HPV &Vaccine Bill Brieger | 15 Mar 2023
Malawi Experiences HPV vaccination Shortages as Registration Increases Among Adolescents Girls
By Jordan Kerr and originally posted in the Social and Behavioral Foundations of Primary Health Care Blog.
 Malawi is making strides in increasing HPV vaccinations among adolescent girls across the nation. Since the official implementation of the HPV vaccine program in 2019, 20 out of the 29 districts in Malawi have begun administering the vaccine to adolescent girls between the age of 9 and 14. Despite this success, Malawi continues to be one of the leading countries worldwide in cervical cancer-related mortality. New cases of cervical cancer in Malawi are reported at a rate five times higher than the global average.
Malawi is making strides in increasing HPV vaccinations among adolescent girls across the nation. Since the official implementation of the HPV vaccine program in 2019, 20 out of the 29 districts in Malawi have begun administering the vaccine to adolescent girls between the age of 9 and 14. Despite this success, Malawi continues to be one of the leading countries worldwide in cervical cancer-related mortality. New cases of cervical cancer in Malawi are reported at a rate five times higher than the global average.
 This highly preventable disease places a more significant burden on low-income countries like Malawi due to poor access to healthcare services and resources. International agencies are improving their outreach efforts to reach girls not enrolled in school and address vaccine hesitancy in districts with higher vaccine refusal rates. Due to this outreach vaccine registration is improving however healthcare facilities are experiencing stockouts. In some districts, healthcare facilities are reporting that the main reason individuals are not receiving vaccinations is that they are running out of vaccine stocks.
This highly preventable disease places a more significant burden on low-income countries like Malawi due to poor access to healthcare services and resources. International agencies are improving their outreach efforts to reach girls not enrolled in school and address vaccine hesitancy in districts with higher vaccine refusal rates. Due to this outreach vaccine registration is improving however healthcare facilities are experiencing stockouts. In some districts, healthcare facilities are reporting that the main reason individuals are not receiving vaccinations is that they are running out of vaccine stocks.
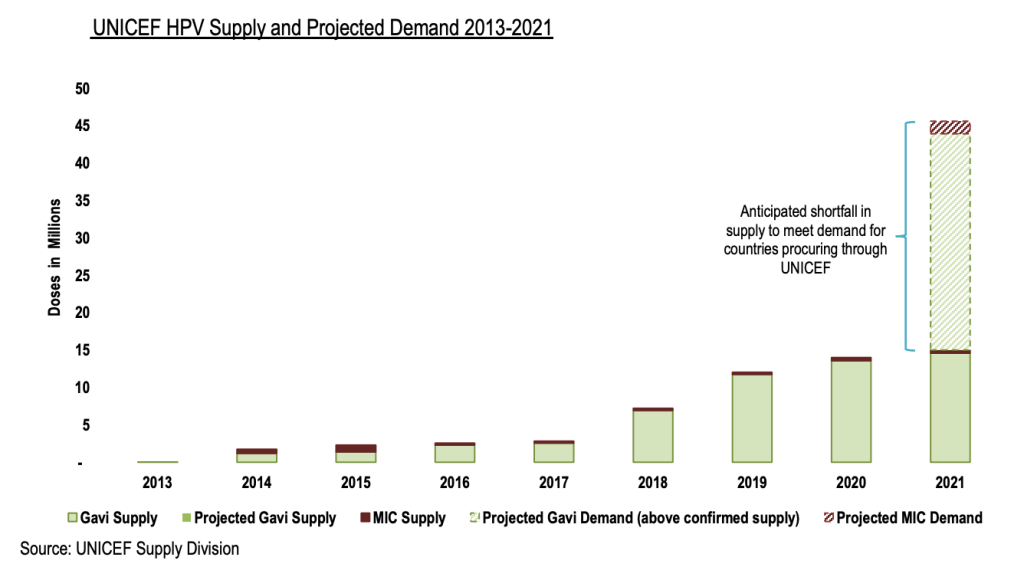
The World Health Organization (WHO) set a goal in 2018 to eliminate cervical cancer by increasing HPV vaccination uptake globally. This initiative has shown to be successful in addressing disparities in low- and middle-income countries however, in 2020 an HPV vaccination shortage began and is expected to continue through 2025.
The Center for Strategic and International Studies (CSIS) presents several strategies that can be used to address this shortage to keep on track with the goal to eliminate cervical cancer. Efforts must be taken to support facilities developing the HPV vaccine to ensure stockouts do not continue. We need policymakers to lobby for policies that increase funding for vaccination development and establish priority vaccination allocations to countries like Malawi that are experiencing high mortality rates from cervical cancer
Schistosomiasis &water Bill Brieger | 15 Mar 2023
Effective Strategies to Eliminate Schistosomiasis in School Children in Rural Parts of Ghana
By Lauren Koranteng and originally posted in the Social and Behavioral Foundations of Primary Health Care Blog.
“Overcoming poverty is not a task of charity, it is an act of justice. Like Slavery and Apartheid, poverty is not natural. It is man-made and it can be overcome and eradicated by the actions of human beings. Sometimes it falls on a generation to be great. You can be that great generation. Let your greatness blossom.” – Nelson Mandela
 According to the World Health Organization, Schistosomiasis is a “disease of poverty that leads to chronic ill-health “. It is caused by a parasitic worm that lives in freshwater snails. The larval forms of the parasite is released by the snails. Humans who make contact with the water during various activities like recreation, agriculture and also for livelihood get infected. The prevalence rate in Ghana is 23.3% , however there are some areas that have localized prevalence levels that are >50% ( Kulinkina et al).
A vulnerable population that is often infected are school aged children who access the waters mostly for recreational reasons (Antwi et al).
These are usually school aged children who live in hard to reach areas in the country with poor sanitation. It is important for the disease to be controlled because chronic ill health also impacts the cognitive abilities of the children.
Praziquantel is a drug used for preventative chemotherapy against Schistosomiasis. It offers a solution to eradication of the disease and could be executed through drug administration of praziquantel through the school system. This kind of mass administration has been done before in the country, but unfortunately, the behavior of children swimming in these infected waters did not change. This behavior of continuous exposure of children to these water bodies presented a limited factor in the eradication of this disease and intervention.
Using the national health insurance program in the country, praziquantel can be made available again but through school programs in these rural areas. Additionally, the school curriculum can include health education that will encourage children to avoid fresh water bodies where possible.
Sanitation improvement and reduced human and infected water contact will also be a priority health development goal.
So, in working with stakeholders such as the Ghana Health Service and the Ministry of Education, a realistic plan can be developed and executed. This can include a mass drug administration program, health education and sanitation improvement. This may be reasonable interventions to use to support children who are in contact with fresh water bodies and at a high risk of contracting Schistosomiasis.
According to the World Health Organization, Schistosomiasis is a “disease of poverty that leads to chronic ill-health “. It is caused by a parasitic worm that lives in freshwater snails. The larval forms of the parasite is released by the snails. Humans who make contact with the water during various activities like recreation, agriculture and also for livelihood get infected. The prevalence rate in Ghana is 23.3% , however there are some areas that have localized prevalence levels that are >50% ( Kulinkina et al).
A vulnerable population that is often infected are school aged children who access the waters mostly for recreational reasons (Antwi et al).
These are usually school aged children who live in hard to reach areas in the country with poor sanitation. It is important for the disease to be controlled because chronic ill health also impacts the cognitive abilities of the children.
Praziquantel is a drug used for preventative chemotherapy against Schistosomiasis. It offers a solution to eradication of the disease and could be executed through drug administration of praziquantel through the school system. This kind of mass administration has been done before in the country, but unfortunately, the behavior of children swimming in these infected waters did not change. This behavior of continuous exposure of children to these water bodies presented a limited factor in the eradication of this disease and intervention.
Using the national health insurance program in the country, praziquantel can be made available again but through school programs in these rural areas. Additionally, the school curriculum can include health education that will encourage children to avoid fresh water bodies where possible.
Sanitation improvement and reduced human and infected water contact will also be a priority health development goal.
So, in working with stakeholders such as the Ghana Health Service and the Ministry of Education, a realistic plan can be developed and executed. This can include a mass drug administration program, health education and sanitation improvement. This may be reasonable interventions to use to support children who are in contact with fresh water bodies and at a high risk of contracting Schistosomiasis.
 According to the World Health Organization, Schistosomiasis is a “disease of poverty that leads to chronic ill-health “. It is caused by a parasitic worm that lives in freshwater snails. The larval forms of the parasite is released by the snails. Humans who make contact with the water during various activities like recreation, agriculture and also for livelihood get infected. The prevalence rate in Ghana is 23.3% , however there are some areas that have localized prevalence levels that are >50% ( Kulinkina et al).
A vulnerable population that is often infected are school aged children who access the waters mostly for recreational reasons (Antwi et al).
These are usually school aged children who live in hard to reach areas in the country with poor sanitation. It is important for the disease to be controlled because chronic ill health also impacts the cognitive abilities of the children.
Praziquantel is a drug used for preventative chemotherapy against Schistosomiasis. It offers a solution to eradication of the disease and could be executed through drug administration of praziquantel through the school system. This kind of mass administration has been done before in the country, but unfortunately, the behavior of children swimming in these infected waters did not change. This behavior of continuous exposure of children to these water bodies presented a limited factor in the eradication of this disease and intervention.
Using the national health insurance program in the country, praziquantel can be made available again but through school programs in these rural areas. Additionally, the school curriculum can include health education that will encourage children to avoid fresh water bodies where possible.
Sanitation improvement and reduced human and infected water contact will also be a priority health development goal.
So, in working with stakeholders such as the Ghana Health Service and the Ministry of Education, a realistic plan can be developed and executed. This can include a mass drug administration program, health education and sanitation improvement. This may be reasonable interventions to use to support children who are in contact with fresh water bodies and at a high risk of contracting Schistosomiasis.
According to the World Health Organization, Schistosomiasis is a “disease of poverty that leads to chronic ill-health “. It is caused by a parasitic worm that lives in freshwater snails. The larval forms of the parasite is released by the snails. Humans who make contact with the water during various activities like recreation, agriculture and also for livelihood get infected. The prevalence rate in Ghana is 23.3% , however there are some areas that have localized prevalence levels that are >50% ( Kulinkina et al).
A vulnerable population that is often infected are school aged children who access the waters mostly for recreational reasons (Antwi et al).
These are usually school aged children who live in hard to reach areas in the country with poor sanitation. It is important for the disease to be controlled because chronic ill health also impacts the cognitive abilities of the children.
Praziquantel is a drug used for preventative chemotherapy against Schistosomiasis. It offers a solution to eradication of the disease and could be executed through drug administration of praziquantel through the school system. This kind of mass administration has been done before in the country, but unfortunately, the behavior of children swimming in these infected waters did not change. This behavior of continuous exposure of children to these water bodies presented a limited factor in the eradication of this disease and intervention.
Using the national health insurance program in the country, praziquantel can be made available again but through school programs in these rural areas. Additionally, the school curriculum can include health education that will encourage children to avoid fresh water bodies where possible.
Sanitation improvement and reduced human and infected water contact will also be a priority health development goal.
So, in working with stakeholders such as the Ghana Health Service and the Ministry of Education, a realistic plan can be developed and executed. This can include a mass drug administration program, health education and sanitation improvement. This may be reasonable interventions to use to support children who are in contact with fresh water bodies and at a high risk of contracting Schistosomiasis.
Children &Mortality &Vaccine Bill Brieger | 14 Mar 2023
THE RTS,S MALARIA VACCINE: A Solution to Nigeria’s Constant Public Health Crisis
By Blessing George & Chino Nduaka and originally posted in the Social and Behavioral Foundations of Primary Health Care Blog.
 More than 50% of deaths from malaria are from four African countries, and Nigeria heads the list, contributing a significant part at more than 30%. Nigeria faces a major public health burden, with an estimated 65 million cases and over 100,000 deaths in 2021, representing over 50% of malaria cases in West Africa. With most outpatient visits in Nigeria being caused by malaria, this disease has taken a toll on the economy.
Malaria is among the top five causes of under-five mortality in Nigeria. Over the years, various organizations have joined hands in the fight against this deadly disease. However, Nigeria remains at the top of the list contributing significantly to the mortality rate. Insecticide-treated nets (ITNs), indoor residual spraying, and free sharing of anti-malaria drugs for prophylaxis and treatment constitute ways the country has tackled the disease burden. With the funding allocation repeatedly given by international organizations such as the WHO, the World Bank, and the Global Fund channeled to these interventions that have proved somewhat ineffective, we are at crossroads that begs the question, what next?
In 2016, the world’s pioneer malaria vaccine, RTS, S, sold with the brand name, Mosquirix, was introduced for pilot implementation in three malaria-endemic countries. It has been administered to over a million children with positive results on its effectiveness. In 2022, the Nigerian government officially applied to receive the vaccine through GAVI but was hit back with the response that currently, there is an insufficient supply of vaccines.
More than 50% of deaths from malaria are from four African countries, and Nigeria heads the list, contributing a significant part at more than 30%. Nigeria faces a major public health burden, with an estimated 65 million cases and over 100,000 deaths in 2021, representing over 50% of malaria cases in West Africa. With most outpatient visits in Nigeria being caused by malaria, this disease has taken a toll on the economy.
Malaria is among the top five causes of under-five mortality in Nigeria. Over the years, various organizations have joined hands in the fight against this deadly disease. However, Nigeria remains at the top of the list contributing significantly to the mortality rate. Insecticide-treated nets (ITNs), indoor residual spraying, and free sharing of anti-malaria drugs for prophylaxis and treatment constitute ways the country has tackled the disease burden. With the funding allocation repeatedly given by international organizations such as the WHO, the World Bank, and the Global Fund channeled to these interventions that have proved somewhat ineffective, we are at crossroads that begs the question, what next?
In 2016, the world’s pioneer malaria vaccine, RTS, S, sold with the brand name, Mosquirix, was introduced for pilot implementation in three malaria-endemic countries. It has been administered to over a million children with positive results on its effectiveness. In 2022, the Nigerian government officially applied to receive the vaccine through GAVI but was hit back with the response that currently, there is an insufficient supply of vaccines.
 Nigeria tops the list of the global malaria mortality rate and should be prioritized. The Nigerian Ministry of Health, in collaboration with the Nigerian Primary Healthcare agency, needs to fight for the health of its citizens, respond to GAVI, and state the concrete reasons why the country should be prioritized. The goal is to ensure that these vaccines are made available for the under-5 population in Nigeria by 2025 such that in the malaria world report of 2030, Nigeria should not be named a major contributing country to malaria mortality.
Nigeria tops the list of the global malaria mortality rate and should be prioritized. The Nigerian Ministry of Health, in collaboration with the Nigerian Primary Healthcare agency, needs to fight for the health of its citizens, respond to GAVI, and state the concrete reasons why the country should be prioritized. The goal is to ensure that these vaccines are made available for the under-5 population in Nigeria by 2025 such that in the malaria world report of 2030, Nigeria should not be named a major contributing country to malaria mortality.

https://www.everydayhealth.com/malaria/world-health-organization-approves-first-malaria-vaccine/
 Nigeria tops the list of the global malaria mortality rate and should be prioritized. The Nigerian Ministry of Health, in collaboration with the Nigerian Primary Healthcare agency, needs to fight for the health of its citizens, respond to GAVI, and state the concrete reasons why the country should be prioritized. The goal is to ensure that these vaccines are made available for the under-5 population in Nigeria by 2025 such that in the malaria world report of 2030, Nigeria should not be named a major contributing country to malaria mortality.
Nigeria tops the list of the global malaria mortality rate and should be prioritized. The Nigerian Ministry of Health, in collaboration with the Nigerian Primary Healthcare agency, needs to fight for the health of its citizens, respond to GAVI, and state the concrete reasons why the country should be prioritized. The goal is to ensure that these vaccines are made available for the under-5 population in Nigeria by 2025 such that in the malaria world report of 2030, Nigeria should not be named a major contributing country to malaria mortality.
Typhoid &water Bill Brieger | 14 Mar 2023
Typhoid fever in Lagos, Nigeria
By Peace Ige, and originally posted in the Social and Behavioral Foundations of Primary Health Care Blog.
In Nigeria, typhoid fever continues to be a significant disease, and its prevalence is on the rise. The disease is transmitted through the oral consumption of contaminated food or water and can also be spread through personal contact due to unsanitary practices (Enabulele et al., 2016). The increasing incidence of antibiotic-resistant strains of the bacteria makes treating typhoid fever challenging. The lack of proper surveillance, limited laboratory capacity, and inadequate data availability in Nigeria make it difficult to assess the actual prevalence of typhoid fever. 
There needs to be more reliable and consistent data on the incidence of typhoid fever in Lagos and Nigeria, making it challenging to assess the disease’s prevalence accurately. This under-reporting is due to several reasons, including using antibiotics before confirmatory laboratory tests and patients’ failure to seek medical attention, as laboratory services are often not affordable (Enabulele et al., 2016).
According to a study published in The American Journal of Tropical Medicine and Hygiene (primary article), the lack of epidemiological data tracking regarding typhoid fever in sub-Saharan Africa prompted the World Health Organization (WHO) to call for a continent-wide approach to generate more accurate disease incidence and antimicrobial susceptibility data in 2008. The study emphasizes the importance of antibiotic resistance as a significant health security issue, as S. Typhi has developed resistance to multiple drugs, making it difficult to treat.
Typhoid fever remains endemic in Lagos, Nigeria, and the larger sub-Saharan Africa region, posing a significant public health challenge. To address this issue, coordinated efforts are needed from all stakeholders. Strengthening surveillance systems to collect accurate data on typhoid fever incidence, prevalence, and antimicrobial susceptibility is critical (Enabulele et al., 2016). This requires government funding to improve laboratory infrastructure and trained personnel. Accessible data can guide policy decisions and interventions. Improving sanitation and hygiene practices is also vital to combating typhoid fever.
The government should invest in improving access to potable water, wastewater management systems, and community education on personal hygiene practices. Public and private sector partnerships can be established to improve water and sanitation infrastructure in vulnerable communities. Increased vaccination campaigns are a cost-effective intervention in reducing the incidence of typhoid fever. The Nigerian government should increase the coverage of the typhoid fever vaccine in Lagos state, especially for vulnerable populations such as children and those in low-income communities.
A robust public health campaign should promote vaccine uptake and raise awareness of typhoid fever and its causes. A multi-sectoral approach is needed to address the root causes of typhoid fever in Lagos. Collaboration between the government, healthcare providers, the private sector, and other stakeholders is necessary to ensure the implementation of effective interventions. Advocacy efforts are necessary to ensure political commitment and support for policies addressing typhoid fever in Lagos. By implementing these strategies, Lagos can reduce the incidence and impact of typhoid fever on its population.
Lagos, Nigeria, must take responsibility for addressing the issue of typhoid fever and external support. The World Health Organization (WHO) has already called for a continental approach to generate accurate disease incidence and antimicrobial susceptibility data, and Nigeria must take advantage of this support. One of the critical areas where external support is essential is strengthening the healthcare system’s capacity for surveillance and diagnosis of typhoid fever. This includes improving laboratory facilities and providing training for healthcare workers.
Support from organizations such as WHO and the Centers for Disease Control and Prevention (CDC) can help develop effective policies and programs to control the spread of typhoid fever. Another area where external support is critical is promoting research into new and effective treatments for typhoid fever. This includes developing new antibiotics and vaccines and studying the disease’s epidemiology and ecology to understand better how it spreads and can be prevented.
External support is essential in helping to raise awareness of the issue of typhoid fever and its impact on public health in Nigeria. By working with local communities and stakeholders, external organizations can help to educate people about the disease, how it is spread, and how it can be prevented. This can create a sense of urgency around the issue and mobilize local communities and governments to take action.

The bluish line in the graph shows the rate of S. Typhi that can resist ampicillin. The orange line shows Chlora6mphenicol-resistant S. Typhi. Co-trimoxazole-resistant Staphylococcus typhi prevalence is shown by the gray line. S. the yellow line shows Typhi tetracycline resistance. The dark blue line shows the proportion of S. Typhi resistant to ciprofloxacin. The green line shows cefuroxime-resistant S. Typhi.
In 2003, cefuroxime entered clinical use. The red line shows the proportion of S. Typhi strains resistant to cefotaxime. In 2008, cefotaxime was made available to the public. In conclusion, typhoid fever remains a significant public health issue in Lagos, Nigeria. The persistence of the disease can be attributed to poor surveillance, inadequate data availability, restricted laboratory capacity, and resource and financial limitations that contribute to poor quality water, sanitation, and hygiene infrastructure.
The adoption of proper measures can significantly reduce the incidence of typhoid fever in Lagos. The Lagos State Government and stakeholders in Nigeria must show more commitment and will to provide the necessary means to combat the endemic disease. The involvement of external forces such as WHO, CDC, and other international organizations in promoting the eradication of the disease is essential. Their support in generating more accurate disease incidence and antimicrobial susceptibility data, improving laboratory capacity, and providing resources for disease surveillance and control is a significant step toward eradicating the disease.”
All stakeholders must work together to ensure the necessary measures are taken to end the endemic disease. With proper measures in place, we can significantly reduce the incidence of typhoid fever in Lagos, Nigeria, and ultimately eradicate the disease.
IPTp &Malaria in Pregnancy &Resistance Bill Brieger | 02 Mar 2023
Are we prepared to protect pregnant women from malaria as SP resistance spreads
Adegbola and colleagues note that “the efficacy of SP-IPTp is threatened by the emergence of sulfadoxine-pyrimethamine resistant malaria parasites, “which has been observed in East Africa. They therefore, studied the situation in Nigeria, the country with the highest malaria burden in the continent. Their study showed that “the prevalence of VAGKGS haplotype seems to be increasing in prevalence.”
In conclusion, they worried that, “If this is similar in effect to the emergence of 581G in East Africa, the efficacy of SP-IPTp in the presence of these novel Pfdhps mutants should be re-assessed” in Nigeria. This situation threatens the use of sulfadoxine-pyrimethamine (SP) in two major prevention programs including intermittent preventive treatment during pregnancy (IPTp) and seasonal malaria chemoprevention (SMC) for children.
The benefits of IPTp using SP is the ability to administer chemoprevention in a single directly observed dose. Alternative medications are being explored, but from the behavioral intervention perspective, the low cost and simplicity afforded by SP is ideal.
 The IPTp strategy had been modified a decade ago from requiring 2 doses, to monthly doses from the second trimester onwards because of parasite resistance or what is also termed drug tolerance by the parasite. Tolerance implies that the drug may still work, but at higher or more frequent doses. Such changes have cost and behavior change implications. Many country reports from the Malaria Indicator Surveys show an expected drop-off in uptake of SP between the first and third doses. For example in the 2021 Nigeria MIS IPTp1 uptake was 58%, while IPTp3 had reduced to 31%.
The IPTp strategy had been modified a decade ago from requiring 2 doses, to monthly doses from the second trimester onwards because of parasite resistance or what is also termed drug tolerance by the parasite. Tolerance implies that the drug may still work, but at higher or more frequent doses. Such changes have cost and behavior change implications. Many country reports from the Malaria Indicator Surveys show an expected drop-off in uptake of SP between the first and third doses. For example in the 2021 Nigeria MIS IPTp1 uptake was 58%, while IPTp3 had reduced to 31%.
A related problem in Nigeria is the ubiquitous availability of SP in medicine shops across the country in contrast to official policy limiting it to use in IPTp and SMC. The challenge is finding affordable and feasible alternative medicines for IPTp. In the meantime, we have not even reached coverage targets using SP nor fully achieved rollout of companion interventions such as the use of Insecticide Treated Nets. Much work is still needed to protect pregnant women and fetuses from the malaria induced problems of anemia, low-birth-weight, stillbirth, and more.
A related study from Cameroon: The occurrence of sub-microscopic P. falciparum parasites resistant to SP and intense malaria transmission poses persistent risk of malaria infection during pregnancy in the area. ITN usage and monitoring spread of resistance are critical.
https://malariajournal.biomedcentral.com/articles/10.1186/s12936-023-04485-7