Innovation &Invest in Malaria Control &Vaccine &World Malaria Day &Zero Malaria Bill Brieger | 25 Apr 2023
World Malaria Day: Investing in Malaria Vaccines
 World Malaria Day 2023 is focusing on three key themes, Investment, Innovation, and Implementation, the 3 I’s. The recently approved malaria vaccines and those still under development embody these themes fully. They all represent decades of investment in innovation, research, and now implementation.
World Malaria Day 2023 is focusing on three key themes, Investment, Innovation, and Implementation, the 3 I’s. The recently approved malaria vaccines and those still under development embody these themes fully. They all represent decades of investment in innovation, research, and now implementation.
After extensive several decades of clinical research and three years of field implementation in Ghana, Malawi, and Kenya by the World Health Organization and National Malaria and Immunization Programs, the RTS,S/AS01 malaria vaccine is being rolled out with assistance of GAVI, the Global Vaccine Alliance. During the malaria vaccine implementation program (MVIP) and also based on GAVI’s philosophy for vaccine programs generally, a key strategy was to provide RTS,S as routine immunization services alongside other essential services including a comprehensive package of malaria control and elimination interventions. RTS,S is not only being made available to the three MVIP countries, but as supplies come on board, other falciparum malaria endemic countries have started to apply for supplies and funding through GAVI.
 It was well known from the beginning that although RTS,s might be first out the gate, other vaccines would be following closely on its heels. The benefits as well as the efficacy limitations of RTS,S were well known. Therefore, talk was common for new products being available by 2026. Now in 2023, countries have started to move ahead on another vaccine candidate.
It was well known from the beginning that although RTS,s might be first out the gate, other vaccines would be following closely on its heels. The benefits as well as the efficacy limitations of RTS,S were well known. Therefore, talk was common for new products being available by 2026. Now in 2023, countries have started to move ahead on another vaccine candidate.
BBC reported that “Ghana is the first country to approve a(nother) new malaria vaccine that has been described as a ‘world-changer’ by the scientists who developed it.” R21 appears to be more effective than its predecessor, so Ghana’s drug regulators moved ahead quickly using final trial data on the vaccine’s safety and effectiveness, which is not even public, to approve it. Interestingly, this move is in parallel to the World Health Organization’s consideration of approving the vaccine. Shortly thereafter, Nigerian medicine regulators also approved R21. Reuters noted that these “approvals are unusual as they have come before the publication of final-stage trial data for the vaccine.” The actual roll out will ultimately depend on official publication of the safety data and sourcing of funds.
 As mentioned above, these malaria vaccines represented considerable investment of time and resources, embody the kind of innovation that is needed to tackle malaria as drug and insecticide resistance threaten progress toward elimination, and require detailed planning right down to the grassroots levels to ensure that a malaria vaccine delivery is part of a comprehensive package of malaria and child health services.
As mentioned above, these malaria vaccines represented considerable investment of time and resources, embody the kind of innovation that is needed to tackle malaria as drug and insecticide resistance threaten progress toward elimination, and require detailed planning right down to the grassroots levels to ensure that a malaria vaccine delivery is part of a comprehensive package of malaria and child health services.
We need to return to the theme of investment. While international organizations, universities, ministries of health, and of course pharmaceutical companies have been investing in developing a safe, effective, and feasible product, these innovative products will not save lives until funds are invested for both purchase and service delivery are guaranteed. GAVI and Partners have put together over $200 million in support for RTS,S implementation for three years. The first window was open in September 2022 for the initial three MVIP countries, and a second window for others, depending on available supplies was open in December 2022.
Investment FOR implementation is a challenging subject because GAVI and collaborating agencies are not a bottomless well of money. What level of national investment by a country to protect its own children is feasible? Is there the national political will to contribute and invest in children in endemic countries, and not continue depending heavily on donors?
Malaria vaccines are a perfect example of what the 3 I’s can achieve. But beyond celebrating this addition to the malaria elimination toolkit, will we also be celebrating commitments by endemic countries of local funds to make zero malaria a reality?
Capacity Building &CHW &Community &Elimination &Health Education &Indoor Residual Spraying &IPTp &ITNs &Malaria in Pregnancy &World Malaria Day &Zero Malaria Bill Brieger | 25 Apr 2021
Twenty Years of Malaria Day Observances: Jhpiego at the Forefront
 In 2001 the first Africa Malaria Day (AMD) was observed. The opportunity to mark progress and exhort increased efforts for the continent continued through 2007. Then in 2008, the concept of World Malaria Day (WMD) took over, though it could not be denied that the bulk of malaria morbidity, mortality and intervention still was focused on African countries. Other countries have made progress such as the recent certification of malaria elimination in Argentina and El Salvador, but twenty years after the first AMD/WMD, Africa is still leading the way for creative, sustained intervention against the disease, despite threats to resources from economic downturns and new pandemic diseases.
In 2001 the first Africa Malaria Day (AMD) was observed. The opportunity to mark progress and exhort increased efforts for the continent continued through 2007. Then in 2008, the concept of World Malaria Day (WMD) took over, though it could not be denied that the bulk of malaria morbidity, mortality and intervention still was focused on African countries. Other countries have made progress such as the recent certification of malaria elimination in Argentina and El Salvador, but twenty years after the first AMD/WMD, Africa is still leading the way for creative, sustained intervention against the disease, despite threats to resources from economic downturns and new pandemic diseases.
Below we go straight to Africa to share activities and observances of WMD 2021 from Jhpiego’s African Malaria Technical Officers. After reading through, please watch “Jhpiego Leaves No One Behind | World Malaria Day, 2021″ on YouTube.
 “Saramed” from Guinea reports that Guinea, like other countries in the world, celebrates World Malaria Day under the theme: ” Zero Malaria, Draw a Line on Malaria “. We are currently conducting the following activities:
“Saramed” from Guinea reports that Guinea, like other countries in the world, celebrates World Malaria Day under the theme: ” Zero Malaria, Draw a Line on Malaria “. We are currently conducting the following activities:
- Lectures and debates on malaria in medical faculties and health schools;
- Animation of debate programs on malaria in public and private radios and televisions of the country,
- Advocacy and sensitization of religious and other influential people
- Carrying out a package of activities (administration of IPT to pregnant women who have missed their ANC appointment, community distribution of LLINs, screening and treatment of confirmed cases, awareness raising on malaria) in high incidence localities.
These activities is in line with the WHO approach of “high burden, high impact”.
 Noella Umulisa reports that the WMD celebration took place in Eastern Province, in Bugesera district in the Mareba sector. Due to COVID-19 pandemic ,only 100 persons were invited to the event.This year’s the national theme is “Zero Malaria starts with me”.
Noella Umulisa reports that the WMD celebration took place in Eastern Province, in Bugesera district in the Mareba sector. Due to COVID-19 pandemic ,only 100 persons were invited to the event.This year’s the national theme is “Zero Malaria starts with me”.
Key activities during the event included …
- Visit of breeding sites under sentinel surveillance
- Visit of indoor residual spraying (IRS) sites
- Launching of the Awareness of the population using drones on the ongoing IRS campaign in this time of COVID-19
- Song by CHWs
- Certificate to Integrated Vector Management (IVM) Training of Trainers who will train others up to village level
- Speech of the Director General ,the guest of honor.
 From Burkina Faso, Yousseff Sawadogo and Moumouni Bonkoungou shared photos of the celebration that featured a giant Insecticide-Treated Net, a speech by the US Ambassador, a malaria song composed by a nurse, an official speech by the President of the National Assembly, and national recognition given to one of the current Jhpiego staff members, Thiery Ouedraogo, who at one time also served as director of the national malaria control program. He was decorated by the country’s authorities as a knight of the order of merit.
From Burkina Faso, Yousseff Sawadogo and Moumouni Bonkoungou shared photos of the celebration that featured a giant Insecticide-Treated Net, a speech by the US Ambassador, a malaria song composed by a nurse, an official speech by the President of the National Assembly, and national recognition given to one of the current Jhpiego staff members, Thiery Ouedraogo, who at one time also served as director of the national malaria control program. He was decorated by the country’s authorities as a knight of the order of merit.
 Bright Orgi from Jhpiego’s TiPToP malaria in pregnancy project in Nigeria ?? shared photos from a series of compound meetings in the community to mark WMD 2021. The meetings focused on malaria prevention and treatment. Provided opportunities to rural communities to ask questions on malaria issues. Here we can see that observance of WMD must be taken to the people who actually suffer from malaria and need to be actively involved in its solution. Deo Cibinda from the Democratic Republic of the Congo share photos of a national celebration, seen to the left.
Bright Orgi from Jhpiego’s TiPToP malaria in pregnancy project in Nigeria ?? shared photos from a series of compound meetings in the community to mark WMD 2021. The meetings focused on malaria prevention and treatment. Provided opportunities to rural communities to ask questions on malaria issues. Here we can see that observance of WMD must be taken to the people who actually suffer from malaria and need to be actively involved in its solution. Deo Cibinda from the Democratic Republic of the Congo share photos of a national celebration, seen to the left.
 Finally, As Kristen Vibbert noted, “These are such amazing World Malaria Day stories. I’m so heartened to see all of these great country efforts to remind everyone of how the fight against malaria must continue despite the Covid-19 pandemic.” Charles Wanga tweeted, “We know how to defeat #malaria. But that’s not enough. We must do more to save pregnant women and children from the deadly scourge. This #WorldMalariaDay and everyday, because@Jhpiego leaves no one behind in our fight to #EndMalaria for good in Africa, and everywhere”
Finally, As Kristen Vibbert noted, “These are such amazing World Malaria Day stories. I’m so heartened to see all of these great country efforts to remind everyone of how the fight against malaria must continue despite the Covid-19 pandemic.” Charles Wanga tweeted, “We know how to defeat #malaria. But that’s not enough. We must do more to save pregnant women and children from the deadly scourge. This #WorldMalariaDay and everyday, because@Jhpiego leaves no one behind in our fight to #EndMalaria for good in Africa, and everywhere”
Diagnosis &Elimination &Funding &IPTp &ITNs &Journalists/Media &Malaria in Pregnancy &Migration &Zero Malaria Bill Brieger | 26 Sep 2020
Malaria News Today 2020-09-26: supporting and strengthening malaria programs
Today’s selection of abstracts and news looks at the role of the media in supporting malaria programs, mass treatment to prevent Imported malaria, problems managing malaria in pregnancy services, malaria research in Mali and health systems strengthening to support malaria control in Guinea. Follow links to read mor details.
GHS calls for media support to eradicate malaria

The media has a role in supporting malaria programs
The Ghana Health Service (GHS) has called on journalists to support the Service to deliver integrated health package through accurate messages towards malaria eradication in the country.“Also, we need your support to set malaria as a national development agenda. This will drive advocacy for political will, increase partnership, availability and accessibility of effective tool for prevention, diagnoses and treatment of malaria in all the vulnerable populations.”
Dr Anthony Adofo Ofosu, the Deputy Director General, GHS, said this at the launch of “Zero malaria starts with me” campaign in Accra. The launch coincided with a sensitisation programme by the African Media and Malaria Research Network (AMMRN), the National Malaria Control Programme and the Speak Up African Organisation. The Deputy Director General said “It is the belief of the GHS that with effective engagement…we will be able to eradicate malaria from the country in the near future.”
Mass radical treatment of a group of foreign workers to mitigate the risk of re-establishment of malaria in Sri Lanka
Following malaria elimination, Sri Lanka was free from indigenous transmission for six consecutive years, until the first introduced case was reported in December 2018. The source of transmission (index case) was a member of a group of 32 migrant workers from India and the location of transmission was their residence reporting a high prevalence of the primary vector for malaria. Despite extensive vector control the situation was highly susceptible to onward transmission if another of the group developed malaria. Therefore, Mass Radical Treatment (MRT) of the group of workers for Plasmodium vivax malaria was undertaken to mitigate this risk.
The workers were screened for malaria by microscopy and RDT, their haemoglobin level assessed, and tested for Glucose 6 phosphate dehydrogenase deficiency (G6PD) using the Care Start RDT and Brewers test prior to treatment with chloroquine (CQ) 25 mg/kg body weight (over three days) and primaquine (PQ, based on G6PD test results) (0.25 mg/kg/day bodyweight for 14 days) following informed consent. All were monitored for adverse events. None of the foreign workers were parasitaemic at baseline screening.
Mass treatment may be an option in prevention of reintroduction settings for groups of migrants who are likely to be carrying latent malaria infections, and resident in areas of high receptivity. However, in the case of Plasmodium vivax and Plasmodium ovale, a more reliable and affordable point-of-care test for G6PD activity would be required. Most countries which are eliminating malaria now are in the tropical zone and face considerable and similar risks of malaria re-introduction due to massive labour migration between them and neighbouring countries. Regional elimination of malaria should be the focus of global strategy if malaria elimination from countries is to be worthwhile and sustainable.
Managing intermittent preventive treatment of malaria in pregnancy challenges: an ethnographic study of two Ghanaian administrative regions
Malaria in pregnancy (MiP) is an important public health problem across sub-Saharan Africa. The package of measures for its control in Ghana in the last 20 years include regular use of long-lasting insecticide-treated bed nets (LLINs), directly-observed administration (DOT) of intermittent preventive treatment with sulfadoxine-pyrimethamine (IPTp-SP) and prompt and effective case management of MiP. Unfortunately, Ghana like other sub-Saharan African countries did not achieve the reset Abuja targets of 100% of pregnant women having access to IPTp and 100% using LLINs by 2015.
This ethnographic study explored how healthcare managers dealt with existing MiP policy implementation challenges and the consequences on IPTp-SP uptake and access to maternal healthcare. Healthcare managers addressed frequent stock-outs of malaria programme drugs and supplies from the National Malaria Control Programme and delayed reimbursement from the NHIS, by instituting co-payment, rationing and prescribing drugs for women to buy from private pharmacies.
 Some clients did not receive the recommended 5?+?doses of SP, others did not obtain LLINs early and some did not obtain treatment for MiP. Healthcare providers felt frustrated whenever they could not provide comprehensive care to women who could not afford comprehensive maternal and MiP care. For Ghana to achieve her goal of controlling MiP, the Ministry of Health and other supporting institutions need to ensure prompt reimbursement of funds, regular supply of programme drugs and medical supplies to public, faith-based and private health facilities.
Some clients did not receive the recommended 5?+?doses of SP, others did not obtain LLINs early and some did not obtain treatment for MiP. Healthcare providers felt frustrated whenever they could not provide comprehensive care to women who could not afford comprehensive maternal and MiP care. For Ghana to achieve her goal of controlling MiP, the Ministry of Health and other supporting institutions need to ensure prompt reimbursement of funds, regular supply of programme drugs and medical supplies to public, faith-based and private health facilities.
Malaria prevention program continuation in Guinea
CRS Guinea is the Principal Recipient (PR) in Malaria prevention program continuation grant by the Global Fund for the new cycle of funding (NFM) (January 2021-December 2023). Community health is a top priority of the Ministry of Health as a primary strategy to increase accessibility and coverage to basic health services. Under the new Global Fund grant, the community health component will be expanded to six districts, in addition to two pilot districts, Kindia and Telimele. CRS will also support coordination with other donors, including World Bank, UNICEF, Gavi, European Union and the Guinea Ministry of Health to implement the national community health strategy in 12 health districts supported by Global Fund malaria project.
The United States and Mali Celebrate 60 Years of Friendship and Partnership
Thirty years ago, our National Institutes of Health created a Malaria Research and Training Center, which is now a component of the International Center for Excellence in Research in Mali. Until today, it serves as a reference center with over 700 Malian scientists and support staff who work on malaria and other infectious diseases. Together, we have dropped malaria prevalence rates in Mali by an astounding 60 percent since 2012.
Ivermectin &Larvicide &MDA &Vaccine &Zero Malaria Bill Brieger | 25 Apr 2019
Zero Malaria Starts with Universal Coverage: Part 3 Innovations and New Interventions
Newer malaria interventions are coming on board, and whether these will be used of a large scale or targeted to certain epidemiological contexts remains to be seen. In each case, one will need to examine if in each context one can measure whether the intervention is universally accessible to and used by the intended population or subgroup.
 After 30 years of research and testing, a malaria vaccine is ready to go through implementation testing in Malawi, Ghana and Kenya. This pilot of the vaccine, known as RTS,S, will be made available to children up to 2 years of age with the Malawi launching first during the week of World Malaria Day.
After 30 years of research and testing, a malaria vaccine is ready to go through implementation testing in Malawi, Ghana and Kenya. This pilot of the vaccine, known as RTS,S, will be made available to children up to 2 years of age with the Malawi launching first during the week of World Malaria Day.
WHO explains that, “The malaria vaccine pilot aims to reach about 360,000 children per year across the three countries. Ministries of health will determine where the vaccine will be given; they will focus on areas with moderate-to-high malaria transmission, where the vaccine can have the greatest impact.” There will be a strong monitoring component to identify coverage levels as well as any implementation challenges and adverse effects that may only become visible in a larger scale intervention that the typical efficacy trials. Implementation is occurring in areas with a relatively strong existing malaria control effort, with an intent to learn how a vaccine can complement a total control package.
 Mass Drug Administration (MDA, also known as preventive chemotherapy) has been a successful strategy for controlling and eliminating neglected tropical diseases with special reference to onchocerciasis, lymphatic filariasis, trachoma, soil transmitted helminths and schistosomiasis. MDA use in malaria has been limited due to a number of financial and logistical challenges, not the least of which is the need to achieve high coverage over several periods of distribution. This is why WHO recommends, “Use of MDA for the elimination of P. falciparum malaria can be considered in areas approaching interruption of transmission where there is good access to treatment, effective implementation of vector control and surveillance, and a minimal risk of re-introduction of infection.”
Mass Drug Administration (MDA, also known as preventive chemotherapy) has been a successful strategy for controlling and eliminating neglected tropical diseases with special reference to onchocerciasis, lymphatic filariasis, trachoma, soil transmitted helminths and schistosomiasis. MDA use in malaria has been limited due to a number of financial and logistical challenges, not the least of which is the need to achieve high coverage over several periods of distribution. This is why WHO recommends, “Use of MDA for the elimination of P. falciparum malaria can be considered in areas approaching interruption of transmission where there is good access to treatment, effective implementation of vector control and surveillance, and a minimal risk of re-introduction of infection.”
Another link with MDA for a different disease, onchocerciasis, has pointed to a potential new malaria intervention. Around ten years ago it was observed that after ivermectin treatment for onchocerciasis in Senegal survivorship of malaria vectors was reduced. Subsequently the potential effect of ivermectin has been intentionally researched with the outcome that, “Frequently repeated mass administrations of ivermectin during the malaria transmission season can reduce malaria episodes among children without significantly increasing harms in the populace.” Mathematical models for onchocerciasis control have predicted the need to achieve annual coverage targets below what could be called universal levels. Using ivermectin for mosquito control would require more frequent dosing and higher coverage.
Although not defined as ‘new’ it is important to include mention of additional vector interventions like larviciding and indoor residual spraying, as these present technical and coverage challenges. For example, larviciding interventions either chemical or biological, do not cover individuals. These focus on breeding sites in communities. This may require better use of the concept of geographical coverage as has been used in onchocerciasis control wherein the proportion of endemic villages reached is monitored.
For example, in Mali the NTD program aimed to achieve 80% program coverage of individuals eligible for preventive chemotherapy and 100% geographical coverage yearly. This means all villages should be reached. In reality, the program achieved 85% geographical coverage for lymphatic filariasis and over 90% for onchocerciasis.
In conclusion, we have seen that defining as well as achieving universal coverage of malaria interventions is a challenging prospect. For example, do we base our monitoring on households, villages, or populations? Do we have the funds and technical capacity to implement and sustain the level of coverage required to have an impact on malaria transmission and move toward elimination? Are we able to introduce new, complimentary and appropriate interventions as a country moves closer to elimination?
Diagnosis &Essential Medicines &IPTi &Malaria in Pregnancy &Seasonal Malaria Chemoprevention &Treatment &Zero Malaria Bill Brieger | 25 Apr 2019
Zero Malaria Starts with Universal Coverage: Part 2 Preventive and Curative Treatments
April hosts several important global health days or observances. On World Health Day 2019 WHO stressed that, “Universal health coverage (UHC) is WHO’s number one goal. Key to achieving it is ensuring that everyone can obtain the care they need, when they need it, right in the heart of the community.” Nationwide monitoring through the Demographic and Health Surveys (DHS), the Malaria Indicator Surveys (MIS) and the Multi-Indicator Cluster Surveys (MICS) can document the status of appropriate malaria treatment and intermittent preventive treatment in pregnant women (IPTp).
 Definitions of indicators have evolved for treatment-related malaria interventions. When Intermittent Preventive Treatment for pregnant women (IPTp) began in the early 2000s, the recommended dosing was twice during pregnancy after the first trimester one month apart in high and/or stable transmission areas. Due to lessening efficacy of sulfadoxine-pyrimethamine (SP), the dosage recommendation has changed to at least three times, still a month apart from the beginning of the second trimester.
Definitions of indicators have evolved for treatment-related malaria interventions. When Intermittent Preventive Treatment for pregnant women (IPTp) began in the early 2000s, the recommended dosing was twice during pregnancy after the first trimester one month apart in high and/or stable transmission areas. Due to lessening efficacy of sulfadoxine-pyrimethamine (SP), the dosage recommendation has changed to at least three times, still a month apart from the beginning of the second trimester.
This updated policy was broadcast widely between 2012 and 2013, but it took countries some time to build capacity and scale up for the expanded coverage goals. UNICEF Data5 again show that between 2014 and 2017 coverage was far below either 80% of pregnant women, let alone reaching them universally (Figure 2). Most countries achieved 30% or less coverage. Zambia at 50% was the highest. Low coverage leaves both pregnant women and the unborn child at risk for anemia and death in the former and low birth weight, still birth or miscarriage for the latter. The World Malaria Report of 2018 estimates that three doses of IPTp were received by only 22% of pregnant women in the target countries in 2017.
The concept of IPT was investigated for infants and children during by a consortium of researchers in several African Countries. It was found that IPTi with SP could have a positive effect on preventing malaria. To operationalize this concept, the World Health Organization developed what is known as Seasonal Malaria Chemoprevention (SMC) that would be delivered in the Sahel region of West Africa where malaria transmission itself is seasonal and where there are some countries with very low transmission with implications for malaria elimination.
 The SMC delivery process was not linked to immunization but provided by community health workers and volunteers. SP and Amodiaquine (SP-AQ) were used in combination and provided monthly, three or four times during the rainy/high transmission season. Coverage was targeted at children below school age. It is only recently that SMC has been scaled up to reach all eligible countries or states and regions within designated countries.
The SMC delivery process was not linked to immunization but provided by community health workers and volunteers. SP and Amodiaquine (SP-AQ) were used in combination and provided monthly, three or four times during the rainy/high transmission season. Coverage was targeted at children below school age. It is only recently that SMC has been scaled up to reach all eligible countries or states and regions within designated countries.
WHO states that SMC focuses on, “children aged 3–59 months (and) reduces the incidence of clinical attacks and severe malaria by about 75%.” In some countries the coverage is extended to primary school aged children, making comparisons and calculations of coverage (universal por otherwise) challenging.
 The World Malaria Report of 2018 notes that, “In 2017, 15.7 million children in 12 countries in Africa’s Sahel subregion were protected through seasonal malaria chemoprevention (SMC) programs. However, about 13.6 million children who could have benefited from this intervention were not covered, mainly due to a lack of funding.” This implies that 54% of eligible children were reached. Coverage of SMC can refer to receiving any of the doses or as having received all the monthly doses offered by a nation’s malaria control program. Specifically, the World Malaria Report 2018 drew on surveys in 7 countries that provided 4 monthly doses to determine that 53% of children received all doses.
The World Malaria Report of 2018 notes that, “In 2017, 15.7 million children in 12 countries in Africa’s Sahel subregion were protected through seasonal malaria chemoprevention (SMC) programs. However, about 13.6 million children who could have benefited from this intervention were not covered, mainly due to a lack of funding.” This implies that 54% of eligible children were reached. Coverage of SMC can refer to receiving any of the doses or as having received all the monthly doses offered by a nation’s malaria control program. Specifically, the World Malaria Report 2018 drew on surveys in 7 countries that provided 4 monthly doses to determine that 53% of children received all doses.
 Determining coverage for malaria treatment for sick people is not as straightforward as finding out the numbers who slept under an ITN or swallowed IPTp doses, and even those are not simple. As defined, correct treatment first consists of parasitological diagnosis, which at the primary care level could be by microscopy or rapid diagnostic test (RDT). The next issue is treating only those with positive tests. Finally, the treatment must consist of age- or weight-specific doses of an approved artemisinin-based combination therapy (ACT) drug. Very few clinic records or surveys document whether the treatment given is ‘correct’ by these standards.
Determining coverage for malaria treatment for sick people is not as straightforward as finding out the numbers who slept under an ITN or swallowed IPTp doses, and even those are not simple. As defined, correct treatment first consists of parasitological diagnosis, which at the primary care level could be by microscopy or rapid diagnostic test (RDT). The next issue is treating only those with positive tests. Finally, the treatment must consist of age- or weight-specific doses of an approved artemisinin-based combination therapy (ACT) drug. Very few clinic records or surveys document whether the treatment given is ‘correct’ by these standards.
WHO addresses the need for achieving universal access to malaria diagnostic testing and notes this will not be easy. They provide a successful example of Senegal, where following the introduction of malaria RDTs in 2007, malaria diagnostic testing rates rose rapidly from 4% to 86% (by 2009). Logistics, funding, training and supportive supervision complicate implementation.
UNICEF Data report that performance of malaria diagnostics in febrile children in surveys 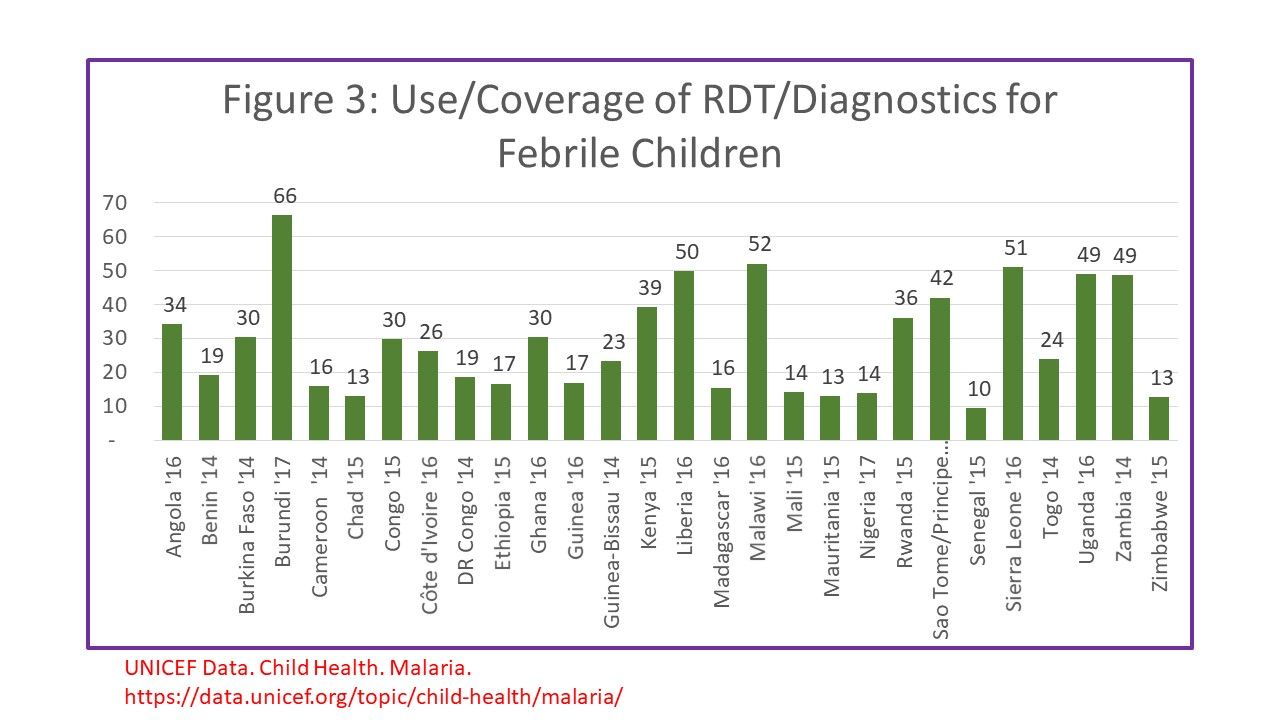 between 2014-17 was approximately 30% on average for countries with national surveys within that time frame (Figure 3). Only 4 countries achieved 50% or better. Most surveys then go on to report the number of febrile children who received ACTs, but do not necessary indicate how many who were correctly diagnoses were given ACTs vs those who received ACT but did not receive a test or tested negative.
between 2014-17 was approximately 30% on average for countries with national surveys within that time frame (Figure 3). Only 4 countries achieved 50% or better. Most surveys then go on to report the number of febrile children who received ACTs, but do not necessary indicate how many who were correctly diagnoses were given ACTs vs those who received ACT but did not receive a test or tested negative.
The Nigeria 2015 Malaria Indicator Survey Illustrates this dilemma. Among 2600 children who reported having a fever in the two weeks preceding the survey, 66.1% sought advice (or care). Overall, 12.6% of febrile children received a diagnostic test as defined in the question as to whether the child was stuck on the finger or heel to obtain blood. Among the febrile children 37.6% reportedly were given some type of antimalarial drug. Overall 15.5% of febrile children were given an ACT. Even if ACTs were given only to tested children, not all tests would have been positive.
The overall implication of measuring treatment without a link to testing is that if more children receive any, let alone the correct drugs, is that evidence for actual presence of disease. We have a long way to go to measure malaria treatment coverage correctly, not to mention achieving universal coverage with appropriate treatment. Different malaria treatment-related interventions with different steps and different target groups in different regions of Africa and the World make defining, no less achieving UHC, a huge challenge.
ITNs &Universal Coverage &Vector Control &Zero Malaria Bill Brieger | 25 Apr 2019
Zero Malaria Starts with Universal Coverage: Part 1 Nets
WHO says, “Malaria elimination and universal health coverage go hand in hand,” at a special event during the 72st World Health Assembly. To achieve zero malaria, the goal of involving everyone from the policy maker to the community member must have a focus on achieving universal health coverage (UHC) of all malaria interventions ranging from insecticide treated bednets (ITNs) to appropriate provision of malaria diagnostics and medicines. Many of the studies to date have focused on ITNs, which include long-lasting insecticide treated nets (LLINs), but nationwide monitoring through the Demographic and Health Surveys (DHS), the Malaria Indicator Surveys (MIS) and the Multi-Indicator Cluster Surveys (MICS).
UNICEF’s website provides a data repository that includes the most recent DHS, MIS and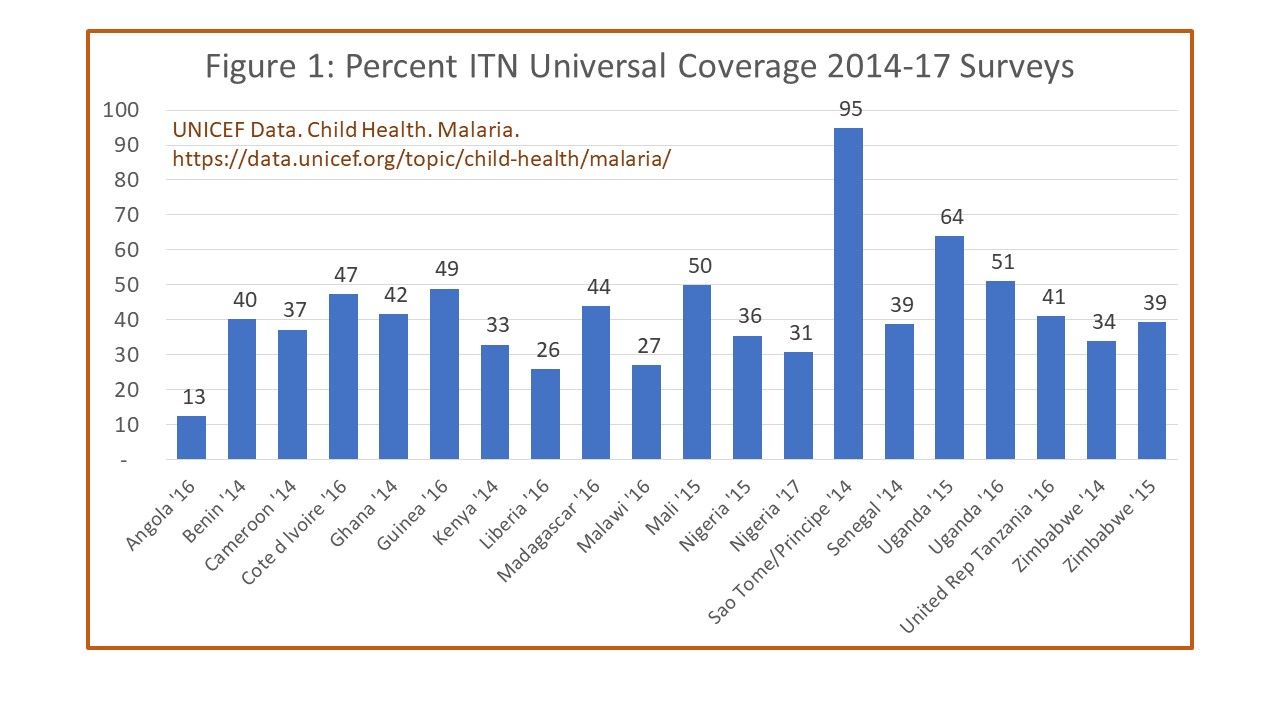 MICS survey data per country between 2014 and 2017. For the indicator of one ITN per to people in a household, shows Angola at only 13%, most countries for which recent data are available reached between 40-50%. Only two achieved above 60% on a point-in-time survey, Uganda at 62% and Sao Tome and Principe at 95%. The website shows information that where there were multiple surveys in a country during the period, there were variations, sometimes quite wide, over the years. Aside from the fact that the surveys may have had slightly different procedures, the problem remains of achieving and sustaining UHC for ITNs.
MICS survey data per country between 2014 and 2017. For the indicator of one ITN per to people in a household, shows Angola at only 13%, most countries for which recent data are available reached between 40-50%. Only two achieved above 60% on a point-in-time survey, Uganda at 62% and Sao Tome and Principe at 95%. The website shows information that where there were multiple surveys in a country during the period, there were variations, sometimes quite wide, over the years. Aside from the fact that the surveys may have had slightly different procedures, the problem remains of achieving and sustaining UHC for ITNs.
Another factor that affects maintaining UHC for ITNs, assuming the target can be met is the durability of nets. The physical integrity as well as the insecticide efficacy can decline over time. Intact nets may lose their insecticide through improper washing and drying, yet still prevent mosquito bites to the individual sleeping under them. Nets with holes may still maintain a minimal level of effective insecticide and may not fully prevent bites but ultimately kill the mosquito that flies through. Researchers in Senegal have been grappling with these challenges.
 Program managers must themselves grapple with whether such compromised nets count toward universal coverage as well as how often to conduct net replacement campaigns. A report from community surveys in Uganda during 2017 found that, “Long-lasting insecticidal net ownership and coverage have reduced markedly in Uganda since the last net distribution campaign in 2013/14.” UHC for ITNs is always a moving target.
Program managers must themselves grapple with whether such compromised nets count toward universal coverage as well as how often to conduct net replacement campaigns. A report from community surveys in Uganda during 2017 found that, “Long-lasting insecticidal net ownership and coverage have reduced markedly in Uganda since the last net distribution campaign in 2013/14.” UHC for ITNs is always a moving target.
A frequently unaddressed issue in seeking to improve ITN coverage is whether it makes a difference in malaria disease. A study in Malawi reported that although ITNs per household increased from 1.1 in 2012 to 1.4 in 2014, the prevalence of malaria in children increased over the period from 28% to 32%. The authors surmised that factors such as insecticide resistance, irregular ITN use and inadequate coordinated use of other malaria control interventions may have influenced the results. This shows that UHC for ITNs cannot be viewed in isolation.
This brings up the issue of the role of the many different vector control measures available. Researchers in Côte d’ Ivoire examined the use of eave nets and window screening. At present eave nets are mainly deployed in research contexts but use of window and door screening and netting are a commercially available interventions that households employ on their own. One wonders then whether UHC should focus on how the household and the people therein are protected by any malaria vector intervention.
 Here the discussion should focus on the question raised by colleagues in the USAID/PMI Vectorworks Project. WHO declared a goal of universal ITN coverage in 2009 using the target f one ITN/LLIN for every two household members. Vectorworks found that a decade on only one instance of a country briefly achieving 80% of this UHC net target, whereas no others reached above 60%. In fact, the bigger the household, the less chance there was of meeting the two people for one ITN target. Just because people live in a household that has the requisite number of nets, does not guarantee the actual target for sleeping under a net can be achieved because of practical or cultural realities in a household. Neither the minimal indicator of having at least one net in a household, or the ideal or ‘perfect’ indicator of UHC are satisfactory for judging population protection.
Here the discussion should focus on the question raised by colleagues in the USAID/PMI Vectorworks Project. WHO declared a goal of universal ITN coverage in 2009 using the target f one ITN/LLIN for every two household members. Vectorworks found that a decade on only one instance of a country briefly achieving 80% of this UHC net target, whereas no others reached above 60%. In fact, the bigger the household, the less chance there was of meeting the two people for one ITN target. Just because people live in a household that has the requisite number of nets, does not guarantee the actual target for sleeping under a net can be achieved because of practical or cultural realities in a household. Neither the minimal indicator of having at least one net in a household, or the ideal or ‘perfect’ indicator of UHC are satisfactory for judging population protection.
The Vectorworks team suggests that, “Population ITN access indicator is a far better indicator of ‘universal coverage’ because it is based on individual people,” and can be compared to, “The proportion of the population that used an ITN the previous night, which enables detailed analysis of specific behavioral gaps nationally as well as among population subgroups.” Population access to ITNs therefore, provides a batter basis for more realistic policies and strategies.
We have seen that defining as well as achieving universal coverage of malaria interventions is a challenging prospect. For example, do we base our monitoring on households or populations? Do we have the funds and technical capacity to implement and sustain the level of coverage required to have an impact on malaria transmission and move toward elimination? Are we able to introduce new, complimentary and appropriate interventions as a country moves closer to elimination?
A useful perspective would be determination if households and individuals even benefit from any part of the malaria package, even if everyone does not have access and utilize all components. This may be why zero malaria has to start with each person living in endemic areas.