Elimination &MDA &NTDs &poverty &Schistosomiasis &Trachoma &Vector Control Bill Brieger | 13 Jun 2023
Eliminating NTDs as a Public Health Problem May Not Be Enough
The concept and goal of eliminating a disease appears simple on the surface, but complications ensue when the words “as a public health problem” are added. We know that the distinction exists between eradication and elimination with the former being globally and the latter being nationally or regionally. The sum total action of eliminating a disease from all endemic countries therefore results in total global eradication.
 The challenge comes when we try to qualify the concept of elimination. The US CDC defined elimination of disease as, “Reduction to zero of the incidence of a specified disease in a defined geographical area as a result of deliberate efforts; continued intervention measures are required.” Thus, there is no more transmission. Following from this eradication is defined as, “Permanent reduction to zero of the worldwide incidence of infection caused by a specific agent as a result of deliberate efforts; intervention measures are no longer needed.” Penn Medicine summarized this as, “Elimination means stopping the transmission of a disease in a specific geographic area or country, but not worldwide. Elimination is a crucial step in the path toward eradication, requiring constant monitoring and interventions to keep serious diseases at bay.”
The challenge comes when we try to qualify the concept of elimination. The US CDC defined elimination of disease as, “Reduction to zero of the incidence of a specified disease in a defined geographical area as a result of deliberate efforts; continued intervention measures are required.” Thus, there is no more transmission. Following from this eradication is defined as, “Permanent reduction to zero of the worldwide incidence of infection caused by a specific agent as a result of deliberate efforts; intervention measures are no longer needed.” Penn Medicine summarized this as, “Elimination means stopping the transmission of a disease in a specific geographic area or country, but not worldwide. Elimination is a crucial step in the path toward eradication, requiring constant monitoring and interventions to keep serious diseases at bay.”
The foregoing definitions seem straightforward, but what does elimination as a public health problem or a disease of public health concern mean? The World Health Organization recently “congratulate(d) Benin and Mali for eliminating trachoma as a public health problem. Concerning another neglected tropical disease (NTD), lymphatic filariasis (LF), global control programs are aiming “to reduce the prevalence of infection below target thresholds and to alleviate the suffering of people affected by lymphoedema and hydrocele.” Wiegand and colleagues in The Lancet Global Health note that, “For schistosomiasis, the criterion for elimination as a public health problem (EPHP) is defined as less than 1% prevalence of heavy-intensity infections (ie, ?50 Schistosoma haematobium eggs per 10 mL of urine or ?400 Schistosoma mansoni eggs per g of stool).” They take issue with the fact that such definitions mean that morbidity still exists, though at very levels, so elimination of transmission has not really occurred for any of these NTDs.
 Because the social, environmental, and behavioral conditions that favor transmission may still exists, one cannot guarantee that incidence such diseases may not increase again. All three diseases, LF, Schistosomiasis, and Trachoma have been tackled primarily through preventive chemotherapy, is simply put, using mass drug administration (MDA) over a period of years until active surveillance determines that “infection (is) below target thresholds.” Trachoma does have its SAFE strategy which includes water, sanitation and hygiene interventions, but drugs can reduce the disease without long term achievements in such activities have become sustainable.
Because the social, environmental, and behavioral conditions that favor transmission may still exists, one cannot guarantee that incidence such diseases may not increase again. All three diseases, LF, Schistosomiasis, and Trachoma have been tackled primarily through preventive chemotherapy, is simply put, using mass drug administration (MDA) over a period of years until active surveillance determines that “infection (is) below target thresholds.” Trachoma does have its SAFE strategy which includes water, sanitation and hygiene interventions, but drugs can reduce the disease without long term achievements in such activities have become sustainable.
Prada et al. in the Journal of Infectious Diseases warn that there can be resurgence of a disease that was documented to be eliminated as a public health problem. They explain that the transmission assessment survey held after several MDA rounds for LF may not be enough to guarantee that low levels of transmission and eventual elimination are achieved. They conclude that, “The risk of resurgence after achieving current targets is low and is hard to predict using just current prevalence. Although resurgence is often quick (<5 years), it can still occur outside of the currently recommended post-intervention surveillance period of 4–6 years,” and recommend monitoring beyond this period.
 Toor and co-researchers suggest for NTD programs that, “as case numbers drop and elimination comes into prospect, transmission reduction through other interventions, such as vector control and sanitation, becomes crucial in reducing the probability and speed of resurgence, particularly when MDA or screening programs are halted. Surveillance activities for detecting elimination and resurgence become increasingly important to ensure that successes are maintained.”
Toor and co-researchers suggest for NTD programs that, “as case numbers drop and elimination comes into prospect, transmission reduction through other interventions, such as vector control and sanitation, becomes crucial in reducing the probability and speed of resurgence, particularly when MDA or screening programs are halted. Surveillance activities for detecting elimination and resurgence become increasingly important to ensure that successes are maintained.”
Ultimately, unless the context of NTD transmission is addressed, elimination will be an elusive goal. Therefore, as WHO advocated on the recent World NTD Day, “Everybody, including leaders and communities, to confront the inequalities that drive NTDs and to make bold, sustainable investments to free the world’s most vulnerable communities affected by NTDs from a vicious cycle of disease and poverty.”
Anemia &Dracunculiasis Guinea Worm &Elimination &Leishmaniasis &MDA &Schistosomiasis Bill Brieger | 09 Sep 2020
NTD News Today 2020-09-09 from ASTMH
![]() The current table of contents from the American Journal of Tropical Medicine and Hygiene features several important articles on neglected tropical diseases and malaria. Below are abstracts of several with links to the journal.
The current table of contents from the American Journal of Tropical Medicine and Hygiene features several important articles on neglected tropical diseases and malaria. Below are abstracts of several with links to the journal.
Agent-Based Simulation for Seasonal Guinea Worm Disease in Chad Dogs
The campaign to eradicate dracunculiasis (Guinea worm [GW] disease) and its causative pathogen Dracunculus medinensis (GW) in Chad is challenged by infections in domestic dogs, which far outnumber the dwindling number of human infections. We present an agent-based simulation that models transmission of GW between a shared water source and a large population of dogs. The simulation incorporates various potential factors driving the infections including external factors and two currently used interventions, namely, tethering and larvicide water treatments.
By defining and estimating infectivity parameters and seasonality factors, we test the simulation model on scenarios where seasonal patterns of dog infections could be driven by the parasite’s life cycle alone or with environmental factors (e.g., temperature and rainfall) that could also affect human or dog behaviors (e.g., fishing versus farming seasons).
We show that the best-fitting model includes external factors in addition to the pathogen’s life cycle. From the simulation, we estimate that the basic reproductive number, R 0, is approximately 2.0; our results also show that an infected dog can transmit the infection to 3.6 other dogs, on average, during the month of peak infectivity (April). The simulation results shed light on the transmission dynamics of GWs to dogs and lay the groundwork for reducing the number of infections and eventually interrupting transmission of GW.
Village Response to Mass Drug Administration for Schistosomiasis in Mwanza Region, Northwestern Tanzania
Are We Missing Socioeconomic, Cultural, and Political Dimensions?
Praziquantel (PZQ)-based mass drug administration (MDA) is the main approach for controlling schistosomiasis in endemic areas. Interventions such as provision and use of clean and safe water, minimizing contacts with infested water, disposal of human waste in latrines, and snail control provide additional key interventions to break the transmission cycle and could complement and perhaps sustain the benefits of MDA. However, all interventions deployed need to be accepted by the targeted communities. A qualitative study was conducted to examine factors that might differentiate villages which did not show a substantial decrease in Schistosoma mansoni prevalence despite repeated, high treatment coverage referred to as “persistent hotspot villages” from villages which showed a substantial decrease in prevalence referred to as “responding (RES) villages.” A convenient sample of adults was drawn from eight villages. Thirty-nine key informants were interviewed and 16 focus groups were held with a total of 123 participants. Data were analyzed manually using a thematic content approach. In both hotspot and RES villages, schistosomiasis was not considered to be a priority health problem because of its chronic nature, lack of knowledge and awareness, and poverty among study communities.
Hotspot villages exhibited poor leadership style, lack of or insufficient social engagement, little or lack of genuine community participation, little motivation, and commitment to schistosomiasis control compared with RES villages where there were commitment and motivation to fight schistosomiasis. We support the view of scholars who advocate for the adoption of a biosocial approach for effective and sustainable PZQ-based MDA for schistosomiasis control.
Assessment of Incubation Period of Cutaneous Leishmaniasis due to Leishmania major in Tunisia
The period between the infective sandfly bites and appearance of cutaneous leishmaniasis (CL) lesions is still hypothetical and little studied. This work aimed at assessing the incubation time of zoonotic CL (ZCL) due to Leishmania major using a standardized methodology. The retrospective analysis used the epidemiological, clinical, and biological information available in the database recording all the CL cases diagnosed at the Parasitology Department of the Pasteur Institute of Tunis during 2015–2019. It allowed for the selection of 92 privileged observations 1) of confirmed CL cases with presentation suggestive of ZCL form 2) living in northern regions free of ZCL 3) with a single infective trip of less than a week to ZCL foci during transmission season and 4) with accurate dates of travel and onset of lesions. Incubation length computed in this population ranged from 1 to 21 weeks, with a median of 5 weeks (interquartile range: 3–8.5 weeks).
Schistosoma mansoni Vector Snails in Antigua and Montserrat
Snail-Related Considerations Pertinent to a Declaration of Elimination of Human Schistosomiasis.
Investigations leading to a WHO-validated declaration of elimination of schistosomiasis transmission are contemplated for several countries, including Caribbean island nations. With assistance from the Pan American Health Organization, we undertook freshwater snail surveys in two such nations, Antigua and Barbuda, and Montserrat in September and October 2017. Historically, the transmission of Schistosoma mansoni supported by the Neotropical vector snail Biomphalaria glabrata occurred in both countries. Transmission on the islands is thought to have been interrupted by the treatment of infected people, improved sanitation, introduction of competitor snails, and on Montserrat with the eruption of the Soufrière volcano which decimated known B. glabrata habitats. Guided by the available literature and local expertise, we found Biomphalaria snails in seven of 15 and one of 14 localities on Antigua and Montserrat, respectively, most of which were identified anatomically and molecularly as Biomphalaria kuhniana.
Two localities on Antigua harbored B. glabrata, but no schistosome infections in snails were found. For snail-related aspects of validation of elimination, there are needs to undertake basic local training in medical malacology, be guided by historical literature and recent human schistosomiasis surveys, improve and validate sampling protocols for aquatic habitats, enlist local expertise to efficiently find potential transmission sites, use both anatomical and molecular identifications of schistosomes or putative vector snail species found, if possible determine the susceptibility of recovered Biomphalaria spp. to S. mansoni, publish survey results, and provide museum vouchers of collected snails and parasites as part of the historical record.
Decreased Mortality of falciparum Malaria in Anemic Prisoners of War?
Modern clinical trials have suggested that anemia protects against malaria mortality. Military records of the Second World War in Asia were examined to see if there was support for this hypothesis. When relatively well-nourished Imperial Japanese Navy sailors captured on Nauru (n = 799) were imprisoned on the Fauro Islands, 26% died from falciparum malaria. Similarly treated but very malnourished colocated Imperial Army soldiers experienced low stable malaria mortality. One-fifth of previously healthy Australian Army soldiers (n = 252) retreating from New Britain died largely because of malaria in April 1942. Malnourished prisoners of war, who were as a group very anemic, both Australian Army soldiers in Thailand and Japanese Army soldiers in Papua New Guinea, had high malaria rates but very low (< 3%) mortality rates. Malaria immunity does not adequately explain this dichotomy, suggesting that severe nutritional deprivation may be protective against malaria mortality possibly because of iron-deficiency anemia.
COVID-19 &Diagnosis &Ebola &Malaria in Pregnancy &MDA &NTDs &Trachoma &Zoonoses Bill Brieger | 08 Sep 2020
Malaria News Today 2020-09-08
Today we share news and abstracts concerning detecting malaria in pregnancy, news about the opening remarks from the WHO Director General at a special malaria and COVID-19 webinar, resumption of NTD activities after COVID-19 restrictions reduced, and mapping of Ebola carrying bats whose territory overlaps malaria in Africa. Click on the links to read more.
Prevalence and clinical impact of malaria infections detected with a highly sensitive HRP2 rapid diagnostic test in Beninese pregnant women
While sub-microscopic malarial infections are frequent and potentially deleterious during pregnancy, routine molecular detection is still not feasible. This study aimed to assess the performance of a Histidine Rich Protein 2 (HRP2)-based ultrasensitive rapid diagnostic test (uRDT, Alere Malaria Ag Pf) for the detection of infections of low parasite density in pregnant women.
This study demonstrates the higher performance of uRDT, as compared to cRDTs, to detect low parasite density P. falciparum infections during pregnancy, particularly in the 1st trimester. uRDT allowed the detection of infections associated with maternal anaemia.
The distribution range of Ebola virus carriers in Africa may be larger than previously assumed
Since Ebola overlaps both symptomatically and geographically with malaria in Africa, it is “Worrying that science has hitherto underestimated the range of Ebola-transmitting bat and fruit bat species. In this case, the models would provide a more realistic picture,” explains Dr. Lisa Koch
Based on ecological niche modeling, his team was able to show that the respective bat and fruit bat species are able to thrive in West and East Africa, including large parts of Central Africa. A wide belt of potential habitats extends from Guinea, Sierra Leone, and Liberia in the west across the Central African Republic, the Republic of the Congo and the Democratic Republic of the Congo to Sudan and Uganda in the East. A few of the studied bats and fruit bats may even occur in the eastern part of South Africa.
WHO Director-General’s Opening Remarks At the Webinar – Responding to the Double Challenge of Malaria and Covid-19
 The WHO Director General is encouraged by efforts to maintain malaria services despite the COVID-19 outbreak, but says, “I would like to recognize and applaud all these efforts, and to thank all of you who have worked so hard to preserve and maintain those services to the greatest degree possible. However, despite these actions, it breaks my heart to report that we still expect to see an increase in cases and deaths from malaria.
The WHO Director General is encouraged by efforts to maintain malaria services despite the COVID-19 outbreak, but says, “I would like to recognize and applaud all these efforts, and to thank all of you who have worked so hard to preserve and maintain those services to the greatest degree possible. However, despite these actions, it breaks my heart to report that we still expect to see an increase in cases and deaths from malaria.
“In a recent WHO survey of 105 countries, 46% of countries reported disruptions in malaria diagnosis and treatment. These disruptions threaten to set us back even further in realizing our shared vision for a malaria-free world.”
NTD Disease treatments restart in Africa as COVID-19 restrictions ease
It is not just malaria services that have been disrupted by COVID-19 responses. Treatment programmes that will reach millions of Africans at risk from debilitating neglected tropical diseases (NTDs) have restarted in a significant step towards COVID-19 recovery. Around one million people in Jigawa state, Nigeria have received antibiotics to treat the blinding eye disease trachoma and stop it from spreading.
Nigeria is the first country that Sightsavers and partners has supported to resume work on NTDs, which can have a devastating impact on some of the poorest communities in the world, with other African countries due to follow soon. In April, the threat of COVID-19 led the World Health Organization to recommend suspending mass treatment campaigns, which treat and prevent these diseases, but it has since provided guidance on restarting activities safely.
Asymptomatic &Burden &Dengue &Diagnosis &Ebola &Elimination &Epidemiology &Health Systems &ITNs &MDA &Mosquitoes &NTDs &Schistosomiasis &Schools &Vector Control &Zoonoses Bill Brieger | 30 Jun 2019
The Weekly Tropical Health News 2019-06-29
Below we highlight some of the news we have shared on our Facebook Tropical Health Group page during the past week.
Polio Persists
If all it took to eradicate a disease was a well proven drug, vaccine or technology, we would not be still reporting on polio, measles and guinea worm, to name a few. In the past week Afghanistan reported 2 wild poliovirus type 1 (WPV1) cases, and Pakistan had 3 WPV1 cases. Circulating vaccine-derived poliovirus type 2 (cVDPV2) was reported in Nigeria (1), DRC (4) and Ethiopia (3) from healthy community contacts.
Continued Ebola Challenges
In the seven days from Saturday to Friday (June 28) there were 71 newly confirmed Ebola Cases and 56 deaths reported by the Democratic Republic of Congo’s Ministry of Health. As Ebola cases continue to pile up in the Democratic Republic of the Congo (DRC), with 12 more confirmed Thursday and 7 more Friday, a USAID official said four major donors have jump-started a new strategic plan for coordinating response efforts. To underscore the heavy toll the outbreak has caused, among its 2,284 cases, as noted on the World Health Organization Ebola dashboard today, are 125 infected healthcare workers, including 2 new ones, DRC officials said.
Pacific Standard explained the differences in Ebola outbreaks between DRC today and the West Africa outbreak of 2014-16. On the positive side are new drugs used in organized trials for the current outbreak. The most important factor is safe, effective vaccine that has been tested in 2014-16, but is now a standard intervention in the DRC. While both Liberia and Sierra Leone had health systems and political weaknesses as post-conflict countries, DRC’s North Kivu and Ituri provinces are currently a war zone, effectively so for the past generation. Ebola treatment centers and response teams are being attacked. There are even cultural complications, a refusal to believe that Ebola exists. So even with widespread availability of improved technologies, teams may not be able to reach those in need.
To further complicate matters in the DRC, Doctors Without Borders (MSF) “highlighted ‘unprecedented’ multiple crises in the outbreak region in northeastern DRC. Ebola is coursing through a region that is also seeing the forced migration of thousands of people fleeing regional violence and is dealing with another epidemic. Moussa Ousman, MSF head of mission in the DRC, said, ‘This time we are seeing not only mass displacement due to violence but also a rapidly spreading measles outbreak and an Ebola epidemic that shows no signs of slowing down, all at the same time.’”
NIPAH and Bats
Like Ebola, NIPAH is zoonotic, and also involves bats, but the viruses differ. CDC explains that, “Nipah virus (NiV) is a member of the family Paramyxoviridae, genus Henipavirus. NiV was initially isolated and identified in 1999 during an outbreak of encephalitis and respiratory illness among pig farmers and people with close contact with pigs in Malaysia and Singapore. Its name originated from Sungai Nipah, a village in the Malaysian Peninsula where pig farmers became ill with encephalitis.
A recent human outbreak in southern India has been followed up with a study of local bats. In a report shared by ProMED, out of 36 Pteropus species bats tested for Nipah, 12 (33%) were found to be positive for anti-Nipah bat IgG antibodies. Unlike Ebola there are currently no experimental drugs or vaccines.
Climate Change and Dengue
Climate change is expected to heighten the threat of many neglected tropical diseases, especially arboviral infections. For example, the New York Times reports that increases in the geographical spread of dengue fever. Annually “there are 100 million cases of dengue infections severe enough to cause symptoms, which may include fever, debilitating joint pain and internal bleeding,” and an estimated 10,000 deaths. Dengue is transmitted by Aedes mosquitoes that also spread Zika and chikungunya. A study, published Monday in the journal Nature Microbiology, found that in a warming world there is a strong likelihood for significant expansion of dengue in the southeastern United States, coastal areas of China and Japan, as well as to inland regions of Australia. “Globally, the study estimated that more than two billion additional people could be at risk for dengue in 2080 compared with 2015 under a warming scenario.”
Schistosomiasis – MDA Is Not Enough, and Neither Are Supplementary Interventions
Schistosomiasis is one of the five neglected tropical diseases (NTDs) that are being controlled and potentially eliminated through mass drug administration (MDA) of preventive chemotherapy (PCT), in this case praziquantel. In The Lancet Knopp et al. reported that biannual MDA substantially reduced Schistosomiasis haematobium prevalence and infection intensity but was insufficient to interrupt transmission in Zanzibar. In addition, neither supplementary snail control or behaviour change activities did not significantly boost the effect of MDA. Most MDA programs focus on school aged children, and so other groups in the community who have regular water contact would not be reached. Water and sanitation activities also have limitations. This raises the question about whether control is acceptable for public health, or if there needs to be a broader intervention to reach elimination?
Trachoma on the Way to Elimination
Speaking of elimination, WHO has announced major “sustained progress” on trachoma efforts. “The number of people at risk of trachoma – the world’s leading infectious cause of blindness – has fallen from 1.5 billion in 2002 to just over 142 million in 2019, a reduction of 91%.” Trachoma is another NTD that uses the MDA strategy.
The news about NTDs from Dengue to Schistosomiasis to Trachoma is complicated and demonstrates that putting diseases together in a category does not result in an easy choice of strategies. Do we control or eliminate or simply manage illness? Can our health systems handle the needs for disease elimination? Is the public ready to get on board?
Malaria Updates
And concerning being complicated, malaria this week again shows many facets of challenges ranging from how to recognize and deal with asymptomatic infection to preventing reintroduction of the disease once elimination has been achieved. Several reports this week showed the particular needs for malaria intervention ranging from high burden areas to low transmission verging on elimination to preventing re-introduction in areas declared free from the disease.
In South West, Nigeria Dokunmu et al. studied 535 individuals aged from 6 months were screened during the epidemiological survey evaluating asymptomatic transmission. Parasite prevalence was determined by histidine-rich protein II rapid detection kit (RDT) in healthy individuals. They found that, “malaria parasites were detected by RDT in 204 (38.1%) individuals. Asymptomatic infection was detected in 117 (57.3%) and symptomatic malaria confirmed in 87 individuals (42.6%).
Overall, detectable malaria by RDT was significantly higher in individuals with symptoms (87 of 197/44.2%), than asymptomatic persons (117 of 338/34.6%)., p = 0.02. In a sub-set of 75 isolates, 18(24%) and 14 (18.6%) individuals had Pfmdr1 86Y and 1246Y mutations. Presence of mutations on Pfmdr1 did not differ by group. It would be useful for future study to look at the effect of interventions such as bednet coverage. While Southwest Nigeria is a high burden area, the problem of asymptomatic malaria will become an even bigger challenge as prevalence reduces and elimination is in sight.
Sri Lanka provides a completely different challenge from high burden areas. There has been no local transmission of malaria in Sri Lanka for 6 years following elimination of the disease in 2012. Karunasena et al. report the first case of introduced vivax malaria in the country by diagnosing malaria based on microscopy and rapid diagnostic tests. “The imported vivax malaria case was detected in a foreign migrant followed by a Plasmodium vivax infection in a Sri Lankan national who visited the residence of the former. The link between the two cases was established by tracing the occurrence of events and by demonstrating genetic identity between the parasite isolates. Effective surveillance was conducted, and a prompt response was mounted by the Anti Malaria Campaign. No further transmission occurred as a result.”
Bangladesh has few but focused areas of malaria transmission and hopes to achieve elimination of local transmission by 2030. A particular group for targeting interventions is the population of slash and burn cultivators in the Rangamati District. Respondents in this area had general knowledge about malaria transmission and modes of prevention and treatment was good according to Saha and the other authors. “However, there were some gaps regarding knowledge about specific aspects of malaria transmission and in particular about the increased risk associated with their occupation. Despite a much-reduced incidence of malaria in the study area, the respondents perceived the disease as life-threatening and knew that it needs rapid attention from a health worker. Moreover, the specific services offered by the local community health workers for malaria diagnosis and treatment were highly appreciated. Finally, the use of insecticide-treated mosquito nets (ITN) was considered as important and this intervention was uniformly stated as the main malaria prevention method.”
Kenya offers some lessons about low transmission areas but also areas where transmission may increase due to climate change. A matched case–control study undertaken in the Western Kenya highlands. Essendi et al. recruited clinical malaria cases from health facilities and matched to asymptomatic individuals from the community who served as controls in order to identify epidemiological risk factors for clinical malaria infection in the highlands of Western Kenya.
“A greater percentage of people in the control group without malaria (64.6%) used insecticide-treated bed nets (ITNs) compared to the families of malaria cases (48.3%). Low income was the most important factor associated with higher malaria infections (adj. OR 4.70). Houses with open eaves was an important malaria risk factor (adj OR 1.72).” Other socio-demographic factors were examined. The authors stress the need to use local malaria epidemiology to more effectively targeted use of malaria control measures.
The key lesson arising from the forgoing studies and news is that disease control needs strong global partnerships but also local community investment and adaptation of strategies to community characteristics and culture.
Ivermectin &Larvicide &MDA &Vaccine &Zero Malaria Bill Brieger | 25 Apr 2019
Zero Malaria Starts with Universal Coverage: Part 3 Innovations and New Interventions
Newer malaria interventions are coming on board, and whether these will be used of a large scale or targeted to certain epidemiological contexts remains to be seen. In each case, one will need to examine if in each context one can measure whether the intervention is universally accessible to and used by the intended population or subgroup.
 After 30 years of research and testing, a malaria vaccine is ready to go through implementation testing in Malawi, Ghana and Kenya. This pilot of the vaccine, known as RTS,S, will be made available to children up to 2 years of age with the Malawi launching first during the week of World Malaria Day.
After 30 years of research and testing, a malaria vaccine is ready to go through implementation testing in Malawi, Ghana and Kenya. This pilot of the vaccine, known as RTS,S, will be made available to children up to 2 years of age with the Malawi launching first during the week of World Malaria Day.
WHO explains that, “The malaria vaccine pilot aims to reach about 360,000 children per year across the three countries. Ministries of health will determine where the vaccine will be given; they will focus on areas with moderate-to-high malaria transmission, where the vaccine can have the greatest impact.” There will be a strong monitoring component to identify coverage levels as well as any implementation challenges and adverse effects that may only become visible in a larger scale intervention that the typical efficacy trials. Implementation is occurring in areas with a relatively strong existing malaria control effort, with an intent to learn how a vaccine can complement a total control package.
 Mass Drug Administration (MDA, also known as preventive chemotherapy) has been a successful strategy for controlling and eliminating neglected tropical diseases with special reference to onchocerciasis, lymphatic filariasis, trachoma, soil transmitted helminths and schistosomiasis. MDA use in malaria has been limited due to a number of financial and logistical challenges, not the least of which is the need to achieve high coverage over several periods of distribution. This is why WHO recommends, “Use of MDA for the elimination of P. falciparum malaria can be considered in areas approaching interruption of transmission where there is good access to treatment, effective implementation of vector control and surveillance, and a minimal risk of re-introduction of infection.”
Mass Drug Administration (MDA, also known as preventive chemotherapy) has been a successful strategy for controlling and eliminating neglected tropical diseases with special reference to onchocerciasis, lymphatic filariasis, trachoma, soil transmitted helminths and schistosomiasis. MDA use in malaria has been limited due to a number of financial and logistical challenges, not the least of which is the need to achieve high coverage over several periods of distribution. This is why WHO recommends, “Use of MDA for the elimination of P. falciparum malaria can be considered in areas approaching interruption of transmission where there is good access to treatment, effective implementation of vector control and surveillance, and a minimal risk of re-introduction of infection.”
Another link with MDA for a different disease, onchocerciasis, has pointed to a potential new malaria intervention. Around ten years ago it was observed that after ivermectin treatment for onchocerciasis in Senegal survivorship of malaria vectors was reduced. Subsequently the potential effect of ivermectin has been intentionally researched with the outcome that, “Frequently repeated mass administrations of ivermectin during the malaria transmission season can reduce malaria episodes among children without significantly increasing harms in the populace.” Mathematical models for onchocerciasis control have predicted the need to achieve annual coverage targets below what could be called universal levels. Using ivermectin for mosquito control would require more frequent dosing and higher coverage.
Although not defined as ‘new’ it is important to include mention of additional vector interventions like larviciding and indoor residual spraying, as these present technical and coverage challenges. For example, larviciding interventions either chemical or biological, do not cover individuals. These focus on breeding sites in communities. This may require better use of the concept of geographical coverage as has been used in onchocerciasis control wherein the proportion of endemic villages reached is monitored.
For example, in Mali the NTD program aimed to achieve 80% program coverage of individuals eligible for preventive chemotherapy and 100% geographical coverage yearly. This means all villages should be reached. In reality, the program achieved 85% geographical coverage for lymphatic filariasis and over 90% for onchocerciasis.
In conclusion, we have seen that defining as well as achieving universal coverage of malaria interventions is a challenging prospect. For example, do we base our monitoring on households, villages, or populations? Do we have the funds and technical capacity to implement and sustain the level of coverage required to have an impact on malaria transmission and move toward elimination? Are we able to introduce new, complimentary and appropriate interventions as a country moves closer to elimination?
CHW &Community &ITNs &Ivermectin &Mapping &MDA &Seasonal Malaria Chemoprevention Bill Brieger | 04 Jul 2018
Mapping to Integrate Filariasis and Onchocerciasis Control with Malaria Interventions
 William R Brieger (wbriege1@jhu.edu) and Gilbert Burnham (gburnha1@jhu.edu) of The Johns Hopkins Bloomberg School of Public Health, Department of International Health presented ideas about mapping and integration of neglected tropical diseases and malaria interventions at the Malaria World Congress, Melbourne, Australia, July 2018
William R Brieger (wbriege1@jhu.edu) and Gilbert Burnham (gburnha1@jhu.edu) of The Johns Hopkins Bloomberg School of Public Health, Department of International Health presented ideas about mapping and integration of neglected tropical diseases and malaria interventions at the Malaria World Congress, Melbourne, Australia, July 2018
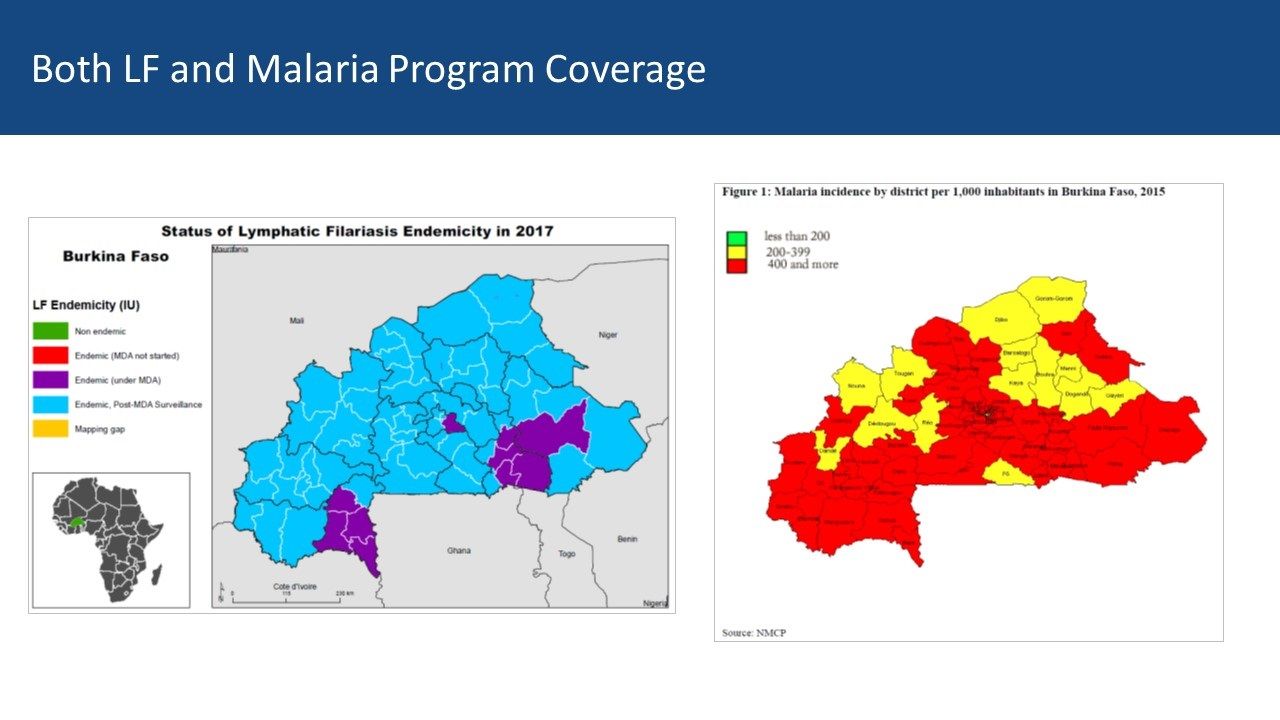
Overview: Lymphatic Filariasis (LF) and Malaria share a common vector in sub-Saharan Africa. Mass Drug Administration (MDA) is a strategy that is common to both diseases. Where the diseases overlap there is the potential opportunity to coordinate both vector control and MDA to achieve synergy in program results. The example of Burkina Faso, supplemented with information from Ghana, serves as an example of what could be integrated and what actually happens.
 Background: Thirty years ago then veterinary drug, ivermectin, was found effective in controlling neglected tropical diseases (NTDs), specifically two human filarial diseases: onchocerciasis and lymphatic filariasis (LF). The drug manufacturer donates 300 million treatments annually to eliminate both diseases. Since then, annual community based mass drug administration (MDA) efforts have resulted in millions of treatments in endemic countries and great progress has been made toward elimination of transmission. Through observation and experimentation, ivermectin was found to kill malaria carrying mosquitoes when they bite people who have taken ivermectin making it a useful tool for vector control.
Background: Thirty years ago then veterinary drug, ivermectin, was found effective in controlling neglected tropical diseases (NTDs), specifically two human filarial diseases: onchocerciasis and lymphatic filariasis (LF). The drug manufacturer donates 300 million treatments annually to eliminate both diseases. Since then, annual community based mass drug administration (MDA) efforts have resulted in millions of treatments in endemic countries and great progress has been made toward elimination of transmission. Through observation and experimentation, ivermectin was found to kill malaria carrying mosquitoes when they bite people who have taken ivermectin making it a useful tool for vector control.

CHWs in Burkina Faso demonstrating how to measure height to determine ivermectin dosage
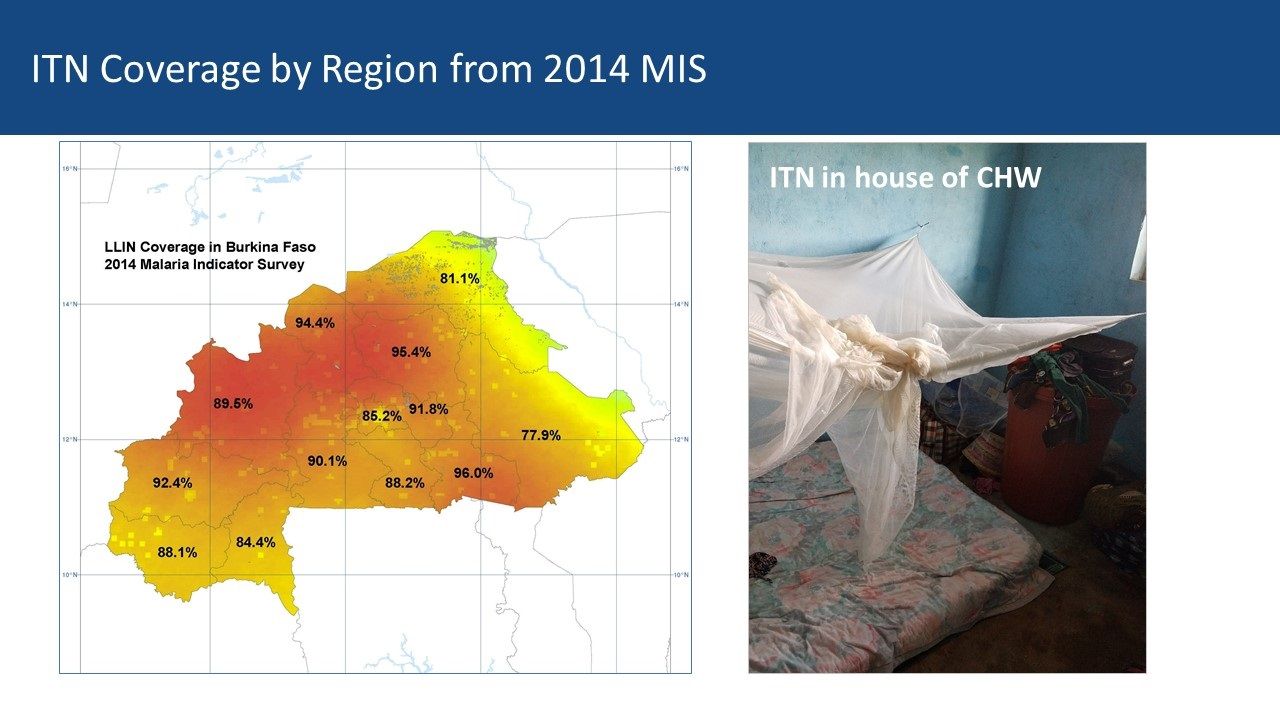
Community Health Workers’ Role: Current research is examining how dosing and timing of treatments may impact national malaria vector control efforts. Comparing maps between malaria and LF can be a starting point for adapting ivermectin MDAs for malaria vector control. Burkina Faso MDAs are operationalized by community health workers (CHWs) who are part of a national program that provides treatment for common illnesses and also conducts village level onchocerciasis and LF MDAs. Vector Control with Long Lasting Insecticide Treated Nets In most of rural Africa, malaria and lymphatic Filariasis are co-endemic and share the same anopheles mosquito vector.
However, that does not mean that there is a coordinated effort to plan distribution of LLINs despite the fact that the intervention meets the needs of both disease control efforts. The current NTD programs in Burkina Faso and Ghana focus on Preventive Chemotherapy (PCT) delivered through Mass Drug Administration (MDA). Vector Control is seen as essential in areas co-endemic with LF, Loa loa and Malaria – mapping helps identify priority areas for vector control.
 Vector Control by Chance: In Ghana, the NTD/LF elimination program was unaware of the LLIN coverage data available in the NMCP housed in an adjacent building. This illustrates the lack of collaboration between the two programs. Thus where — and if — vector control benefits the reduction of both diseases, it is often by chance where LF is concerned. The International NGO, The Carter Center, may be the only one that includes vector control as part of its programming for both malaria and LF in Nigeria. This practice should be replicated by other partners and country programs where possible.
Vector Control by Chance: In Ghana, the NTD/LF elimination program was unaware of the LLIN coverage data available in the NMCP housed in an adjacent building. This illustrates the lack of collaboration between the two programs. Thus where — and if — vector control benefits the reduction of both diseases, it is often by chance where LF is concerned. The International NGO, The Carter Center, may be the only one that includes vector control as part of its programming for both malaria and LF in Nigeria. This practice should be replicated by other partners and country programs where possible.
 Mass Drug Administration: MDA is the major strategy for control of five PCT diseases in the NTD program, and LF is one of those. Currently MDA anti-malarial drugs has been considered in limited situations in countries where there are areas that have very low transmission In the future countries may consider research that shows mosquitocidal effects of Onchocerciasis and LF MDAs with ivermectin. Otherwise for malaria, a special intervention called Seasonal Malaria Chemoprevention (SMC) is used in an MDA-like approach to reach young children in the African Sahel during high transmission months. In both cases, existing cadres of (usually volunteer) community health workers are the front line providers of MDA.
Mass Drug Administration: MDA is the major strategy for control of five PCT diseases in the NTD program, and LF is one of those. Currently MDA anti-malarial drugs has been considered in limited situations in countries where there are areas that have very low transmission In the future countries may consider research that shows mosquitocidal effects of Onchocerciasis and LF MDAs with ivermectin. Otherwise for malaria, a special intervention called Seasonal Malaria Chemoprevention (SMC) is used in an MDA-like approach to reach young children in the African Sahel during high transmission months. In both cases, existing cadres of (usually volunteer) community health workers are the front line providers of MDA.
Burkina Faso LF Map from ESPEN: Mapping shows 10 of 70 health districts are currently doing LF MDA, though all have done it. Thus CHWs in all districts are experienced in ivermectin MDA. The malaria map shows that two-thirds of districts have a malaria incidence of 400/1000 or more while 14 have lower incidence. There is an overlap between current LF MDA districts and higher incidence malaria districts Both LF and Malaria Program Coverage can be seen to overlap in [program maps.

Ghana CHWs explain how they conduct MDA
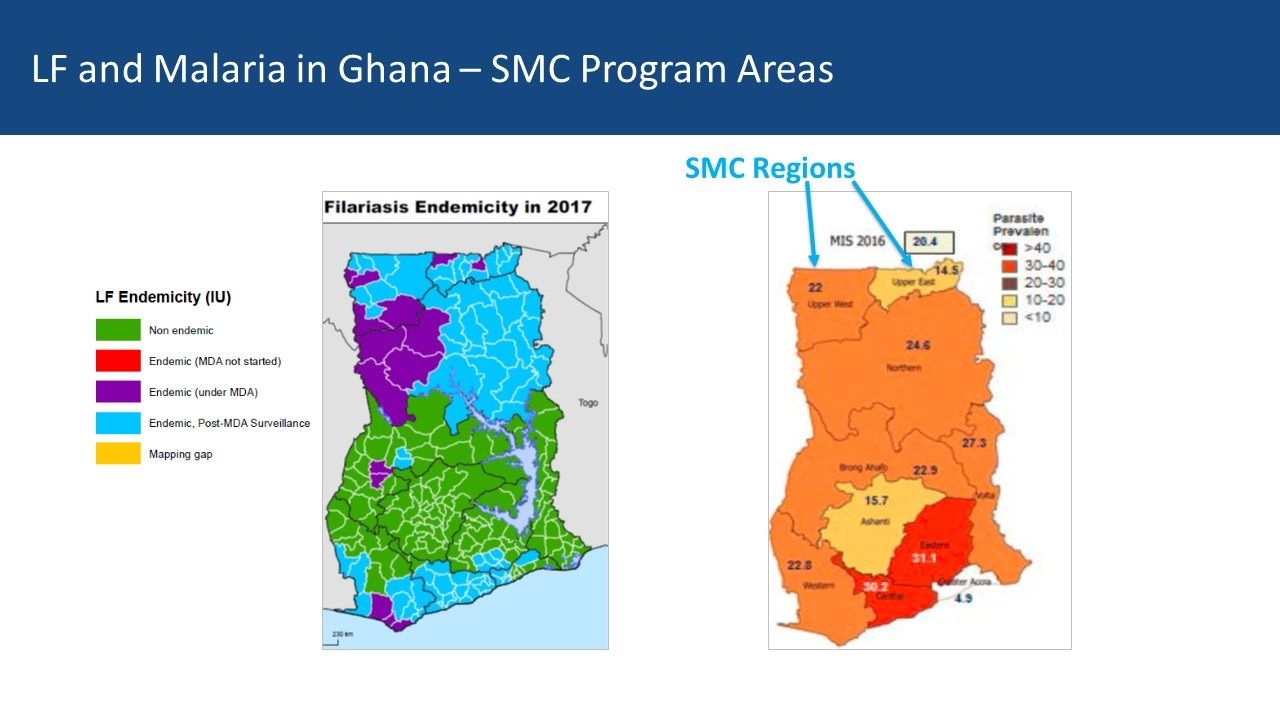
Ghana Experiences: Ghana provides a contrasting example. There five regions in central Ghana that are mostly non-endemic for LF but do have moderate malaria transmission In the south two regions with former LF MDA activity overlap with higher malaria endemicity While four northern regions have lower malaria parasite prevalence, they do have current and recent LF MDAs Community Directed Distributors work with LF MDA in Ghana
Conclusions: Malaria elimination will need a mix of strategies to be successful. Therefore, it is not too early for malaria and NTD program managers, as well as their respective donors, to begin comparing maps to identify possibilities for adapting ivermectin MDAs for malaria vector control. Even though one endemic disease is nearing control or elimination, the infrastructure put in place to accomplish this can be mobilized for other disease control efforts – as long as we map where interventions and resources have been targeted.
Elimination &Ivermectin &MDA &NTDs &Procurement Supply Management Bill Brieger | 16 Jun 2018
Many Neglected Tropical Diseases: What About Eliminating Them?

Testing to see if transmission of lymphatic filariasis has stopped in Burkina Faso
Two things we need to note about the list of 20 diseases that the World Health Organization and partners classify as Neglected Tropical Diseases (NTDs). First, diseases like Rabies, Snakebite/envenoming, and Leprosy, while certainly more common in the tropics now, have in the past been global in distribution. Secondly some of the diseases have not been neglected. Onchocerciasis or river blindness has been the focus of a global partnership since 1975, and transmission in the America’s and much of the Sahel in Africa has been halted. Elimination of Dracunculiasis or Guinea Worm has also been the subject of many World Health Assembly Resolutions, and concerted effort has brought the number of cases down from 3.5 million in 1986 to 30 in 2017. What is more to the point about these diseases is that they affect neglected people, the poor and vulnerable in remote rural areas or urban slums.
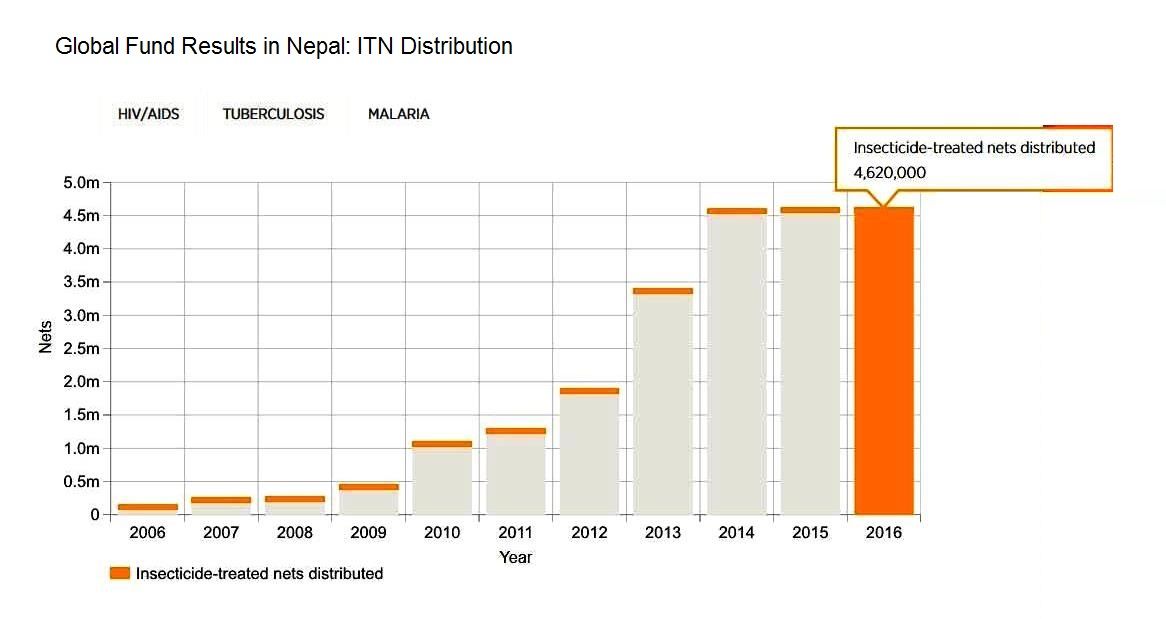
Still when we can compare NTD control programs with the rise of major disease control efforts like the Global Fund to fight AIDS, Tuberculosis and Malaria, the President’s Emergency Program For AIDS Relief, the President’s Malaria Initiative, World Bank Malaria Booster Program, Global A Vaccine Initiative among others, we can see that the global community has been able to focus major financial resources on a few diseases. Now with the Sustainable Development Goals, that focus expanded from infectious to Non-Communicable Diseases. It is natural therefore to fear that tropical health problems that are responsible for major loss of life and economic capacity will not be adequately addressed.

A system of rewards helped identify the last cases in many guinea worm endemic countries
Based on the World Health Organization’s 2020 Roadmap on NTDs, the London Declaration on NTDs recognized a “tremendous opportunity to control or eliminate at least 10 of these devastating diseases by the end of the decade” (i.e. by 2020). These include eradication of Guinea worm disease, and elimination by 2020 of lymphatic filariasis (LF), leprosy, sleeping sickness {human African trypanosomiasis) and blinding trachoma. In addition drug access programmes should help control by 2020 schistosomiasis, soil-transmitted helminthes (STH), Chagas disease, visceral leishmaniasis and river blindness (onchocerciasis).
Five of the diseases are notable in that they can either be controlled or eliminated through Mass Drug Administration (MDA) using Preventive Chemo-Therapy (PCT). This effort is aided by drug donation programs at the global level and community based MDA at the local level. Ten companies were signatories to the London Declaration and contributed to drug donation programs to achieve MDA. According to WHO,
Preventive chemotherapy is aimed at optimizing the largescale use of safe, single-dose medicines and offers the best means of reducing the extensive morbidity associated with four helminthiases (lymphatic filariasis, onchocerciasis, schistosomiasis and soil-transmitted helminthiases) (6). Additionally, the large-scale administration of azithromycin – a key component of the SAFE strategy for trachoma (that is, lid surgery (S), antibiotics to treat the community pool of infection (A), facial cleanliness (C) and environmental improvement (E)) – is amenable to close coordination and, in future, possibly co-administration with interventions targeted at helminthiases.

Community health workers are the cornerstone of many NTD elimination programs
Targets for the 5 PCT diseases vary. The aim is to eliminate LF and Trachoma by 2020. Although the efforts against onchocerciasis have been running the longest, the refocus from control to elimination meant increasing the geographical scope of intervention, and now elimination may not be feasible until 2025. With a focus mainly on the school aged and based populations, programs against schistosomiasis and STH talk of control, not elimination, although some endemic countries hope that elimination may be possible if the focus of these programs expands. So far, Togo is the only Sub-Saharan African country to have eliminated LF, and Ghana to have eliminated Trachoma.
Partnerships, funding and drug donations need to be strengthened if more countries are to join the ranks of Togo and Nepal.
Asia &Case Management &Diagnosis &Elimination &MDA Bill Brieger | 12 May 2017
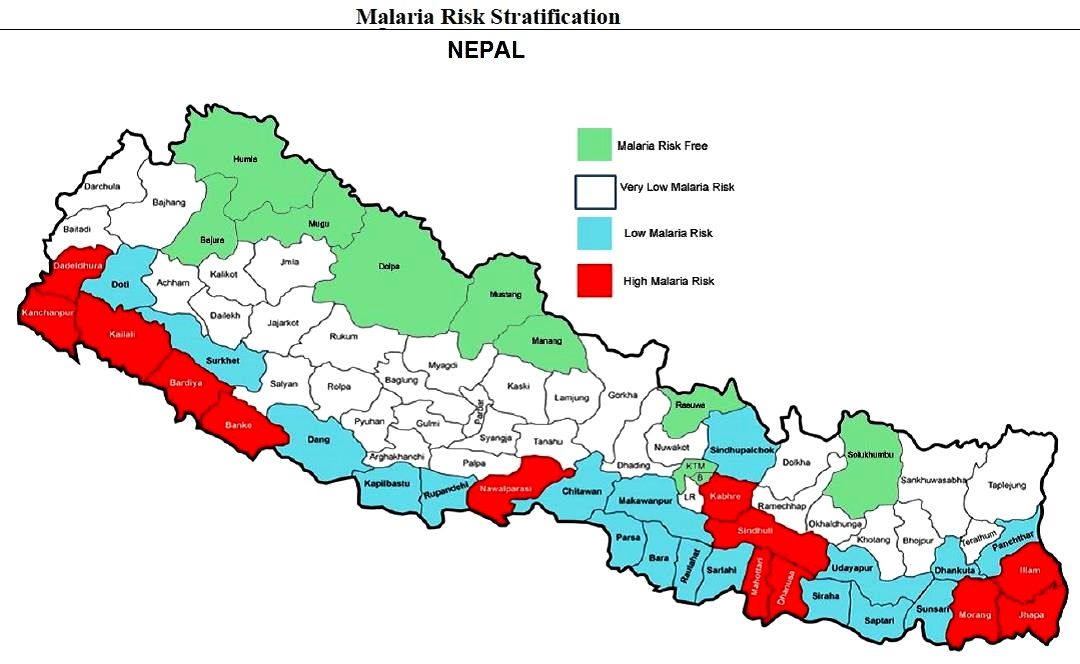
Nepal on the Path to Malaria Elimination
Jhpiego’s Emmanuel Le Perru has been placed with Nepal’s malaria control program by the Maternal and Child Survival Program (USAID) to strengthen the agency’s overall response to malaria as well as ensure top performance of Nepal’s Global Fund Malaria grant. Emmanuel shares his experiences with us here.
From 3,000 cases in 2010, Nepal reported around 1,000 cases in 2016, including 85% Plasmodium vivax cases. However private sector reporting is almost null so number of total cases may be the double. Nepal’s National Malaria Strategic  Plan (NMSP) targets Elimination by 2022 (0 indigenous cases) with WHO certification by 2026.
Plan (NMSP) targets Elimination by 2022 (0 indigenous cases) with WHO certification by 2026.
Ward Level Micro-stratification is an important step for targeting appropriate interventions. Key interventions in the NMSP include case notification system by SMS (from health post workers or district vector control inspectors) to a Malaria Disease Information System, later to be merged with DHIS2. Case investigation teams conduct case and foci profiling as well as “passive cases” active detection and treatment (including staff from district such as surveillance coordinator, vector control inspector, and entomologist).
 Malaria Mobile Clinics actively search/treat new cases in high risk areas (slums, brick factories, river villages or flooded areas, migrant workers villages, etc.). PCR diagnosis with Dry Blood Spot or Whole Blood is used to identify low density parasite cases, relapses or re-introduction. Coming up in April-June 2018 will be a Pilot of MDA (primaquine) for Plasmodium vivax in isolated settings (80% of cases in the country are P vivax).
Malaria Mobile Clinics actively search/treat new cases in high risk areas (slums, brick factories, river villages or flooded areas, migrant workers villages, etc.). PCR diagnosis with Dry Blood Spot or Whole Blood is used to identify low density parasite cases, relapses or re-introduction. Coming up in April-June 2018 will be a Pilot of MDA (primaquine) for Plasmodium vivax in isolated settings (80% of cases in the country are P vivax).
Recent successes in the national malaria effort include the number of cases notified by SMS went from 0% to 45%. Also the number of cases fully investigated went from 22% to 52%, though this needs to go up to 95% for elimination. 73% of districts are now submitting timely malaria data reports per national guidelines, an increase from 52% in November 2015.

The border runs right through this town making importation of malaria cases easy
The Global Fund (GFATM) malaria grant rating went from B2 to A2. Nepal Epidemiology Disease Control Division (EDCD), WHO and GFATM are keen to pilot MDA for P vivax in isolated setting which MCSP/Jhpiego Advisor taking the lead.
Moving forward the malaria elimination effort needs to address Indo-Nepal Cross boarder collaboration since 45% cases are imported. Hopefully WHO will help EDCD Nepal to propose a plan of action to India. The program still needs to convince partners of relevance of malaria mobile clinics vs community testing and of the relevance of MDA for P vivax. More entomological and PCR/laboratory expertise is needed. With these measures malaria elimination should be in sight.

Diagnosis &Elimination &Ivermectin &MDA &Treatment Bill Brieger | 20 Nov 2016
Leadership and Support for Malaria Pre-Elimination in Nepal
Emmanuel Le Perru, Jhpiego field staff in Nepal, shared his experiences in aiding the malaria pre-elimination efforts in the country during a retreat that preceded the 65th Annual Meeting of the American Society of Tropical Medicine and Hygiene in Atlanta. Here are some highlights of his talk.
 Malaria Pre-Elimination efforts are targeting 0 deaths as well as investigation of 100% of confirmed cases in Nepal. Systematic entomology investigation/interventions are required. Glucose-6-Phosphate Dehydrogenase deficiency (enzyme genetic defect causing hemolysis with primaquine) testing for Plasmodium vivax in high G6PDd prevalence communities is required. Cases should receive treatment within 72 hours of symptoms for Pf (to quickly prevent transmission and gametocyte reservoir). There is also a need to distinguish between indigenous and imported cases.
Malaria Pre-Elimination efforts are targeting 0 deaths as well as investigation of 100% of confirmed cases in Nepal. Systematic entomology investigation/interventions are required. Glucose-6-Phosphate Dehydrogenase deficiency (enzyme genetic defect causing hemolysis with primaquine) testing for Plasmodium vivax in high G6PDd prevalence communities is required. Cases should receive treatment within 72 hours of symptoms for Pf (to quickly prevent transmission and gametocyte reservoir). There is also a need to distinguish between indigenous and imported cases.
Jhpiego is providing technical assistance and capacity building for Nepal’s Ministry of Health pre-elimination efforts as follows:
- Integrated Vector Management
- Micro-stratification
- Entomology curriculum to be conducted in medical college (need new positions)
- Case-based Surveillance guidelines
- Private-sector engagement (for increased reporting and product quality control/procurement such as Antigen RDTs)
- Capacity Assessments in 9 health systems strengthening components at central and district levels (Jhpiego Malaria Implementation Guide)
- Human resources: clear job descriptions and performance goals
- Leadership & Management development program
 Program highlights include the fact that the Global Fund malaria grant rating improved from B2 (inadequate but demonstrating potential) in January 2016, but now A2 (meeting expectations) in November 2016. Concept note for operational research at 2 or 3 border check points has been developed in order to determine whether such intervention (communication & voluntary screening) is cost-effective and relevant to catch/target imported cases, raise awareness on malaria available services, detect/prevent sources of potential outbreaks. This will inform GFATM on the relevance to fund such intervention. A similar approach was done at the China-Myanmar border but was not recognized by not WHO.
Program highlights include the fact that the Global Fund malaria grant rating improved from B2 (inadequate but demonstrating potential) in January 2016, but now A2 (meeting expectations) in November 2016. Concept note for operational research at 2 or 3 border check points has been developed in order to determine whether such intervention (communication & voluntary screening) is cost-effective and relevant to catch/target imported cases, raise awareness on malaria available services, detect/prevent sources of potential outbreaks. This will inform GFATM on the relevance to fund such intervention. A similar approach was done at the China-Myanmar border but was not recognized by not WHO.
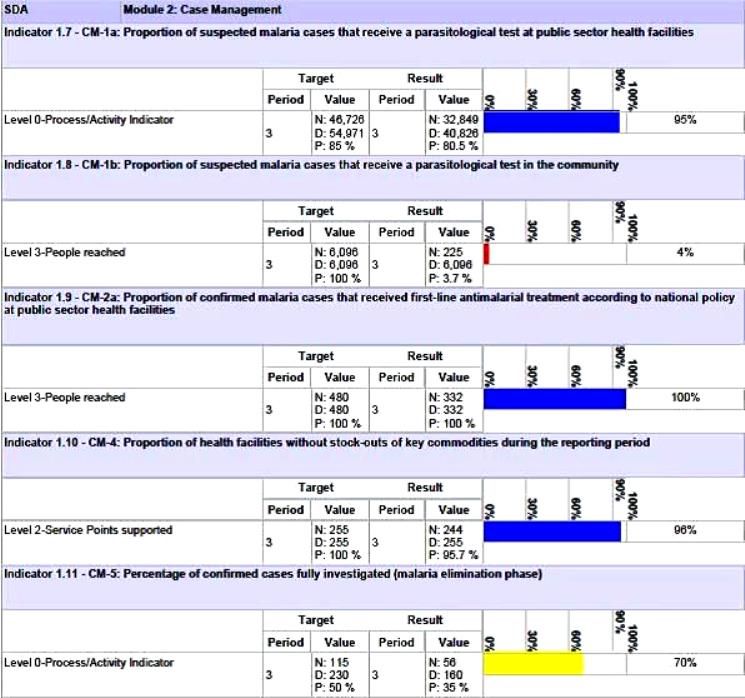
Nepal’s Global Fund Grant Indicators for Malaria Case Management
Although the National Malaria Strategic Plan refers to high risk groups (forest workers, national parks security personnel, refugees, prisoners, etc.) evidence is needed to back this up. A study or improved investigation forms are needed to identify such groups and use this information to design appropriate behavior change communications and other interventions.
Special Programming Highlights include proposing a focus on Closed/Isolated Settings/Foci (limited migration, duration and population) to WHO and GFATM. Considering a targeted mass drug administration (MDA) Plasmodium vivax (not yes recommended by WHO) with Primaquine/G6PD testing. Consideration is being given to new drugs in the pipeline such as Ivermectin. Molecular Testing using Polymerase Chain Reaction (PCR) to detect low parasitemia, asymptomatic or re-infection cases (Pv includes inactive/dormant sporozoites known as hypnozoites) is being proposed.
Community based testing as proposed in the Global Fund grant needs strengthening. Therefore RDT use by Female Community Health Volunteer is being considered. Active case detection is another possibility for those areas moving toward pre-elimination. As mentioned, there is also need for studies of asymptomatic infection.
Lessons learned so far for best practices for efforts in identifying specific pre-elimination interventions include the value of getting consensus at national level through the Malaria Technical Working Group. There is also need to challenge WHO recommendations and engage dialogue to get creative. At present there is a risk of a Catch 22 situation wherein the GFATM asks for innovative interventions but at the same time tries to adhere strictly WHO to existing guidance.
The Nepalese malaria program is in constant dialogue with the GFATM Fund Portfolio Manager and team on the local context and technical challenges in order to get them involved in looking for innovative solutions.
Challenges arise in malaria diagnostics. While systematic microscopy is the gold standard, quality can be poor because of low stain/re-agent quality, constant staff turnover and donor reluctance to fund additional training. Also microscopy confirmation and slide quality control are time consuming, and often this process is not clear or well followed. PCR require specific equipment, training and qualifications. Takes time to be operational.
There are opportunities moving forward. Progress could be made if there were more “elimination experts” to position to influencer to WHO to seek and propose new interventions for the pre-elimination stage. Nepal provides an ideal opportunity to test new ideas. It will also be necessary for the national malaria program staff to receive regular technical updates on program issues such as new drugs (Ivermectin?) and on-going pilots of MDA.