Advocacy &coronavirus &Fever &HIV &IPTp &Journalists/Media &Malaria in Pregnancy &Plasmodium/Parasite &Private Sector &Tuberculosis Bill Brieger | 06 Oct 2020
Malaria News Today 2020-10-06: malaria in pregnancy, parasites surviving fever and private sector support
Today’s news featured a media briefing by the RBM Partnership and AMMREN on the challenges of protecting pregnant women from malaria. Additional news expands on these challenges. Research looks at how malaria parasites withstand the heat of a patient’s fever. Finally examples are presented of collaboration between international organizations and the private sector for malaria and disease control. Follow the links to gain more information.
Speed Up IPTp Scale-Up: a media briefing on maternal health
 A panel discussion and media briefing on new approaches and lessons learned formed part of an online global call to end malaria in pregnancy with intermittent preventive treatment. The briefing on Tuesday, 6 October 2020, was sponsored by the Roll Back Malaria Partnership and AMMREN. The RBM website features background on the call to action.
A panel discussion and media briefing on new approaches and lessons learned formed part of an online global call to end malaria in pregnancy with intermittent preventive treatment. The briefing on Tuesday, 6 October 2020, was sponsored by the Roll Back Malaria Partnership and AMMREN. The RBM website features background on the call to action.
The panel discussion included Dr. Aminata Cisse ep. Traore, Sous Directrice de la Santé de la Reproduction/Direction Générale de la Santé et de l’Hygiène Publique, Ministére de la Santé et de l’Hygiène Publique, Mali; Dr. Anshu Banerjee, Director Department of Maternal, Newborn, Child, Adolescent Health & Ageing, World Health Organization (WHO), and Dr. Pedro Alonso, Director Global Malaria Programme, WHO. The discussion was moderated by Mildred Komey, Malaria in Pregnancy Focal Person, National Malaria Control Program, Ghans Health Service.
 The discussion covered the importance of launching this call now, what we’ve learned over the last few years, and examples of innovative strategies from Mali. There was a Q&A session with journalists after the presentations.
The discussion covered the importance of launching this call now, what we’ve learned over the last few years, and examples of innovative strategies from Mali. There was a Q&A session with journalists after the presentations.
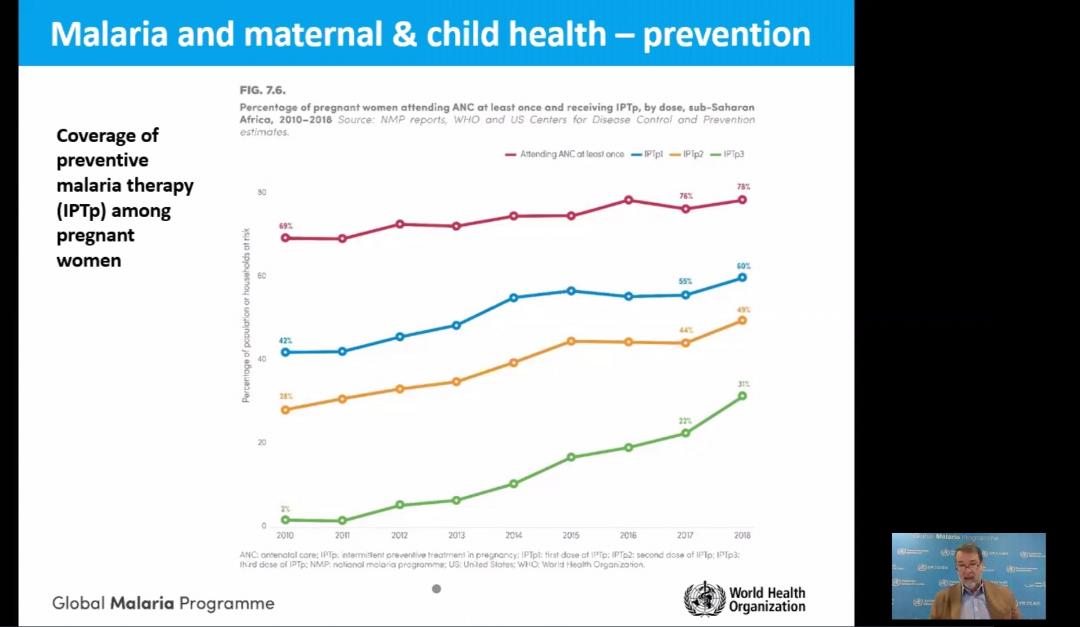
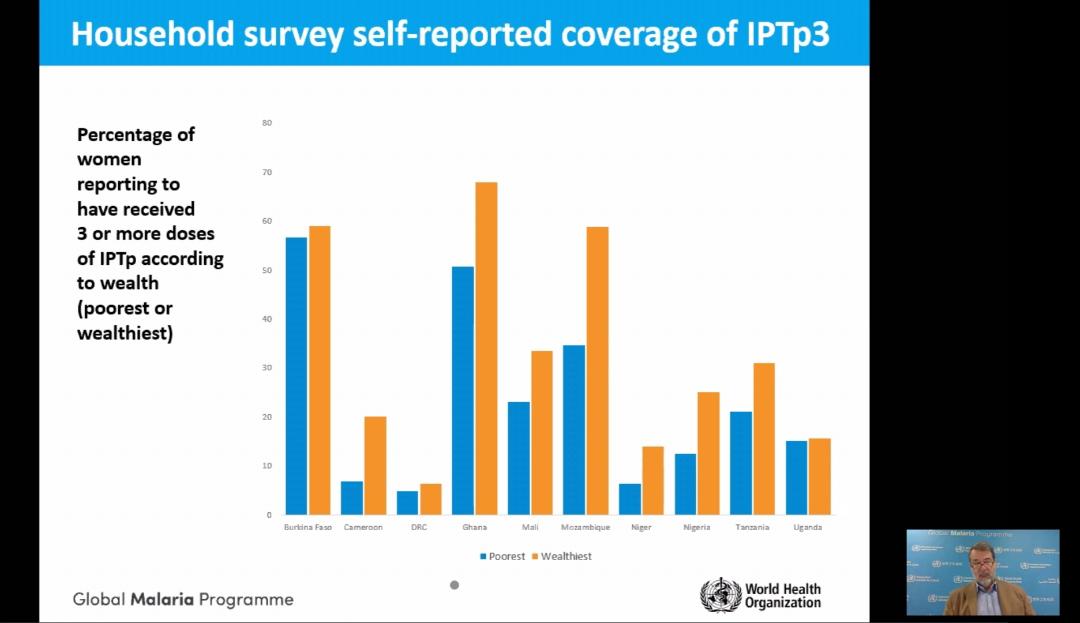
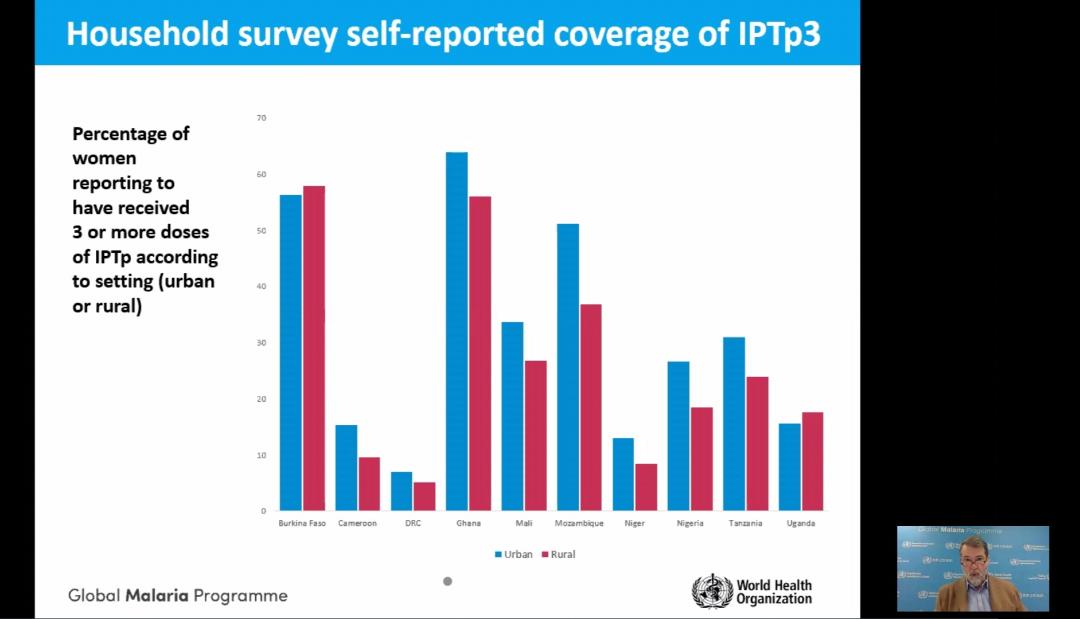
The presentation by Dr Alonso showed the progress in achieving IPTp coverage goals. He also pointed out the social and economic factors that affect access and equity to intermittent preventive treatment of malaria in pregnancy and protection of maternal health (see slides).
Experts say Africa must scale-up malaria protection for pregnant women
 In support of the RBM/AMMREN briefing described above, Sola Ogundipe reports that amidst the COVID-19 pandemic in sub-Saharan Africa, malaria – one of the world’s oldest diseases – is impacting disproportionately on pregnant women and children aged under five.
In support of the RBM/AMMREN briefing described above, Sola Ogundipe reports that amidst the COVID-19 pandemic in sub-Saharan Africa, malaria – one of the world’s oldest diseases – is impacting disproportionately on pregnant women and children aged under five.
For a pregnant woman, her fetus, and the newborn child malaria infection carries substantial risks. Calling for a speedy scale-up to boost protection against malaria for pregnant women in Africa, the Roll Back Malaria, RBM Partnership to End Malaria Working Group is issuing an urgent appeal to leaders and health policymakers to increase access to Intermittent Preventive Treatment during pregnancy, IPTp, among eligible pregnant women in sub-Saharan Africa.
 Along with stakeholders, the RBM Partnership is pushing for scale-up coverage of three doses of IPTp to reach all eligible women in sub-Saharan Africa by 2025. In 2019, according to the RBM Partnership, an estimated 11 million pregnant women in sub-Saharan Africa, or 29 percent of all pregnancies were infected with malaria.
Along with stakeholders, the RBM Partnership is pushing for scale-up coverage of three doses of IPTp to reach all eligible women in sub-Saharan Africa by 2025. In 2019, according to the RBM Partnership, an estimated 11 million pregnant women in sub-Saharan Africa, or 29 percent of all pregnancies were infected with malaria.
How malaria parasites withstand a fever’s heat
The parasites that cause 200 million cases of malaria each year can withstand feverish temperatures that make their human hosts miserable. Now, a team is beginning to understand how they do it. The researchers have identified a lipid-protein combo that springs into action to gird the parasite’s innards against heat shock.
Understanding how malaria protects its cells against heat and other onslaughts could lead to new ways to fight tough-to-kill strains, researchers say. Findings could lead to ways to maximize our existing antimalarial arsenal.
Global Fund and Chevron – United Against HIV, TB and Malaria
The Global Fund and Chevron Corporation have celebrated a 12-year partnership that served as an example of the private sector’s contribution to the fight against infectious diseases and to building resilient health systems. Chevron, a Global Fund partner since January 2008, has supported Global Fund programs against HIX4 tuberculosis and malaria for a total investment of US$60 million in Angola, Indonesia, Nigeria, the Philippines, South Africa, Thailand and Vietnam.
Chevron’s partnership has contributed to helping more than a million people living with HIV access lifesaving antiretroviral therapy; supported efforts to distribute over one million long-lasting insecticide-treated mosquito nets to families to prevent malaria; helped detect thousands of TB cases; promoted education programs for the young, and helped build stronger health systems.
In Nigeria, Chevron’s $5 million investment from October 2017 to December 201 9 supported the national HIV and TB programs, reaching key and vulnerable populations, as well as interventions aimed at strengthening the health system. Sustainable and resilient systems for health are indispensable in the fight against the epidemics of HIV TB and malaria, as well as the first line of defense against new diseases like COVID-19. “With rising cases of COVID-1 9, the stakes are very high. Deaths from HIV, TB and malaria are likely to increase. Investments by partners like Chevron are fundamental.
Cholera &commodities &Community &coronavirus &Costs &COVID-19 &Culture &Epidemiology &Guidelines &Health Systems &HIV &Microscopy &Mosquitoes &Plasmodium/Parasite &Refugee &Sahel &Seasonal Malaria Chemoprevention &Surveillance &Tuberculosis Bill Brieger | 22 Sep 2020
Malaria News Today 2020-09-22: covering three continents
Today’s stories cover three continents including Surveillance for imported malaria in Sri Lanka, community perceptions in Colombia and Annual Fluctuations in Malaria Transmission Intensity in 5 sub-Saharan countries. In addition there is an overview of microscopy standards and an Integrated Macroeconomic Epidemiological Demographic Model to aid in planning malaria elimination. We also see how COVID-19 is disturbing Seasonal Malaria Chemoprevention activities in Burkina Faso. Read more by following the links in the sections below.
Will More of the Same Achieve Malaria Elimination?
… Results from an Integrated Macroeconomic Epidemiological Demographic Model. Historic levels of funding have reduced the global burden of malaria in recent years. Questions remain, however, as to whether scaling up interventions, in parallel with economic growth, has made malaria elimination more likely today than previously. The consequences of “trying but failing” to eliminate malaria are also uncertain. Reduced malaria exposure decreases the acquisition of semi-immunity during childhood, a necessary phase of the immunological transition that occurs on the pathway to malaria elimination. During this transitional period, the risk of malaria resurgence increases as proportionately more individuals across all age-groups are less able to manage infections by immune response alone. We developed a robust model that integrates the effects of malaria transmission, demography, and macroeconomics in the context of Plasmodium falciparum malaria within a hyperendemic environment.
The authors analyzed the potential for existing interventions, alongside economic development, to achieve malaria elimination. Simulation results indicate that a 2% increase in future economic growth will increase the US$5.1 billion cumulative economic burden of malaria in Ghana to US$7.2 billion, although increasing regional insecticide-treated net coverage rates by 25% will lower malaria reproduction numbers by just 9%, reduce population-wide morbidity by ?0.1%, and reduce prevalence from 54% to 46% by 2034. As scaling up current malaria control tools, combined with economic growth, will be insufficient to interrupt malaria transmission in Ghana, high levels of malaria control should be maintained and investment in research and development should be increased to maintain the gains of the past decade and to minimize the risk of resurgence, as transmission drops. © The American Society of Tropical Medicine and Hygiene [open-access]
Microscopy standards to harmonise methods for malaria clinical research studies
 Research Malaria Microscopy Standards (ReMMS) applicable to malaria clinical research studies have been published in Malaria Journal. The paper describes the rationale for proposed standards to prepare, stain and examine blood films for malaria parasites. The standards complement the methods manual(link is external) previously published by the World Health Organization and UNICEF/UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases (TDR). The standards aim to promote consistency and comparability of data from microscopy performed for malaria research and hence to strengthen evidence for improvements in malaria prevention, diagnostics and treatment.
Research Malaria Microscopy Standards (ReMMS) applicable to malaria clinical research studies have been published in Malaria Journal. The paper describes the rationale for proposed standards to prepare, stain and examine blood films for malaria parasites. The standards complement the methods manual(link is external) previously published by the World Health Organization and UNICEF/UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases (TDR). The standards aim to promote consistency and comparability of data from microscopy performed for malaria research and hence to strengthen evidence for improvements in malaria prevention, diagnostics and treatment.
Microscopy is important in both malaria diagnosis and research. It is used to differentiate between Plasmodium species and stages and to estimate parasite density in the blood – an important determinant of the severity of disease. It is also used to monitor the effectiveness of drugs based on the rate at which parasites recrudesce or are cleared from the blood.
While rapid diagnostic tests have replaced microscopy in some contexts, microscopy remains an essential tool to support clinical diagnosis and research. The standardisation of methods allows direct comparisons from studies conducted across different points in time and location. This facilitates individual participant data meta-analyses, recognised as the gold standard approach to generate evidence for improvements in interventions and hence patient outcomes.
Estimating Annual Fluctuations in Malaria Transmission Intensity and in the Use of Malaria Control Interventions in Five Sub-Saharan African Countries
RTS,S/AS01E malaria vaccine safety, effectiveness, and impact will be assessed in pre- and post-vaccine introduction studies, comparing the occurrence of malaria cases and adverse events in vaccinated versus unvaccinated children. Because those comparisons may be confounded by potential year-to-year fluctuations in malaria transmission intensity and malaria control intervention usage, the latter should be carefully monitored to adequately adjust the analyses. This observational cross-sectional study is assessing Plasmodium falciparum parasite prevalence (PfPR) and malaria control intervention usage over nine annual surveys performed at peak parasite transmission. Plasmodium falciparum parasite prevalence was measured by microscopy and nucleic acid amplification test (quantitative PCR) in parallel in all participants, and defined as the proportion of infected participants among participants tested. Results of surveys 1 (S1) and 2 (S2), conducted in five sub-Saharan African countries, including some participating in the Malaria Vaccine Implementation Programme (MVIP), are reported herein; 4,208 and 4,199 children were, respectively, included in the analyses.
Plasmodium falciparum parasite prevalence estimated using microscopy varied between study sites in both surveys, with the lowest prevalence in Senegalese sites and the highest in Burkina Faso. In sites located in the MVIP areas (Kintampo and Kombewa), PfPR in children aged 6 months to 4 years ranged from 24.8% to 27.3%, depending on the study site and the survey. Overall, 89.5% and 86.4% of children used a bednet in S1 and S2, of whom 68.7% and 77.9% used impregnated bednets. No major difference was observed between the two surveys in terms of PfPR or use of malaria control interventions. © The American Society of Tropical Medicine and Hygiene [open-access]
Community perception of malaria in a vulnerable municipality in the Colombian Pacific
Malaria primarily affects populations living in poor socioeconomic conditions, with limited access to basic services, deteriorating environmental conditions, and barriers to accessing health services. Control programmes are designed without participation from the communities involved, ignoring local knowledge and sociopolitical and cultural dynamics surrounding their main health problems, which implies imposing decontextualized control measures that reduce coverage and the impact of interventions. The objective of this study was to determine the community perception of malaria in the municipality of Olaya Herrera in the Colombian Pacific.
A 41-question survey on knowledge, attitudes, and practices (KAP) related to malaria, the perception of actions by the Department of Health, and access to the health services network was conducted. In spite of the knowledge about malaria and the efforts of the Department of Health to prevent it, the community actions do not seem to be consistent with this knowledge, as the number of cases of malaria is still high in the area.
Use of a Plasmodium vivax genetic barcode for genomic surveillance and parasite tracking in Sri Lanka
Sri Lanka was certified as a malaria-free nation in 2016; however, imported malaria cases continue to be reported. Evidence-based information on the genetic structure/diversity of the parasite populations is useful to understand the population history, assess the trends in transmission patterns, as well as to predict threatening phenotypes that may be introduced and spread in parasite populations disrupting elimination programmes. This study used a previously developed Plasmodium vivax single nucleotide polymorphism (SNP) barcode to evaluate the population dynamics of P. vivax parasite isolates from Sri Lanka and to assess the ability of the SNP barcode for tracking the parasites to its origin.
A total of 51 P. vivax samples collected during 2005–2011, mainly from three provinces of the country, were genotyped for 40 previously identified P. vivax SNPs using a high-resolution melting (HRM), single-nucleotide barcode method. The proportion of multi-clone infections was significantly higher in isolates collected during an infection outbreak in year 2007. Plasmodium vivax parasite isolates collected during a disease outbreak in year 2007 were more genetically diverse compared to those collected from other years. In-silico analysis using the 40 SNP barcode is a useful tool to track the origin of an isolate of uncertain origin, especially to differentiate indigenous from imported cases. However, an extended barcode with more SNPs may be needed to distinguish highly clonal populations within the country.
Coronavirus rumours and regulations mar Burkina Faso’s malaria fight
 By Sam Mednick, Thomson Reuters Foundation: MOAGA, Burkina Faso – Health worker Estelle Sanon would hold the 18-month-old and administer the SMC dose herself, but because of coronavirus she has to keep a distance from her patients. “If I am standing and watching the mother do it, it’s as if I’m not doing my work,” said Sanon, a community health volunteer assisting in a seasonal campaign to protect children in the West African country from the deadly mosquito-borne disease.
By Sam Mednick, Thomson Reuters Foundation: MOAGA, Burkina Faso – Health worker Estelle Sanon would hold the 18-month-old and administer the SMC dose herself, but because of coronavirus she has to keep a distance from her patients. “If I am standing and watching the mother do it, it’s as if I’m not doing my work,” said Sanon, a community health volunteer assisting in a seasonal campaign to protect children in the West African country from the deadly mosquito-borne disease.
Burkina Faso is one of the 10 worst malaria-affected nations in the world, accounting for 3% of the estimated 405,000 malaria deaths globally in 2018, according to the World Health Organization (WHO). More than two-thirds of victims are children under five. Now there are fears malaria cases could rise in Burkina Faso as restrictions due to coronavirus slow down a mass treatment campaign and rumours over the virus causing parents to hide their children, according to health workers and aid officials.
“COVID-19 has the potential to worsen Burkina Faso’s malaria burden,” said Donald Brooks, head of the U.S. aid group Initiative: Eau, who has worked on several public health campaigns in the country. “If preventative campaigns can’t be thoroughly carried out and if people are too scared to come to health centres … it could certainly increase the number of severe cases and the risk of poor outcomes.”
During peak malaria season, from July to November, community health workers deploy across Burkina Faso to treat children with seasonal malaria chemoprevention (SMC). This is the second year the campaign will cover the whole country with more than 50,000 volunteers going door-to-door, said Gauthier Tougri, coordinator for the country’s anti-malaria programme. Logistics were already challenging. Violence linked to jihadists and local militias has forced more than one million people to flee their homes, shuttered health clinics and made large swathes of land inaccessible. Now the coronavirus has made the task even harder, health workers said.
People in Cape Verde evolved better malaria resistance in 550 years
Yes, we are still evolving. And one of the strongest examples of recent evolution in people has been found on the Cape Verde islands in the Atlantic, where a gene variant conferring a form of malaria resistance has become more common.
Portuguese voyagers settled the uninhabited islands in 1462, bringing slaves from Africa with them. Most of the archipelago’s half a million inhabitants are descended from these peoples. Most people of West African origin have a variant in a gene called DARC that protects.
Deadly malaria and cholera outbreaks grow amongst refugees as COVID pandemic strains health systems.
Apart from the strain on health facilities during the pandemic, in some countries such as Somalia, Kenya and Sierra Leone, we are seeing that a fear of exposure to COVID-19 has prevented parents from taking their children to hospital, delaying diagnosis and treatment of malaria and increasing preventable deaths. COVID restrictions in some countries have also meant pregnant women have missed antimalarial drugs. Untreated malaria in pregnant women can increase the risk of anaemia, premature births, low birth weight and infant death. According to the World Health Organization (WHO), 80% of programs designed to fight HIV, tuberculosis and malaria have been disrupted due to the pandemic and 46% of 68 countries report experiencing disruptions in the treatment and diagnosis of malaria.
Integration &NTDs &Tuberculosis Bill Brieger | 24 Mar 2017
World Tuberculosis Day: United We Can End TB and Tropical Diseases
 The theme of World TB Day is to Unite to end TB: leave no one behind. The communities affected by TB are also ones where tropical diseases like onchocerciasis and malaria are endemic. A successful strategy to control one disease should ideally be “united” with all basic primary health care interventions, thereby truly leaving no one behind.
The theme of World TB Day is to Unite to end TB: leave no one behind. The communities affected by TB are also ones where tropical diseases like onchocerciasis and malaria are endemic. A successful strategy to control one disease should ideally be “united” with all basic primary health care interventions, thereby truly leaving no one behind.
While the causative agents differ between TB and tropical diseases such as malaria, lymphatic filariasis and Dengue, control of these diseases shares a common goal – “an urgent need to develop new vaccines for HIV/AIDS, malaria, and tuberculosis, as well as for respiratory syncytial virus and those chronic and debilitating (mostly parasitic) infections known as neglected tropical diseases (NTDs).” In addition to prevention, there is also need for integrated “treatment pipelines directed at NTDs, Malaria, tuberculosis (TB), and human immunodeficiency virus (HIV)/AIDS,” according to Asada.
There is also a need for integrated primary health care (PHC) programming. In the Journal of Infectious Diseases. Simon reports on linkages showing that, “Recent research suggests that NTDs can affect HIV and AIDS, tuberculosis (TB), and malaria disease progression. A combination of immunological, epidemiological, and clinical factors can contribute to these interactions and add to a worsening prognosis for people affected by HIV/AIDS, TB, and malaria.”
 The possibility of integrating directly observed treatment (DOT) for TB treatment into community health worker (CHW)/PHC programs that addressed malaria treatment and onchocerciasis control was tested by the Tropical Disease Research Program (TDR) some years ago. CHWs in a few of the study sites were able to successfully include DOT for TB in their community duties, but in other sites community and health worker fears about stigma inhibited action.
The possibility of integrating directly observed treatment (DOT) for TB treatment into community health worker (CHW)/PHC programs that addressed malaria treatment and onchocerciasis control was tested by the Tropical Disease Research Program (TDR) some years ago. CHWs in a few of the study sites were able to successfully include DOT for TB in their community duties, but in other sites community and health worker fears about stigma inhibited action.
TB, malaria and NTDs are among the conditions referred to as the infectious diseases of poverty. We will not eliminate poverty by tackling these diseases one-by-one. A “United” and integrated approach from national to community level is needed.
coinfection &Epidemiology &Tuberculosis Bill Brieger | 24 Mar 2014
World TB Day: considering malaria coinfection
Typical of our big disease mindset, most donor agencies think of HIV-Tuberculosis coinfection when addressing a connection among the three Global Fund diseases. Take as an example a recent News Flash from the Global Fund: “In a major step toward addressing the growing number of people affected by co-infection with tuberculosis and HIV, the Global Fund is improving the way it approaches treatment programs in countries with high rates of each disease. Millions of people infected with both TB and HIV could benefit from better services.”
 The possible neglect of TB and malaria interactions might be understood by the fact that HIV and TB have much wider areas of endemicity than malaria. On the other hand both HIV and TB are disproportionately represented in malaria endemic Africa. At present the main connection between malaria and TB is the fact that they must share out of the same ‘envelope’ when new Global Fund support is distributed through the new funding mechanism to countries, a process that some see as moving more toward donor control and AID effectiveness and away from human rights.
The possible neglect of TB and malaria interactions might be understood by the fact that HIV and TB have much wider areas of endemicity than malaria. On the other hand both HIV and TB are disproportionately represented in malaria endemic Africa. At present the main connection between malaria and TB is the fact that they must share out of the same ‘envelope’ when new Global Fund support is distributed through the new funding mechanism to countries, a process that some see as moving more toward donor control and AID effectiveness and away from human rights.
Today the Stop-TB Partnership and related organizations are observing World TB day by noting that at least one-third of newly infected people will not get appropriate treatment. Poor access to or inadequate and inappropriate treatment plagues all three diseases, especially where health systems are weak. We need an integrated approach to strengthen systems and improve care.
In the meantime, researchers have maintained interest in possible interactions between TB and malaria. For example Ann-Kristin Mueller and colleagues have published a study entitled, “An Experimental Model to Study Tuberculosis-Malaria Coinfection upon Natural Transmission of Mycobacterium tuberculosis and Plasmodium berghei,” using a mouse model. A slide presentation on their work is also seen at the website. As Mueller notes, “Concurrent infections most likely modulate the respective immune response to each single pathogen and may thereby affect pathogenesis and disease outcome. Coinfected patients may also respond differentially to anti-infective interventions.”
Mueller puts is mildly when she says that TB-malaria coinfection “has not been studied in detail.” We might need to step back in time over 2900 years where according to Lalremruata and colleagues, “the notion that the agricultural boom and dense crowding occurred in this region (southwest of modern Cairo), especially under the Ptolemies, highly increased the probability for the manifestation and spread of tuberculosis. Here we extend back-wards to ca. 800 BC new evidence for malaria tropica and human tuberculosis co-occurrence in ancient Lower Egypt.”
In a 2013 review on “Co-infection of tuberculosis and parasitic diseases in humans,” Xin-Xu Li and Xiao-Nong Zhou found only two direct reports of malaria and TB co-infection, one a case report from 1945 and the other on host response in malaria and depression of defense against tuberculosis from 1999.
Finally a review of hospital records from 2007 in Luanda, Angola found that Malaria was diagnosed during admission and hospital stay in 37.5% of TB patients. Clearly the time has come to take coinfection seriously as both a research and service delivery topic.