Elimination &Research Bill Brieger | 30 May 2014
New operational research projects in malaria elimination
 Kate Whitfield is sharing with us the following information about MESA‘s operational research …
Kate Whitfield is sharing with us the following information about MESA‘s operational research …
New operational research projects in malaria elimination started in April 2014, after being selected for funding through MESA (the Malaria Eradication Scientific Alliance).
 The MESA operational research portfolio includes: proof-of-concept of novel vector control and diagnostic tools, use of mapping technologies for surveillance and tailored response, and mobile phone applications for hard to reach populations. Urban, rural and forest settings are addressed. The projects are summarised below …
The MESA operational research portfolio includes: proof-of-concept of novel vector control and diagnostic tools, use of mapping technologies for surveillance and tailored response, and mobile phone applications for hard to reach populations. Urban, rural and forest settings are addressed. The projects are summarised below …
- Mopping up and getting to zero: mapping residual malaria transmission for targeted response in urban Lusaka, Zambia.
- Using voice]based technology to improve access to malaria care and treatment among high risk mobile population of forest goers in Cambodia.
- Applying novel nucleic acid surveillance to malaria elimination in South Cotabato Province, Mindanao, The Philippines.
- Efficacy and safety of high]dose ivermectin in reducing malaria transmission.
 inety-one proposals were submitted to the call and after a thorough review process with an independent Peer Review Panel, 4 were selected for funding. The Peer Review Panel was composed of 12 experts from all over the globe. You can find a schematic of the review process through this link.
inety-one proposals were submitted to the call and after a thorough review process with an independent Peer Review Panel, 4 were selected for funding. The Peer Review Panel was composed of 12 experts from all over the globe. You can find a schematic of the review process through this link.
MESA (the Malaria Eradication Scientific Alliance) follows-up on the mal ERA agenda and provides a dedicated platform for the community in order to accelerate the translation of the science of malaria eradication for impact.
ITNs &Malaria in Pregnancy Bill Brieger | 26 May 2014
Women’s Education and Bed Net Use in Nigeria
Concern about women’s and girl’s education in Nigeria and worldwide has peaked with the abduction of around 300 female secondary school school students in northeastern Nigeria. Normally we see many positive benefits of women’s education in various health indicators, but it appears that bednet use does not follow that trend neatly.
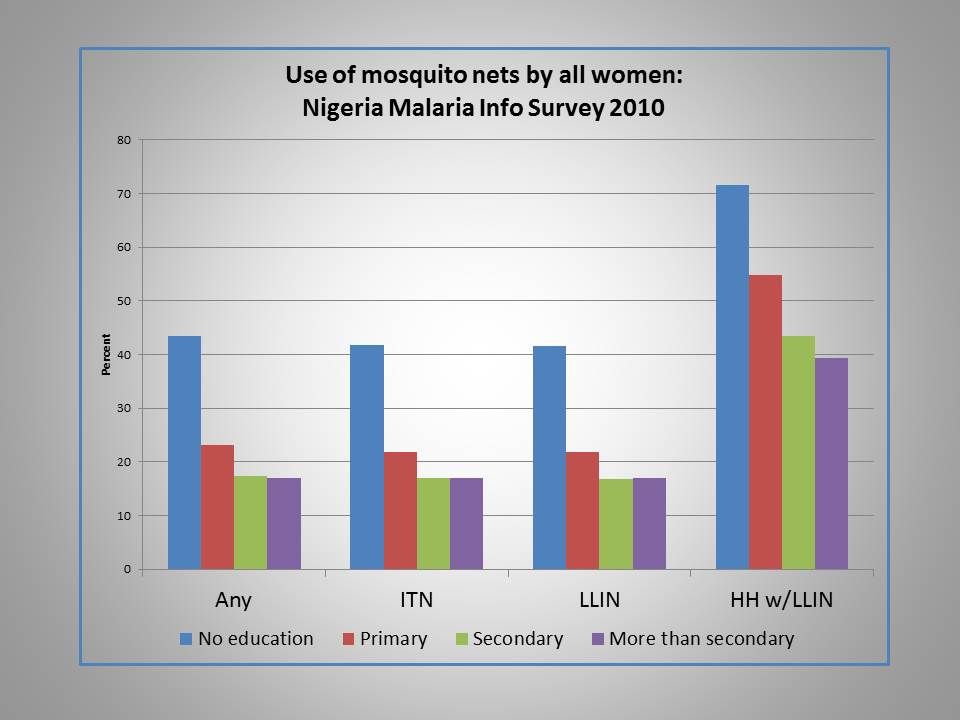 Analysis of bednet use in the Nigeria Malaria Indicator Survey (MIS) of 2010 found that ironically net use of all kinds, including ordinary nets, insecticide treated nets and long lasting insecticide-treated nets actually decreased as educational level of women increased.
Analysis of bednet use in the Nigeria Malaria Indicator Survey (MIS) of 2010 found that ironically net use of all kinds, including ordinary nets, insecticide treated nets and long lasting insecticide-treated nets actually decreased as educational level of women increased.
Interestingly the same picture is painted for levels of wealth with 41% in the lowest quintile using any kind of net the night before the survey versus 16% for the highest quintile. Also of note, 19% of urban women reported using any kind of net versus 34% in the rural areas.
In contrast the 2010 Nigerian MIS found that only 22% of women without education had received any antenatal care (ANC) during a recent pregnancy compared to 89% with greater than secondary education. Getting at least two doses of intermittent preventive treatment (IPTp) during ANC was only 7% for those without formal education, but 24% for those with higher than secondary education. Why does bednet use show a reverse trend here?
One factor may be the delivery mechanism. ANC and IPTp require utilization of a service with all the economic and intra-family dynamics that this implies. Nets have so far been mainly provided during outreach campaigns. Is there an element of equity going on here with an effort to reach the less educated and poorer segment of society with nets?
Also educated people and those with relatively greater wealth may have better housing conditions that are less likely to encourage mosquito entry. Such families may perceive that they have less need for nets if they actually have ceilings and windows with netting.
Just by way of comparison, a similar picture of net use was was seen in the Malawi MIS of 2012. That survey only recorded three levels of education and the contrast between highest and lowest use was only about 10% points compared to 25% difference in Nigeria.
Colleagues have recently documented gaps in net access and use across many countries. We need to ensure not only that nets reach a house, but that adequate numbers of nets are available for universal coverage (UC = at least one for every two residents – though this adequacy calculation depends on cultural sleeping patterns).
Malaria control efforts since 2009 have been aiming at UC, but various surveys have shown this goal to be elusive, let alone sustainable, since nets need to be replaced every 2-3 years. It is encouraging if some element of equity might underlie net distribution, but we still need to learn more about why people get and use nets or alternatives to ensure that all women and other household members are truly protected from malaria.
Epidemiology &Mapping &water Bill Brieger | 23 May 2014
Satellite Mapping, an important step toward malaria control and elimination in Nigeria
Omede Ogu of Nigeria’s Federal Ministry of Health reports on efforts to undertake mapping of malaria in the country as a basis for better planning of control and eventual elimination efforts.
 The National Malaria Elimination Program (NMEP) has been meeting with the team from the National Space Research and Development Agency (NASRDA). Progress on pilot malaria mapping in Niger State is being reviewed, though the study is yet to be concluded. NMEP is also looking at opportunities that exist to expand their initial mapping to cover the whole of the country. Discussions are underway on next steps and development of a road map or a framework for the study going forward.
The National Malaria Elimination Program (NMEP) has been meeting with the team from the National Space Research and Development Agency (NASRDA). Progress on pilot malaria mapping in Niger State is being reviewed, though the study is yet to be concluded. NMEP is also looking at opportunities that exist to expand their initial mapping to cover the whole of the country. Discussions are underway on next steps and development of a road map or a framework for the study going forward.
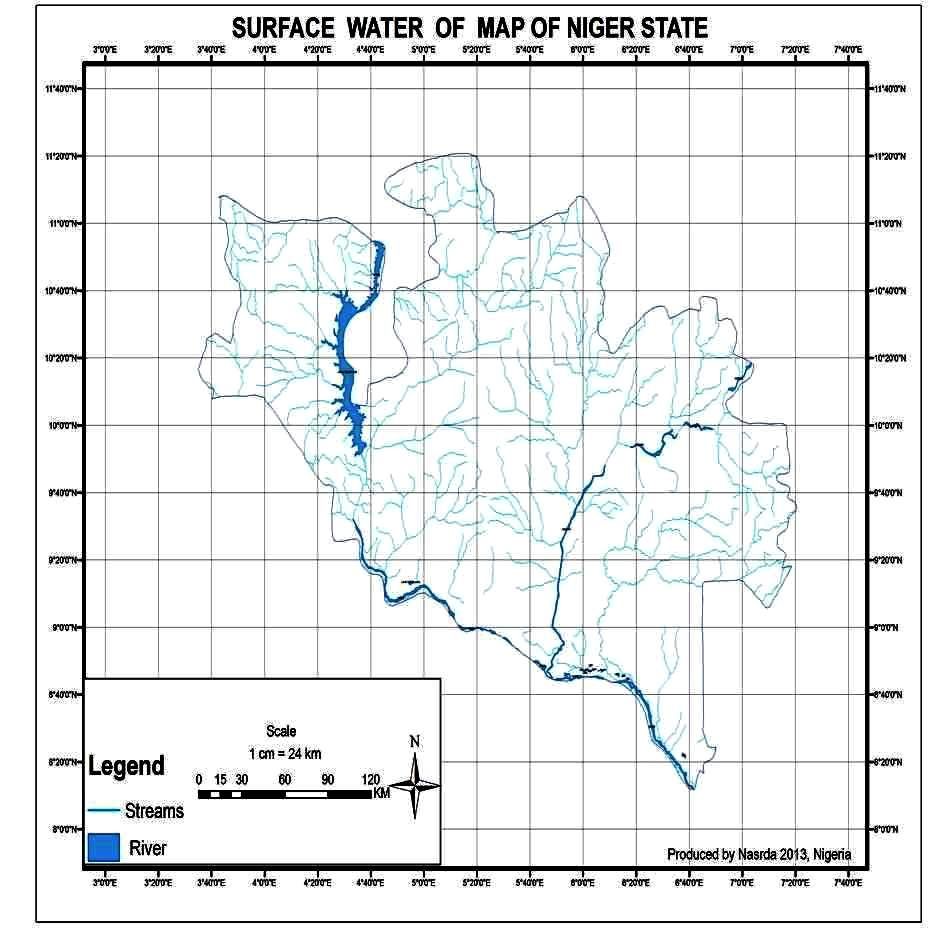
NASRDA explained that the current mapping effort was aimed is to use satellite-based technology to map surface water for Malaria Control in North-central Nigeria with Niger State as a Pilot study. They noted that data in inaccessible locations such as the marshy areas, thick forests, rugged terrain etc. were previously unavailable for relevant environmental policy and decision making in the region and Nigeria.
In addition is will be possible to do infrastructural mapping and inventory of health care facilities, in order to identify and assess the state of health care facilities, how accessible and future areas of need provision of these facilities in the country.
So far NASRDA has identified settlements, and locations of hospitals and health centres throughout Niger State using Global Positioning System (GPS). They have also identified water bodies and wetlands locations throughout the state.
Finally they are developing a map of Surface Water and wetlands in the state showing these in relation to locations of settlements, hospitals and health centres. NMEP is planning to link with colleagues doing similar mapping in Kenya.
NMEP plans to have the final report of the study ready by October for dissemination. Major partners with funding lines in their 2014 work plans for this study are the National Primary Health Care Development Agency (NPHCDA) and NASRDA. Additional funding and support is being sought.
Kenya already is using its mapping to focus appropriate malaria interventions. All countries will benefit in better mapping for targeting their malaria control and elimination efforts.
Indoor Residual Spraying &Integrated Vector Management &Mosquitoes Bill Brieger | 21 May 2014
Indoor Residual Spraying – not a one-trick pony
Jasson Urbach and Donald Roberts claim that the malaria fight is hurt by flimsy anti-DDT research as they opine in Business Day (South Africa) on 9th May 2014. They are particularly exercised by an article on possible DDT effects on bird egg shells. Despite the controversy sparked by the article, there is no evidence that any individual country nor WHO itself is recommending removal of DDT from the arsenal of chemicals used in indoor residual spraying (IRS) to control malaria.

PMI: http://www.pmi.gov/how-we-work/technical-areas/indoor-residual-spraying
There is something about DDT that raises hackles among proponents and detractors. But malaria vector control planners do have choices. WHO recommends 14 insecticides for indoor residual spraying against malaria vectors as seen below in an list updated on 25 October 2013:
- DDT
- Malathion
- Fenitrothion
- Pirimiphos-methyl
- Pirimiphos-methyl
- Bendiocarb
- Propoxur
- Alpha-cypermethrin
- Bifenthrin
- Cyfluthrin
- Deltamethrin
- Deltamethrin
- Etofenprox
- Lambda-cyhalothrin
Ironically DDT tops the list. No chemical is 100% safe, so the caveat with any of these chemicals is that, “WHO recommendations on the use of pesticides in public health are valid ONLY if linked to WHO specifications for their quality control. WHO specifications for public health pesticides are available on the Internet.
Interestingly, a bigger concern should be the potential for mosquitoes to develop resistance to any of the above mentioned insecticides. This is why it is important to avoid putting all our eggs – soft or hard shelled – in one basket. Ideally insecticides should be rotated often to prevent resistance from developing.
Decisions to embark on IRS and choice of insecticides should be based on national and sub-national environmental and epidemiological characteristics, not emotional attachment to any particular product.
Communication &Education Bill Brieger | 19 May 2014
Educating the Media on Malaria Control
The mass media – electronic, print and now social – play an important role in the fight against malaria. The media reach diverse audiences from villagers to policy makers. Because of their potential influence, the media must have the story right when it comes to malaria.
 A news story published online this morning from a highly malaria-endemic country shows how some subtle but important mistakes can give wrong impressions and lead to wrong actions. The fact that the information is attributed to “medical science experts” does not mean that the reporters quoted them in the correct context.
A news story published online this morning from a highly malaria-endemic country shows how some subtle but important mistakes can give wrong impressions and lead to wrong actions. The fact that the information is attributed to “medical science experts” does not mean that the reporters quoted them in the correct context.
The first example from the story is, “Spending on malaria and dengue fever treatment programmes should be controlled, with more efforts directed to preventive measures …” As a disease caused by a virus, dengue does not have a definitive treatment, if by treatment we mean a cure.
Life saving palliative care is important in dengue, but dengue in Africa usually goes undiagnosed and is unfortunately often treated by wasting malaria drugs. The issue is not reducing treatment funds, but using rapid diagnostic tests so that we will not waste our expensive malaria medicines on non-malarial fevers.
The article next talks about how scientists in the country, “are advising the government to authorise controlled use of the banned pesticide DDT to strengthen mosquito eradication and bite control programmes in the country.” DDT has been used for indoor residual spraying against the malaria carrying anopheles mosquitoes. This fits into the anopheles behavior of resting on walls after biting.
By contrast dengue is carried by Aedes aegypti mosquitoes. They are the ones that breed in pots, tins, etc. around the house, and DDT is not a major part of the efforts to control them. Household members are responsible for removing or not even allowing such small collections of water to occur in their houses, on their property and among their neighbors.
A final odd claim is that, “Donor funded health programmes are disadvantaged because the in-country implementers ‘accept each and every thing directed to them by the donors without challenging their ideas.’” For the biggest malaria funding programs this is not true. The Global Fund for years has required that countries submit their own proposals that were developed and passed through their own national country coordinating mechanisms.
Now Global Fund is requiring countries to submit their own national malaria strategies as a basis for funding. The Global Fund is a financial organization, not a technical one, and thus is not directing countries what to do other that spend their money well on scientifically sound interventions.
Other donors work together with national malaria control programs and their partners to develop country specific and relevant operational plans. Donors do encourage countries to implement scientifically proven guidance that is developed by international technical committees whose members include scientists from endemic countries.
The points above could create unfortunate misunderstandings by the public (about insecticides), professionals (about treatment) and policy makers (about donor support). The media should foster appropriate and timely action against malaria, not confuse the public.
Burden &Malaria in Pregnancy &NCDs Bill Brieger | 16 May 2014
Malaria, Hypertension and Pregnancy: where communicable and non-communicable diseases may cross paths
 Tomorrow, May 17th, is World Hypertension Day. Much attention of recent has been focused on the importance of non-communicable diseases (NCDs) like hypertension in terms of global burden, and concerns have been expressed that communicable or infectious diseases (CDs) may become neglected, although they still cause huge levels of morbidity and mortality. What people may not realize is that there are connections between the NCDs and the CDs.
Tomorrow, May 17th, is World Hypertension Day. Much attention of recent has been focused on the importance of non-communicable diseases (NCDs) like hypertension in terms of global burden, and concerns have been expressed that communicable or infectious diseases (CDs) may become neglected, although they still cause huge levels of morbidity and mortality. What people may not realize is that there are connections between the NCDs and the CDs.
 Better research is needed to document the relationships and influences of one on the other, but some preliminary work has been done with pregnant women who are susceptible to both hypertension and malaria. What does that combination do?
Better research is needed to document the relationships and influences of one on the other, but some preliminary work has been done with pregnant women who are susceptible to both hypertension and malaria. What does that combination do?
What the existing literature implies so far is that malaria in pregnancy may in fact be associated with hypertension in some cases and that both conditions can lead to intra-uterine growth retardation and low birth weight. Also boys who were born to mothers with malaria in pregnancy had excess hypertension in their first year of life and girls had higher SBP.
 The role of malaria in pregnancy in low birth weight is well established. Furthermore Lackland and colleagues shared that, “there have been numerous ecologic and observational studies that identified significant inverse associations of birth weight with blood pressure levels at various ages in later life.” A graphic posted to the right shows potential malaria and hypertension interactions. These are areas that deserve more observation, documentation and research.
The role of malaria in pregnancy in low birth weight is well established. Furthermore Lackland and colleagues shared that, “there have been numerous ecologic and observational studies that identified significant inverse associations of birth weight with blood pressure levels at various ages in later life.” A graphic posted to the right shows potential malaria and hypertension interactions. These are areas that deserve more observation, documentation and research.
Overall we can see that there is not a real dichotomy between CDs and NCDs, and both interact in the health of individuals, families and communities.
Community Bill Brieger | 12 May 2014
Community case management – in the community or of the community?
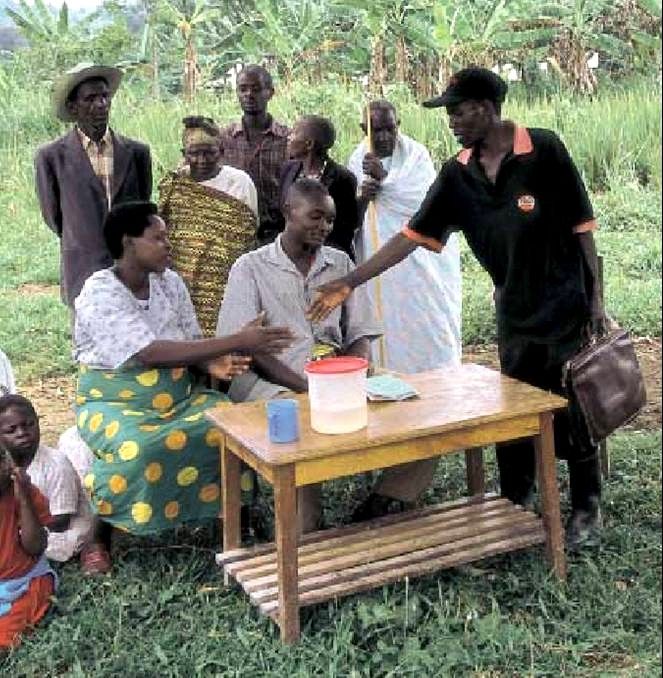
In response to sharing of the following article: “Community case management of malaria: exploring support, capacity and motivation of community medicine distributors in Uganda” by Banek et al., a colleague responded that it, “confirms what is known from ever: communities do not sustain their CHWs. When the INGO (international NGO) withdraws, CHWs drop their tools, this is history.”
 The article itself, a qualitative assessment of community medicine distributors (CMDs) from a program of home/community based management (HBM) of malaria in Uganda that was started around 2002, did paint a bleak picture of volunteer motivation, support and supervision. Unfortunately the article focused either on the motivation of the individual CMDs or on the health system and its employees. We do not come away from reading this article with an understanding of the role of the community and why the CMDs felt disappointed at the level of community support they received.
The article itself, a qualitative assessment of community medicine distributors (CMDs) from a program of home/community based management (HBM) of malaria in Uganda that was started around 2002, did paint a bleak picture of volunteer motivation, support and supervision. Unfortunately the article focused either on the motivation of the individual CMDs or on the health system and its employees. We do not come away from reading this article with an understanding of the role of the community and why the CMDs felt disappointed at the level of community support they received.
In fact community volunteers do not always drop out or if they do, communities can actually replace them if the program is organized well. The African Program for Onchocerciasis Control (APOC) has maintained community distribution of ivermectin since 1997-98 in now over 120,000 villages. The key to the success of community directed distributors (CDDs) of ivermectin was the approach that focused on getting community commitment, not on individual volunteers.
In fact this approach, now know as community directed intervention (CDI) has been found appropriate to delivering a package of simple interventions, including community case management of malaria. What makes the difference in CDI is first the determination of what constitutes a community and secondly that the community itself manages the interventions, not individual volunteers, though CDDs who are selected by the community certainly play a major role.
 First, what is the ‘community?’ Experience with APOC has shown that one needs to consult with local people on the ground to determine what is a community. When program planners, for example, in eastern Nigeria thought lets encourage ‘the community’ to select a couple volunteers, they did not realize that an ‘autonomous community’ or town, while having its own chief and council, was actually made up of 4-6 ‘villages’ of from 1,000 to 5,000 people having their own leaders. If the community/town selected a couple volunteers two problems occurred – 1) the workload was high and CDDs became discouraged and 2) not all villages were represented so villages without CDDs felt neglected and did not participate well.
First, what is the ‘community?’ Experience with APOC has shown that one needs to consult with local people on the ground to determine what is a community. When program planners, for example, in eastern Nigeria thought lets encourage ‘the community’ to select a couple volunteers, they did not realize that an ‘autonomous community’ or town, while having its own chief and council, was actually made up of 4-6 ‘villages’ of from 1,000 to 5,000 people having their own leaders. If the community/town selected a couple volunteers two problems occurred – 1) the workload was high and CDDs became discouraged and 2) not all villages were represented so villages without CDDs felt neglected and did not participate well.
A closer look by sociologists involved in the program learned what was the smallest natural unit of commnuity. They saw that in fact even the villages were made up of kin groups of 100-200 people. Ultimately it was found that selection of CDDs by their kin group worked best. They could be held accountable by close relatives and friends and they would have a manageable volunteer workload.
The supplies needed did not vary much as the population estimates still accounted for the whole town. The design of the training was simplified enough and held in local schools or other public buildings so that costs were minimal. Peer support and meetings at the nearest health facility played an important and low cost function in supervision.
Similar lessons were learned in western Nigeria which had a different settlement pattern based on towns and satellite farm hamlets. As long as family compounds in town (kin groups) and outlying hamlets were directly involved in selecting and supervising their own volunteers, the services were delivered. Communities could chose as many volunteers as they needed, and when additional service components were added, communities could decide to increase the number of CDDs so that no one volunteer was burdened with the whole package.
 A number of articles have arisen from the Uganda home based management of malaria project and work continues with the support of other NGOs and government agencies. What is of interest is the fact that over the history of the work, little has been said about the community. One WHO publication that discussed the early stages mentioned “Selection of distributors in Uganda took place during village council meetings,” but there was also reference to having “at least two distributors in each parish and more in larger communities.”
A number of articles have arisen from the Uganda home based management of malaria project and work continues with the support of other NGOs and government agencies. What is of interest is the fact that over the history of the work, little has been said about the community. One WHO publication that discussed the early stages mentioned “Selection of distributors in Uganda took place during village council meetings,” but there was also reference to having “at least two distributors in each parish and more in larger communities.”
The districts of Uganda are divided into counties which themselves are divided into sub-counties, and are further divided into parishes and villages. It appears that parishes may have several villages, so again it is not clear whether the Uganda HBM project was based on the smallest natural units of community or not.
Banek and colleagues conclude that, “social factors that impact on the implementation of community-based programmes, such as community perceptions and acceptability and community health worker motivation, remain understudied.” The reality is that people in the malaria world have not communicated well with people working on onchocerciasis and NTDs. Had they done so, they would realize that there has been much study on how to set up sustainable volunteer programs in thousands and thousands of villages that put the community in charge. It is not enough to work in the community, the community must be in charge
Borders &Surveillance Bill Brieger | 02 May 2014
Failure of malaria control efforts in northern Zambia

UNICEF, Zambia http://www.unicef.org/zambia/5109_8454.html
World Malaria Day 2014 was observed at the Johns Hopkins Bloomberg School of Public Health on Friday 25 April. 21 posters were presented. Below is the abstract of a third poster presented William Moss and colleagues from the Southern Africa International Centers of Excellence for Malaria Research.
Despite distribution of insecticide-treated bed nets, indoor residual spraying and case management with rapid diagnostic tests and artemisinin-based combination therapy, the burden of malaria remains high in northern Zambia.

RBM Impact Series Zambia http://www.rbm.who.int/ProgressImpactSeries/report7.html
Through passive case detection at health care facilities and active case detection through community-based surveys, we have documented persistently high parasite prevalence in Nchelenge District, Luapula Province, Zambia on the border of Lake Mweru with the Democratic Republic of Congo. Individual and household level risk factors for malaria were assessed and a spatial risk map constructed.
Pyrethroid resistance in local Anopheles funestus populations likely contributes to failure of current control efforts. Potentially contributing to malaria transmission is population movement from the lakeside to inland as fishing and agricultural seasons alternate.
Equally important may be cross-border movement between Nchelenge District, Zambia and Katanga Province in the Democratic Republic of Congo, suggesting the importance of epidemiological and entomological studies of cross-border malaria.
Borders &Surveillance Bill Brieger | 01 May 2014
Resurgent Malaria in Eastern Zimbabwe
 World Malaria Day 2014 was observed at the Johns Hopkins Bloomberg School of Public Health on Friday 25 April. 21 posters were presented. Below is the abstract of another poster presented William Moss and colleagues from the Southern Africa International Centers of Excellence for Malaria Research.
World Malaria Day 2014 was observed at the Johns Hopkins Bloomberg School of Public Health on Friday 25 April. 21 posters were presented. Below is the abstract of another poster presented William Moss and colleagues from the Southern Africa International Centers of Excellence for Malaria Research.
Eastern Zimbabwe has experienced recent large outbreaks of malaria after a history of successful control. Through passive case detection at health care facilities and active case detection through community-based surveys, we have documented seasonal malaria outbreaks in Mutasa District, Manicaland Province, Zimbabwe on the border with Mozambique.
We identified individuals with subpatent parasitemia who may be responsible for sustaining transmission during the dry season.
Pyrethroid resistance in local Anopheles funestus populations likely contributes to failure of current control efforts.
Potentially contributing to malaria transmission is population movement across the border with Mozambique.
* * * * * * *
Of interest, The Standard newspaper of Zimbabwe recently reported on this problem saying that, “Malaria burden remains high in border towns in Zimbabwe, especially in areas close to Mozambique, health experts have said. While the overall national statistics indicate a major decline from 5 000 deaths to 300 per year, border districts like Mudzi are still recording high cases.”
Epidemiology &Surveillance Bill Brieger | 01 May 2014
The feasibility of achieving and sustaining “malaria-free zones” in southern Zambia
World Malaria Day 2014 was observed at the Johns Hopkins Bloomberg School of Public Health on Friday 25 April. 21 posters were presented. Below is the abstract of a poster presented William Moss and colleagues from the Southern Africa International Centers of Excellence for Malaria Research.
 The Government of Zambia is committed to creating “malaria-free zones” in southern Zambia. Through passive case detection at health care facilities and active case detection through community-based surveys, we have documented a dramatic decline in the burden of malaria in the catchment area of Macha Hospital, Choma District, Southern Province, Zambia from 2008 through 2013.
The Government of Zambia is committed to creating “malaria-free zones” in southern Zambia. Through passive case detection at health care facilities and active case detection through community-based surveys, we have documented a dramatic decline in the burden of malaria in the catchment area of Macha Hospital, Choma District, Southern Province, Zambia from 2008 through 2013.

Macha Hospital: https://www.flickr.com/photos/inmed/sets/72157625850417125/
However, residual foci of transmission exist and the potential for repeated importation remains. We identified individuals with subpatent parasitemia and gametocytemia who may be responsible for sustained, low-level transmission and evaluated reactive case detection strategies to identify and treat these individuals using simulation models.
Factors associated with sustained insecticide-treated bed net use were evaluated in light of the declining burden of malaria. Parasite bar coding of 24 SNPs should permit the identification of imported parasites.
Results of a longitudinal analysis of changes in antibody responses to 500 Plasmodium falciparum antigens using a protein microarray should allow detection of residual transmission and document loss of humoral immunity in the absence of exposure.