Capacity Building &CHW &Community &Elimination &Health Education &Indoor Residual Spraying &IPTp &ITNs &Malaria in Pregnancy &World Malaria Day &Zero Malaria Bill Brieger | 25 Apr 2021
Twenty Years of Malaria Day Observances: Jhpiego at the Forefront
 In 2001 the first Africa Malaria Day (AMD) was observed. The opportunity to mark progress and exhort increased efforts for the continent continued through 2007. Then in 2008, the concept of World Malaria Day (WMD) took over, though it could not be denied that the bulk of malaria morbidity, mortality and intervention still was focused on African countries. Other countries have made progress such as the recent certification of malaria elimination in Argentina and El Salvador, but twenty years after the first AMD/WMD, Africa is still leading the way for creative, sustained intervention against the disease, despite threats to resources from economic downturns and new pandemic diseases.
In 2001 the first Africa Malaria Day (AMD) was observed. The opportunity to mark progress and exhort increased efforts for the continent continued through 2007. Then in 2008, the concept of World Malaria Day (WMD) took over, though it could not be denied that the bulk of malaria morbidity, mortality and intervention still was focused on African countries. Other countries have made progress such as the recent certification of malaria elimination in Argentina and El Salvador, but twenty years after the first AMD/WMD, Africa is still leading the way for creative, sustained intervention against the disease, despite threats to resources from economic downturns and new pandemic diseases.
Below we go straight to Africa to share activities and observances of WMD 2021 from Jhpiego’s African Malaria Technical Officers. After reading through, please watch “Jhpiego Leaves No One Behind | World Malaria Day, 2021″ on YouTube.
 “Saramed” from Guinea reports that Guinea, like other countries in the world, celebrates World Malaria Day under the theme: ” Zero Malaria, Draw a Line on Malaria “. We are currently conducting the following activities:
“Saramed” from Guinea reports that Guinea, like other countries in the world, celebrates World Malaria Day under the theme: ” Zero Malaria, Draw a Line on Malaria “. We are currently conducting the following activities:
- Lectures and debates on malaria in medical faculties and health schools;
- Animation of debate programs on malaria in public and private radios and televisions of the country,
- Advocacy and sensitization of religious and other influential people
- Carrying out a package of activities (administration of IPT to pregnant women who have missed their ANC appointment, community distribution of LLINs, screening and treatment of confirmed cases, awareness raising on malaria) in high incidence localities.
These activities is in line with the WHO approach of “high burden, high impact”.
 Noella Umulisa reports that the WMD celebration took place in Eastern Province, in Bugesera district in the Mareba sector. Due to COVID-19 pandemic ,only 100 persons were invited to the event.This year’s the national theme is “Zero Malaria starts with me”.
Noella Umulisa reports that the WMD celebration took place in Eastern Province, in Bugesera district in the Mareba sector. Due to COVID-19 pandemic ,only 100 persons were invited to the event.This year’s the national theme is “Zero Malaria starts with me”.
Key activities during the event included …
- Visit of breeding sites under sentinel surveillance
- Visit of indoor residual spraying (IRS) sites
- Launching of the Awareness of the population using drones on the ongoing IRS campaign in this time of COVID-19
- Song by CHWs
- Certificate to Integrated Vector Management (IVM) Training of Trainers who will train others up to village level
- Speech of the Director General ,the guest of honor.
 From Burkina Faso, Yousseff Sawadogo and Moumouni Bonkoungou shared photos of the celebration that featured a giant Insecticide-Treated Net, a speech by the US Ambassador, a malaria song composed by a nurse, an official speech by the President of the National Assembly, and national recognition given to one of the current Jhpiego staff members, Thiery Ouedraogo, who at one time also served as director of the national malaria control program. He was decorated by the country’s authorities as a knight of the order of merit.
From Burkina Faso, Yousseff Sawadogo and Moumouni Bonkoungou shared photos of the celebration that featured a giant Insecticide-Treated Net, a speech by the US Ambassador, a malaria song composed by a nurse, an official speech by the President of the National Assembly, and national recognition given to one of the current Jhpiego staff members, Thiery Ouedraogo, who at one time also served as director of the national malaria control program. He was decorated by the country’s authorities as a knight of the order of merit.
 Bright Orgi from Jhpiego’s TiPToP malaria in pregnancy project in Nigeria ?? shared photos from a series of compound meetings in the community to mark WMD 2021. The meetings focused on malaria prevention and treatment. Provided opportunities to rural communities to ask questions on malaria issues. Here we can see that observance of WMD must be taken to the people who actually suffer from malaria and need to be actively involved in its solution. Deo Cibinda from the Democratic Republic of the Congo share photos of a national celebration, seen to the left.
Bright Orgi from Jhpiego’s TiPToP malaria in pregnancy project in Nigeria ?? shared photos from a series of compound meetings in the community to mark WMD 2021. The meetings focused on malaria prevention and treatment. Provided opportunities to rural communities to ask questions on malaria issues. Here we can see that observance of WMD must be taken to the people who actually suffer from malaria and need to be actively involved in its solution. Deo Cibinda from the Democratic Republic of the Congo share photos of a national celebration, seen to the left.
 Finally, As Kristen Vibbert noted, “These are such amazing World Malaria Day stories. I’m so heartened to see all of these great country efforts to remind everyone of how the fight against malaria must continue despite the Covid-19 pandemic.” Charles Wanga tweeted, “We know how to defeat #malaria. But that’s not enough. We must do more to save pregnant women and children from the deadly scourge. This #WorldMalariaDay and everyday, because@Jhpiego leaves no one behind in our fight to #EndMalaria for good in Africa, and everywhere”
Finally, As Kristen Vibbert noted, “These are such amazing World Malaria Day stories. I’m so heartened to see all of these great country efforts to remind everyone of how the fight against malaria must continue despite the Covid-19 pandemic.” Charles Wanga tweeted, “We know how to defeat #malaria. But that’s not enough. We must do more to save pregnant women and children from the deadly scourge. This #WorldMalariaDay and everyday, because@Jhpiego leaves no one behind in our fight to #EndMalaria for good in Africa, and everywhere”
Economics &Indoor Residual Spraying &IRS Bill Brieger | 16 Nov 2020
Epidemiological and Projected Economical Impact of Indoor Residual Spraying in Ngoma District, Rwanda
 This year the Annual Meeting of the American Society of Tropical Medicine and Hygiene is virtual. We will feature some of the abstracts over the coming week. Our first selection from the 69th meeting is a study from Rwanda on indoor residual spraying by Michee S. Kabera (see author list and affiliations at end) wherein we learn about the benefits of averting malaria cases.
This year the Annual Meeting of the American Society of Tropical Medicine and Hygiene is virtual. We will feature some of the abstracts over the coming week. Our first selection from the 69th meeting is a study from Rwanda on indoor residual spraying by Michee S. Kabera (see author list and affiliations at end) wherein we learn about the benefits of averting malaria cases.
IRS in Ngoma District
Malaria remains a major public health problem and is among the leading causes of morbidity and mortality in Rwanda. Indoor Residual Spraying (IRS) is a core vector control intervention in Rwanda that supplement Insecticide-treated bed nets (ITNs). Ngoma district is located in Eastern province of Rwanda bordering with Burundi in South. The first IRS round was conducted in the above district in April 2019 (before the high peak season of May-June) with the support of the Government of Rwanda and The Global Funds.
 The IRS coverage rate was 98.9% with a protected population of 357,058 using “Pirimiphos methyl 300 CS. Using RHMIS, we compared malaria cases respectively reported for a period of 12 months before IRS (April 2018 to March 2019) and after IRS (April 2019 to March 2020). The total number of uncomplicated malaria cases was significantly dropped down by 82%, from 581,742 before IRS to 105,120 cases after IRS. The incidence per 1000 inhabitants decreased from 1,502 to 265 respectively.
The IRS coverage rate was 98.9% with a protected population of 357,058 using “Pirimiphos methyl 300 CS. Using RHMIS, we compared malaria cases respectively reported for a period of 12 months before IRS (April 2018 to March 2019) and after IRS (April 2019 to March 2020). The total number of uncomplicated malaria cases was significantly dropped down by 82%, from 581,742 before IRS to 105,120 cases after IRS. The incidence per 1000 inhabitants decreased from 1,502 to 265 respectively.
Moreover, the inpatient cases also significantly decreased by 87.7%, from 1037 before IRS to 170 cases after IRS. The cost of conducting IRS in Ngoma district was USD 2,104,007 including both the cost for Insecticides and operation. The invested cost per averted malaria case was USD 4.4. Using the minimum average cost of USD 8.6 for treating an episode of the disease including direct cost and the opportunity costs of travel and waiting time (1,2); the total benefit due to averted malaria cases is estimated to USD 4,132,313.
Applying the average cost for inpatient malaria case which is estimated to USD US$60.44 (4), the benefit due to the averted malaria inpatient cases is equal to USD 52,401. The total benefit for averted outpatients and inpatients is estimated to USD 4,184,714. In conclusion, there was a significant decrease of out and inpatient malaria cases just one year after IRS in Ngoma district.
Furthermore, if we compare the IRS expenditures and the benefits related to the averted malaria cases, there was an important cost benefit. We expect more economic impact as malaria cases may continue to decrease.
Authors and Affiliations
Michee S. Kabera(1), Noella Noella(2), Emmanuel Hakizimana(1), Dunia Munyakanage(1), Jean Louis Mangala(1), Kaendi Munguti(3), Aimable Mbituyumuremyi(1) 1.Rwanda Biomedical Center, Kigali, Rwanda, 2.JHPIEGO, Kigali, Rwanda, 3.President’s Malaria Initiative, Kigali, Rwanda
Asymptomatic &Borders &Children &Elimination &Indoor Residual Spraying &IRS &Migration &Mosquitoes &Pharmacovigilence Bill Brieger | 08 Oct 2020
Malaria News Today 2020-10-08: the role of travel, asymptomatic disease and gut microbiome from AJTMH
![]() The American Journal of Tropical Medicine and Hygiene has several new articles on malaria. Abstracts are shared. Two articles examine the role of travel in malaria transmission, both cross-border and rural-urban. Another considers the effect on pharmacokinetics of lumefantrine due to gut bacteria. In Uganda indoor spraying has reduced transmission, but asymptomatic cases remain among children. The challenges of asymptomatic malaria to elimination efforts is also examined in India. Links to the articles are found below.
The American Journal of Tropical Medicine and Hygiene has several new articles on malaria. Abstracts are shared. Two articles examine the role of travel in malaria transmission, both cross-border and rural-urban. Another considers the effect on pharmacokinetics of lumefantrine due to gut bacteria. In Uganda indoor spraying has reduced transmission, but asymptomatic cases remain among children. The challenges of asymptomatic malaria to elimination efforts is also examined in India. Links to the articles are found below.
Evidence of Microbiome–Drug Interaction between the Antimalarial Lumefantrine and Gut Microbiota in Mice
The antimalarial drug lumefantrine exhibits erratic pharmacokinetics. Intersubject variability might be attributed, in part, to differences in gut microbiome–mediated drug metabolism. We assessed lumefantrine disposition in healthy mice stratified by enterotype to explore associations between the gut microbiota and lumefantrine pharmacokinetics. Gut microbiota enterotypes were classified according to abundance and diversity indices from 16S rRNA sequencing. Pharmacokinetic parameters were computed using noncompartmental analysis. Two distinct enterotypes were identified.
Maximal concentration (C max) and total drug exposure measured as the area under the drug concentration–time curve (AUC0–24) differed significantly between the groups. The mean and standard deviation of C max were 660 ± 220 ng/mL versus 390 ± 59 ng/mL (P = 0.02), and AUC0–24 was 9,600 ± 2,800 versus 5,800 ± 810 ng × h/mL (P = 0.01). In healthy mice intragastrically dosed with the antimalarial drug lumefantrine in combination with artemether, lumefantrine exposure was associated with gut bacterial community structure. Studies of xenobiotic–microbiota interactions can inform drug posology and elucidate mechanisms of drug disposition.
Malaria Transmission, Infection, and Disease following Sustained Indoor Residual Spraying of Insecticide in Tororo, Uganda
Tororo, a district in Uganda with historically high malaria transmission intensity, has recently scaled up control interventions, including universal long-lasting insecticidal net distribution in 2013 and 2017, and sustained indoor residual spraying (IRS) of insecticide since December 2014. We describe the burden of malaria in Tororo 5 years following the initiation of IRS. We followed a cohort of 531 participants from 80 randomly selected households in Nagongera subcounty, Tororo district, from October 2017 to October 2019. Mosquitoes were collected every 2 weeks using CDC light traps in all rooms where participants slept, symptomatic malaria was identified by passive surveillance, and microscopic and submicroscopic parasitemia were measured every 4 weeks using active surveillance. Over the 2 years of follow-up, 15,780 female anopheline mosquitos were collected, the majority (98.0%) of which were Anopheles arabiensis.
recently scaled up control interventions, including universal long-lasting insecticidal net distribution in 2013 and 2017, and sustained indoor residual spraying (IRS) of insecticide since December 2014. We describe the burden of malaria in Tororo 5 years following the initiation of IRS. We followed a cohort of 531 participants from 80 randomly selected households in Nagongera subcounty, Tororo district, from October 2017 to October 2019. Mosquitoes were collected every 2 weeks using CDC light traps in all rooms where participants slept, symptomatic malaria was identified by passive surveillance, and microscopic and submicroscopic parasitemia were measured every 4 weeks using active surveillance. Over the 2 years of follow-up, 15,780 female anopheline mosquitos were collected, the majority (98.0%) of which were Anopheles arabiensis.
The daily human biting rate was 2.07, and the annual entomological inoculation rate was 0.43 infective bites/person/year. Only 38 episodes of malaria were diagnosed (incidence 0.04 episodes/person/year), and there were no cases of severe malaria or malarial deaths. The prevalence of microscopic parasitemia was 1.9%, and the combined prevalence of microscopic and submicroscopic parasitemia was 10.4%, each highest in children aged 5–15 years (3.3% and 14.0%, respectively). After 5 years of intensive vector control measures in Tororo, the burden of malaria was reduced to very low transmission levels. However, a significant proportion of the population remained parasitemic, primarily school-aged children with submicroscopic parasitemia, providing a potential reservoir for malaria transmission.
Malaria Diagnosed in an Urban Setting Strongly Associated with Recent Overnight Travel: A Case–Control Study from Kampala, Uganda
Malaria is frequently diagnosed in urban Kampala, despite low transmission intensity. To evaluate the association between recent travel out of Kampala and malaria, we conducted a matched case–control study. Cases were febrile outpatients with a positive malaria test; controls were febrile outpatients with a negative test. For every two cases, five controls were selected, matching on age. Data were collected on recent overnight travel out of Kampala (past 60 days), destination and duration of travel, and behavioral factors, including sleeping under an insecticide-treated net (ITN) during travel. From July to August 2019, 162 cases and 405 controls were enrolled. The locations of residence of cases and controls were similar. More controls were female (62.7% versus 46.3%, P < 0.001). Overall, 158 (27.9%) participants reported recent overnight travel.
Travelers were far more likely to be diagnosed with malaria than those who did not travel (80.4% versus 8.6%, OR 58.9, 95% CI: 23.1–150.1, P < 0.001). Among travelers, traveling to a district not receiving indoor residual spraying of insecticide (OR 35.0, 95% CI: 4.80–254.9, P < 0.001), no ITN use (OR 30.1, 95% CI: 6.37–142.7, P < 0.001), engaging in outdoor activities (OR 22.0, 95% CI: 3.42–141.8, P = 0.001), and age < 16 years (OR 8.36, 95% CI: 2.22–56.2, P = 0.03) were associated with increased odds of malaria. Kampala residents who traveled overnight out of the city were at substantially higher risk of malaria than those who did not travel. For these travelers, personal protection measures, including sleeping under an ITN when traveling, should be advocated.
Prevalence of Asymptomatic Malaria Parasitemia in Odisha, India: A Challenge to Malaria Elimination
The prevalence of malaria in India is decreasing, but it remains a major concern for public health administration. The role of submicroscopic malaria and asymptomatic malaria parasitemia and their persistence is being explored. A cross-sectional survey was conducted in the Kandhamal district of Odisha (India) during May–June 2017. Blood samples were collected from 1897 individuals for screening of asymptomatic parasitemia. Samples were screened using rapid diagnostic tests (RDTs) and examined microscopically for Plasmodium species. Approximately 30% of randomly selected samples (n = 586) were analyzed using real-time PCR (qPCR), and the genetic diversity of Plasmodium falciparum was analyzed.
The prevalence of Plasmodium species among asymptomatic individuals detected using qPCR was 18%, which was significantly higher than that detected by microscopy examination (5.5%) or RDT (7.3%). Of these, 37% had submicroscopic malaria. The species-specific prevalence among asymptomatic malaria-positive cases for P. falciparum, Plasmodium vivax, and mixed infection (P. falciparum and P. vivax) by qPCR was 57%, 29%, and 14%, respectively. The multiplicity of infection was 1.6 and 1.2 for the merozoite surface protein-1 gene (msp1) and (msp2), respectively. Expected heterozygosity was 0.64 and 0.47 for msp1 and msp2, respectively. A significant proportion of the study population, 105/586 (18%), was found to be a reservoir for malaria infection, and identification of this group will help in the development of elimination strategies.
Travel Is a Key Risk Factor for Malaria Transmission in Pre-Elimination Settings in Sub-Saharan Africa: A Review of the Literature and Meta-Analysis
By sustaining transmission or causing malaria outbreaks, imported malaria undermines malaria elimination efforts. Few studies have examined the impact of travel on malaria epidemiology. We conducted a literature review and meta-analysis of studies investigating travel as a risk factor for malaria infection in sub-Saharan Africa using PubMed. We identified 22 studies and calculated a random-effects meta-analysis pooled odds ratio (OR) of 3.77 (95% CI: 2.49–5.70), indicating that travel is a significant risk factor for malaria infection.
Odds ratios were particularly high in urban locations when travel was to rural areas, to more endemic/high transmission areas, and in young children. Although there was substantial heterogeneity in the magnitude of association across the studies, the pooled estimate and directional consistency support travel as an important risk factor for malaria infection.
Indoor Residual Spraying &Integrated Vector Management &ITNs &Monkeys &Mosquitoes &Nigeria &Plasmodium/Parasite &Seasonal Malaria Chemoprevention &Urban &Vector Control Bill Brieger | 21 Sep 2020
Malaria News Today 2020-09-21: Vectors, Cities and Chimpanzees
First we look at how disease can influence urban planning. We have four news stories focus on field activities for vector control from Hyderabad, India, Borno State, Nigeria, Papua New Guinea and CHAD. Finally there is an ancestry article of sorts examining plasmodia in chimpanzees and humans. Click on the links to read full details.
Can Covid-19 inspire a new way of planning African cities?
 Health crises are not new in Africa. The continent has grappled with infectious diseases on all levels, from local (such as malaria) to regional (Ebola) to global (Covid-19). The region has often carried a disproportionately high burden of global infectious outbreaks.
Health crises are not new in Africa. The continent has grappled with infectious diseases on all levels, from local (such as malaria) to regional (Ebola) to global (Covid-19). The region has often carried a disproportionately high burden of global infectious outbreaks.
How cities are planned is critical for managing infectious diseases. Historically, many urban planning innovations emerged in response to health crises. The global cholera epidemic in the 1800s led to improved urban sanitation systems. Respiratory infections in overcrowded slums in Europe inspired modern housing regulations during the industrial era.
Urban planning in Africa during colonisation followed a similar pattern. In Anglophone Africa, cholera and bubonic plague outbreaks in Nairobi (Kenya) and Lagos (Nigeria) led to new urban planning strategies. These included slum clearance and urban infrastructure upgrades. Urban planning in French colonial Africa similarly focused on health and hygiene issues, but also safety and security.
Unfortunately regional experiences with cholera, malaria and even Ebola in African cities provide little evidence that they have triggered a new urban planning ethic that prioritises infectious outbreaks. Our recent research paper discusses three areas that can transform urban planning in the continent to prepare for future infectious outbreaks, using lessons from Covid-19.
The Coronavirus and other viruses like Ebola have always been ‘out there’ in nature.
 But it’s only when we disrupt the natural habitats of the wild animals. Deadly viruses stay beneath the surface and need just one moment of triggering to emerge in the atmosphere and take the world by storm – historian Dr Mark Honigsbaum. The point is we cannot prevent all spillover events or predict precisely when or where the next one will happen. What we can do — and should do often — is invest in local laboratories and diagnostic services so that we can spot unusual outbreaks early and close them down quickly
But it’s only when we disrupt the natural habitats of the wild animals. Deadly viruses stay beneath the surface and need just one moment of triggering to emerge in the atmosphere and take the world by storm – historian Dr Mark Honigsbaum. The point is we cannot prevent all spillover events or predict precisely when or where the next one will happen. What we can do — and should do often — is invest in local laboratories and diagnostic services so that we can spot unusual outbreaks early and close them down quickly
We should note that Plasmidium Knowlesi is an example of a form of malaria from monkeys that arose because of urban expansion on forest habitats.
Hyderabad: People sensitised on mosquito breeding
As part of a novel initiative, every Sunday 10 am, 10 minute programme, the entomology wing of Greater Hyderabad Municipal Corporation conducted awareness drive on mosquito breeding grounds at various places on Sunday. They explained the importance of cleanliness and the ways the mosquito breeding takes place in stagnated water. Speaking on the occasion, Banjara Hills Corporator Gadwal Vijayalaxmi called upon everyone not to allow accumulation of water in containers, utensils and surroundings.
Borno, WHO Administer Malaria Prevention Drug on 2.1m Children
WHO National Coordinator Malaria Emergencies in Nigeria, Dr. Iniabasi Nglas gave the figure during a four round Malaria Chemoprevention Campaigns (MPCs aka SMC) in 25 of the 27 local government areas of Borno State. During the advocacy, Nglas said the IDP camps “are given special attention for there is high threat of malaria infection due to the environment. Record has shown that the treatment has reduced malaria morbidity in the state.” She revealed that during the first cycle, 1.9 million children were targeted but due to high reception 2.1 million children were administered with the drug.
Rotary Against Malaria Distributes Nets in PNG
ROTARY Against Malaria has finally completed its distribution of bed net mosquito nets throughout the Eastern Highlands Province (EHP) after three months. Team leader of Rotary Against Malaria in the province, Helmut Magino, during a ceremony in Goroka, acknowledged his working staff, the Eastern Highlands Provincial Health Authority, district health officers, logistic company Mapai Transport, Summer Institute of Linguistics (SIL)
and the communities in Papua New Guinea.
“Without these partners, our work in distributing mosquito nets wouldn’t have been successful,” Mr Magino said. “Mapai Transport assisted with vehicles to travel to the remote parts in Okapa, Henganofi and Lufa. “SIL assisted with distribution via airplane to remote parts which are not connected by road like in Obura-Wonenara district.” The volunteer-run organisation funded by Global Fund, a US-based organisation, distributed 145,900 mosquito nets in the province. “We distributed around 45,000 nets to Okapa and Lufa, 35,000 to Obura-Wonenara and 66,900 to rural areas in Goroka district. “We will visit EHP again next year to distribute nets …”
Donating Emergency IRS Supplies to CHAD
Last week, despite the COVID-19 pandemic, a Hercules military transport aircraft took off from an Israeli military base in the south, filled to capacity with items donated by Israeli Flying Aid IFA and the American Jewish Committee (AJC) — 2,000 six-person tents, personal protection equipment (PPE) for medical teams, backpack sprayers to eradicate malaria-carrying mosquitos, and more.
Why humans can run marathons and apes cannot (implication for plasmodium species)
Chimpanzees share more than 99 percent of their genes with modern humans, but the CMAH gene is one of the areas of difference. Two to three million years ago, gorillas, chimpanzees, and other primates were dying from a type of malaria called Plasmodium reichenowi (Science, 2011;331:540-542). At that time, all primates had a surface protein called Neu5Gc on their cells that was made from Neu5Ac. Then along came a primate with a gene that had lost its ability to make Neu5Gc from Neu5Ac, so it had only Neu5Ac (Proc Natl Acad Sci USA, Sept 6, 2005;102(36):12819-12824).
That pre-human did not die from malaria like other primates, his and her children lived and proliferated, and today their descendants (all humans) have a gene that makes Neu5Ac instead of Neu5Gc. As often happens in nature, the malaria parasite then modified its genetic makeup into a variant called Plasmodium falciparum which can infect humans, but not chimpanzees, so today humans can be infected only with Plasmodium falciparum and chimpanzees can be infected only with Plasmodium reichenowi. This same genetic mutation gave homo sapiens greater endurance so they were able to run long distances while the apes could not, which gave humans an advantage in hunting for food (J Hum Evol, 2014;66:64-82).
COVID-19 &Indoor Residual Spraying &Integrated Vector Management &IRS &Mosquitoes Bill Brieger | 20 Sep 2020
Malaria News Today 2020-09-20: Controlling Mosquitoes
 Abstracts and news look at mosquito control measures including screening eaves and indoor residual spraying from Malaria Journal. Mosquito-associated bacteria, fungi, and even viruses represent untapped tools. Finally one can buy and wear a face mask and help eliminate malaria. Click the links to get more information
Abstracts and news look at mosquito control measures including screening eaves and indoor residual spraying from Malaria Journal. Mosquito-associated bacteria, fungi, and even viruses represent untapped tools. Finally one can buy and wear a face mask and help eliminate malaria. Click the links to get more information
Evaluating effectiveness of screening house eaves
… a potential intervention for reducing indoor vector densities and malaria prevalence in Nyabondo, western Kenya. Mosquito-proofing of houses using wire mesh screens is gaining greater recognition as a practical intervention for reducing exposure to malaria transmitting mosquitoes. Screening potentially protects all persons sleeping inside the house against transmission of mosquito-borne diseases indoors. The study assessed the effectiveness of house eaves screening in reducing indoor vector densities and malaria prevalence in Nyabondo, western Kenya. 160 houses were selected for the study, with half of them randomly chosen for eaves screening with fibre-glass coated wire mesh (experimental group) and the other half left without screening (control group).
At all the three parasitological follow-up survey points, house screening significantly reduced the malaria prevalence by 100% (p?<?0.001), 63.6% (p?=?0.026), and 100% (p?<?0.001) in the 1st, 2nd and 3rd follow-up surveys respectively. The study demonstrated that house eave screening has potential to reduce indoor vector densities and malaria prevalence in high transmission areas.
Rapid reduction of malaria transmission following the introduction of indoor residual spraying
… in previously unsprayed districts: an observational analysis of Mopti Region, Mali, in 2017. The National Malaria Control Programme (NMCP) of Mali has had recent success decreasing malaria transmission using 3rd generation indoor residual spraying (IRS) products in areas with pyrethroid resistance, primarily in Ségou and Koulikoro Regions. In 2015, national survey data showed that Mopti Region had the highest under 5-year-old (u5) malaria prevalence at 54%—nearly twice the national average—despite having high access to long-lasting insecticidal nets (LLINs) and seasonal malaria chemoprevention (SMC). Accordingly, in 2016 the NMCP and other stakeholders shifted IRS activities from Ségou to Mopti. A set of retrospective, eco-observational time-series analyses were performed using monthly incidence rates of rapid diagnostic test (RDT)-confirmed malaria cases reported in the District Health Information System 2 (DHIS2) from January 2016 until February 2018.
At HFs in communities of Mopti where IRS was introduced in 2017, peak incidence fell by an average of 42% (CI95 31–63%) between these years, a significantly greater decrease (p?=?0.040) almost double what was seen in the comparator HFCAs. The opposite effect was observed in Ségou Region, where peak incidence at those HFs where IRS was withdrawn after the 2016 campaign increased by an average of 106% (CI95 63–150%) from year to year, also a significant difference-in-differences compared to the comparator no-IRS HFs (p?<?0.0001).
Annual IRS campaigns continue to make dramatic contributions to the seasonal reduction of malaria transmission in communities across central Mali, where IRS campaigns were timed in advance of peak seasonal transmission and utilized a micro-encapsulated product with an active ingredient that was of a different class than the one found on the LLINs used throughout the region and to which local malaria vectors were shown to be susceptible. Strategies to help mitigate the resurgence of malaria cases that can be expected should be prioritized whenever the suspension of IRS activities in a particular region is considered.
COVID-19 Mask Raises Money for Malaria Elimination
Goodbye Malaria was founded by African entrepreneurs who truly believe African creativity is the key to solving Africa’s biggest problems. “From saving lives to saving livelihoods – the birth of the Goodbye Malaria mask.” Mask initiative helps to raise funds support on-the-ground malaria elimination in Southern Africa. it empowers local crafters to create stylish merchandise using Goodbye Malaria’s iconic shwe shwe fabric. Goodbye Malaria co-founder Kim Lazarus said: “We have never asked the public for donations, instead, offering consumers an opportunity to support malaria elimination efforts through their purchase of our merchandise.” (see photo above)
Prospects and Pitfalls: Next-Generation Tools to Control Mosquito-Transmitted Disease
Annual Review of Microbiology reports that Mosquito-transmitted diseases, including malaria and dengue, are a major threat to human health around the globe, affecting millions each year. A diverse array of next-generation tools has been designed to eliminate mosquito populations or to replace them with mosquitoes that are less capable of transmitting key pathogens. Many of these new approaches have been built on recent advances in CRISPR/Cas9-based genome editing. These initiatives have driven the development of pathogen-resistant lines, new genetics-based sexing methods, and new methods of driving desirable genetic traits into mosquito populations.
Many other emerging tools involve microorganisms, including two strategies involving Wolbachia that are achieving great success in the field. At the same time, other mosquito-associated bacteria, fungi, and even viruses represent untapped sources of new mosquitocidal or antipathogen compounds. Although there are still hurdles to be overcome, the prospect that such approaches will reduce the impact of these diseases is highly encouraging.
Children &Indoor Residual Spraying &IPTp &ITNs &Malaria in Pregnancy Bill Brieger | 23 Feb 2020
Preventing Malaria in Mozambique: the 2018 Malaria Indicator Survey Summarized
 The Demographic and Health Survey Program has recently released the 2018 Malaria Indicator Survey for Mozambique. Below is a summary of some of the key findings. These focus on access and use of insecticide-treated nets, intermittent preventive treatment in pregnancy and case management
The Demographic and Health Survey Program has recently released the 2018 Malaria Indicator Survey for Mozambique. Below is a summary of some of the key findings. These focus on access and use of insecticide-treated nets, intermittent preventive treatment in pregnancy and case management
While “82% of Mozambican households have at least one ITN, and half have at least one ITN for each two people,” these achievements do not reach universal coverage targets. That said, the ownership of at least one net by a household did increase from 51% in 2011 to the recent 82%. Likewise 23% of households met the universal coverage target of one net per two people in a household in 2011 compared to 51% in 2018. The pace of progress may appear good, but this must be seen in light of lack of growth in donor funding and greater calls for countries to assume more financial responsibility for disease control.
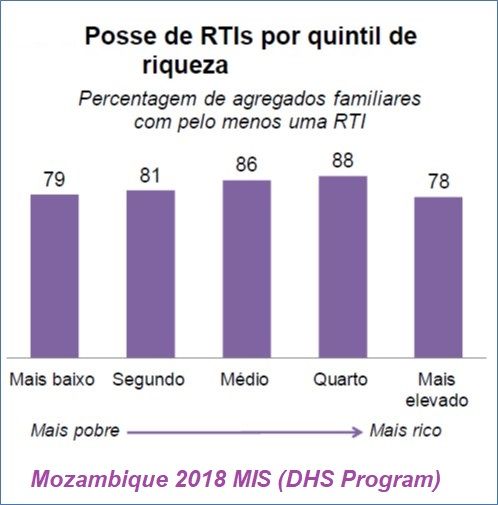 Of interest is the fact that net ownership is spread somewhat evenly over the economic class quintiles. Ideally we would want to see better ownership figures for the lower quintiles.
Of interest is the fact that net ownership is spread somewhat evenly over the economic class quintiles. Ideally we would want to see better ownership figures for the lower quintiles.
Households obtained their nets from three major sources. “Most ITNs (87%) were obtained in mass distribution campaigns, 4% in prenatal consultations (PNC) and 6% are purchased in stores or markets.” While the proportion getting their nets through PNC may roughly reflect the proportion of the population who are pregnant at a given time, the survey is not specifically a snapshot of this population in real time. Thus, one could question whether distribution of ITNs through routine health services is fully functioning.
Since it was noted that only half of households have the ideal number of ITNs to reach universal coverage of their members, it is not surprising that only, “69% of the population of households’ family members have access to an ITN. This means that 7 in every 10 people could sleep under an ITN if each ITN in a household were used by a maximum of two people.” On the positive side, this represents an approximate doubling of use of ITNs since 2011.
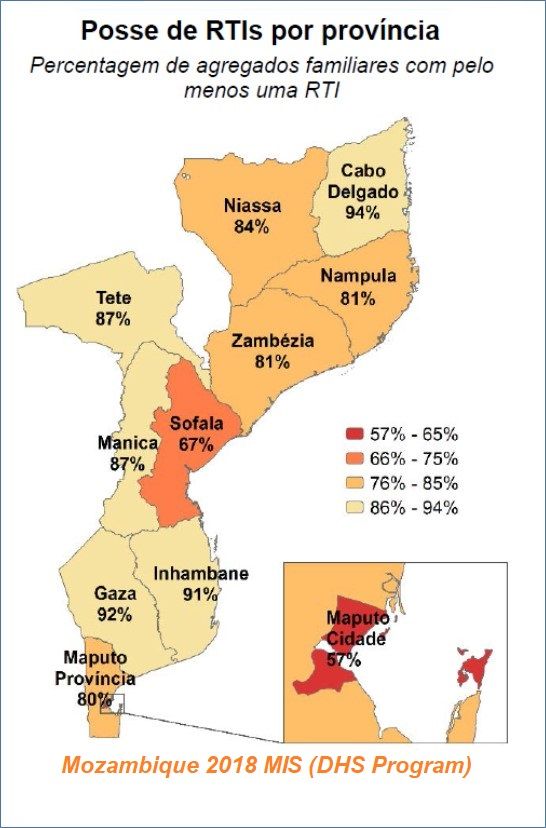 The survey further notes that those segments of the population traditionally viewed as “vulnerable” fared a bit better: “73% of children under 5 years and 76% of pregnant women slept under an ITN the night before investigation.” This too, represents a doubling from 2011. There is also geographical variation where it appears that the more rural provinces have higher rates of use.
The survey further notes that those segments of the population traditionally viewed as “vulnerable” fared a bit better: “73% of children under 5 years and 76% of pregnant women slept under an ITN the night before investigation.” This too, represents a doubling from 2011. There is also geographical variation where it appears that the more rural provinces have higher rates of use.
It would appear that IRS is not a major component of malaria control. Household coverage with indoor residual spray “decreased from 19% in 2011 to 11% in 2015, and then increased to 16% in 2018.” Urban coverage (23%) of IRS in the twelve months prior to the survey is twice as high as the percentage in rural areas (12%).
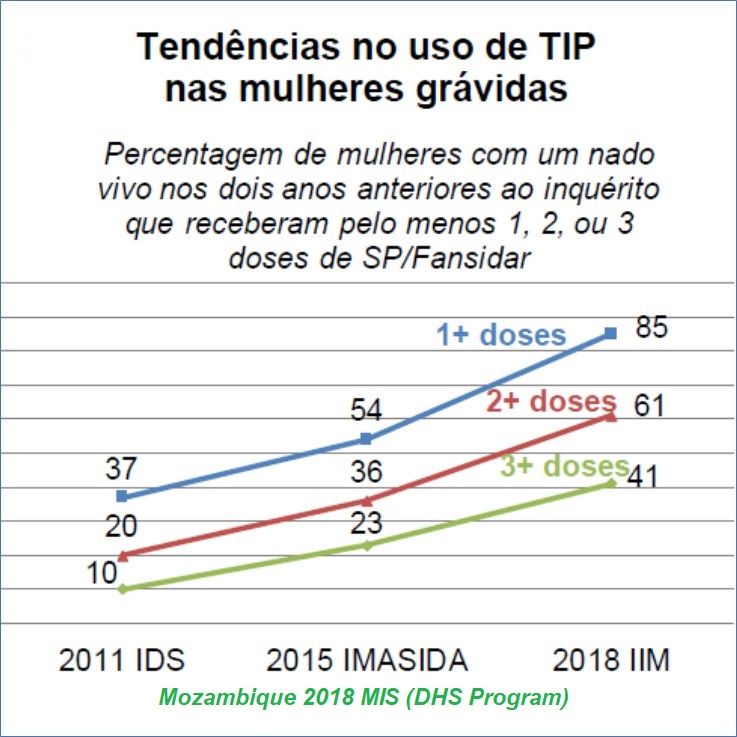 Although still not meeting targets, Mozambique has seen major progress in providing IPTp for pregnant women. Over the period from 2011 to 2018 the proportion of pregnant women receiving even one dose rose from 37% to 85%. Since WHO has set targets for at least 3 monthly doses from the 13th week of pregnancy, Mozambique’s coverage of the third dose increased from 10% to 41% with wide variation among provinces.
Although still not meeting targets, Mozambique has seen major progress in providing IPTp for pregnant women. Over the period from 2011 to 2018 the proportion of pregnant women receiving even one dose rose from 37% to 85%. Since WHO has set targets for at least 3 monthly doses from the 13th week of pregnancy, Mozambique’s coverage of the third dose increased from 10% to 41% with wide variation among provinces.
UNICEF shared data from 2015 to show that 51% of pregnant women in Mozambique attended 4 PNC/ANC visits, implying that there are missed opportunities for achieving at least 3 doses of IPTp. Also, since more women are now getting the first dose of IPTp, hopefully more can also get an ITN at PNC.
These national surveys (MIS, DHS) are invaluable for assessing progress and planning what interventions need to be strengthened where and among whom. They also show that progress is slow, reinforcing global concerns that malaria elimination will still be a challenge by 2050.
Borders &Diagnosis &Elimination &Environment &Gender &Health Education &Health Workers &Indoor Residual Spraying &IRS &ITNs &Mosquitoes &Plasmodium/Parasite &Vector Control Bill Brieger | 07 Jul 2019
The Weekly Tropical Health News 2019-07-06: Eliminating Malaria in Low Transmission Settings
This week started with articles that drew attention to the challenges of malaria in low transmission areas and with low density infections. Malaria Journal has provided several insightful articles toward this end.
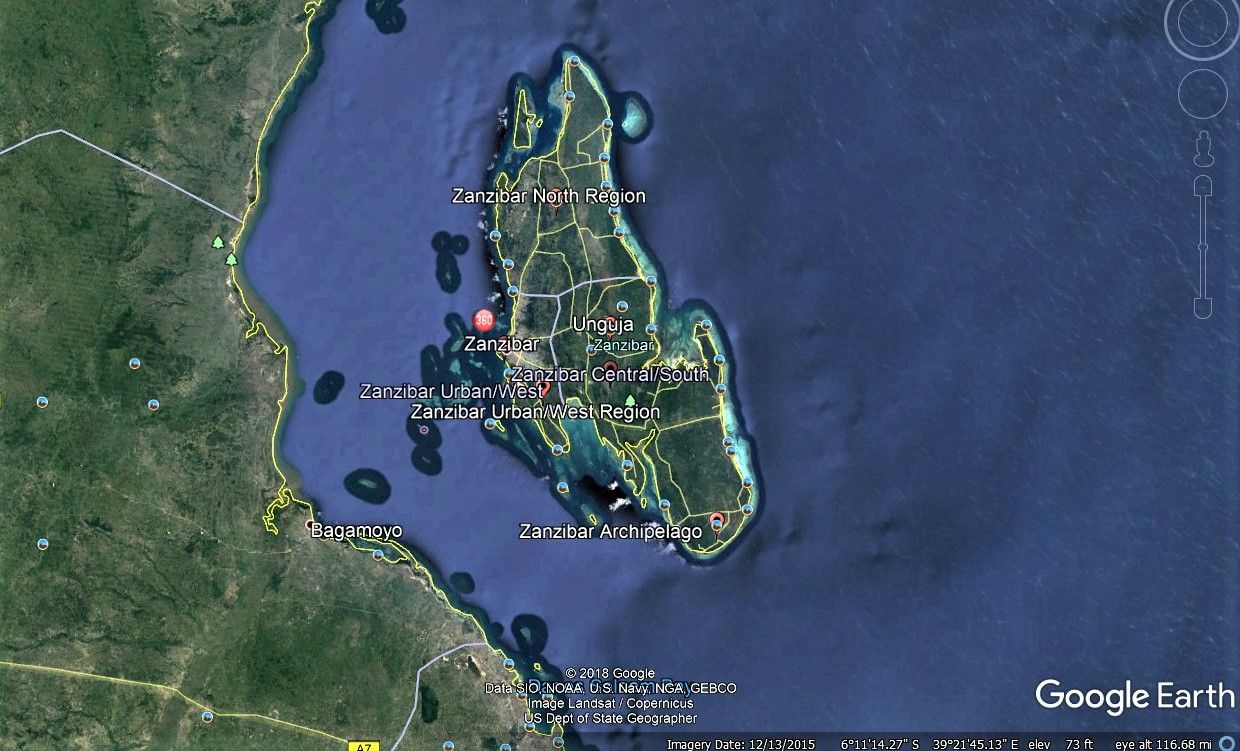 Being an island has certainly helped Zanzibar make progress toward malaria elimination as witness the fact that malaria prevalence has remained below 1% for the past decade. Not only does Zanzibar still face threats of infection from the mainland, it may also experience an upsurge locally if residual transmission and the role of human behavior and community actions are not well understood. April Monroe et al. conducted in-depth interviews with community members and local leaders across six sites on Unguja, Zanzibar as well as semi-structured community observations of night-time activities and special events to learn more.
Being an island has certainly helped Zanzibar make progress toward malaria elimination as witness the fact that malaria prevalence has remained below 1% for the past decade. Not only does Zanzibar still face threats of infection from the mainland, it may also experience an upsurge locally if residual transmission and the role of human behavior and community actions are not well understood. April Monroe et al. conducted in-depth interviews with community members and local leaders across six sites on Unguja, Zanzibar as well as semi-structured community observations of night-time activities and special events to learn more.
While there was high reported ITN use, there were also times when people were exposed t mosquitoes while being outdoors during biting times. This could be around the house, or at special night events like such as weddings, funerals, and religious ceremonies. Men spent more time outdoors than women. Clearly appropriate interventions and needed and should be promoted in culturally appropriate ways in order to further reduce and eventually eliminate transmission.
Angela Early and colleagues presented findings on a diagnostic process of deep sequencing for understanding the dynamics and complexity of Plasmodium infections, but stress that knowing the lower limit of detection is challenging. They present “a new amplicon analysis tool, the Parallel Amplicon Sequencing Error Correction (PASEC) pipeline, is used to evaluate the performance of amplicon sequencing on low-density Plasmodium DNA samples.”
The authors learned that, “four state-of-the-art tools resolved known haplotype mixtures with similar sensitivity and precision.” They also cautioned that, “Samples with very low parasitemia and very low read count have higher false positive rates and call for read count thresholds that are higher than current default recommendations.” Better understanding of the genetic mix of plasmodium infections as countries move toward low transmission and elimination is crucial for selecting appropriate interventions and evaluating their outcomes.
 Hannah Edwards and co-researchers examined conditions for malaria transmission along the Thailand-Myanmar border in areas approaching malaria elimination. While prevalence may be less than 1%, residual transmission still occurs. Transmission occurs not only around residences but in the forests where people work. The researchers therefore looked at the behavior of both humans and insects. Overall, they found that, “Community members frequently stayed overnight at subsistence farm huts or in the forest. Entomological collections showed higher biting rates of primary vectors in forested farm hut sites and in a more forested village setting compared to a village with clustered housing and better infrastructure.”
Hannah Edwards and co-researchers examined conditions for malaria transmission along the Thailand-Myanmar border in areas approaching malaria elimination. While prevalence may be less than 1%, residual transmission still occurs. Transmission occurs not only around residences but in the forests where people work. The researchers therefore looked at the behavior of both humans and insects. Overall, they found that, “Community members frequently stayed overnight at subsistence farm huts or in the forest. Entomological collections showed higher biting rates of primary vectors in forested farm hut sites and in a more forested village setting compared to a village with clustered housing and better infrastructure.”
While mosquitoes preferred to bite inside huts, their threat was magnified by those who did not use long lasting insecticide-treated nets (LLINs). While out in the farms and forests, people tended to wake early and increase their likelihood of being bitten. The authors discuss the challenges of dual residences in terms of LLIN ownership and even concerning the potential access to indoor residual spraying. The definition for universal net coverage needs to expand from one net per two people to include adequate nets wherever people are located.
 The Amazonian area of Brazil is another area working toward malaria elimination, in particular, Plasmodium vivax. Felipe Leão Gomes Murta et al. also looked at the human side of the equation and identified misperceptions by both community members and health workers that could inhibit elimination efforts. They found, “many myths regarding malaria transmission and treatment that may hinder the sensitization of the population of this region in relation to the use of current control tools and elimination strategies, such as mass drug administration (MDA),” and LLINs.
The Amazonian area of Brazil is another area working toward malaria elimination, in particular, Plasmodium vivax. Felipe Leão Gomes Murta et al. also looked at the human side of the equation and identified misperceptions by both community members and health workers that could inhibit elimination efforts. They found, “many myths regarding malaria transmission and treatment that may hinder the sensitization of the population of this region in relation to the use of current control tools and elimination strategies, such as mass drug administration (MDA),” and LLINs.
Problematic perceptions included mention by both groups that the use of insecticide-treated nets, may cause skin irritations and allergies. Both community members and health professionals said malaria is “an impossible disease to eliminate because it is intrinsically associated with forest landscapes.” They concluded that such perceptions can be a barrier to control and elimination.
Efforts to eliminate malaria from low transmission settings are an essential to the overall global goals. These four articles tell us that close attention to and better understanding of humans, parasites and mosquitoes is still needed to achieve these goals.
Elimination &Indoor Residual Spraying &Integrated Vector Management Bill Brieger | 02 Oct 2015
Initial Evidence Of A Reduction In Malaria Incidence Following Indoor Residual Spraying With Actellic 300 Cs In A Setting With Pyrethroid Resistance: Mutasa District, Zimbabwe
Mufaro Kanyangarara and her PhD thesis adviser, Luke Mullany of the Johns Hopkins Bloomberg School of Public Health Department of International Health, have been looking into the challenges of controlling and eventually eliminating malaria in a multi-country context in southern Africa. We are sharing abstracts from her pioneering work including the following which explores indoor residual spraying in Zimbabwe in a District near the Mozambique border.
 In order to reduce the vector population and interrupt disease transmission, IRS with appropriate insecticides is essential. In response to local vector resistance, the Zimbabwe NMCP with support from PMI began a large-scale IRS campaign with organophosphates in four high transmission districts in Manicaland province – Chimanimani, Mutare, Mutasa and Nyanga. Using HMIS data, the present study reports on the effect of switching from pyretheroids to OP on malaria morbidity in one of the four high transmission districts selected. In the subsequent high transmission season following the switch from pyretheroids to organophosphates, there was evidence of a 43% decline in malaria incidence reported by health facilities from wards in Mutasa District treated with organophosphates, after accounting for possible confounding by environmental variables. Previous research shows that switching to organophospates effectively reduced biting rates and vector densities in areas with pyretheroid resistant strains in Ghana, Benin and Tanzania. Although previous research focused on using entomological data to show the reduction in the vector population following application of Actellic, organophosphates, this study adds to the literature by showing a decline in malaria transmission using health facility surveillance data.
In order to reduce the vector population and interrupt disease transmission, IRS with appropriate insecticides is essential. In response to local vector resistance, the Zimbabwe NMCP with support from PMI began a large-scale IRS campaign with organophosphates in four high transmission districts in Manicaland province – Chimanimani, Mutare, Mutasa and Nyanga. Using HMIS data, the present study reports on the effect of switching from pyretheroids to OP on malaria morbidity in one of the four high transmission districts selected. In the subsequent high transmission season following the switch from pyretheroids to organophosphates, there was evidence of a 43% decline in malaria incidence reported by health facilities from wards in Mutasa District treated with organophosphates, after accounting for possible confounding by environmental variables. Previous research shows that switching to organophospates effectively reduced biting rates and vector densities in areas with pyretheroid resistant strains in Ghana, Benin and Tanzania. Although previous research focused on using entomological data to show the reduction in the vector population following application of Actellic, organophosphates, this study adds to the literature by showing a decline in malaria transmission using health facility surveillance data.
In the present study, there were variations in rainfall and temperature over the study period, and these changes were associated with changes in malaria incidence. The study results also indicated malaria transmission in Mutasa District was driven by rainfall, proximity to second order streams, elevation and temperature. These results concur with previous research, which found that elevation, temperature, and rainfall are positively associated with malaria incidence. After adjustment for climatic variables and seasonality, malaria incidence rates a downward trend following the 2014 IRS campaign and thus supporting the plausible conclusion that switching to organophosphates in this setting contributed to the observed public health benefits. No major political, socio-economic, or health-care changes with the potential to reduce malaria morbidity by almost half occurred in Mutasa District during the study period.
 Typically data from health facilities only includes data on the number of suspected cases. The HMIS in Zimbabwe is more sophisticated in that it allows reports of confirmed malaria cases. In calculating of incidence rates, the denominator used was the catchment area population size. The reliability of this value has been questioned as this assumes that people will visit the closest health facility/health facility in their catchment area. It is noteworthy to mention that in the present study the main results did not chance after including an offset for catchment area population size. This indicates that in the Zimbabwean context, the reported catchment area population size may be a reliable estimate. The study also underscores the utility of HMIS data in the evaluation of population level interventions. The HMIS has the advantage of providing quality data quickly and easily, with minimal additional investment. Additionally, HMIS reflects the burden of disease on the health system. Results from this study further suggest that passive surveillance data from the HMIS in Zimbabwe was sufficiently sensitive to detect IRS related reduction in malaria morbidity among residents of Mutasa District.
Typically data from health facilities only includes data on the number of suspected cases. The HMIS in Zimbabwe is more sophisticated in that it allows reports of confirmed malaria cases. In calculating of incidence rates, the denominator used was the catchment area population size. The reliability of this value has been questioned as this assumes that people will visit the closest health facility/health facility in their catchment area. It is noteworthy to mention that in the present study the main results did not chance after including an offset for catchment area population size. This indicates that in the Zimbabwean context, the reported catchment area population size may be a reliable estimate. The study also underscores the utility of HMIS data in the evaluation of population level interventions. The HMIS has the advantage of providing quality data quickly and easily, with minimal additional investment. Additionally, HMIS reflects the burden of disease on the health system. Results from this study further suggest that passive surveillance data from the HMIS in Zimbabwe was sufficiently sensitive to detect IRS related reduction in malaria morbidity among residents of Mutasa District.
There are several important limitations of this study that should be highlighted. Causal inferences between spraying and improvements in malaria incidence should be made with caution as spraying was not implemented as an intervention in a randomized control trial. However, data from 14 health facilities located in unsprayed wards were included in the analysis to serve as a comparison and help understand any possible changes in malaria morbidity unassociated with the 2014 IRS campaign. Although the univariate model indicated that health facilities in unsprayed wards carried a lower burden of malaria, the multivariable model showed no significant differences between health facilities in sprayed and unsprayed wards prior to the IRS pilot, suggesting that climatic variables included in the model adequately adjusted for differences. However, it should be noted that although the study adjusted for environmental factors, it did not account for other factors like population movement, changes in treatment seeking behaviors, changes in the coverage of ITNs during the study period. The model developed in this analysis assumed that these factors remained constant over the study period. This seems reasonable given that the rural population of Mutasa is relatively stable, with access to health facilities providing malaria diagnosis and treatment. Additionally, although the number of suspected malaria cases was not explicitly model, a descriptive analysis does not indicate changes in diagnostic practice over the study period (data not shown). The HMIS in Zimbabwe has been in place for decades and has previously been used to evaluate the impact of changes in malaria morbidity, construct empirical seasonality maps and describe the spatial and temporal distribution of malaria.
Despite these potential limitations, health surveillance systems provide a feasible and efficient means of collecting longitudinal data on measures of malaria morbidity. The pronounced decline in malaria morbidity observed in this study is evidence supporting the benefit of switching to an insecticide class with a different mode of action in response to pyretheroid resistance. Although the IRS strategy implemented by ZNMCP and PMI was successful, continued entomological monitoring will be necessary. Additionally, with emerging resistance to multiple insecticides, this approach may not be sustainable over time. There is need for the development of novel strategies to manage insecticide resistance.
Borders &Elimination &Indoor Residual Spraying &Monitoring &Surveillance &Vector Control Bill Brieger | 13 Jun 2015
Moving toward Malaria Elimination in Botswana
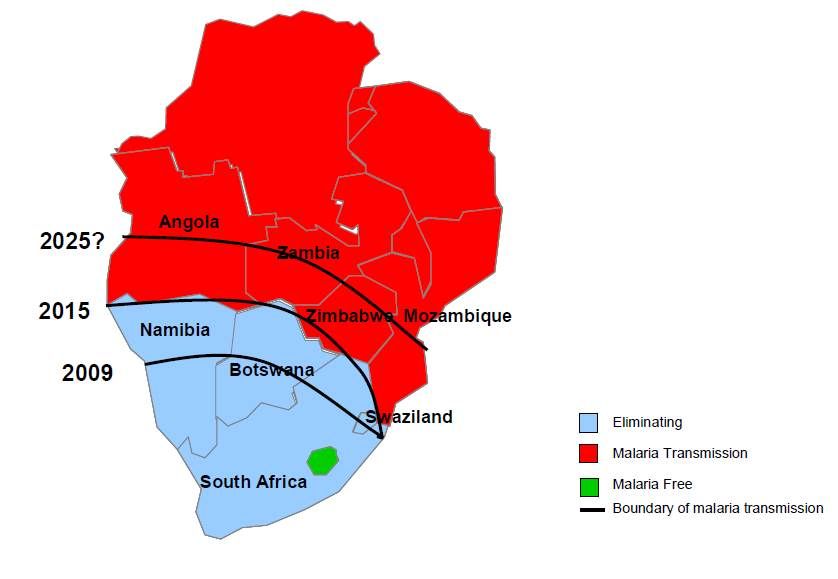 The just concluded 2015 Global Health Conference in Botswana, hosted by Boitekanelo College at Gaborone International Convention Centre on 11-12 June provided us a good opportunity to examine how Botswana is moving toward malaria elimination. Botswana is one of the four front line malaria elimination countries in the Southern African Development Community and offers lessons for other countries in the region. Combined with the 4 neighboring countries to the north, they are known collectively as the “Elimination Eight”.
The just concluded 2015 Global Health Conference in Botswana, hosted by Boitekanelo College at Gaborone International Convention Centre on 11-12 June provided us a good opportunity to examine how Botswana is moving toward malaria elimination. Botswana is one of the four front line malaria elimination countries in the Southern African Development Community and offers lessons for other countries in the region. Combined with the 4 neighboring countries to the north, they are known collectively as the “Elimination Eight”.
The malaria elimination countries are characterised by low leves of transmission in focal areas of the country, often in seasonal or epidemic form. The pathway to malaria elimination requires that a country or defined areas in a country reach a slide positivity rates during peak malaria season of < 5%.
 Chihanga Simon et al. provide us a good outline of 60+ years of Botswana’s movements along the pathway beginning with indoor residual spraying (IRS) in the 1950s. Since then the country has expanded vector control to strengthened case management and surveillance. Particular recent milestones include –
Chihanga Simon et al. provide us a good outline of 60+ years of Botswana’s movements along the pathway beginning with indoor residual spraying (IRS) in the 1950s. Since then the country has expanded vector control to strengthened case management and surveillance. Particular recent milestones include –
- 2009: Malaria elimination policy required all cases to be tested before treatment malaria elimination target set for 2015
- 2010: Malaria Strategic Plan 2010–15 using recommendations from programme review of 2009; free LLINs
- 2012: Case-based surveillance introduced
The national malaria elimination strategy includes the following: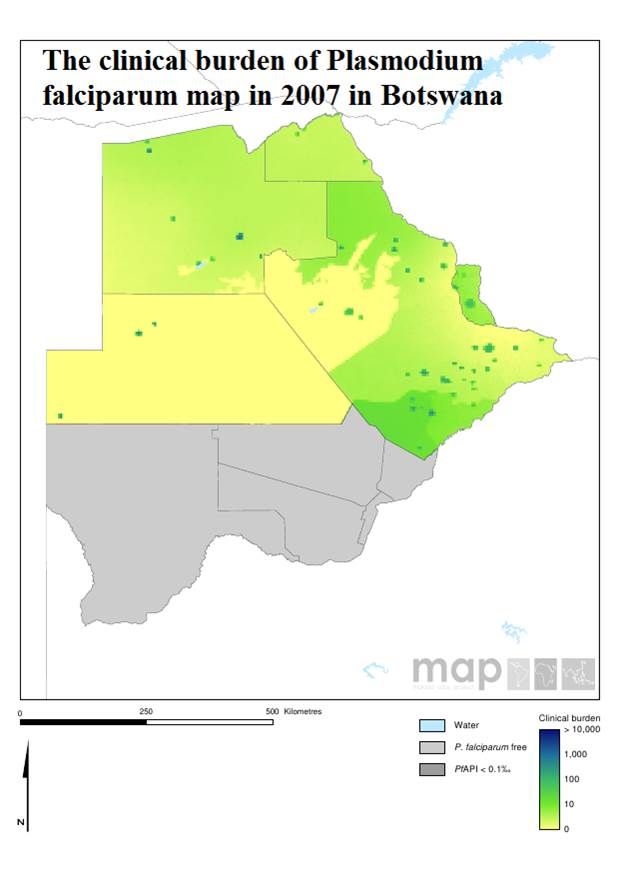
- Focus distribution LLIN & IRS in all transmission foci/high risk districts
- Detect all malaria infections through appropriate diagnostic methods and provide effective treatment
- Develop a robust information system for tracking of progress and decision making
- Build capacity at all levels for malaria elimination
Botswana like other malaria endemic countries works with the Roll Back Malaria Partnership to compile an annual road map that identifies progress made and areas for improvement. The 2015 Road Map shows that –
- 116,229 LLINs distributed during campaigns in order to maintain universal coverage in the 6 high risk districts
- 200,721 IRS Operational Target structures sprayed
- 2,183,238 RDTs distributed and 9,876 microscopes distributed
- While M&E, Behavior Change, and Program Management Capacity activities are underway
 Finally the African Leaders Malaria Alliance (ALMA) provides quarterly scorecards on each member. Botswana is making a major financial commitment to its malaria elimination commodity and policy needs. There is still need to sustain high levels of IRS coverage in designated areas.
Finally the African Leaders Malaria Alliance (ALMA) provides quarterly scorecards on each member. Botswana is making a major financial commitment to its malaria elimination commodity and policy needs. There is still need to sustain high levels of IRS coverage in designated areas.
Monitoring and evaluation is crucial to malaria elimination. Botswana has a detailed M&E plan that includes a geo-referenced surveillance system, GIS and malaria database training for 60 health care workers, traininf for at least 80% of health workers on Case Based Surveillance in 29 districts, and regular data analysis and feedback.
M&E activities also involve supervision visits for mapping of cases, foci and interventions, bi-annual malaria case management audits, enhanced diagnostics through PCR and LAMP as well as Knowledge, Attitudes, Behaviour, and Practice surveys.
Malaria elimination activities are not simple. Just because cases drop, our job is easier. Botswana, like its neighbors in the ‘Elimination Eight’ is putting in place the interventions and resources needed to see malaria really come to an end in the country. Keep up the good work!
Indoor Residual Spraying &Integrated Vector Management &Mosquitoes Bill Brieger | 21 May 2014
Indoor Residual Spraying – not a one-trick pony
Jasson Urbach and Donald Roberts claim that the malaria fight is hurt by flimsy anti-DDT research as they opine in Business Day (South Africa) on 9th May 2014. They are particularly exercised by an article on possible DDT effects on bird egg shells. Despite the controversy sparked by the article, there is no evidence that any individual country nor WHO itself is recommending removal of DDT from the arsenal of chemicals used in indoor residual spraying (IRS) to control malaria.

PMI: http://www.pmi.gov/how-we-work/technical-areas/indoor-residual-spraying
There is something about DDT that raises hackles among proponents and detractors. But malaria vector control planners do have choices. WHO recommends 14 insecticides for indoor residual spraying against malaria vectors as seen below in an list updated on 25 October 2013:
- DDT
- Malathion
- Fenitrothion
- Pirimiphos-methyl
- Pirimiphos-methyl
- Bendiocarb
- Propoxur
- Alpha-cypermethrin
- Bifenthrin
- Cyfluthrin
- Deltamethrin
- Deltamethrin
- Etofenprox
- Lambda-cyhalothrin
Ironically DDT tops the list. No chemical is 100% safe, so the caveat with any of these chemicals is that, “WHO recommendations on the use of pesticides in public health are valid ONLY if linked to WHO specifications for their quality control. WHO specifications for public health pesticides are available on the Internet.
Interestingly, a bigger concern should be the potential for mosquitoes to develop resistance to any of the above mentioned insecticides. This is why it is important to avoid putting all our eggs – soft or hard shelled – in one basket. Ideally insecticides should be rotated often to prevent resistance from developing.
Decisions to embark on IRS and choice of insecticides should be based on national and sub-national environmental and epidemiological characteristics, not emotional attachment to any particular product.