Advocacy &Community &Diagnosis &Education &Elimination &Epidemiology &India &IRS &ITNs &Malaria &Plasmodium/Parasite &Procurement Supply Management &Research &Strategy &Surveys &Vaccine &Vector Control &World Malaria Day Bill Brieger | 24 Apr 2025
The Johns Hopkins Bloomberg School of Public Health Dean’s Lecture on Malaria
Professor Jane Carlton, PhD, Director of Johns Hopkins Malaria Research Institute was introduced by Dean Ellen MacKenzie to give a Dean’s Lecture entitled “Malaria: History, current status, and the promise of ‘omics and AI.”

Prof. Carlton first gave an overview of JHMRI, which was founded in 2001. She stepped into director role in 2023. She started with the encouraging premise that AI and ‘omics can supercharge our research and pointed out the power of comparative genomics on understanding parasites and disease. Her goal is to translate discovery into real world impact through collaborations.
The talk started with a brief malaria history. Malaria was described as an ancient disease and remains one of top infectious diseases worldwide. There were 2.63 million cases and more than half a million deaths in 83 endemic countries in 2023. Today 44 countries are malaria-free.
Up until now, Prof. Carlton noted, the malaria map has been shrinking. There was a precipitous decline in malaria in India from 23 million cases to 2 million. The disease is a true humanitarian issue with a large impact on people living in resource-limited settings where housing is basic and offers no protection from mosquitoes.

The JHMRI is supported by Bloomberg philanthropies, and from that base faculty research examines, among others, better methods for controlling mosquitoes (see slide), new diagnostic tests and therapeutics, and the next generation of vaccines. Key assets to support research include mosquito insectaries and a malaria parasite core. The insectaries produce 60,000 mosquitoes per week, and with these it is possible to complete the life cycle in the laboratory.
Continuing education is another important function of JHMRI which has three conferences per year including the upcoming World Malaria Day 2025 symposium. One can also learn from the Malaria Minute podcast. The upcoming “Vector Encounter” provides sharing and learning for researchers.

JHMRI studies malaria at field sites in Africa and Asia where country collaborators are partners. Emphasis is on local capacity building in countries like Zambia, Ethiopia, Kenya, and Uganda. Researchers and the national malaria control programs in these countries work hand-in-hand.
JHMRI is involved in developing the next generation of vaccines. One approach if a human monoclonal antibody that prevents malaria infections. Another develops a vaccine that transcends’ malaria parasite strains with structure guided mimicry of an essential P. falciparum receptor-ligand complex enhances cross neutralizing antibodies. A third example asks “How many parasites does it take to cause malaria?” and assesses infection likelihood through mosquito parasite burden.
To understand the theme of her talk, Prof. Carlton reviewed the promise of ‘omics and AI in the context of her work at a center of excellence in India. Pioneering work using Malaria camps in hard-to-reach villages in Odisha, India. The main activities mobilized villagers to gather for mass screening, treatment, education, and intensified vector control. From there, Indoor Residual Spraying was planned and insecticide treated bednets were distributed. Other maternal and child health activities were incorporated. After three rounds/visits in the remote villages a great drop of malaria cases was seen. WHO lauded the camps.

In addition to lessons about the importance of surveillance, mixed strategies, and community mobilization for controlling malaria, the team learned about the growing challenge of reduced effectiveness of Rapid Diagnostic Tests. The problem arose because tests were dependent on a protein that was no longer being expressed due to Pfhrp2 gene deletions, leading to false negative test results. The team was encouraged to identify more proteins to find a more stable and central one to use in testing. Through machine learning, this work is ongoing but promising.
While we are on the verge of several research and programmatic breakthroughs, Prof. Carlton reminded the audience that we are in calamitous times. She recalled that the United States has been the top donor government to malaria efforts through Presidents Malaria Initiative and Global Fund to Fight AIDS, Tuberculosis, and Malaria. PMI was founded in 2005, and has contributed to a decline in malaria death rates of close to 50%.

With suspension of funding, an estimated increase of 12.5-17.9 million malaria cases and 71,000-166,000 malaria deaths are expected this year. Already there are serious impacts on the supply chain for major malaria commodities as estimated by the Roll Back Malaria Partnership as seen on their RBM dashboard and supply chain gap estimates where six endemic countries have less than a 3-month supply of RDTs and eleven have less than a 6-month supply.
Prof Carlton ended by saying, “I think the hope is in science, right? The hope is in research. There are definitely new initiatives, new tools which are coming to the forefront, some of which I mentioned, and several of which we’re developing here at the malaria Research Institute. I do know the World Health Organization has got together with other countries to provide additional funding and support for those countries who have lost support through PMI.”
Advocacy &Announcement &Invest in Malaria Control &Research &World Malaria Day Bill Brieger | 09 Apr 2025
Prepare for World Malaria Day 2025
 The RBM Partnership to End Malaria has developed a communication kit to help plan for the upcoming World Malaria Day on April 25th. Below are some of the highlights and links they have shared.
The RBM Partnership to End Malaria has developed a communication kit to help plan for the upcoming World Malaria Day on April 25th. Below are some of the highlights and links they have shared.
To mark World Malaria Day 2025, the RBM Partnership to End Malaria in collaboration with World Health Organization (WHO) have developed a Messaging Framework and Social Media Toolkit to support partners and individuals in raising awareness and advocating for a malaria-free world.
Objectives for this year include…
- Re-energize efforts at all levels, from global policy to community action, to accelerate progress towards malaria elimination
- Advocate for increased investment in malaria control and elimination programs, including through stepped-up domestic financing and successful replenishments for the Global Fund and Gavi in 2025.
- Promote innovative strategies and approaches to tackle evolving challenges in malaria
- Prioritize country ownership, actively engage communities, and implement data-driven strategies
 The emphasis is on three pillars. First in REINVEST, which recognized that “Malaria control and elimination programs don’t just save lives – they’re also a smart economic investment for malaria-endemic countries and their international partners.”
The emphasis is on three pillars. First in REINVEST, which recognized that “Malaria control and elimination programs don’t just save lives – they’re also a smart economic investment for malaria-endemic countries and their international partners.”
The second pillar calls on us to REIMAGINE. We must Accelerate innovation by investing in the research and development of new and more effective antimalarial drugs, diagnostics, insecticides, vaccines and vector control methods” and turning that research into action.
 The third pillar is a call to REIGNITE based on “a renewed sense of urgency and commitment is needed to accelerate the fight against malaria.” This is called the “Big Push against malaria (and) is a multistakeholder effort to drive progress.”
The third pillar is a call to REIGNITE based on “a renewed sense of urgency and commitment is needed to accelerate the fight against malaria.” This is called the “Big Push against malaria (and) is a multistakeholder effort to drive progress.”
Follow the links to learn more and plan action.
Climate &Ecosystems &Elimination &Environment &Equity &Gender &Genetics &Monitoring &Mosquitoes &Research &Surveillance Bill Brieger | 25 Apr 2024
Drought, Malaria, and Climate Equity
The 2024 World Malaria Day Theme of “Gender, Health Equity, and Human Rights” cannot be divorced from the inequities of climate change wherein the countries that contribute the least to the problem suffer the most, including the deleterious effects of changing malaria geographics. The current severe drought in Zambia, Zimbabwe, and Malawi is a case in point.
 As a recent headline in VOA news states, “UN officials in Zambia to assess worst drought in 20 years.” The government has declared a drought officially where it “has affected a total of 8 provinces across the country with highest impacts in Southern, Central, Eastern, North-western, Western, and Lusaka Provinces.”
As a recent headline in VOA news states, “UN officials in Zambia to assess worst drought in 20 years.” The government has declared a drought officially where it “has affected a total of 8 provinces across the country with highest impacts in Southern, Central, Eastern, North-western, Western, and Lusaka Provinces.”
Drought should not be confused with a “normal” dry season. What we are seeing in Southern Africa now is an extended dry period in what should have been the rainy season. A study in Mali suggests that adult malaria-carrying mosquitoes “have endured the dry season by aestivating—the hot-weather equivalent of hibernating.” Unfortunately, an extended dry period of a drought may be more difficult to endure for the adults, but possibly the eggs are more resistant. Additional studies paint a more complicated picture.
Weather cycles intensify with climate change. El Niño, which can lead to droughts also produces warming in higher elevations so there tends to be an increase in malaria transmission in areas in the highlands.
Research in Zambia published just two years ago reported increasing trends of malaria in areas covering over 47% of all health facilities, while a declining trend was seen in areas covering 27% of health facilities. The decreasing trend was noticeable in the south, where malaria risk is lowest, and current drought conditions higher. The authors stress the need for continued geographic surveillance and implementation of control strategies geared to the conditions in each area.
A systematic review of the effects of climate change identified “vector borne disease (including malaria, dengue and West Nile Virus)” as a major concern as well as “nutrition-related effects (including general malnutrition and mortality, micronutrient malnutrition, and anti-nutrient consumption),” which compromises the ability of children to fight disease. The review found different impacts of drought ranging from increase mortality a year after a drought, to the disappearance of some vector species. The lesson is that each country needs to monitor their situation carefully. For Zambia, UNICEF reports that, “significant number are children, at risk of food insecurity, acute malnutrition, and disease.”
Research on drought effects on malaria arose from a study that examined the effects of drought on malaria infection (genetic) complexity and transmission in lizards (Plasmodium mexicanum and Sceloporus occidentalis). The authors noted that, “relationship between rainfall and parasite prevalence is somewhat more ambiguous.” Thus, the authors recommended that more information is needed about human malaria parasites and drought since “drought may cause shifts in human disease outcomes independent of any changes to prevalence.”
The United Nations challenges us by observing that, “Due to the complex relationship between malaria and climate change, gaps in knowledge still exist in the mechanisms of the linkage.” Changes in temperature, rainfall, and humidity need to be monitored for effects on vectors, parasites, and human movement. The current situation requires a more nuanced and complex approach to interventions if malaria elimination can be achieved while also preventing gender discrimination, promoting health equity and preserving human rights.
Elimination &Eradication &Health Systems &Helminths/Worms &ITNs &Journalists/Media &Leishmaniasis &NGOs &Nigeria &NTDs &Partnership &Repellent &Research &Schistosomiasis &Technical Assistance &Treatment Bill Brieger | 29 Sep 2020
Malaria News Today 2020-09-28/29: media involvement, NGOs, monitoring and research
A variety of malaria and related issues have arisen over the past two days. A media coalition for malaria elimination formed in Ghana. A Nigerian NGO stresses the importance of addressing malaria on Nigeria’s 60th Independence Day (October 1). An innovative technology foundation is supporting various malaria and NTD treatment and diagnostic research efforts. Click on links below to read the details.
Media Coalition for malaria control and elimination launched
A Media Coalition comprising of selected journalists and editors, has been launched in Ghana under the umbrella of the “Zero Malaria Starts with Me” campaign to eliminate malaria by 2030. The Coalition, which aimed to enhance the quality and quantity of malaria coverage, and support broader advocacy efforts, was launched at a workshop in Accra organized by the National Malaria Control Programme (NMCP), in collaboration with the African Media and Malaria Research Network and Speak Up Africa, an advocacy and communication Organisation based in Senegal.
The workshop brought together media personnel from across the regions, who nominated their Regional Executives, with two National Co-Chairpersons coming from Greater Accra. The Members of the Coalition, made a firm declaration of their commitment towards the elimination of malaria in Ghana by the year 2030, by championing the fight, taking responsibility for their roles through proactive, regular, accurate, and high-quality media output of news on malaria.
Chinwe Chibuike Foundation Set To Flag-off Full Scale Malaria Eradication Program On Independence Day
![]() A Nigeria indigenous and international non-governmental organization, envisioned to create a conducive environment towards the accessibility of healthcare facilities and improved educational opportunities, has joined the fight against the bizzare challenges of Malaria. The renowned Nigeria-USA humanitarian organization, Chinwe Chibuike Foundation is collaborating with other organizations to flagoff a full scale malaria eradication exercise tagged “Nigeria at 60 Malaria Eradication Project”, on the 1st of October 2020.
A Nigeria indigenous and international non-governmental organization, envisioned to create a conducive environment towards the accessibility of healthcare facilities and improved educational opportunities, has joined the fight against the bizzare challenges of Malaria. The renowned Nigeria-USA humanitarian organization, Chinwe Chibuike Foundation is collaborating with other organizations to flagoff a full scale malaria eradication exercise tagged “Nigeria at 60 Malaria Eradication Project”, on the 1st of October 2020.
According to the founder and President of Chinwe Chibuike Foundation, Ms Gloria Chibuike, during an interview session with Pulse TV few days ago, she noted the forthcoming Nigeria At 60 Malaria Eradication Program will be different and of more impact, especially with the full scale approach and introduction a new Malaria repellant Band.
While emphasizing on the extensive features of the project, Ms Gloria described Malaria as one of the biggest problems in Africa at the moment, considering the increased number of recorded deaths and infection. She narrated that the discovery of the new malaria repellent band was timely and off-course very efficient, especially with testimonies from few persons who have already tried the brand.
Drugs and Diagnostics: Malaria and NTDs
The Global Health Innovative Technology (GHIT) Fund announced today a total of 1.37 billion yen (US$13 million*) to invest in seven partnerships to develop new lifesaving drugs and diagnostics for malaria, Buruli ulcer, Chagas disease, leishmaniasis, schistosomiasis, and soil-transmitted helminths (STH). This includes three newly funded projects and four that will receive continued funding. The RBM Partnership is planning on how to monitor and provide technical support for ITN programs. Click the links within each section to read details.
As of September 29, GHIT’s portfolio includes 50 ongoing projects: 26 discovery projects, 16 preclinical projects and eight clinical trials (Appendix 3). The total amount of investments since 2013 is 22.3 billion yen (US$211 million).
Support the Improvement of Operational Efficiency of ITN Campaigns
The Alliance for Malaria Prevention (AMP) is a workstream within the RBM Partnership to End Malaria. With malaria indicators stagnating and intense pressure to improve access and use of effective ITNs, WHO has renewed focus on stratifying vector control strategies in countries. Along with the introduction of new, more expensive ITNs, countries are now challenged to determine where they should deploy different ITN types to manage insecticide resistance within limited funding envelopes, as well as to identify more efficient ways to implement mass ITN distribution.
 Countries that have accessed AMP technical assistance have significantly improved their capacity to modify and update strategies and tools to increase ITN access, use and accountability. They have also continued to identify further gaps and look for effective ways to address them. Now AMP planning to support update and finalization of ITN tracking tool, aligned with priorities across major partners (GF, PMI, RBM).
Countries that have accessed AMP technical assistance have significantly improved their capacity to modify and update strategies and tools to increase ITN access, use and accountability. They have also continued to identify further gaps and look for effective ways to address them. Now AMP planning to support update and finalization of ITN tracking tool, aligned with priorities across major partners (GF, PMI, RBM).
coronavirus &COVID-19 &Ebola &Elimination &iCCM &IPTi &IPTp &IRS &ITNs &Research Bill Brieger | 25 Apr 2020
Zero Malaria Starts after Lockdown?
 The novel 2019 coronavirus, also known as COVID-19 and SARS-COV2, is casting a heavy shadow over the 2020 World Malaria Day. People are trying to remain upbeat declaring the tagline “zero malaria starts with me,” but nothing can hide the fear that the current pandemic will both disrupt the current delivery of essential malaria preventive and treatment services, but will have longer term impacts on malaria funding and our capacity to learn new ways to reach malaria elimination goals. As we can see in the graphic to the right, accessible, lifesaving, community-based services may be especially hard hit.
The novel 2019 coronavirus, also known as COVID-19 and SARS-COV2, is casting a heavy shadow over the 2020 World Malaria Day. People are trying to remain upbeat declaring the tagline “zero malaria starts with me,” but nothing can hide the fear that the current pandemic will both disrupt the current delivery of essential malaria preventive and treatment services, but will have longer term impacts on malaria funding and our capacity to learn new ways to reach malaria elimination goals. As we can see in the graphic to the right, accessible, lifesaving, community-based services may be especially hard hit.
 Another ironic image is the indoor residual spray (IRS) team member with a face mask needed for protection from the insecticides being sprayed. When will such teams be able to go back into homes? When can household members actually pack out their belongings so that spraying can commence? When will such masks not be needed for intensive care COVID-19 case management instead?
Another ironic image is the indoor residual spray (IRS) team member with a face mask needed for protection from the insecticides being sprayed. When will such teams be able to go back into homes? When can household members actually pack out their belongings so that spraying can commence? When will such masks not be needed for intensive care COVID-19 case management instead?
WHO is urging “countries to move quickly to save lives from malaria in sub-Saharan Africa” because “New analysis supports the WHO call to minimize disruptions to malaria prevention and treatment services during the COVID-19 pandemic.” This will be difficult in high burden countries like Nigeria that are already on lockdown with over 1,000 coronavirus cases detected already. Modeling by WHO and partners has projected, “Severe disruptions to insecticide-treated net campaigns and in access to antimalarial medicines could lead to a doubling in the number of malaria deaths in sub-Saharan Africa this year compared to 2018.”
 The Global Malaria Program offers guidance for tailoring malaria interventions to the present circumstances. Great concern is drawn from previous epidemic situations when observing that, “it is essential that other killer diseases, such as malaria, are not ignored. We know from the recent Ebola outbreak in west Africa that a sudden increased demand on fragile health services can lead to substantial increases in morbidity and mortality from other diseases, including malaria. The COVID-19 pandemic could be devastating on its own – but this devastation will be substantially amplified if the response undermines the provision of life-saving services for other diseases.”
The Global Malaria Program offers guidance for tailoring malaria interventions to the present circumstances. Great concern is drawn from previous epidemic situations when observing that, “it is essential that other killer diseases, such as malaria, are not ignored. We know from the recent Ebola outbreak in west Africa that a sudden increased demand on fragile health services can lead to substantial increases in morbidity and mortality from other diseases, including malaria. The COVID-19 pandemic could be devastating on its own – but this devastation will be substantially amplified if the response undermines the provision of life-saving services for other diseases.”
Specifically, GMP recommends that national malaria programs should ensure the following:
- a focal point for malaria is a member of the National COVID-19 Incident Management Team.
- continued engagement with all relevant national COVID-19 stakeholders and partners.
- continued access to and use of recommended insecticide-treated mosquito nets (ITNs)
- continuation of planned targeted indoor residual spraying (IRS)
- early care-seeking for fever and suspected malaria by the general population to prevent a spike in severe malaria
- access to case management services in health facilities and communities with diagnostic confirmation through rapid diagnostic tests [RDTs]
- treatment of confirmed malaria cases with approved protocols
- continued delivery of planned preventive services normally provided to specific target populations (SMC, IPTi, IPTp)
- the safety of all malaria personnel and their clients in the process of carrying out the above interventions
 In editorial in the American Journal of Tropical Medicine and Hygiene by Yanow and Good address the damaging longer term impact of the present shutdown. “The impacts of research shutdowns will be felt long after the pandemic. Many scientists study diseases that do not share the same obvious urgency as COVID-19 and yet take a shocking toll on human life. For example, malaria infects more than 200 million people and takes the lives of nearly half a million people, mostly young children, each year.1 During laboratory closures and without clinical studies, there will be no progress toward treating and preventing malaria: no progress toward new drugs, vaccines, or diagnostics.”
In editorial in the American Journal of Tropical Medicine and Hygiene by Yanow and Good address the damaging longer term impact of the present shutdown. “The impacts of research shutdowns will be felt long after the pandemic. Many scientists study diseases that do not share the same obvious urgency as COVID-19 and yet take a shocking toll on human life. For example, malaria infects more than 200 million people and takes the lives of nearly half a million people, mostly young children, each year.1 During laboratory closures and without clinical studies, there will be no progress toward treating and preventing malaria: no progress toward new drugs, vaccines, or diagnostics.”
The case for continuing malaria services to save hundreds of thousands of lives is not difficult to make. The actual implementation during lockdowns and quarantines is a management challenge. The importance of malaria testing to provide patients with appropriate care for the right disease is crucial. The question is whether in resource strapped endemic countries these decisions and management arrangements can be made in a timely fashion and for the long term whether the next generation of research can proceed with much needed new medicines and technologies.
Case Management &coronavirus &COVID-19 &Research &water Bill Brieger | 31 Mar 2020
COVID19 Challenges for African Researchers
 Not surprisingly COVID-19 related travel restrictions and bans now occur throughout the world, and for African researchers, this means inability to travel for research related collaborations, planning meetings and conferences. Thus, it becomes necessary to ask, “What can we do here at home,” especially considering increasing restrictions on local movement and gatherings.
Not surprisingly COVID-19 related travel restrictions and bans now occur throughout the world, and for African researchers, this means inability to travel for research related collaborations, planning meetings and conferences. Thus, it becomes necessary to ask, “What can we do here at home,” especially considering increasing restrictions on local movement and gatherings.
In the very short time since COVID-19 was finally and officially recognized in China, many research articles have been published. Although these obviously focus on China, they raise possible research questions that need to be addressed in Africa, especially those countries still at the early stages of the epidemic.
Obviously, studies on the clinical management are needed, and one group of Chinese researchers are examining “biological products have broadly applied in the prevention and treatment of severe epidemic diseases, they are promising in blocking novel coronavirus infection,” especially based on reports from previous coronavirus experiences like SARS and MERS.[1] Other studies have examined the role of managing blood glucose levels[2], anticoagulant treatment[3] and the potential of antiviral treatment,[4] among others. What aspects of clinical management will become important to African patients’ survival?
 In the process of requesting adequate diagnostic, monitoring and treatment supplies and equipment generally for the country, the tertiary and research hospitals need to ensure they have made requests for the equipment and supplies that are needed not just to provide life-saving treatment, but also to test appropriate approaches in the local setting. Each setting is different and must be studied because already there are anecdotal reports of younger age groups being affected by severe disease in the USA compared to earlier reports from China.
In the process of requesting adequate diagnostic, monitoring and treatment supplies and equipment generally for the country, the tertiary and research hospitals need to ensure they have made requests for the equipment and supplies that are needed not just to provide life-saving treatment, but also to test appropriate approaches in the local setting. Each setting is different and must be studied because already there are anecdotal reports of younger age groups being affected by severe disease in the USA compared to earlier reports from China.
Taking a lesson from the Ebola epidemic in West Africa, there is need to study how COVID-19 will affect the delivery of health care, especially malaria services. Patrick Walker and colleagues[5] modeled the effects of health systems disruption on malaria including challenges in receiving based treatment when clinics were overwhelmed, seen as possible sources of disease and finally shut down as health workers themselves died. Outreach services like insecticide-treated net distribution were also stopped, and the efforts of community health workers were curtailed. To what extent is that happening with COVID-19?
Until there are proven drugs and vaccines, it is extremely important to learn about local epidemiology[6] in order to develop appropriate strategies to prevent the spread of COVID-19. This effort should involve researchers from many disciplines such as public health specialists, anthropologists, sociologists, educationists, and psychologists.
While the medical research mentioned above is carried out in hospitals and clinics, people conducting social and epidemiological studies ideally should be in the community where we can observe people washing their hands or not, gathering in groups or not, and finding out why they do these things. We need formative research to help develop health education, and at the same time ensure social and educational scientists can gather information to evaluate whether the health education as appropriate and worked.
Likewise, research is needed on health systems[7] and must involve political scientists, economists, public administrators, and of course public health specialists, also. A great danger exists for people who cannot keep a social distance from themselves such as those incarcerated in prison and living in camps for refugees and internally displaced people,[8] a common problem throughout the continent. They too need to get into the organizations and systems that provide care and learn what the policy makers and decision makers are thinking.
 As Bronwyn Bruton has observed,[9] “Some 40 percent of Africans live in water-stressed environments in which obtaining access to clean water—let alone soap—is an insurmountable daily hurdle, and for those populations, even simple measures to prevent the spread of the virus, such as frequent handwashing, will be out of reach.” In addition he asks difficult questions about what happens to children who are home and cannot go to school, the vast numbers of people in the informal economy who cannot rely on a salary, if they stay home, and the many people in conflict zones. These are questions that urgently need to be studied in Africa.
As Bronwyn Bruton has observed,[9] “Some 40 percent of Africans live in water-stressed environments in which obtaining access to clean water—let alone soap—is an insurmountable daily hurdle, and for those populations, even simple measures to prevent the spread of the virus, such as frequent handwashing, will be out of reach.” In addition he asks difficult questions about what happens to children who are home and cannot go to school, the vast numbers of people in the informal economy who cannot rely on a salary, if they stay home, and the many people in conflict zones. These are questions that urgently need to be studied in Africa.
Answers to our COVID-19 research questions are needed urgently, probably much sooner than funding can be found to support such research. The question for our African research colleagues is what can be done now with resources at hand in an environment where movement is restricted? We will definitely need speedy responses from our Institutional Ethics Review Boards and be creative in our use of research methods.
Roxana Elliott[10] reports that data collection in the diverse African region “is difficult, especially when measuring statistics such as mobile penetration, which require face-to-face data collection in order to include those who cannot be reached via mobile. Language barriers, lack of infrastructure, and the sheer number of people throughout Sub-Saharan Africa make collecting face-to-face data nearly impossible due to cost and time constraints, especially in rural areas.” She, therefore, suggests that mobile-based surveying methodologies can alleviate these issues. She also recommends a country-by-country approach, and hence we see that in 2017 an estimate of 32% of the population had a smartphone 48% a basic phone, and 20% no phone.
How can social and health researchers design studies using this mobile resource to answer vital COVID-19 questions in the nearest future? If our students are now at home, can they, for example, be contacted to observe, at a safe distance, the human health related actions in their communities? Can they interview family members to learn why people practice prevention or not? Can they relate family experiences seeking health services for suspected respiratory illness? Can they report on the water supply situation in the rural and urban areas where they are staying?
There are the questions which African colleagues can debate at a proper social distance (via phone, zoom, Skype, WhatsApp, and others), and come up with creative ways to find answers to prevent a worsening epidemic in Africa.
References
[1] Yan CX, Li J, Shen X, Luo L, Li Y, Li MY. [Biological Product Development Strategies for Prevention and Treatment of Coronavirus Disease 2019. Article in Chinese] Sichuan Da Xue Xue Bao Yi Xue Ban. 2020 Mar;51(2):139-145. doi: 10.12182/20200360506. (English abstract in PubMed).
[2] Ma WX, Ran XW. [The Management of Blood Glucose Should be Emphasized in the Treatment of COVID-19. Article in Chinese]. Sichuan Da Xue Xue Bao Yi Xue Ban. 2020 Mar;51(2):146-150. doi: 10.12182/20200360606.
[3] Tang N, Bai H, Chen X, Gong J, Li D, Sun Z.Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost. 2020 Mar 27. doi: 10.1111/jth.14817. [Epub ahead of print]
[4] Wu J, Li W, Shi X, Chen Z, Jiang B, Liu J, Wang D, Liu C, Meng Y, Cui L, Yu J, Cao H, Li L. Early antiviral treatment contributes to alleviate the severity and improve the prognosis of patients with novel coronavirus disease (COVID-19).J Intern Med. 2020 Mar 27. doi: 10.1111/joim.13063. [Epub ahead of print]
[5] Patrick G T Walker, Michael T White, Jamie T Griffin, Alison Reynolds, Neil M Ferguson, Azra C Ghani. Malaria morbidity and mortality in Ebola-affected countries caused by decreased health-care capacity, and the potential effect of mitigation strategies: a modelling analysis. www.thelancet.com/infection Published online April 24, 2015 http://dx.doi.org/10.1016/S1473-3099(15)70124-6
[6] Luan RS, Wang X, Sun X, Chen XS, Zhou T, Liu QH, Lü X, Wu XP, Gu DQ, Tang MS, Cui HJ, Shan XF, Ouyang J, Zhang B, Zhang W, Sichuan University Covid-ERG.[Epidemiology, Treatment, and Epidemic Prevention and Control of the Coronavirus Disease 2019: a Review. Article in Chinese]. Sichuan Da Xue Xue Bao Yi Xue Ban. 2020 Mar;51(2):131-138. doi: 10.12182/20200360505.
[7] Philip Obaji, Kim Hjelmgaard and Chris Erasmus Coronavirus infections in Africa are rapidly rising. Its weak health systems may buckle. USA Today. Updated 27 March 2020, Accessed 29 March 2020. https://www.usatoday.com/story/news/world/2020/03/27/coronavirus-africa-preparedness-rising-covid-19-infections/5076620002/
[8] Nick Turse. In West African Coronavirus Hotspot, War Has Left 700,000 Homeless and Exposed. The Intercept. March 26 2020, 5:33 p.m. https://theintercept.com/2020/03/26/burkina-faso-africa-coronavirus/
[9] Bronwyn Bruton. What does the coronavirus mean for Africa?. Atlantic Council. Tue, Mar 24, 2020. https://atlanticcouncil.org/blogs/africasource/what-does-the-coronavirus-mean-for-africa/
[10] Roxana Elliott. Mobile Phone Penetration Throughout Sub-Saharan Africa. GeoPoll (In Market Research, Tech & Innovation). Posted July 8, 2019 https://www.geopoll.com/blog/mobile-phone-penetration-africa/
Capacity Building &Costs &Research &Seasonal Malaria Chemoprevention &Surveillance &Treatment Bill Brieger | 04 May 2018
Multilateral Initiative for Malaria: Posters Range from Prevention to Cost to E-Learning and Beyond
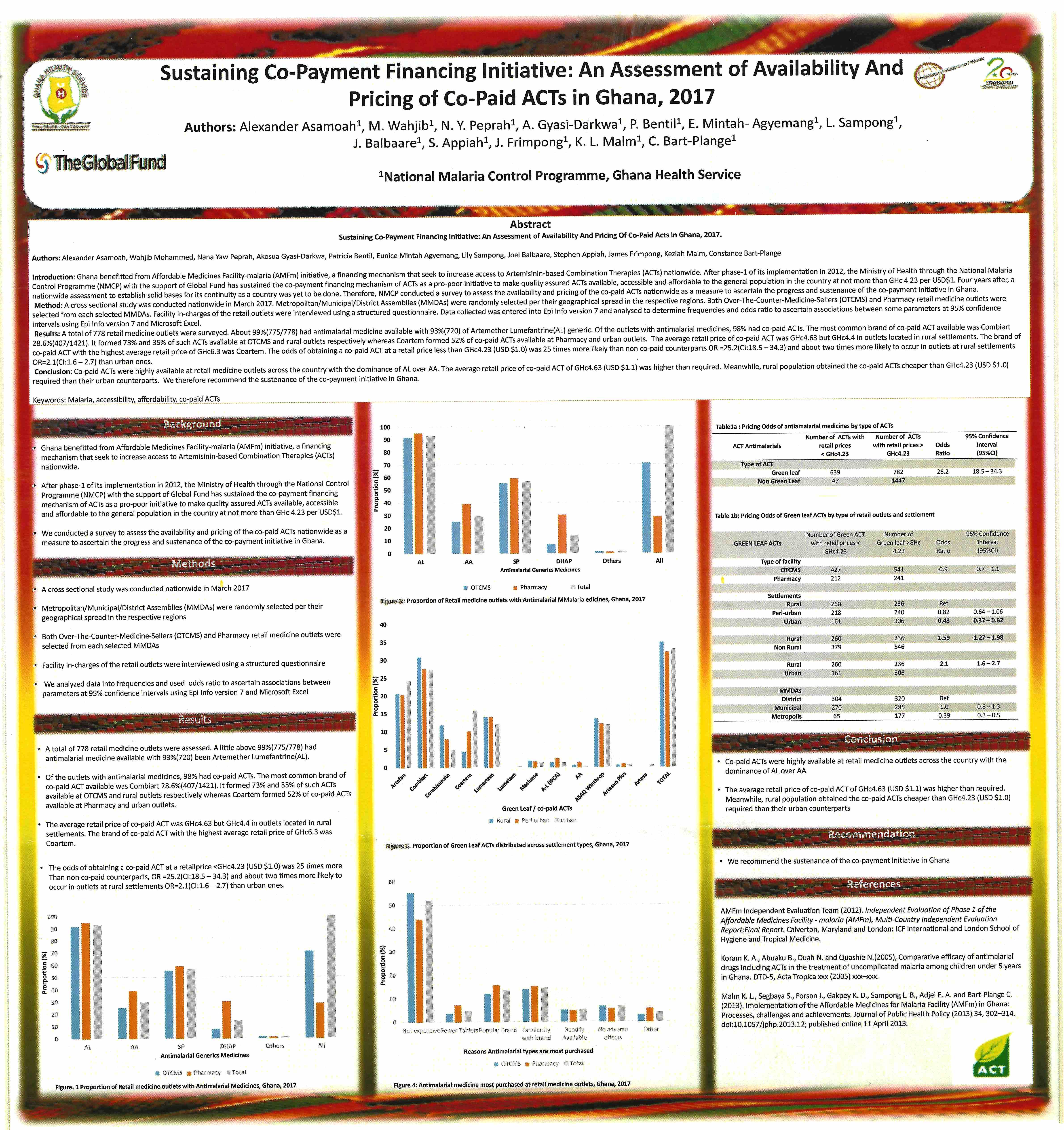
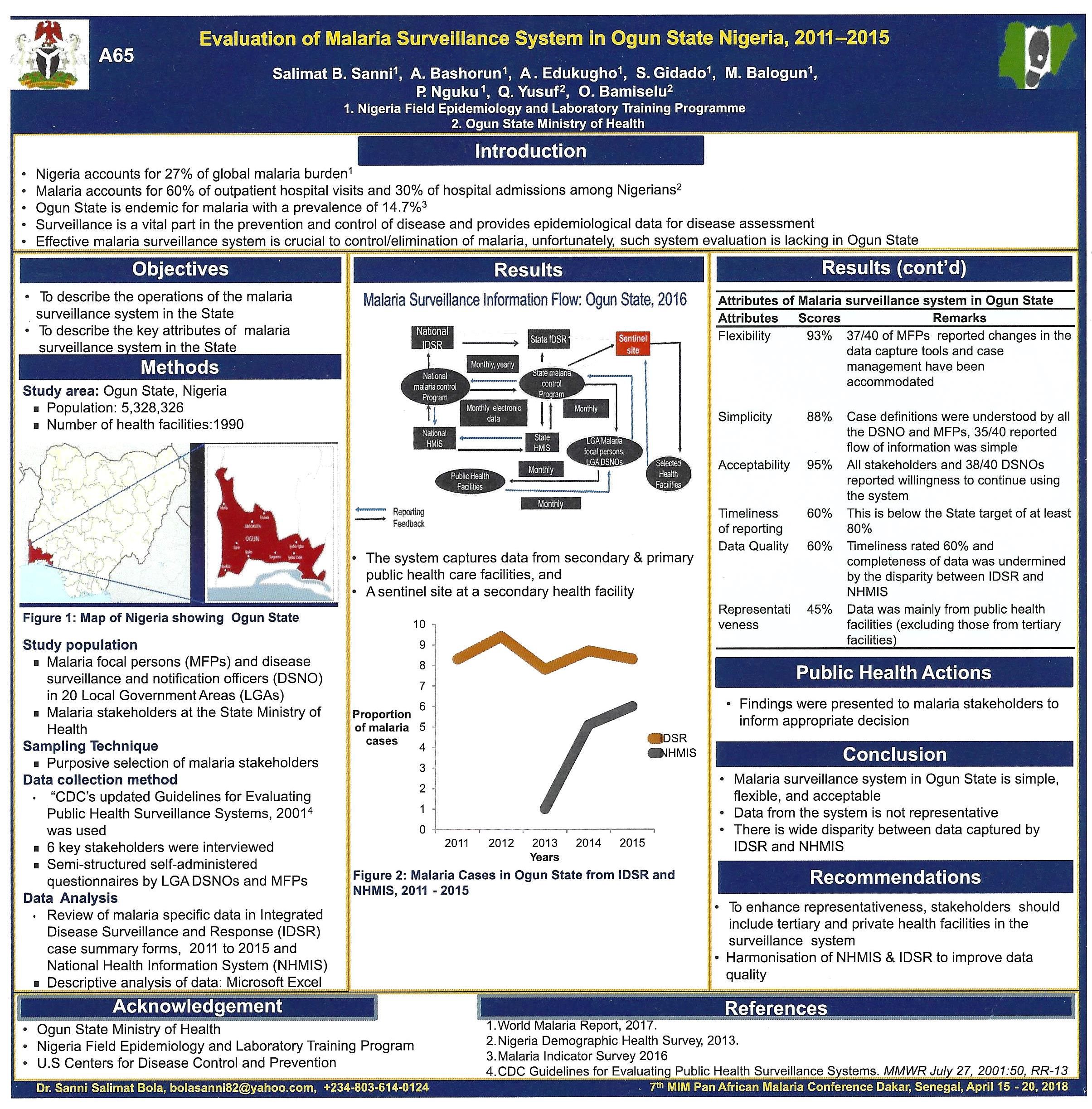
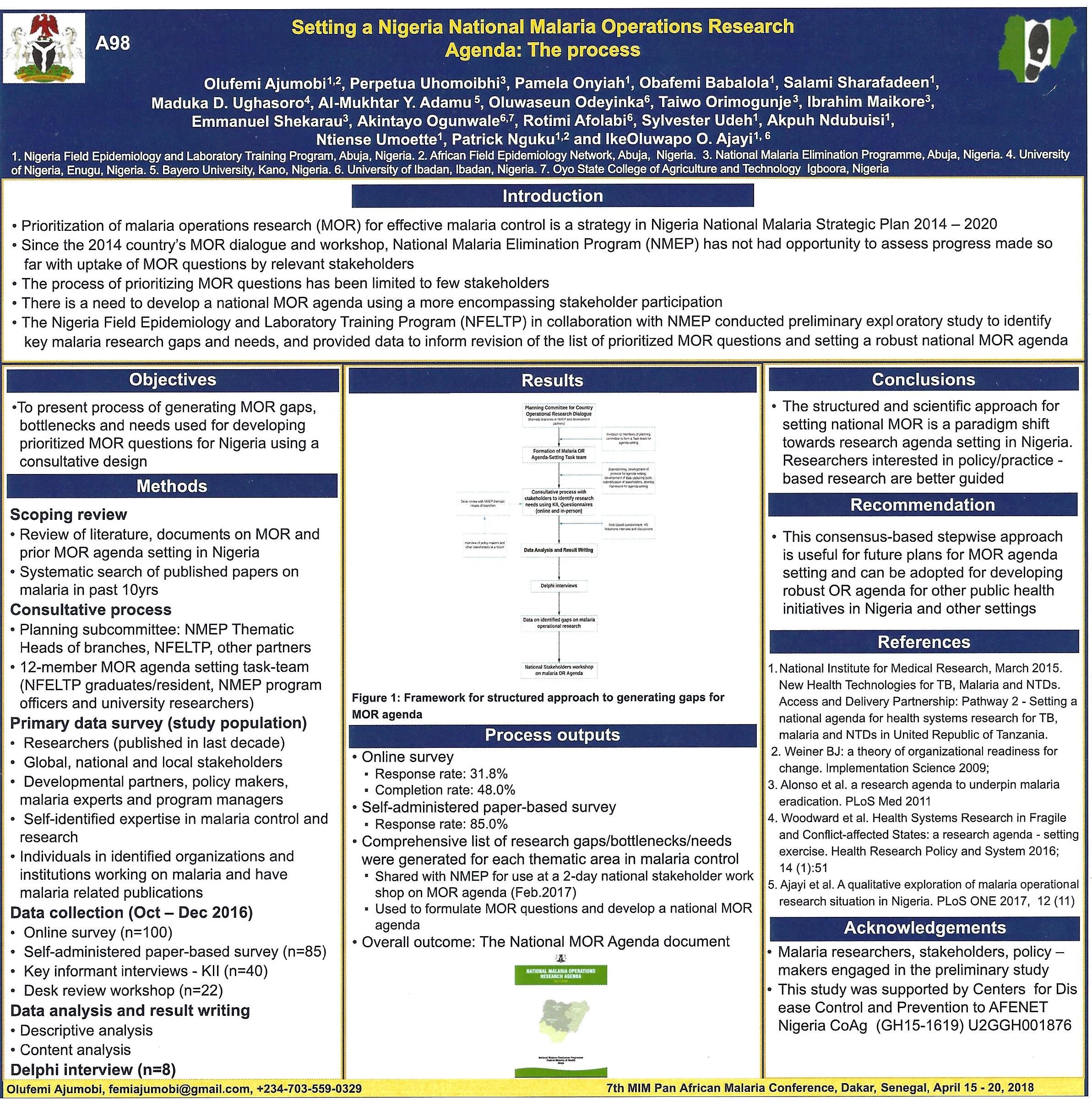
A major feature of all conferences are the poster sessions. These are often overlooked due to timing and placement. Fortunately at the recent 7th Multilateral Initiative for Malaria Conference in Dakar, tea breaks and lunch were made available in the poster tent ensuring more people came to view. Even so some people may have missed the valuable knowledge shared through this medium. We tweeted many of the posters during the event, but below are six posters in more detail.
These range from evaluating a malaria surveillance system to financing systems to sustain malaria drug supplies, including through community pharmacies. The potential of E-Learning for malaria capacity building was explored, and the process pf establishing a national malaria operations research agenda was presented. Several posters examined the seasonal malaria chemoprevention (SMC) program in the Sahel of West Africa including one from Mali as seen below.
Please contact the authors for additional information and updates. Readers who presented a poster at MIM are welcome to share their findings with us.



Capacity Building &Human Resources &Learning/Training &Research Bill Brieger | 19 Apr 2018
MIM – Fostering the next generation of malaria researchers in Africa – gaps and emerging opportunities
Dr Olumide Ogundahunsi of the of the Unicef-UNDP-World Bank-WHO Tropical Disease Research Program (best known as TDR) helped organize a symposium on the history and future goals of the Multilateral Initiative for Malaria (MIM) at the current MIM Conference. He describes the symposium, efforts to launch a MIM Society, and related issues below.
 Dakar is hosting the 7th Multilateral Initiative for Malaria (MIM) Pan Africa Malaria Conference 21 years after the first such gathering of malaria researchers in the city in 1997. At that time Northern research and development organizations including NIH/Fogarty, WHO/TDR, Wellcome Trust, SIDA and others sought to take measure of the malaria research experience and needs of African scientists and scientific institutions. It was challenging at that time to find strong and representative core of malaria researchers across the continent. Arising from that first conference was the development of MIM and a plan for building the capacity of African researchers through a series of malaria research grants that included both postgraduate training as well as support for applying the acquired skills in undertaking malaria research.
Dakar is hosting the 7th Multilateral Initiative for Malaria (MIM) Pan Africa Malaria Conference 21 years after the first such gathering of malaria researchers in the city in 1997. At that time Northern research and development organizations including NIH/Fogarty, WHO/TDR, Wellcome Trust, SIDA and others sought to take measure of the malaria research experience and needs of African scientists and scientific institutions. It was challenging at that time to find strong and representative core of malaria researchers across the continent. Arising from that first conference was the development of MIM and a plan for building the capacity of African researchers through a series of malaria research grants that included both postgraduate training as well as support for applying the acquired skills in undertaking malaria research.

Dr John Reeder, Director of TDR and Prof Fred Binka
Between 1997 and 2007 MIM supported Fifty six (56) research capacity strengthening (RCS) grants through the Special programme for research and training in Tropical diseases (TDR) for an aggregate amount of $12.9 million from 1997 to 2007. The grants responded to basic gaps in capacity, research tools/commodities/supplies and communication. The latter reflected a major need for researchers to connect with the global malaria research community to learn and share.
These grants under the aegis of the MIM/TDR task force on Malaria RCS addressed the following broad research themes: Pathogenesis and Immunology of Malaria, malaria vector control (including insecticide resistance), Chemotherapy and antimalarial drug resistance, research and development of new tools from natural products, and research to facilitate malaria control interventions. At the Symposium Representatives of the 56 MIM grantees from West, Central, East and Southern Africa shared experiences during and after completion of their MIM grant. These included –
- Professor Francine Ntoumi, Malaria immunology and pathogenesis research capacity in Central Africa, University Marien Ngouabi, Brazzaville, Republic of Congo
- Professor Lizette Koekemoer, Malaria vector research capacity in Africa, University of the Witwatersrand, Johannesburg, South Africa
- Professor Abdoulaye Djimde, Malaria treatment and antimalarial drug resistance in West Africa., Univerity of Bamako, Bamako, Mali
- Professor Wilfred Mbacham, Malaria treatment and antimalarial drug resistance in Central Africa, Univeristy of Younde 1, Younde, Cameroon
- Professor Kwadwo Koram, Malaria epidemiology research capacity for elimination and control in Africa, Noguchi Memorial Institute for Medical Research and University of Ghana, Accra, Ghana
These speakers demonstrate MIM’s and their own specific achievements in following areas:
- -Capacity built with infrastructure, technology transfer, skill acquisition and graduate students and postdocs trained (including their current status/subsequent contribution to malaria research and (or) control)
- -Resources/other grants leveraged
- -Collaborations established and sustained
- -Contributions to national and regional malaria research capacity, control and elimination.

MIM ‘alumni’ speaking at the Symposium
Since that time those receiving the MIM RCS were able to benefit from further TDR and other malaria research grants and in the process have themselves helped develop new generations of malaria scientists in the universities and institutes where they work. MIM has continued to address the original research gaps. The holding of six subsequent Pan-African conferences. Grants were also provided for establishing satellite communications systems at three institutions where grantees were based.
Participants in this process who attended the current conference (MIM2018) were able to help achieve on of the objectives of the symposium that is “highlighting the importance of continuous investment in training and monitoring of young African scientists.” The symposium also articulated the unmet and emerging gaps in research capacity of particular relevance to malaria control and elimination.

Visiting the TDR booth to discuss MIM experiences and research opportunities
MIM started and continues as a partnership among Northern and African research organizations with a rotating secretariat. For the past 10 years the MIM secretariat has been based in Africa, and most recently in Cameroon in the Biotechnology Centre of the University of Yaoundé.
Going forward the MIM is evolving into the MIM Society, a broad-based society which will focus among others on organizing regular MIM conferences, promoting research capacity strengthening and foster and unite the different initiative on the continent and worldwide. The MIM society will also invigorate the young African scientist to emerge as outstanding researchers and leaders with ground breaking innovation in science and its applications to development.
The MIM Society will be a global non-profit organization whose mission is to unite all human resources, young and experienced, working on malaria (from researchers over implementers, teachers, producers, funders, policy makers) to strengthen and sustain the capacity of malaria affected countries and to be an umbrella organization for all malaria related initiatives. The MIM Society through its members will guarantee capacity building goals for malaria researchers set by MIM 20 years ago will be carried forward for another 20 years and more.
Diagnosis &Research Bill Brieger | 10 Nov 2016
Urine Rapid Diagnostic Test for Malaria: Results Published
Results of testing the innovative Urine Rapid Diagnostic Test for Malaria developed by Fyodor Biotech have been published in the Journal of Clinical Microbiology. Authors from multiple collaborating institutions include Wellington A. Oyibo, Nnenna Ezeigwe, Godwin Ntadom, Oladipo O. Oladosu, Kaitlin Rainwater, Wendy O’Meara, Evaezi Okpokoro, and William Brieger. The abstract appears below.
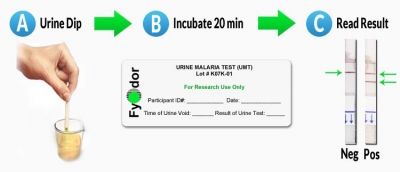 Background: The need to expand malaria diagnosis alongside policy requirements for mandatory testing before treatment motivates exploration of non-invasive rapid diagnostic tests (RDTs). We report the outcome of the first cross-sectional, single-blind clinical performance evaluation of a Urine Malaria Test (UMT) for Plasmodium falciparum (Pf) malaria diagnosis in febrile patients.
Background: The need to expand malaria diagnosis alongside policy requirements for mandatory testing before treatment motivates exploration of non-invasive rapid diagnostic tests (RDTs). We report the outcome of the first cross-sectional, single-blind clinical performance evaluation of a Urine Malaria Test (UMT) for Plasmodium falciparum (Pf) malaria diagnosis in febrile patients.
Methods: Matched urine and fingerprick blood from participants ?2 years with fever (axillary temperature ?37.5°C) or history of fever in the preceding 48 hours were tested with UMT and microscopy (as gold standard). BinaxNOW® (Pf/Pan) blood RDT was done to assess relative performance. Urinalysis and Rheumatoid Factor (RF) tests were conducted to evaluate possible interference. Diagnostic performance characteristics were computed at 95% CI.

UMT is winner of innovations prize
Results: Of 1,800 participants screened, 1,691 were enrolled; 566 (34%) were febrile, 1,125 (66%) afebrile; test positivity among enrolled participants: 341 (20%) by microscopy, 419 (25%) UMT, 676 (40%) BinaxNow Pf and 368 (22%) BinaxNow Pan. UMT sensitivity among febrile patients (for whom the test is indicated) was 85% and specificity 84%. Among febrile children ?5 years, UMT sensitivity was 93%, specificity 83%. Area under receiver-operator characteristic curve (AUC) of UMT (0.84) was not significantly different from Binax Pf (0.86) or Binax Pan (0.87), indicating that the tests do not differ in overall performance. Gender, seasons, and RF did not impact UMT performance. Leukocytes, hematuria and urobilinogen concentration in urine were associated with lower UMT specificity.
Conclusion: UMT performance was comparable to BinaxNOW Pf/Pan tests, and is a promising tool to expand malaria testing in public and private healthcare settings where there are challenges to blood-based malaria diagnosis testing.
Funding &Research Bill Brieger | 24 Jun 2016
Malaria Plus Brexit – let’s hope no Malexit
 No one knows for certain the full implications of Britain’s narrow vote to leave the European Union (EU). Since Britain has been a major player in malaria research and development aid, questions naturally arise of whether the British exit (Brexit) from the EU will affect development aid and global research generally and malaria aid and research specifically.
No one knows for certain the full implications of Britain’s narrow vote to leave the European Union (EU). Since Britain has been a major player in malaria research and development aid, questions naturally arise of whether the British exit (Brexit) from the EU will affect development aid and global research generally and malaria aid and research specifically.
Earlier this week the Brookings Institution examined the ways that a Brexit could affect Africa. Here are some of the possibilities adapted to malaria –
- Volatility in the global economic market will affect not only the British economy but also those of malaria endemic countries, possibly reducing the reducing available funds for national contributions to malaria control at home, a major goal for sustaining malaria control and elimination
- Britain specifically may not be able to sustain its financial contributions to malaria aid through the Global Fund, bilateral malaria programs and of course it would no longer contribute to the European Development Fund which currently stands at nearly 15% of its total.
- The British economy which like all modern nations depends on trade would be affected by the need to renegotiate hundreds of trade agreements around the world. Less trade likely means less income and less development aid.
In both 2014 and 2015 the United Kingdom contributed 8% of the total contributions received by the Global Fund to fight HIV, TB and Malaria. In addition “UK’s official development assistance (ODA) is expected to rise to £11.3bn when it hits the 0.7% target. With a population of about 63 million, the figure works out at roughly £137 per Brit.” In 2012 the malaria component was estimated at 2%.
Patrick Vallance and Tim Wells examine the importance of global collaboration on malaria research. This requires the free flow of researchers and their needed supplies across national borders, especially malaria research that has had to date a pan-European character. They describe the collaboration needed “between commercial and non-profit organizations, and between academic science and medicine. Without such partnerships, advances in fighting this deadly disease would not have been possible.”
Vallance and Wells give the example of “GSK’s research site in Tres Cantos, Spain. The lab operates with the support and advice of a broad range of actors, including GSK, the Wellcome Trust, the European Union, and MMV (Medicines for Malaria Venture), as well as various other product-development partnerships and academic centers.” Such efforts may be jeopardized when permits for malaria scientists to work in other countries are more difficult to obtain.
There may be other aid mechanisms too, the Commonwealth Secretariat being one. During World Malaria Day in 2012 the Commonwealth Secretariat pledged to assist in sustaining the gains made in tackling malaria. We hope that Brexit will not become an exit for malaria commitments and saving lives.