Today’s news featured a media briefing by the RBM Partnership and AMMREN on the challenges of protecting pregnant women from malaria. Additional news expands on these challenges. Research looks at how malaria parasites withstand the heat of a patient’s fever. Finally examples are presented of collaboration between international organizations and the private sector for malaria and disease control. Follow the links to gain more information.
Speed Up IPTp Scale-Up: a media briefing on maternal health
A panel discussion and media briefing on new approaches and lessons learned formed part of an online global call to end malaria in pregnancy with intermittent preventive treatment. The briefing on Tuesday, 6 October 2020, was sponsored by the Roll Back Malaria Partnership and AMMREN. The RBM website features background on the call to action.
The panel discussion included Dr. Aminata Cisse ep. Traore, Sous Directrice de la Santé de la Reproduction/Direction Générale de la Santé et de l’Hygiène Publique, Ministére de la Santé et de l’Hygiène Publique, Mali; Dr. Anshu Banerjee, Director Department of Maternal, Newborn, Child, Adolescent Health & Ageing, World Health Organization (WHO), and Dr. Pedro Alonso, Director Global Malaria Programme, WHO. The discussion was moderated by Mildred Komey, Malaria in Pregnancy Focal Person, National Malaria Control Program, Ghans Health Service.
The discussion covered the importance of launching this call now, what we’ve learned over the last few years, and examples of innovative strategies from Mali. There was a Q&A session with journalists after the presentations.
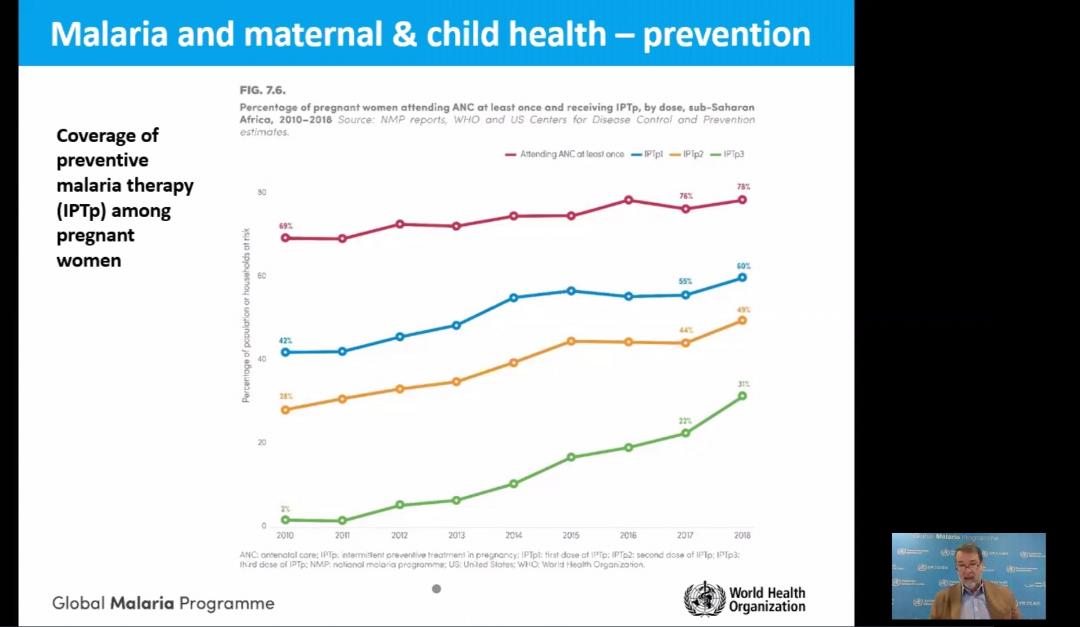
The presentation by Dr Alonso showed the progress in achieving IPTp coverage goals. He also pointed out the social and economic factors that affect access and equity to intermittent preventive treatment of malaria in pregnancy and protection of maternal health (see slides).
Experts say Africa must scale-up malaria protection for pregnant women
For a pregnant woman, her fetus, and the newborn child malaria infection carries substantial risks. Calling for a speedy scale-up to boost protection against malaria for pregnant women in Africa, the Roll Back Malaria, RBM Partnership to End Malaria Working Group is issuing an urgent appeal to leaders and health policymakers to increase access to Intermittent Preventive Treatment during pregnancy, IPTp, among eligible pregnant women in sub-Saharan Africa.
Along with stakeholders, the RBM Partnership is pushing for scale-up coverage of three doses of IPTp to reach all eligible women in sub-Saharan Africa by 2025. In 2019, according to the RBM Partnership, an estimated 11 million pregnant women in sub-Saharan Africa, or 29 percent of all pregnancies were infected with malaria.
Understanding how malaria protects its cells against heat and other onslaughts could lead to new ways to fight tough-to-kill strains, researchers say. Findings could lead to ways to maximize our existing antimalarial arsenal.
Global Fund and Chevron – United Against HIV, TB and Malaria
The Global Fund and Chevron Corporation have celebrated a 12-year partnership that served as an example of the private sector’s contribution to the fight against infectious diseases and to building resilient health systems. Chevron, a Global Fund partner since January 2008, has supported Global Fund programs against HIX4 tuberculosis and malaria for a total investment of US$60 million in Angola, Indonesia, Nigeria, the Philippines, South Africa, Thailand and Vietnam.
Chevron’s partnership has contributed to helping more than a million people living with HIV access lifesaving antiretroviral therapy; supported efforts to distribute over one million long-lasting insecticide-treated mosquito nets to families to prevent malaria; helped detect thousands of TB cases; promoted education programs for the young, and helped build stronger health systems.
In Nigeria, Chevron’s $5 million investment from October 2017 to December 201 9 supported the national HIV and TB programs, reaching key and vulnerable populations, as well as interventions aimed at strengthening the health system. Sustainable and resilient systems for health are indispensable in the fight against the epidemics of HIV TB and malaria, as well as the first line of defense against new diseases like COVID-19. “With rising cases of COVID-1 9, the stakes are very high. Deaths from HIV, TB and malaria are likely to increase. Investments by partners like Chevron are fundamental.
Differentiating malaria parasite species is something science can do today, but in the 1800s the debate was over what actually caused the disease. This ability to test and diagnose gives us an important surveillance tool, the 3Ts. News from Ghana is that malaria deaths are reducing, and Guatemala is focusing on elimination. Read more at the links in each section.
Wyss Researchers Develop Malaria Diagnostic Procedure Capable of Differentiating Malaria Species
Researchers at Harvard’s Wyss Institute have developed a new malaria diagnostic test that efficiently detects and can distinguish between species of malaria parasites,
the new procedure significantly improves upon current diagnostic methods, which fail to differentiate between types of malaria. Procedures that only identify Plasmodium falciparum can lead to severe consequences for patients, since other types of malaria are resilient to therapies designed to treat Plasmodium falciparum because they enter a dormant stage in the human liver.
These genes help explain how malaria parasites survive treatment with common drug.
In a paper published September 23 in Nature Communications, Whitehead Institute Member Sebastian Lourido and colleagues use genome screening techniques in the related parasite Toxoplasma gondii (T. gondii) to identify genes that affect the parasites’ susceptibility to artemisinin. Two genes stood out in the screen: one that makes the drug more lethal, and another that helps the parasite survive the treatment…
Test, Treat, and Track: Strengthening Malaria Response Capabilities in Sierra Leone
A public-private partnership in Sierra Leone aimed to build capacity for testing, treating, and tracking malaria. The post notes the “public-private partnership in Sierra Leone was a collaboration between USAID’s Human Resources for Health in 2030 (HRH2030) program; the U.S. President’s Malaria Initiative (PMI), the Global Fund to Fight AIDS, Tuberculosis and Malaria; the Pharmacy Consultancy of Sierra Leone; and the Sierra Leone National Malaria Control Program”.
NMCP partnered with pharmacies to strengthen their malaria case management capabilities. Anitta and her colleague Brenda Stafford, a trained pharmacist and Procurement and Supply Management officer, led the initiative, going pharmacy-to-pharmacy to train staff on the NMCP’s “Three T” approach: Test, Treat, and Track.
To address the first T, private pharmacies were given free malaria rapid diagnostic tests. According to 2016 data, only half of children under-five with fever received appropriate malaria testing. For the second T, the pharmacists were trained on malaria prevention, treating patients with uncomplicated malaria, and referring patients with severe malaria to health facilities. As for the last T, tracking malaria test results is key in forecasting the spread of disease. NMCP provided pharmacies with two forms that track results: a registry form to track patient information and a summary form which aggregates that into monthly data reports
Miasma War over cause of malaria was heated
Nicole Layton of the Chowan Herald reported that in the 1850s, two North Carolina doctors had a heated and protracted battle over the cause of malaria in the state. This Miasma War is so famous. So what the heck is Miasma? Those fans of Charles Dickens can tell you that at one point miasmas were thought to be the main vector for disease transmission.
During Dickens’ time in London the air was very foul and rather visible because of wood and coal and it smelled bad due to the lack of indoor plumbing. It was thought that this foul air was the cause of disease. Because our part of North Carolina had a lot of rotting vegetation and swamps there was certainly foul air about and very noticeable illness. So the general thought was that malaria was a result of this bad air.
Escuintla, Guatemala: Clinton Health Access Initiative (CHAI)
CHAI’s Guatemala Malaria Team is supporting the Ministry of Health’s National Malaria Program by providing technical assistance and supporting programmatic planning, execution, monitoring and evaluation of effective interventions in the department of Escuintla in southern Guatemala. Over the past five years, CHAI has engaged in the country and helped them make meaningful steps towards orienting their national strategic plans and systems towards the historical goal of malaria elimination.
CHAI’s Guatemala team works in close coordination with the Ministry of Health and other international partners to design, plan, execute and evaluate the impact of the country´s elimination-focused interventions in Escuintla.
Ghana: Malaria deaths in children under five reduce
Ghana has recorded a reduction in malaria deaths in children under five by 83 per cent over the last eight years, the National Malaria Control Programme (NMCP) has said. The rate of malaria-related deaths reduced from 0.6 per cent in 2012 to 0.1 per cent in 2019, showing significant inroads in malaria-related deaths among children. Malaria-related deaths of all ages also reduced by 2,799 in 2012 to 333 by end of 2019, representing an 88 per cent reduction.
Ramatsobane Johanna Ledwaba provides us with a guest blog to address the need to reach more school aged girls with vaccines for human papilloma (HPV) virus in South Africa and in the process prevent cervical cancer. Her blog originally appeared in Social, Cultural & Behavioral Issues in PHC & Global Health.
Cervical cancer is the first most common cancer in women and the first leading cancer related-deaths among South African women, aged 15-44 years. More that 12,000 women are diagnosed with cervical cancer annually, of which 5,500 die from cancer— age-specific incidence rate (15-44 years) of 41.8 per 100,000 women per year and age-specific mortality rate (15-44 years) of 11,7 per 100,000 women per year. Reasons for such a high mortality rate include, low screening coverage of 19.3%, and late presentation with an advanced stage compounded by the high HIV epidemic. The World Health Organization recommends a 2-dose HPV vaccination among girls of 9-13 years.
In 2014, the South African National Department of Health introduced a school-based HPV vaccination policy— using 2-dose Cervarix vaccine, as prevention for cervical cancer among girls aged 9 and above in grade 4 attending public schools. The policy aimed to vaccinate 500, 000 young girls from 18,000 public schools before their sexual debut.
HPV vaccine campaign poster distributed by the Department of Health. Source: Government Communication and Information SystemPreliminary data showed that 91% of schools were reached and 87% age eligible grade 4 girls were vaccinated, however there is a high dropout rate in the second dose.
Although the programme seems a success thus far, there is a need for expanded coverage of the vaccine to include higher grades that could potentially house girls of ages 11-13 years. In addition, the vaccine must be widely available at public health facilities for girls who were missed at school because they changed schools or dropped out.
Girls attending private schools are presumed to access HPV vaccine through the private health sector, however the HPV vaccine coverage in the private health sector remains low due to high costs and lack of awareness— which suggest that there is low coverage in private schools. Therefore, the vaccine must be expanded to include private schools. This gap may lead to poor coverage of HPV vaccination and may also increase perceptions or hesitancy against the vaccine because it is not widely available for all girls of targeted age. No girl must be left behind.
The full 2017 Malaria Indicator Survey (MIS) results have been published for Tanzania providing an opportunity to look at the findings in more detail. Several important factors need highlighting since Tanzania is part of a regional block where some countries are activly considering malaria elimination – the E8 countries of the Southern Africa Development Community.
So far Tanzania has come close to achieving a target of 80% of households owning insecticide treated nets (ITNs) with 78% on the mainland and 79% in Zanzibar. A closer look shows that there is still a ways to go to get to universal coverage or at least one net for every two persons in the household. With this indicator 45% of mainland and 42% of Zanzibar households have met the target, meaning that there are unprotected people in a majority of households across the country. This indicator experienced a drop from a 2011 “high” of 56%, a drop to 39% in 2015 and a slight recovery to 45% in 2017.
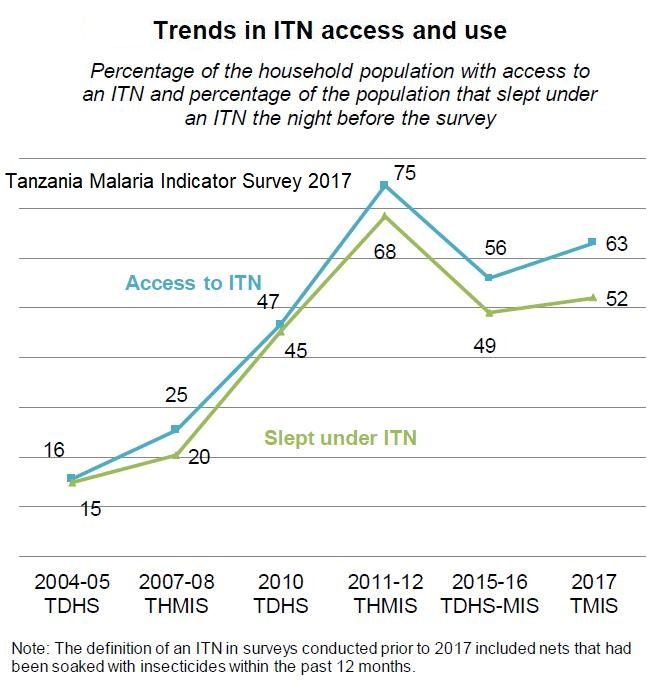
Even the universal coverage target requires that people actually sleep under the nets. What the MIS report shows is that although 63% of people had access to an ITN, only 52% reported sleeping under one the night before the survey.
Equity remains an issue with 69% of households in the lowest wealth quintile owning at least one net compared to 81% and 83% in the middle and fourth quintiles. Although households in the highest quintile had 78% ownership, this group is more likely to live in better quality housing that prevents the ingress of most mosquitoes. Also residents in urban areas have an edge over rural counterparts in terms of net access.
The report show that 55% of children under 5 years of age and 51% of pregnant women slept under an ITN. This is down from 72% and 75% respectively in 2011.
We learn that 90% of existing nets were obtained through some form of public sector campaign including mass distribution (62%), village coupons redeemable at health centers (15%), and school campaigns (4%). Only 5% were obtained through routine services (ANC, child immunization) indicating that efforts to ‘keep up’ after mass campaigns need to be strengthened. The 10% of nets, whether treated or not, that were obtained in shops and markets cost the owner in the neighborhood of US$5.00.
Uptake of doses of intermittent preventive treatment for malaria in pregnancy has slowly but steadily increased over the past 15 years and stood at 83% for one dose, 56% for two doses and 26% for three in this most recent MIS. With the current target being three or more doses needed for optimal protection, Tanzania still has a far long way to go, especially considering that accessing ITNs through ANC services is also low..
Andrianandraina Ralaivaomisa, Eliane Razafimandimby, Jean Pierre Rakotovao, Lalanirina Ravony Harintsoa, Sedera Aurélien Mioramalala, Rachel Favero, Katherine Wolf, Patricia Gomez, Jocelyn Razafindrakoto, and Laurent Kapesa of MCSP/Jhpiego (Johns Hopkins University Affiliate), the Madagascar Ministry of Public Health and USAID presented their findings about febrile illness care seeking in Madagascar at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. Details follow below.
Malaria Care and Treatment in Madagascar is hampered by low perception of malaria risk among caregivers. There is use of self-medication and a lack of health provider knowledge about malaria prevention and treatment in pregnant women. Low-quality care in primary health facilities is another concern (Source: WHO. 2015. Guidelines for the treatment of malaria, 3rd ed.).
As seen in the attached, Study Objectives focus on Caregivers and Pregnant Women as well as Health Providers to determine barriers to effective care seeking of febrile illnesses.
Both Qualitative and Quantitative Approaches were used. Among care seekers we conducted 16 focus group discussion sessions with 128 caregivers and pregnant women. There were also in-depth interviews with 32 pregnant women and 16 caregivers of children under 15. For Health Providers we conducted in-depth interview with 32 public and private health providers and administered 16 knowledge tests and case studies to health providers. We also reviewed logistic management information system records with 16 health
Barriers for Caregivers are seen in the attached table. Barriers were faced by both care seekers and those who did not seek care, but were more common among non-seekers.
Three tables follow that show perceptions of public sector providers, private providers and community health workers. There were positive and negative perceptions of each group of providers.
Health Provider Practices were also studied. They had low adherence to national guidelines for fever and malaria case management. Health workers reported high stock-outs rates of critical commodities (artemisinin-based combination therapy, artesunate). There was also lack of respectful care. Fortunately health provider diagnostic practices included 100% compliance with rapid diagnostic testing in cases of fever. They took temperatures and did physical exams appropriate to client’s symptoms and used microscopy at centers with local laboratory
General Bottlenecks to Timely Care Seeking still existed. There was insecurity due to political situation in some regions. Inability to pay for care or medications was common. Alternative health behaviors included seeking care with traditional healers, and self-medication. There was fear by clients of going to health facilities and inaccurate perceptions of care provided by formal health care system
Recommendations start with the need to train providers and CHWs on national treatment guidelines for managing fever in all age groups and in pregnant women. Efforts are needed to strengthen onsite provider mentoring and supportive supervision and improve respectful care of clients, especially in public sector. Since care seeking still based on cultural norms, there is need to strengthen community/family education about febrile illness dangers and advantages of timely care seeking. Communities can also consider forming “mutuelle” community insurance schemes to relieve cost of care burden.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Kate Klein as part of her Master of Science in Public Health program in Social and Behavioral Interventions at the Johns Hopkins Bloomberg School of Public Health undertook a study of the potential for private sector involvement in malaria prevention in Ghana. She shares a summary of her work here. During her practicum in Ghana she was hosted by JHU’s Center for Communications Programs and its USAID supported VectorWorks Program. Her practicum she was also supported by the JHU Center for Global Health, and she presented her findings in a poster at the CGH’s Global Health Day on 30th March 2017. Her essay readers/advisers were Dr. Elli Leontsini (Department of International Health) and Kathryn Bertram (Center for Communication Programs).
Malaria is endemic in all parts of Ghana and significantly burdens families, communities, and economies. Malaria remains a leading cause of morbidity and mortality in Ghana; it accounts for eight percent of deaths in the country (The Global Fund, Ghana). It was also responsible for about 38% of outpatient visits, 27.3% of admissions in health facilities, and 48.5% of under-five deaths in 2015 (Nonvignon et al., 2016). In Ghana, the estimated cost of malaria to businesses in 2014 alone was estimated to be US$6.58 million, and 90% of these were direct costs (Nonvignon et al., 2016). Malaria leads to reduced productivity due to increased worker absenteeism and increased health care spending, which negatively impact business returns and tax revenue to the state (Nabyonga et al., 2011).
Although long-lasting insecticidal treated nets (LLINs) are a well-documented strategy to prevent disease in developing countries, most governments, including Ghana, lack the resources needed to comprehensively control malaria. The Global Fund (GF), USAID/President’s Malaria Initiative (PMI Ghana), and the United Kingdom Department for International Development (DfID Ghana) are the main donors for the national malaria control strategy and have worked primarily with the public sector (World Malaria Report, 2015). As government funding remains unable to close the funding gap for malaria, there is an increasing need to revitalize the private sector in sales and distribution of this life-saving technology.
A “Journey mapping” exercise to consider the process of employers buying and distributing nets to employees, created during a PSMP advocacy workshop in December 2016
Ghana is looking to the private sector to encourage a departure from previous dependence on donor-funded free bed nets. The Private Sector Malaria Prevention (PSMP at JHU) project is being implemented in Southern Ghana to increase commercial sector distribution of LLINs. Three case studies served as a situation analysis and exemplified the potential for the PSMP: a rubber producing company, a mining company and a brewery.
All three had experience in malaria control and prevention but only one had specific experience with LLINs (which dovetailed well with its own corporate strengths in logistics management as exemplified by other bottling companies in Africa). Another supported the idea of adding LLINs to its existing indoor residual spraying and community health education efforts, but needed to consider how to develop the flexibility to engage in multiple malaria interventions.
The third had had the right climate and leadership to be able to partner with PSMP, but recently underwent a takeover by a large multinational brewing company and the resulting period of transition could potentially complicate their participation in LLIN distribution efforts from a budgetary standpoint. Generally these companies had the understanding of the potential benefits to the company of situating malaria control within their structure, and thus being early candidates for adoption of the PSMP.
While the three case study companies recognized the business case for malaria, this was not a unanimous opinion among other five companies interviewed. Their concerns ranged from a preference toward treatment interventions to concerns expressed by employees about the difficulty of achieving high levels of net usage due to an array of complaints surrounding sleeping under LLINs. Some of these others had financial constraints.
Through case studies and interviews PSMP was able to identify various challenges moving forward as well as areas where further clarity must be sought. PSMP learned that several companies are pouring their resources into strong treatment and case management programs, and one challenge will be determining how to push for preventative action, such as LLIN distribution, when treatment mechanisms are so established and bias exists.
For those companies who are making tremendous strides in malaria prevention, bringing recognition to these successes through advocacy will be necessary for encouraging future participation and convincing other similar employers of the benefits of starting their own LLIN distribution programs. Finally, PSMP needs to prioritize clarifying viewpoints on LLIN efficacy and use, with a focus on understanding why employers may hold unfavorable views and what it would take to overturn them.
In the future it will be necessary to move beyond the occupational considerations specific to mining and agro-industrial operations and consider how the work has changed the environment into a malaria habitat and the non-traditional work hours that may create more significant Anopheles mosquito exposures. PSMP should gather specific information on lifestyle, housing, and work environments during future visits with employers so that companies that have the most to gain through LLIN distribution are identified and targeted.
The technology of insecticide treated nets (ITNs) to prevent malaria has been around for over three decades. ITNs have evolved from a process of semi-annual soaking and impregnating nets with a safe insecticide at the household or community level to long lasting insecticide-treated nets (LLINs) where the insecticide is integrated into the nets during the manufacturing process. The challenge has always been guaranteeing enough currently treated nets to cover the population and impede malaria transmission.
Recently Rwanda announced its intentions to establish LLIN manufacturing in-country. The Ministry of Trade and Industry has begun screening of bidders. The government’s main rationale for this move is projected the need for a large and continuous supply of LLINs in the country through 2020, “making it a prudent to set up a production plant in the country.” When this information was shared with our malaria/tropical health update mailing list a number of readers expressed interest and hope that their own governments would follow suit. This post provides some background for readers to consider.
The idea of locally made mosquito nets is not new. MacCormack and Snow documented that, “95% of people were already sleeping under locally-made nets,” in The Gambia in the 1980s. Likewise in Burkina Faso it was common to find nets made from imported materials or local cotton that were sewn by local tailors.
The idea of drawing on the combination of local or regional textile and chemical industries to produce an ITN kit containing both net and approved insecticide for home/community soaking was tested in several countries by the USAID sponsored NetMark project between 1999–2009. Although the project made ITNs available at reduced prices and resulted in gains in awareness, ownership, and use of nets, “none of the countries reached the ambitious Abuja targets.”
Even at reduced prices the ITNs made available through this commercial sector approach were still more expensive than most families could afford. In addition partway through the project the emphasis shifted from local products to imported LLiNs leaving a leaving a very bitter taste, particularly in Nigeria with its large industrial sector, in mouths of the textile and chemical partners who during malaria partners meetings at the time expressed a sense of betrayal.
Talk arose in Nigeria about the potential for starting LLIN production in the country, but no one stepped forward with funding or technical assistance. In the meantime, on the other side of the continent, A to Z Textiles of Tanzania entered into a partnership and by 2003 LLINs were being produced in Arusha. Sumitomo Chemical provided a royalty-free technology license to the company for its Olyset LLINs. “By 2010, Olyset Net production capacity (at A to Z) reached 30 million LLINs per year, creating 8,000 jobs; more than half of the global Olyset Net output and an outstanding contribution to the local economy.”
Over the years A to Z Textiles were hard pressed, just like the few other LLIN manufacturers, to meet global demand. Over the period, the focus changed from protecting young children and pregnant women to universal coverage of the population. Also research and actual use found that the lifespan of an LLIN was not the 5 years as initially projected, but more like two. These factors meant that supply could rarely meet demand for regular replacement nets. No wonder Rwanda wants its own LLIN factory!
In addition to supply issues, does local availability of LLINs make a difference in fighting malaria? Regular studies by the Demographic and Health Survey group of USAID in Tanzania found that ITN use increased over time by children below five years of age. The most recent survey still shows that the 2010 Abuja target of 80% was not met (let alone a target of universal coverage), but the findings hint at the importance of having locally available LLINs.
Let’s wish Rwanda success in establishing its LLIN manufacturing capacity. For colleagues in Nigeria and elsewhere who have expressed interest in this issue, your advocacy work is just beginning.
“On February 2, 2010, NAFDAC launched the NAFDAC MAS, putting the power of product verification right in the hands of the consumer. MAS is powered by Sproxil’s award-winning cloud-based Mobile Product Authentication™ technology, and remains the world’s largest nation-wide implementation of consumer-facing SMS anti-counterfeiting technology in the world.”
Below are two malaria medicine packets recently purchased. After scratching the small label (see it circled, we got the SMS messages as posted. The NAFDAC registration number alone is not enough to ascertain the validity. This is a smart procedure, even without a smart phone. Of course one still needs to read the expiry dates!
1. OK Genuine P-Alaxin Tablet. Your PIN:949769012921 NRN:04-9495 Problem? Call 08039012929 NAFDAC & Bliss Care Sproxil SMS
2. OK Original Lonart DS tabs NRN:04-9927 Use mosquito nets to help avoid malaria Problem? Call 08039012929 NAFDAC & GREENLIFE CARE Sproxil Solution
In this posting Hajara Moses John of the Bauchi State Agency for the Control of HIV/AIDS, TBL and Malaria [BACATMA] shares lessons learned in supervising medicine sellers.
Our team had planned supervisory visit last week to patent medicine vendors (PMVs) where shop owners have been taught the correct management of childhood illnesses. Our experience one particular shop pulled together so many lessons about training and supervision, and we are sharing this here. In the first shop we visited that day we found a boy aged 12 behind the counter. I took on the role of a mystery client, and mentioned some symptoms to the boy. “My 5-year old son is at home with catarrh. His nose is really running and his breathing is fast. What do you recommend I give him?”
The boy mentioned a local brand of antihistamine. I asked if there was anything else we should do, and the boy said that should work fine.
Next I said my two-year old daughter was also unwell. She was having fever, shivers with aches and pains. Did he have any suggestions for her? His prompt answer was “Ampiclox.”
I then asked him where the owner of the shop was. He said, “Oh my father has traveled.” I asked what class the boy was in school, to which he said the first class of junior secondary school.
Word of our visit must have spread in the area, because then a woman rushed in who it turned out to be the boy’s mother and asked how she could help us.
We explained that we were from the Ministry and were going around to help medicine shop owners improve the quality of their services. The mother happily reported that she had received training “in malaria and those other small small diseases of pickin,” from the Minsirty fo health and again from a NGO.
I went back to case of the child with a respiratory infection and pointed out the breath counting beads on the table. She said it was her husband who had done the training where the beads were explained but never taught her how to use them. We then spent some time explaining to the mother and her son about the beads and demonstrated how to use them, and also explained about management of fever.
Finally I asked the mother why she was not in the shop since her husband had traveled. She said she was in the kitchen preparing lunch for the children, and as the oldest, the 12-year old was assumed capable of running the shop. We encouraged her to discuss as a family how they could share what they have learned about managing child illness and always ensure that a competent person is available in the shop.
Training of PMVs is not a simple matter. The person trained may not always be in the shop nor share what he/she learned with other salespeople. Supervision is necessary in order to reinforce what was learned during training and provides an opportunity to teach others on-the-job. PMVs provide a large portion of the services in many African communities, and we must ensure that they can focus on quality.
Jhpiego staff will again present a poster at the Tuesday noon (Nov 4) session of the American Society of Tropical Medicine and Hygiene Annual Meeting. Augustine M. Ngindu, Muthoni M. Kariuki, Sanyu Kigondu, Johnstone Akatu, Isaac M. Malonza, with support from USAID’s Maternal and Child Health Integrated Project (MCHIP) will share experiences with a poster titled, “Improving maternal and neonatal health: Complementary role of the private sector increasing uptake of intermittent preventive treatment for malaria in pregnancy in Kenya.” The abstract is provided below.
Malaria in pregnancy (MIP) is associated with poor pregnancy outcomes including maternal anaemia, intrauterine growth retardation and low birth weight. Kenya changed its policy on intermittent preventive treatment using Sulfadoxine Pyrimethamine (IPTp-SP) in 1998. However, IPTp coverage rates have remained low: 4% in 2003, 14% in 2007, 15% in 2008 and 25 % in 2010.
To increase the coverage rate, MCHIP supported malaria control and reproductive health divisions of the ministry of health, first to harmonize knowledge among service providers on provision of IPTp-SP in 2011, and second to train community health workers (CHWs) on sensitization of pregnant women to start early antenatal care (ANC) attendance in 2012.
A community survey conducted in 2013 showed a significant increase in the proportion of pregnant women receiving two or more IPTp doses from 25% to 63%, the highest increase in IPTp uptake since 1998. Following the successful scale up of IPTp, one sub-county conducted an assessment of its health facilities to determine quality of data on ANC clients accessing IPTp-SP.
A total of 15 (58%) out all 26 health facilities in the sub-county (public – 6 out of 8, faith-based – 2 out 3 and private – 7 out of 15) were selected. Data on new ANC clients, revisits and IPTp doses given was collected from the ANC registers.
Among the assessed health facilities 13 (87%) out of the 15 were registering new ANC cases, revisits and provided IPTp-SP (public 6, faith based 2, private 5. One private clinic provided ANC services to revisits and IPTp2 doses only after the clients had been registered in public facilities, the second did not offer ANC services.
In 2013 the government declared provision of free maternity services in public facilities but ANC clients have continued to utilize services from the private sector. This is an indication of the untapped potential in the private sector in increasing access to high impact interventions and importance of supporting the sector by all partners to provide these interventions.
Such complementary efforts if implemented will not only result in enabling the country to move towards achievement of set targets but also improve pregnancy outcomes through reduction in effects of
malaria in pregnancy.
Sign up for daily or weekly articles from Bill highlighting the most noteworthy developments in newspapers and scientific journals. Click here to register.
 A panel discussion and media briefing on new approaches and lessons learned formed part of an online global call to end malaria in pregnancy with intermittent preventive treatment. The briefing on Tuesday, 6 October 2020, was sponsored by the Roll Back Malaria Partnership and AMMREN. The RBM website features background on the call to action.
A panel discussion and media briefing on new approaches and lessons learned formed part of an online global call to end malaria in pregnancy with intermittent preventive treatment. The briefing on Tuesday, 6 October 2020, was sponsored by the Roll Back Malaria Partnership and AMMREN. The RBM website features background on the call to action.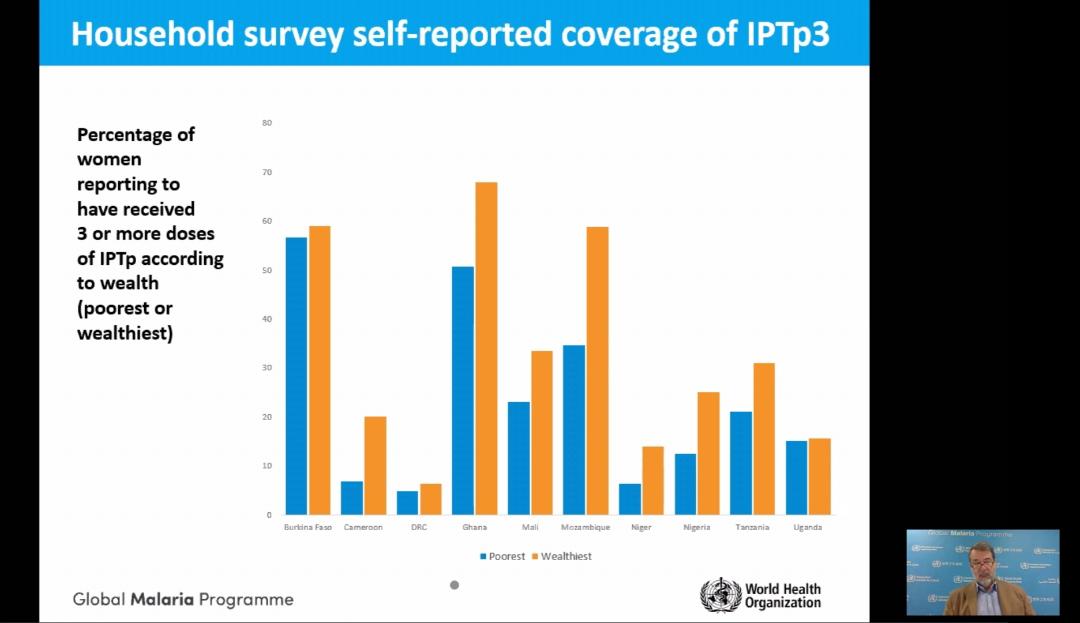 The discussion covered the importance of launching this call now, what we’ve learned over the last few years, and examples of innovative strategies from Mali. There was a Q&A session with journalists after the presentations.
The discussion covered the importance of launching this call now, what we’ve learned over the last few years, and examples of innovative strategies from Mali. There was a Q&A session with journalists after the presentations.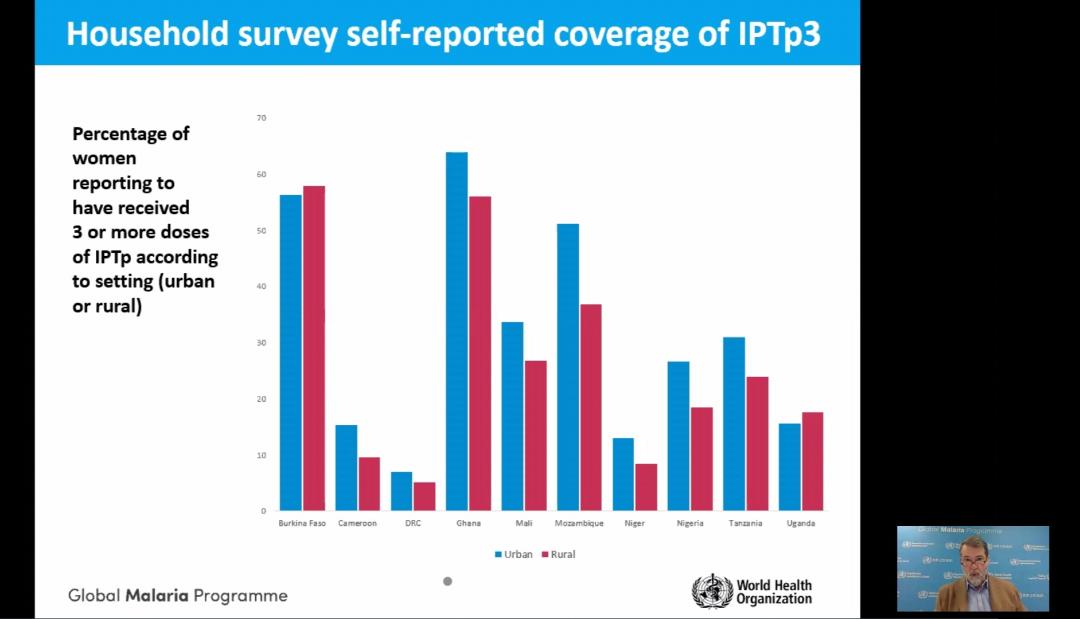 In support of the RBM/AMMREN briefing described above, Sola Ogundipe reports that amidst the COVID-19 pandemic in sub-Saharan Africa, malaria – one of the world’s oldest diseases – is impacting disproportionately on pregnant women and children aged under five.
In support of the RBM/AMMREN briefing described above, Sola Ogundipe reports that amidst the COVID-19 pandemic in sub-Saharan Africa, malaria – one of the world’s oldest diseases – is impacting disproportionately on pregnant women and children aged under five. Along with stakeholders, the RBM Partnership is pushing for scale-up coverage of three doses of IPTp to reach all eligible women in sub-Saharan Africa by 2025. In 2019, according to the RBM Partnership, an estimated 11 million pregnant women in sub-Saharan Africa, or 29 percent of all pregnancies were infected with malaria.
Along with stakeholders, the RBM Partnership is pushing for scale-up coverage of three doses of IPTp to reach all eligible women in sub-Saharan Africa by 2025. In 2019, according to the RBM Partnership, an estimated 11 million pregnant women in sub-Saharan Africa, or 29 percent of all pregnancies were infected with malaria.
 The full 2017 Malaria Indicator Survey (MIS) results have been published for Tanzania providing an opportunity to look at the findings in more detail. Several important factors need highlighting since Tanzania is part of a regional block where some countries are activly considering malaria elimination – the E8 countries of the Southern Africa Development Community.
The full 2017 Malaria Indicator Survey (MIS) results have been published for Tanzania providing an opportunity to look at the findings in more detail. Several important factors need highlighting since Tanzania is part of a regional block where some countries are activly considering malaria elimination – the E8 countries of the Southern Africa Development Community.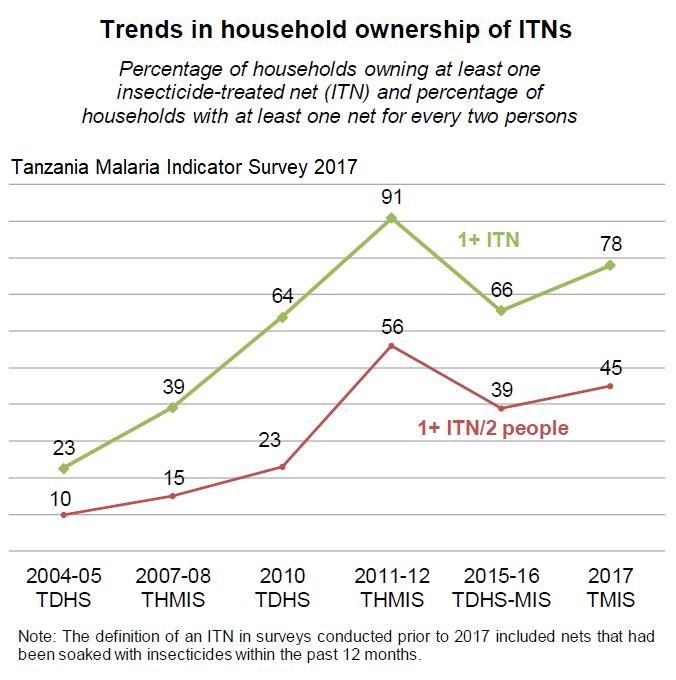
 The report show that 55% of children under 5 years of age and 51% of pregnant women slept under an ITN. This is down from 72% and 75% respectively in 2011.
The report show that 55% of children under 5 years of age and 51% of pregnant women slept under an ITN. This is down from 72% and 75% respectively in 2011.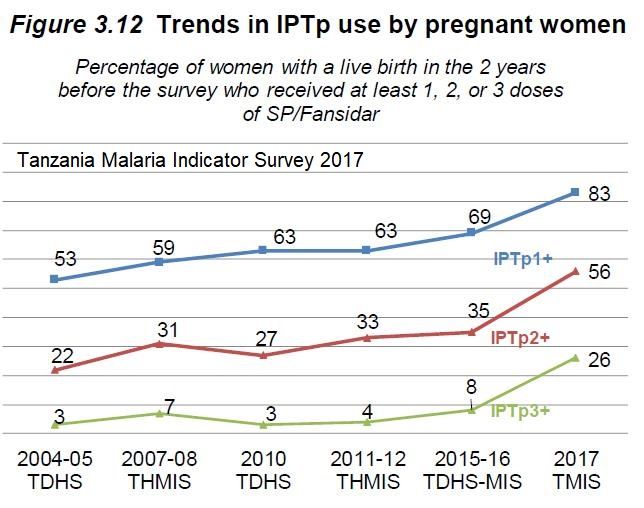 indicating that efforts to ‘keep up’ after mass campaigns need to be strengthened. The 10% of nets, whether treated or not, that were obtained in shops and markets cost the owner in the neighborhood of US$5.00.
indicating that efforts to ‘keep up’ after mass campaigns need to be strengthened. The 10% of nets, whether treated or not, that were obtained in shops and markets cost the owner in the neighborhood of US$5.00. Andrianandraina Ralaivaomisa, Eliane Razafimandimby, Jean Pierre Rakotovao, Lalanirina Ravony Harintsoa, Sedera Aurélien Mioramalala, Rachel Favero, Katherine Wolf, Patricia Gomez, Jocelyn Razafindrakoto, and Laurent Kapesa of MCSP/Jhpiego (Johns Hopkins University Affiliate), the Madagascar Ministry of Public Health and USAID presented their findings about febrile illness care seeking in Madagascar at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. Details follow below.
Andrianandraina Ralaivaomisa, Eliane Razafimandimby, Jean Pierre Rakotovao, Lalanirina Ravony Harintsoa, Sedera Aurélien Mioramalala, Rachel Favero, Katherine Wolf, Patricia Gomez, Jocelyn Razafindrakoto, and Laurent Kapesa of MCSP/Jhpiego (Johns Hopkins University Affiliate), the Madagascar Ministry of Public Health and USAID presented their findings about febrile illness care seeking in Madagascar at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene. Details follow below.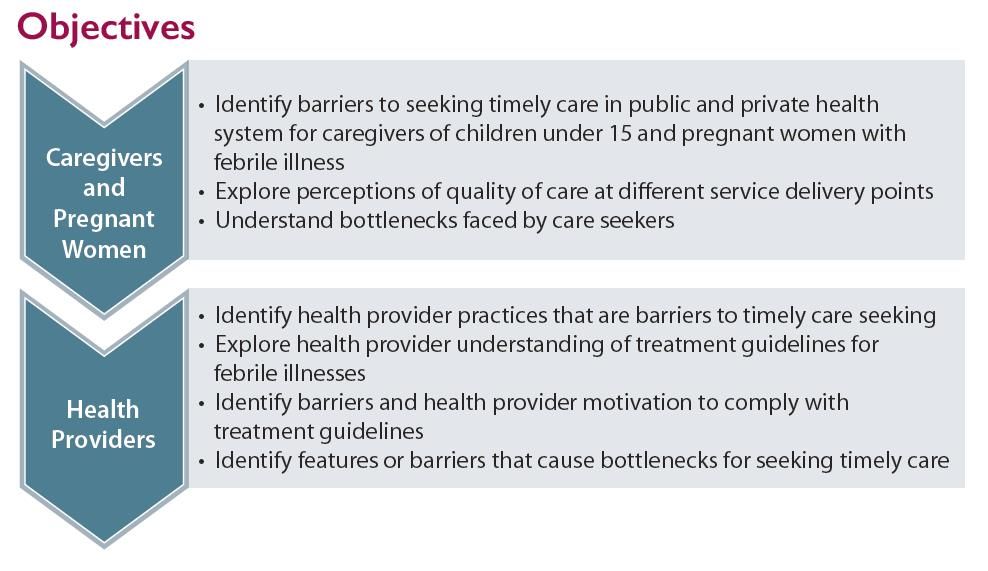 Malaria Care and Treatment in Madagascar is hampered by low perception of malaria risk among caregivers. There is use of self-medication and a lack of health provider knowledge about malaria prevention and treatment in pregnant women. Low-quality care in primary health facilities is another concern (Source: WHO. 2015. Guidelines for the treatment of malaria, 3rd ed.).
Malaria Care and Treatment in Madagascar is hampered by low perception of malaria risk among caregivers. There is use of self-medication and a lack of health provider knowledge about malaria prevention and treatment in pregnant women. Low-quality care in primary health facilities is another concern (Source: WHO. 2015. Guidelines for the treatment of malaria, 3rd ed.).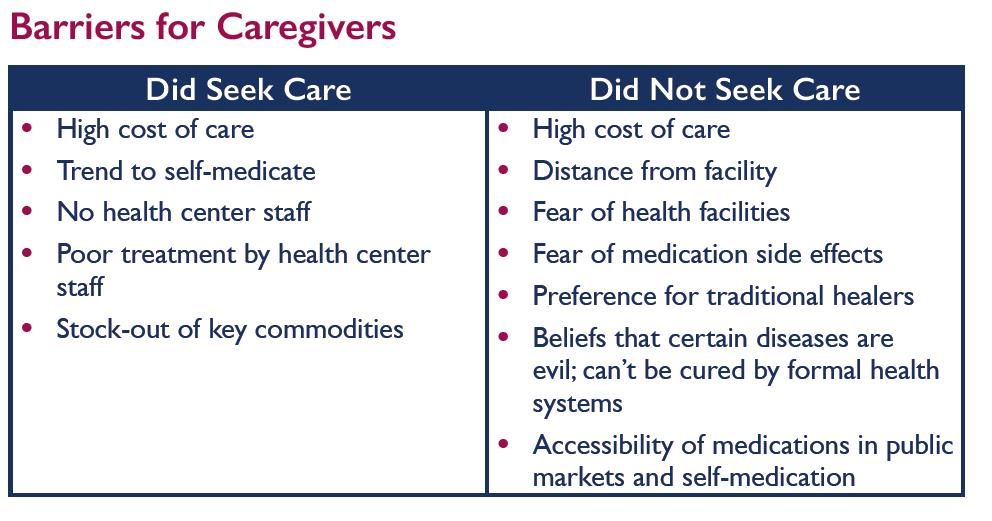 Both Qualitative and Quantitative Approaches were used. Among care seekers we conducted 16 focus group discussion sessions with 128 caregivers and pregnant women. There were also in-depth interviews with 32 pregnant women and 16 caregivers of children under 15. For Health Providers we conducted in-depth interview with 32 public and private health providers and administered 16 knowledge tests and case studies to health providers. We also reviewed logistic management information system records with 16 health
Both Qualitative and Quantitative Approaches were used. Among care seekers we conducted 16 focus group discussion sessions with 128 caregivers and pregnant women. There were also in-depth interviews with 32 pregnant women and 16 caregivers of children under 15. For Health Providers we conducted in-depth interview with 32 public and private health providers and administered 16 knowledge tests and case studies to health providers. We also reviewed logistic management information system records with 16 health Barriers for Caregivers are seen in the attached table. Barriers were faced by both care seekers and those who did not seek care, but were more common among non-seekers.
Barriers for Caregivers are seen in the attached table. Barriers were faced by both care seekers and those who did not seek care, but were more common among non-seekers.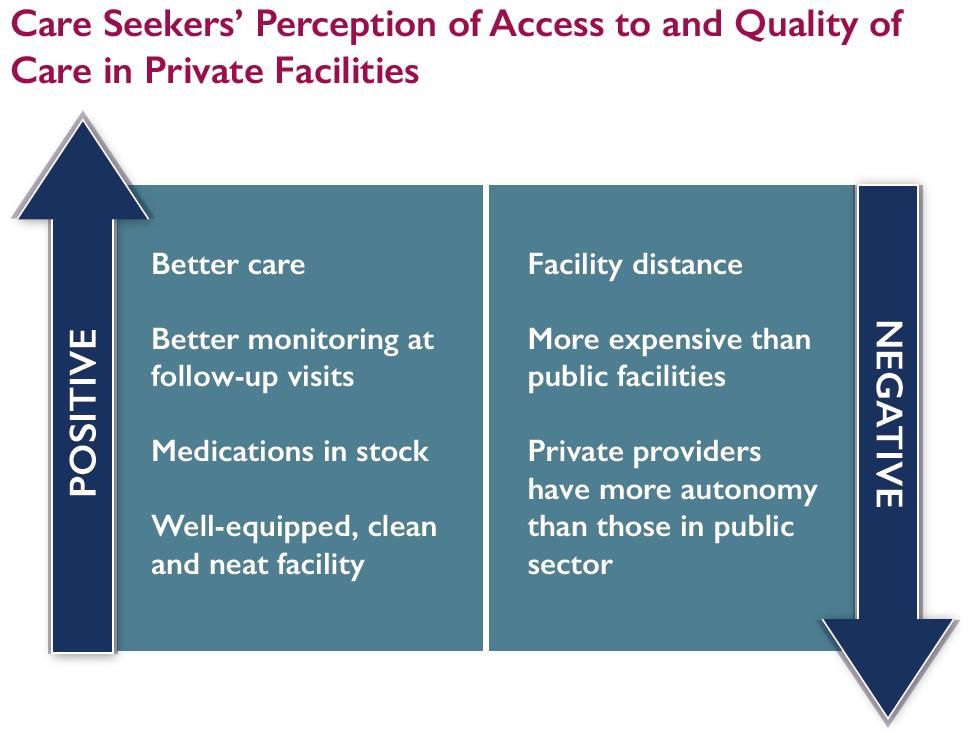 There were positive and negative perceptions of each group of providers.
There were positive and negative perceptions of each group of providers.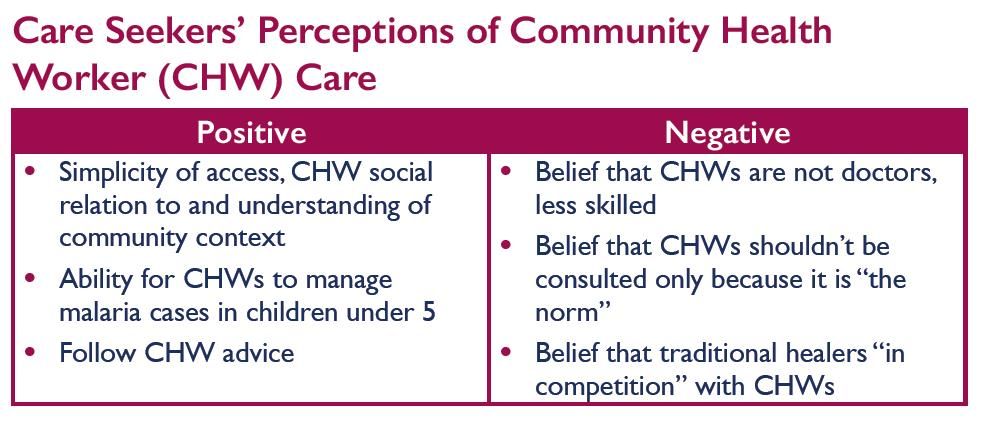 General Bottlenecks to Timely Care Seeking still existed. There was insecurity due to political situation in some regions. Inability to pay for care or medications was common. Alternative health behaviors included seeking care with traditional healers, and self-medication. There was fear by clients of going to health facilities and inaccurate perceptions of care provided by formal health care system
General Bottlenecks to Timely Care Seeking still existed. There was insecurity due to political situation in some regions. Inability to pay for care or medications was common. Alternative health behaviors included seeking care with traditional healers, and self-medication. There was fear by clients of going to health facilities and inaccurate perceptions of care provided by formal health care system This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.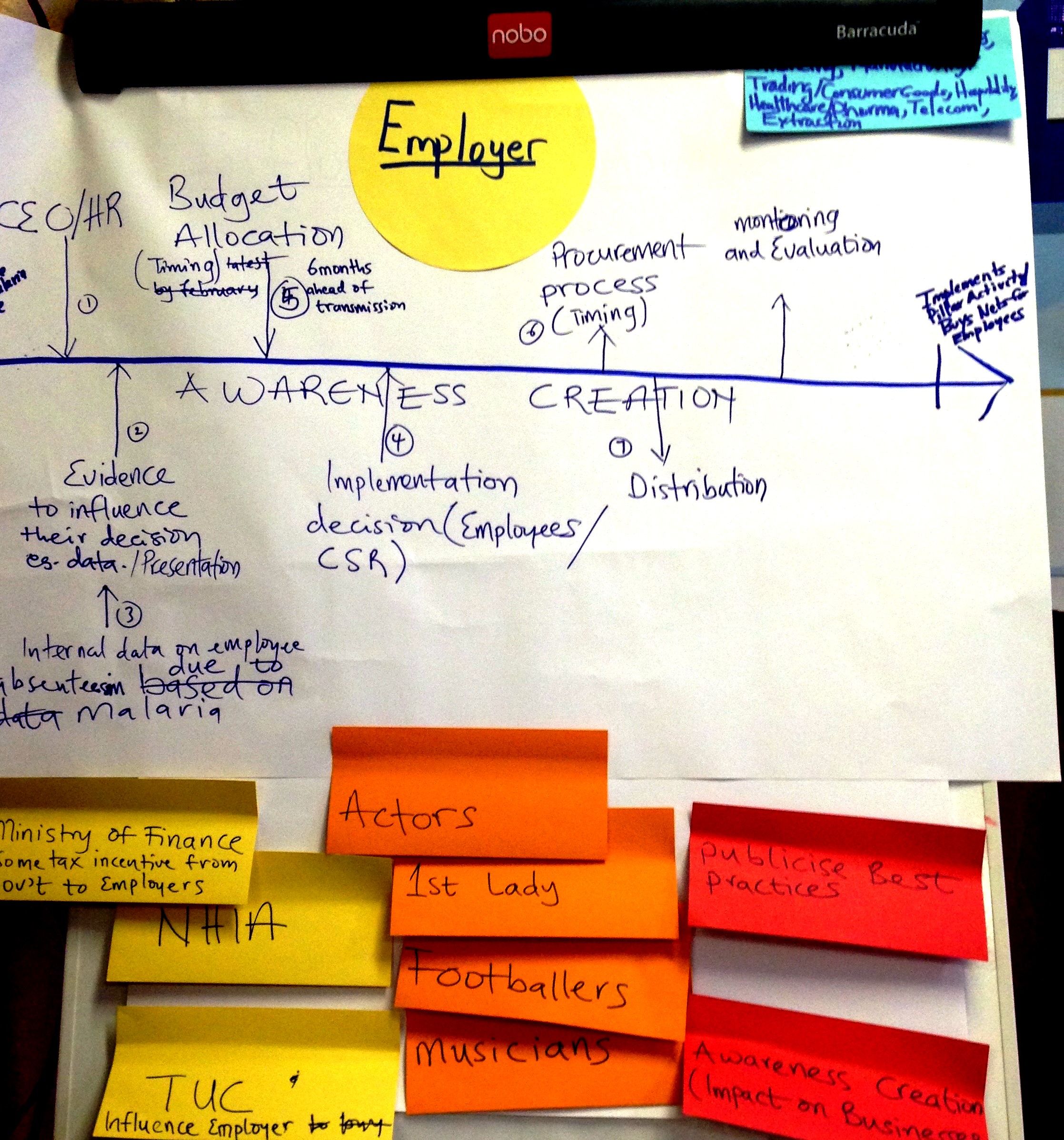
 While the three case study companies recognized the business case for malaria, this was not a unanimous opinion among other five companies interviewed. Their concerns ranged from a preference toward treatment interventions to concerns expressed by employees about the difficulty of achieving high levels of net usage due to an array of complaints surrounding sleeping under LLINs. Some of these others had financial constraints.
While the three case study companies recognized the business case for malaria, this was not a unanimous opinion among other five companies interviewed. Their concerns ranged from a preference toward treatment interventions to concerns expressed by employees about the difficulty of achieving high levels of net usage due to an array of complaints surrounding sleeping under LLINs. Some of these others had financial constraints. Recently Rwanda announced its intentions to establish LLIN manufacturing in-country. The Ministry of Trade and Industry has begun screening of bidders. The government’s main rationale for this move is projected the need for a large and continuous supply of LLINs in the country through 2020, “making it a prudent to set up a production plant in the country.” When this information was shared with our malaria/tropical health update mailing list a number of readers expressed interest and hope that their own governments would follow suit. This post provides some background for readers to consider.
Recently Rwanda announced its intentions to establish LLIN manufacturing in-country. The Ministry of Trade and Industry has begun screening of bidders. The government’s main rationale for this move is projected the need for a large and continuous supply of LLINs in the country through 2020, “making it a prudent to set up a production plant in the country.” When this information was shared with our malaria/tropical health update mailing list a number of readers expressed interest and hope that their own governments would follow suit. This post provides some background for readers to consider. nets,” in The Gambia in the 1980s. Likewise in Burkina Faso it was common to find nets made from imported materials or local cotton that were sewn by local tailors.
nets,” in The Gambia in the 1980s. Likewise in Burkina Faso it was common to find nets made from imported materials or local cotton that were sewn by local tailors. Even at reduced prices the ITNs made available through this commercial sector approach were still more expensive than most families could afford. In addition partway through the project the emphasis shifted from local products to imported LLiNs leaving a leaving a very bitter taste, particularly in Nigeria with its large industrial sector, in mouths of the textile and chemical partners who during malaria partners meetings at the time expressed a sense of betrayal.
Even at reduced prices the ITNs made available through this commercial sector approach were still more expensive than most families could afford. In addition partway through the project the emphasis shifted from local products to imported LLiNs leaving a leaving a very bitter taste, particularly in Nigeria with its large industrial sector, in mouths of the textile and chemical partners who during malaria partners meetings at the time expressed a sense of betrayal. Talk arose in Nigeria about the potential for starting LLIN production in the country, but no one stepped forward with funding or technical assistance. In the meantime, on the other side of the continent, A to Z Textiles of Tanzania entered into a partnership and by 2003 LLINs were being produced in Arusha. Sumitomo Chemical provided a royalty-free technology license to the company for its Olyset LLINs. “By 2010, Olyset Net production capacity (at A to Z) reached 30 million LLINs per year, creating 8,000 jobs; more than half of the global Olyset Net output and an outstanding contribution to the local economy.”
Talk arose in Nigeria about the potential for starting LLIN production in the country, but no one stepped forward with funding or technical assistance. In the meantime, on the other side of the continent, A to Z Textiles of Tanzania entered into a partnership and by 2003 LLINs were being produced in Arusha. Sumitomo Chemical provided a royalty-free technology license to the company for its Olyset LLINs. “By 2010, Olyset Net production capacity (at A to Z) reached 30 million LLINs per year, creating 8,000 jobs; more than half of the global Olyset Net output and an outstanding contribution to the local economy.” In addition to supply issues, does local availability of LLINs make a difference in fighting malaria? Regular studies by the Demographic and Health Survey group of USAID in Tanzania found that ITN use increased over time by children below five years of age. The most recent survey still shows that the 2010 Abuja target of 80% was not met (let alone a target of universal coverage), but the findings hint at the importance of having locally available LLINs.
In addition to supply issues, does local availability of LLINs make a difference in fighting malaria? Regular studies by the Demographic and Health Survey group of USAID in Tanzania found that ITN use increased over time by children below five years of age. The most recent survey still shows that the 2010 Abuja target of 80% was not met (let alone a target of universal coverage), but the findings hint at the importance of having locally available LLINs.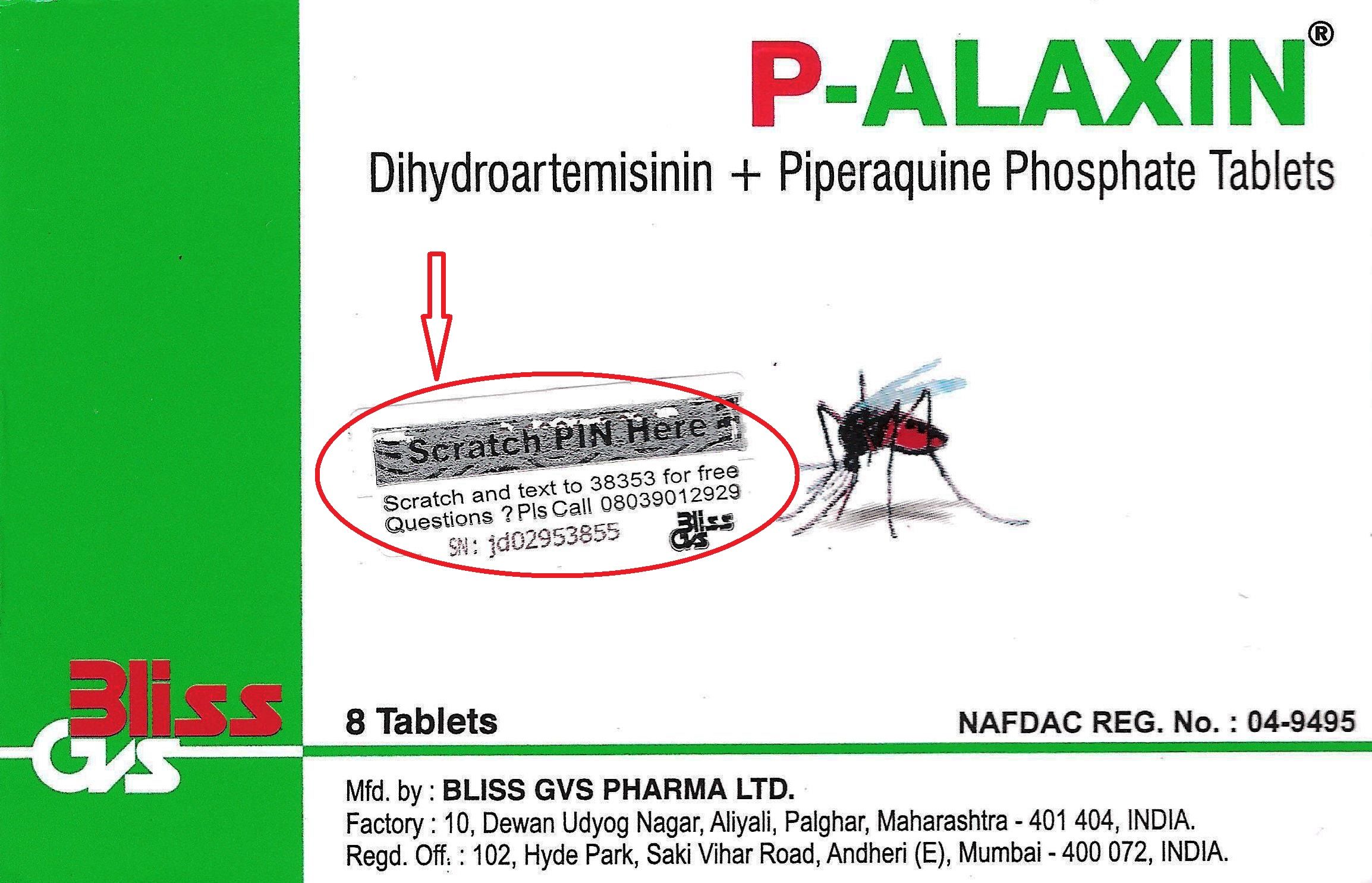 1. OK Genuine P-Alaxin Tablet. Your PIN:949769012921 NRN:04-9495 Problem? Call 08039012929 NAFDAC & Bliss Care Sproxil SMS
1. OK Genuine P-Alaxin Tablet. Your PIN:949769012921 NRN:04-9495 Problem? Call 08039012929 NAFDAC & Bliss Care Sproxil SMS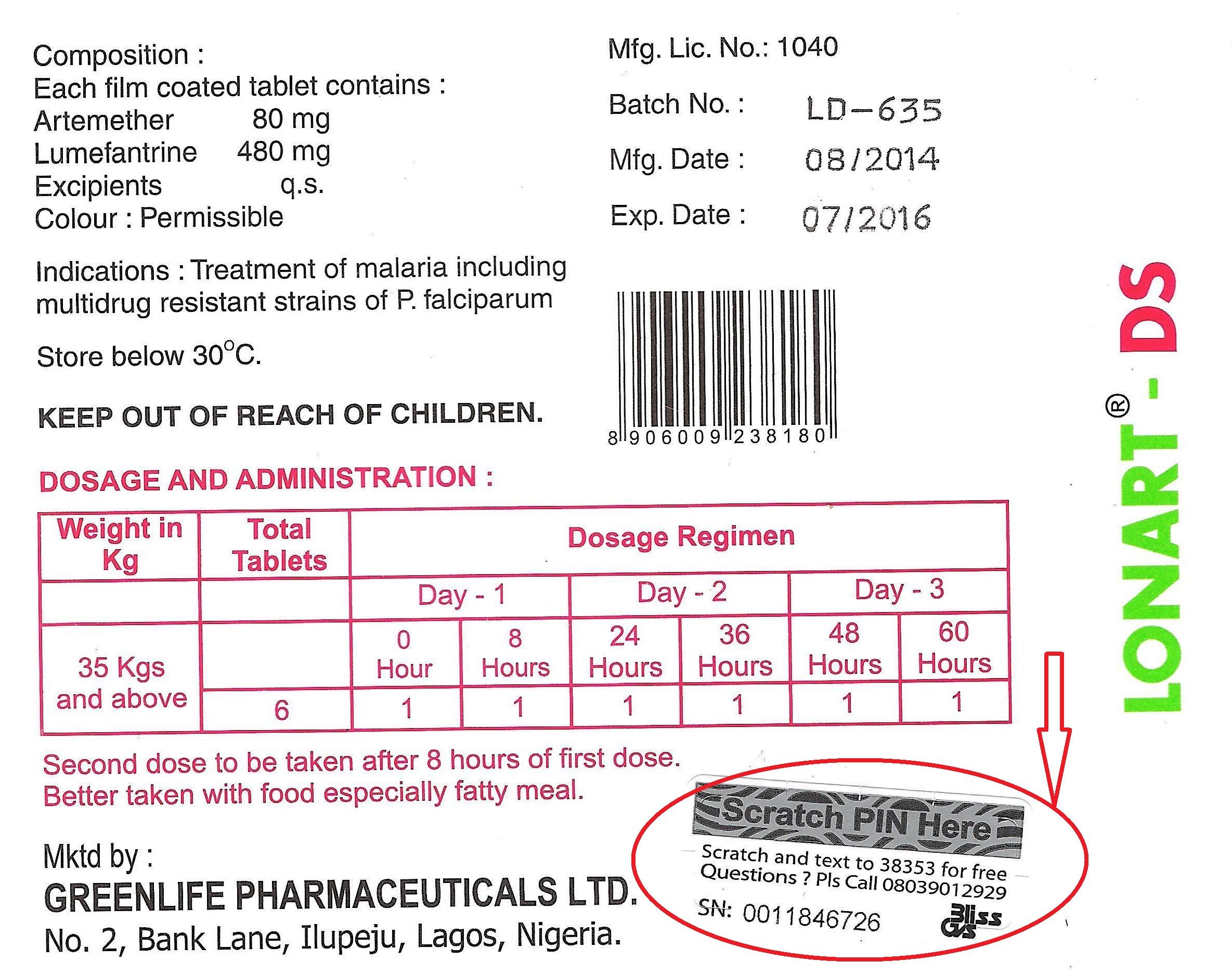 2. OK Original Lonart DS tabs NRN:04-9927 Use mosquito nets to help avoid malaria Problem? Call 08039012929 NAFDAC & GREENLIFE CARE Sproxil Solution
2. OK Original Lonart DS tabs NRN:04-9927 Use mosquito nets to help avoid malaria Problem? Call 08039012929 NAFDAC & GREENLIFE CARE Sproxil Solution In this posting Hajara Moses John of the Bauchi State Agency for the Control of HIV/AIDS, TBL and Malaria [BACATMA] shares lessons learned in supervising medicine sellers.
In this posting Hajara Moses John of the Bauchi State Agency for the Control of HIV/AIDS, TBL and Malaria [BACATMA] shares lessons learned in supervising medicine sellers. Malaria in pregnancy (MIP) is associated with poor pregnancy outcomes including maternal anaemia, intrauterine growth retardation and low birth weight. Kenya changed its policy on intermittent preventive treatment using Sulfadoxine Pyrimethamine (IPTp-SP) in 1998. However, IPTp coverage rates have remained low: 4% in 2003, 14% in 2007, 15% in 2008 and 25 % in 2010.
Malaria in pregnancy (MIP) is associated with poor pregnancy outcomes including maternal anaemia, intrauterine growth retardation and low birth weight. Kenya changed its policy on intermittent preventive treatment using Sulfadoxine Pyrimethamine (IPTp-SP) in 1998. However, IPTp coverage rates have remained low: 4% in 2003, 14% in 2007, 15% in 2008 and 25 % in 2010.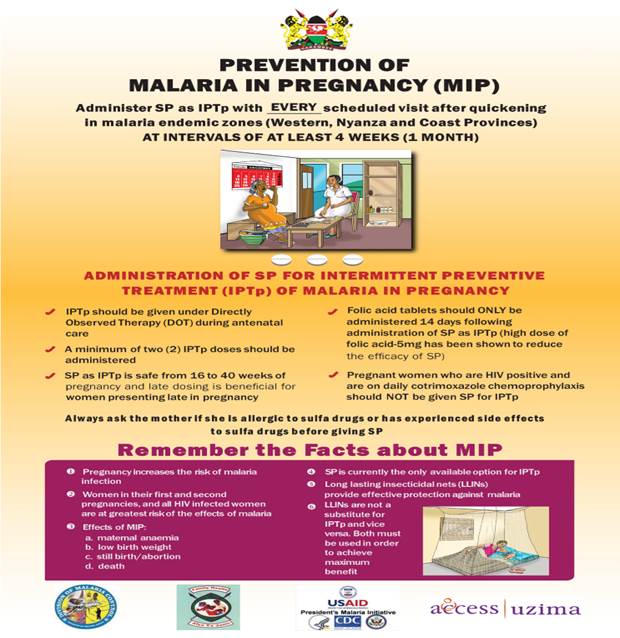 A community survey conducted in 2013 showed a significant increase in the proportion of pregnant women receiving two or more IPTp doses from 25% to 63%, the highest increase in IPTp uptake since 1998. Following the successful scale up of IPTp, one sub-county conducted an assessment of its health facilities to determine quality of data on ANC clients accessing IPTp-SP.
A community survey conducted in 2013 showed a significant increase in the proportion of pregnant women receiving two or more IPTp doses from 25% to 63%, the highest increase in IPTp uptake since 1998. Following the successful scale up of IPTp, one sub-county conducted an assessment of its health facilities to determine quality of data on ANC clients accessing IPTp-SP. e assessed health facilities 13 (87%) out of the 15 were registering new ANC cases, revisits and provided IPTp-SP (public 6, faith based 2, private 5. One private clinic provided ANC services to revisits and IPTp2 doses only after the clients had been registered in public facilities, the second did not offer ANC services.
e assessed health facilities 13 (87%) out of the 15 were registering new ANC cases, revisits and provided IPTp-SP (public 6, faith based 2, private 5. One private clinic provided ANC services to revisits and IPTp2 doses only after the clients had been registered in public facilities, the second did not offer ANC services.