Advocacy &Community &Diagnosis &Education &Elimination &Epidemiology &India &IRS &ITNs &Malaria &Plasmodium/Parasite &Procurement Supply Management &Research &Strategy &Surveys &Vaccine &Vector Control &World Malaria Day Bill Brieger | 24 Apr 2025
The Johns Hopkins Bloomberg School of Public Health Dean’s Lecture on Malaria
Professor Jane Carlton, PhD, Director of Johns Hopkins Malaria Research Institute was introduced by Dean Ellen MacKenzie to give a Dean’s Lecture entitled “Malaria: History, current status, and the promise of ‘omics and AI.”

Prof. Carlton first gave an overview of JHMRI, which was founded in 2001. She stepped into director role in 2023. She started with the encouraging premise that AI and ‘omics can supercharge our research and pointed out the power of comparative genomics on understanding parasites and disease. Her goal is to translate discovery into real world impact through collaborations.
The talk started with a brief malaria history. Malaria was described as an ancient disease and remains one of top infectious diseases worldwide. There were 2.63 million cases and more than half a million deaths in 83 endemic countries in 2023. Today 44 countries are malaria-free.
Up until now, Prof. Carlton noted, the malaria map has been shrinking. There was a precipitous decline in malaria in India from 23 million cases to 2 million. The disease is a true humanitarian issue with a large impact on people living in resource-limited settings where housing is basic and offers no protection from mosquitoes.

The JHMRI is supported by Bloomberg philanthropies, and from that base faculty research examines, among others, better methods for controlling mosquitoes (see slide), new diagnostic tests and therapeutics, and the next generation of vaccines. Key assets to support research include mosquito insectaries and a malaria parasite core. The insectaries produce 60,000 mosquitoes per week, and with these it is possible to complete the life cycle in the laboratory.
Continuing education is another important function of JHMRI which has three conferences per year including the upcoming World Malaria Day 2025 symposium. One can also learn from the Malaria Minute podcast. The upcoming “Vector Encounter” provides sharing and learning for researchers.

JHMRI studies malaria at field sites in Africa and Asia where country collaborators are partners. Emphasis is on local capacity building in countries like Zambia, Ethiopia, Kenya, and Uganda. Researchers and the national malaria control programs in these countries work hand-in-hand.
JHMRI is involved in developing the next generation of vaccines. One approach if a human monoclonal antibody that prevents malaria infections. Another develops a vaccine that transcends’ malaria parasite strains with structure guided mimicry of an essential P. falciparum receptor-ligand complex enhances cross neutralizing antibodies. A third example asks “How many parasites does it take to cause malaria?” and assesses infection likelihood through mosquito parasite burden.
To understand the theme of her talk, Prof. Carlton reviewed the promise of ‘omics and AI in the context of her work at a center of excellence in India. Pioneering work using Malaria camps in hard-to-reach villages in Odisha, India. The main activities mobilized villagers to gather for mass screening, treatment, education, and intensified vector control. From there, Indoor Residual Spraying was planned and insecticide treated bednets were distributed. Other maternal and child health activities were incorporated. After three rounds/visits in the remote villages a great drop of malaria cases was seen. WHO lauded the camps.

In addition to lessons about the importance of surveillance, mixed strategies, and community mobilization for controlling malaria, the team learned about the growing challenge of reduced effectiveness of Rapid Diagnostic Tests. The problem arose because tests were dependent on a protein that was no longer being expressed due to Pfhrp2 gene deletions, leading to false negative test results. The team was encouraged to identify more proteins to find a more stable and central one to use in testing. Through machine learning, this work is ongoing but promising.
While we are on the verge of several research and programmatic breakthroughs, Prof. Carlton reminded the audience that we are in calamitous times. She recalled that the United States has been the top donor government to malaria efforts through Presidents Malaria Initiative and Global Fund to Fight AIDS, Tuberculosis, and Malaria. PMI was founded in 2005, and has contributed to a decline in malaria death rates of close to 50%.

With suspension of funding, an estimated increase of 12.5-17.9 million malaria cases and 71,000-166,000 malaria deaths are expected this year. Already there are serious impacts on the supply chain for major malaria commodities as estimated by the Roll Back Malaria Partnership as seen on their RBM dashboard and supply chain gap estimates where six endemic countries have less than a 3-month supply of RDTs and eleven have less than a 6-month supply.
Prof Carlton ended by saying, “I think the hope is in science, right? The hope is in research. There are definitely new initiatives, new tools which are coming to the forefront, some of which I mentioned, and several of which we’re developing here at the malaria Research Institute. I do know the World Health Organization has got together with other countries to provide additional funding and support for those countries who have lost support through PMI.”
Advocacy &Announcement &Invest in Malaria Control &Research &World Malaria Day Bill Brieger | 09 Apr 2025
Prepare for World Malaria Day 2025
 The RBM Partnership to End Malaria has developed a communication kit to help plan for the upcoming World Malaria Day on April 25th. Below are some of the highlights and links they have shared.
The RBM Partnership to End Malaria has developed a communication kit to help plan for the upcoming World Malaria Day on April 25th. Below are some of the highlights and links they have shared.
To mark World Malaria Day 2025, the RBM Partnership to End Malaria in collaboration with World Health Organization (WHO) have developed a Messaging Framework and Social Media Toolkit to support partners and individuals in raising awareness and advocating for a malaria-free world.
Objectives for this year include…
- Re-energize efforts at all levels, from global policy to community action, to accelerate progress towards malaria elimination
- Advocate for increased investment in malaria control and elimination programs, including through stepped-up domestic financing and successful replenishments for the Global Fund and Gavi in 2025.
- Promote innovative strategies and approaches to tackle evolving challenges in malaria
- Prioritize country ownership, actively engage communities, and implement data-driven strategies
 The emphasis is on three pillars. First in REINVEST, which recognized that “Malaria control and elimination programs don’t just save lives – they’re also a smart economic investment for malaria-endemic countries and their international partners.”
The emphasis is on three pillars. First in REINVEST, which recognized that “Malaria control and elimination programs don’t just save lives – they’re also a smart economic investment for malaria-endemic countries and their international partners.”
The second pillar calls on us to REIMAGINE. We must Accelerate innovation by investing in the research and development of new and more effective antimalarial drugs, diagnostics, insecticides, vaccines and vector control methods” and turning that research into action.
 The third pillar is a call to REIGNITE based on “a renewed sense of urgency and commitment is needed to accelerate the fight against malaria.” This is called the “Big Push against malaria (and) is a multistakeholder effort to drive progress.”
The third pillar is a call to REIGNITE based on “a renewed sense of urgency and commitment is needed to accelerate the fight against malaria.” This is called the “Big Push against malaria (and) is a multistakeholder effort to drive progress.”
Follow the links to learn more and plan action.
Advocacy &Vaccine Bill Brieger | 25 Apr 2022
World Immunization Week Starts with World Malaria Day
 One might think initially that the convergence of World Malaria Day and World Immunization Week would simply be a coincidence. This year there is a major connection since WHO has approved the first ever RTS,S/AS01 malaria vaccine which has undergone decades to clinical testing and most recently, a successful 3-year pilot intervention in Malawi, Kenya, and Ghana.
One might think initially that the convergence of World Malaria Day and World Immunization Week would simply be a coincidence. This year there is a major connection since WHO has approved the first ever RTS,S/AS01 malaria vaccine which has undergone decades to clinical testing and most recently, a successful 3-year pilot intervention in Malawi, Kenya, and Ghana.
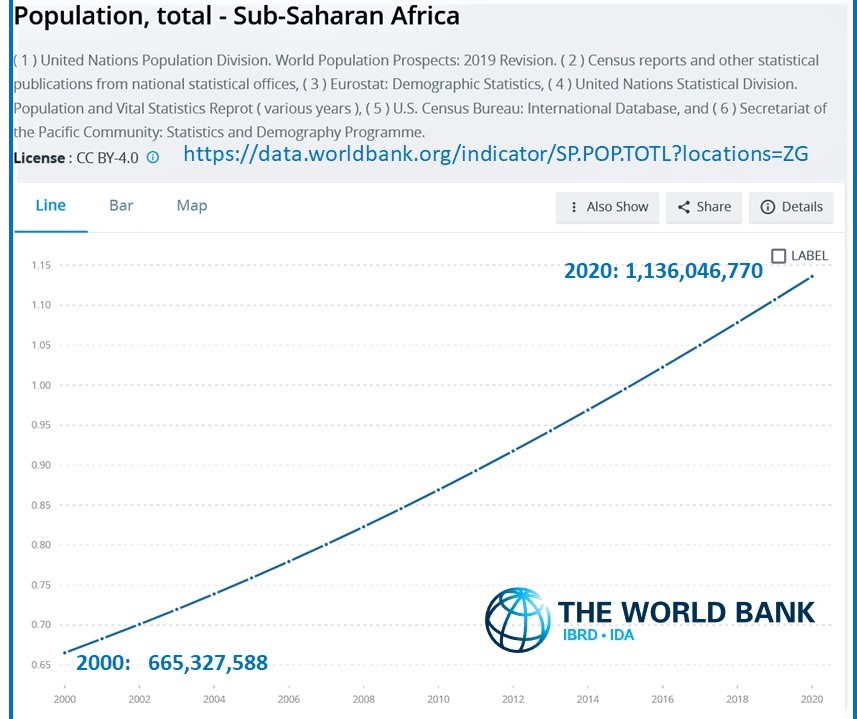 During her keynote address at the Johns Hopkins Malaria Institute’s World Malaria Day Webinar today, The WHO Regional Director for the African Region, Dr. Matshidiso Moeti, stressed the importance of integrated disease control efforts drawing on the region’s efforts to tackle neglected tropical diseases, COVID-19 and of course, malaria. She highlighted the importance of surveillance, and in That context pointed out a serious fact. The population of sub-Saharan Africa had doubled since the start of the Roll Back Malaria initiative, meaning that to achieve the same level of coverage of key interventions, one needs to reach many more people, whether for malaria control or child immunization.
During her keynote address at the Johns Hopkins Malaria Institute’s World Malaria Day Webinar today, The WHO Regional Director for the African Region, Dr. Matshidiso Moeti, stressed the importance of integrated disease control efforts drawing on the region’s efforts to tackle neglected tropical diseases, COVID-19 and of course, malaria. She highlighted the importance of surveillance, and in That context pointed out a serious fact. The population of sub-Saharan Africa had doubled since the start of the Roll Back Malaria initiative, meaning that to achieve the same level of coverage of key interventions, one needs to reach many more people, whether for malaria control or child immunization.
Thus, increasing targets and goals affect both immunization and malaria programs, as well as efforts to roll out the malaria vaccine. At present there is only one producer of the vaccine, GlaxoSmithKline, and while that company is working with another company in India to produce RTS,S in the global south, GSK is maintaining control of the AS01 adjuvant. Production targets have so far been geared to meeting the needs in the pilot districts of the three intervention countries, and for the foreseeable future this will address less than 10% of need in P. falciparum endemic areas, especially in Africa.
 WHO and partners including UNICEF and GAVI are in the process of figuring out equitable ways to distribute what is available now and encouraging the ramp up of vaccine production. The need to vaccine technology transfer to Africa is also being considered. Additionally, eyes are focused on new malaria vaccine candidates which might come on board in about five years.
WHO and partners including UNICEF and GAVI are in the process of figuring out equitable ways to distribute what is available now and encouraging the ramp up of vaccine production. The need to vaccine technology transfer to Africa is also being considered. Additionally, eyes are focused on new malaria vaccine candidates which might come on board in about five years.
The current malaria vaccine, while reducing severe disease, does not have the highest efficacy, and experts caution that is is therefore, not a silver bullet. They do explain that the vaccine is an important addition to the malaria toolkit, and should be a central part of integrated malaria control planning. At present though, we are not only running in place to meet the needs of an ever increasing number of children at risk, and we also must cope in an ethical and efficient way with limited supplies of the vaccine for the near future. This is the double challenge to start Malaria Day and Vaccine Week.
Advocacy &COVID-19 &Insecticide &Mosquitoes &poverty &Resistance &Severe Malaria Bill Brieger | 22 Oct 2020
Malaria News Today 2020-10-22
![]() The search for adjunctive therapy to aid in recovery from cerebral malaria is explored in Malaria Journal. A faster acting crystalline form of an insecticide is studied. In Nigeria the National Malaria Elimination Program advocates for equal footing with COVID-19 action. Links to full stories and abstracts are found below.
The search for adjunctive therapy to aid in recovery from cerebral malaria is explored in Malaria Journal. A faster acting crystalline form of an insecticide is studied. In Nigeria the National Malaria Elimination Program advocates for equal footing with COVID-19 action. Links to full stories and abstracts are found below.
Dimethyl fumarate reduces TNF and Plasmodium falciparum induced brain endothelium activation in vitro
Neida K. Mita-Mendoza, and colleagues studied Cerebral malaria (CM) which is associated with morbidity and mortality despite the use of potent anti-malarial agents. Brain endothelial cell activation and dysfunction from oxidative and inflammatory host responses and products released by Plasmodium falciparum-infected erythrocytes (IE), are likely the major contributors to the encephalopathy, seizures, and brain swelling that are associated with CM. The development of adjunctive therapy to reduce the pathological consequences of host response pathways could improve outcomes.
To accurately reflect clinically relevant parasite biology a unique panel of parasite isolates derived from patients with stringently defined CM was developed. The effect of TNF and these parasite lines on primary human brain microvascular endothelial cell (HBMVEC) activation in an in vitro co-culture model was tested. HBMVEC activation was measured by cellular release of IL6 and nuclear translocation of NF?B. The transcriptional and functional effects of dimethyl fumarate (DMF), an FDA approved drug which induces the NRF2 pathway, on host and parasite induced HBMVEC activation was characterized. In addition, the effect of DMF on parasite binding to TNF stimulated HBMVEC in a semi-static binding assay was examined.
The findings provide evidence that targeting the nuclear factor E2-related factor 2 ( NRF2) pathway in tumour necrosis factor (TNF) and parasite activated human brain microvascular endothelial cell (HBMVEC) mediates multiple protective pathways and may represent a novel adjunctive therapy to improve infection outcomes in CM.
Fast-acting insecticide polymorph could boost malaria-control efforts
Chemistry World reports on a faster-acting version of a common insecticide could boost malaria control efforts. The new crystalline form of deltamethrin is absorbed by mosquitoes 12 times faster than commercial forms and could help to limit malaria transmission despite growing rates of insecticide resistance.
Microcystals of contact insecticides like deltamethrin are crucial ingredients in indoor sprays and treated bed nets used to combat malaria-spreading mosquitoes. But many mosquito populations are developing resistance to these compounds, which is harming efforts to control the disease.
Treat Malaria as National Health Emergency, NEMP tells Federal Government
The Coordinator of National Malaria Elimination Programme (NEMP), has asked the federal government to tackle malaria as a national health emergency in the same manner COVID-19 pandemic is being handled. Against the background of increasing poverty in the country, Civil Society in Malaria Control, Immunisation and Nutrition (ACOMIN) has said there is a direct linkage between malaria scourge and the level of poverty in communities.
Speaking at a meeting with the civil society group involved in anti malaria advocacy, Coordinator of NEMP, said the current level of funding of the health sector by government is unacceptably low.
Advocacy &coronavirus &Fever &HIV &IPTp &Journalists/Media &Malaria in Pregnancy &Plasmodium/Parasite &Private Sector &Tuberculosis Bill Brieger | 06 Oct 2020
Malaria News Today 2020-10-06: malaria in pregnancy, parasites surviving fever and private sector support
Today’s news featured a media briefing by the RBM Partnership and AMMREN on the challenges of protecting pregnant women from malaria. Additional news expands on these challenges. Research looks at how malaria parasites withstand the heat of a patient’s fever. Finally examples are presented of collaboration between international organizations and the private sector for malaria and disease control. Follow the links to gain more information.
Speed Up IPTp Scale-Up: a media briefing on maternal health
 A panel discussion and media briefing on new approaches and lessons learned formed part of an online global call to end malaria in pregnancy with intermittent preventive treatment. The briefing on Tuesday, 6 October 2020, was sponsored by the Roll Back Malaria Partnership and AMMREN. The RBM website features background on the call to action.
A panel discussion and media briefing on new approaches and lessons learned formed part of an online global call to end malaria in pregnancy with intermittent preventive treatment. The briefing on Tuesday, 6 October 2020, was sponsored by the Roll Back Malaria Partnership and AMMREN. The RBM website features background on the call to action.
The panel discussion included Dr. Aminata Cisse ep. Traore, Sous Directrice de la Santé de la Reproduction/Direction Générale de la Santé et de l’Hygiène Publique, Ministére de la Santé et de l’Hygiène Publique, Mali; Dr. Anshu Banerjee, Director Department of Maternal, Newborn, Child, Adolescent Health & Ageing, World Health Organization (WHO), and Dr. Pedro Alonso, Director Global Malaria Programme, WHO. The discussion was moderated by Mildred Komey, Malaria in Pregnancy Focal Person, National Malaria Control Program, Ghans Health Service.
 The discussion covered the importance of launching this call now, what we’ve learned over the last few years, and examples of innovative strategies from Mali. There was a Q&A session with journalists after the presentations.
The discussion covered the importance of launching this call now, what we’ve learned over the last few years, and examples of innovative strategies from Mali. There was a Q&A session with journalists after the presentations.
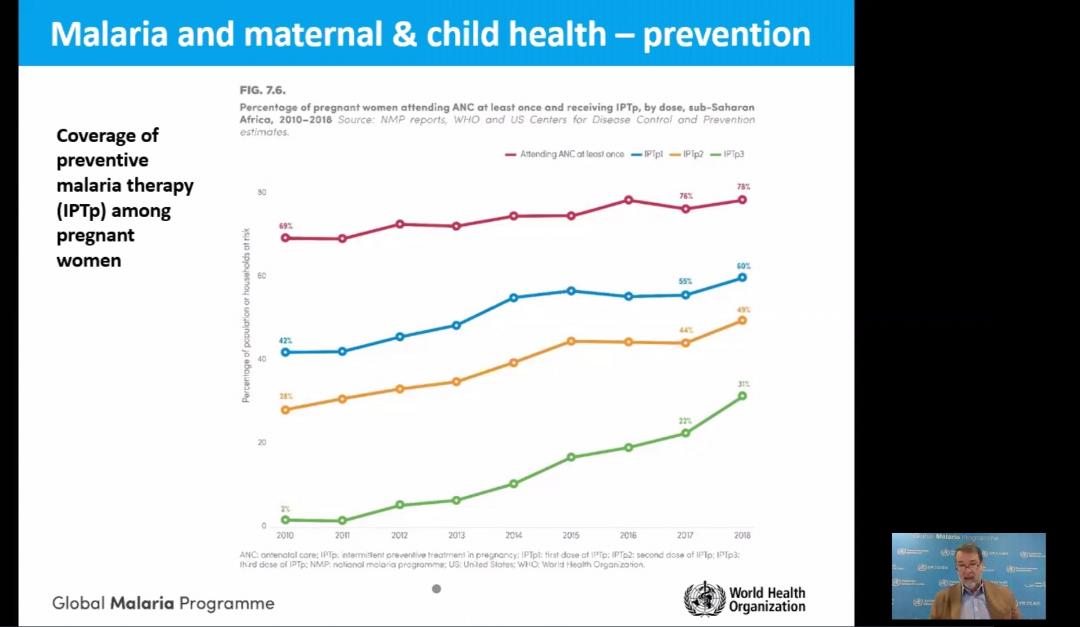
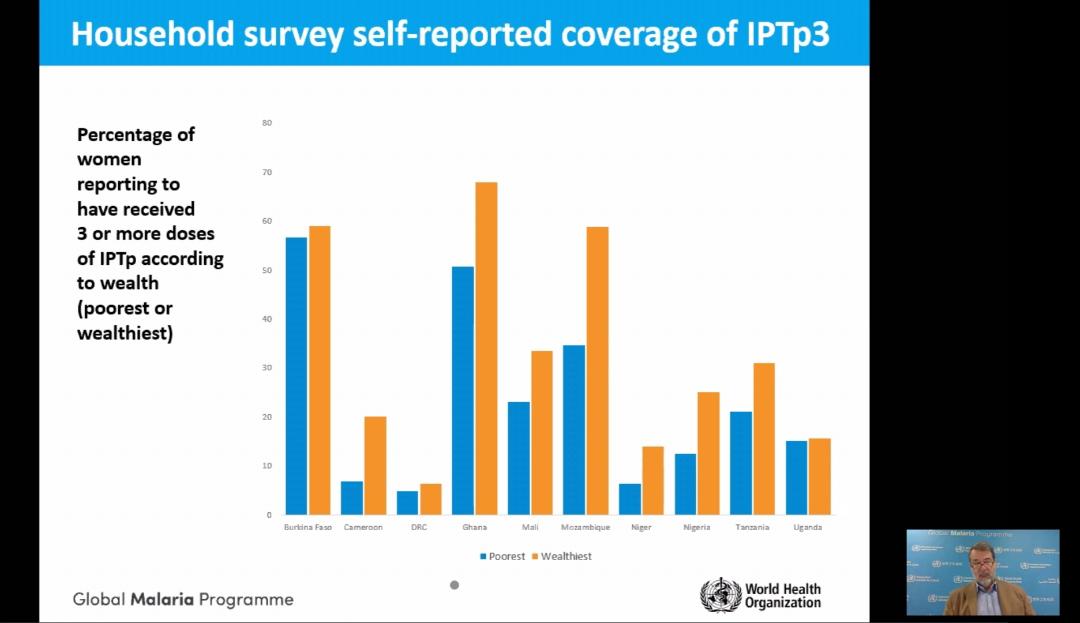
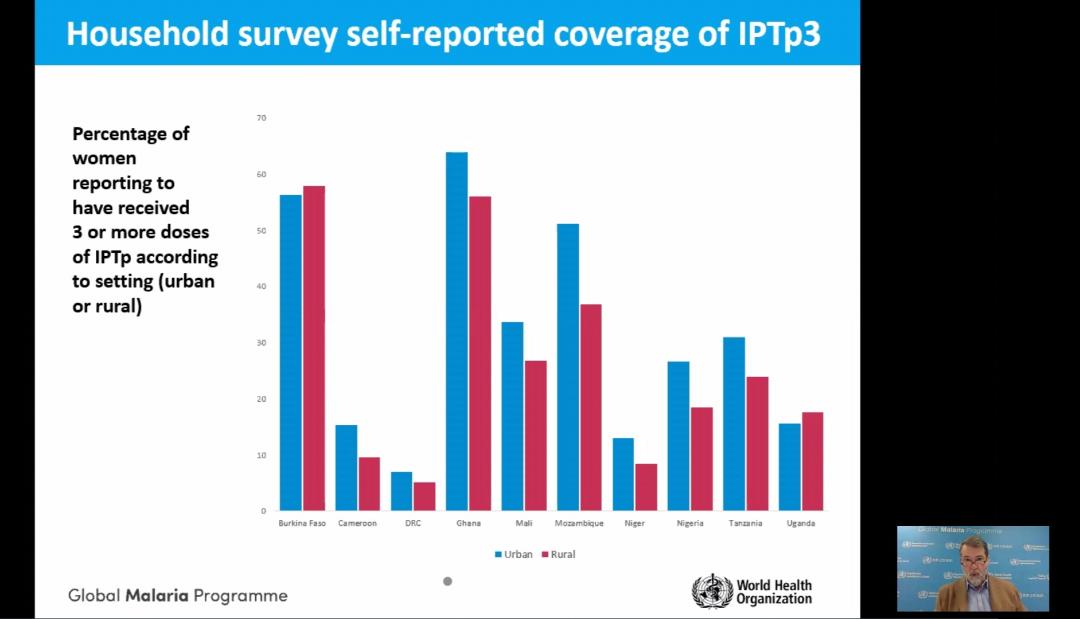
The presentation by Dr Alonso showed the progress in achieving IPTp coverage goals. He also pointed out the social and economic factors that affect access and equity to intermittent preventive treatment of malaria in pregnancy and protection of maternal health (see slides).
Experts say Africa must scale-up malaria protection for pregnant women
 In support of the RBM/AMMREN briefing described above, Sola Ogundipe reports that amidst the COVID-19 pandemic in sub-Saharan Africa, malaria – one of the world’s oldest diseases – is impacting disproportionately on pregnant women and children aged under five.
In support of the RBM/AMMREN briefing described above, Sola Ogundipe reports that amidst the COVID-19 pandemic in sub-Saharan Africa, malaria – one of the world’s oldest diseases – is impacting disproportionately on pregnant women and children aged under five.
For a pregnant woman, her fetus, and the newborn child malaria infection carries substantial risks. Calling for a speedy scale-up to boost protection against malaria for pregnant women in Africa, the Roll Back Malaria, RBM Partnership to End Malaria Working Group is issuing an urgent appeal to leaders and health policymakers to increase access to Intermittent Preventive Treatment during pregnancy, IPTp, among eligible pregnant women in sub-Saharan Africa.
 Along with stakeholders, the RBM Partnership is pushing for scale-up coverage of three doses of IPTp to reach all eligible women in sub-Saharan Africa by 2025. In 2019, according to the RBM Partnership, an estimated 11 million pregnant women in sub-Saharan Africa, or 29 percent of all pregnancies were infected with malaria.
Along with stakeholders, the RBM Partnership is pushing for scale-up coverage of three doses of IPTp to reach all eligible women in sub-Saharan Africa by 2025. In 2019, according to the RBM Partnership, an estimated 11 million pregnant women in sub-Saharan Africa, or 29 percent of all pregnancies were infected with malaria.
How malaria parasites withstand a fever’s heat
The parasites that cause 200 million cases of malaria each year can withstand feverish temperatures that make their human hosts miserable. Now, a team is beginning to understand how they do it. The researchers have identified a lipid-protein combo that springs into action to gird the parasite’s innards against heat shock.
Understanding how malaria protects its cells against heat and other onslaughts could lead to new ways to fight tough-to-kill strains, researchers say. Findings could lead to ways to maximize our existing antimalarial arsenal.
Global Fund and Chevron – United Against HIV, TB and Malaria
The Global Fund and Chevron Corporation have celebrated a 12-year partnership that served as an example of the private sector’s contribution to the fight against infectious diseases and to building resilient health systems. Chevron, a Global Fund partner since January 2008, has supported Global Fund programs against HIX4 tuberculosis and malaria for a total investment of US$60 million in Angola, Indonesia, Nigeria, the Philippines, South Africa, Thailand and Vietnam.
Chevron’s partnership has contributed to helping more than a million people living with HIV access lifesaving antiretroviral therapy; supported efforts to distribute over one million long-lasting insecticide-treated mosquito nets to families to prevent malaria; helped detect thousands of TB cases; promoted education programs for the young, and helped build stronger health systems.
In Nigeria, Chevron’s $5 million investment from October 2017 to December 201 9 supported the national HIV and TB programs, reaching key and vulnerable populations, as well as interventions aimed at strengthening the health system. Sustainable and resilient systems for health are indispensable in the fight against the epidemics of HIV TB and malaria, as well as the first line of defense against new diseases like COVID-19. “With rising cases of COVID-1 9, the stakes are very high. Deaths from HIV, TB and malaria are likely to increase. Investments by partners like Chevron are fundamental.
Advocacy &Case Management &Children &Education &Seasonal Malaria Chemoprevention Bill Brieger | 02 Feb 2019
A child’s personal experiences with malaria lead to a life career fighting the disease
Gbenga Jokodola tells his story of growing up to fight malaria in Nigeria. Gbenga has a MPH in Field Epidemiology from the University of Ibadan, and a BPharm from Ahmadu Bello University. He is currently working with Malaria Consortium as a Zonal Project Manager on the Seasonal Malaria Chemoprevention (SMC) Project, delivering preventive care to over 400,000 children between the ages of 3 – 59 months in Jigawa and Katsina States of Nigeria. He has worked on several malaria projects over the years sponsored by Unicef, the Global Fund, Catholic Relief Services and the Bill & Melinda Gates Foundation. As he narrates below, his early experiences with malaria were formative of his present focus in life.

At 3 months of age Gbenga was probably still protected from malaria by maternal antibodies and did not realize what malaria held in store for his future
Growing up in Zaria, northern Nigeria in the 70s and 80s was one of the best experience any child could ask for. I lived with my parents in two rented rooms in a compound on one of the streets in Sabon Gari Zaria – a community that had virtually all the tribes in Nigeria and of course, with all the love and communal living you can ever get from a true Nigerian community.
In such loving setting we enjoyed as children, I imagined that mosquito communities also lived around our pit latrine and backyard. I imagined that parent-mosquitoes trained their off-springs very well on how to bite and fly away tactfully, how to dodge the usual clap-like manner we use in killing mosquitoes, which homes to avoid visiting, and so on.
I was reputed to be a strong boy then, one of the few kids who were “strong”; I was a “tough” boy who rarely fell ill to malaria. Then, it was common to hear, “Gbenga is a strong boy”. I ate and slept in any room in our compound – with or without covering from mosquito and was hailed for doing so by my friends who often fall ill to malaria.
Life lesson as a Primary School pupil: There is no immunity against malaria
One day, the “malaria forces” (mosquitoes) taught me a life lesson: Indeed, there is no immunity against malaria.
My local Government primary school rotated school attendance between morning and afternoon every week. As an 8-year-old, while preparing for my afternoon school I suddenly felt very cold and sleepy at the same time and decided to lie down briefly on my senior brother’s 6-spring bed in our sitting room. Shortly after, I was shivering and sweating profusely under 3 of my mother’s wrappers.
Help was not immediately near as most people were out. My head was pounding like I was a piece of yam being pounded with a pestle in my mother’s mortar. My stomach was churning. All the while, I kept saying “I am a strong boy, I will not be sick”! I was in that state for over an hour. I began to wonder if I was strong after all and will not end up dying. I could no longer talk but my teeth were chattering.

Gbenga second from left at about 7 years old in company of Sisters and friends in the compound
Sweating profusely, yet I was cold! I was helpless. It was in this state that one of our neighbor’s daughters walked into our sitting room, wondering if there was any food to eat. Immediately she saw the “strong man” shivering under 3 wrappers, she raised an alarm. Her shout saved me as neighbors immediately rushed into our sitting room. Among them was a relation of the landlord, a beautiful “Aunty” Esther, who was visiting from the Ahmadu Bello University school of Nursing. As soon as she came over, she said: “this is malaria!”.
Aunty Esther immediately organized and rescued me that day; she saved the life of the “strong man”! She quickly sought iced-cold water and toweled my body with my father’s “untouchable” towel hanging on the door of the inner room. Ah, what a good feel it was! She then gave me a sweet syrup which I later found out to be Paracetamol syrup. After about 30 minutes, she returned with a plate of hot rice and stew, encouraging me to eat before treatment with anti-malarial medication. I struggled to eat the rice, angry that I had lost my ever-available appetite! I only took few spoons, amidst the encouragement I received from all present.
I was then given an injection by Aunty Nurse Esther, tucked back into the bed and told to prepare to sleep. She then said, “Gbenga, no school for you today, okay? You even need to get well before you resume school”. Everyone knew I loved school. I had to lose a precious school day (and three more days) to malaria! So, I simply focused on staying alive, wondering which “wicked” mosquito bit me. That was the day I dramatically lost my title of “strong man” to malaria, painfully realizing that I was not immune to malaria at all!
My treatment against malaria was continued with further jabs of the needle (twice a day) over the course of the next 3 days at the Dispensary/Primary Health Unit “Aunty” Esther directed my parents to. I got well and resumed school after the third day. Later, I researched and found out I was treated with a sedative, Chloroquine and Paracetamol.
Gbenga with classmates at First Baptist Church, Benin Street, Sabon Gari Zaria
My parents later introduced “Sunday-Sunday Medicine” (one Sweetened pyrimethamine tablet weekly) against Malaria to our diet on Sundays. With this painful encounter with Malaria, I resolved to fight mosquitoes; I was determined to regain my “strong man” title. I made up my mind to be a community health worker, saving communities from diseases like malaria.
Fast-forward to Year 2007: My new twist in combating Malaria
By the year 2007, my personal malaria episodes had lessened with greater knowledge of the disease. In addition, the application of the preventive, diagnostic and treatment procedures reduced my malaria episodes to about 1 in 3 years. With each episode, I normally use laboratory test (microscopy) to confirm if severity is +, ++, or even +++. Thereafter, I get a prescription from a Physician on appropriate medication to use.
However, while practicing in Abuja, I encountered a tearful case of death from malaria, of an 8-year old beautiful daughter of a colleague. Three days prior to her death, a Community Pharmacist had dispensed anti-malarial medication to her, based on prescription tendered by the father from a Government hospital he had earlier taken her to. The news of her death brought back memories of how I would have died as

ACCESS-SMC Project: Scaling up access to seasonal malaria chemoprevention in the Sahel
an 8-year old from this same Malaria. Yes, this same Malaria! That death of the 8-year old triggered a fresh resolve in me to step up my fight with mosquitoes and combat malaria squarely at community, state, National and global levels.
Still at War with Malaria in 2018
Now armed with post-graduate training in Public Health/Epidemiology and field-based experience, my Malaria diagnosis strategy has now changed. I now use Rapid Diagnostic Test Kits (RDT). If confirmed positive, I receive prescription on the most applicable Artemisinin-based combination Therapy (ACT) to use.
My malaria story continues and will only end when mosquitoes are defeated – when children and adults no longer fall ill nor die from mosquito bites that cause malaria.
You can follow Gbenga on Twitter.
Advocacy &Community &Leadership &Surveillance &Women Bill Brieger | 05 Jul 2018
Global Civil Society for Malaria Elimination (CS4ME)
 CS4ME was created during the Global Malaria Civil Society Strategising and Advocacy Pre-Meeting jointly convened by the Global Fund Advocates Network Asia-Pacific (GFAN AP) and APCASO held on 29th and 30th June 2018, prior to the First Malaria Wor1d Congress in Melbourne, Australia, with the support of the Malaria World
CS4ME was created during the Global Malaria Civil Society Strategising and Advocacy Pre-Meeting jointly convened by the Global Fund Advocates Network Asia-Pacific (GFAN AP) and APCASO held on 29th and 30th June 2018, prior to the First Malaria Wor1d Congress in Melbourne, Australia, with the support of the Malaria World  Congress, Global Fund to Fight AIDS, Tuberculosis and Malaria, and the Burnet Institute. An interim working group mode up of individuals that attended the Pre-Meeting was established to coordinate, recommend processes and mechanisms, identify resources and support necessary for CS4ME going forward. For more Information please contact Ms Olivia Ngou Zongue <ngouolivia@gmail.com> of the Interim Working Group of CS4ME for further information. The Declaration arising from their meeting if provided below.
Congress, Global Fund to Fight AIDS, Tuberculosis and Malaria, and the Burnet Institute. An interim working group mode up of individuals that attended the Pre-Meeting was established to coordinate, recommend processes and mechanisms, identify resources and support necessary for CS4ME going forward. For more Information please contact Ms Olivia Ngou Zongue <ngouolivia@gmail.com> of the Interim Working Group of CS4ME for further information. The Declaration arising from their meeting if provided below.
GLOBAL CIVIL SOCIETY FOR MALARIA ELIMINATION (CS4ME) DECLARATION
MALARIA WORLD CONGRESS 1ST-5TH JULY 2018
MELBOURNE, AUSTRALIA
Firm in the belief that empowered community and civil society are game-changers in health responses, we, representatives of national, regional and global malaria communities and civil society attending the First Malaria World Congress, have come together and formed the Global Civil Society for Malaria Elimination (CS4ME) as part of our commitment to joint advocacy for more effective, sustainable, people-centred, rights-based, equitable, and inclusive malaria programmes and Interventions.
At a time when the world has the resources and tools to prevent and treat malaria, it is unconscionable how people – mainly from impoverished, vulnerable and underserved communities – continue to die from the disease. While we commend the efforts of governments and the international community that brought the world closer to malaria elimination, we call for greater accountability, political will and action, resource investments, and sense of urgency to eliminate the disease.
CS4ME makes the following call to the governments of implementing countries, donor countries and other duty bearers:
FRAME MALARIA RESPONSES IN THE CONTEXT Of SOCIAL JUSTICE AND HUMAN RIGHTS, AND WITHIN UNIVERSAL HEALTH COVERAGE
Significant progress has been attained during the past 10 years to reduce the burden of malaria throughout the world and in working towards achieving malaria elimination. As countries enter into the elimination phase, we see again and again the epidemic concentrating among the most marginalised, remote, and disenfranchised communities. In South East Asia, the concentration of malaria among communities barred from accessing quality and affordable health services has accelerated the emergence of drug resistance that now threatens the wor1d at large. Everywhere, the last mile of elimination becomes a matter of access to health for impoverished and marginalised communities, in particular, refugees, ethnic minorities, indigenous communities, migrant and mobile populations – with many of the risks faced by these groups compounded further amongst women and girls.
Including the most local, represents a strategic investment contributing to appropriate, effective service delivery and people-driven surveillance and response.
We call on national governments, international institutions, bilateral and multilateral donors to prioritise and increase funding allocations for community-driven community and civil society initiatives. We request that specific funding streams be made available to community groups, and their access supported through peer-to-peer technical assistance.
Furthermore, we request that key performance indicators that enable accountability for bringing malaria services to the underserved be developed and implemented.
PARTNER WITH CIVIL SOCIETY AND COMMUNITY ACTORS FOR AN EFFECTIVE MALARIA SURVEILLANCE AND RESPONSE
As surveillance becomes an essential pillar for malaria elimination, the need for timely and robust data is increasingly critical. Essential evidence includes routine data, qualitative and quantitative research, as well as experience, lessons learned and the voices from affected communities. Support is required to build the ability of civil society to generate evidence, as well as to communicate it effectively to ensure that community-generated evidence will be able to influence decisions and result in sustained change.
To eliminate malaria, surveillance requires a response. Communities and civil society are the first responders, and will have the clearest insight Into what responses are effective in their context or on behalf of their constituents.
We demand that communities and civil society organisations be given equitable access to data and other information that can inform field-level response. We call for transparent information systems and multi-directional information flows in order to enable dialogue, and inform decisions at all levels. We urge the building up of surveillance systems that involve communities as analysts, advisors, decision-makers and responders.
We, malaria communities and civil society, offer our support, expertise, and lived experiences In contributing towards our shared vision of malaria elimination. We are fully committed to working alongside other stakeholders to build stronger, more inclusive and effective partnerships and sustainable responses towards elimination of malaria in this lifetime.
Advocacy &Case Management &Community &IPTp &ITNs Bill Brieger | 30 Apr 2018
Burkina Faso Celebrated World Malaria Day with Pledges to Defeat Malaria
 Burkina Faso celebrated World Malaria Day with pledges to Defeat Malaria on 25th April 2018. Dr Ousman Badolo. Technical Director of Jhpiego’s USAID/PMI Supported Improving Malaria Care (IMC) Project describes below the event in the village of Kamboinsin, not far from the capital, Ouagadougou. Ibrahim Sawadogo from IMC provided the photographs.
Burkina Faso celebrated World Malaria Day with pledges to Defeat Malaria on 25th April 2018. Dr Ousman Badolo. Technical Director of Jhpiego’s USAID/PMI Supported Improving Malaria Care (IMC) Project describes below the event in the village of Kamboinsin, not far from the capital, Ouagadougou. Ibrahim Sawadogo from IMC provided the photographs.
The day started with a proclamation of malaria day from Burkina Faso’s President, Roch Marc Christian Kaboré, to his assembled cabinet and the press. The president recognized that malaria is still a major public health issue in the country, and while deaths are decreasing, the incidence of malaria is not. The President called for a greater commitment of resources by all partners to insure that malaria can be defeated in Burkina Faso by 2030.
 Kamboinsin village in Sig-Noghin Health District was the site of further observances organized by the National Malaria Control Program, later that afternoon. This district was chosen because of having among the highest incidence rates for malaria in the region. Many partners set up booths to share their work in malaria with partners and citizens of the district. Included were three research centers (Centre Muraz, CNRFP and IRD), and three USAID programs supported by the President’s Malaria Initiative in Burkina Faso (Procurement and Supply Management [PSM], IMC and VectorLink), among others.
Kamboinsin village in Sig-Noghin Health District was the site of further observances organized by the National Malaria Control Program, later that afternoon. This district was chosen because of having among the highest incidence rates for malaria in the region. Many partners set up booths to share their work in malaria with partners and citizens of the district. Included were three research centers (Centre Muraz, CNRFP and IRD), and three USAID programs supported by the President’s Malaria Initiative in Burkina Faso (Procurement and Supply Management [PSM], IMC and VectorLink), among others.
 During the program both the Minister for Health and the US Ambassador spoke. The Minister highlighted the main strategies that Burkina Faso is employing to reduce and eliminate malaria including regular use of insecticide treated nets (ITN), seasonal malaria chemoprevention, Intermittent Preventive Treatment in Pregnancy (IPTp), Prompt and Appropriate Case Management and other Vector Control Strategies.
During the program both the Minister for Health and the US Ambassador spoke. The Minister highlighted the main strategies that Burkina Faso is employing to reduce and eliminate malaria including regular use of insecticide treated nets (ITN), seasonal malaria chemoprevention, Intermittent Preventive Treatment in Pregnancy (IPTp), Prompt and Appropriate Case Management and other Vector Control Strategies.
The US Ambassador shared a real-life story of a pregnant woman who during her current pregnancy decided to register early for Antenatal Care (ANC) as encouraged by the IMC project. She was able to get several doses of IPTp as required as well as obtain an ITN on her first visit, unlike in her previous pregnancies.
 Entertainment was provided by the comedian Hypolythe Wangrawa (alias M’ba Bouanga) who presented a sketch involving his ‘son’ who was not encouraging his wife to attend ANC and receive malaria prevention services. M’ba Bouanga chastised the son and an actor playing a midwife explained to the family the value of attending ANC and preventing malaria. Singers Maria Bissongo, Miss Oueora and Aicha Junior provided the audience with a song that embodied a variety of malaria prevention and care messages.
Entertainment was provided by the comedian Hypolythe Wangrawa (alias M’ba Bouanga) who presented a sketch involving his ‘son’ who was not encouraging his wife to attend ANC and receive malaria prevention services. M’ba Bouanga chastised the son and an actor playing a midwife explained to the family the value of attending ANC and preventing malaria. Singers Maria Bissongo, Miss Oueora and Aicha Junior provided the audience with a song that embodied a variety of malaria prevention and care messages.
 A highlight of the occasion was recognition of high performing health districts in the country. They were judged on criteria including good management of malaria commodity stocks, reduced case fatality rates, use of diagnostic tests to confirm malaria before treatment and coverage of at least three doses of IPTp. Four districts were given awards, Titao, Thyou, Boussouma and Batie, while Charles de Gaul Pediatric Hospital was also recognized.
A highlight of the occasion was recognition of high performing health districts in the country. They were judged on criteria including good management of malaria commodity stocks, reduced case fatality rates, use of diagnostic tests to confirm malaria before treatment and coverage of at least three doses of IPTp. Four districts were given awards, Titao, Thyou, Boussouma and Batie, while Charles de Gaul Pediatric Hospital was also recognized.
One can watch a video of the proclamation by the President on the National Facebook page. More details of the events are found in the following media: Lefaso.net and Paalga Observer.
World Malaria Day in Burkina Faso demonstrated the political will and commitment to “defeat malaria.” More and more national resources will be needed to reach the endline in 2030.
Advocacy &Case Management &Children &CHW &Community &Elimination &Funding &iCCM &Invest in Malaria Control &IPTp &ITNs Bill Brieger | 25 Apr 2018
On World Malaria Day the realities of resurgence should energize the call to ‘Beat Malaria’
 Dr Pedro Alonso who directed the World Health Organization’s Global Malaria Program, has had several opportunities in the past two weeks to remind the global community that complacency on malaria control and elimination must not take hold as there are still over 400,000 deaths globally from malaria each year. At the Seventh Multilateral Initiative for Malaria Conference (MIM) in Dakar, Dr Alonso drew attention to the challenges revealed in the most recent World Malaria Report (WMR). While there have been decreases in deaths, there are places where the number of actual cases is increasing.
Dr Pedro Alonso who directed the World Health Organization’s Global Malaria Program, has had several opportunities in the past two weeks to remind the global community that complacency on malaria control and elimination must not take hold as there are still over 400,000 deaths globally from malaria each year. At the Seventh Multilateral Initiative for Malaria Conference (MIM) in Dakar, Dr Alonso drew attention to the challenges revealed in the most recent World Malaria Report (WMR). While there have been decreases in deaths, there are places where the number of actual cases is increasing.
 Around twenty years ago the course of malaria changed with the holding of the first MIM, also in Dakar and the establishment of the Roll Bank Malaria (RBM) Partnership. These were followed in short order by the Abuja Declaration that set targets for 2010 and embodied political in endemic countries, as well as major funding mechanisms such as the Global Fund to fight AIDS, TB and Malaria. This spurred what has been termed a ‘Golden Decade’ of increasing investment and intervention coverage, leading to decreasing malaria morbidity and mortality. The Millennium Development Goals provided additional impetus to reduce the toll of malaria by 2015.
Around twenty years ago the course of malaria changed with the holding of the first MIM, also in Dakar and the establishment of the Roll Bank Malaria (RBM) Partnership. These were followed in short order by the Abuja Declaration that set targets for 2010 and embodied political in endemic countries, as well as major funding mechanisms such as the Global Fund to fight AIDS, TB and Malaria. This spurred what has been termed a ‘Golden Decade’ of increasing investment and intervention coverage, leading to decreasing malaria morbidity and mortality. The Millennium Development Goals provided additional impetus to reduce the toll of malaria by 2015.
 On Facebook Live yesterday Dr Alonso talked about that ‘Golden Decade.’ There was a 60% decrease in mortality and a 40% decreases in malaria cases. But progress slowing down and we may be stalled at a crossroads. He noted that history show unless accelerate efforts, malaria will come back with a vengeance. Not only is renewed political leadership and funding, particularly from affected countries needed, but we also need new tools. Dr Alonso explained that the existing tools allowed 7m deaths be diverted in that golden decade, but these tools are not perfect. We are reaching limits on these tools such that we need R&D for tools to enable quantum leap forward. Even old tools like nets are threatened by insecticide resistance, and research on alternative safe insecticides is crucial.
On Facebook Live yesterday Dr Alonso talked about that ‘Golden Decade.’ There was a 60% decrease in mortality and a 40% decreases in malaria cases. But progress slowing down and we may be stalled at a crossroads. He noted that history show unless accelerate efforts, malaria will come back with a vengeance. Not only is renewed political leadership and funding, particularly from affected countries needed, but we also need new tools. Dr Alonso explained that the existing tools allowed 7m deaths be diverted in that golden decade, but these tools are not perfect. We are reaching limits on these tools such that we need R&D for tools to enable quantum leap forward. Even old tools like nets are threatened by insecticide resistance, and research on alternative safe insecticides is crucial.
 Dr Alonso at MIM pointed to the worrying fact that investment in malaria overall peaked in 2013. Investment by endemic countries themselves has remained stable throughout and never gone reached $1 billion despite advocacy and leadership groups like the Africa Leaders Malaria Alliance. The 2017 WMR shows that while 16 countries achieved a greater that 20% reduction in malaria cases, 25 saw a greater that 20% increase in cases. The outnumbering of decreasing countries by increasing was 4 to 8 in Africa, the region with the highest burden of the disease. Overall 24 African countries saw increases in cases between 2015 and 2016 versus 5 that saw a decrease. A review of the Demographic and Health and the Malaria Information Surveys in recent years show that most countries continue to have difficulty coming close to the Abuja 2010 targets for Insecticide treated net (ITN) use, prompt and appropriate malaria case management and intermittent preventive treatment of malaria in pregnancy (IPTp).
Dr Alonso at MIM pointed to the worrying fact that investment in malaria overall peaked in 2013. Investment by endemic countries themselves has remained stable throughout and never gone reached $1 billion despite advocacy and leadership groups like the Africa Leaders Malaria Alliance. The 2017 WMR shows that while 16 countries achieved a greater that 20% reduction in malaria cases, 25 saw a greater that 20% increase in cases. The outnumbering of decreasing countries by increasing was 4 to 8 in Africa, the region with the highest burden of the disease. Overall 24 African countries saw increases in cases between 2015 and 2016 versus 5 that saw a decrease. A review of the Demographic and Health and the Malaria Information Surveys in recent years show that most countries continue to have difficulty coming close to the Abuja 2010 targets for Insecticide treated net (ITN) use, prompt and appropriate malaria case management and intermittent preventive treatment of malaria in pregnancy (IPTp).
 The coverage gap is real. The WMR shows that while there have been small but steady increase in 3 doses of IPTp, coverage of the first dose has leveled off. Also while ownership of a net by households has increased, less than half of households have at least one net for every two residents.
The coverage gap is real. The WMR shows that while there have been small but steady increase in 3 doses of IPTp, coverage of the first dose has leveled off. Also while ownership of a net by households has increased, less than half of households have at least one net for every two residents.
In contrast a new form of IPT – seasonal malaria chemoprevention (SMC) for children in the Sahel countries has taken off with over 90% of children receiving at least one of the monthly doses during the high transmission season. Community case management is taking off as is increased use of rapid diagnostic testing. Increased access to care may explain how in spite of increased cases, deaths can be reduced. This situation could change rapidly if drug resistance spreads.
 While some international partners are stepping up, we are far short of the investment needed. The Gates Foundation is pledging more for research and development to address the need for new tools as mentioned by Dr Alonso. A big challenge is adequate funding to sustain the implementation of both existing tools and the new ones when they come online. Even in the context of a malaria elimination framework, WHO stresses the need to maintain appropriate levels of intervention with case management, ITNs and other measures regardless of the stage of elimination at which a country or sub-strata of a country is focused.
While some international partners are stepping up, we are far short of the investment needed. The Gates Foundation is pledging more for research and development to address the need for new tools as mentioned by Dr Alonso. A big challenge is adequate funding to sustain the implementation of both existing tools and the new ones when they come online. Even in the context of a malaria elimination framework, WHO stresses the need to maintain appropriate levels of intervention with case management, ITNs and other measures regardless of the stage of elimination at which a country or sub-strata of a country is focused.
Twenty years after the formation of RBM and 70 years after the foundation of WHO, the children, families and communities of endemic countries are certainly ready to beat malaria. The question is whether the national and global partners are equally ready.
Advocacy &Borders &Children &Conflict &Costs &Epidemiology &Funding &Human Resources &Leadership &Monitoring &Mortality &NTDs &Partnership &Surveillance Bill Brieger | 03 Feb 2018
African Leaders Malaria Alliance Recognizes Country Achievements, Adds NTDs to its Scorecard
 The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
The 30th African Union (AU) Heads of State Summit at its headquarters in Addis Ababa, Ethiopia provided an important opportunity to bring the challenges of infectious diseases on the continent to the forefront. Led by the African Leaders Malaria Alliance (ALMA), two major activities occurred, raising greater awareness and commitment to fighting neglected tropical diseases (NTDs) and recognizing the contributions countries have made in the fight against malaria.
 For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
For many years ALMA has maintained Scorecard for Accountability and Action by monitoring country progress on key malaria interventions. It later added key maternal and child health indicators. At the AU Summit ALMA announced that NTD indicators would be added to the scorecards which are reported by country and in summary.
The scorecard will now “report progress for the 47 NTD-affected countries in sub-Saharan Africa in their strategies to treat and prevent the five most common NTDs: lymphatic filariasis, onchocerciasis, schistosomiasis, soil-transmitted helminths and trachoma. By adding NTDs to the scorecard, African leaders are making a public commitment to hold themselves accountable for progress on these diseases.”
 In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
In the press release Joy Phumaphi, Executive Secretary ofALMA, explained that, “Malaria and NTDs both lay their heaviest burden on the poor, rural and marginalised. They also share solutions, from vector control to community-based treatment. Adding NTDs to our scorecard will help give leaders the information they need to end the cycle of poverty and reach everyone, everywhere with needed health care.” This will be an opportunity to demonstrate, for example, that, “In 2016, 40 million more people were reached with preventive treatment for at least one NTD than the year before.”
The combination is based on the logic that NTDs and malaria are both diseases of poverty. Malaria and several NTDs are also vector-borne. Also community platforms are a foundation for delivering needed drugs and supplies to tackle these diseases. Ultimately the decision shows that Heads of State are holding themselves accountable for progress in eliminating these diseases.
 At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
At a malaria-focused side meeting of the AU Summit Dr. Kebede Worku (Ethiopia’s State Minister of Health) shared that his government has been mobilizing large amount of resources to the fight against malaria which has led to the shrinking of morbidity and mortality since 2005. He also stressed that Africans should be committed to eliminate malaria by the year 2030. “Failing to do so is to repeat the great failure of 1960s faced at the global malaria fighting.”
 The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
The highlight for the malaria community at the Summit was the recognition of six countries that have made exemplary progress in the past year. The 6 countries that are leading the way to a Malaria-Free Africa by 2030 are Algeria, Comoros, Madagascar, the Gambia, Senegal, and Zimbabwe, recognized by ALMA for their sharp decline in malaria cases. Madagascar, the Gambia, Senegal and Zimbabwe Reduced malaria cases by more than 20 percent from 2015 to 2016. Algeria and Comoros are on track to achieve a more than 40 percent drop in cases by 2020.
H.E . Dr. Barnabas Sibusiso Dlamini, the Prime Minister of the Kingdom of Swaziland, whose King and Head of State is the current chair of ALMA, warned all endemic countries that, “When we take our eyes off malaria, the cost for our countries is huge. Yet if we increase our efforts to control and eventually eliminate malaria, the yield we get from it is tremendous. It is time that we dig deep into our pockets and provide malaria programmes with the needed resources.”
 Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
Mentioning the need for resources raises a flag that calls on us to be a bit more circumspect about progress. IRINNews notes that this is a critical time in the fight against malaria, when threatened funding cuts could tip the balance in an already precarious struggle. IRIN takes the example of Zambia to raise caution. They report that the results of malaria control and the government efforts have been uneven. While parasite prevalence among small children is down almost by half in some areas, many parts of the country have seen increases in prevalence
IRIN concludes that, “For now, the biggest challenge for Zambia will be closing the gap in its malaria elimination strategy, which will cost around $160 million a year and is currently only about 50 percent funded – two thirds from international donors and one third from the Zambian government. Privately, international donors say the government must spend more money on its malaria programme if it is to succeed.” Cross-border transmission adds to the problem.
Internal strife is another challenge to malaria success. “The recent nurses’ strike which lasted for five months may have cost Kenya a continental award in reducing the prevalence of malaria during the 30th African Union Summit in Ethiopia on Sunday.” John Muchangi in the Star also noted that, “However, Kenya lost momentum last year and a major malaria outbreak during the prolonged nurses’ strike killed more than 30 people within two weeks in October.”
 Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Finally changes in epidemiology threaten efforts to eliminate malaria in Africa. Nkumana, et al. explain that, “Although the burden of Plasmodium falciparum malaria is gradually declining in many parts of Africa, it is characterized by spatial and temporal variability that presents new and evolving challenges for malaria control programs. Reductions in the malaria burden need to be sustained in the face of changing epidemiology whilst simultaneously tackling significant pockets of sustained or increasing transmission. Many countries like Zambia thus face both a financial and an epidemiological challenge.
Fortunately ALMA is equipped with the monitoring and advocacy tools to ensure that its members recognize and respond to such challenges. The Scorecards will keep the fight against the infectious diseases of poverty on track.