CHW &Community &IPTi &ITNs &Malaria in Pregnancy &Treatment Bill Brieger | 01 Nov 2015
Community Directed Interventions to Enhance PHC and MCH
William Brieger of the Department of International Health, JHU Bloomberg School of Public Health, delivered the keynote address to the Community Based Primary Health Care Working Group at the 2015 American Public Health Association in Chicago. The focus was on Community Directed Interventions (CDI) as a way to enhance implementation of primary health care and maternal and child health. Some excerpt from the talk follow.
 The origins of the CDI Approach are based in Onchocerciasis Control and the implementation research done by the Tropical Disease Research (TDR) Program of WHO and collaborating agencies to help establish the foundational guidance of the African Program for Onchocerciasis Control in 1995. Since then we have seen an expansion of CDI into other health issues
The origins of the CDI Approach are based in Onchocerciasis Control and the implementation research done by the Tropical Disease Research (TDR) Program of WHO and collaborating agencies to help establish the foundational guidance of the African Program for Onchocerciasis Control in 1995. Since then we have seen an expansion of CDI into other health issues
We should start discussion with an understanding of ‘community’ which Rifkin et al. (1988) defined as a group of people living in the same defined area sharing basic values, organization, and interests. White (1982) proposed that community is an informally organized social entity which is characterized by a sense of identity. Manderson et al. (1992) in their work for TDR defined community as a population which is geographically focused but which also exists as a discrete social entity, with a local collective identity and corporate purpose.
Communities are people sharing values and institutions. Community is based on locality (geographic), interdependent social groups, interpersonal relationships expressed through social networks and built on s culture that includes values, norms, and attachments to the community as a whole as well as to its parts. Prior to developing any community intervention we must understand the boundaries, composition and structure of a community from the perspectives of its own members, as their local knowledge and participation are central to success.
 Community Systems Strengthening has been taken up by the Global Fund in order to enhance coverage of various health interventions such as HIV drugs and bednets to prevent malaria. Community systems are community?led structures and mechanisms used by communities through which community members and community based organizations and groups interact, coordinate and deliver their responses to the challenges and needs affecting their communities. Many community systems are small?scale and/or informal. Others are more extensive – they may be networked between several organizations and involve various sub?systems. For example, a large care and support system may have distinct sub?systems for comprehensive home?based care, providing nutritional support, counselling, advocacy, legal support, and referrals for access to services and follow?up.
Community Systems Strengthening has been taken up by the Global Fund in order to enhance coverage of various health interventions such as HIV drugs and bednets to prevent malaria. Community systems are community?led structures and mechanisms used by communities through which community members and community based organizations and groups interact, coordinate and deliver their responses to the challenges and needs affecting their communities. Many community systems are small?scale and/or informal. Others are more extensive – they may be networked between several organizations and involve various sub?systems. For example, a large care and support system may have distinct sub?systems for comprehensive home?based care, providing nutritional support, counselling, advocacy, legal support, and referrals for access to services and follow?up.
Efficacy, Social Control and Cohesion are important characteristics of communities that enable them to take on project and solve problems. Collective Efficacy is a perceived ability to work together. Social control provides evidence that communities are able to enforce their norms. Cohesion describes social interaction that brings people together. A strong sense of identity and a sense of belonging describe communities that can get things done. These characteristics lead to community competency to collaborate effectively in identifying the problems/needs of the community, achieve a working consensus on goals and priorities, agree on ways and means to implement the agreed-upon goals, and collaborate effectively in the required actions.
 It is important to distinguish between Community Based Intervention (CBI) and Community Directed Intervention. CBI takes place in the community but a Health/Development agency exercises authority over decisions on project design and implementation. Project activities (e.g., service delivery dates and procedures) are designed by the agency. Activities simply happen in the community.
It is important to distinguish between Community Based Intervention (CBI) and Community Directed Intervention. CBI takes place in the community but a Health/Development agency exercises authority over decisions on project design and implementation. Project activities (e.g., service delivery dates and procedures) are designed by the agency. Activities simply happen in the community.
With CDI the community exercises authority over decisions and decides on acceptable method to implement projects. This ensures sensitivity to local decision-making structures and social life. Activities happen both in and by the community; the community is in control.
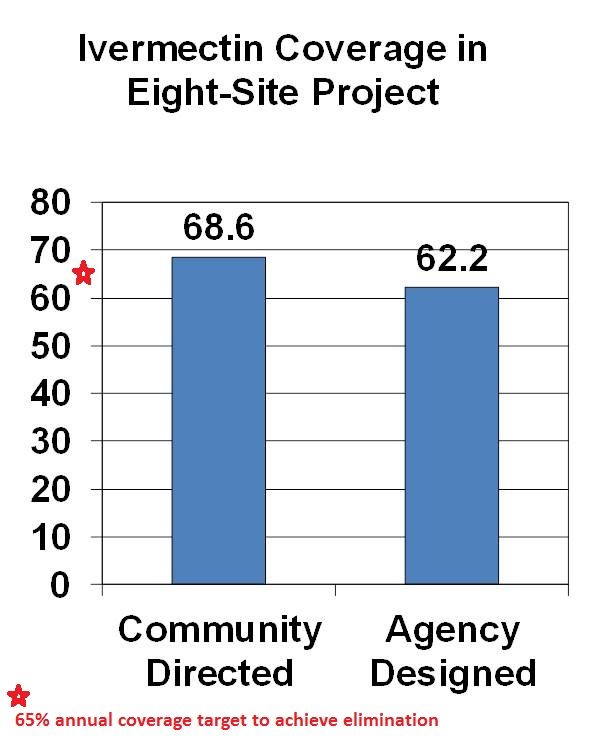
CDI was pioneered for Onchocerciasis (River Blindness) Control as community directed treatment with ivermectin (CDTI). When communities are in charge, coverage is better than when ivermectin distribution is centrally organized by a health agency. The original 1995 CDI field testing showed better ivermectin coverage when the community was in charge of distribution. Since the beginning of CDTI, over 200,000 villages in 18 African countries have been distributing ivermectin annually through their own efforts. Lessons learned over the years are that CDI works best when 1) the smallest level of an organized community is the basis of action (e.g. a hamlet, a clan/kin group) and 2) communities are encouraged to choose as many CDDs as they think they need to get the job done. This means that the community is in charge, not individual volunteers who can be replaced anytime the community finds the need.
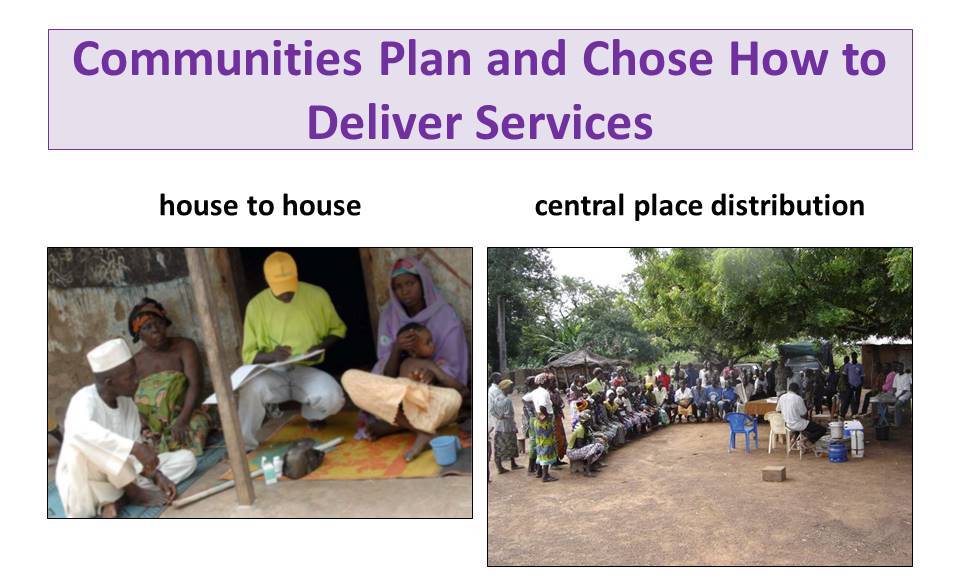
With CDI for onchocerciasis or any other health program, Communities plan and chose how to deliver services. This may be house-to-house, central place distribution or a combination. Health workers provide training and supervision to volunteer village health workers called community directed distributors (CDDs).
 TDR observed that CDI naturally expanded to include other services wanted by the community such as immunization, community development, water and sanitation, agriculture and forestry, HIV-AIDS, family planning, guinea worm, Vitamin A. TDR and APOC then decided that CDI with other service components should be systematically tested. The project sites added in a systematic manner other interventions to existing CDTI programs including home management of malaria, ITN distribution & promotion, TB DOTS, Vitamin A in addition to continued ivermectin distribution. These services varied in complexity and communities responded by dividing the work among several different volunteers.
TDR observed that CDI naturally expanded to include other services wanted by the community such as immunization, community development, water and sanitation, agriculture and forestry, HIV-AIDS, family planning, guinea worm, Vitamin A. TDR and APOC then decided that CDI with other service components should be systematically tested. The project sites added in a systematic manner other interventions to existing CDTI programs including home management of malaria, ITN distribution & promotion, TB DOTS, Vitamin A in addition to continued ivermectin distribution. These services varied in complexity and communities responded by dividing the work among several different volunteers.
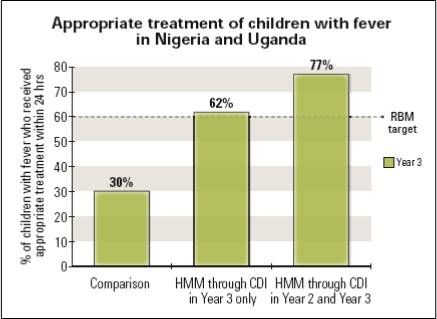 Coverage of interventions like malaria case management, ITN promotion and Vitamin A distribution was higher in the intervention areas compared to the delivery of these services through the routine health system. TB DOTS presented the only challenge because of the social stigma associated with the disease. The study concluded that CDI can effectively incorporate high impact, evidence based interventions while at the same time maintaining and increasing ivermectin coverage. Since CDI does not rely on one volunteer but whole community effort, the problem of overburdening on community health worker did not arise. Other incterventions ould benefit from CDI such as Misoprostol, Intermittent Preventive Treatment, Deworming, Oral Rehydration solution, Zinc, Cotrimoxazole, Amoxicillin, Soap for handwashing and WaterGuard treatment kits.
Coverage of interventions like malaria case management, ITN promotion and Vitamin A distribution was higher in the intervention areas compared to the delivery of these services through the routine health system. TB DOTS presented the only challenge because of the social stigma associated with the disease. The study concluded that CDI can effectively incorporate high impact, evidence based interventions while at the same time maintaining and increasing ivermectin coverage. Since CDI does not rely on one volunteer but whole community effort, the problem of overburdening on community health worker did not arise. Other incterventions ould benefit from CDI such as Misoprostol, Intermittent Preventive Treatment, Deworming, Oral Rehydration solution, Zinc, Cotrimoxazole, Amoxicillin, Soap for handwashing and WaterGuard treatment kits.
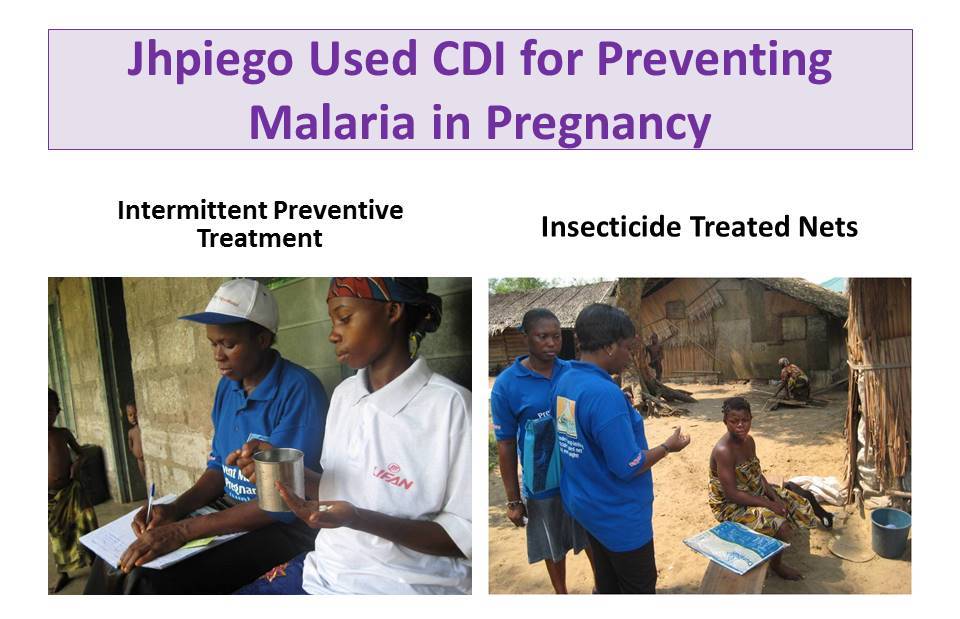 Jhpiego an NGO affiliate of the Johns Hopkins University used CDI to deliver malaria in pregnancy (MIP) prevention services in Nigeria including Intermittent Preventive Treatment and Insecticide Treated Nets. Contrary to fears that CDI would detract from antenatal care attendance, the work of CDDs actually ensured that ANC attendance increased over time. Through CDI IPTp coverage increased compared to control communities and more pregnant women slept under ITNs regularly.
Jhpiego an NGO affiliate of the Johns Hopkins University used CDI to deliver malaria in pregnancy (MIP) prevention services in Nigeria including Intermittent Preventive Treatment and Insecticide Treated Nets. Contrary to fears that CDI would detract from antenatal care attendance, the work of CDDs actually ensured that ANC attendance increased over time. Through CDI IPTp coverage increased compared to control communities and more pregnant women slept under ITNs regularly.
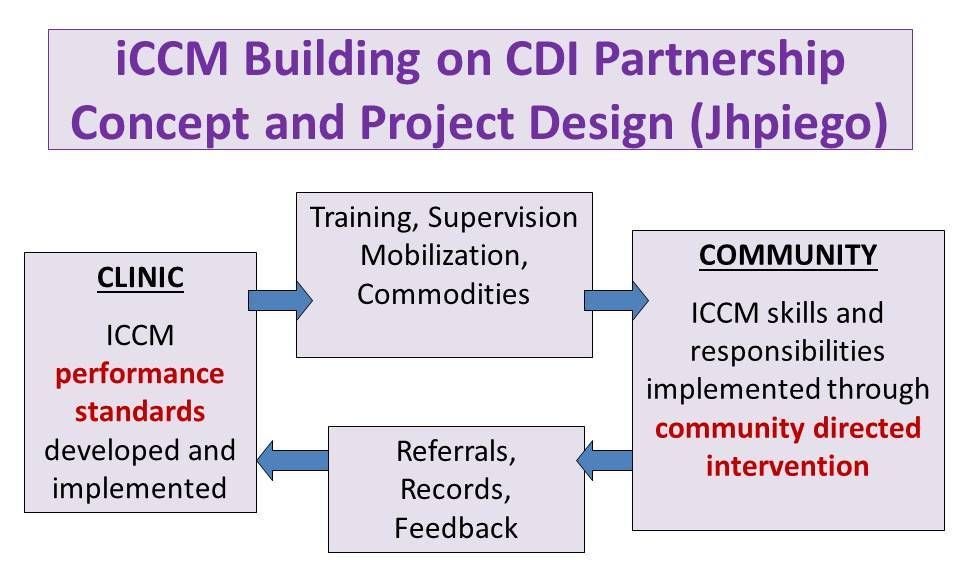 Jhpiego next expanded CDI for MIP into integrated Community Case Management (iCCM), thus taking community case management beyond community based care. Giving communities responsibility for organizing and managing their services using the CDI approach meant greater access to services whenever people need them. Using the CDI approach to iCCM CDDs reached 7,504 clients who presented signs and symptoms of malaria. CDDs successfully conducted malaria diagnosis using the rapid diagnostic test (RDT) kits. Overall, 47.8% tested positive while 52.2% tested negative. CDDs adhered to guidelines and all the 3,587 clients with positive RDT results received appropriate anti-malarial medicines. As appropriate 21.0% were treated for diarrhoea, 11.0% for pneumonia (of whom 68.0% were referred to the health facility)
Jhpiego next expanded CDI for MIP into integrated Community Case Management (iCCM), thus taking community case management beyond community based care. Giving communities responsibility for organizing and managing their services using the CDI approach meant greater access to services whenever people need them. Using the CDI approach to iCCM CDDs reached 7,504 clients who presented signs and symptoms of malaria. CDDs successfully conducted malaria diagnosis using the rapid diagnostic test (RDT) kits. Overall, 47.8% tested positive while 52.2% tested negative. CDDs adhered to guidelines and all the 3,587 clients with positive RDT results received appropriate anti-malarial medicines. As appropriate 21.0% were treated for diarrhoea, 11.0% for pneumonia (of whom 68.0% were referred to the health facility)
 A Supervisory Checklist and Performance Standards were developed and used for Assessing CDD performance. The results were discussed at monthly CDD meetings at their nearest health facilities. This led to further improvements in History taking, Examination, Conducting RDTs for Malaria and Illness Management.
A Supervisory Checklist and Performance Standards were developed and used for Assessing CDD performance. The results were discussed at monthly CDD meetings at their nearest health facilities. This led to further improvements in History taking, Examination, Conducting RDTs for Malaria and Illness Management.
TDR has done further scoping to learn if CDI would be acceptable by health workers and community members in Urban, Nomadic and Underserved Rural Communities. CDI was favorable received. In conclusion we have learned over the years that CDI can involve women, families and communities in meeting their own health needs.
Communication &IPTp &Malaria in Pregnancy Bill Brieger | 28 Oct 2015
Factors associated with the uptake of malaria prophylaxis during pregnancy among female caretakers in Madagascar
Grace N. Awantang, Stella O. Babalola, Hannah Koenker, and Nan Lewicky of the Johns Hopkins Bloomberg School of Public Health, Center for Communication Programs presented a poster today on IPTp uptake in Madagascar. Their Abstract follows:
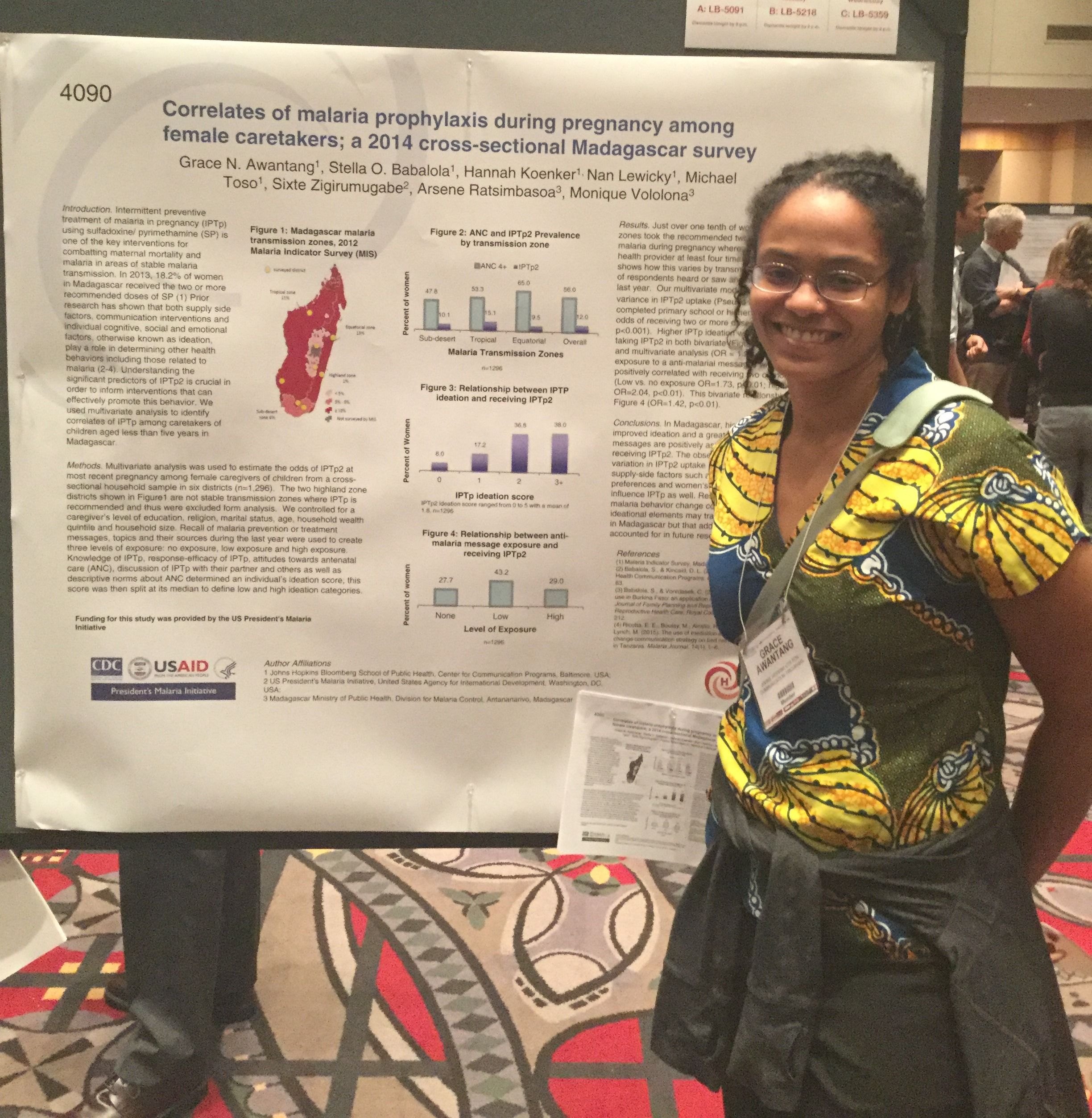 Intermittent preventive treatment of malaria in pregnancy (IPTp) is one of the key interventions promoted for combatting maternal mortality and malaria. In Madagascar, supply side factors such as SP availability and ANC attendance are barriers to practicing IPTp.
Intermittent preventive treatment of malaria in pregnancy (IPTp) is one of the key interventions promoted for combatting maternal mortality and malaria. In Madagascar, supply side factors such as SP availability and ANC attendance are barriers to practicing IPTp.
Less than one fifth of women (18.4%) at risk for malaria take the recommended two doses of sulfadoxine/pyrimethamine (SP) to prevent malaria during pregnancy whereas about half (49.7%) visit a health provider at least four times during pregnancy. Understanding the significant predictors of IPTp2 is crucial in order to inform interventions that can effectively promote this behavior.
Prior research has shown that both communication campaigns and individual cognitive, social and emotional factors, ideation, play a role in determining other health behaviors including malaria. We examined the correlates of IPTp2 using cross-sectional household survey data collected from female caretakers of children under five years of age.
 Caregiver recall of any anti-malaria messages during the past year was used to determine their exposure to health communication. Knowledge of IPTp, response-efficacy of IPTp, attitudes towards antenatal care (ANC), attitudes towards ANC, discussion of IPTp, and descriptive norm about ANC determined a person’s ideation score.
Caregiver recall of any anti-malaria messages during the past year was used to determine their exposure to health communication. Knowledge of IPTp, response-efficacy of IPTp, attitudes towards antenatal care (ANC), attitudes towards ANC, discussion of IPTp, and descriptive norm about ANC determined a person’s ideation score.
Of 1,589 female caretakers, over half (56.8%) were exposed to an anti-malarial message and a tenth (10.8%) mentioned SP as the drug used by pregnant women to prevent malaria. Message exposure, IPTp ideation and education level were all significant predictors of IPTp2 uptake in multivariate analysis.
Uptake was lowest among caretakers in the Highland transmission zone where transmission is unstable and highest in the Sub-desert transmission zone. Results suggest that both individual ideation and exposure to anti-malaria behavior change communication play a significant role in IPTp uptake among women in Madagascar.
The small portion of the variation in IPTp2 uptake explained by the measured covariates suggests that programmatic efforts should address supply-side factors that hinder access to ANC and preventive treatment of malaria during pregnancy.
IPTp &Malaria in Pregnancy Bill Brieger | 28 Oct 2015
“There is no free here, you have to pay” – IPTp in Mali
Colleagues[i] from the Johns Hopkins Bloomberg School of Public Health and the University of Sciences, Techniques, and Technologies of Bamako presented a poster today examining costs for obtaining IPTp at the American Society of Tropical Medicine 64th Annual Meeting. Their Abstract on actual and perceived costs as barriers to intermittent preventive treatment of malaria in pregnancy in Mali appears below.
 “There is no free here,” the words of a Malian husband, illustrate how perceptions of cost can deter uptake of intermittent preventive treatment of malaria in pregnancy (IPTp). Following WHO recommendations, the Malian Ministry of Health (MOH) recommends three doses of IPTp at monthly intervals. However, despite a national policy that IPTp be provided free of charge, only 35% of pregnant women receive at least one dose and less than 20% receive two or more doses.
“There is no free here,” the words of a Malian husband, illustrate how perceptions of cost can deter uptake of intermittent preventive treatment of malaria in pregnancy (IPTp). Following WHO recommendations, the Malian Ministry of Health (MOH) recommends three doses of IPTp at monthly intervals. However, despite a national policy that IPTp be provided free of charge, only 35% of pregnant women receive at least one dose and less than 20% receive two or more doses.
We explored perceptions and experiences of IPTp cost in Mali, and their impact on uptake, using qualitative interviews and focus groups with pregnant women, husbands and mothers-in-law. We also interviewed and observed health workers at four health centers two in Sikasso Region and two in Koulikoro.
 Despite national-level policies, actual IPTp costs varied widely at our study sites – between regions, facilities, and visits. Pregnant women may pay for IPTp, receive it free, or both at different times. Health centers often charge a lump sum for ANC visits that include both some free and some fee-based drugs and services. This makes it difficult for women and families to decipher which services are free and which require payments.
Despite national-level policies, actual IPTp costs varied widely at our study sites – between regions, facilities, and visits. Pregnant women may pay for IPTp, receive it free, or both at different times. Health centers often charge a lump sum for ANC visits that include both some free and some fee-based drugs and services. This makes it difficult for women and families to decipher which services are free and which require payments.
As a result, some forego even free care that, because it is not itemized, appears not to be free. Varying costs also complicate household budgeting for health care, particularly as women often rely on their husbands or husbands’ families for money.
While health facilities operating under the cost-recovery model strive to provide free IPTp, their own financial constraints often make this impossible. Preventing malaria in pregnancy depends upon women receiving the recommended doses of IPTp. However, it is clear that both actual and perceived costs are currently barriers to IPTp uptake.
Given the confusion around cost of services in the two study regions, more detailed national-level studies of both perceived and actual costs could help inform policy and program decisions promoting IPTp. These studies should evaluate both quantitatively and qualitatively the cost information provided by health facilities and pharmacies to pregnant women and their families.
[i] Emily A. Hurley, Namratha Rao, Meredith C. Klein, Hawa Diarra, Samba I. Diop, Seydou Doumbia, & Steven A. Harvey
IPTp &Malaria in Pregnancy Bill Brieger | 28 Oct 2015
Intermittent Preventive Treatment in Pregnancy: Increasing the Doses in Burkina Faso
 Colleagues[1] from the Jhpiego/USAID Burkina Faso Improving Malaria Care Program are presenting a poster at the American Society of Tropical Medicine 64th Annual Meeting Wednesday 28 October 2015. Visit Poster 1655. In the meantime review the abstract below.
Colleagues[1] from the Jhpiego/USAID Burkina Faso Improving Malaria Care Program are presenting a poster at the American Society of Tropical Medicine 64th Annual Meeting Wednesday 28 October 2015. Visit Poster 1655. In the meantime review the abstract below.
In Burkina Faso, Antenatal Care (ANC) is a national platform for malaria in pregnancy prevention and control. The 2010 Demographic and Health Survey showed a good initial ANC registration rate (95%), but over 56% of pregnant women in rural areas do not register until their second or third trimester. Thus they may have missed the full regimen of ANC services including Long Lasting Insecticide-treated nets and intermittent preventive treatment of malaria in pregnancy (IPTp). In 2010 only 10.6% of pregnant women nationally and 8.4% in rural areas received two doses of IPTp.
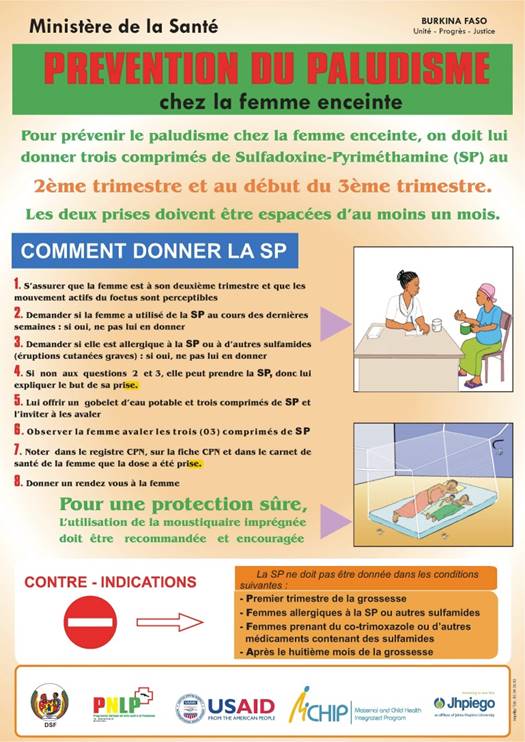 The USAID-supported Improving Malaria Care (IMC) project in Burkina Faso has been providing technical assistance and training to health districts and their ANC staff on implementing updated (2012) WHO IPTp guidelines. The recommended provision of IPTp at every ANC visit from the 13th week of pregnancy onward leads to the possibility of 3 or more doses per woman. The new guidance was incorporated into the update of Burkina Faso’s malaria strategy and has been disseminated since September 2014.
The USAID-supported Improving Malaria Care (IMC) project in Burkina Faso has been providing technical assistance and training to health districts and their ANC staff on implementing updated (2012) WHO IPTp guidelines. The recommended provision of IPTp at every ANC visit from the 13th week of pregnancy onward leads to the possibility of 3 or more doses per woman. The new guidance was incorporated into the update of Burkina Faso’s malaria strategy and has been disseminated since September 2014.
Annual data from the Health Management and information System for 2014 from three districts (Batie, Po and Ouargaye) and 61 health clinics where IMC has been working were collected and summarized. A total of 26,909 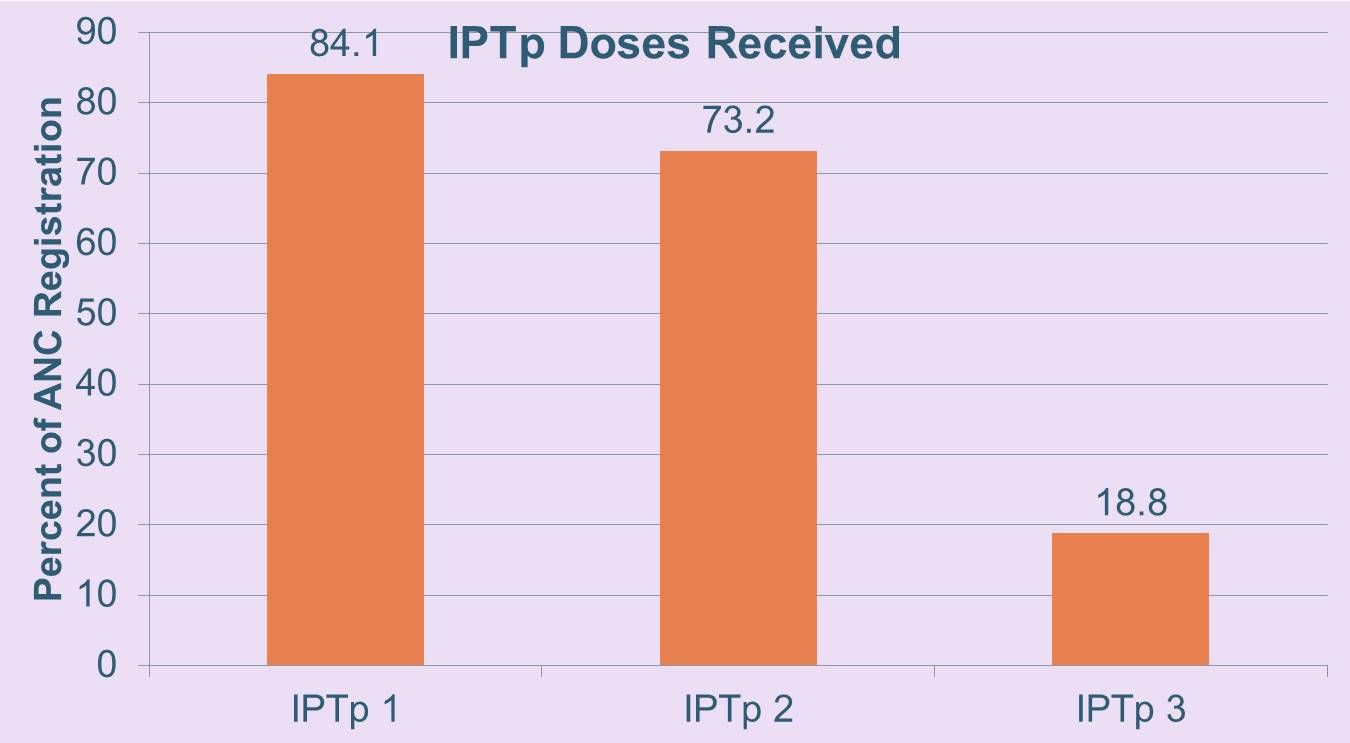 women registered for ANC. Of these 89.7%, 73.2% and 39.8% attended ANC twice, three and four times respectively. Of those registered 84.1%, 73.2% and 18.8% received IPTp once, twice and thrice. Eleven (17.7%) had not started the updated IPTp guidance. The Ministry of Health also experienced stock-outs of sulfadoxine-pyrimethamine.
women registered for ANC. Of these 89.7%, 73.2% and 39.8% attended ANC twice, three and four times respectively. Of those registered 84.1%, 73.2% and 18.8% received IPTp once, twice and thrice. Eleven (17.7%) had not started the updated IPTp guidance. The Ministry of Health also experienced stock-outs of sulfadoxine-pyrimethamine.
Based on this slow implementation and uptake of IPTp3+, the IMC project in collaboration with the National Malaria Control Program is examining ways to strengthen antenatal malaria prevention including capacity building for ANC staff and community IPTp provision.
[1] Ousman Badolo, Stanislas P. Nebie, Mathurin Dodo, Thierry Ouedraogo, Rachel Waxman, William R. Brieger
Advocacy &IPTp &Malaria in Pregnancy Bill Brieger | 26 Oct 2015
Health systems strengthening: Advocacy facilitates availability of sulfadoxine-pyrimethamine for prevention of malaria in pregnancy in Kenya
Colleagues[1] from Jhpiego’s Kenya office and the Ministry of Health are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Tuesday 27th October 2015. Please stop by Poster LB-5225 and discuss the results as presented in the Abstract below.
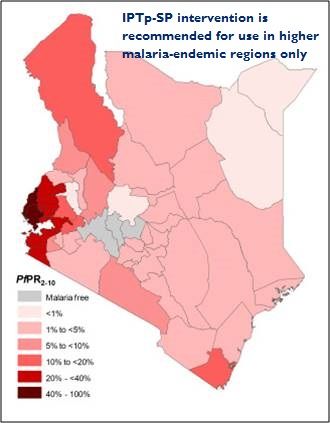 In malaria endemic areas, infection with malaria during pregnancy is often associated with poor pregnancy outcomes. Although effective intervention measures are available including use of sulfadoxine pyrimethamine (SP) for intermittent preventive treatment of malaria in pregnancy (IPTp) coverage rates have remained low.
In malaria endemic areas, infection with malaria during pregnancy is often associated with poor pregnancy outcomes. Although effective intervention measures are available including use of sulfadoxine pyrimethamine (SP) for intermittent preventive treatment of malaria in pregnancy (IPTp) coverage rates have remained low.
In Kenya, IPTp2 is at 38% in malaria endemic counties some of the key factors influencing IPTp uptake being SP stock-outs. The national government has been supplying SP but on devolution of health services to county governments it became the responsibility of the counties. There are many competing financial demands at county level and SP stock out is frequent.
 In February 2015 the national government disseminated a memo to county governments advising them to procure SP to avert the worsening SP stock out situation. After issuance of the memo, USAID’S flagship Maternal and Child Survival Program (MCSP) held discussions with the County Directors of Health (CDHs) and shared the quantification formula for SP requirement for the respective counties.
In February 2015 the national government disseminated a memo to county governments advising them to procure SP to avert the worsening SP stock out situation. After issuance of the memo, USAID’S flagship Maternal and Child Survival Program (MCSP) held discussions with the County Directors of Health (CDHs) and shared the quantification formula for SP requirement for the respective counties.
MCSP advocated for procurement of SP especially during the peak malaria transmission period May-August 2015. The CDHs on realizing the cost was not high made immediate arrangements for procurement of SP.
Bungoma County procured enough SP tablets to cover the peak malaria transmission season and distributed them to the health facilities. Results on analysed ANC data from facilities showed that the number of pregnant women accessing IPTp had reduced from 7,845 in October 2014 to 3,856 in February 2015.
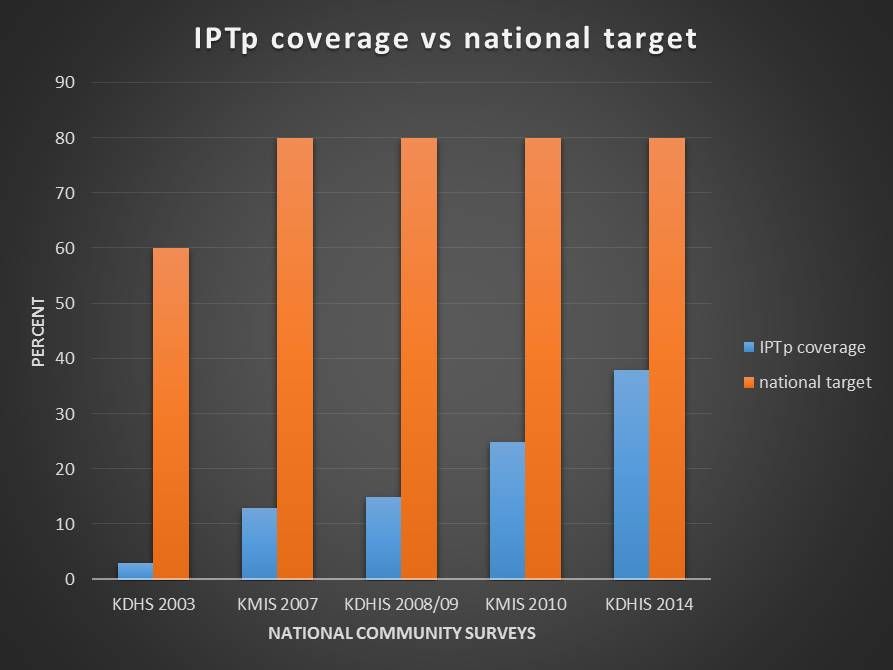 One month after procurement and distribution of SP, the number accessing SP increased from 3,856 to 6,769. To improve pregnancy outcomes in malaria endemic areas it is vital to reduce the effects of malaria during pregnancy. Use of IPTp-SP during pregnancy has been shown to improve pregnancy outcomes however, coverage rates of the intervention have remained below the national target due to several influencing factors like the SP stock-out situation experienced in Kenya.
One month after procurement and distribution of SP, the number accessing SP increased from 3,856 to 6,769. To improve pregnancy outcomes in malaria endemic areas it is vital to reduce the effects of malaria during pregnancy. Use of IPTp-SP during pregnancy has been shown to improve pregnancy outcomes however, coverage rates of the intervention have remained below the national target due to several influencing factors like the SP stock-out situation experienced in Kenya.
The use of advocacy with relevant authorities in Bungoma County leading to improvement in the SP stock out situation is considered a best practice in ensuring health commodity security and is being replicated in other malaria endemic counties.
[1] Augustine M. Ngindu, Gathari G. Ndirangu, Wekesa Kubasu, Isaac M. Malonza
Malaria in Pregnancy &Quality of Services Bill Brieger | 26 Oct 2015
Institutionalization of Quality of Care in Health Facilities Improves Management of Malaria in Pregnancy in Tanzania
Jasmine W. Chadewa and Rita Mutayoba of Jhpiego’s Dar es Salaam, Tanzania, office are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Tuesday 27th October 2015. Please stop by Poster 680 and discuss the results as presented in the Abstract below.
 Malaria in Pregnancy (MiP) is one of the contributors to maternal mortality in Tanzania which persists at a ratio of 410/100,000 live births. Tanzania implements WHO’s three-pronged approach to prevent MiP (use of insecticide treated bednets (ITNs), intermittent preventive treatment (IPTp) with sulfadoxine-pyrimethamine (SP) and prompt diagnosis and treatment).
Malaria in Pregnancy (MiP) is one of the contributors to maternal mortality in Tanzania which persists at a ratio of 410/100,000 live births. Tanzania implements WHO’s three-pronged approach to prevent MiP (use of insecticide treated bednets (ITNs), intermittent preventive treatment (IPTp) with sulfadoxine-pyrimethamine (SP) and prompt diagnosis and treatment).
Efforts are ongoing to improve IPTp and ITN coverage which is 33% and 75%, respectively. Jhpiego, in collaboration with the Ministry of Health and Social Welfare, worked in 251 health facilities to improve the quality of maternal and neonatal health by building the capacity of health care providers through training, supportive supervision, mentoring and coaching. A total of 7,181 providers and 400 tutors were trained on MiP prevention and treatment.
A quality of care study used the same methodology and sampling approach in 2010 and 2012, combining observations of women during antenatal care, inventory and record review as well as health worker knowledge. A team of MNH experts underwent clinical updates, training and orientation to the study tools.
 Data collection teams visited facilities, made observations and entered data into smart phones. The study was conducted in 12 regional hospitals and 38 lower level facilities in 12 regions including Zanzibar with a total of 391 and 366 ANC observations made in 2010 and 2012, respectively.
Data collection teams visited facilities, made observations and entered data into smart phones. The study was conducted in 12 regional hospitals and 38 lower level facilities in 12 regions including Zanzibar with a total of 391 and 366 ANC observations made in 2010 and 2012, respectively.
Between 2010 and 2012, the percentage of women receiving an ITN increased by 26% (p value = <0.0001). The change observed was due to a 33% increase in offering ITN vouchers at health centers and dispensaries. A slight improvement was seen in provision of IPTp(SP) from 62% in 2010 to 65% in 2012.
In Tanzania, application of the quality improvement approach contributed to improving MiP services. Moving forward, there is a need for the Ministry to continue strengthening ANC with effective monitoring and routine supervision to increase coverage of MiP prevention. Districts management teams and facilities need to ensure availability of SP and provide regular technical updates on the national service standards including counseling at ANC and birth preparedness.
Malaria in Pregnancy &Performance Bill Brieger | 26 Oct 2015
Health Systems Strengthening: Improving quality of services for prevention of malaria in pregnancy through the Standards-Based Management and Reward approach in Kenya
Colleagues[1] from the USAID-MCSP Project and Jhpiego (an affiliate of the Johns Hopkins Bloomberg School of public Health) are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Monday 26th October 2015. Please stop by Poster 385 and discuss the results as presented in the Abstract below
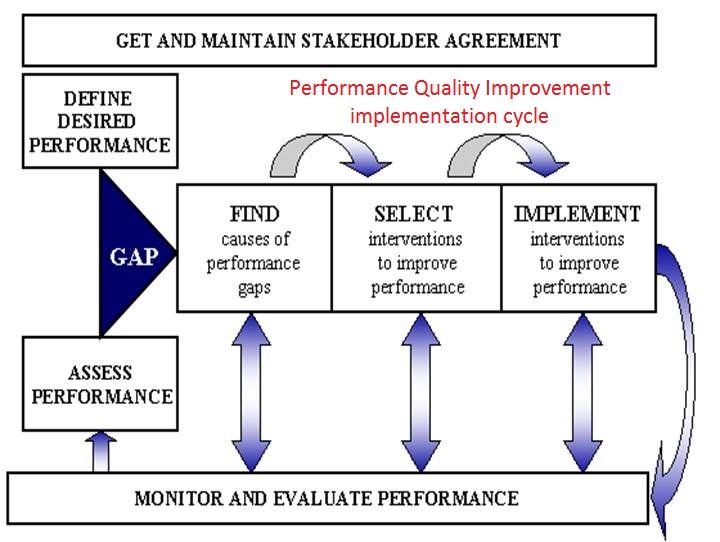 Performance quality improvement (PQI) is one of Jhpiego’s 9 health systems strengthening components in provision of health services towards improvement of maternal health including better pregnancy outcomes. The Standards-Based Management and Reward (SBM-R) approach has been used in improving as well as assessing the quality of services provided at health facilities.
Performance quality improvement (PQI) is one of Jhpiego’s 9 health systems strengthening components in provision of health services towards improvement of maternal health including better pregnancy outcomes. The Standards-Based Management and Reward (SBM-R) approach has been used in improving as well as assessing the quality of services provided at health facilities.
Kenya developed 15 malaria in pregnancy (MIP) SBM-R standards for use by service providers in provision of MIP services and is also used by supervisors to assess the quality of services provided at service delivery points. Facility incharges were trained on the 15 MIP SBM-R performance standards and they oriented service providers in their facilities on use of the performance standards.
 A baseline on SBM-R practices was done in all facilities before orientation in Kakamega east and Kakamega central subcounties and 1st assessment on practices done after three months of practice. A total of 30 health facility incharges from the two malaria endemic subcounties (Kakamega east 16 Kakamega central 14) were trained on the 15 MIP SBM-R performance standards.
A baseline on SBM-R practices was done in all facilities before orientation in Kakamega east and Kakamega central subcounties and 1st assessment on practices done after three months of practice. A total of 30 health facility incharges from the two malaria endemic subcounties (Kakamega east 16 Kakamega central 14) were trained on the 15 MIP SBM-R performance standards.
The facility incharges oriented 291 service providers (127 Kakamega east, 164 Kakamega central) on use of SBM-R performance standards in provision of MIP services in health facilities. Baseline assessment had an average score of 57% for Kakamega east and 58% for Kakamega central.
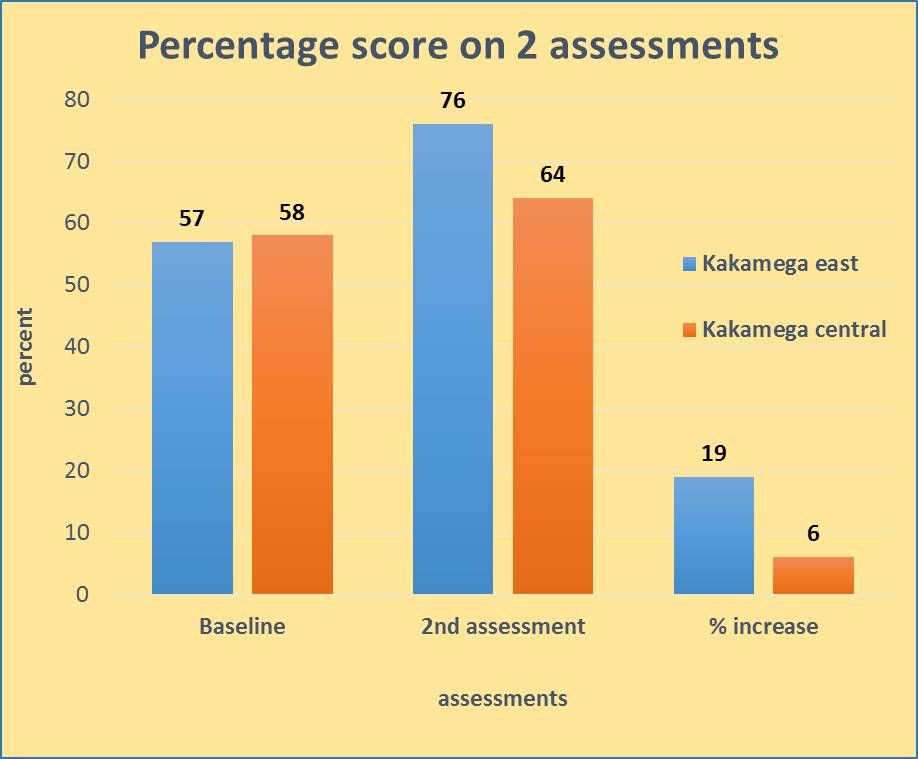 1st assessments were conducted after three months of practice and showed an average score of 76% for Kakamega east and 64% for Kakamega central giving an overall increase in score of 19% and 13% between baseline and 1st assessment for Kakamega east in Kakamega central respectively.
1st assessments were conducted after three months of practice and showed an average score of 76% for Kakamega east and 64% for Kakamega central giving an overall increase in score of 19% and 13% between baseline and 1st assessment for Kakamega east in Kakamega central respectively.
Use of MIP SBM-R performance standards ensures services provided at health facility level are in line with WHO recommendations and national guidelines. Establishment of PQI as a health systems strengthening component is feasible and is an approach that would make available quality MIP services at facility level. Provision of quality MIP services ensures protection of pregnant women against the effects of malaria in pregnancy.
[1] Augustine M. Ngindu, Gathari Ndirangu, Sanyu N. Kigondu, Isaac M. Malonza
Epidemiology &Malaria in Pregnancy Bill Brieger | 25 Oct 2015
Prevalence and Factors Associated with Malaria in Pregnancy in Rural Rwandan Health Facilities: A Cross-sectional Study
Colleagues[1] from the Rwanda Ministry of Health, Jhpiego and the Johns Hopkins Bloomberg School of public Health are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Monday 26th October 2015. Please stop by Poster 315 and discuss the results as presented in the Abstract below.
Malaria in pregnancy (MIP) is a serious health risk for the pregnant woman and fetus and associated 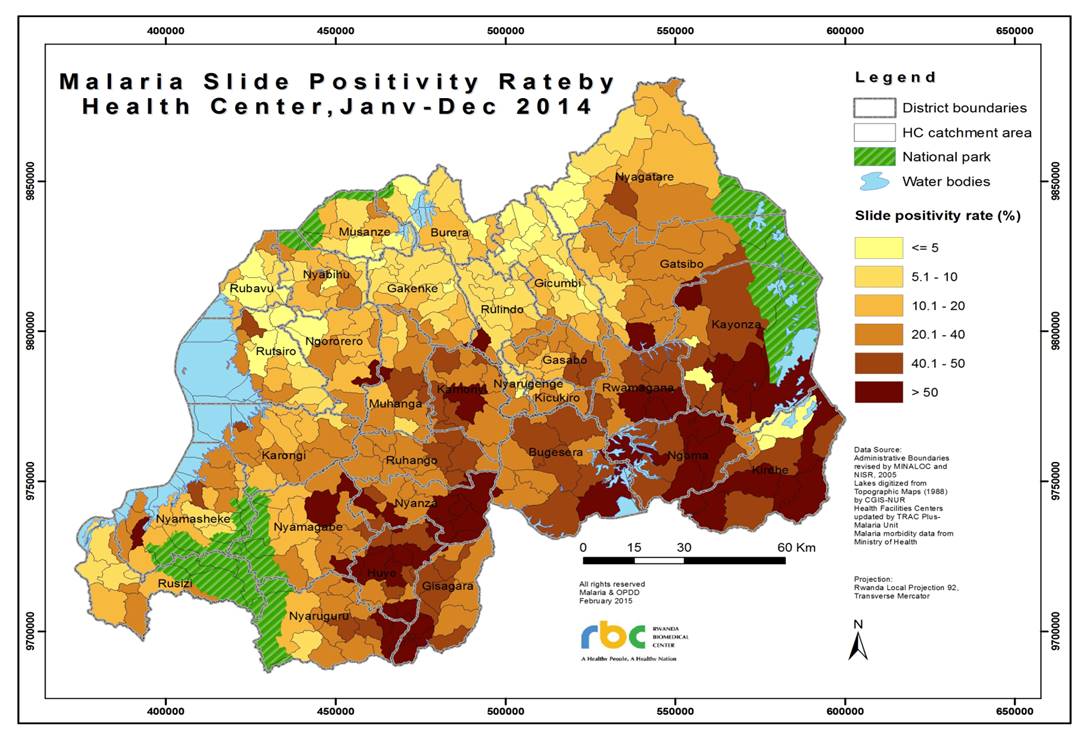 with mortality in the perinatal period. In Rwanda there has been no accurate national estimate of malaria prevalence among pregnant women. In 2011, a cross-sectional study of 6 districts in 3 malaria transmission zones (low, medium and high) in Rwanda was conducted to estimate the prevalence of peripheral parasitemia in pregnant women. Data were collected from consenting women presenting to antenatal clinics (ANC) for the first time in their current pregnancy including age, parity, gestation, ITN availability and use.
with mortality in the perinatal period. In Rwanda there has been no accurate national estimate of malaria prevalence among pregnant women. In 2011, a cross-sectional study of 6 districts in 3 malaria transmission zones (low, medium and high) in Rwanda was conducted to estimate the prevalence of peripheral parasitemia in pregnant women. Data were collected from consenting women presenting to antenatal clinics (ANC) for the first time in their current pregnancy including age, parity, gestation, ITN availability and use.
Blood was obtained for malaria testing using microscopy, rapid diagnosis tests and polymerase chain reaction (PCR). A total of 4,037 pregnant women were recruited with median age of 27 years, and 3,781 (93.7%) had usable PCR samples. The prevalence of MIP by PCR was 5.6%.
 Nearly 20% of women’s families did not have a net, and 8.7% of these tested positive compared to 4.9% of women whose family owned an ITN. For those who did not sleep under an ITN the previous night, 8.1% tested positive compared with 4.8% who slept under an ITN. Malaria prevalence by parity ranged from 5.5% (parity 0-1), to 5.4% (parity 2-3), and 6.5% (parity 4 or more). The two districts that bordered highly endemic countries had MIP prevalence rates of 10% and above. Those testing positive were treated according to national guidelines.
Nearly 20% of women’s families did not have a net, and 8.7% of these tested positive compared to 4.9% of women whose family owned an ITN. For those who did not sleep under an ITN the previous night, 8.1% tested positive compared with 4.8% who slept under an ITN. Malaria prevalence by parity ranged from 5.5% (parity 0-1), to 5.4% (parity 2-3), and 6.5% (parity 4 or more). The two districts that bordered highly endemic countries had MIP prevalence rates of 10% and above. Those testing positive were treated according to national guidelines.
Despite a significant decline of 86% in malaria prevalence in the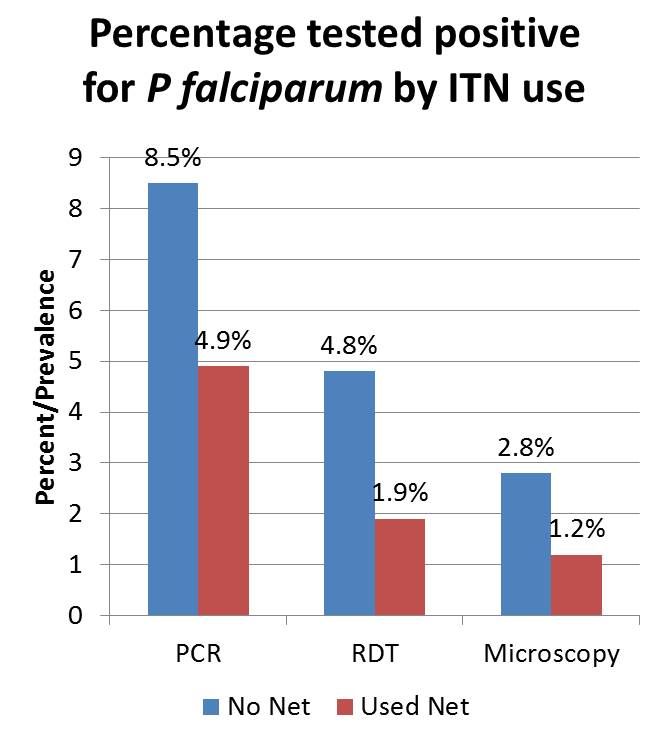 general population from 2005 to 2011, MIP prevalence remains high, especially in border districts. Our study also showed that ITN ownership and use among these pregnant women is below the national target. In order to address this gap, ITN distribution to achieve universal access, and educational campaign targeted at pregnant women on the use of ITN are recommended. Furthermore, early detection and treatment of MIP at ANC and regional collaboration to reduce cross-border malaria transmission should be prioritized.
general population from 2005 to 2011, MIP prevalence remains high, especially in border districts. Our study also showed that ITN ownership and use among these pregnant women is below the national target. In order to address this gap, ITN distribution to achieve universal access, and educational campaign targeted at pregnant women on the use of ITN are recommended. Furthermore, early detection and treatment of MIP at ANC and regional collaboration to reduce cross-border malaria transmission should be prioritized.
————————–
[1] Corine Karema, William R. Brieger, Irenee Umulisa, Aline Uwimana, Jeremie Zoungrana, Beata Mukarugwiro, Rachel Favero, Elaine Roman, Barbara Rawlins, Tharcisse Munyaneza, Fidele Ngabo, David Sullivan, Jean Baptiste Mazarati, Rukundo Alphonse, Agnes Binagwaho
Congenital Malaria &Elimination &IPTp &Malaria in Pregnancy Bill Brieger | 25 Jun 2015
Congenital malaria: A neglected global health concern
Reena Sethi, DrPH Candidate in International Health, The Johns Hopkins Bloomberg School of Public Health and Senior Monitoring and Evaluation Adviser, Jhpiego shares with us the challenges of malaria acquired from the pregnant mother by their newborn child.
 Strategies and recommendations to prevent the transmission of HIV from a mother to her child are known but less information is available on the epidemiology and management of malaria transmitted from pregnant women to their newborns. As presented in a review of congenital infections, one of the lesser known effects of malaria in pregnancy is the maternal-fetal transmission of infected erythrocytes that can result in poor perinatal outcomes. While clinical malaria in newborns is rare, most likely due to the transplacental transfer of maternal antibodies and the inhibitory effect of fetal hemoglobin on the development of malaria parasites, it is unclear what the true incidence of this condition is in Africa and Asia.
Strategies and recommendations to prevent the transmission of HIV from a mother to her child are known but less information is available on the epidemiology and management of malaria transmitted from pregnant women to their newborns. As presented in a review of congenital infections, one of the lesser known effects of malaria in pregnancy is the maternal-fetal transmission of infected erythrocytes that can result in poor perinatal outcomes. While clinical malaria in newborns is rare, most likely due to the transplacental transfer of maternal antibodies and the inhibitory effect of fetal hemoglobin on the development of malaria parasites, it is unclear what the true incidence of this condition is in Africa and Asia.
Recently published studies in Burkina Faso estimated the incidence of congenital malaria to be 2.1% and the prevalence of mother-to-child transmission of asymptomatic malaria to be 18.5% in one health center in Ouagadougou; in one hospital in Papua, Indonesia, congenital malaria was said to occur in 8 out of 1000 live births from 2005 to 2010; and in a study in one hospital in Madhya Pradesh, India, the incidence of congenital malaria was 29 out of 1000 live births. In a study involving six hospitals in Nigeria, the overall incidence of congenital malaria was found to be 5.1%. Transmission has been associated with both Plasmodium falciparum and Plasmodium vivax. The uncertainty and variation in estimates are likely related to the source of the tested blood (umbilical cord blood or infant peripheral blood), presentation of symptoms that are similar to neonatal sepsis, as well as the lack of capacity to conduct high quality diagnostic tests.
Since congenital malaria results from the transmission of parasites from the mother to the baby (presumably through placental transmission), prevention of malaria through the use of IPTp when appropriate reduces maternal parasitemia, most likely resulting in a lower rate of transmission of malaria to the newborn. In a study in Côte d’Ivoire, factors that protected mothers from placental malaria parasitaemia were the use of IPTp (SP) or ITNs during pregnancy and multigravidity. A study in Ibadan, Nigeria found that IPT-SP was effective in preventing maternal and placental malaria as well as improving pregnancy outcomes among parturient women. Researchers in Southern Ghana reported that placental malaria decreased after the implementation of IPTp.
However, in settings where IPTp is ineffective, the effect of alternative strategies, such as intermittent screening and testing in pregnancy (ISTp) on placental malaria should be examined. Little evidence is currently available on the efficacy of ISTp on maternal and newborn outcomes.
Further research also needs to be conducted in diverse settings to develop a standardized definition for congenital malaria and to understand the short and long-term consequences of this condition in order to establish guidelines for diagnosis and treatment. In pre-elimination contexts, where acquired malaria immunity may be reduced, further evidence is needed on the feasibility of screening all febrile babies and following newborns born to women with malaria during pregnancy and of other possible strategies to improve infant outcomes.
IPTp &Malaria in Pregnancy Bill Brieger | 23 Apr 2015
Burkina Faso: Defeating Malaria by Investing in Expanding Intermittent Preventive Treatment in Pregnancy
 In Burkina Faso, Antenatal Care (ANC) is a national platform for malaria in pregnancy prevention and control. The 2010 Demographic and Health Survey showed a good initial ANC registration rate (95%), but over 56% of pregnant women in rural areas do not register until their second or third trimester. Thus they may have missed the full regimen of ANC services including Long Lasting Insecticide-treated nets and intermittent preventive treatment of malaria in pregnancy (IPTp).
In Burkina Faso, Antenatal Care (ANC) is a national platform for malaria in pregnancy prevention and control. The 2010 Demographic and Health Survey showed a good initial ANC registration rate (95%), but over 56% of pregnant women in rural areas do not register until their second or third trimester. Thus they may have missed the full regimen of ANC services including Long Lasting Insecticide-treated nets and intermittent preventive treatment of malaria in pregnancy (IPTp).
In 2010 only 10.6% of pregnant women nationally and 8.4% in rural areas received two doses of IPTp. Now WHO recommends more doses. This had improved by the time the 2014 Malaria Information Survey was completed to 68% for one dose, 48% for two and 22% for three doses.
Jhpiego’s USAID-supported Improving Malaria Care (IMC) project in Burkina Faso has been providing technical assistance and training to health districts and their ANC staff on implementing updated (2012) WHO IPTp guidelines. The recommended provision of IPTp at every ANC visit from the 13th week of pregnancy onward leads to the possibility of 3 or more doses per woman. The new guidance was incorporated into the update of Burkina Faso’s malaria strategy and has been disseminated since September 2014.
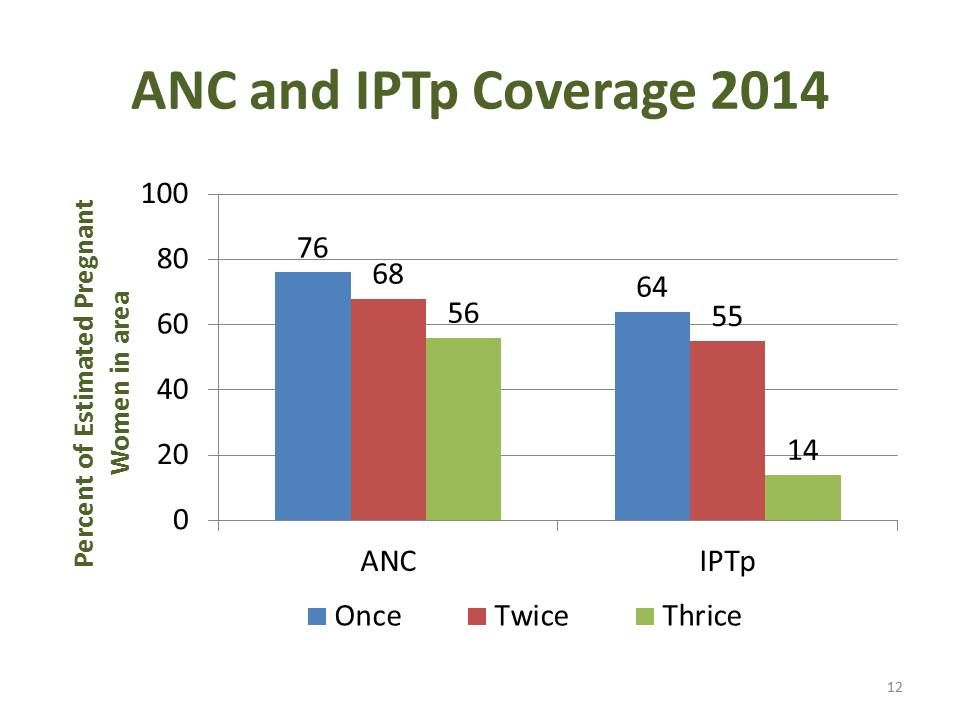 Annual data from the Health Management and information System for 2014 from three districts (Batie, Po and Ouargaye) and 61 health clinics where IMC has been working were collected and summarized. A total of 26,909 women registered for ANC our of the estimated 35,420 in the Three districts.
Annual data from the Health Management and information System for 2014 from three districts (Batie, Po and Ouargaye) and 61 health clinics where IMC has been working were collected and summarized. A total of 26,909 women registered for ANC our of the estimated 35,420 in the Three districts.
The chart at the left shows coverage of ANC visits and IPTp provision based on the estimated 2014 population of pregnant women in the districts. Eleven (17.7%) clinics had not started the updated IPTp guidance. The Ministry of Health also experienced stock-outs of sulfadoxine-pyrimethamine.
Being new IPTp3+ poses challenges and needs greater investment. The IMC project in collaboration with the National Malaria Control Program is examining ways to invest in stronger antenatal malaria prevention including capacity building for ANC staff and provision of IPTp by the existing network of volunteer community health workers.