Asymptomatic &Elimination &Eradication &Monkeys &Mosquitoes &Resistance &Vaccine Bill Brieger | 23 Aug 2019
Biology and Malaria Eradication: Are there Barriers?
During a press conference prior to the release of the executive summary of 3-year study of trends and future projections for the factors and determinants that underpin malaria by its Strategic Advisory Group on Malaria Eradication (SAGme), WHO outlined some hopeful signs emanating from the SAGme including
- Lack of biological barriers to malaria eradication
- Recognition of the massive social and economic benefits that would provide a return on investment in eradication, and
- Megatrends in the areas of factors such as land use, climate, migration, urbanization that could inhibit malaria transmission
 Concerning the first point, the executive summary notes that, “We did not identify biological or environmental barriers to malaria eradication. In addition, our review of models accounting for a variety of global trends in the human and biophysical environment over the next three decades suggest that the world of the future will have much less malaria to contend with.”
Concerning the first point, the executive summary notes that, “We did not identify biological or environmental barriers to malaria eradication. In addition, our review of models accounting for a variety of global trends in the human and biophysical environment over the next three decades suggest that the world of the future will have much less malaria to contend with.”
The group did agree that, “using current tools, we will still have 11 million cases of malaria in Africa in 2050.” So one wonders whether there are biological barriers or not.
Interestingly the group did identify, “Potential biological threats to malaria eradication include development of insecticide and antimalarial drug resistance, vector population dynamics and altered vector behaviour. For example, Anopheles vectors might adapt to breeding in polluted water, and mosquito vector species newly introduced to Africa, such as Anopheles stephensi, could spread more widely into urban settings.”
This discussion harkens back to an important conceptual article by Bruce Aylward and colleagues that raised the question in the American Journal of Public Health, “When Is a Disease Eradicable?” They outlined three important criteria that had been proposed at two international conferences in 1997 and 1998.
- biological and technical feasibility
- costs and benefits, and
- societal and political considerations
Their further expansion on the biological issues using smallpox as an example is instructive. They noted that not only are humans essential for the life cycle of the organism, but that there was no other reservoir for the causative virus, and the virus could not amplify in the environment. In short, there were no vectors, as in the case of malaria. The relatively recent documentation of transmission of malaria between humans and other primates of different plasmodium species is another biological concern. At this point, Malaysia, for example, is reporting more cases of Plasmodium knowlesi in humans that either P vivax or P falciparum.
Another biological issue identified by Aylward and colleagues was the fact that smallpox had one effective and proven intervention, the vaccine. Application of the vaccine could be targeted using photograph disease recognition cards as the signs were quite specific to the disease. Malaria has several effective interventions, but most strategies emphasize the importance of using a combination of these, and implementation is met with a number of management and logistical challenges. The signs and symptoms of malaria are confused with a number of febrile illnesses.
Finally, two other issues raised concern. Insecticide resistance was recognized in the first malaria eradication effort, and is raising its head again, as pointed out by SAGme. Comparing smallpox and yaws, the challenge of latent or sub-clinical/asymptomatic infection was mentioned. Malaria too, is beleaguered with this problem.
Clearly, we must not lose momentum in the marathon (not a race) to eliminate malaria, but we must, as WHO stressed at the press conference, increase our research and development efforts to strengthen existing tools and develop new once to address the biological and logistical challenges.
Cholera &Vaccine Bill Brieger | 19 Aug 2019
Doubling a Cholera Response: Applying a single-dose OCV strategy to outbreak control in South Sudan

91,000 people die from cholera every year. Cholera is a burden which is carried by some of the poorest and most vulnerable people in the world. This disease, which puts about 1.4 billion people at risk annually, is most predominant in low-income nations. One of these nations is South Sudan. Since its independence in 2011, South Sudan has been plagued by ongoing conflict, displacements, poverty, and disease outbreaks. In South Sudan’s most recent cholera outbreak, there were already 20,000 cases before the outbreak could be brought under control.
Controlling a cholera outbreak requires a combination of approaches; water and sanitation, hygiene promotion, case management, and reactive vaccination campaigns. The oral cholera vaccine (OCV) revolutionized cholera responses and made it possible protect people from this dangerous disease. OCV campaigns are still incredibly resource intense and traditionally target each person with 2-doses of the vaccine. In places like South Sudan, even reaching these people once is difficult, finding them a second time requires a great deal of motivation, resources, and creativity. In the rainy season, large swaths of South Sudan are flooded and become swamps. This is also the time of year that people are most at risk of cholera. A vaccination campaign requires vaccination teams to literally walk through the swamps for hours, or even days, to reach the affected areas.

Fortunately, a more streamlined approach is possible, and has even been tested in emergency cholera responses in South Sudan. There is a growing body of evidence that supports a single-dose strategy for OCV campaigns. In settings where cholera is endemic, like South Sudan, a single dose of OCV can be as effective as 2 doses for controlling an outbreak. Adopting this strategy would allow the same amount of vaccine to protect double the amount of people. It would also save on the logistical costs of trying to reach each person twice. While a second dose of cholera vaccine makes sense for routine immunization programs because it provides prolonged coverage, it is costly and limiting to an emergency response. In a cholera outbreak, the State Ministries of Health may look to a single-dose strategy to more efficiently control the outbreak and protect their people.
Polio &Vaccine Bill Brieger | 19 Aug 2019
Recent Surge in Polio Cases in Pakistan Necessitates Urgent Review of Strategy
As part of the course on Social and Behavioral Foundations in Primary Health Care, Muhammad N Asghar posted in the class blog. We have shared these thoughts below.
 Pakistan is one of the three polio endemic countries and recent surge in cases shows that eradication of the disease demands an urgent change in strategy. A look at previous five year cases in Pakistan shows a positive progress in reduction of new polio cases; from 307(2014) to 12(2018), but new cases still appeared in almost every province. The reasons behind this country wide presence of disease can be attributed to internal displacement due to conflicts, weak health systems and operational and resource risks. But the alarming increase in number of new polio cases during 2019 has reversed the whole progress made so far as the number of new cases as of today stands at 53. 32 out of 53 cases are reported from KPK region, which had observed massive internal displacement during last decade but the number of IDPs has decreased from last two years due to stability in the region.
Pakistan is one of the three polio endemic countries and recent surge in cases shows that eradication of the disease demands an urgent change in strategy. A look at previous five year cases in Pakistan shows a positive progress in reduction of new polio cases; from 307(2014) to 12(2018), but new cases still appeared in almost every province. The reasons behind this country wide presence of disease can be attributed to internal displacement due to conflicts, weak health systems and operational and resource risks. But the alarming increase in number of new polio cases during 2019 has reversed the whole progress made so far as the number of new cases as of today stands at 53. 32 out of 53 cases are reported from KPK region, which had observed massive internal displacement during last decade but the number of IDPs has decreased from last two years due to stability in the region.
 This recent surge in polio cases in the the province is mainly due to increase in vaccine refusals due to rumors regarding side effects caused by the vaccine on social media. Official sources reported that after rumors refusals to vaccinate increased by 85% in the province. But high number of cases in other provinces when compared with last year cases indicate that multiple factors are hindering the progress towards containment and eradication of the polio virus disease from the country, which can be attributed to homelessness and poor sanitation, operational issues for vaccine delivery, conflicts, cross border movement etc.
This recent surge in polio cases in the the province is mainly due to increase in vaccine refusals due to rumors regarding side effects caused by the vaccine on social media. Official sources reported that after rumors refusals to vaccinate increased by 85% in the province. But high number of cases in other provinces when compared with last year cases indicate that multiple factors are hindering the progress towards containment and eradication of the polio virus disease from the country, which can be attributed to homelessness and poor sanitation, operational issues for vaccine delivery, conflicts, cross border movement etc.
This situation demands urgent review of existing strategy for polio eradication as number of new cases are increasing rapidly. There is a need to work on multiple aspects to make the anti-polio drive successful; some key aspects include detailed geo-mapping of the population at basic level and identification of missed areas to ensure every child is vaccinated, involving community and religious leaders, NGOs, CSOs for confidence building and education of the community, expansion of partnership with nutrition, hygiene, water sectors, and robust rebuttal of rumors and strict action against those involved in such heinous activities etc. There is a new political government of helm, which is sensitive to the social sector issues and taking measures to provide homes, health facilities and education to the disadvantaged sections. International agencies (GPEI, WHO) shall coordinate with the political government to review the existing strategy for revamping it, so that not only the current surge can be contained but the disease can be eradicated from the country to achieve the target of polio free world.

Borders &Ebola Bill Brieger | 18 Aug 2019
Ebola Crisis Takes a Turn: Increased US Intervention Necessary
As part of the course on Social and Behavioral Foundations in Primary Health Care, Allan Ciciriello posted in the class blog. We have shared his thoughts below.

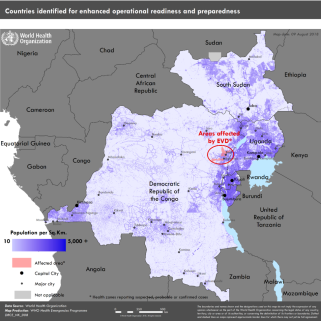
Historically, the 2018 – 2019 Ebola outbreak is the biggest the Democratic Republic of the Congo has ever seen. As a whole, it is also the second largest documented epidemic of the disease on record. The epicenter of the eruption is located in the Kivu region, which has also been in the midst of a conflict between the Congolese military and rebel groups, which has prevented necessary assistance from making its way into the country. Due to the decline of the situation over the past year, culminating with a confirmed case of Ebola in the capital city of Goma, the World Health Organization officially announced it as a Public Health Emergency of International Concern in July 2019.
The spread of the virus to bordering countries is a matter of great importance in the global health community. This includes the nations of Burundi, Rwanda, South Sudan, and Uganda. Given that Goma is a major transportation hub connecting these territories together, it is imperative that the transmission of Ebola be stopped quickly in the Kivu region.
The United States must change its current policies on intervening in the Democratic Republic of the Congo Ebola outbreak. Most important is contributing additional funding to sustain the World Health Organization’s role in halting the spread of the virus within the current borders, while also supporting the surrounding nations’ prevention efforts. USAID is a critical source of backing in this ongoing battle, and without them it is likely to falter. I would also reconsider the hesitancy of placing United States government personnel on the frontlines, because as the problem gets more dire the harder it will be to act from within the country. The CDC is another key player in this game, and I would advise the US take advantage of the United Nations Organization Stabilization Mission in the Democratic Republic of the Condo’s (also known as MONUSCO) peacekeeping forces to get public health workers back on the frontline with guaranteed protection from rebel militias.
Borders &Diagnosis &Ebola &Elimination &Integrated Vector Management &ITNs &Mosquitoes &NTDs &Snakebite &Trachoma &Urban Bill Brieger | 04 Aug 2019
Tropical Health Update 2019-08-04: Ebola, Malaria Vectors, Snakebite and Trachoma
In the past week urban transmission in Goma, a city of at least 2 million inhabitants in eastern Democratic republic of Congo, was documented as a gold miner came home and infected his wife and child. To get a grip on the spread of the disease, DRC is considering another vaccine, not without some controversy. WHO provides detailed guidance on all aspects of response. On the malaria front we have learned more about malaria vectors, natural immunity and reactive case detection.
Ebola Challenges: Vaccines, Urban Transmission
 The current Ebola vaccine being deployed to over 150,000 people in North Kivu and Ituri Provinces was itself an experimental intervention during 2016 when it was first used in the largest ever outbreak located in West Africa. BBC reports that, “World Health Organization (WHO) data show the Merck vaccine has a 97.5% efficacy rate for those who are immunised, compared to those who are not.”
The current Ebola vaccine being deployed to over 150,000 people in North Kivu and Ituri Provinces was itself an experimental intervention during 2016 when it was first used in the largest ever outbreak located in West Africa. BBC reports that, “World Health Organization (WHO) data show the Merck vaccine has a 97.5% efficacy rate for those who are immunised, compared to those who are not.”
The proposed addition of a Johnson and Johnson vaccine would be in that same experimental phase if introduced in DRC now. It has been proven safe as well as effective in other primates. The challenge is that even though the Merck vaccine supplies are near 500,000, this is not enough to cover the potential needs in an area with over 10 million people, although Merck is still producing more. At present, BBC says, “Those pushing for the use of the new Johnson & Johnson vaccine, had proposed using it to create a protective wall, vaccinating people outside the outbreak zone.” In addition, the new national response team is concerned that “Only about 50% of cases of Ebola in the Democratic Republic of Congo are being identified.”
Finally, there is the issue of community mistrust of government workers and challenging logistics. “There are also concerns that the new vaccine – which requires two injections 56 days apart – may be difficult to administer in a region where the population is highly mobile, and insecurity is rife.”
If efforts at vaccination are needed soon in Goma, up to 2 million doses might be needed. Reuters reports that, “Congolese authorities were racing to contain an Ebola epidemic on Thursday, after a gold miner with a large family contaminated several people in the east’s main city of Goma before dying of the hemorrhagic fever.” Readers may recall that the West Africa outbreak of 2014-16 in Guinea, Sierra Leone and Liberia accelerated greatly after infected people went to major cities in search of help.
The miner is the second ‘imported case into Goma, which borders Rwanda, but because his family lives there, he has already infected his wife and one of his 10 children. Contacts are being traced and monitored, but this urban and border threat is one of the factors that led WHO to finally declare the current outbreak a public health emergency.
Malaria
As we move toward malaria elimination Reactive Case Detection (RCD) has been proposed as an integral part of these efforts with the hopes that is can be conceived of as a way of gradually decreasing transmission, according to an article in Malaria Journal. In fact, the value of RCD may be limited as follows:
- RCD alone can eliminate malaria in only a very limited range of settings, where transmission potential is very low
- In other settings, it is likely to reduce disease burden and help maintain the disease-free state in the face of imported infections
Another article looks at “natural exposure to gametocytes that can result in the development of immunity against the gametocyte by the host as well as genetic diversity in the gametocyte.” The researchers learned that there can be variations in immune response depending on season and geography. This information is helpful in planning malaria elimination interventions.
On the vector front a baseline susceptibility testing was conducted in 16 countries in sub-Saharan Africa for neonicotinoids. “The target site of neonicotinoids represents a novel mode of action for vector control, meaning that cross-resistance through existing mechanisms is less likely.” The findings will help in the preparation for rollout of clothianidin formulations as part of national IRS rotation strategies by PMI and other partners.
 Researchers also called on us to learn more about malaria vectors in other parts of the world. In order to eliminate Plasmodium falciparum from the Caribbean and Central America program planners should consider local vector characteristics such as An. albimanus. They found that, “House-screening and repellent IRS are potentially highly effective against An. albimanus if people are indoors during the evening.”
Researchers also called on us to learn more about malaria vectors in other parts of the world. In order to eliminate Plasmodium falciparum from the Caribbean and Central America program planners should consider local vector characteristics such as An. albimanus. They found that, “House-screening and repellent IRS are potentially highly effective against An. albimanus if people are indoors during the evening.”
Vectors are also of concern on the edges of malaria transmission, particularly in South Africa, one of the ‘elimination eight’ countries of the Southern Africa Development Community. Researchers examined the, “potential role of Anopheles parensis and other Anopheles species in residual malaria transmission, using sentinel surveillance sites in the uMkhanyakude District of northern KwaZulu-Natal Province.” They found Anopheles parensis is a potential but minimal vector of malaria in South Africa “owing to its strong zoophilic tendency.” On the other hand, An. arabiensis was found to be the major vector responsible for residual malaria transmission in South Africa. Since these mosquitoes were found in outdoor-placed resting traps, interventions are needed to control outdoor-resting of vector populations.
NTDs of Concern
During the week, the member states of the African Union renewed their commitment to fight and permanently eliminate Neglected Tropical Diseases. Africa.com reported that, “Achievements to date include 1 billion people treated against at least one NTD and 37 countries have completed the removal of at least one NTD.”
Although some reports have discounted the idea of trachoma in Namibia, there may be reason to re-examine the situation. On Twitter Anthony Solomon notes that Namibia needs #trachoma prevalence surveys. A just-completed joint Ministry of Health & Social Services/@WHO mission found active trachoma & trichiasis in Zambezi & Kunene Regions.
 The Times of India draws attention to snakebite. It says that “Under-reported and inadequately treated, fatalities in India are estimated at close to 50,000 a year, the world’s highest.”
The Times of India draws attention to snakebite. It says that “Under-reported and inadequately treated, fatalities in India are estimated at close to 50,000 a year, the world’s highest.”
Overall we can see that the concept of ‘neglect’ has several uses. There is neglect if half of Ebola cases are undetected. There is neglect if we do not understand malaria vectors in low transmission areas. Finally, there is neglect if we do not conduct up-to-date disease surveys to determine whether a disease is present or not. Elimination of tropical diseases is challenging when key processes are neglected.