Borders &Conflict &COVID-19 &Ebola &Epidemic &One Health &Yellow Fever Bill Brieger | 10 May 2023
Outbreaks Emergency Preparedness And Response In Uganda
Solomon Afolabi, a graduating MPH student from the JHU Bloomberg School of Public Health examined the challenge of epidemics and outbreaks in Africa with special reference to Uganda as an example. The abstract of his report is found below.
According to the WHO, preparedness for emergency health conditions like infectious disease outbreaks should be an ongoing action supported by adequate funding, resources, partnerships, and political will that is executed at all levels to keep it sustained. Emergency preparedness is a framework that identifies practical in-country health emergency preparedness principles and elements by acknowledging lessons learned from previous response activities for priority planning, implementation, and reinforcing operational capacities.
 Uganda is an ecological hotspot for various infectious diseases making the country liable to outbreaks. In the last two decades, multiple significant outbreaks have occurred, prominent of which are from yellow fever, Ebola virus disease, and COVID-19 global pandemic. Efforts to build a strategic framework for emergency outbreak preparedness and to strengthen the national operational capacity led to the establishment of the Ugandan National Institute of Public Health (UNIPH) in 2013.
Uganda is an ecological hotspot for various infectious diseases making the country liable to outbreaks. In the last two decades, multiple significant outbreaks have occurred, prominent of which are from yellow fever, Ebola virus disease, and COVID-19 global pandemic. Efforts to build a strategic framework for emergency outbreak preparedness and to strengthen the national operational capacity led to the establishment of the Ugandan National Institute of Public Health (UNIPH) in 2013.
This paper presents a blend of literature that takes account of the successes, challenges faced, and gaps identified in the preparedness and response capacities to the infectious disease outbreaks experienced in the last two decades. It also reviewed how the national efforts had fared in operational readiness for an emergency response to epidemics, building a resilient health system, practicing the One-Health human-animal-environment interface, and in government, community, and individual capacities to contribute effectively to strengthen the national emergency preparedness and response to these frequent disease outbreaks. The findings revealed that Uganda’s outbreak preparedness had made much progress over two decades, from the overwhelming Sudan strain Ebola virus outbreak in 2000-2001 to a similar episode from the same species in 2022 to 2023.
The response measures that feature the activation of a national response plan by the MoH were well coordinated locally to swiftly lead to the activation of NTF, NRRT, DTF, DRRT, and VHTs for immediate mobilization and deployment of operational resources to affected districts. The response was strengthened by well-organized local coordination by the MoH and development partners (WHO, CDC, UN agencies, etc.). The immediate setting up of treatment and isolation centers, provision of Ebola kits, training of more health workers, and coverage of 10 high-risk districts ensured a significant impact.
The provision of more than 5000 doses of vaccines with the support of WHO and partners was a global capacity milestone impact, and the country was declared Ebola-free in a record 69 days. Uganda’s current national emergency preparedness and response plan has received commendations locally and from global international partners, having progressively built capacity from lessons learned in just over a decade of responding to frequent infectious disease outbreaks and using the recommendations proffered accordingly.
This sustained momentum of preparedness supported the swift transition to contain COVID-19 and laid a good foundation for their strengthened readiness for an emergency response to outbreaks.
Conflict &ITNs Bill Brieger | 30 Oct 2022
Insecticide Treated Mosquito Nets in Conflict-Affected Fragile States
Marwa Ramadan of the Alexandria Faculty of Medicine, Alexandria, Egypt and William Brieger of the Johns Hopkins Bloomberg School of Public Health are presenting this information at the Annual Meeting of the American Society of Tropical Medicine and Hygiene in Seattle.
 Studies have highlighted the potential impact of conflict and displacement on malaria prevention and mitigation efforts, but few investigated the effect of subnational conflict intensity on access and utilization of mosquito nets in fragile countries.
Studies have highlighted the potential impact of conflict and displacement on malaria prevention and mitigation efforts, but few investigated the effect of subnational conflict intensity on access and utilization of mosquito nets in fragile countries.
This study bridges the gap by applying a conflict intensity lens to the analysis of access and utilization of Insecticide Treated Nets (ITN) in two conflict-affected fragile states (Nigeria and Democratic Republic of Congo (DRC)), where at least 45 % of global malaria deaths occur.
We used the Demographic health survey (DHS) and the Uppsala Conflict Data Program for information on access and utilization of nets and conflict events respectively. Access was defined as the percentage of population with at least one ITN per 2 household members, while utilization was defined as the percentage of population who slept under an ITN the night before the survey in households with at least 1 ITN.
To define conflict intensity, we linked household clusters to conflict events within a 50 km distance using ArcGIS. Conflict intensity was then categorized into medium or high intensity conflict and no or low intensity conflict using a cut-off of 2 or more deaths per 100, 000 population per cluster. Access and utilization of ITNs was compared by conflict intensity at the household cluster level.
Analysis of data from 281,689 individuals living in 58,183 households revealed that 42.8% (CI: 42.3 – 43.3%) and 39.9% (CI: 39.5 – 40.1%) of members living in neighborhoods with medium and high intensity conflict in DRC and Nigeria respectively had access to ITNS compared to 47.9% (CI: 47.6 – 48.1%) and 51.0% (CI: 50.8 – 51.2%) in no or low intensity conflict.
Similarly, 65.1% (CI: 64.3 – 65.9%) and 62.8% (CI: 62.3 – 63.3%) of those living in medium or high intensity conflict in DRC and Nigeria respectively utilized ITNS compared to 69.2 % (CI: 68.8 %-69.6 %) and 65.7% (CI: 65.4-66.0%) in no or low intensity conflict.
National malaria control programs must consider that access and utilization of ITNS are statistically significantly lower in neighborhoods with medium or high intensity conflict and target supporting interventions accordingly.
Capacity Building &Conflict &Health Systems &Integration Bill Brieger | 07 Sep 2020
Malaria News Today 2020-09-07
Today’s updates are brief and look at Vietnam in Southeast Asia and South Sudan in Africa. Both are concerned with health systems issues. Please click on links to read more details.
Malaria Week 2020 – Why Integration Could Be the Key to Elimination
Hosted by the Government of Vietnam, Malaria Week 2020 (7-11 September) brings together government officials and diverse partners to drive forward the elimination of malaria from Asia Pacific by 2030. This year’s theme centres on the three I’s – Inclusion. Integration. Innovation – and captures the ambition to unite the region and harness innovation as efforts intensify to eradicate malaria globally and in Asia Pacific. Key topics in the series this week include surveillance systems, sustaining health financing, and innovation within the malaria landscape.
Given the backdrop of COVID-19 to this year’s event, discussions will have a focus on sustaining health financing and in particular malaria interventions during a pandemic, the critical role of community-based approaches in health systems strengthening and the need for strong surveillance and timely reporting, in addition to the role of innovation and private provider engagement in accelerating malaria elimination and strengthening health security.
Healthcare in South Sudan: A Fractured System
A limited access to healthcare facilities, medical supplies in South Sudan results in high number of preventable deaths. high rates of tuberculosis, HIV/AIDS, malaria, and diarrheal diseases in country.
The South Sudanese population has very limited access to healthcare facilities, with only 44% of the population living within a one-hour walk of a medical center. This adds an extra burden on those in need of medical attention as the majority of the population has to walk for an extended time to reach a medical center. During a time of civil unrest, traveling for an extended period comes with increased exposure to the risk of ambushes and looting.
Conflict &Diagnosis &Ebola &ITNs &Mosquitoes &Plasmodium/Parasite &Resistance &Vaccine Bill Brieger | 29 Jul 2019
Tropical Health Update 2019-07-28: Ebola and Malaria Crises
This posting focuses on Malaria and Ebola, both of which have been the recent focus of some disturbing news. The malaria community has been disturbed by the clear documentation of resistance to drugs in Southeast Asia. Those working to contain Ebola in the northeast of the Democratic Republic of Congo saw a change in political leadership even in light of continued violence and potential cross-border spread.
Malaria Drug Resistance
Several sources reported on studies in the Lancet Infectious Diseases concerning the spread of Multidrug-Resistant Malaria in Southeast Asia. Reuters explained that by sing genomic surveillance, researchers concurred that “strains of malaria resistant to two key anti-malarial medicines are becoming more dominant” and “spread aggressively, replacing local malaria parasites,” becoming the dominant strains in Vietnam, Laos and northeastern Thailand.”
 The focus was on “the first-line treatment for malaria in many parts of Asia in the last decade has been a combination of dihydroartemisinin and piperaquine, also known as DHA-PPQ,” and resistance had begun to spread in Cambodia between 2007 and 2013. Authors of the study noted that while, “”Other drugs may be effective at the moment, but the situation is extremely fragile, and this study highlights that urgent action is needed.” They further warned of an 9impending Global Health Emergency.
The focus was on “the first-line treatment for malaria in many parts of Asia in the last decade has been a combination of dihydroartemisinin and piperaquine, also known as DHA-PPQ,” and resistance had begun to spread in Cambodia between 2007 and 2013. Authors of the study noted that while, “”Other drugs may be effective at the moment, but the situation is extremely fragile, and this study highlights that urgent action is needed.” They further warned of an 9impending Global Health Emergency.
NPR notes that “Malaria drugs are failing at an “alarming” rate in Southeast Asia” and provided some historical context about malaria drug resistance arising in this region since the middle of the 20th century. “Somehow antimalarial drug resistance always starts in that part of the world,” says Arjen Dondorp, who leads malaria research at the Mahidol Oxford Tropical Medicine Research Unit in Bangkok and who was a lead author of the report about the randomized trial. Ironically, “one reason could have something to do with the relatively low levels of malaria there. When resistant parasites emerge, they are not competing against a dominant nonresistant strain of malaria and are possibly able to spread easier.
When we are talking about monitoring resistance in low resource and logistically and politically challenging areas, we need to think of appropriate diagnostic tools at the molecular level. Researchers in Guinea-Bissau conducted a proof of concept study and used malaria rapid diagnostic tests applied for parallel sequencing for surveillance of molecular markers. While they noted that, “Factors such as RDT storage prior to DNA extraction and parasitaemia of the infection are likely to have an effect on whether or not parasite DNA can be successfully analysed … obtaining the necessary data from used RDTs, despite suboptimal output, becomes a feasible, affordable and hence a justifiable method.”
A Look at Insecticide Treated Nets
On a positive note, Voice of America provides more details on the insecticide treated net (ITN) monitoring tool developed called “SmartNet” by Dr Krezanoski in collaboration with the Consortium for Affordable Medical Technologies in Uganda. The net uses strips of conductive fabric to detect when it’s in use. Dr. Krezanoski was happy to find that people given the net used it no differently that if they were not being observed. The test nets made it clear who what using and not using this valuable health investment and when it was in use. Such fine tuning will be deployed to design interventions to educate net users based on their real-life use patterns.
Another important net issue is local beliefs that may influence use. We can find out when people use nets, but we also need to determine why. In Tanzania, researchers found that people think mosquitoes that bite in the early evening when people are outside relaxing are harmless. As one community member said, “I only fear those that bite after midnight. We’ve always been told that malaria is spread by mosquitoes that bite after midnight.”
Even if people do use their ITNs correctly, we still need to worry about insecticide resistance. A study in Afghanistan reported that, “Resistance to different groups of insecticides in the field populations of An. stephensi from Kunar, Laghman and Nangarhar Provinces of Afghanistan is caused by a range of metabolic and site insensitivity mechanisms.” The authors conclude that vector control programs need to be better prepared to implement insecticide resistance management strategies.
Ebola Crisis Becomes (More) Political
Headlines such as “Congo health minister resigns over response to Ebola crisis” confronted the global health community this week. this happened after the DRC’s relatively new president took control of the response. The President set up a new government office to oversee the response to an outbreak outside of the Ministry of Health which was managing the current outbreak and the previous ones. The new board was set up without the knowledge of the Minister who was traveling to the effected provinces at the time.
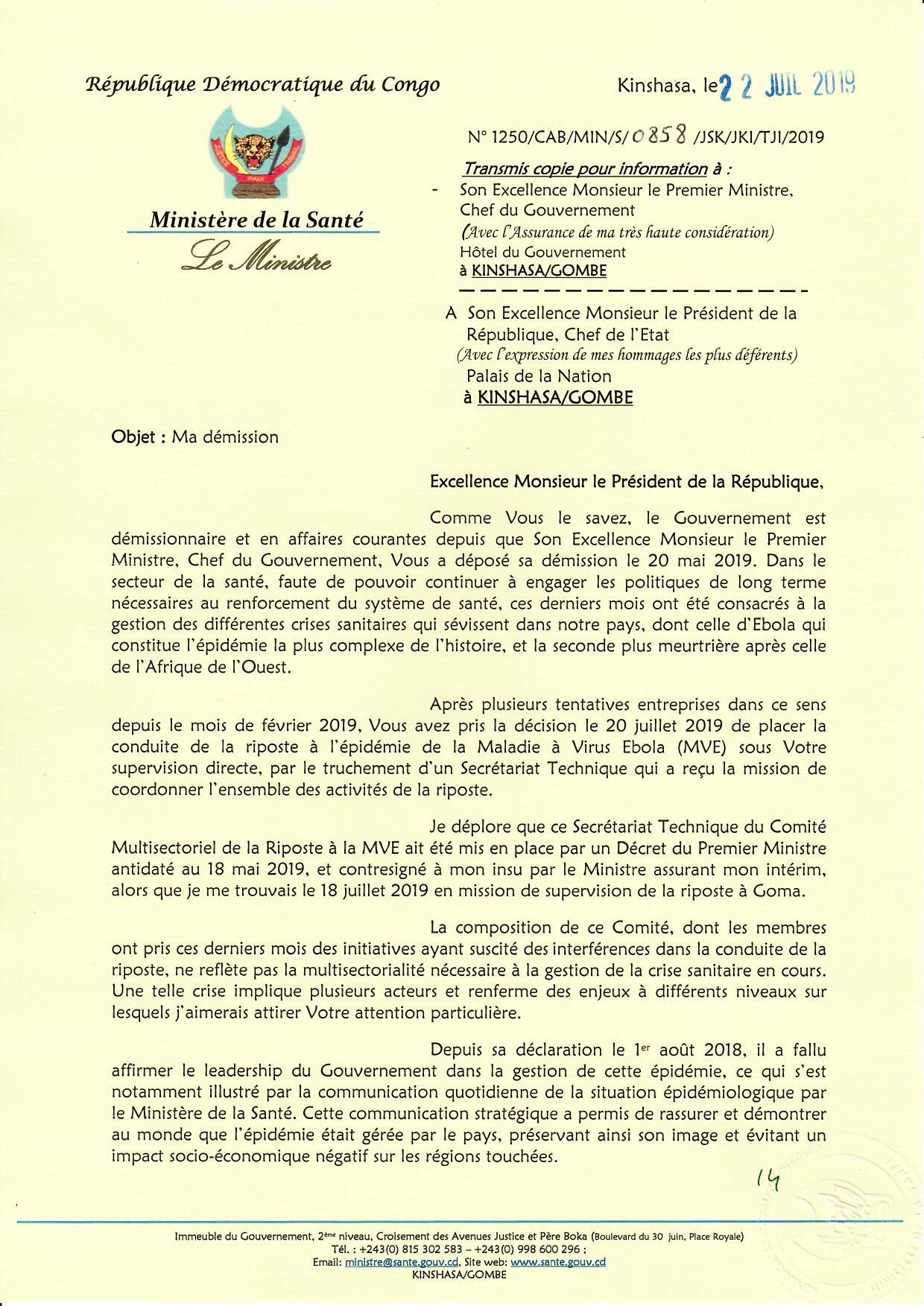 The former Minister, Dr Oly Ilunga stated on Twitter that, “Suite à la décision de la @Presidence_RDC. de gérer à son niveau l’épidémie d’#Ebola, j’ai remis ma démission en tant que Ministre de la Santé ce lundi. Ce fut un honneur de pouvoir mettre mon expertise au service de notre Nation pendant ces 2 années importantes de notre Histoire. (Following the decision of the @Presidence_RDC to manage the # Ebola outbreak, I resigned as Minister of Health on Monday. It was an honor to be able to put my expertise at the service of our Nation during these two important years of our History.)
The former Minister, Dr Oly Ilunga stated on Twitter that, “Suite à la décision de la @Presidence_RDC. de gérer à son niveau l’épidémie d’#Ebola, j’ai remis ma démission en tant que Ministre de la Santé ce lundi. Ce fut un honneur de pouvoir mettre mon expertise au service de notre Nation pendant ces 2 années importantes de notre Histoire. (Following the decision of the @Presidence_RDC to manage the # Ebola outbreak, I resigned as Minister of Health on Monday. It was an honor to be able to put my expertise at the service of our Nation during these two important years of our History.)
 The former Minister also warned that the “Multisectoral Ebola Response Committee would interfere with the ongoing activities of national and international health workers on the ground in North Kivu and Ituri provinces.” Part of the issue may likely have been “pressure to approve a new vaccine in addition to one that has already been used to protect more than 171,000 people.” People had warned about the potential confusion to the public as well as ethical issues if a second vaccine was used, especially one that did not have the strong accumulated evidence from both the current outbreak as well as the previous one in West Africa.
The former Minister also warned that the “Multisectoral Ebola Response Committee would interfere with the ongoing activities of national and international health workers on the ground in North Kivu and Ituri provinces.” Part of the issue may likely have been “pressure to approve a new vaccine in addition to one that has already been used to protect more than 171,000 people.” People had warned about the potential confusion to the public as well as ethical issues if a second vaccine was used, especially one that did not have the strong accumulated evidence from both the current outbreak as well as the previous one in West Africa.
One might have thought that this would be a time when stability was needed since “The WHO earlier this month declared the outbreak a Public Health Emergency of International Concern, a rare step meant to highlight the urgency of the moment that has been used only four times before.” In addition, “the World Bank said it would release $300 million from a special fund set aside for crises like viral outbreaks to help cover the cost of the response.”
Unfortunately one of the msain impediments to successful Ebola control, violence in the region, continues. CIDRAP stated that. “the Allied Democratic Forces (ADF), a rebel group, attacked two villages near Beni, killing 12 people who live in the heart of the Democratic Republic of the Congo’s (DRC’s) ongoing Ebola outbreak. The terrorists killed nine in Eringeti and three in Oicha, according to Reuters. ADF has not publicly pledged allegiance to the Islamic state (ISIL), but that hasn’t stopped ISIL from claiming responsibility for the attacks.” It will take more than a change of structure in Kinshasa to deal with the realities on the ground.
 CIDRAP also observed that since the resignation of the Health Minister, “DRC officials have provided no update on the outbreak, including statistics on the number of deaths, health workers infected, or suspected cases.” The last was seen on 21 July 2019.
CIDRAP also observed that since the resignation of the Health Minister, “DRC officials have provided no update on the outbreak, including statistics on the number of deaths, health workers infected, or suspected cases.” The last was seen on 21 July 2019.
ReliefWeb reports that, “Adding to the peril, the Ebola-affected provinces share borders with Rwanda and Uganda, with frequent cross-border movement for personal travel and trade, increasing the chance that the virus could spread beyond the DRC. There have already been isolated cases of Ebola reported outside of the outbreak zone.”
These are troubling times when parasites and mosquitoes are becoming more resistant to our interventions and when governments and communities are resistant to a clear and stable path to disease containment and control.
Advocacy &Borders &Children &Conflict &Costs &Epidemiology &Funding &Human Resources &Leadership &Monitoring &Mortality &NTDs &Partnership &Surveillance Bill Brieger | 03 Feb 2018
African Leaders Malaria Alliance Recognizes Country Achievements, Adds NTDs to its Scorecard
 The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
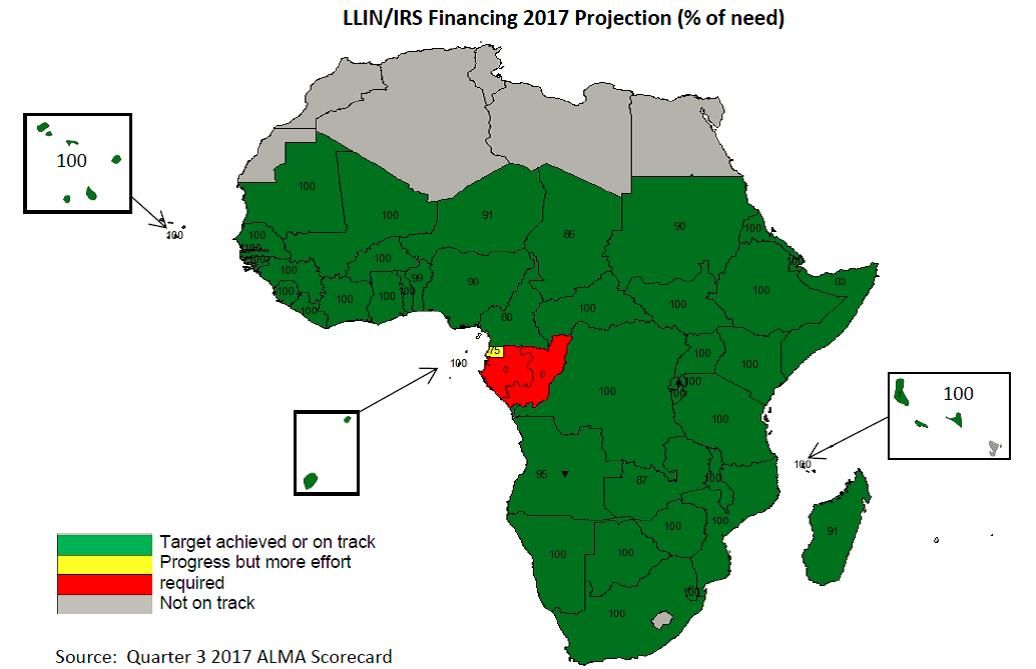
 For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
The scorecard will now “report progress for the 47 NTD-affected countries in sub-Saharan Africa in their strategies to treat and prevent the five most common NTDs: lymphatic filariasis, onchocerciasis, schistosomiasis, soil-transmitted helminths and trachoma. By adding NTDs to the scorecard, African leaders are making a public commitment to hold themselves accountable for progress on these diseases.”
 In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
The combination is based on the logic that NTDs and malaria are both diseases of poverty. Malaria and several NTDs are also vector-borne. Also community platforms are a foundation for delivering needed drugs and supplies to tackle these diseases. Ultimately the decision shows that Heads of State are holding themselves accountable for progress in eliminating these diseases.
 At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
 The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
H.E . Dr. Barnabas Sibusiso Dlamini, the Prime Minister of the Kingdom of Swaziland, whose King and Head of State is the current chair of ALMA, warned all endemic countries that, “When we take our eyes off malaria, the cost for our countries is huge. Yet if we increase our efforts to control and eventually eliminate malaria, the yield we get from it is tremendous. It is time that we dig deep into our pockets and provide malaria programmes with the needed resources.”
 Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
IRIN concludes that, “For now, the biggest challenge for Zambia will be closing the gap in its malaria elimination strategy, which will cost around $160 million a year and is currently only about 50 percent funded – two thirds from international donors and one third from the Zambian government. Privately, international donors say the government must spend more money on its malaria programme if it is to succeed.” Cross-border transmission adds to the problem.
Internal strife is another challenge to malaria success. “The recent nurses’ strike which lasted for five months may have cost Kenya a continental award in reducing the prevalence of malaria during the 30th African Union Summit in Ethiopia on Sunday.” John Muchangi in the Star also noted that, “However, Kenya lost momentum last year and a major malaria outbreak during the prolonged nurses’ strike killed more than 30 people within two weeks in October.”
 Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Fortunately ALMA is equipped with the monitoring and advocacy tools to ensure that its members recognize and respond to such challenges. The Scorecards will keep the fight against the infectious diseases of poverty on track.
Conflict &Emergency &Mortality Bill Brieger | 31 May 2016
Malaria, War and Death
In wars in malaria endemic areas, malaria can cause more damage than what occurs on the battlefield. The United States just observed its annual Memorial Day where those who died serving the country are remembered. Wing Beats, the journal of the Florida Mosquito Associations reported on the status of malaria vectors in the state of Georgia and stressed the damage malaria did during the US Civil War:
- “From 1861 to1866 malaria was the second most commonly diagnosed ailment – diarrhea/dysentery was first – among Union troops, with over 1.3 million cases. Although sold iers native to the South were much more likely to have experienced malaria growing up, they also suffered deaths and incapacitation that affected the timing and outcome of battles.”
 During the Korean conflict, “paragonimiasis, malaria, and amoebiasis were the most fatal parasitic diseases during the early 1950s in the Korean Peninsula,” and consequently were responsible for deaths of prisoners of war. The U.S. military received a severe damage during World War II in the Pacific where it was said that “more soldiers were lost by malaria than by battle itself.” The experience led to hundreds of units specialized in controlling malaria in Korea.
During the Korean conflict, “paragonimiasis, malaria, and amoebiasis were the most fatal parasitic diseases during the early 1950s in the Korean Peninsula,” and consequently were responsible for deaths of prisoners of war. The U.S. military received a severe damage during World War II in the Pacific where it was said that “more soldiers were lost by malaria than by battle itself.” The experience led to hundreds of units specialized in controlling malaria in Korea.
In Europe during World War II, people in concentration camps and prisoners of war were used in experiments. “In Dachau Professor Claus Schilling tested synthetic malaria drugs and injected helpless prisoners with high and sometimes lethal doses.” Malaria as a biological warfare agent was demonstrated in Italy where “The German army’s 1943 flooding of the Pontine Marshes south of Rome, which later caused a sharp rise in malaria cases among Italian civilians, has recently been described by historian Frank Snowden as a unique instance of biological warfare and bioterrorism.”
Today malaria continues to produce death in conflict zones. “The area of Walikale in North Kivu, Democratic Republic of Congo, is intensely affected by conflict and population displacement.” The most frequently reported cause of death among the local population was fever/malaria at 34.1% .
During the civil war in Côte d’Ivoire “the availability and use of protective measures against mosquito bites and accessibility to health care infrastructure deteriorated.” A study of resettlement camps of displaced families after the Angolan civil war “Malnutrition was the leading cause of death (34%), followed by fever or malaria (24%) and war or violence (18%).”
Some of the most highly malaria endemic countries in the world still experience conflicts. Malaria kills directly, it can be used as a weapon, and war disrupts efforts to control it. If we are to “end malaria for good,” we might also think about trying to end war and conflict, too.