Epidemiology &IPTp &ITNs &Malaria in Pregnancy &Morbidity &Treatment Bill Brieger | 26 Jun 2017
Burundi: when will citizens see real protection from malaria?
Preliminary findings from Burundi’s 2015-16 DHS have been made available. The country has a long way to go to meet targets for basic control of malaria.
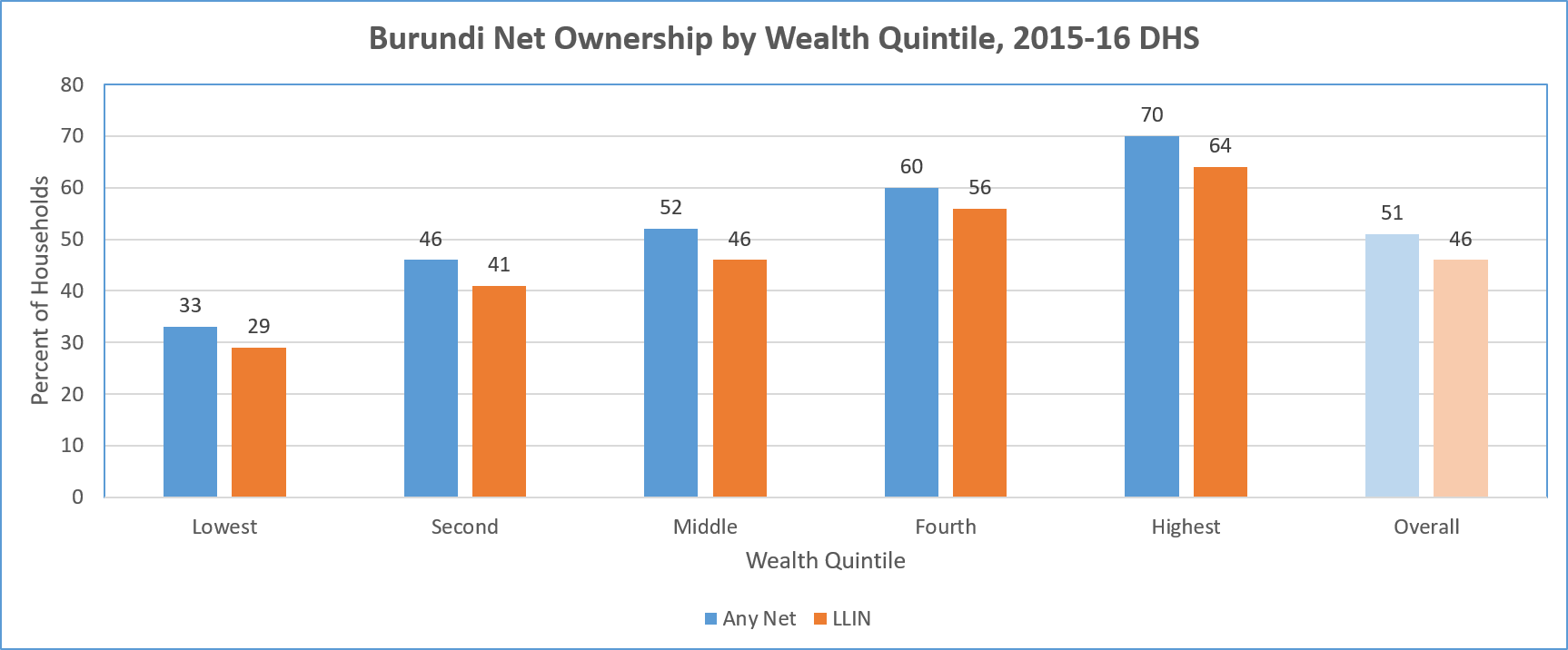 LLIN availability by household is an overall disappointing 32%. Ironically there is greater coverage of households in in urban areas (50%) than rural (30%). There is also great variation among the provinces with 52% coverage in Bujumbura metropolitan but only 19% in Canzuko. The overall average is less than one treated net per household.
LLIN availability by household is an overall disappointing 32%. Ironically there is greater coverage of households in in urban areas (50%) than rural (30%). There is also great variation among the provinces with 52% coverage in Bujumbura metropolitan but only 19% in Canzuko. The overall average is less than one treated net per household.
A major concern is equity. The chart above shows a steep gradation from 19% coverage among the lowest fifth of the wealth quintile, up to 48% in the highest. Even in households that have at least one net, only 17% of of people slept under a net the night before the survey.
In terms of use by those traditionally defined as vulnerable, the DHS shows only 40% of children below 5 years of age overall slept under a treated net the night prior to the survey. Even in households that own at least one net, 78% of these children slept under one.
A similar pattern is seen for treated net use by pregnant women. Overall 44% slept under a treated net, and 84% did so in households that owned at least one treated net. The internal household dynamics of net use where one is available does appear to favor these two groups.
Overall coverage of Intermittent Preventive Treatment for pregnant women is very low. Less than 30% of pregnant women received even the first dose of SP. This decreased to 21% for two doses and 13% for three. In contrast to net coverage, more rural women (31%) received the first dose of IPTp than urban ones (19%).
 Nearly 40% of children below five years of age were found to have had a fever in the two weeks preceding the survey. Among those care was sought for only two-thirds. Eleven percent of those with fever received an artemisinin-based combination therapy drug. The report did not mention whether these children had received any testing prior to treatment, so appropriateness of treatment cannot be judged. Prevalence testing of the children in the sample found 38% with parasitemia. Therefore one might assume that more children should have received ACTs.
Nearly 40% of children below five years of age were found to have had a fever in the two weeks preceding the survey. Among those care was sought for only two-thirds. Eleven percent of those with fever received an artemisinin-based combination therapy drug. The report did not mention whether these children had received any testing prior to treatment, so appropriateness of treatment cannot be judged. Prevalence testing of the children in the sample found 38% with parasitemia. Therefore one might assume that more children should have received ACTs.
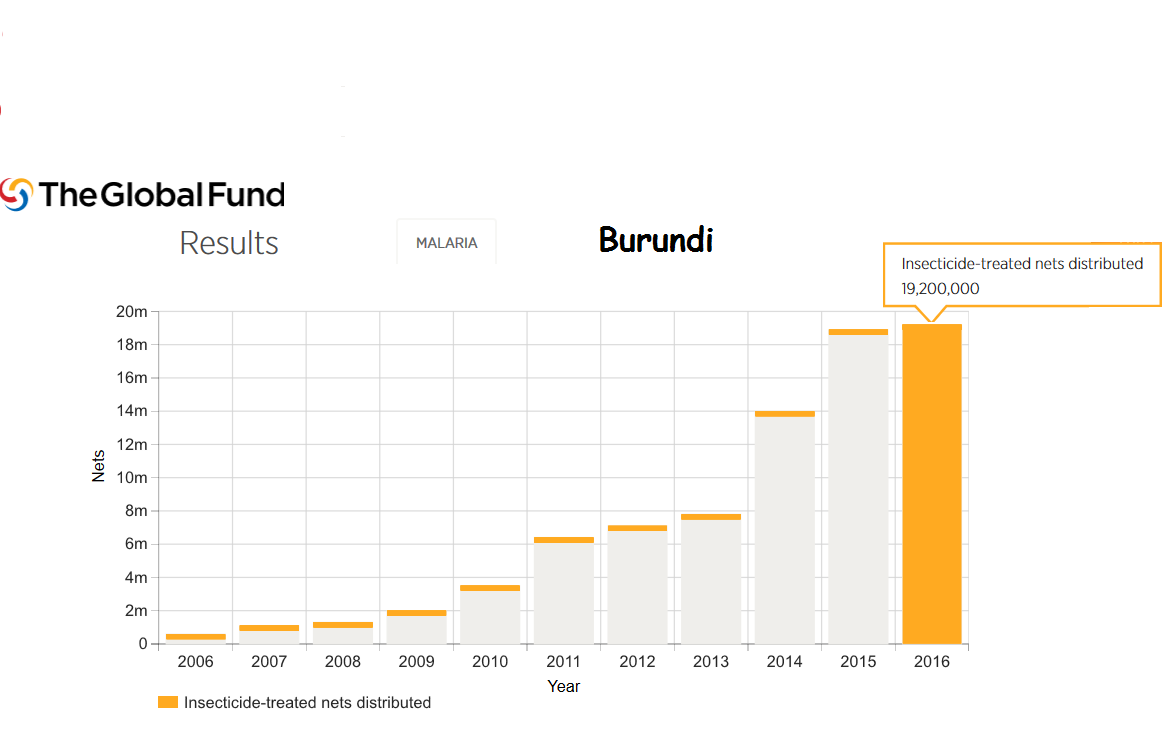
Burundi still faces major political and social challenges. Even so Burundi is the recipient of malaria support from the Global Fund. For example 18 million LLINs were distributed in 2015 and 19 million in 2016.
Much work is needed to bring Burundi even close to universal coverage of malaria interventions. In today’s climate of questionable donor commitment, it is hoped that regional partners may play a role since malaria knows no boundaries.
Refugee Bill Brieger | 20 Jun 2017
Refugees and Malaria
 June 20th is World Refugee Day. The United Nations explains that, “Refugees are among the most vulnerable people in the world. The 1951 Refugee Convention and its 1967 Protocol help protect them.” This protection includes the right to public relief and assistance, and in that context the UN High Commission for Refugees aims to provide refugees with “clinics, schools and water wells for shelter inhabitants and gives them access to health care and psychosocial support during their exile.” Major physical health problems and symptoms of internally displaced persons in Sub-Saharan Africa included were fever/malaria among 85% of children and 48% of adults.
June 20th is World Refugee Day. The United Nations explains that, “Refugees are among the most vulnerable people in the world. The 1951 Refugee Convention and its 1967 Protocol help protect them.” This protection includes the right to public relief and assistance, and in that context the UN High Commission for Refugees aims to provide refugees with “clinics, schools and water wells for shelter inhabitants and gives them access to health care and psychosocial support during their exile.” Major physical health problems and symptoms of internally displaced persons in Sub-Saharan Africa included were fever/malaria among 85% of children and 48% of adults.
Many of today’s refugees are located in malaria endemic areas of the world, and movement from familiar areas to uncertainly increases refugees’ exposure to malaria. As the Roll Back Malaria Partnership noted, “exposure to malaria is significantly increased when moving from low- to high- transmission areas, because they have no acquired immunity and frequently little knowledge of malaria prevention or treatment.”
Efforts to prevent malaria among refugees who came from South Sudan in in Northern Uganda is crucial as they experience malaria as one of their major health problems. This led to the provision of intermittent preventive treatment for malaria (IPTc) in two refugee camps among children aged 6 months to 14 years through help from Médecins Sans Frontières.
In Australia guidelines for assessing needs for services for refugees include an emphasis on person-centred care and risk-based rather than universal screening for hepatitis C virus, malaria, schistosomiasis and sexually transmissible infections.” Based on country of origin “refugees and asylum seekers to Australia and includes country-specific recommendations for screening for malaria, schistosomiasis and hepatitis C.” This includes use of malaria Rapid Diagnostic tests.
Efforts to reach refugee populations with insecticide treated bednets can be a challenge. Studies in a displaced persons camp in the Democratic Republic of the Congo found that there was lower access to nets by camp dwelling children than those in nearby settled villages. Considering the high burden of malaria in the area the authors recommended increased attention to net distribution for these internal refugees.
World Refugee Day is a time for people in malaria national control/elimination programs to take note of the refugee and displaced populations within their boundaries and step up efforts to protect everyone.
Blood Borne &Epidemiology Bill Brieger | 14 Jun 2017
Donate Blood, Not Malaria
 June 14th is World Blood Donor Day. This year’s theme stresses the importance of donating now before a disaster strikes. This requires good storage facilities (and strong systems) in countries where disasters may occur, which may not always be the case. We know that blood donation facilities are concerned about testing for infectious diseases like HIV and Hepatitis C. What of malaria?
June 14th is World Blood Donor Day. This year’s theme stresses the importance of donating now before a disaster strikes. This requires good storage facilities (and strong systems) in countries where disasters may occur, which may not always be the case. We know that blood donation facilities are concerned about testing for infectious diseases like HIV and Hepatitis C. What of malaria?
Studies have found that when people return to a non-endemic setting from malaria endemic countries, “Semi-immune individuals are more likely to transmit malaria as they may be asymptomatic” and serological data, not just circumstantial epidemiological information are also needed that if transmission through blood donations are to be prevented. There is also concern about the longevity of malaria infection depending on the species of Plasmodium in different parts of the world.
In endemic countries malaria antibodies can be present in basically all of asymptomatic adult blood donors. Unfortunately currently available screening assays appear unsuitable to minimize transfusion malaria.
Researchers in Brazil reported that, “The real-time PCR with TaqMan probes enabled the identification of P. vivax in a high proportion of clinically healthy donors, highlighting the potential risk for transfusion-transmitted malaria. Additionally, this molecular diagnostic tool can be adopted as a new laboratory screening method in haemotherapy centres, especially in malaria-endemic areas.”
Knowing the seasonal prevalence of malaria among blood donors in Bamako, Kouriba et al. suggest “A prevention strategy of transfusion malaria based on the combination of selection of blood donors through the medical interview, promoting a voluntary low-risk blood donation and screening all blood bags intended to be transfused” to vulnerable groups.
So while we recognize the life saving importance of adequate blood donations and supplies for transfusion, we also stress the importance of blood safety and expand our horizons to the possibility that malaria may be one of the potential problems shared with blood.