Capacity Building &Case Management &Funding &Health Systems &IPTp &ITNs &Leadership Bill Brieger | 09 Feb 2019
Guinea: The Challenge of Malaria Control in a Post-Ebola Context
The preliminary 2018 Demographic and Health Survey (DHS) data have been released for Guinea (Conakry). Since the last DHS in 2012, Guinea and its neighbors experienced the largest Ebola outbreak in history, an event that damaged already weak health systems.
 The previous DHS showed very weak malaria indicators. Only 47% of households had at least one ITN, which averages to 0.8 ITNs per person (compared to the universal coverage of 2.0). Among vulnerable groups only 26% of children below the age of 5 years slept under an ITN, as did 28% of pregnant women. Very few, 18%, pregnant women got two doses of IPTp, and only 5% of febrile children received ACTs (testing was not reported then).
The previous DHS showed very weak malaria indicators. Only 47% of households had at least one ITN, which averages to 0.8 ITNs per person (compared to the universal coverage of 2.0). Among vulnerable groups only 26% of children below the age of 5 years slept under an ITN, as did 28% of pregnant women. Very few, 18%, pregnant women got two doses of IPTp, and only 5% of febrile children received ACTs (testing was not reported then).
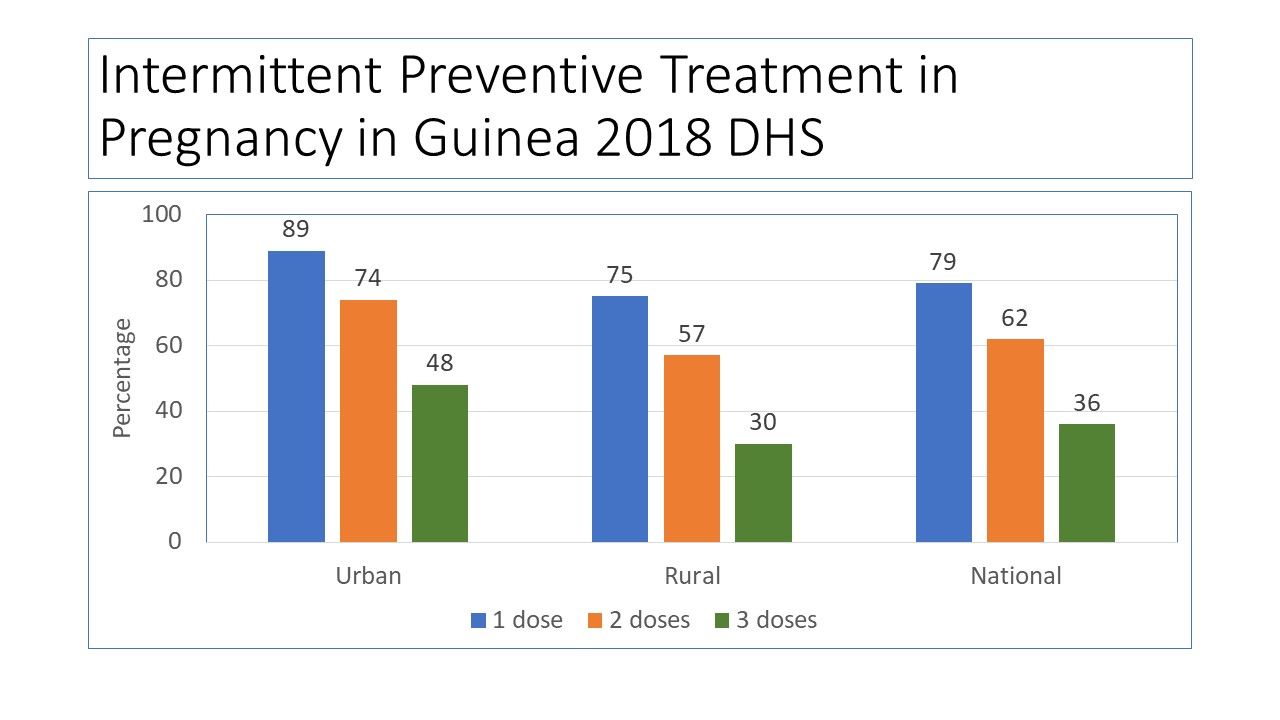
 Not much has changed concerning ITN coverage as reported in 2018. Slight improvements are seen in IPTp (which now requires 3 or more doses) and malaria testing and treatment for children. Ironically none of the indicators has passed the original 2006 Roll Back Malaria target of 60%, let alone 80% for 2010 and not of course the drive for universal coverage.
Not much has changed concerning ITN coverage as reported in 2018. Slight improvements are seen in IPTp (which now requires 3 or more doses) and malaria testing and treatment for children. Ironically none of the indicators has passed the original 2006 Roll Back Malaria target of 60%, let alone 80% for 2010 and not of course the drive for universal coverage.
 DHS has released a preliminary report for 2018 and the malaria component is summarized in the charts posted here. The national coverage for ITNs is 44%, slightly lower than 2012, but the average per household member is slightly higher at 1.1. Again, these numbers do not mark significant progress. Looking at wealth and ITN ownership there is a slight benefit in terms of equity in net possession among those with lower income, but this must be seen in the overall context of very low basic coverage.
DHS has released a preliminary report for 2018 and the malaria component is summarized in the charts posted here. The national coverage for ITNs is 44%, slightly lower than 2012, but the average per household member is slightly higher at 1.1. Again, these numbers do not mark significant progress. Looking at wealth and ITN ownership there is a slight benefit in terms of equity in net possession among those with lower income, but this must be seen in the overall context of very low basic coverage.
 Having a net in the household and using it are different challenges as seen in the reports of sleeping under the net on the night prior to the survey among children under 5 years of age and pregnant women. The sad finding is that even in households that own a net, the coverage of these two groups remains very low. This is reflected in the low net per person ratio nationally (1.1).
Having a net in the household and using it are different challenges as seen in the reports of sleeping under the net on the night prior to the survey among children under 5 years of age and pregnant women. The sad finding is that even in households that own a net, the coverage of these two groups remains very low. This is reflected in the low net per person ratio nationally (1.1).
 One would almost wonder if malaria is a neglected disease in Guinea. The reality is that since 2003, Guinea has received around $172 million US dollars in malaria project funding from the Global Fund. Its most recent annual funding from the US President’s Malaria Initiative (PMI) is around $14 million. Of that PMI funding 24% was designated for nets and related activities, while 52% was to be spent on medicines, diagnostics and pharmaceutical management. These investments include systems strengthening and capacity building in addition to commodities.
One would almost wonder if malaria is a neglected disease in Guinea. The reality is that since 2003, Guinea has received around $172 million US dollars in malaria project funding from the Global Fund. Its most recent annual funding from the US President’s Malaria Initiative (PMI) is around $14 million. Of that PMI funding 24% was designated for nets and related activities, while 52% was to be spent on medicines, diagnostics and pharmaceutical management. These investments include systems strengthening and capacity building in addition to commodities.
PMI provides the needed context: “Since the country was declared Ebola-free in in June of 2016, Guinea continues to make positive advances towards building a strong health system in line with the health recovery plan. The government continues to mobilize internal and external resources for rolling out the health system recovery plan, but much remains to be done if this plan is to yield the intended results.” Areas in particular need of strengthening within the National Malaria Control Program include coordination, health information systems, leadership, supervision and logistics.
Three years have passed since the last Ebola case in Guinea. Hopefully the country can stave off another outbreak and at the same time strengthen its health system. Guinea may not yet be targeted for malaria elimination, but until systems are strengthened, the resources going into malaria control will not be able to push malaria indicators toward saving more lives.
Health Information &Health Systems &Health Workers &Leadership Bill Brieger | 30 Oct 2018
Assessing Organizational Capacity to Deliver Malaria Services in Rural Liberia
 Swaliho F. Kamara, Wede Tate, Allyson R. Nelson, Lauretta N. Se, Lolade Oseni, Gladys Tetteh of MCSP/Jhpiego are presenting a poster at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene on Malaria Service delivery in rural Liberia. Their findings are shared below:
Swaliho F. Kamara, Wede Tate, Allyson R. Nelson, Lauretta N. Se, Lolade Oseni, Gladys Tetteh of MCSP/Jhpiego are presenting a poster at the 2018 Annual Meeting of the American Society of Tropical Medicine and Hygiene on Malaria Service delivery in rural Liberia. Their findings are shared below:
 In Liberia Malaria prevalence in children under 5 is 45% nationally and higher in rural counties (NMCP et al. 2017). The National Malaria Control Program (NMCP) leads the rollout of malaria prevention and control activities to county health teams (CHTs), per the National Malaria Strategic Plan (2016–2020). A key donor supporting malaria prevention and control, the President’s Malaria Initiative (PMI), has been committed to the Ministry of Health and Social Welfare (MOHSW) strategy since 2008, when it began working in three out of 15 malaria-affected counties. PMI supports CHTs in their management of local health systems and service delivery oversight. As part of an expansion program to five additional rural, neglected, high-burden counties in 2017, the United States Agency for International Development (USAID)/ PMI-funded Maternal and Child Survival Program (MCSP) assessed CHTs’ organizational capacity to identify ways to improve the quality of malaria health services.
In Liberia Malaria prevalence in children under 5 is 45% nationally and higher in rural counties (NMCP et al. 2017). The National Malaria Control Program (NMCP) leads the rollout of malaria prevention and control activities to county health teams (CHTs), per the National Malaria Strategic Plan (2016–2020). A key donor supporting malaria prevention and control, the President’s Malaria Initiative (PMI), has been committed to the Ministry of Health and Social Welfare (MOHSW) strategy since 2008, when it began working in three out of 15 malaria-affected counties. PMI supports CHTs in their management of local health systems and service delivery oversight. As part of an expansion program to five additional rural, neglected, high-burden counties in 2017, the United States Agency for International Development (USAID)/ PMI-funded Maternal and Child Survival Program (MCSP) assessed CHTs’ organizational capacity to identify ways to improve the quality of malaria health services.
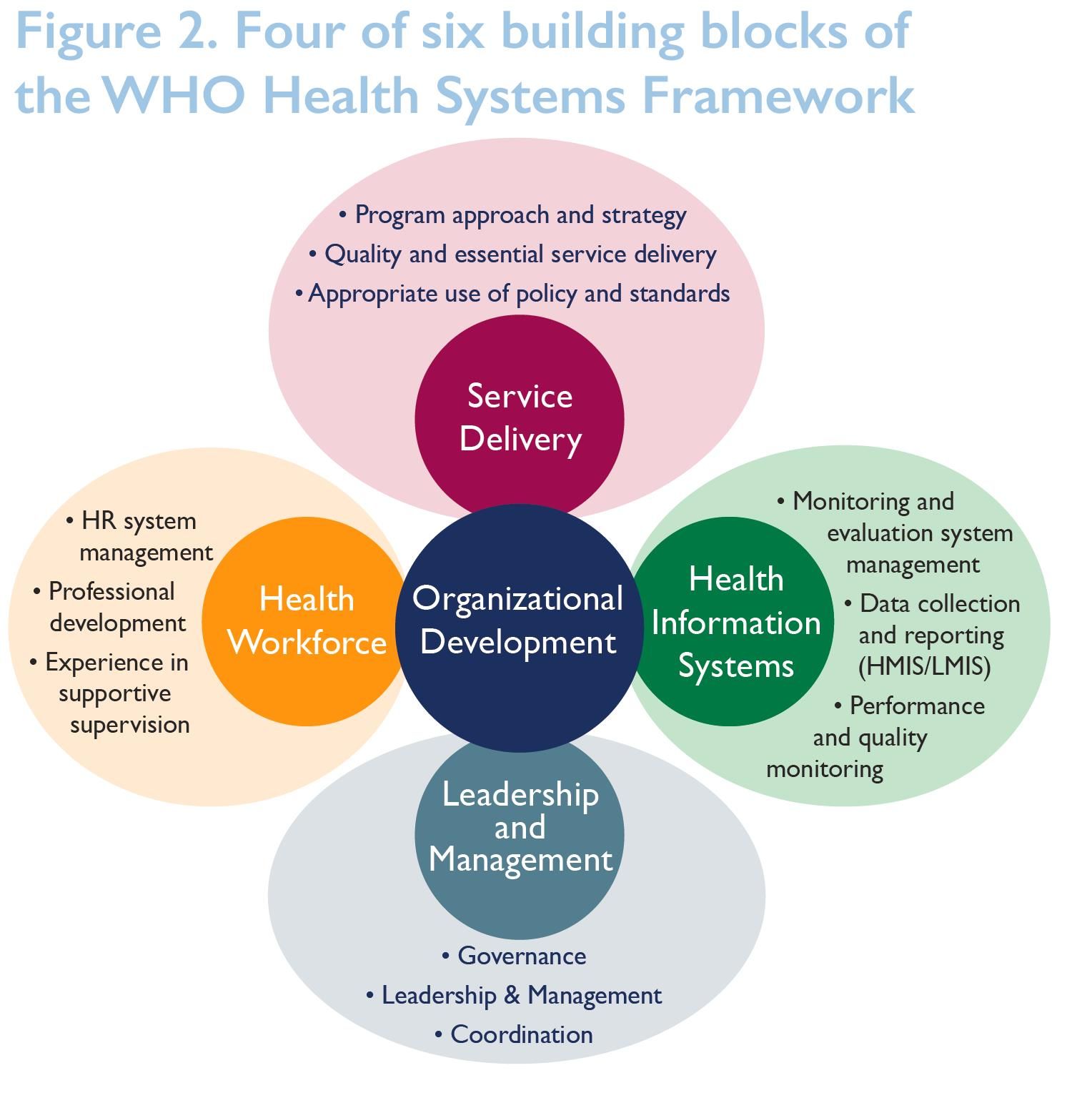 We assessed CHTs’ capacity using a modified organizational capacity assessment (OCA) tool that was used by the USAID’s Rebuilding Basic Health Services (RBHS) project to assess the capacity of the MOHSW, CHTs, and district health teams (DHTs), capturing four of the six World Health Organization (WHO) building blocks of the Health Systems Framework. We also assessed all 30 districts in five counties. Performed desk review, review of self- evaluations, and face- to-face validation interviews. The assessment focused on processes, not physical systems, so the capacity and knowledge of the respondents may have influenced results in some of counties.
We assessed CHTs’ capacity using a modified organizational capacity assessment (OCA) tool that was used by the USAID’s Rebuilding Basic Health Services (RBHS) project to assess the capacity of the MOHSW, CHTs, and district health teams (DHTs), capturing four of the six World Health Organization (WHO) building blocks of the Health Systems Framework. We also assessed all 30 districts in five counties. Performed desk review, review of self- evaluations, and face- to-face validation interviews. The assessment focused on processes, not physical systems, so the capacity and knowledge of the respondents may have influenced results in some of counties.
 Scoring Structure of the OCA Tool: Following each assessment, MCSP used a detailed summary sheet (Figure 3) to display the aggregate scores for each subarea under all key domains, then generated an overall score for each domain. The total score was then expressed as a percentage for each key domain. The majority of the assessment involved asking specific questions about performing malaria interventions per the project scope.
Scoring Structure of the OCA Tool: Following each assessment, MCSP used a detailed summary sheet (Figure 3) to display the aggregate scores for each subarea under all key domains, then generated an overall score for each domain. The total score was then expressed as a percentage for each key domain. The majority of the assessment involved asking specific questions about performing malaria interventions per the project scope.
Effective Interventions were determined:
- Health Workforce Interventions …
- Trained health care workers.
- Trained supervisors on revised supervision tool.
- Performed quarterly supervision and mentoring.
- Leadership and Governance
- Identified a malaria focal point.
- Activated functional health-sector coordination committees.
- Held quarterly review meetings.
- Health Information System
- Provided health management information systems (HMIS) forms to health facilities.
- Facilitated in-service training on onsite data verification.
 Results showed that CHTs’ overall average score was 87% in service delivery, 65% in health information systems, 78% in health workforce, and 70% in leadership/management. Interventions addressing gaps identified in health workforce, leadership and governance, and health information systems resulted in improved service delivery (see Figure 4).
Results showed that CHTs’ overall average score was 87% in service delivery, 65% in health information systems, 78% in health workforce, and 70% in leadership/management. Interventions addressing gaps identified in health workforce, leadership and governance, and health information systems resulted in improved service delivery (see Figure 4).
 In conclusion, The OCA tool helps to identify common challenges, assist with systemwide improvements across CHTs or DHTs, evaluate progress, and meet specific needs. Future efforts are needed to improve the tool’s specificity, the weighting attached to different sections and issues, and its relevance to different types of organizations. Training is an important component to capacity-building, but it is just one part of the picture. Need to improve the way organizations and CHTs/DHTs coordinate with partners to improve all health interventions. Need to focus on application and results of capacity-building, not on capacity as an end in itself.
In conclusion, The OCA tool helps to identify common challenges, assist with systemwide improvements across CHTs or DHTs, evaluate progress, and meet specific needs. Future efforts are needed to improve the tool’s specificity, the weighting attached to different sections and issues, and its relevance to different types of organizations. Training is an important component to capacity-building, but it is just one part of the picture. Need to improve the way organizations and CHTs/DHTs coordinate with partners to improve all health interventions. Need to focus on application and results of capacity-building, not on capacity as an end in itself.
This poster was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Cooperative Agreement AID-OAA-A-14-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government.
Advocacy &Community &Leadership &Surveillance &Women Bill Brieger | 05 Jul 2018
Global Civil Society for Malaria Elimination (CS4ME)
 CS4ME was created during the Global Malaria Civil Society Strategising and Advocacy Pre-Meeting jointly convened by the Global Fund Advocates Network Asia-Pacific (GFAN AP) and APCASO held on 29th and 30th June 2018, prior to the First Malaria Wor1d Congress in Melbourne, Australia, with the support of the Malaria World
CS4ME was created during the Global Malaria Civil Society Strategising and Advocacy Pre-Meeting jointly convened by the Global Fund Advocates Network Asia-Pacific (GFAN AP) and APCASO held on 29th and 30th June 2018, prior to the First Malaria Wor1d Congress in Melbourne, Australia, with the support of the Malaria World  Congress, Global Fund to Fight AIDS, Tuberculosis and Malaria, and the Burnet Institute. An interim working group mode up of individuals that attended the Pre-Meeting was established to coordinate, recommend processes and mechanisms, identify resources and support necessary for CS4ME going forward. For more Information please contact Ms Olivia Ngou Zongue <ngouolivia@gmail.com> of the Interim Working Group of CS4ME for further information. The Declaration arising from their meeting if provided below.
Congress, Global Fund to Fight AIDS, Tuberculosis and Malaria, and the Burnet Institute. An interim working group mode up of individuals that attended the Pre-Meeting was established to coordinate, recommend processes and mechanisms, identify resources and support necessary for CS4ME going forward. For more Information please contact Ms Olivia Ngou Zongue <ngouolivia@gmail.com> of the Interim Working Group of CS4ME for further information. The Declaration arising from their meeting if provided below.
GLOBAL CIVIL SOCIETY FOR MALARIA ELIMINATION (CS4ME) DECLARATION
MALARIA WORLD CONGRESS 1ST-5TH JULY 2018
MELBOURNE, AUSTRALIA
Firm in the belief that empowered community and civil society are game-changers in health responses, we, representatives of national, regional and global malaria communities and civil society attending the First Malaria World Congress, have come together and formed the Global Civil Society for Malaria Elimination (CS4ME) as part of our commitment to joint advocacy for more effective, sustainable, people-centred, rights-based, equitable, and inclusive malaria programmes and Interventions.
At a time when the world has the resources and tools to prevent and treat malaria, it is unconscionable how people – mainly from impoverished, vulnerable and underserved communities – continue to die from the disease. While we commend the efforts of governments and the international community that brought the world closer to malaria elimination, we call for greater accountability, political will and action, resource investments, and sense of urgency to eliminate the disease.
CS4ME makes the following call to the governments of implementing countries, donor countries and other duty bearers:
FRAME MALARIA RESPONSES IN THE CONTEXT Of SOCIAL JUSTICE AND HUMAN RIGHTS, AND WITHIN UNIVERSAL HEALTH COVERAGE
Significant progress has been attained during the past 10 years to reduce the burden of malaria throughout the world and in working towards achieving malaria elimination. As countries enter into the elimination phase, we see again and again the epidemic concentrating among the most marginalised, remote, and disenfranchised communities. In South East Asia, the concentration of malaria among communities barred from accessing quality and affordable health services has accelerated the emergence of drug resistance that now threatens the wor1d at large. Everywhere, the last mile of elimination becomes a matter of access to health for impoverished and marginalised communities, in particular, refugees, ethnic minorities, indigenous communities, migrant and mobile populations – with many of the risks faced by these groups compounded further amongst women and girls.
Including the most local, represents a strategic investment contributing to appropriate, effective service delivery and people-driven surveillance and response.
We call on national governments, international institutions, bilateral and multilateral donors to prioritise and increase funding allocations for community-driven community and civil society initiatives. We request that specific funding streams be made available to community groups, and their access supported through peer-to-peer technical assistance.
Furthermore, we request that key performance indicators that enable accountability for bringing malaria services to the underserved be developed and implemented.
PARTNER WITH CIVIL SOCIETY AND COMMUNITY ACTORS FOR AN EFFECTIVE MALARIA SURVEILLANCE AND RESPONSE
As surveillance becomes an essential pillar for malaria elimination, the need for timely and robust data is increasingly critical. Essential evidence includes routine data, qualitative and quantitative research, as well as experience, lessons learned and the voices from affected communities. Support is required to build the ability of civil society to generate evidence, as well as to communicate it effectively to ensure that community-generated evidence will be able to influence decisions and result in sustained change.
To eliminate malaria, surveillance requires a response. Communities and civil society are the first responders, and will have the clearest insight Into what responses are effective in their context or on behalf of their constituents.
We demand that communities and civil society organisations be given equitable access to data and other information that can inform field-level response. We call for transparent information systems and multi-directional information flows in order to enable dialogue, and inform decisions at all levels. We urge the building up of surveillance systems that involve communities as analysts, advisors, decision-makers and responders.
We, malaria communities and civil society, offer our support, expertise, and lived experiences In contributing towards our shared vision of malaria elimination. We are fully committed to working alongside other stakeholders to build stronger, more inclusive and effective partnerships and sustainable responses towards elimination of malaria in this lifetime.
Gender &Leadership &Women Bill Brieger | 23 Mar 2018
Women Making Malaria History
March is Women’s History Month and thus a time to examine the role of women in bringing an end to malaria. For many years studies at the household level have told us that women often lack the financial independence or social support to make important decisions about malaria treatment and prevention for themselves and their children. Furthermore, as WHO notes, “Gender norms and values … influence the division of labour, leisure patterns, and sleeping arrangements may lead to different patterns of exposure to mosquitoes for men and women.” As part of the solution to these problems, it is important to look at women role models in the fight against the disease – at women making malaria history.
 One of these role models is Tu Youyou who became one of three scientists to win the 2015 Nobel Prize for medicine. Her work of over 40 years was virtually unknown to the outside world until then, but her study of artemisinin medicinal compounds has saved the lives of millions.
One of these role models is Tu Youyou who became one of three scientists to win the 2015 Nobel Prize for medicine. Her work of over 40 years was virtually unknown to the outside world until then, but her study of artemisinin medicinal compounds has saved the lives of millions.
 Moving from the lab to the community one can find role models who have broken role stereotypes. A few years ago President’s Malaria Initiative-funded Africa Indoor Residual Spraying (AIRS) project drew out attention to Maimouna Sanogo as a woman making a difference. She helped protect people in her country from malaria through her work as a supervisor on AIRS indoor residual spraying project in Mali. The AIRS project reported that, “As a woman in a leadership role, Maimouna is a trailblazer. In Mali, only 37% of women participate in the labor force, while participation is nearly double among Malian men (70%).”
Moving from the lab to the community one can find role models who have broken role stereotypes. A few years ago President’s Malaria Initiative-funded Africa Indoor Residual Spraying (AIRS) project drew out attention to Maimouna Sanogo as a woman making a difference. She helped protect people in her country from malaria through her work as a supervisor on AIRS indoor residual spraying project in Mali. The AIRS project reported that, “As a woman in a leadership role, Maimouna is a trailblazer. In Mali, only 37% of women participate in the labor force, while participation is nearly double among Malian men (70%).”
Women have played crucial leadership roles in national malaria programs. Dr TO Sofola as Director of Nigeria’s National Malaria Control Program (NMCP, now National Malaria Elimination Program) guided the transition of case management policy to the use of artemisinin-based combination therapy, oversaw planning for the first massive national LLIN campaign, guided development of the World Bank Booster Program support, helped strengthen Nigeria’s first Global Fund Malaria Grants, and brought state level malaria control programs into the national strategy process. Women have also led NMCPs in Malawi, Kenya and other countries.
 Dr Rose Leke, Emeritus Professor of Immunology and Parasitology, Faculty of Medicine and Biomedical Sciences, University of Yaounde, Cameroon, was one of six people to be given the Kwame Nkrumah Scientific Award for Women in 2011. Dr Leke explained the challenges facing women, “Science is still a challenging field for women to enter, and even more so in which to progress. At the university, I have seen many promising young women finish their studies and start jobs as assistants only to either get stuck in that position indefinitely or eventually leave to take care of their families. There just wasn’t the mentorship or financial support for research needed for them to be able to progress. It was an issue I really took to heart.” Therefore, Dr Leke and colleagues started the HIGHER Women Consortium in Cameroon. We provided training and mentorship to young women researchers.
Dr Rose Leke, Emeritus Professor of Immunology and Parasitology, Faculty of Medicine and Biomedical Sciences, University of Yaounde, Cameroon, was one of six people to be given the Kwame Nkrumah Scientific Award for Women in 2011. Dr Leke explained the challenges facing women, “Science is still a challenging field for women to enter, and even more so in which to progress. At the university, I have seen many promising young women finish their studies and start jobs as assistants only to either get stuck in that position indefinitely or eventually leave to take care of their families. There just wasn’t the mentorship or financial support for research needed for them to be able to progress. It was an issue I really took to heart.” Therefore, Dr Leke and colleagues started the HIGHER Women Consortium in Cameroon. We provided training and mentorship to young women researchers.
Women in academics, research, government and front line programs have and continue to make history in the efforts to eliminate malaria. As Dr Leke’s example shows, these women leaders can make sure no one stands in the way of ensuring that the next generation of women scientists, managers and field workers make malaria history.
Advocacy &Borders &Children &Conflict &Costs &Epidemiology &Funding &Human Resources &Leadership &Monitoring &Mortality &NTDs &Partnership &Surveillance Bill Brieger | 03 Feb 2018
African Leaders Malaria Alliance Recognizes Country Achievements, Adds NTDs to its Scorecard
 The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
 For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
The scorecard will now “report progress for the 47 NTD-affected countries in sub-Saharan Africa in their strategies to treat and prevent the five most common NTDs: lymphatic filariasis, onchocerciasis, schistosomiasis, soil-transmitted helminths and trachoma. By adding NTDs to the scorecard, African leaders are making a public commitment to hold themselves accountable for progress on these diseases.”
 In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
The combination is based on the logic that NTDs and malaria are both diseases of poverty. Malaria and several NTDs are also vector-borne. Also community platforms are a foundation for delivering needed drugs and supplies to tackle these diseases. Ultimately the decision shows that Heads of State are holding themselves accountable for progress in eliminating these diseases.
 At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
 The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
H.E . Dr. Barnabas Sibusiso Dlamini, the Prime Minister of the Kingdom of Swaziland, whose King and Head of State is the current chair of ALMA, warned all endemic countries that, “When we take our eyes off malaria, the cost for our countries is huge. Yet if we increase our efforts to control and eventually eliminate malaria, the yield we get from it is tremendous. It is time that we dig deep into our pockets and provide malaria programmes with the needed resources.”
 Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
IRIN concludes that, “For now, the biggest challenge for Zambia will be closing the gap in its malaria elimination strategy, which will cost around $160 million a year and is currently only about 50 percent funded – two thirds from international donors and one third from the Zambian government. Privately, international donors say the government must spend more money on its malaria programme if it is to succeed.” Cross-border transmission adds to the problem.
Internal strife is another challenge to malaria success. “The recent nurses’ strike which lasted for five months may have cost Kenya a continental award in reducing the prevalence of malaria during the 30th African Union Summit in Ethiopia on Sunday.” John Muchangi in the Star also noted that, “However, Kenya lost momentum last year and a major malaria outbreak during the prolonged nurses’ strike killed more than 30 people within two weeks in October.”
 Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Fortunately ALMA is equipped with the monitoring and advocacy tools to ensure that its members recognize and respond to such challenges. The Scorecards will keep the fight against the infectious diseases of poverty on track.
Elimination &Eradication &Leadership &Mortality &Resistance Bill Brieger | 29 Dec 2015
Does Malaria Meet the Criteria for Eradication?
 What it is that makes a disease “eradicable,” or more correctly what makes it possible to eliminate malaria in each country leading to the total eradication world-wide. Bruce Aylward and colleagues identified three main sets of factors by drawing on lessons of four previous attempts to eradicate diseases (including the first effort at malaria eradication in the 1950s and ‘60s).[1]
What it is that makes a disease “eradicable,” or more correctly what makes it possible to eliminate malaria in each country leading to the total eradication world-wide. Bruce Aylward and colleagues identified three main sets of factors by drawing on lessons of four previous attempts to eradicate diseases (including the first effort at malaria eradication in the 1950s and ‘60s).[1]
- biological and technical feasibility
- costs and benefits, and
- societal and political considerations
So far smallpox is the only success because as Aylward et al. pointed out biologically, humans were the only reservoir and on the technical side a very effective vaccine was developed. The eradication campaign was promoted in clear terms of economic and related benefits. While the early malaria eradication efforts started with political will and recognition of the potential economic benefits of malaria eradication, the will was not sustained over two decades. On the technical side at that time there was only one main tool again malaria, indoor residual insecticide spraying, and mosquitoes quickly developed resistance to the chemicals. Are we better able to meet the three eradication criteria today?
Today’s technical challenges are embodied in intervention coverage problems. The World Malaria Report of 2015[2] (WMR2015) explains that the problem is most pronounced in the 15 highest burden countries, and consequently these showed the slowest declines in morbidity and mortality over the past 15 years. Use of insecticide treated nets and intermittent preventive treatment for pregnant women hovers around 50%, while appropriate case management of malaria lags well below 20%, a far cry from the goals of universal coverage. A further explanation of the technical challenges as outlined in the WMR2015 lies in “weaknesses in health systems in countries with the greatest malaria burden.”
The economic benefits criteria should be most pronounced in the high burden countries, but these are also generally ones with low personal income. Ironically, the WMR2015 points out that it is the high costs of malaria care and the malaria burden that further weaken health systems. More investment is needed in order to see more economic benefits.
Biological challenges to elimination are also identified in the WMR2015. Examples of existing and arising biological difficulties include –
- Plasmodium vivax malaria which requires a more complicated regimen to affect a cure.
- “Since 2010, of 78 countries reporting (insecticide resistance) monitoring data, 60 reported resistance to at least one insecticide in one vector population.
- “P. falciparum resistance to artemisinins has now been detected in five countries in the Greater Mekong subregion.” Historically chloroquine and sulfadoxine-pyrimethamine resistance spread from this area and now artemisinin resistance marks a ‘Third Wave” of resistance emanating from the region.[3]
- “Human cases of malaria due to P. knowlesi have been recorded – this species causes malaria among monkeys in certain forested areas of South-East Asia,” and so far human-to- human transmission has not been documented.
On the positive side greater political support to elimination efforts has been expressed by the African Leaders Malaria Alliance (ALMA) who met at the African Union Leaders Summit in Addis Abba early in 2015 and resolved to eliminate malaria by 2030.[4] This call to action was backed up with an expansion of ALMA’s quarterly scorecard rating system of African countries’ performance to include elimination indicators.[5]
In conclusion, political will exists, but needs to be backed with greater financial investment in order to produce economic benefits. Time is of the essence in taking action because biological and technical forces are pressing against elimination. 2030 seems far, but we cannot wait another 15 years to take action against these challenges to malaria elimination.
[1] Aylward B, Hennessey KA, Zagaria N, Olivé J, Cochi S. When Is a Disease Eradicable? 100 Years of Lessons Learned. American Journal of Public Health, 2000; 90(10): 1515-20.
[2] World Health Organization. World Malaria Report 2015. WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland, 2015.
[3] IRIN (news service of the UN Office for the Coordination of Humanitarian Affairs). “Third wave” of malaria resistance lurks on Thai-Cambodia border. August 29, 2014. http://www.irinnews.org/report/100549/third-wave-of-malaria-resistance-lurks-on-thai-cambodia-border
[4] United Nations Secretary-General’s Special Envoy on MDGs. African Leaders Call for Elimination of Malaria by 2030. Feb. 3, 2015. http://www.mdghealthenvoy.org/african-leaders-call-for-elimination-of-malaria-by-2030/
[5] African Malaria Leaders Alliance. ALMA 2030 Scorecard Towards Malaria Elimination, December 2014. http://alma2030.org/sites/default/files/sadc-elimination-scorecard/alma_scorecards_poster_english.pdf
Advocacy &Leadership &Women Bill Brieger | 08 Mar 2015
Leading by Example: Senegal’s Minister of Health supports the “Zero Malaria! Count Me In!” campaign
Yacine Djibo, Founder & President of Speak Up Africa is helping focus International Women’s Day (March 8th) on efforts to protect women from malaria in Senegal. She is highlighting the commitments of 8 strong and beautiful women, in Senegal, that are dedicated to eliminating malaria in their country. These commitments are part of an inclusive mass communication campaign that aims to launch a national movement in favor of malaria elimination in Senegal: the “Zero Malaria! Count Me In” campaign
 International Women’s Day, represents an opportunity to celebrate the achievements of women all around the world. This year’s theme is “Empowering Women – Empowering Humanity: Picture it” envisions a world where each woman and girl can exercise her choices, such as participating in politics, getting an education or fighting malaria. Below is the second feature on women fighting malaria.
International Women’s Day, represents an opportunity to celebrate the achievements of women all around the world. This year’s theme is “Empowering Women – Empowering Humanity: Picture it” envisions a world where each woman and girl can exercise her choices, such as participating in politics, getting an education or fighting malaria. Below is the second feature on women fighting malaria.
Pr. Awa Marie Coll Seck, the former Executive Secretary of the Roll Back Malaria Partnership pursues her fight against malaria in her own country, Senegal, as Minister of Health. Known for her smooth diplomatic skills and experience in policy formulation, she leads an aggressive reform striving to eliminate all deaths due to malaria in Senegal.

Pr. Awa Marie Coll Seck, Minister of Health and Social Action, Senegal
As global leadership increasingly realizes that the international strategy demands a strong local response and the most active engagement of beneficiaries, Senegal’s Minister of Health walks the talk. The Zero Malaria! Count Me In! campaign aims at creating a movement around the importance of accountability and individual responsibility when it comes to putting an end to this preventable disease. Malaria elimination demands the coordinated efforts of all sectors of society.
As the Minister of Health pledges to build capacity within health facilities so that they are able to properly manage simple and severe cases of malaria, the Zero Malaria! Count Me In! campaign insists on the necessary parallel commitment that Senegalese people need to make in order for the country to reach its malaria elimination objective.
Since the past decade, the country has made tremendous progress and reduced malaria mortality by 62%. Over 6.5 million of insecticide treated mosquito nets were distributed throughout the country and lifesaving medicines are now available in public health facilities free of charge.
Women being the primary caretakers of their families, International Women Day is the perfect occasion to celebrate the leadership of Senegalese women throughout the country, without whom, malaria elimination could never become a reality.
Thank you Minister for leading by example and proving that actions speak louder than words.
Happy International Women Day to all!
*****
Headquartered in Dakar, Senegal, Speak Up Africa is a creative health communications and advocacy organization dedicated to catalyzing African leadership, enabling policy change, securing resources and inspiring individual action for the most pressing issue affecting Africa’s future: child health.
Leadership Bill Brieger | 01 Feb 2011
ALMA – long time no see
Since African Leaders Malaria Alliance (ALMA) was formed nearly two years ago, we hear only occasionally about its efforts to rally political will. The last major news came in August 2010 at the 15th African Union Summit when leaders pledged a commitment to malaria in the context of maternal and child health. ALMA still maintains a website and a blog with recent and occastional postings, but generally its activities have been somewhat off the radar of the major media outlets.
Now during the during the 16th African Union Summit in Addis Ababa ALMA has resurfaced in public view. The occasion was award of recognition to four heads of state for their support of malaria programs. Recipients of the 2011 ALMA Award for Excellence are the heads of state of Guinea, Kenya, Uganda and Tanzania.
Although currently comprised of only 35 heads of states, ALMA notes as progress that, “Of the 45 malaria-endemic countries in Africa, 62% have removed tariffs on anti-malarial medicines, 42% have removed tariffs on LLINs, and 31 countries have taken measures to curtail the use of oral artemisinin-based monotherapies,” as reported by the Malaria Policy Center.
In addressing the Group, the UN Secretary General praised them for working toward the goal of Universal Coverage, He explained that, “The African Leaders Malaria Alliance is breaking down barriers, forging partnerships and getting supplies to families in record time. This is remarkable progress. We need to encourage it and use the response to malaria as a model for battling other illnesses and social ills.”
This is a challenging time for leadership in the fight against malaria. Not all heads of state have been watching the store as it were, since several Global Fund grants have been suspended on their watch due to corruption, often by government agencies serving as grant recipients. Uganda, one of the four awardees of this year’s ALMA Excellence Awards, has had its own brush with the Global Fund.
Kenya was one of the countries covered in a 2008 study by the Global Fund of conflict of interest within its Country Coordinating Mechanism. Kenya was also singled out in an Office of the Inspector General Report to the 21st GFATM Board Meeting as one of the countries that had implemented less than half of the recommendations arising from its audit.
The East African Magazine recently published an African Presidents’ Index that ranken leaders on such factors as press freedom, corruption, democracy and human development. The ALMA award recipients ranked as follows out of 52:
- Guinea – 29th at 42% score and a grade of FÂ
- Kenya – 16th at 53% and a grade of C
- Uganda – 20th at 50% and a grade of D+
- Tanzania – 10th at 60% and a grade of B-
Hopefully the recognition by ALMA for malaria achievements will have an overall positive effect on leadership and political will in all areas of governance and human development. Progress on one issue (health) and one disease (malaria) alone can not have a long lasting effect on defeating poverty and enhancing dignity of life in Africa.
Eradication &Funding &Leadership Bill Brieger | 05 Jun 2010
Fifty Years – independence and malaria in Africa
 The New York Times points out that “17 African countries, including Nigeria, gained independence in 1960.” Apparently there are few major commemorations. The Times quotes Ibrahima Thioub, a Senegalese historian, who said, “It’s tough to mobilize people for celebrations, because the flowers of independence have faded. The last 50 years have not at all met the people’s hopes and expectations.”
The New York Times points out that “17 African countries, including Nigeria, gained independence in 1960.” Apparently there are few major commemorations. The Times quotes Ibrahima Thioub, a Senegalese historian, who said, “It’s tough to mobilize people for celebrations, because the flowers of independence have faded. The last 50 years have not at all met the people’s hopes and expectations.”
Have these 50 years brought Africa any closer to independence from malaria? It was during those years in the late 1950s and early 1960s when most countries were gaining independence that the first effort to eradicate malaria failed. We have had twelve years of rolling back malaria now – are the critical factors in place to ensure that eliminating the disease is feasible now?
The New York Times article addresses critical factors – ranging from weakness of institutions like parliaments to gaps in civil society engagement – that would impede public health and social welfare programs including malaria control. African intellectuals quoted in the article bemoan that “democracy is held hostage by elites,” and the public accepts that “power is a matter of essences, a heritage, something in the blood, that what is normal for a state is unlimited monarchy.” While both power and malaria may be ‘in the blood’, the former does not appear to be as easily transmissible or shareable, making the latter all the less easy to control.
The Times notes that, “… there is the reliance on heavy inflows of foreign aid, which equaled a quarter to nearly a third of government spending in countries like Burkina Faso, Cameroon and Mali in 2008.” Clearly this includes inputs from the Global Fund, The World Bank Booster Program and the US President’s Malaria Initiative (PMI). What aspects of health programming are not covered by aid is often paid out of pocket by the public, which is already impoverished by diseases like malaria.
Although there have been recent worries about both the level of donor funding moving forward and the willingness of countries to sustain programs should donor funding collapse, there are some positive signs from the donor side. The US Government is increasing its malaria focus beyond the 15 PMI countries to include at least Burkina Faso, Burundi, Nigeria, Democratic Republic of the Congo and Sudan, and the Global Fund is embarking on a new ‘grant architecture.’
Known as ‘single stream funding’ the new Global Fund grant architecture “will shift the Global Fund towards a more program-based approach, with significantly improved harmonization and alignment, improving its support of holistic health planning and implementation,” to each principle recipients. This should simplify management, provide continuity, and reduce transaction costs – so even if funding does not increase as desired, there still may be savings and efficiencies for the allocated resources.
There are signs that we may get closer to independence from malaria this year as strides are being made to achieve universal coverage of malaria interventions. It may take another 50 years to see whether malaria can truly be eradicated. Hopefully when many endemic African countries will be observing their 100th year of independence, malaria will have become a thing of the past.
Leadership &Malaria in Pregnancy Bill Brieger | 26 Dec 2009
USAID – new director confirmed
The US Senate has given the development community a holiday gift. The indo-Asian News Service reports, “The Senate unanimously on Thursday confirmed the nomination of Shah, 36, and some three dozen other officials nominated by President Barack Obama before taking its Christmas break.”
Rajiv Shah has training in medicine and economics and has worked with the US Department of Agriculture. This gives him a broad development perspective and hopefully will ensure nutrition issues are not forgotten, “having championed Obama’s global food security initiative.”
Shah has also worked with the private and the NGO sectors, important partners in USAID’s work.
When Shah was nominated, President Obama said, “Rajiv brings fresh ideas and the dedication and impressive background necessary to help guide USAID as it works to achieve this important goal.”
There are those who are worried that fresh ideas alone may not be enough to guide an agency with such wide scope. NationalJournal.com remarked that, “Then there is the question of seasoning. While development junkies trade war stories of remote missions and malaria like currency, Shah has almost zero field experience. He may be the smartest guy in the room, but he doesn’t have that wellspring to draw on.”
During confirmation hearings Senator Richard G. Lugar posed a question about the future of the successful disease control programs initiated by the US Government in recent years. Shah explained that …
The welcome increase in funding for health assistance since 2000, particularly for combating HIV and malaria, has largely been targeted to African countries where disease and overall poor health conditions have had substantial socio-economic impact. That said, there are still tremendous unmet health and development needs in these countries. The Administration is committed to a broad Global Health Initiative that takes account of the range of health and development needs and, if confirmed, I look forward to working with Congress on this important issue.
The United Nations Foundations congratulated the President on Shah’s nomination and reiterated its own priorities which address both disease control and strengthening maternal and child health (MCH) services:
The United Nations Foundation is particularly focused on development goals related to global health, including our efforts to eradicate polio, reduce measles mortality, and eliminate malaria worldwide. In light of the unmet need in the world for maternal health and family planning, I hope that USAID’s new leadership will keep women’s health and international family planning a priority.
A good example of the nexus between malaria control and MCH is the challenge of preventing and treating malaria in pregnancy (MIP). Pregnant women bear a disproportionate burden of malaria that threatens their survival and that of the fetus and the newborn child. Without strong a antenatal and reproductive health foundation, MIP control cannot reach those in need.
If Shah does have this bigger picture of malaria control in mind, we can hope for a broadening of malaria intervention into MCH programs that go beyond the limits of the 15 countries that constrained the potential impact of the President’s Malaria Initiative.