% in 2014 to 41.2% nationally in 2015. Moving ahead Burkina Faso will Improve SP supply chain management, Pilot an IPTp distribution at the community level in three districts, Provide job aids throughout ANC clinics, and Provide support to district team for data review and analysis.
In Burkina Faso, IPTp2-SP increased from 54.8% in 2013 to 82.3% nationally in 2015 and IPTp3-SP increased from 13.5% in 2014 to 41.2% nationally in 2015. Moving ahead Burkina Faso will Improve SP supply chain management, Pilot an IPTp distribution at the community level in three districts, Provide job aids throughout ANC clinics, and Provide support to district team for data review and analysis.
In Malawi, in targeted project sites across 15 districts, IPTp1 uptake increased from 44% in 2012 to 87% in 2015, while IPT2 increased from 16% to 61% over the same time period. Lessons learned from scale up include –
- Consistent availability of SP for IPTp is critical to increasing coverage
- A clear policy put in place to guide IPTp implementation is crucial

- A strong partnership between the Reproductive Health Directorate and National Malaria Control Programme is necessary
- Intensification of information, education, and communication is crucial to increase uptake of ANC services
- Strong collaboration, planning, and coordination between partners and other stakeholders improve ANC attendance
- Antenatal clinics offers enormous opportunities for delivering the malaria prevention package, such as IPTp and insecticide-treated nets, to pregnant women
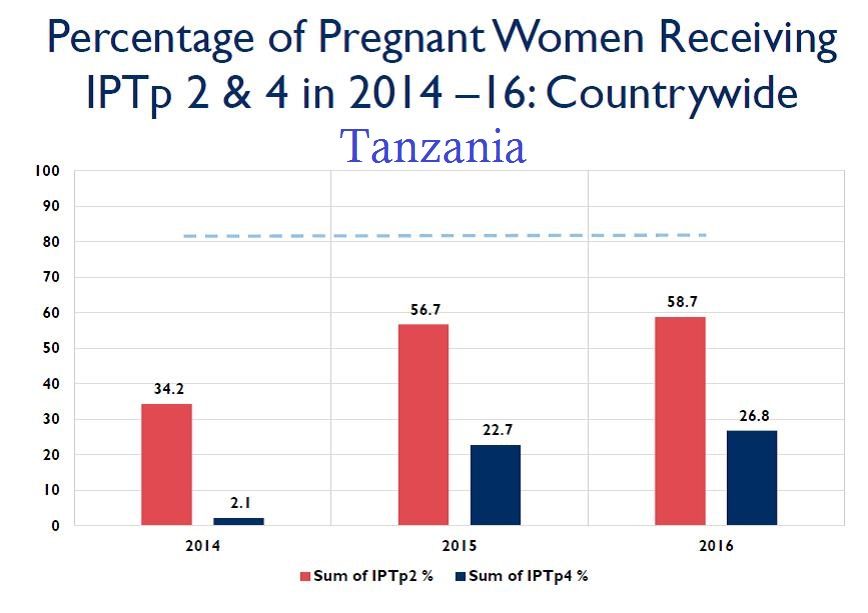 In Tanzania, IPTp2-SP increased from 34% in 2014 to 57% in 2015 and IPTp4-SP was reported at 22% in 225 facilities across 16 districts, in 2015. Program learning in Tanzania identified that consistent availability of commodities at facility level can complement Government’s and partners’ efforts to ensure provision of quality MiP services. Despite increased number of trained health care workers and regular supportive supervision and mentoring, increasing uptake of IPTp will continue to be a challenge unless malaria commodities such as mRDT and SP are available at health facilities. Redistribution of commodities among facilities could be crucial balancing the stock.
In Tanzania, IPTp2-SP increased from 34% in 2014 to 57% in 2015 and IPTp4-SP was reported at 22% in 225 facilities across 16 districts, in 2015. Program learning in Tanzania identified that consistent availability of commodities at facility level can complement Government’s and partners’ efforts to ensure provision of quality MiP services. Despite increased number of trained health care workers and regular supportive supervision and mentoring, increasing uptake of IPTp will continue to be a challenge unless malaria commodities such as mRDT and SP are available at health facilities. Redistribution of commodities among facilities could be crucial balancing the stock.
 Moving forward Tanzania plans to use alternative funding to procure malaria commodities at health facility (e.g., Community Health Fund, National Health Insurance Fund, basket fund). Other efforts will include conducting onsite mentorship and coaching, data collection and interpretation, selecting sentinel sites for collecting IPTp3, working with Ministry of Health HMIS to revise HMIS tools when opportunity arises, and training Community Health Workers (CHWs) on maternal, neonatal and child health interventions including early booking of ANC services.
Moving forward Tanzania plans to use alternative funding to procure malaria commodities at health facility (e.g., Community Health Fund, National Health Insurance Fund, basket fund). Other efforts will include conducting onsite mentorship and coaching, data collection and interpretation, selecting sentinel sites for collecting IPTp3, working with Ministry of Health HMIS to revise HMIS tools when opportunity arises, and training Community Health Workers (CHWs) on maternal, neonatal and child health interventions including early booking of ANC services.
These three country examples demonstrate that progress is challenging but possible. The call to action for increased IPTp access and use is stronger today.
IPTi &Malaria in Pregnancy &Procurement Supply Management Bill Brieger | 15 Nov 2016
Improving IPTp uptake and mitigating Stock-outs in Bungoma County, Kenya
A poster entitled “Improving Pregnancy Outcomes: Alleviating Stock-Outs of Sulfadoxine-Pyrimethamine in Bungoma, Kenya” was presented by Augustine Ngindu, Gathari Ndirangu, Waqo Ejersa, David Omoit, and Mildred Mudany from Jhpiego’s Kenya Team at the 65th annual meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. The abstract follows …
 WHO recommends intermittent preventive treatment of malaria in pregnancy using sulfadoxine pyrimethamine (IPTp-SP) to be provided at antenatal care (ANC) clinic. The Malaria Policy in Kenya requires that All pregnant women in malaria-endemic areas receive free intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine (IPTp-SP), have access to free malaria diagnosis and treatment when presenting with fever, and have access to long-lasting insecticidal nets.
WHO recommends intermittent preventive treatment of malaria in pregnancy using sulfadoxine pyrimethamine (IPTp-SP) to be provided at antenatal care (ANC) clinic. The Malaria Policy in Kenya requires that All pregnant women in malaria-endemic areas receive free intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine (IPTp-SP), have access to free malaria diagnosis and treatment when presenting with fever, and have access to long-lasting insecticidal nets.
Kenya’s Strategic Direction between 2014–2018 was revised to reflect the following:
- All pregnant women in the 14 malaria-endemic counties shall receive at least three doses of IPTp-SP
- Annual quantification of SP based on consumption to ensure adequate supplies
- Training, retraining and supervision of health care workers
- Dissemination of appropriate IPTp messages and materials
 Ministry of Health (MOH) used to procure SP until 2013 when health services were devolved to counties and procurement of became the responsibility of county governments. This presented a major challenge as counties had not factored SP in their budgets. Consequently, counties experienced SP stock-outs from October 2014. In Bungoma County the number of pregnant women receiving IPTp dropped by 51% from 7,845 in October 2014 to 3,865 in February 2015.
Ministry of Health (MOH) used to procure SP until 2013 when health services were devolved to counties and procurement of became the responsibility of county governments. This presented a major challenge as counties had not factored SP in their budgets. Consequently, counties experienced SP stock-outs from October 2014. In Bungoma County the number of pregnant women receiving IPTp dropped by 51% from 7,845 in October 2014 to 3,865 in February 2015.
To alleviate the situation (MOH) at national level requested counties to procure SP. Advocacy efforts with Bungoma County by the Maternal and Child Survival Program focused on prioritization of SP procurement at least once every quarter. As a result of this intervention, Bungoma County procured SP from February to July 2015.
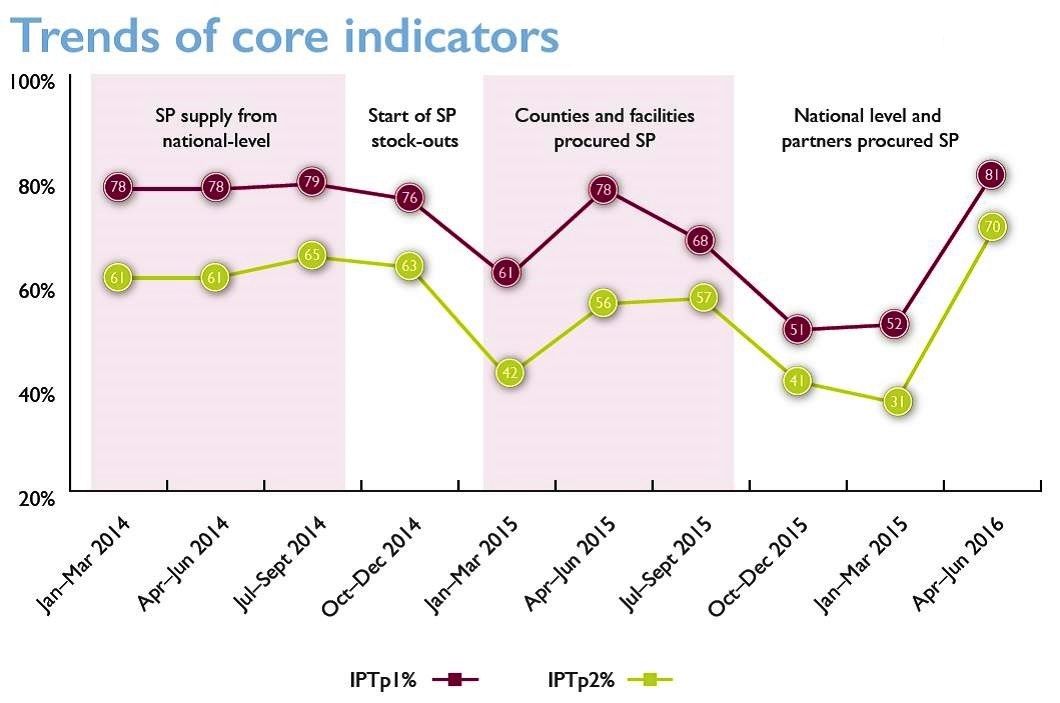 The county advised health facilities to procure additional SP doses if the supplied stocks ran out. The procurement led to a 117% increase in the number of pregnant women receiving IPTp; from 3,865 in February to 8,404 in July 2015.
The county advised health facilities to procure additional SP doses if the supplied stocks ran out. The procurement led to a 117% increase in the number of pregnant women receiving IPTp; from 3,865 in February to 8,404 in July 2015.
The fiscal year ended in June 2015 and no funds were available to procure additional SP until October 2015. This contributed to a 33% decrease in the number of pregnant women receiving IPTp from 8,404 in July to 5,672 in October 2015. As a response to support counties, MOH at national level procured 2.24 million SP doses in November/December for 14 MIP-focus counties which were received at health facilities in February 2016.
In conclusion, Bungoma County applied feasible mitigation measures including county level procurement of SP, supplemented by additional procurement at health facility and national levels. This is a practice which is replicable in other counties to ensure continued availability of SP to protect pregnant women from effects of malaria in pregnancy.
CHW &Community &IPTi &ITNs &Malaria in Pregnancy &Treatment Bill Brieger | 01 Nov 2015
Community Directed Interventions to Enhance PHC and MCH
William Brieger of the Department of International Health, JHU Bloomberg School of Public Health, delivered the keynote address to the Community Based Primary Health Care Working Group at the 2015 American Public Health Association in Chicago. The focus was on Community Directed Interventions (CDI) as a way to enhance implementation of primary health care and maternal and child health. Some excerpt from the talk follow.
 The origins of the CDI Approach are based in Onchocerciasis Control and the implementation research done by the Tropical Disease Research (TDR) Program of WHO and collaborating agencies to help establish the foundational guidance of the African Program for Onchocerciasis Control in 1995. Since then we have seen an expansion of CDI into other health issues
The origins of the CDI Approach are based in Onchocerciasis Control and the implementation research done by the Tropical Disease Research (TDR) Program of WHO and collaborating agencies to help establish the foundational guidance of the African Program for Onchocerciasis Control in 1995. Since then we have seen an expansion of CDI into other health issues
We should start discussion with an understanding of ‘community’ which Rifkin et al. (1988) defined as a group of people living in the same defined area sharing basic values, organization, and interests. White (1982) proposed that community is an informally organized social entity which is characterized by a sense of identity. Manderson et al. (1992) in their work for TDR defined community as a population which is geographically focused but which also exists as a discrete social entity, with a local collective identity and corporate purpose.
Communities are people sharing values and institutions. Community is based on locality (geographic), interdependent social groups, interpersonal relationships expressed through social networks and built on s culture that includes values, norms, and attachments to the community as a whole as well as to its parts. Prior to developing any community intervention we must understand the boundaries, composition and structure of a community from the perspectives of its own members, as their local knowledge and participation are central to success.
 Community Systems Strengthening has been taken up by the Global Fund in order to enhance coverage of various health interventions such as HIV drugs and bednets to prevent malaria. Community systems are community?led structures and mechanisms used by communities through which community members and community based organizations and groups interact, coordinate and deliver their responses to the challenges and needs affecting their communities. Many community systems are small?scale and/or informal. Others are more extensive – they may be networked between several organizations and involve various sub?systems. For example, a large care and support system may have distinct sub?systems for comprehensive home?based care, providing nutritional support, counselling, advocacy, legal support, and referrals for access to services and follow?up.
Community Systems Strengthening has been taken up by the Global Fund in order to enhance coverage of various health interventions such as HIV drugs and bednets to prevent malaria. Community systems are community?led structures and mechanisms used by communities through which community members and community based organizations and groups interact, coordinate and deliver their responses to the challenges and needs affecting their communities. Many community systems are small?scale and/or informal. Others are more extensive – they may be networked between several organizations and involve various sub?systems. For example, a large care and support system may have distinct sub?systems for comprehensive home?based care, providing nutritional support, counselling, advocacy, legal support, and referrals for access to services and follow?up.
Efficacy, Social Control and Cohesion are important characteristics of communities that enable them to take on project and solve problems. Collective Efficacy is a perceived ability to work together. Social control provides evidence that communities are able to enforce their norms. Cohesion describes social interaction that brings people together. A strong sense of identity and a sense of belonging describe communities that can get things done. These characteristics lead to community competency to collaborate effectively in identifying the problems/needs of the community, achieve a working consensus on goals and priorities, agree on ways and means to implement the agreed-upon goals, and collaborate effectively in the required actions.
 It is important to distinguish between Community Based Intervention (CBI) and Community Directed Intervention. CBI takes place in the community but a Health/Development agency exercises authority over decisions on project design and implementation. Project activities (e.g., service delivery dates and procedures) are designed by the agency. Activities simply happen in the community.
It is important to distinguish between Community Based Intervention (CBI) and Community Directed Intervention. CBI takes place in the community but a Health/Development agency exercises authority over decisions on project design and implementation. Project activities (e.g., service delivery dates and procedures) are designed by the agency. Activities simply happen in the community.
With CDI the community exercises authority over decisions and decides on acceptable method to implement projects. This ensures sensitivity to local decision-making structures and social life. Activities happen both in and by the community; the community is in control.
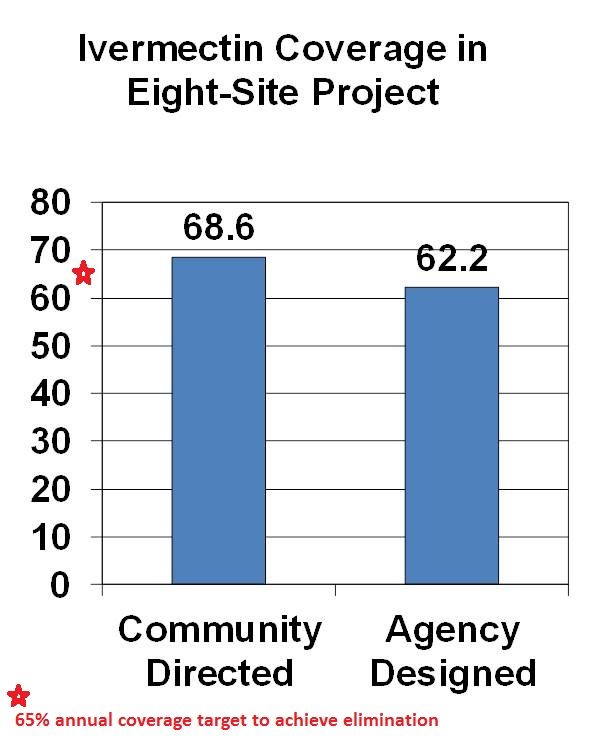
CDI was pioneered for Onchocerciasis (River Blindness) Control as community directed treatment with ivermectin (CDTI). When communities are in charge, coverage is better than when ivermectin distribution is centrally organized by a health agency. The original 1995 CDI field testing showed better ivermectin coverage when the community was in charge of distribution. Since the beginning of CDTI, over 200,000 villages in 18 African countries have been distributing ivermectin annually through their own efforts. Lessons learned over the years are that CDI works best when 1) the smallest level of an organized community is the basis of action (e.g. a hamlet, a clan/kin group) and 2) communities are encouraged to choose as many CDDs as they think they need to get the job done. This means that the community is in charge, not individual volunteers who can be replaced anytime the community finds the need.
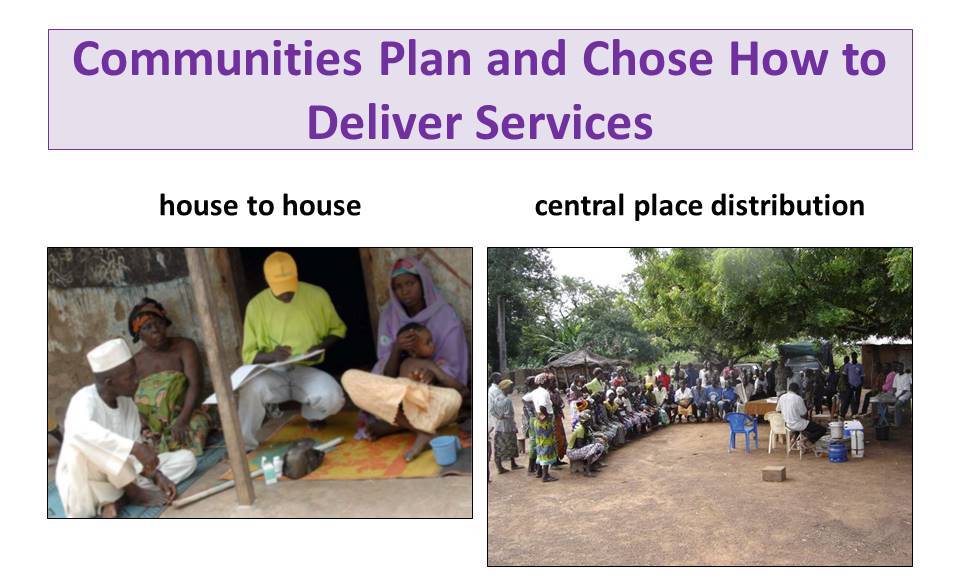
With CDI for onchocerciasis or any other health program, Communities plan and chose how to deliver services. This may be house-to-house, central place distribution or a combination. Health workers provide training and supervision to volunteer village health workers called community directed distributors (CDDs).
 TDR observed that CDI naturally expanded to include other services wanted by the community such as immunization, community development, water and sanitation, agriculture and forestry, HIV-AIDS, family planning, guinea worm, Vitamin A. TDR and APOC then decided that CDI with other service components should be systematically tested. The project sites added in a systematic manner other interventions to existing CDTI programs including home management of malaria, ITN distribution & promotion, TB DOTS, Vitamin A in addition to continued ivermectin distribution. These services varied in complexity and communities responded by dividing the work among several different volunteers.
TDR observed that CDI naturally expanded to include other services wanted by the community such as immunization, community development, water and sanitation, agriculture and forestry, HIV-AIDS, family planning, guinea worm, Vitamin A. TDR and APOC then decided that CDI with other service components should be systematically tested. The project sites added in a systematic manner other interventions to existing CDTI programs including home management of malaria, ITN distribution & promotion, TB DOTS, Vitamin A in addition to continued ivermectin distribution. These services varied in complexity and communities responded by dividing the work among several different volunteers.
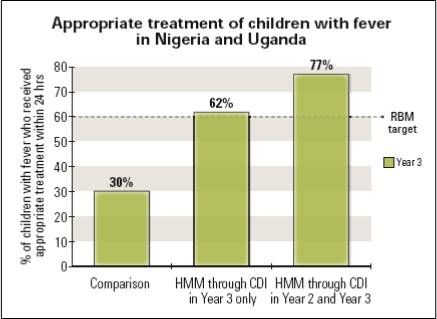 Coverage of interventions like malaria case management, ITN promotion and Vitamin A distribution was higher in the intervention areas compared to the delivery of these services through the routine health system. TB DOTS presented the only challenge because of the social stigma associated with the disease. The study concluded that CDI can effectively incorporate high impact, evidence based interventions while at the same time maintaining and increasing ivermectin coverage. Since CDI does not rely on one volunteer but whole community effort, the problem of overburdening on community health worker did not arise. Other incterventions ould benefit from CDI such as Misoprostol, Intermittent Preventive Treatment, Deworming, Oral Rehydration solution, Zinc, Cotrimoxazole, Amoxicillin, Soap for handwashing and WaterGuard treatment kits.
Coverage of interventions like malaria case management, ITN promotion and Vitamin A distribution was higher in the intervention areas compared to the delivery of these services through the routine health system. TB DOTS presented the only challenge because of the social stigma associated with the disease. The study concluded that CDI can effectively incorporate high impact, evidence based interventions while at the same time maintaining and increasing ivermectin coverage. Since CDI does not rely on one volunteer but whole community effort, the problem of overburdening on community health worker did not arise. Other incterventions ould benefit from CDI such as Misoprostol, Intermittent Preventive Treatment, Deworming, Oral Rehydration solution, Zinc, Cotrimoxazole, Amoxicillin, Soap for handwashing and WaterGuard treatment kits.
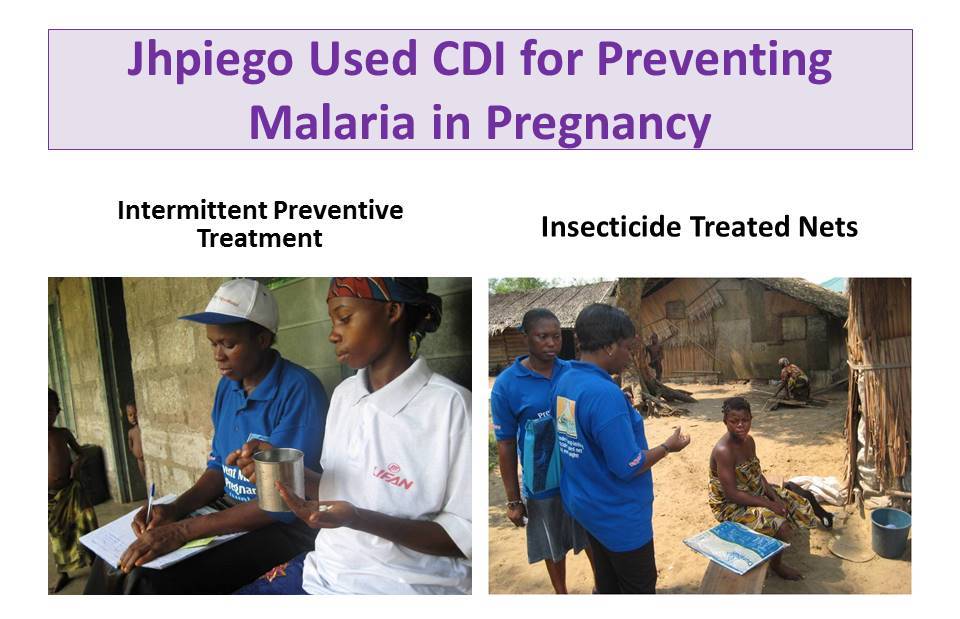 Jhpiego an NGO affiliate of the Johns Hopkins University used CDI to deliver malaria in pregnancy (MIP) prevention services in Nigeria including Intermittent Preventive Treatment and Insecticide Treated Nets. Contrary to fears that CDI would detract from antenatal care attendance, the work of CDDs actually ensured that ANC attendance increased over time. Through CDI IPTp coverage increased compared to control communities and more pregnant women slept under ITNs regularly.
Jhpiego an NGO affiliate of the Johns Hopkins University used CDI to deliver malaria in pregnancy (MIP) prevention services in Nigeria including Intermittent Preventive Treatment and Insecticide Treated Nets. Contrary to fears that CDI would detract from antenatal care attendance, the work of CDDs actually ensured that ANC attendance increased over time. Through CDI IPTp coverage increased compared to control communities and more pregnant women slept under ITNs regularly.
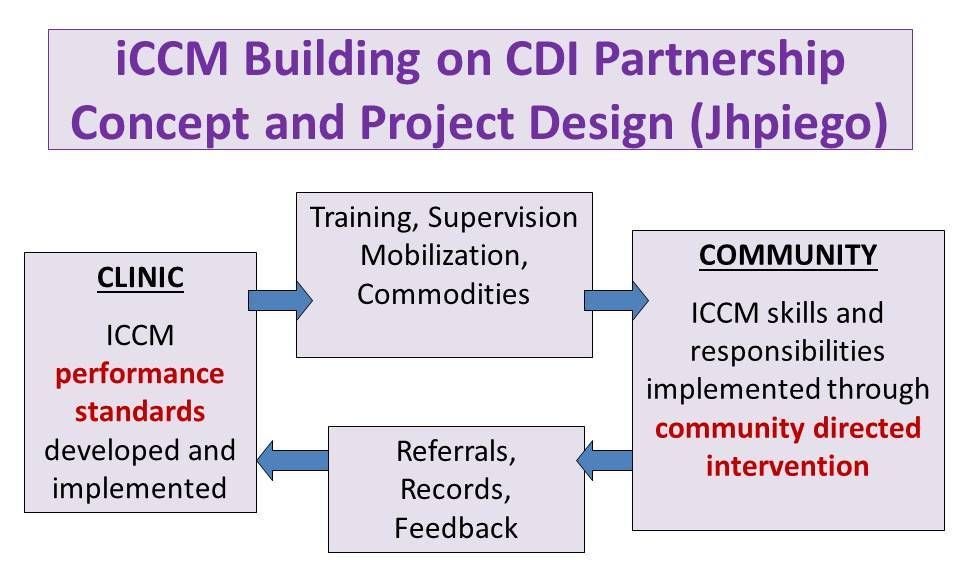 Jhpiego next expanded CDI for MIP into integrated Community Case Management (iCCM), thus taking community case management beyond community based care. Giving communities responsibility for organizing and managing their services using the CDI approach meant greater access to services whenever people need them. Using the CDI approach to iCCM CDDs reached 7,504 clients who presented signs and symptoms of malaria. CDDs successfully conducted malaria diagnosis using the rapid diagnostic test (RDT) kits. Overall, 47.8% tested positive while 52.2% tested negative. CDDs adhered to guidelines and all the 3,587 clients with positive RDT results received appropriate anti-malarial medicines. As appropriate 21.0% were treated for diarrhoea, 11.0% for pneumonia (of whom 68.0% were referred to the health facility)
Jhpiego next expanded CDI for MIP into integrated Community Case Management (iCCM), thus taking community case management beyond community based care. Giving communities responsibility for organizing and managing their services using the CDI approach meant greater access to services whenever people need them. Using the CDI approach to iCCM CDDs reached 7,504 clients who presented signs and symptoms of malaria. CDDs successfully conducted malaria diagnosis using the rapid diagnostic test (RDT) kits. Overall, 47.8% tested positive while 52.2% tested negative. CDDs adhered to guidelines and all the 3,587 clients with positive RDT results received appropriate anti-malarial medicines. As appropriate 21.0% were treated for diarrhoea, 11.0% for pneumonia (of whom 68.0% were referred to the health facility)
 A Supervisory Checklist and Performance Standards were developed and used for Assessing CDD performance. The results were discussed at monthly CDD meetings at their nearest health facilities. This led to further improvements in History taking, Examination, Conducting RDTs for Malaria and Illness Management.
A Supervisory Checklist and Performance Standards were developed and used for Assessing CDD performance. The results were discussed at monthly CDD meetings at their nearest health facilities. This led to further improvements in History taking, Examination, Conducting RDTs for Malaria and Illness Management.
TDR has done further scoping to learn if CDI would be acceptable by health workers and community members in Urban, Nomadic and Underserved Rural Communities. CDI was favorable received. In conclusion we have learned over the years that CDI can involve women, families and communities in meeting their own health needs.
Environment &IPTi Bill Brieger | 14 Jun 2013
Malaria and the Rains of Africa
The World Health Organization is guiding countries across the Sahel of Africa to begin piloting ‘seasonal malaria chemoprevention” or SMC. We recently featured this in the May 2013 issue of Africa Health. WHO explains that “Seasonal malaria chemoprevention is defined as the intermittent administration of full treatment courses of an antimalarial medicine to children during the malaria season in areas of highly seasonal transmission.” This is an outgrowth of several years of research into intermittent preventive treatment for infants (IPTi) and children.
 Malaria program managers wanted a more focused application of IPTi where it would be likely to make a major impact on disease control. Researchers found that areas meeting malaria seasonality definition of 60% of annual incidence within 4 consecutive months were observed more frequently in the Sahel and sub-Sahel than in other parts of Africa, and thus could provide an ideal focus for intervention.
Malaria program managers wanted a more focused application of IPTi where it would be likely to make a major impact on disease control. Researchers found that areas meeting malaria seasonality definition of 60% of annual incidence within 4 consecutive months were observed more frequently in the Sahel and sub-Sahel than in other parts of Africa, and thus could provide an ideal focus for intervention.
What makes transmission more intense in those four months is the rainy season. Ironically we have recently seen a more intense rainy season in the Sahel with serious flooding. IRIN reports that, “The African Centre of Meteorological Applications for Development (ACMAD) in a seasonal weather outlook says near-average or above-average rainfall is likely over the western Sahel, which stretches across Mauritania, Senegal and western and central Niger. These regions are ‘expected to be the area with the highest risk of above average number of extreme precipitating events that may lead to flash floods’.”
What does this flooding mean for SMC? While breeding mosquitoes obviously need the pools that rainwater creates, too much rain may have an opposite effect with flash floods washing out breeding sites (let alone homes and possessions). When flooding results in larger and longer collections of standing water, mosquito breeding may be enhanced, but this will make logistical support for training, supervision, and drug supplies extremely difficult in the region.
 The Sahel is one of the areas in Africa where we might hope for some early progress toward malaria elimination. With global climate changes affecting the region we can only wonder whether the weather will cooperate and allow timely implementation of new interventions. As IRIN implies – contingency planning is extremely important.
The Sahel is one of the areas in Africa where we might hope for some early progress toward malaria elimination. With global climate changes affecting the region we can only wonder whether the weather will cooperate and allow timely implementation of new interventions. As IRIN implies – contingency planning is extremely important.
IPTi Bill Brieger | 17 Sep 2009
Time to Give IPTi a Chance
![]() Eight years ago researchers in Tanzania discovered that giving a full dose of sulphadoxine-pyrimethamine (SP) to infants as intermittent preventive treatment (IPT) has similar positive effects of reduced malaria and anemia as the same process had already shown in pregnant women. This led to the formation of the IPTi Consortium whose aim was to amass the evidence needed so that international bodies could accept and develop guidelines for this life saving intervention.
Eight years ago researchers in Tanzania discovered that giving a full dose of sulphadoxine-pyrimethamine (SP) to infants as intermittent preventive treatment (IPT) has similar positive effects of reduced malaria and anemia as the same process had already shown in pregnant women. This led to the formation of the IPTi Consortium whose aim was to amass the evidence needed so that international bodies could accept and develop guidelines for this life saving intervention.
Although a variety of studies across Africa with support from UNICEF, the Gates Foundation and others have confirmed the benefits of IPTi, there has been reluctance by WHO to endorse this intervention. This may have been based on fears of rising parasite resistance to SP.
Today the Lancet has published a meta or pooled analysis of these IPTi Confortium sponsored studies from trials that were conducted in Mozambique, Gabon, Tanzania and Ghana. IPTi Consortium reports that, “SP has a protective efficacy of 30·3% (95% Confidence Intervals 19·8–39·4, p<0·0001) against clinical malaria, in areas of low to moderate resistance to SP during the first year of life.”
Researchers from the Consortium are realistic: “IPTi is not a ‘not a magic bullet‘ and noted that SP resistance has spread to several parts of Africa, which could limit the effectiveness of the IPTi using this drug. But the intervention could prevent 6 million cases of malaria each year among those most vulnerable to the disease.”
IPTi with SP has been proven not only efficacious, but relatively easy to deliver through infant immunization campaigns and routine immunization services. IPTi has also been shown to be acceptable to the community and parents of these infants. Also IPTi is cheap – about US $0.13-0.23 per dose.
While research will continue to find replacements for SP, there is no reason not to act now using this proven intervention to save lives. It is time for malaria partners and endemic country control programs to come together and operationalize these findings and begin saving lives until such time as a replacement medicine can be found of good efficacy and reasonable cost.
Countries must also remove SP from the shelves of shops and pharmacies where it is sold for treatment so that what remains of its efficacy can be protected until a replacement is found.
The IPTi Consortium is right that there is no magic bullet – this includes nets and treatment drugs, too. All possible and affordable strategies need to be employed to meet the 2015 Millennium Development Goals – saving children’s lives.
Health Systems &IPTi Bill Brieger | 22 Oct 2008
IPTi and EPI – healthy links
Recently we highlighted some lessons that malaria control efforts could learn from immunization program management, and observed that this was important because malaria control interventions such as ITN distribution have often been linked with immunization campaigns. Another link is use of the Expanded Program for Immunization (EPI) services as a delivery mechanism for intermittent preventive treatment for infants (IPTi).
Pool and colleagues have reported on the acceptability of EPI as a channel for IPTi delivery in Tanzania. The researchers concluded that, “In this setting, IPTi delivered together with EPI was generally acceptable. Acceptability was related to prior routinization of EPI [emphasis added] and resonance with traditional practices. Non-adherence was due largely to practical, social and structural factors, many of which could easily be overcome.”
 For example, mothers would have preferred drops instead of tablets for their infants. As with vaccines, mothers knowledge about the whole process was vague and generally consisted of an understanding that the process promoted health rather than controlled specific diseases. Structural factors related to poverty. Despite potential limitations, EPI appears to be a good platform for IPTi delivery.
For example, mothers would have preferred drops instead of tablets for their infants. As with vaccines, mothers knowledge about the whole process was vague and generally consisted of an understanding that the process promoted health rather than controlled specific diseases. Structural factors related to poverty. Despite potential limitations, EPI appears to be a good platform for IPTi delivery.
A review of the Demographic and Health Survey for Tanzania shows that the country has maintained a full immunization coverage rate of around 70% over the past 4 surveys (12 years), but that in the most recent survey (2004) at least 90% of infants had at last one EPI contact. This again speaks well for incorporating IPTi into an existing system that reaches most infants.
The DHS does show some other factors in EPI coverage that would also affect IPTi and reinforces structural factors as a concern. There was lower rural than urban immunization coverage. More educated and wealthier parents were more likely to get their infants immunized that less educated and poorer ones. DPT3 coverage in 2004 was only 75% for those in the lowest wealth quintile compared to 96% among those in the highest quintile.
These wealth/access disparities are no reason to dissociate IPTi from EPI, but they do emphasize the need for overall health reform so that disease prevention interventions equitably reach all children and families.