Health Systems &Policy Bill Brieger | 29 Jun 2014
Model World Health Organization at UNC Gillings School of Public Health
 Neha Acharya, who is the Director of the American Mock World Health Organization conference, set to be held within UNC’s Gillings School of Public Health from October 3rd-5th, has shared the following announcement with us:
Neha Acharya, who is the Director of the American Mock World Health Organization conference, set to be held within UNC’s Gillings School of Public Health from October 3rd-5th, has shared the following announcement with us:
AMWHO is the nation’s very first simulation of the World Health Assembly, and seeks to educate undergraduate and graduate students on the proceedings of global health affairs. This conference will invite over 200 students from all across the nation, and is America’s very first model WHO event.
 The American Mock World Health Organization (AMWHO) is an authentic simulation of the World Health Assembly, the sole decision-making body of the World Health Organization. Participants assume the role of a WHO ambassador, non-governmental organization member, or media representative, and form health related positions based upon their respective roles. Throughout the conference, participants will engage in debates and discussions about a thematic health topic, and work together to create a final working resolution to send to the World Health Organization in Geneva, Switzerland.
The American Mock World Health Organization (AMWHO) is an authentic simulation of the World Health Assembly, the sole decision-making body of the World Health Organization. Participants assume the role of a WHO ambassador, non-governmental organization member, or media representative, and form health related positions based upon their respective roles. Throughout the conference, participants will engage in debates and discussions about a thematic health topic, and work together to create a final working resolution to send to the World Health Organization in Geneva, Switzerland.
Modeled after the Ontario and Montreal World Health Organization conferences set in Canada, the primary focus of all three is to raise student awareness of pertinent health issues facing the world today, as well as to promote understanding of the many roles students can engage in through global health policy. The conference hopes to establish an environment similar to that of the World Health Organization’s Assembly, and educate future global health leaders in the proceedings of international health entities.
This simulation will be the United States’ first model-WHO conference, and is set to take place in Rosenau Hall within the University of North Carolina at Chapel Hill’s campus from October 3rd-5th, continuing in the years to come. Register at www.amwho2014.com? and purchase your $45 ticket! You can also follow plans and progress on twitter.
Health Information &Monitoring Bill Brieger | 22 Jun 2014
Regular data Review Meetings in Mozambique, a Path to Improving Malaria Service Delivery
Health Alliance International (HAI) of the University of Washington, is collaborating with Centro de Investigação Operacional da Beira (CIOB) is based in Beira, Mozambique to improve the quality and use of routine monitoring and evaluation data from the health facility through to the district in Sofala Province. The aim is to strengthen the health system through data for decision making and improve quality and uptake of services. This effort is sponsored by a grant from the Doris Duke Charitable Foundation.
 A key feature of the program is a regular data review meeting where representatives from health facilities in a district come together and each presents his/her standard Ministry of Health service indicators in a simple slide format. After each presentation the speaker received feedback from the group, including members of the district health management team, on successes and challenges and is encouraged to make plans to improve both data quality and service uptake.
A key feature of the program is a regular data review meeting where representatives from health facilities in a district come together and each presents his/her standard Ministry of Health service indicators in a simple slide format. After each presentation the speaker received feedback from the group, including members of the district health management team, on successes and challenges and is encouraged to make plans to improve both data quality and service uptake.
The data review meetings started with an overview of all HIV, reproductive, maternal and child health indicators. Separate review meetings for malaria service indicators have been recently introduced.
According to members of the district teams, the individual facility staff presenters have grown more skilled in formatting their data and presenting to an audience. Overall, participants in these meetings appear enthusiastic and interested in the results of their peers. Constructive critiques are the norm, and speakers express appreciation for suggestions on how they can improve their services and the resulting data.
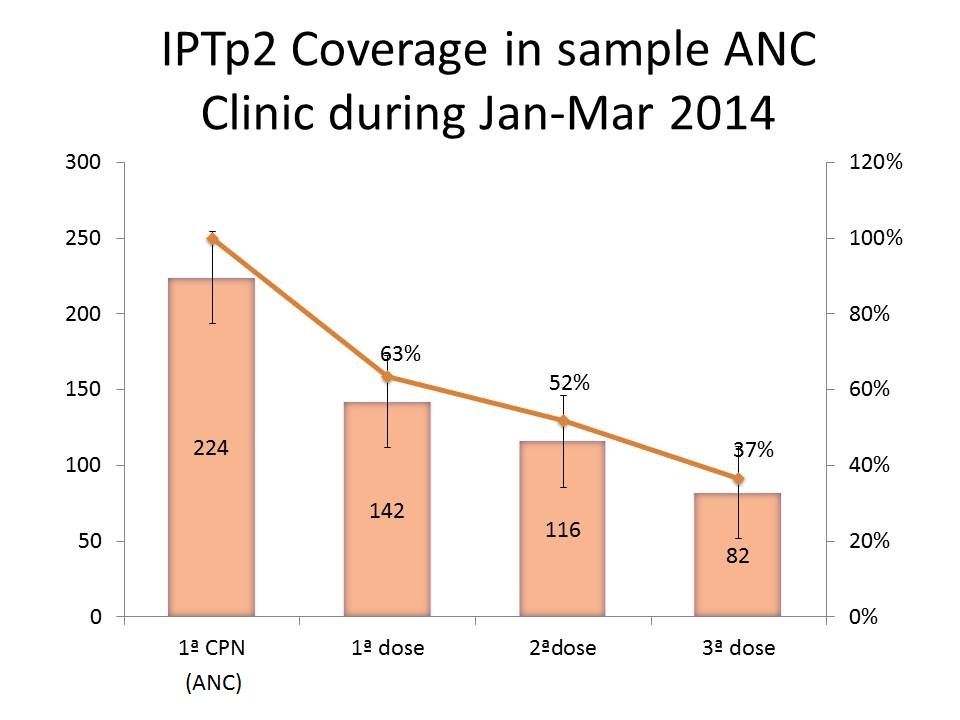 A sample chart from a health facility showing a quarterly review of intermittent preventive treatment for malaria in pregnancy (IPTp) is seen to the right. After viewing this, meeting participants might ask the presenter what are the reasons for the drop-off in coverage. If for example, the problem of late antenatal care (ANC) attendance is mentioned, the group can ask the presenter to consider how to encourage women to attend earlier.
A sample chart from a health facility showing a quarterly review of intermittent preventive treatment for malaria in pregnancy (IPTp) is seen to the right. After viewing this, meeting participants might ask the presenter what are the reasons for the drop-off in coverage. If for example, the problem of late antenatal care (ANC) attendance is mentioned, the group can ask the presenter to consider how to encourage women to attend earlier.
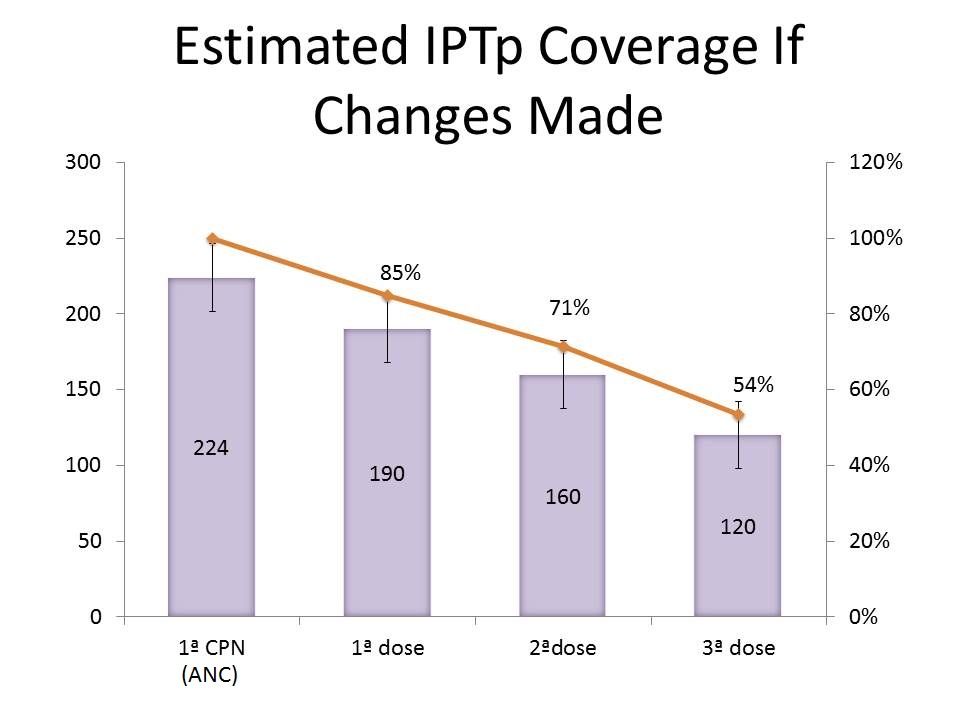 If the presenter then goes back and implements the suggestions, the second chart might reflect the results of improved service uptake. In this way the overall project hopes that close examination of their own data by service providers can strengthen service delivery and the health system.
If the presenter then goes back and implements the suggestions, the second chart might reflect the results of improved service uptake. In this way the overall project hopes that close examination of their own data by service providers can strengthen service delivery and the health system.
We look forward to hearing more about this unique process so that it can be disseminated in other malaria endemic countries.
Community Bill Brieger | 20 Jun 2014
Tanzania Community Health Workers Blog on Malaria and Other Concerns
The Connect Project of Ifakara Health Institute of Tanzania and Columbia Mailman School of Public Health with the support of the Doris Duke Charitable Foundation has trained community health workers known as Community Health Agents (CHAs), or the ancronym WAJA in Swhili, in three districts in Tanzania. The project has encouraged the CHAs to start blogging their experiences and challenges in promoting community health. Below are two examples of their work as it involved malaria. More postings can be viewed on WordPress.
 Boniface Madina Mwandishi, that CHA from Katindiuka Village, is particularly concerned about preventing malaria in pregnant women. When He talked to women in his service area he learned that the net voucher system that allows women to get insecticide treated nets at half the going price of TSH 2,500 (~$1.50) had problems.
Boniface Madina Mwandishi, that CHA from Katindiuka Village, is particularly concerned about preventing malaria in pregnant women. When He talked to women in his service area he learned that the net voucher system that allows women to get insecticide treated nets at half the going price of TSH 2,500 (~$1.50) had problems.
First the vouchers were either late or not available in the nearby health facilities. Many cannot afford to pay the full price. Thus most women are not using nets to protect themselves and their unborn children from malaria.
A village elder complained to Boniface that his wife was not able to obtain a net even until a month after their child was born. The elder stressed that had the vouchers and nets been available more women and children would have been protected from malaria. Boniface will follow up to report on the lapses in the voucher system.
 Castor Mwinamile, the CHA from Mchombe Village, reports on problems with Malaria Rapid Diagnostic Tests (RDTs). He had called mothers together for health education, but they also used the opportunity to complain about the current stock-out of malaria RDTs in the village.
Castor Mwinamile, the CHA from Mchombe Village, reports on problems with Malaria Rapid Diagnostic Tests (RDTs). He had called mothers together for health education, but they also used the opportunity to complain about the current stock-out of malaria RDTs in the village.
Mothers noted that without RDTs the actual disease of their sick child could not be determined easily. Maybe the child with fever had a urinary tract infection or maybe it was malaria. The CHA promised the mothers to inform the project quickly about the stock-out.
While CHAs are given basic phones to communicate with supervisors and among themselves, some do have smart phones and are able to post on the blog and share with their fellow CHAs who may not have a phone.
The feedback to the program and shared learning among the CHAs, enabled by the blog, demonstrate a unique learning and problem solving experience in community health. These two postings also show that the CHAs have made their communities aware of the benefits of malaria services, hence their demand for better access.
There are other postings about malaria on the Sauti ya Waja, so if your Swahili is adequate, we encourage you to also learn from the Community Health Agents of Tanzania.
Elimination &Eradication Bill Brieger | 16 Jun 2014
Guinea Worm, Inching Toward Eradication
Twenty-eight years ago efforts to eradicate guinea worm began in earnest. It was the UN Water Decade, and there was optimism that guinea worm could be the test case for success of the global effort to guarantee adequate and safe water for all.
 As can be seen in the CDC infographic, we have gone from 3.5 million cases to 148 during this time. As we reach toward the tail end of the worm, we find some challenges remain.
As can be seen in the CDC infographic, we have gone from 3.5 million cases to 148 during this time. As we reach toward the tail end of the worm, we find some challenges remain.
On the list of currently endemic countries one finds Chad. Chad was supposed to be in the pre-certification phase, but new cases appeared a few years ago.
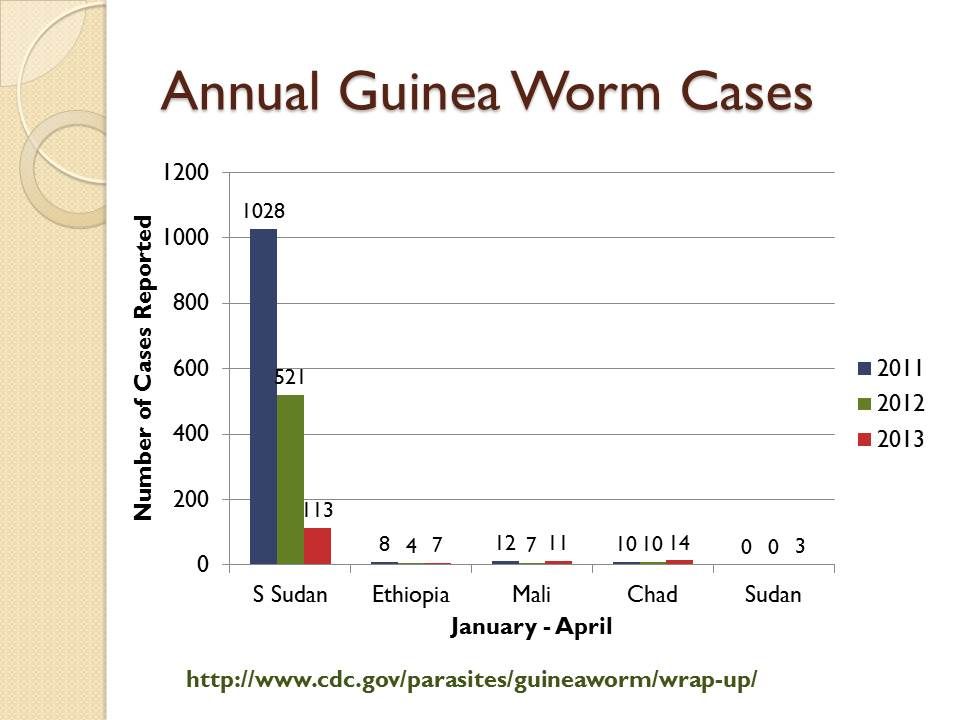 Sudan was the most highly endemic country until South Sudan gained independence and took the guinea worm cases with it. Recently a few cases have also appeared again in the Sudan itself seen in charts derived from CDC’s newsletter, Guinea Worm Wrap-Up.
Sudan was the most highly endemic country until South Sudan gained independence and took the guinea worm cases with it. Recently a few cases have also appeared again in the Sudan itself seen in charts derived from CDC’s newsletter, Guinea Worm Wrap-Up.
Looking at the most recent data from early 2014, one can see that Mali is back to reporting no cases as have Ethiopia and Sudan for 2014. Caution is needed since transmission is more likely in the upcoming rainy season months than in the current dry period.
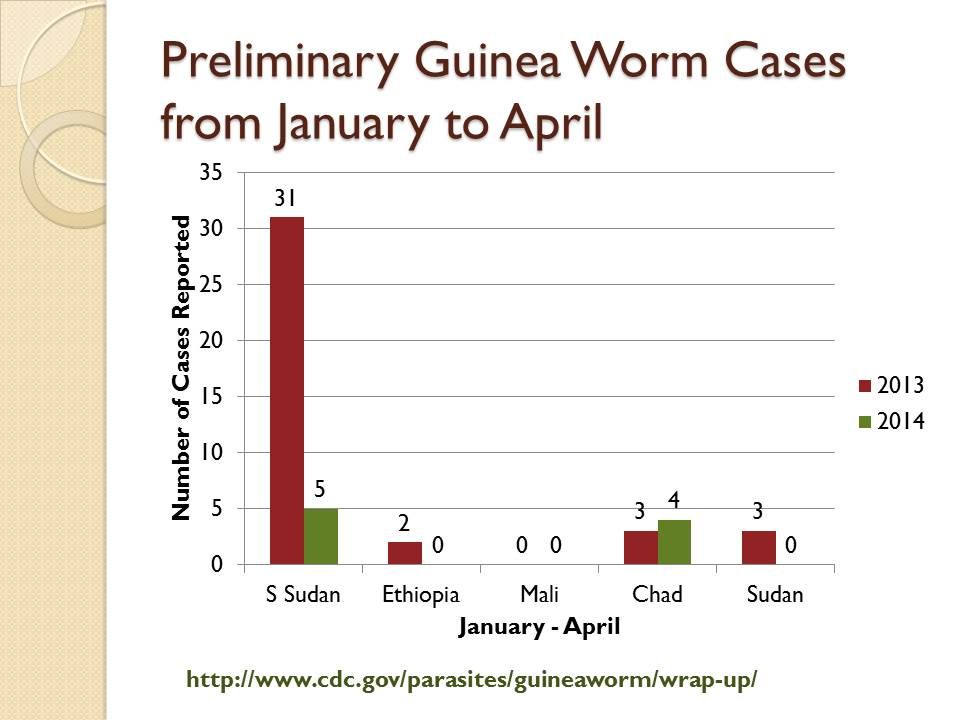 What is common in these areas is either being in a state of conflict or bordering a conflict zone. This makes efforts to detect cases and put interventions in place in a timely manner to prevent the next season’s transmission very difficult.
What is common in these areas is either being in a state of conflict or bordering a conflict zone. This makes efforts to detect cases and put interventions in place in a timely manner to prevent the next season’s transmission very difficult.
Unlike some other diseases, guinea worm has some relatively simple, epidemiologically appropriate and less expensive interventions like cloth water filters, abate/temephos for water source treatment and case containment. Of course investments in improved water supplies will also solve the problem. But without easy access to the communities where transmission is occurring, the disease will persist at this incredibly low level.
Other disease elimination programs are equally affected by the problems of access and conflict, polio being a good example. We know that malaria is also exacerbated in conflict situations, but in the locations where pre-elimination is near, like Swaziland, Botswana, South Africa and Namibia, the main concern is ensuring a strong health system to handle the additional surveillance tasks. Still we should not be complacent, because malaria is also endemic in these very sites where guinea worm stubbornly lingers.
Congenital Malaria &IPTp &ITNs &Malaria in Pregnancy &Mortality Bill Brieger | 12 Jun 2014
Congenital Malaria, an Underappreciated Neonatal Problem
The largest portion of infant deaths occurs in the neonatal period. During those first 28 days, the child is at risk from a variety of problems arising from delivery complications, infections and simply not being kept warm.
 In malaria endemic areas there is the small but important problem of malaria transferred from mother to child, or congenital malaria. The problem occurs with both Plasmodium vivax and falciparum.
In malaria endemic areas there is the small but important problem of malaria transferred from mother to child, or congenital malaria. The problem occurs with both Plasmodium vivax and falciparum.
Congenital malaria in the newborn is often hard to detect. There may be fever, but other signs and symptoms might include anaemia, jaundice, paleness, diarrhoea, vomiting, and general weakness.
Prevalence of congenital malaria in Ghana, for example, ranged from 2% by microscopy to 12% using polymerase chain reaction (PCR). In India microscopy revealed a prevalence of 3% with cases of both vivax and falciparum.
One would hope this problem could be avoided if prevention of malaria in pregnancy was practiced using insecticide treated nets, intermittent preventive treatment (IPTp) and prompt and appropriate case management, but studies still find placental and cord parasiteamia in countries where such interventions are supposed to be integrated into antenatal/prenatal care. In Colombia, “An association was found between congenital malaria and the diagnosis of malaria in the mother during the last trimester of pregnancy or during delivery, and the presence of placental infection.”
Countries are in the process of shifting to the relatively new WHO guidance on IPTp that encourages monthly doses of sulfadoxine-pyrimethamine from the beginning of the second trimester up until delivery. Countries are also trying to ensure universal coverage of ITNs so that women will be using nets prior to even becoming pregnant.
We still have trouble administering to take just two doses of IPTp, but if we want to prevent congenital malaria, we need to ensure that women are protected from malaria in their placentas and are free from parasites right up until they give birth and thereby prevent another cause of neonatal mortality.