Health Systems &Human Resources &Integration &Malaria in Pregnancy Bill Brieger | 02 Nov 2014
Improved Malaria Services in Malawi: Jhpiego and USAID at ASTMH
 Monday afternoon (3 October 2014) at the American Society for Tropical Medicine and Hygiene Annual Meeting in New Orleans, Jhpiego and USAID/PMI are sponsoring a panel on “Integrating and Innovating: Strengthening Care for Mothers and Children with Infectious Diseases.” If you are at the meeting please attend to learn more about our Malaria activities in Malawi.
Monday afternoon (3 October 2014) at the American Society for Tropical Medicine and Hygiene Annual Meeting in New Orleans, Jhpiego and USAID/PMI are sponsoring a panel on “Integrating and Innovating: Strengthening Care for Mothers and Children with Infectious Diseases.” If you are at the meeting please attend to learn more about our Malaria activities in Malawi.
One of the panel presentations is “Improving Malaria Outcomes in Malawi: Focusing on Integration of Services at all Levels” presented by John Munthali, Senior Technical Advisor, Jhpiego/Malawi. John works with Support for Service Delivering Integration-Services (SSDI-S), a USAID bilateral program (2011-2016) with Partnerships in 15 Districts involving the Ministry of Health, Jhpiego, Save the Children International, Care Malawi and Plan International.
 SSDI-Services focuses on Malawi’s Essential Health Package (EHP) Focal Areas with particular emphasis on Maternal Health, Newborn and Child Health, Family Planning and Reproductive Health, HIV/AIDS and TB, Nutrition and Malaria. Aspects of the Malaria Component include Intermittent Preventive Treatment and Insecticide Treated Bed Nets
SSDI-Services focuses on Malawi’s Essential Health Package (EHP) Focal Areas with particular emphasis on Maternal Health, Newborn and Child Health, Family Planning and Reproductive Health, HIV/AIDS and TB, Nutrition and Malaria. Aspects of the Malaria Component include Intermittent Preventive Treatment and Insecticide Treated Bed Nets
SSDI-S is based on Promotion of the continuum of care from household to hospital. Health Facility Approaches address Improved Technical Capacity of Health Workers, Functional Health Facility, and Data-informed Decision Making. Community Approaches involve Improved Technical Capacity of CHWs, Functional Village Clinics, and Community Mobilization. Integration is a major concern such that there are no missed opportunities of EHP services at all levels.
Positive Trends since have been seen since Inception. Malaria in Pregnancy interventions supported the National Malaria Control program to review the Malaria in Pregnancy guidelines and training manuals to adopt the new WHO policy recommendations. 74 Trainers were trained in all 15 districts. MNCH services were established in selected districts. 344 HSAs were trained. 70 community-based Core Groups oriented on MNCH. SSDI supported ongoing MNCH activities through review meetings and distribution of reporting forms.
 As a result of these integrated high impact interventions there has been a remarkable increase in the uptake of IPTp 2 (16% in June 2012 to 64% in Sept. 2013) by pregnant women in the SSDI-services focus districts. Central to this increase is the integration of services at the facility level where malaria has been highly integrated into maternal, newborn and child health. The project has also seen IPTp 1 uptake maintained at above 91% in all the 15 districts
As a result of these integrated high impact interventions there has been a remarkable increase in the uptake of IPTp 2 (16% in June 2012 to 64% in Sept. 2013) by pregnant women in the SSDI-services focus districts. Central to this increase is the integration of services at the facility level where malaria has been highly integrated into maternal, newborn and child health. The project has also seen IPTp 1 uptake maintained at above 91% in all the 15 districts
Malaria Care capacity building has resulted in improved iCCM services delivered by Health Surveillance Assistants (HSAs) at village clinics. iCCM is serving as the foundation for community-based treatment of malaria by HSAs while at facility level IMCI provides an integrated approach to manage childhood illnesses including malaria.
In conclusion, it is feasible to integrate MNCH programs at all levels using SBCC and Systems Strengthening. Having an integrated project looking at the whole spectrum of health services (system strengthening, service delivery and behavior change) can help improve programming & service delivery.
Health Systems &Malaria in Pregnancy Bill Brieger | 01 Nov 2014
Jhpiego Malaria Team at the American Society of Tropical Medicine & Hygiene Conference
Jhpiego’s Malaria Team is co-hosting a symposium on Malaria in Pregnancy and presenting several posters at the upcoming ASTMH 2014 annual meeting in New Orleans, 2-6 November. Below is an outline of these events for those who may be in attendance. Jhpiego also will have a booth in the Exhibition area – please visit it.
Symposium: Integrating and Innovating: Strengthening Care for Mothers and Children with Infectious Diseases, 1:45 – 3:30 p.m., Marriott – Mardi Gras Ballroom D (Third Floor): Co-Faciliators: Elaine Roman, Jhpiego | Erin Eckert, USAID/ PMI
- Improving Malaria Outcomes in Malawi: Focusing on Integration of Services at all Levels, John Munthali, Jhpiego, Malawi
- Performance Quality Improvement Lending to Corrected Documented Outcomes for Intermittent Preventive Treatment in Kenya, Muthoni Kariuki, Jhpiego, Kenya
- The provision of HIV and IPTp Services in Antenatal Care in Malawi: Views of Health Care Providers from a Qualitative Study, P. Stanley Yoder
- Mothers and Mycobacteria: Implications of the Intersection of TB, Pregnancy, and Maternal and Newborn Health, Charlotte Colvin
- Wrap-up: The Growing Role of Infectious Disease in Maternal Mortality Reduction: How to Attain the Post-MDG targets, Allisyn Moran
![]()
Poster Sessions:
Poster Session A: Monday 12:00 – 1:45 p.m., Marriott Grand Ballroom (Third Floor)
- Quality Inspired Project – A Key to Achieving Results with Malaria Interventions, Grace Qorro, Jhpiego Tanzania
- Prevention of Malaria in Pregnancy: Community Health Volunteers (CHVs) Promote Community-based Activities to Increase Uptake of Intermittent Preventive Treatment of Malaria in Pregnancy (IPTp) in Kenya, Augustine Ngindu, Jhpiego Kenya
Poster Session B: Tuesday 12:00 – 1:45 p.m., Marriott Grand Ballroom (Third Floor)
- Improving Maternal and Neonatal Health: Complementary Role of the Private Sector Increasing Uptake of Intermittent Preventive Treatment for Malaria in Pregnancy in Kenya, Augustine Ngindu, Jhpiego, Kenya
Poster Session C: Wednesday 12:00 – 1:45 p.m., Marriott Grand Ballroom (Third Floor)
- Expanding Health Ministry Capacity to Deliver Malaria and Other Health Commodities at the Community Level in Nigeria, Bright Orji, Jhpiego, Nigeria
Health Systems &Malaria in Pregnancy Bill Brieger | 28 Jul 2014
Attending Antenatal Care Does Not Guarantee Antimalaria Services
A new article by Clementine Rossier and colleagues compares access to maternal health services in Ouagadougou, Burkina Faso and Nairobi Kenya. In both settings a very large proportion of pregnant women registered for antenatal care (ANC). Twice the proportion of Nairobi women (47%) attended up to four times compared to those in Ouadougou (22%). In both settings, the likelihood of attending four ANC visits increased with educational level of the women.
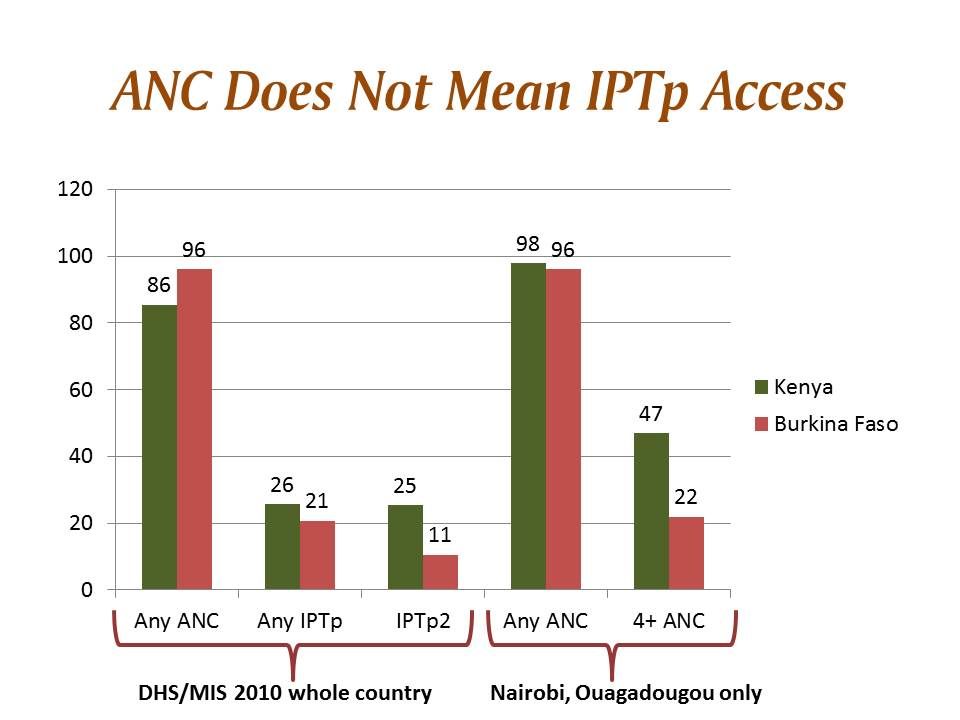 Although the article does not discuss services received at ANC, we can consider the implications for malaria in pregnancy (MIP) control since ANC is a major platform for MIP service delivery. Here the demographic and health survey (DHS) and its malaria indicator survey (MIS) component are of help. Both countries had a national survey in 2010 (their most recent).
Although the article does not discuss services received at ANC, we can consider the implications for malaria in pregnancy (MIP) control since ANC is a major platform for MIP service delivery. Here the demographic and health survey (DHS) and its malaria indicator survey (MIS) component are of help. Both countries had a national survey in 2010 (their most recent).
Interestingly in 2010 Burkina Faso overall had better ANC registration (05%) than Kenya (86%). In neither country was intermittent preventive treatment in pregnancy (IPTp) coverage good. 25.7% of pregnant women in Kenya received one dose of sulfadoxine-pyrimethamine for IPTp, while 20.8% did so in Burkina Faso. IPTp2 coverage in Kenya was similar at 25.4%, but in Burkina Faso it dropped to 10.6%
 The important lesson here is that even with good ANC registration, women have no guarantee of receiving life saving malaria prevention services. If registration was lower we might suspect issues of local beliefs and other community barriers, but the situation in both countries points to health systems failures like inadequate drug supplies and health worker lapses.
The important lesson here is that even with good ANC registration, women have no guarantee of receiving life saving malaria prevention services. If registration was lower we might suspect issues of local beliefs and other community barriers, but the situation in both countries points to health systems failures like inadequate drug supplies and health worker lapses.
The service delivery situation in both countries has changed dramatically since 2010. Kenya has refined its malaria map and is focusing IPTp on areas of stable and high transmission. Burkina Faso has received greater influx of financial support from the Global Fund and the US Agency for International Development. Hopefully the 2014 DHS/MIS studies currently in progress in both countries will paint a better picture. Of course, unless health systems issues are being addressed, funding alone will not solve the malaria service gaps.
Congenital Malaria &IPTp &ITNs &Malaria in Pregnancy &Mortality Bill Brieger | 12 Jun 2014
Congenital Malaria, an Underappreciated Neonatal Problem
The largest portion of infant deaths occurs in the neonatal period. During those first 28 days, the child is at risk from a variety of problems arising from delivery complications, infections and simply not being kept warm.
 In malaria endemic areas there is the small but important problem of malaria transferred from mother to child, or congenital malaria. The problem occurs with both Plasmodium vivax and falciparum.
In malaria endemic areas there is the small but important problem of malaria transferred from mother to child, or congenital malaria. The problem occurs with both Plasmodium vivax and falciparum.
Congenital malaria in the newborn is often hard to detect. There may be fever, but other signs and symptoms might include anaemia, jaundice, paleness, diarrhoea, vomiting, and general weakness.
Prevalence of congenital malaria in Ghana, for example, ranged from 2% by microscopy to 12% using polymerase chain reaction (PCR). In India microscopy revealed a prevalence of 3% with cases of both vivax and falciparum.
One would hope this problem could be avoided if prevention of malaria in pregnancy was practiced using insecticide treated nets, intermittent preventive treatment (IPTp) and prompt and appropriate case management, but studies still find placental and cord parasiteamia in countries where such interventions are supposed to be integrated into antenatal/prenatal care. In Colombia, “An association was found between congenital malaria and the diagnosis of malaria in the mother during the last trimester of pregnancy or during delivery, and the presence of placental infection.”
Countries are in the process of shifting to the relatively new WHO guidance on IPTp that encourages monthly doses of sulfadoxine-pyrimethamine from the beginning of the second trimester up until delivery. Countries are also trying to ensure universal coverage of ITNs so that women will be using nets prior to even becoming pregnant.
We still have trouble administering to take just two doses of IPTp, but if we want to prevent congenital malaria, we need to ensure that women are protected from malaria in their placentas and are free from parasites right up until they give birth and thereby prevent another cause of neonatal mortality.
ITNs &Malaria in Pregnancy Bill Brieger | 26 May 2014
Women’s Education and Bed Net Use in Nigeria
Concern about women’s and girl’s education in Nigeria and worldwide has peaked with the abduction of around 300 female secondary school school students in northeastern Nigeria. Normally we see many positive benefits of women’s education in various health indicators, but it appears that bednet use does not follow that trend neatly.
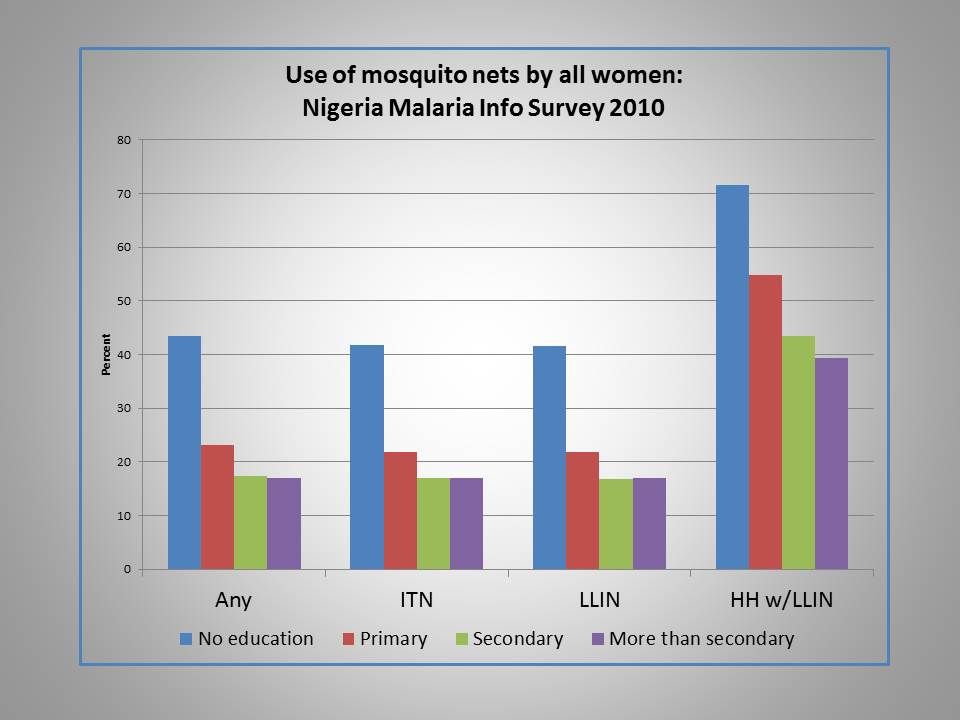 Analysis of bednet use in the Nigeria Malaria Indicator Survey (MIS) of 2010 found that ironically net use of all kinds, including ordinary nets, insecticide treated nets and long lasting insecticide-treated nets actually decreased as educational level of women increased.
Analysis of bednet use in the Nigeria Malaria Indicator Survey (MIS) of 2010 found that ironically net use of all kinds, including ordinary nets, insecticide treated nets and long lasting insecticide-treated nets actually decreased as educational level of women increased.
Interestingly the same picture is painted for levels of wealth with 41% in the lowest quintile using any kind of net the night before the survey versus 16% for the highest quintile. Also of note, 19% of urban women reported using any kind of net versus 34% in the rural areas.
In contrast the 2010 Nigerian MIS found that only 22% of women without education had received any antenatal care (ANC) during a recent pregnancy compared to 89% with greater than secondary education. Getting at least two doses of intermittent preventive treatment (IPTp) during ANC was only 7% for those without formal education, but 24% for those with higher than secondary education. Why does bednet use show a reverse trend here?
One factor may be the delivery mechanism. ANC and IPTp require utilization of a service with all the economic and intra-family dynamics that this implies. Nets have so far been mainly provided during outreach campaigns. Is there an element of equity going on here with an effort to reach the less educated and poorer segment of society with nets?
Also educated people and those with relatively greater wealth may have better housing conditions that are less likely to encourage mosquito entry. Such families may perceive that they have less need for nets if they actually have ceilings and windows with netting.
Just by way of comparison, a similar picture of net use was was seen in the Malawi MIS of 2012. That survey only recorded three levels of education and the contrast between highest and lowest use was only about 10% points compared to 25% difference in Nigeria.
Colleagues have recently documented gaps in net access and use across many countries. We need to ensure not only that nets reach a house, but that adequate numbers of nets are available for universal coverage (UC = at least one for every two residents – though this adequacy calculation depends on cultural sleeping patterns).
Malaria control efforts since 2009 have been aiming at UC, but various surveys have shown this goal to be elusive, let alone sustainable, since nets need to be replaced every 2-3 years. It is encouraging if some element of equity might underlie net distribution, but we still need to learn more about why people get and use nets or alternatives to ensure that all women and other household members are truly protected from malaria.
Burden &Malaria in Pregnancy &NCDs Bill Brieger | 16 May 2014
Malaria, Hypertension and Pregnancy: where communicable and non-communicable diseases may cross paths
 Tomorrow, May 17th, is World Hypertension Day. Much attention of recent has been focused on the importance of non-communicable diseases (NCDs) like hypertension in terms of global burden, and concerns have been expressed that communicable or infectious diseases (CDs) may become neglected, although they still cause huge levels of morbidity and mortality. What people may not realize is that there are connections between the NCDs and the CDs.
Tomorrow, May 17th, is World Hypertension Day. Much attention of recent has been focused on the importance of non-communicable diseases (NCDs) like hypertension in terms of global burden, and concerns have been expressed that communicable or infectious diseases (CDs) may become neglected, although they still cause huge levels of morbidity and mortality. What people may not realize is that there are connections between the NCDs and the CDs.
 Better research is needed to document the relationships and influences of one on the other, but some preliminary work has been done with pregnant women who are susceptible to both hypertension and malaria. What does that combination do?
Better research is needed to document the relationships and influences of one on the other, but some preliminary work has been done with pregnant women who are susceptible to both hypertension and malaria. What does that combination do?
What the existing literature implies so far is that malaria in pregnancy may in fact be associated with hypertension in some cases and that both conditions can lead to intra-uterine growth retardation and low birth weight. Also boys who were born to mothers with malaria in pregnancy had excess hypertension in their first year of life and girls had higher SBP.
 The role of malaria in pregnancy in low birth weight is well established. Furthermore Lackland and colleagues shared that, “there have been numerous ecologic and observational studies that identified significant inverse associations of birth weight with blood pressure levels at various ages in later life.” A graphic posted to the right shows potential malaria and hypertension interactions. These are areas that deserve more observation, documentation and research.
The role of malaria in pregnancy in low birth weight is well established. Furthermore Lackland and colleagues shared that, “there have been numerous ecologic and observational studies that identified significant inverse associations of birth weight with blood pressure levels at various ages in later life.” A graphic posted to the right shows potential malaria and hypertension interactions. These are areas that deserve more observation, documentation and research.
Overall we can see that there is not a real dichotomy between CDs and NCDs, and both interact in the health of individuals, families and communities.
IPTp &Malaria in Pregnancy Bill Brieger | 19 Apr 2014
Finding a Practical Approach to Folic Acid Supplementation and Intermittent Preventive Treatment of Malaria for Pregnant Women
 n 2012 the World Health Organization’s Global Malaria Program reconfirmed the use of intermittent preventive treatment for pregnant women (IPTp) using sulfadoxine-pyrimethamine (SP). IPTp now may be given at each antenatal care (ANC) visit after the first trimester as long as it is a month since the last dose.
n 2012 the World Health Organization’s Global Malaria Program reconfirmed the use of intermittent preventive treatment for pregnant women (IPTp) using sulfadoxine-pyrimethamine (SP). IPTp now may be given at each antenatal care (ANC) visit after the first trimester as long as it is a month since the last dose.
Countries have been moving forward in reviewing and adapting/adopting this guidance where appropriate. One of the key challenges countries have faced is what to do about folic acid, which is given concurrently with IPTp as part of focused ANC. Specifically the guidance states … WHO recommends the administration of folic acid at a dose of 0.4 mg daily; this dose may be safely used in conjunction with SP. Folic acid at a daily dose equal or above 5 mg should not be given together with SP as this counteracts its efficacy as an antimalarial.
This new low dose formulation of folic acid requires accessible and affordable supplies made available through a country’s pharmaceutical procurement system. Manufacturers would need to adjust, and national food and drug approval agencies would need to register the product(s).
All this worry may in fact be a case of closing the barn door after the horses have escaped. Since in many countries women do not register for antenatal care until well into their second trimester, the benefits of folic acid supplementation may in fact me missed. A broader view of the health and nutrition of women of reproductive age is needed, not just the narrow focus of giving folic acid as part of ANC.
The online encyclopedia of Medline explains that “There is good evidence that folic acid can help reduce the risk of certain birth defects (spina bifida and anencephaly). Women who are pregnant or planning to become pregnant should take at least 400 micrograms (mcg) of a folic acid supplement every day.” Let’s look at the term “planning to become pregnant.” This means that women of reproductive age (WRA) who are interested in having children need to ensure that taking folic acid. Since many pregnancies are not “planned” this means folic acid should be a regular part of their lives.
How can this be achieved? First, while it may not be practical, WRA could take regular folic acid tablets. A variety of health and social programs, including secondary schools for those who attend, may be venues to try distribution of supplements. Secondly there are food sources, and thirdly there could be fortification of commercial foods with folic acid.
Again the Medline encyclopedia informs us that, “Folate occurs naturally in the following foods: dark green leafy vegetables, dried beans and peas (legumes), and citrus fruits and juices.” These items are often available in malaria endemic countries and part of a normal diet. Of course, as the American Journal of Clinical Nutrition points out, “Naturally occurring seasonal variations in food consumption patterns have a profound effect” on the availability, cost and use of these food sources.
While commercial food fortification is common in industrialized countries, IRIN also points out that, “use local manufacturers and commercial distribution systems to reach undernourished children in Nigeria, Ghana and Tanzania. All three countries have mandatory fortification of wheat flour with iron and zinc.” Why not add folic acid? Researchers in Kenya found that “Locally available indigenous foods can be used in the formulation of acceptable, low-cost, shelf-stable, nutritious supplementary foods for vulnerable groups,” including folic acid fortification.
We should now focus our attention of the folic acid needs of WRA generally. We must plan for the three possible interventions mentioned above as appropriate to each country and as an ongoing effort to ensure women’s overall health and nutrition. If we succeed, women in malaria endemic countries will enter pregnancy with a strong foundation of folic acid supplementation and not have to depend solely on tablets during the short window when they attend ANC.
Learning/Training &Malaria in Pregnancy &Partnership &Strategy Bill Brieger | 05 Feb 2014
Jhpiego at 40 – commitment to malaria prevention and control in Burkina Faso

Jhpiego 40th Anniversary celebration in Ouagadougou with First Lady, US Ambassador, Minister for Health and Jhpiego’s President and Vice President
Jhpiego was founded in 1973 to provide technical assistance to countries where the risk of maternal mortality and morbidity was quite high. While focusing on local capacity building from the start, Jhpiego’s model for technical assistance has evolved. Burkina Faso first benefitted in 1983 by having health staff attend intensive training at Johns Hopkins Hospital. Subsequently Jhpiego’s work moved to the field, and some of the early trainees became staff on the ground.
Jhpiego established an office in Ouagadougou in 1996, and one of the earliest projects focused on malaria in pregnancy as part of USAID’s flagship program “Maternal and Neonatal Health” (MNH). It was during that time that Jhpiego collaborated with partners like CDC to do some of the early testing of the intermittent preventive treatment of malaria in pregnancy (IPTp) in West Africa. The results of this life-saving intervention were published in the American Journal of Tropical Medicine and Hygiene.
Jhpiego continued to provide technical assistance on malaria in pregnancy interventions and capacity building to the Ministry of Health (MOH) in Burkina Faso through the MNH project and into its successor, USAID’s ACCESS project. Jhpiego worked with partners to update malaria guidelines, training materials, supervisory tools and job aids during this period.
 In 2009 USAID presented the Maternal and Child Health Integrated Project (MCHIP) with the opportunity to carry out an integrated package of malaria care and prevention strengthening with the MOH and particularly the National Malaria Control Program (NMCP). Over a period of three years Jhpiego, the lead organization in MCHIP, working with together with partners from the NMCP and MOH, was able to accomplish among others the following:
In 2009 USAID presented the Maternal and Child Health Integrated Project (MCHIP) with the opportunity to carry out an integrated package of malaria care and prevention strengthening with the MOH and particularly the National Malaria Control Program (NMCP). Over a period of three years Jhpiego, the lead organization in MCHIP, working with together with partners from the NMCP and MOH, was able to accomplish among others the following:
- Updating Malaria policy and guidelines
- Updating Malaria supervisory tools and training of supervisors
- Updating In-service training materials on malaria and training of health facility staff
- Developing a Strategic communications plan and strategy for malaria
- Forming of curriculum update committee on malaria at national training schools for primary health staff
- Training of US Peace Corps Volunteers to support malaria activities in their communities
- Building the capacity and organizational strengthening for the NMCP itself
- Conducting a situation analysis of rapid diagnostic test acceptance and use
- Undertaking a health systems analysis of the strengths and bottlenecks of malaria program implementation in Burkina Faso
 Last week, the Burkina Faso office of Jhpiego hosted the organization’s African Malaria Technical Update Workshop with staff from 15 countries participating. Today Jhpiego is taking its 40th Anniversary celebrations to Ouagadougou. Jhpiego will express appreciation to local partners in the fight against malaria and threats to maternal and child health.
Last week, the Burkina Faso office of Jhpiego hosted the organization’s African Malaria Technical Update Workshop with staff from 15 countries participating. Today Jhpiego is taking its 40th Anniversary celebrations to Ouagadougou. Jhpiego will express appreciation to local partners in the fight against malaria and threats to maternal and child health.
Jhpiego has been committed on the ground in Burkina Faso to building national capacity for controlling malaria specifically for over 15 years. The recent award by USAID of its bilateral program “Improving Malaria Care” to Jhpiego last October cements Jhpiego’s commitment to the country and to reducing malaria for another five years.
IPTp &Malaria in Pregnancy &Reproductive Health Bill Brieger | 21 Nov 2013
Malaria Products Must be Included in Life Saving Commodities for RMNCH
According to the Every Woman Every Child website (EWEC), “A strong focus on reproductive, maternal, child and newborn health (RMCNH) is integral to improving global health. RMNCH is linked to all 8 Millennium Development Goals (MDGs). MDGs 4 (Reduce Child Mortality), 5 (Improve Maternal Health) and 6 (combat HIV/AIDS, malaria and other diseases) each have specific targets and indicators related to RMNCH.” In order to achieve these goals life saving commodities must be made available to all women and children, and as implied in the statement above, they must include commodities that prevent and treat malaria in pregnancy.
The website further states that, “Based on these criteria, an initial list of 13 affordable, effective, but underutilized life-saving commodities were identified for consideration by the Commission. The UN Commission on Life-Saving Commodities for Women and Children aims to increase access to life-saving medicines and health supplies for the world’s most vulnerable people.” Ironically this suggestive list does not include medicine for intermittent preventive treatment of malaria in pregnancy (IPTp), insecticide treated nets (ITNs), malaria rapid diagnostic tests or artemisinin-based combination therapy medicines for malaria treatment.
Yes the list is only suggestive, and yes it is a global list, but WHO estimates that nearly 50 million women will become pregnant in malaria endemic areas each year. That’s a pretty big chunk of the world’s population to neglect.
EWEC does refer to two partner documents for more details on these essential commodities. One document is “The Essential Interventions, Commodities and Guidelines for Reproductive, Maternal, Newborn and Child Health – A global review of the key interventions related to reproductive, maternal, newborn and child Health.” This document mentions generically “Prevention and management of malaria with insecticide treated nets and antimalarial medicines.”
 The second document, “Priority medicines for mothers’ and children’s health, 2011”, also identifies medicines that are in need of enhanced attention and utilization in order to avoid preventable deaths of women and children. This document mentions that commodities exist for malaria services, but refers the reader to the very detailed Global Malaria Program’s “Guidelines for the treatment of malaria” (2nd ed. Geneva, World Health Organization, 2010) that discusses medications for all species of Plasmodium and does not have an easy to view take away on the essential life saving commodities within.
The second document, “Priority medicines for mothers’ and children’s health, 2011”, also identifies medicines that are in need of enhanced attention and utilization in order to avoid preventable deaths of women and children. This document mentions that commodities exist for malaria services, but refers the reader to the very detailed Global Malaria Program’s “Guidelines for the treatment of malaria” (2nd ed. Geneva, World Health Organization, 2010) that discusses medications for all species of Plasmodium and does not have an easy to view take away on the essential life saving commodities within.
Over the past year the Global Malaria Program of WHO has issued guidance for updating malaria in pregnancy interventions, including more frequency IPTp with sulphadoxine-pyrimethamine (SP). The briefing companion document to this new guidance spells out the following life saving benefits if IPTp with appropriate references:
- IPTp-SP prevents the adverse consequences of malaria on maternal and fetal outcomes, such as placental infection, clinical malaria, maternal anaemia, fetal anaemia, low birth weight and neonatal mortality.
- IPTp-SP has recently been shown to be highly cost-effective for both prevention of maternal malaria and reduction of neonatal mortality in areas with moderate or high malaria transmission.
- Despite the spread of SP resistance, IPTp-SP continues to provide significant benefit, resulting in protection against both neonatal mortality (protective efficacy 18%) and low birth weight (21% reduction in LBW) under routine program conditions.
Over the years rarely has IPTp if ever achieved high and sustained coverage. Factors relating to late antenatal care attendance are often mentioned first, but experience has shown that one of the key factors is stock-out of SP. Once SP was no longer a first line treatment drug, it was forgotten – a neglected medicine needed by an often neglected but vulnerable portion of the population. Now is the time to advocate strongly for direct and unconditional listing of SP for IPTp, ITNs and other malaria products among any list of RNMCH life saving commodities.
Community &IPTp &Malaria in Pregnancy Bill Brieger | 15 Nov 2013
Improving Intermittent Preventive Treatment in Pregnancy and Antenatal Care Coverage
The Malaria Communities Program (MCP), supported by the US President’s Malaria Initiative, has increased local and indigenous capacity to undertake community-based malaria prevention and treatment activities; built local ownership of malaria control for the long term in partnership with communities and National Malaria Control Programs (NMCPs); and extended coverage of PMI and NMCP interventions to reach a larger beneficiary population. Below is a summary of the third in a series of MCP case studies found on the website of MCHIP – the USAID Maternal and Child Health Integrated Project.
The full case study on improving coverage of two doses of intermittent preventive treatment in pregnancy (IPTp) and attendance at antenatal care clinics, the main platform for delivering IPTp can be found at: http://www.mchip.net/node/2082
This IPTp/ANC case study focuses on four MCP partners and their contributions to improving the second dose of intermittent preventive treatment in pregnancy (IPTp2) and ANC coverage: Medical Teams International (MTI) Uganda, Episcopal Relief and Development (ERD) Angola, Caritas Senegal, and the Catholic Medical Mission Board (CMMB) Zambia. MCHIP collected multiple forms of data from each MCP partner using qualitative methods, including individual interviews with key project personnel and review of key documents.
MCHIP then compared data across organizations to better understand the total contributions made by the MCP. Some partners conducted surveys and relevant quantitative data are included in this report. Data are limited by a lack of standardized reporting on this topic. Although MIP interventions comprise more than IPTp and ANC, the three sub-themes emerging from this review are: 1) mobilizing communities to increase ANC and IPTp uptake; 2) using behavior change communication (BCC) to inform women and their families about the importance of ANC and IPTp; and 3) improving access to quality ANC services.
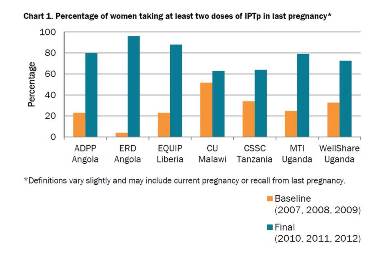 Chart 1 shows results from MCP projects that collected survey data regarding IPTp, and indicates significant improvements in coverage in those project areas. MCP partners built partnerships between communities and health facilities to improve access. As exemplified by strategies such as VHTs accompanying pregnant women to health facilities and assisting midwives in administration of IPTp, when communities and facilities work together the partnership yields not only improved outcomes but also improved attitudes among providers and clients. MTI successfully expanded the Ministry of Health package of Village Health Team services to address malaria in pregnancy in their project area.
Chart 1 shows results from MCP projects that collected survey data regarding IPTp, and indicates significant improvements in coverage in those project areas. MCP partners built partnerships between communities and health facilities to improve access. As exemplified by strategies such as VHTs accompanying pregnant women to health facilities and assisting midwives in administration of IPTp, when communities and facilities work together the partnership yields not only improved outcomes but also improved attitudes among providers and clients. MTI successfully expanded the Ministry of Health package of Village Health Team services to address malaria in pregnancy in their project area.
MCP partners implemented interpersonal communication strategies to increase demand for and use of MIP-related services. MCP partners also encouraged male participation to increase coverage of MIP-related
services.