Case Management &Community &Diagnosis &Drug Development &iCCM &Vaccine Bill Brieger | 12 Nov 2015
Pneumonia and Malaria – similar challenges and pathways to success
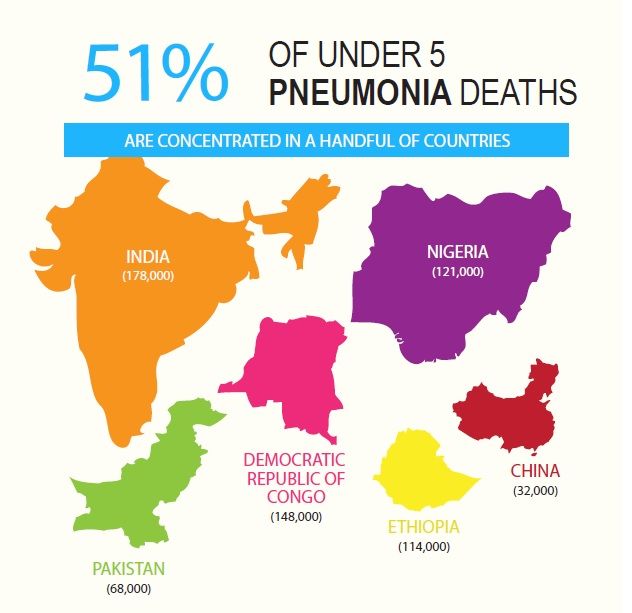 World Pneumonia Day (WPD) helps us focus on the major killers of children globally. While Pneumonia is responsible for more child mortality across the world, in tropical malaria endemic areas both create nearly equal damage (see WPD graphic showing Nigeria and DRC which are both have the highest burden for pneumonia, but also malaria). Of particular concern is case management at the clinic and community level where there is great need to differentiate between these two forms of febrile illness so that the right care is given and lives are saved.
World Pneumonia Day (WPD) helps us focus on the major killers of children globally. While Pneumonia is responsible for more child mortality across the world, in tropical malaria endemic areas both create nearly equal damage (see WPD graphic showing Nigeria and DRC which are both have the highest burden for pneumonia, but also malaria). Of particular concern is case management at the clinic and community level where there is great need to differentiate between these two forms of febrile illness so that the right care is given and lives are saved.
![]() Diagnostics are a particular challenge. While we now have malaria rapid diagnostic test kits that can be used at the community level, we must rely on breath counting for malaria. The Pneumonia Diagnostics Project (see video) “is working to identify the most accurate and acceptable devices for use by frontline health workers in remote settings in Cambodia, Ethiopia, South Sudan and Uganda.”
Diagnostics are a particular challenge. While we now have malaria rapid diagnostic test kits that can be used at the community level, we must rely on breath counting for malaria. The Pneumonia Diagnostics Project (see video) “is working to identify the most accurate and acceptable devices for use by frontline health workers in remote settings in Cambodia, Ethiopia, South Sudan and Uganda.”
Ease of use at low cost must be achieved. One approach to solve the pneumonia diagnostics challenge at community and front line clinic level is to find “mobile phone applications or alternative energy for pulse oximetry,” to test low oxygen levels.
 Vaccine development for both diseases is underway. The challenge for malaria results from the different stages of the parasites life-cycle. Lack of affordable vaccines for pneumonia limits at present widespread preventive action, though public-private partnerships offer hope.
Vaccine development for both diseases is underway. The challenge for malaria results from the different stages of the parasites life-cycle. Lack of affordable vaccines for pneumonia limits at present widespread preventive action, though public-private partnerships offer hope.
Dispersable and correct dose for age prepackaged malaria drugs are already available. Now more child-friendly medicines for pneumonia are being developed. In low resource settings, “amoxicillin dispersible tablets are a better option, particularly for children who can’t swallow pills. They have a longer shelf-life, are cost-effective, don’t need refrigeration, and are easy to administer.”
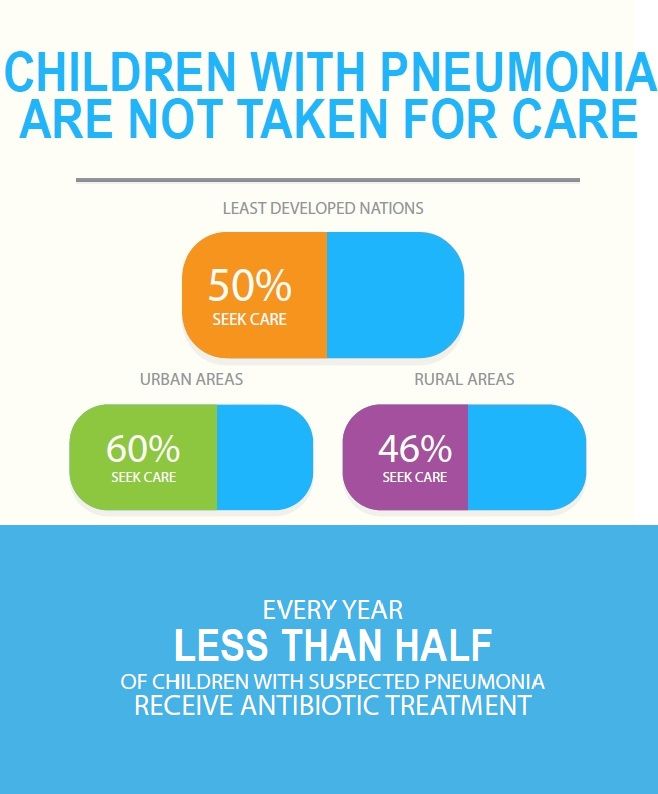
Similarities in the problems and solutions to control these two diseases require that interventions must continue to be developed and implemented jointly in order to benefit children the most. As can be seen again from the WPD graphics (right), many children do not get needed treatment. Integrated case management at all levels is the answer.
Monitoring &Mortality &water Bill Brieger | 05 Nov 2015
The quantitative impact assessment of community health projects in selected African countries by using Lives Saved Tool
 Chulwoo (Charles) Park who has been undertaking the Masters of Science in Public Health at the Johns Hopkins Bloomberg School of Public Health is sharing herein his experiences with the LiST tool in African countries.
Chulwoo (Charles) Park who has been undertaking the Masters of Science in Public Health at the Johns Hopkins Bloomberg School of Public Health is sharing herein his experiences with the LiST tool in African countries.
The Lives Saved Tool (LiST) is a computer-based tool that estimates the impact of scaled up health intervention packages in a quantitative manner. By modeling complex mathematical relationship of coverage difference among interventions for maternal, neonatal and child health (MNCH), LiST shows us quantitative results, such as mortality rates, incidence rates, number of cases averted, percentage of stunting and wasting, number of cause-specific death and lives saved.
Especially, LiST can project and run multiple scenarios for subnational target population in the country not only to evaluate existing MNCH project but also prioritize investments for the future based on the quantitative results. World Vision International (WVI) has implemented LiST analysis to strengthen its evaluation and strategic planning methods for MNCH projects since 2013.
Recently, the mid-term evaluations for Access to Infant and Maternal (AIM)-Health project in Kenya, Mauritania, Sierra Leone, Tanzania, and Uganda were conducted through mixed methods analysis, both qualitative research (in-depth interview and focused group discussion) and quantitative research (LiST) from June to September of 2014.
 Subsequently, LiST was solely utilized to quantify the retrospective impact of Water, Sanitation, and Hygiene (WASH) project in Southern Africa Region (SAR), Malawi, Mozambique and Zambia between 2010 and 2014. The significant impact indicates that the combined effect of all five WVI WASH interventions (improved water source, home water connection, improved sanitation, hand washing with soap, and hygienic disposal of children’s stools) have prevented 989,745 diarrhoeal cases among the under-five target population of 506,019 children.
Subsequently, LiST was solely utilized to quantify the retrospective impact of Water, Sanitation, and Hygiene (WASH) project in Southern Africa Region (SAR), Malawi, Mozambique and Zambia between 2010 and 2014. The significant impact indicates that the combined effect of all five WVI WASH interventions (improved water source, home water connection, improved sanitation, hand washing with soap, and hygienic disposal of children’s stools) have prevented 989,745 diarrhoeal cases among the under-five target population of 506,019 children.
In other words, every single young child prevented 1.96 cases of diarrhea, and prevention rate for diarrhoea was 13% throughout the implementation period. Another results indicate that WVI’s WASH project contributed a 209% mean increase in percentage of under-five lives saved and 15.5% mean decrease in under-five mortality rates across SAR.
- Chulwoo (Charles) Park, MSPH ’15
- Johns Hopkins Bloomberg School of Public Health, Department of International Health, Division of Global Disease Epidemiology and Control
- For more information write to e-mail: park@jhmi.edu
Communication &IPTp &ITNs &Treatment Bill Brieger | 04 Nov 2015
An Ideation Model: Attitudes, Beliefs and Practices Relevant to Malaria Prevention and Treatment in Madagascar and Liberia
Stella Babalola, Nan Lewicky, Grace Awantang, Michael Toso, Hannah Koenker, Arsene Ratsimbasoa, Monique Vololona of the Johns Hopkins Center for Communication Programs and the Division for Malaria Control, Madagascar Presented findings on how local perceptions help predict uptake of malaria interventions at the 143rd American Public Health Association Annual Meeting, October 31 – November 4, 2015, in Chicago. Their presentation on Liberia and Madagascar is summarized below.
While Liberia has an average malaria parasitemia prevalence of 28%, malaria is considerable less common in Madagascar and varies by region and altitude. This difference provides an interesting opportunity to observe similarities and contrasts in community perceptions of the disease.
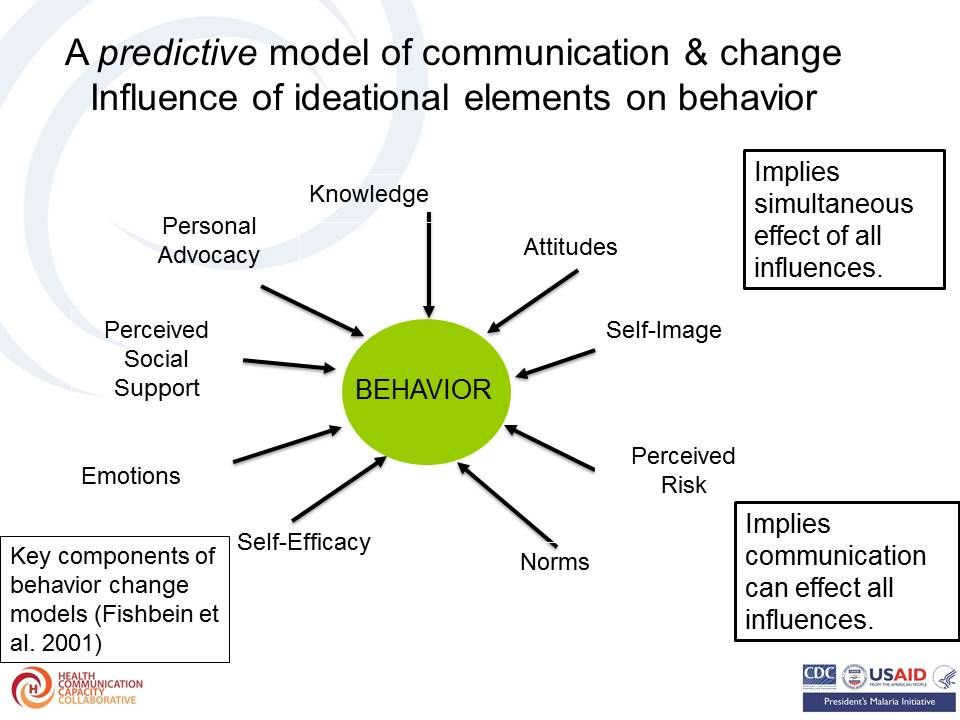
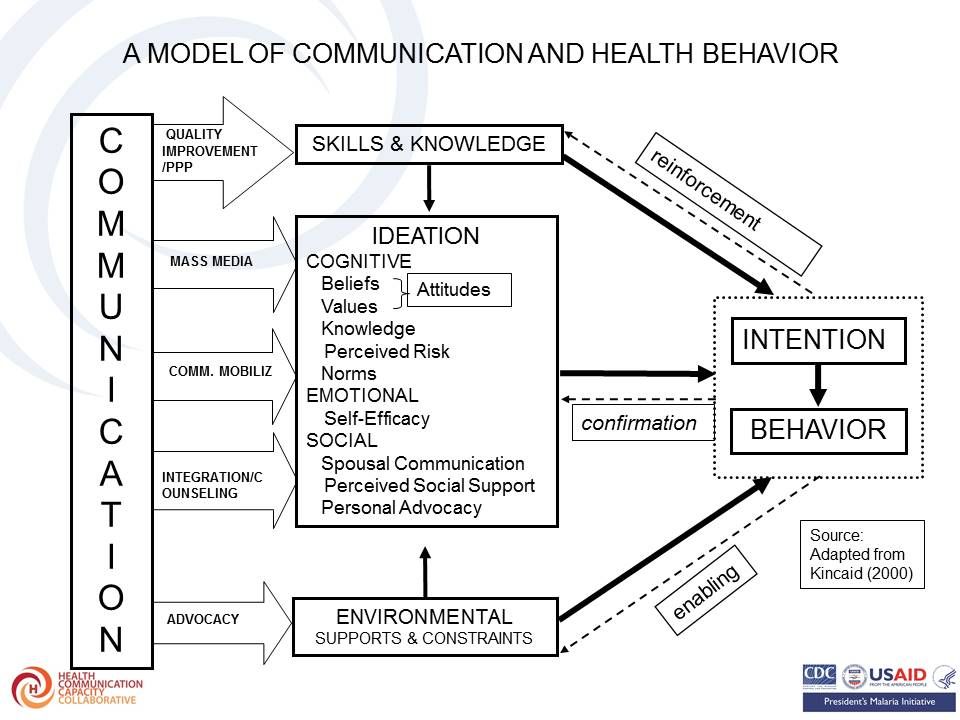 Theoretical basis of the research is based on the Ideation model which has been described as follows and as seen in the attached figures:
Theoretical basis of the research is based on the Ideation model which has been described as follows and as seen in the attached figures:
- “New ways of thinking and the diffusion of those ways of thinking by means of exposure to mass media and social interactions in local, culturally homogeneous communities” – Kincaid, 2000
- “views and ideas that people hold individually” – van de Kaa 1996
 The ideation model has successfully predicted current use of a contraceptive method as well as accessing childhood immunization. The team took up the challenge to learn whether this model would be applicable to malaria interventions.
The ideation model has successfully predicted current use of a contraceptive method as well as accessing childhood immunization. The team took up the challenge to learn whether this model would be applicable to malaria interventions.
Malaria-related ideation was proposed to consist of: Malaria knowledge (cause, symptom, prevention); Perceived susceptibility to malaria; Perceived severity of malaria; Perceived self-efficacy to prevent malaria; and Social interactions about malaria. These may lead to uptake of malaria interventions.
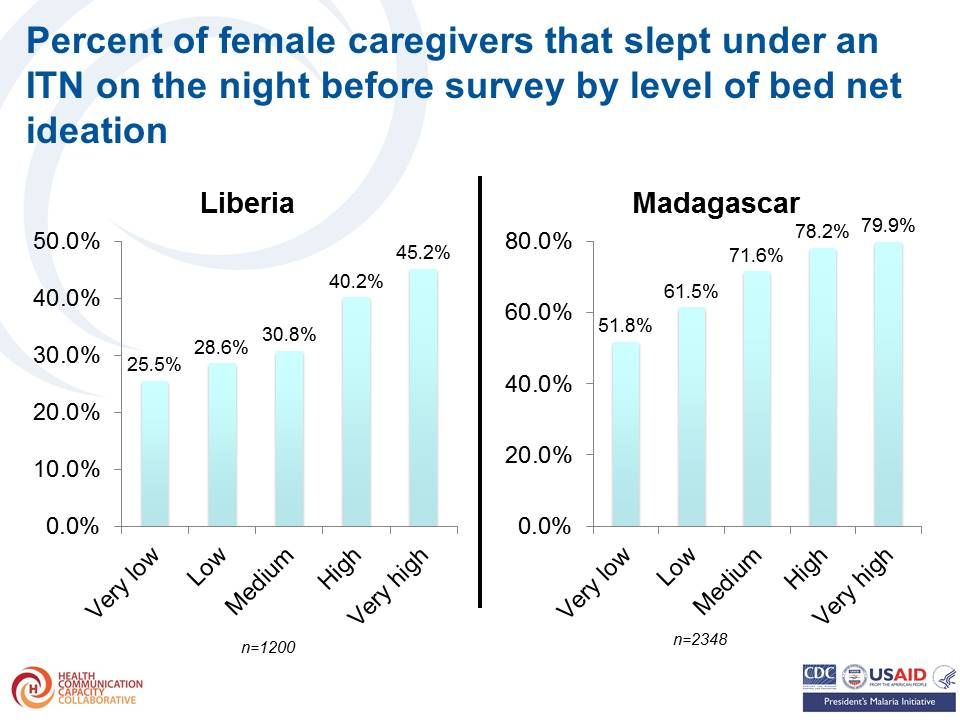
 Items for measuring bed net ideation could include – knowing where to procure a bed net, Willingness to pay for bed net, Having a positive attitudes towards bed net (derived from ten attitudinal statements), Perceived response-efficacy of bed nets, Perceived self-efficacy for procuring and using bed nets, Participation in household decisions about bed nets, Descriptive norm about bed net use and Social interactions about bed net use.
Items for measuring bed net ideation could include – knowing where to procure a bed net, Willingness to pay for bed net, Having a positive attitudes towards bed net (derived from ten attitudinal statements), Perceived response-efficacy of bed nets, Perceived self-efficacy for procuring and using bed nets, Participation in household decisions about bed nets, Descriptive norm about bed net use and Social interactions about bed net use.
Percent of female caregivers that slept under an ITN on the night before survey increased by level (score) of bed net ideation as seen in the graph. Results (odds ratio) of logistic regression of sleeping under an ITN on bed net ideation and other covariates showed a similar trend.
 Intermittent Preventive Treatment of Malaria in Pregnancy ideation measures included the following:
Intermittent Preventive Treatment of Malaria in Pregnancy ideation measures included the following:
- Knows name of the drug for malaria prevention during pregnancy
- Knows the timing of first dose of IPTp
- Has positive attitudes towards ANC and IPTp (derived from four attitudinal statements)
- Perceived response-efficacy of IPTp
- Woman participates in decisions about own health
- Social interactions about malaria and pregnancy
- Descriptive norm about ANC visits
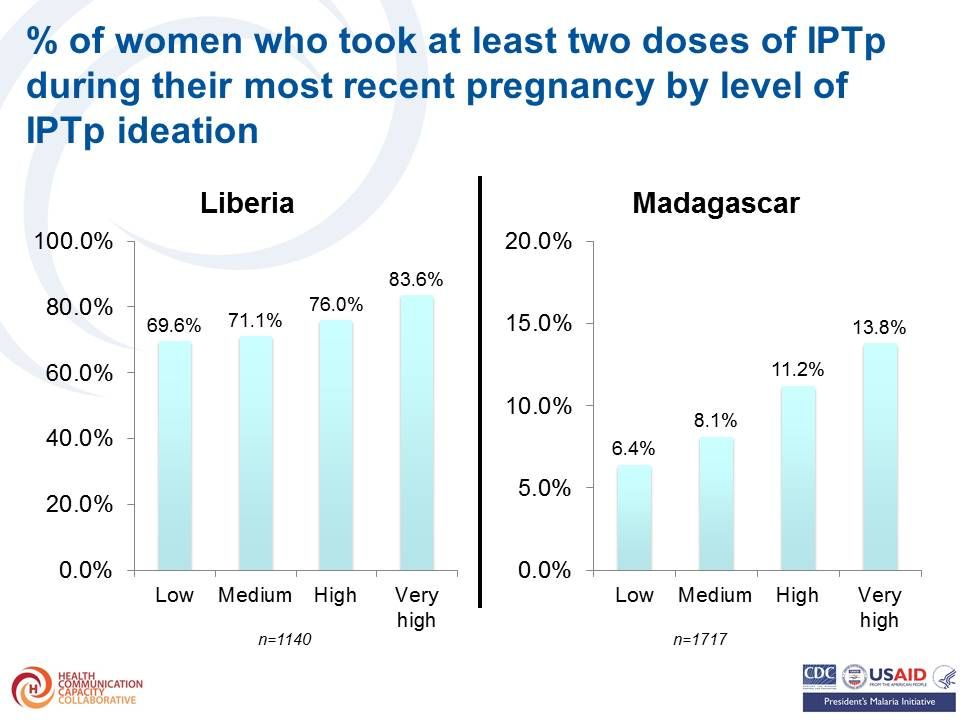 The percent of women who took at least two doses of IPTp during their most recent pregnancy also increased by level of IPTp ideation Likewise the results (odds ratio) of logistic regression of obtaining at least two doses of IPTp on IPTp ideation and other covariates were highest among those with highest levels of ideation.
The percent of women who took at least two doses of IPTp during their most recent pregnancy also increased by level of IPTp ideation Likewise the results (odds ratio) of logistic regression of obtaining at least two doses of IPTp on IPTp ideation and other covariates were highest among those with highest levels of ideation.
Items for measuring case management ideation included –
- Perceived response efficacy of malaria diagnostic test
- Perceived self-efficacy for detecting uncomplicated malaria
- Perceived self-efficacy for detecting severe malaria
- Descriptive norm about prompt treatment of malaria in children
- Social interactions about malaria treatment
- Participation in household decisions about child health
- Positive attitudes towards appropriate malaria treatment
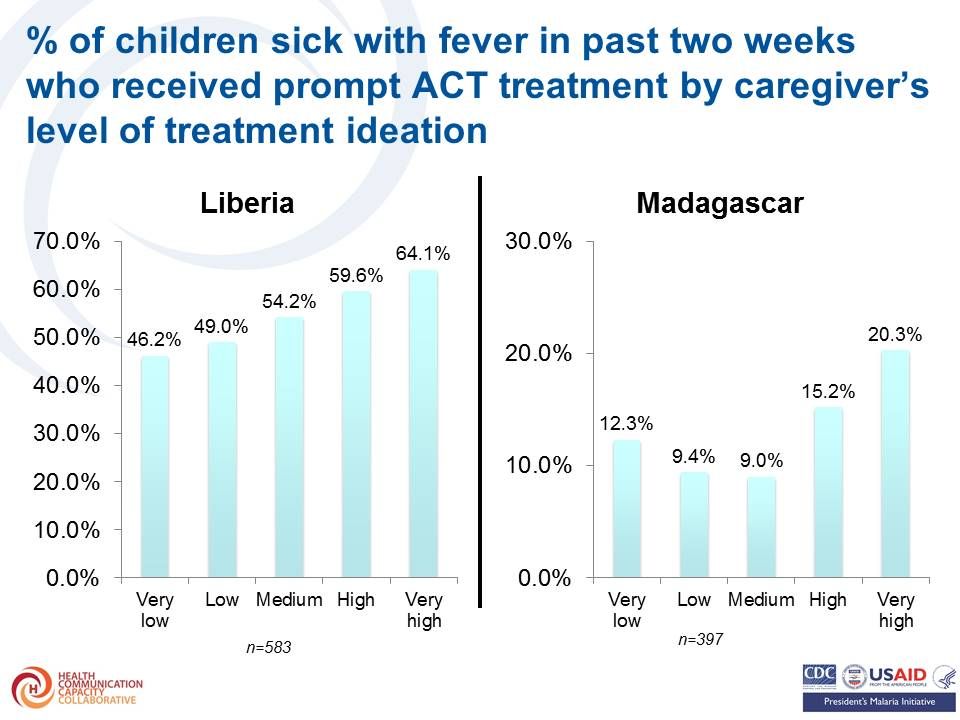 Again the percent of children sick with fever in past two weeks who received prompt ACT treatment by caregiver’s increased with increasing level of treatment ideation. As before the results (odds ratio) of logistic regression of prompt ACT treatment on caregiver’s treatment ideation and other covariates shows highest levels of ideation were associated with greated treatment seeking.
Again the percent of children sick with fever in past two weeks who received prompt ACT treatment by caregiver’s increased with increasing level of treatment ideation. As before the results (odds ratio) of logistic regression of prompt ACT treatment on caregiver’s treatment ideation and other covariates shows highest levels of ideation were associated with greated treatment seeking.
The team concluded that the same ideation model with demonstrated validity for family planning, child immunization, WASH and other health behaviors is relevant for malaria prevention and treatment. Strategically designed messages and interventions addressing ideational variables can help foster adoption of health-protective malaria prevention and treatment behaviors.
The authors acknowledge The US President’s Malaria Initiative (PMI) for technical guidance on the implementation of the surveys and The Ministry of Health and Social Welfare in Liberia and the Ministry of Health in Madagascar for their collaboration on the surveys.
Case Management &Communication &Treatment Bill Brieger | 02 Nov 2015
Case Management of Malaria: A Review and Qualitative Assessment of Social and Behavior Change Communication Strategies in Four Countries
Kamden Hoffmann1 and Michael Toso2 presented a poster today at the 143rd annual meeting of the American Public Health Association in Chicago. Their findings are posted below.
 Introduction. With the introduction and growing availability of combination therapy and rapid diagnostic tests, case management of malaria has evolved and expanded in scope. Social and behavior change communication (SBCC) activities have been developed to influence prompt care seeking behavior, adherence to test results, and completion of full treatment regimens. This review describes SBCC programming, and the extent to which it has been evaluated for impact, in Zambia, Ethiopia, Rwanda, and Senegal.
Introduction. With the introduction and growing availability of combination therapy and rapid diagnostic tests, case management of malaria has evolved and expanded in scope. Social and behavior change communication (SBCC) activities have been developed to influence prompt care seeking behavior, adherence to test results, and completion of full treatment regimens. This review describes SBCC programming, and the extent to which it has been evaluated for impact, in Zambia, Ethiopia, Rwanda, and Senegal.
Objectives. The purpose of this review is to identify promising SBCC practices related to case management at both community and service provider levels in the four focus countries: Zambia, Ethiopia, Rwanda and Senegal. Essential for any large-scale communication strategy is a form of impact assessment. Impact assessments aim to answer the question, “Did the communication strategy achieve the specified objectives?” Impact assessments look at the difference that the strategy made in the overall program environment. The indicators can vary depending on the approach and channels used in the strategy.
An example of an impact indicator for malaria case management could be: the proportion of children under five years old with fever in the last two weeks for whom treatment was sought. Typical data sources include:
- Population-based household surveys, such as the Demographic and Health Survey, the Malaria Indicator Survey, or the Multiple Indicator Cluster Survey.
- Sub-national household surveys, particularly in areas where malaria communication activities were targeted.
Methods. An initial review was undertaken, consisting of a thorough PubMed search for articles related to malaria case management that mentioned SBCC, in the four countries. Malaria case management country-level documents, project reports and related SBCC materials were also collected. Implementing partner reports were gathered from each country related to SBCC and/or malaria case management. A comprehensive list of search terms were used for all four countries.
Qualitative analysis consisted of Key Informant Interviews (KIIs) with members of NMCP SBCC/BCC units within the Ministry of Health, USAID implementing partners, and President’s Malaria Initiative staff. A semi-structured questionnaire was used to gather information related to perceptions and first-hand experiences. A total of nine interviews and four written responses were collected. All interviews were recorded and transcribed. The transcribed interviews and written responses were entered into NVivo 10. An initial codebook was developed based on the semi-structured interview guide. Open and axial coding enhanced the initial codebook as themes were generated in the software.
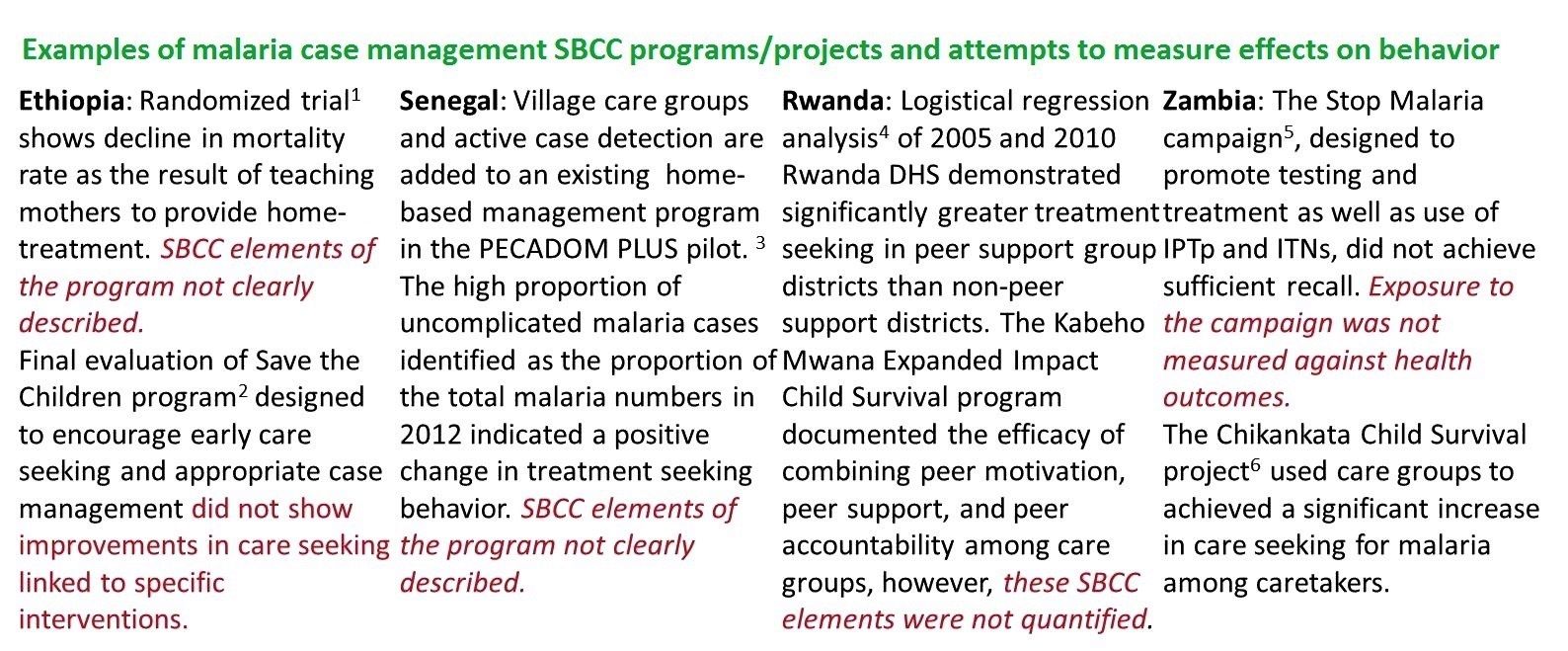
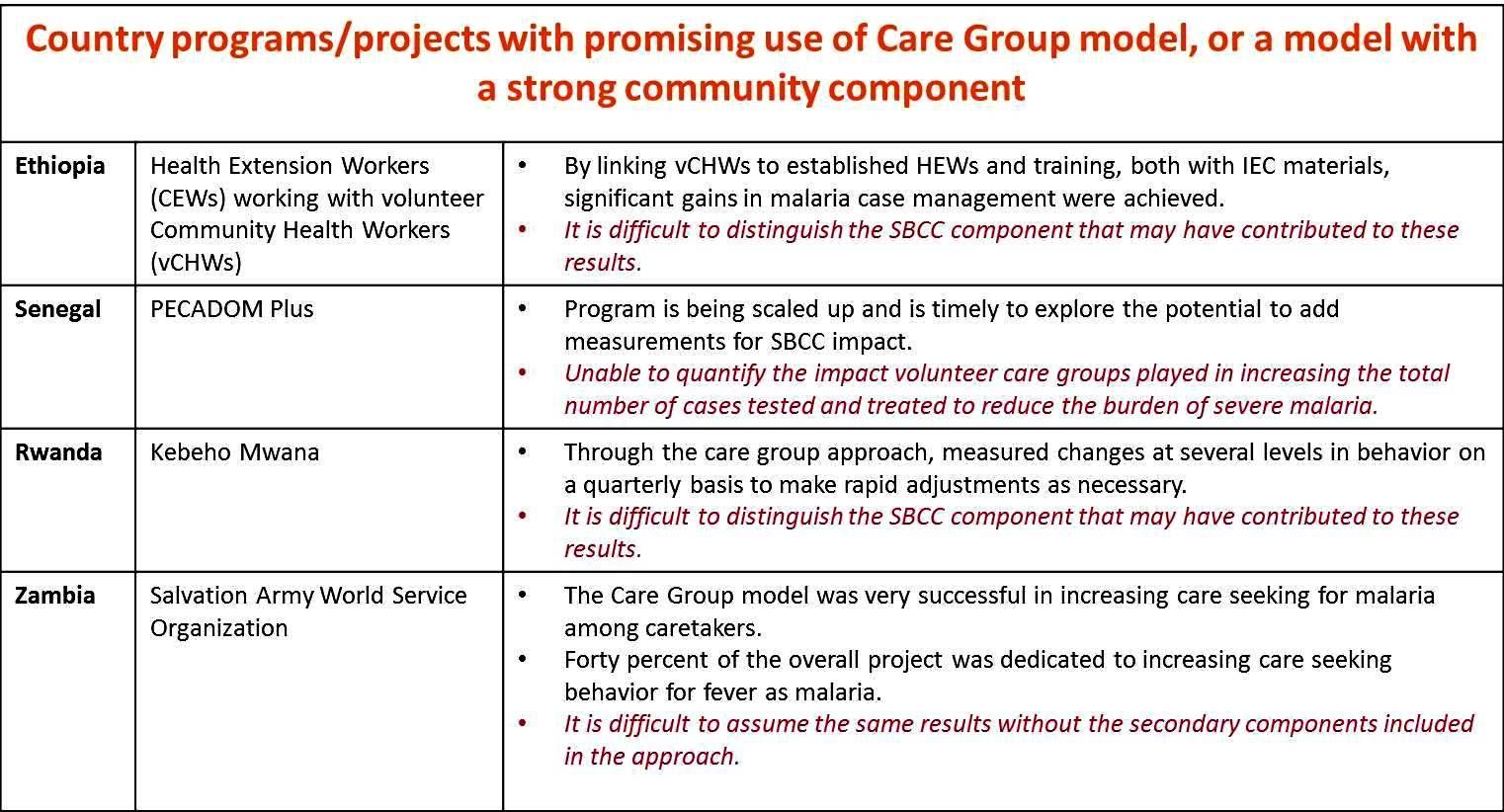
Conclusions. The review was not able to find a substantial amount of material to show gains in the ability to measure impact of SBCC interventions in malaria case management outcomes. Several programs were able to measure changes in care-seeking behavior and uptake of ACTs; however, these types of programs need to be refined in order to measure the specific contribution of malaria SBCC interventions. Each country reviewed presented a program related to either the care group model or a model with a strong community component, and holds promise for further exploration in terms of launch points to expand the measurement of SBCC impact.
 Author Affiliations.
Author Affiliations.
1 Insight Health, 710 Sutter Gate Lane, Morrisville, North Carolina 27560
2 Johns Hopkins Bloomberg School of Public Health, Center for Communication Programs, 111 Market Place Suite 310, Baltimore, MD 21202, USA
Funding for this study was provided by the US President’s Malaria Initiative.
References.
1 Kidane G, Morrow R. Teaching mothers to provide home treatment of malaria in Tigray, Ethiopia: a randomized trial. The Lancet 2000.
2 Innovation for Scale: Enhancing Ethiopia’s Health Extension Package in the Southern Nations and Nationalities People’s Region (SNNPR) Shebedino and Lanfero Woredas, October 1 2007-September 30 2012. Report of the Final Evaluation. December 2012.
3 Linn AM, Ndiaye Y, Hennessee I, et al. Reduction in symptomatic malaria prevalence through proactive community treatment in rural Senegal. Trop Med Int Health. 2015;20(11):1438-1446.
4 Landegger, J., et al. CHW Peer Support Groups for Integration of Health Service Delivery and Improved Performance: Learning from a Peer Group Model in Rwanda
5 Limange, J., et al., Evaluation: Mid-Term Evaluation of the USAID/Zambia Communications Support for Health Program, January 2013, USAID.
6 Salvation Army/Zambia (TSA), Salvation Army World Service Organization (SAWSO), and TSA Chikankata Health Services Chikankata Child Survival Project (CCSP), 2005?2010, Final Evaluation Report. December 2010.
CHW &Community &IPTi &ITNs &Malaria in Pregnancy &Treatment Bill Brieger | 01 Nov 2015
Community Directed Interventions to Enhance PHC and MCH
William Brieger of the Department of International Health, JHU Bloomberg School of Public Health, delivered the keynote address to the Community Based Primary Health Care Working Group at the 2015 American Public Health Association in Chicago. The focus was on Community Directed Interventions (CDI) as a way to enhance implementation of primary health care and maternal and child health. Some excerpt from the talk follow.
 The origins of the CDI Approach are based in Onchocerciasis Control and the implementation research done by the Tropical Disease Research (TDR) Program of WHO and collaborating agencies to help establish the foundational guidance of the African Program for Onchocerciasis Control in 1995. Since then we have seen an expansion of CDI into other health issues
The origins of the CDI Approach are based in Onchocerciasis Control and the implementation research done by the Tropical Disease Research (TDR) Program of WHO and collaborating agencies to help establish the foundational guidance of the African Program for Onchocerciasis Control in 1995. Since then we have seen an expansion of CDI into other health issues
We should start discussion with an understanding of ‘community’ which Rifkin et al. (1988) defined as a group of people living in the same defined area sharing basic values, organization, and interests. White (1982) proposed that community is an informally organized social entity which is characterized by a sense of identity. Manderson et al. (1992) in their work for TDR defined community as a population which is geographically focused but which also exists as a discrete social entity, with a local collective identity and corporate purpose.
Communities are people sharing values and institutions. Community is based on locality (geographic), interdependent social groups, interpersonal relationships expressed through social networks and built on s culture that includes values, norms, and attachments to the community as a whole as well as to its parts. Prior to developing any community intervention we must understand the boundaries, composition and structure of a community from the perspectives of its own members, as their local knowledge and participation are central to success.
 Community Systems Strengthening has been taken up by the Global Fund in order to enhance coverage of various health interventions such as HIV drugs and bednets to prevent malaria. Community systems are community?led structures and mechanisms used by communities through which community members and community based organizations and groups interact, coordinate and deliver their responses to the challenges and needs affecting their communities. Many community systems are small?scale and/or informal. Others are more extensive – they may be networked between several organizations and involve various sub?systems. For example, a large care and support system may have distinct sub?systems for comprehensive home?based care, providing nutritional support, counselling, advocacy, legal support, and referrals for access to services and follow?up.
Community Systems Strengthening has been taken up by the Global Fund in order to enhance coverage of various health interventions such as HIV drugs and bednets to prevent malaria. Community systems are community?led structures and mechanisms used by communities through which community members and community based organizations and groups interact, coordinate and deliver their responses to the challenges and needs affecting their communities. Many community systems are small?scale and/or informal. Others are more extensive – they may be networked between several organizations and involve various sub?systems. For example, a large care and support system may have distinct sub?systems for comprehensive home?based care, providing nutritional support, counselling, advocacy, legal support, and referrals for access to services and follow?up.
Efficacy, Social Control and Cohesion are important characteristics of communities that enable them to take on project and solve problems. Collective Efficacy is a perceived ability to work together. Social control provides evidence that communities are able to enforce their norms. Cohesion describes social interaction that brings people together. A strong sense of identity and a sense of belonging describe communities that can get things done. These characteristics lead to community competency to collaborate effectively in identifying the problems/needs of the community, achieve a working consensus on goals and priorities, agree on ways and means to implement the agreed-upon goals, and collaborate effectively in the required actions.
 It is important to distinguish between Community Based Intervention (CBI) and Community Directed Intervention. CBI takes place in the community but a Health/Development agency exercises authority over decisions on project design and implementation. Project activities (e.g., service delivery dates and procedures) are designed by the agency. Activities simply happen in the community.
It is important to distinguish between Community Based Intervention (CBI) and Community Directed Intervention. CBI takes place in the community but a Health/Development agency exercises authority over decisions on project design and implementation. Project activities (e.g., service delivery dates and procedures) are designed by the agency. Activities simply happen in the community.
With CDI the community exercises authority over decisions and decides on acceptable method to implement projects. This ensures sensitivity to local decision-making structures and social life. Activities happen both in and by the community; the community is in control.
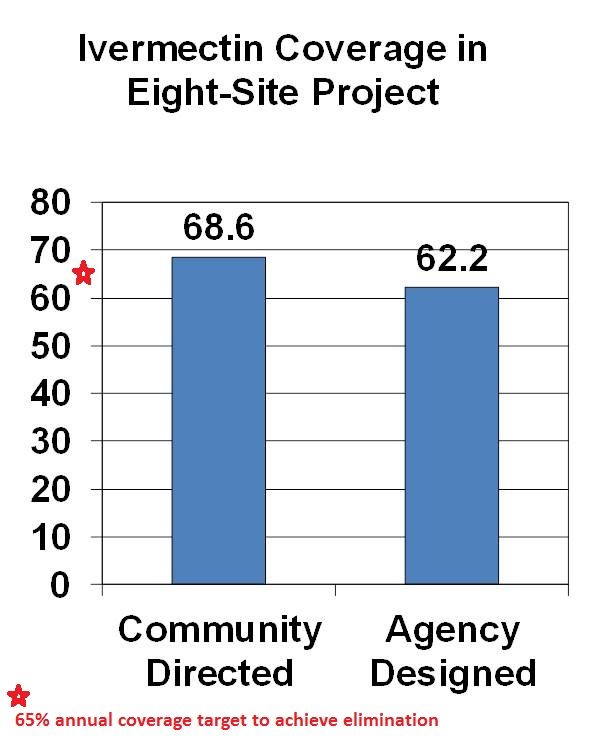
CDI was pioneered for Onchocerciasis (River Blindness) Control as community directed treatment with ivermectin (CDTI). When communities are in charge, coverage is better than when ivermectin distribution is centrally organized by a health agency. The original 1995 CDI field testing showed better ivermectin coverage when the community was in charge of distribution. Since the beginning of CDTI, over 200,000 villages in 18 African countries have been distributing ivermectin annually through their own efforts. Lessons learned over the years are that CDI works best when 1) the smallest level of an organized community is the basis of action (e.g. a hamlet, a clan/kin group) and 2) communities are encouraged to choose as many CDDs as they think they need to get the job done. This means that the community is in charge, not individual volunteers who can be replaced anytime the community finds the need.
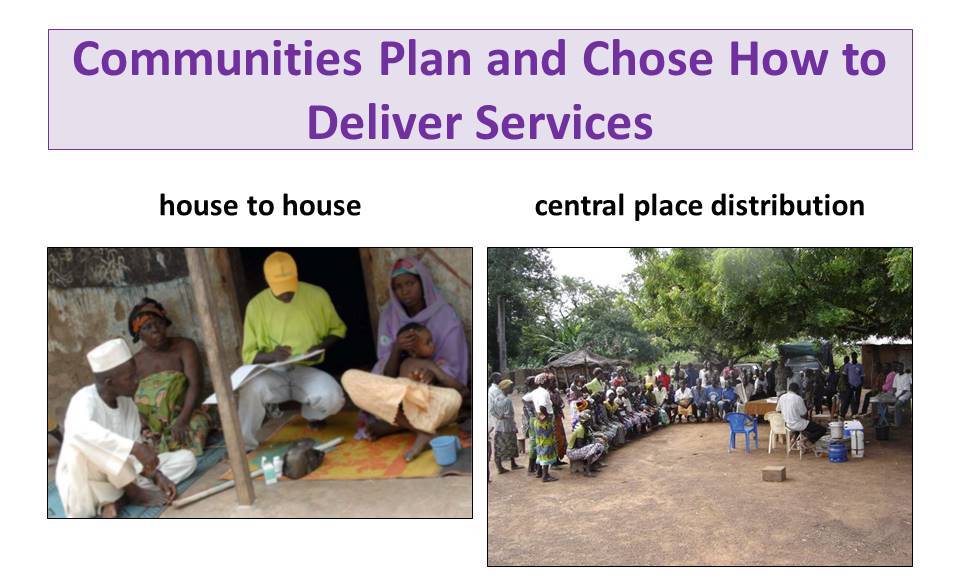
With CDI for onchocerciasis or any other health program, Communities plan and chose how to deliver services. This may be house-to-house, central place distribution or a combination. Health workers provide training and supervision to volunteer village health workers called community directed distributors (CDDs).
 TDR observed that CDI naturally expanded to include other services wanted by the community such as immunization, community development, water and sanitation, agriculture and forestry, HIV-AIDS, family planning, guinea worm, Vitamin A. TDR and APOC then decided that CDI with other service components should be systematically tested. The project sites added in a systematic manner other interventions to existing CDTI programs including home management of malaria, ITN distribution & promotion, TB DOTS, Vitamin A in addition to continued ivermectin distribution. These services varied in complexity and communities responded by dividing the work among several different volunteers.
TDR observed that CDI naturally expanded to include other services wanted by the community such as immunization, community development, water and sanitation, agriculture and forestry, HIV-AIDS, family planning, guinea worm, Vitamin A. TDR and APOC then decided that CDI with other service components should be systematically tested. The project sites added in a systematic manner other interventions to existing CDTI programs including home management of malaria, ITN distribution & promotion, TB DOTS, Vitamin A in addition to continued ivermectin distribution. These services varied in complexity and communities responded by dividing the work among several different volunteers.
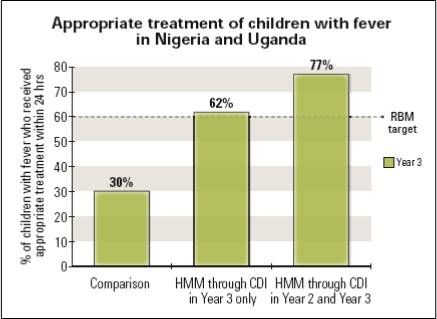 Coverage of interventions like malaria case management, ITN promotion and Vitamin A distribution was higher in the intervention areas compared to the delivery of these services through the routine health system. TB DOTS presented the only challenge because of the social stigma associated with the disease. The study concluded that CDI can effectively incorporate high impact, evidence based interventions while at the same time maintaining and increasing ivermectin coverage. Since CDI does not rely on one volunteer but whole community effort, the problem of overburdening on community health worker did not arise. Other incterventions ould benefit from CDI such as Misoprostol, Intermittent Preventive Treatment, Deworming, Oral Rehydration solution, Zinc, Cotrimoxazole, Amoxicillin, Soap for handwashing and WaterGuard treatment kits.
Coverage of interventions like malaria case management, ITN promotion and Vitamin A distribution was higher in the intervention areas compared to the delivery of these services through the routine health system. TB DOTS presented the only challenge because of the social stigma associated with the disease. The study concluded that CDI can effectively incorporate high impact, evidence based interventions while at the same time maintaining and increasing ivermectin coverage. Since CDI does not rely on one volunteer but whole community effort, the problem of overburdening on community health worker did not arise. Other incterventions ould benefit from CDI such as Misoprostol, Intermittent Preventive Treatment, Deworming, Oral Rehydration solution, Zinc, Cotrimoxazole, Amoxicillin, Soap for handwashing and WaterGuard treatment kits.
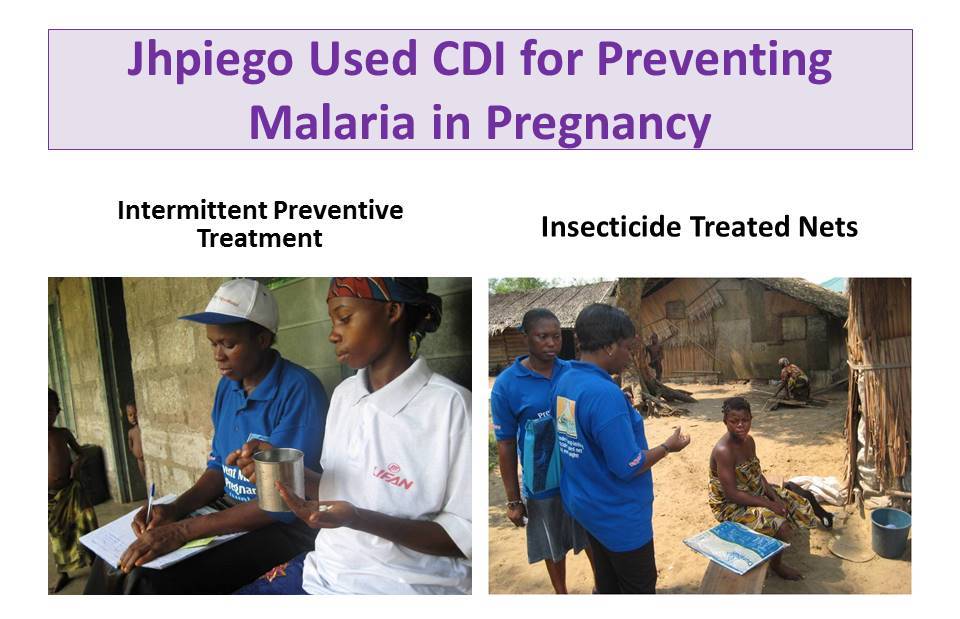 Jhpiego an NGO affiliate of the Johns Hopkins University used CDI to deliver malaria in pregnancy (MIP) prevention services in Nigeria including Intermittent Preventive Treatment and Insecticide Treated Nets. Contrary to fears that CDI would detract from antenatal care attendance, the work of CDDs actually ensured that ANC attendance increased over time. Through CDI IPTp coverage increased compared to control communities and more pregnant women slept under ITNs regularly.
Jhpiego an NGO affiliate of the Johns Hopkins University used CDI to deliver malaria in pregnancy (MIP) prevention services in Nigeria including Intermittent Preventive Treatment and Insecticide Treated Nets. Contrary to fears that CDI would detract from antenatal care attendance, the work of CDDs actually ensured that ANC attendance increased over time. Through CDI IPTp coverage increased compared to control communities and more pregnant women slept under ITNs regularly.
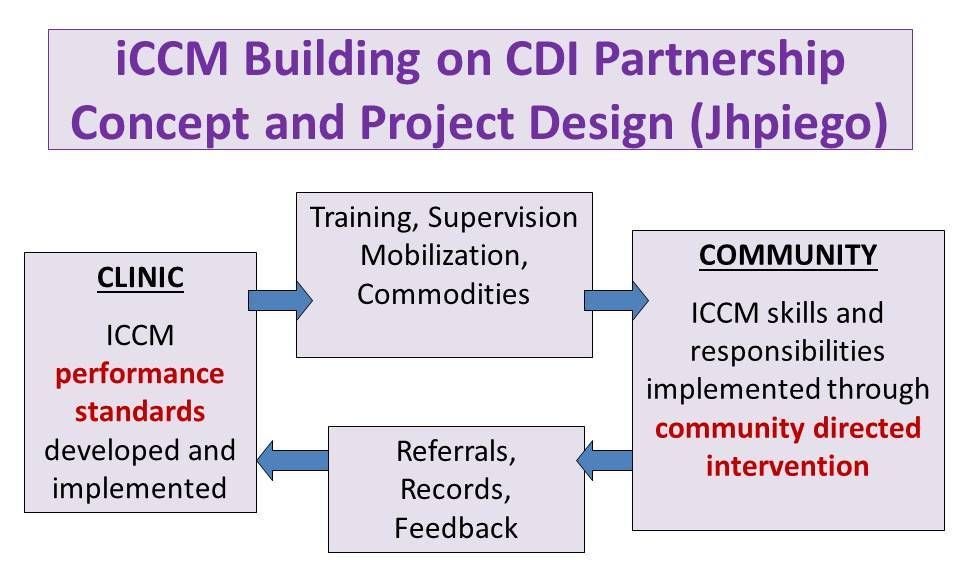 Jhpiego next expanded CDI for MIP into integrated Community Case Management (iCCM), thus taking community case management beyond community based care. Giving communities responsibility for organizing and managing their services using the CDI approach meant greater access to services whenever people need them. Using the CDI approach to iCCM CDDs reached 7,504 clients who presented signs and symptoms of malaria. CDDs successfully conducted malaria diagnosis using the rapid diagnostic test (RDT) kits. Overall, 47.8% tested positive while 52.2% tested negative. CDDs adhered to guidelines and all the 3,587 clients with positive RDT results received appropriate anti-malarial medicines. As appropriate 21.0% were treated for diarrhoea, 11.0% for pneumonia (of whom 68.0% were referred to the health facility)
Jhpiego next expanded CDI for MIP into integrated Community Case Management (iCCM), thus taking community case management beyond community based care. Giving communities responsibility for organizing and managing their services using the CDI approach meant greater access to services whenever people need them. Using the CDI approach to iCCM CDDs reached 7,504 clients who presented signs and symptoms of malaria. CDDs successfully conducted malaria diagnosis using the rapid diagnostic test (RDT) kits. Overall, 47.8% tested positive while 52.2% tested negative. CDDs adhered to guidelines and all the 3,587 clients with positive RDT results received appropriate anti-malarial medicines. As appropriate 21.0% were treated for diarrhoea, 11.0% for pneumonia (of whom 68.0% were referred to the health facility)
 A Supervisory Checklist and Performance Standards were developed and used for Assessing CDD performance. The results were discussed at monthly CDD meetings at their nearest health facilities. This led to further improvements in History taking, Examination, Conducting RDTs for Malaria and Illness Management.
A Supervisory Checklist and Performance Standards were developed and used for Assessing CDD performance. The results were discussed at monthly CDD meetings at their nearest health facilities. This led to further improvements in History taking, Examination, Conducting RDTs for Malaria and Illness Management.
TDR has done further scoping to learn if CDI would be acceptable by health workers and community members in Urban, Nomadic and Underserved Rural Communities. CDI was favorable received. In conclusion we have learned over the years that CDI can involve women, families and communities in meeting their own health needs.