Uncategorized Bill Brieger | 30 Nov 2014
Malaria Diagnostic Service Availability – Mapping of Nigerian Private Sector Service Delivery Outlets
![]() This study was undertaken in seven US President’s Malaria Initiative supported Nigerian States through the Malaria Action Program for States (MAPS) project. Authors include Abiodun Ojo, Bolatito Aiyenigba, Sonny Johnbull, Adamu Onu, Olabanji Ipadeola, Muhammad Salihu, Kolawole Maxwell, Ebenezer Baba, and Abba Umar. Their presentation appeared at the recent annual meeting of the American Society of Tropical Medicine and Hygiene.
This study was undertaken in seven US President’s Malaria Initiative supported Nigerian States through the Malaria Action Program for States (MAPS) project. Authors include Abiodun Ojo, Bolatito Aiyenigba, Sonny Johnbull, Adamu Onu, Olabanji Ipadeola, Muhammad Salihu, Kolawole Maxwell, Ebenezer Baba, and Abba Umar. Their presentation appeared at the recent annual meeting of the American Society of Tropical Medicine and Hygiene.
The private sector’s role in health services in Nigeria has increased in recent times, and provides approximately 60% of health services. The PMI Malaria Action Program for States (MAPS) project currently supports the implementation of parasitological confirmation of malaria cases in public health facilities only in selected states. A mapping exercise was carried out to identify private facilities providing malaria diagnostic services and determine the gaps in existing malaria diagnostic capacity with the aim of designing a strategy for improvement
Questionnaires were administered to the private health facility owners and location data collected using handheld Global Positioning System (GPS) device. Data were collected from all private health facilities in the state capital of each MAPS supported states (Benue, Cross River, Ebonyi, Kogi, Nasarawa, Oyo and Zamfara) in October 2013.
 The questionnaire was designed to assess human resource capacity, method of malaria diagnosis and patient/client workload in the health facility. Data collectors and supervisors were trained on tools and methodology of the survey.
The questionnaire was designed to assess human resource capacity, method of malaria diagnosis and patient/client workload in the health facility. Data collectors and supervisors were trained on tools and methodology of the survey.
Results revealed that 394 private health facilities in 7 state capitals were mapped. Only 24.6% health workers had received training on malaria diagnosis in the last 12 months preceding the survey, while 35% had no formal or on-the?job training.
 Seventy-one health facilities had no routinely available malaria diagnostic services; 55 (77.5%) of these, referred patients to other health facilities where there is availability of malaria diagnosis, 6 (8.5%) prepared microscopy slides and sent to other laboratories for malaria examination, and 10 (14.1%) took no diagnostic action.
Seventy-one health facilities had no routinely available malaria diagnostic services; 55 (77.5%) of these, referred patients to other health facilities where there is availability of malaria diagnosis, 6 (8.5%) prepared microscopy slides and sent to other laboratories for malaria examination, and 10 (14.1%) took no diagnostic action.
Using outpatient and laboratory statistics for the 3 months preceding the survey we found that the overall prevalence of clinically diagnosed malaria in the outpatient clinics was 70.3%. The malaria slide positivity rate was 78.8%. An antimalarial drug was prescribed on average 1.2 times out of every 10 negative malaria test results.
A good pool of human resources exist in private health facilities and their capacity needs to be built on malaria diagnosis especially mRDT for non laboratory staff. Quality of malaria microscopy could be improved with re?training of Laboratory Scientists.
A policy framework that provides for access to quality malaria diagnostic services and commodities while also creating an enabling environment for use of diagnostic results is needed to support the massive scale up of campaigns for malaria control towards elimination
[The contents of the poster/presentation are the responsibility of the Malaria Action Program for States Nigeria and do not necessarily reflect the views of the US Government.]
ITNs Bill Brieger | 28 Nov 2014
Is Mosquito Net Mis-Use Exaggerated
Health Officials commonly berate community members for misusing insecticide treated nets (ITNs) given out during malaria prevention campaigns and programs. Villagers are blamed for doing everything from using nets to catch or dry fish, protect crops or poultry, make football goals and cover their market goods.
For example, The Nairobi Star of 12 March 2012 reported that health officials in Nyanza, Kenya were disturbed that people were using their ITNs to protect their gardens from pests and their kitchens from rodents. The officials threatened to prosecute anyone misusing their nets.
 Likewise the Lusaka Times published a story on 10 July 2011 that ITNs were being misused to made wedding dresses/veils and for fishing. “North-Western Province Minister Daniel Kalenga has directed District Commissioners in the province to report any misuse of Insecticide Treated mosquito Nets (ITNs) to the police as it is an offense under the public health Act.” A similar story appeared in April 2014.
Likewise the Lusaka Times published a story on 10 July 2011 that ITNs were being misused to made wedding dresses/veils and for fishing. “North-Western Province Minister Daniel Kalenga has directed District Commissioners in the province to report any misuse of Insecticide Treated mosquito Nets (ITNs) to the police as it is an offense under the public health Act.” A similar story appeared in April 2014.
There is some theoretical logic to net misuse. Keita Honjo and colleagues concluded from a modeling exercise that, “ITN use for malaria protection can be thwarted in settings of extreme poverty, where an increase in labour productivity by an alternative ITN use can offset the perceived benefits of avoiding malaria infection.”
One has often suspected these challenges to net use border on myth at times. Eisele and colleagues leveled the following critique against the media: “There are a number of potentially damaging misconceptions about insecticide-treated mosquito nets (ITNs) in Africa that have been propagated in media
reports, almost all of which are based on anecdotal accounts.”
Therefore, we were quite interested to learn of a newly published study that analyzed ITN use with “Data from 14 sub-national post-campaign surveys conducted in Ghana, Senegal, Nigeria (10 states), and Uganda between 2009 and 2012 (that) were pooled,” to find out what happens to “lost” nets.
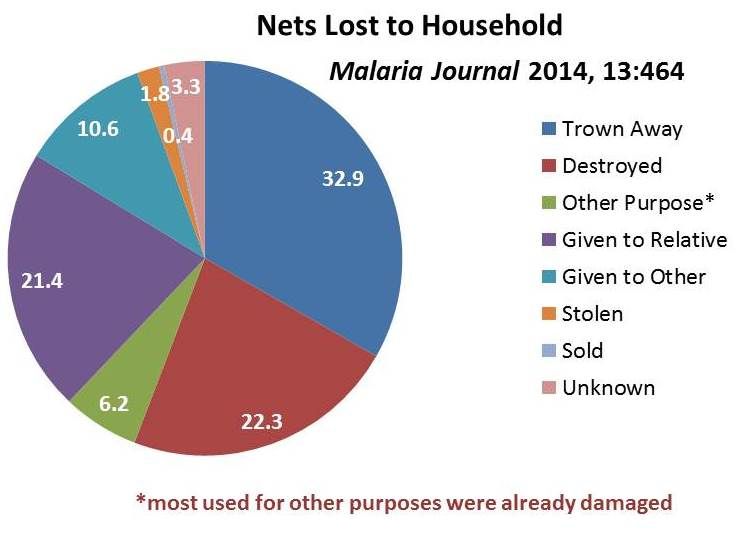 While 16% of 25,447 nets were no longer serving their original purpose, only 6.2% of those were being used for another purpose. Importantly, over 3/4 of those had been damaged prior to re-purposing. The fact that the major reason why nets left the household was because they were given to other users (e.g. relatives) implied that better assessment of community need for nets was required.
While 16% of 25,447 nets were no longer serving their original purpose, only 6.2% of those were being used for another purpose. Importantly, over 3/4 of those had been damaged prior to re-purposing. The fact that the major reason why nets left the household was because they were given to other users (e.g. relatives) implied that better assessment of community need for nets was required.
In fact re-purposing of old nets may be a natural response to failure of health agencies to devise an environmentally safe way of disposing of ITNs that have passed their natural lifetimes. Therefore WHO recommends that National malaria control and elimination programs should work with national environment authorities work together to ensure proper removal of old nets no longer in use to prevent malaria.
This reassuring article certainly takes precedence over newspaper reports of misuse, but we should still be on the look out for net use problems. A classic example appeared in Malaria Journal in 2008 documenting with data and photos the use of ITNs to dry fish along the shores of Lake Victoria. In that case the root cause of the problem was lack of coordination among agencies such that the villages were supplied more nets than they needed. This appears to have been a one-of-a-kind study.
What is more likely to happen, it seems is that households acquire their nets but for various reasons do not always hang them, as was the case with nearly 30% of recipients in a small study in Rivers State, Nigeria. Malaria control programs need to pay more attention to helping people actually hang and use their nets correctly and regularly than simply being satisfied with reporting the numbers distributed.
Treatment Bill Brieger | 19 Nov 2014
Understanding Child Illness and Malaria Care Seeking in Bauchi State Nigeria
Bright Orji, Masduk Abdulkarim, William Sambisa, Amos Paul Bassi, Solomon Thliza, and William Brieger shares a poster at the 2014 American Public Health Association Annual Meeting that focuses on a baseline study for child illness interventions under the USAID Targeted States High Impact Project (TSHIP). The authors work with John Snow International and Jhpiego. The poster abstract follows:
 Seeking of appropriate and quality care for childhood illnesses is a major challenge in much of Africa including Bauchi State, Nigeria. In advance of an intervention to improve available care in the most common points of service (POS), government primary health care centers (PHCs) and patent medicine vendors (PMV), a survey was done of child caregivers in four districts concerning responses to febrile illness, suspected malaria, acute respiratory disease and diarrhea.
Seeking of appropriate and quality care for childhood illnesses is a major challenge in much of Africa including Bauchi State, Nigeria. In advance of an intervention to improve available care in the most common points of service (POS), government primary health care centers (PHCs) and patent medicine vendors (PMV), a survey was done of child caregivers in four districts concerning responses to febrile illness, suspected malaria, acute respiratory disease and diarrhea.
The ethical review committee in the Bauchi State Ministry of Health approved of the study. A total of 3077 children below the age of five were identified in the households sampled.
 Their mothers, fathers or other caregivers consented and were interviewed. Among the children 74% had any Illness, 57% had fever, 26% had cough, and 15% had diarrhoea. Only 8.7% of 1186 febrile children had their blood tested. Care seeking from PMVs varied from 45% with fever, 40% with cough to 36% with diarrhoea.
Their mothers, fathers or other caregivers consented and were interviewed. Among the children 74% had any Illness, 57% had fever, 26% had cough, and 15% had diarrhoea. Only 8.7% of 1186 febrile children had their blood tested. Care seeking from PMVs varied from 45% with fever, 40% with cough to 36% with diarrhoea.
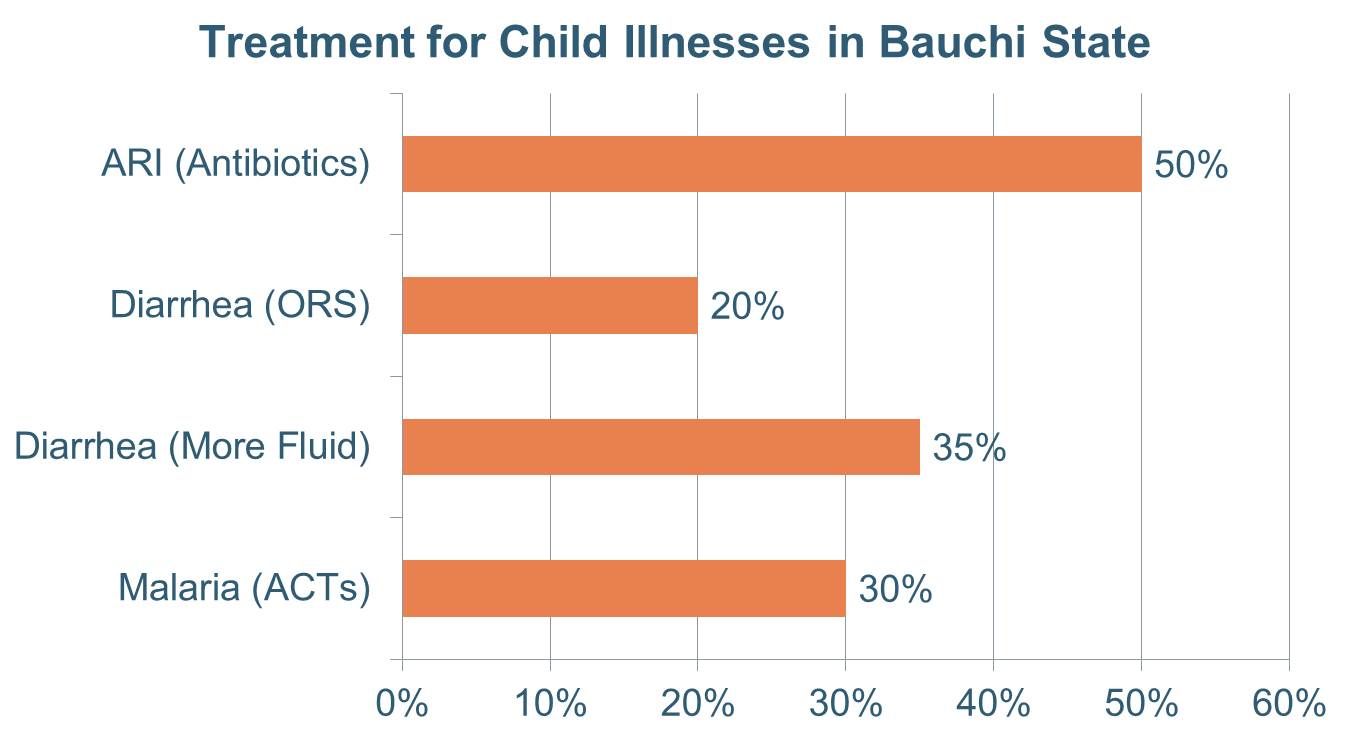
 Care from public sector POS varied from 26-33%. Treatment that might be considered ‘appropriate’ for each also varied with 30% receiving antimalarial drugs for suspected malaria, 20% getting oral rehydration solution for diarrhoea and 50% being given an antibiotic for a suspected acute respiratory illness.
Care from public sector POS varied from 26-33%. Treatment that might be considered ‘appropriate’ for each also varied with 30% receiving antimalarial drugs for suspected malaria, 20% getting oral rehydration solution for diarrhoea and 50% being given an antibiotic for a suspected acute respiratory illness.
The results show that providing quality case management with appropriate commodities through PHCs and PMVs can improve the illness care of a majority of children in Bauchi State, and interventions are currently being planned to do this.
Severe Malaria &Treatment Bill Brieger | 07 Nov 2014
Severe malaria case management practices in selected states in Nigeria: Need for urgent intervention
At the recently concluded American Society of Tropical Medicine and Hygiene 2014 Annual Meeting, USAID’s MAPS Project presented a poster on severe malaria in Nigeria. The authors, Yetunde Oke, Banji Ipadeola, Bolatito Aiyenigba, Grace Nwankwo, Justice Adaji, Olatunde Olotu, Aniefiok Akpasa, and Abba Umar, share their findings below.
![]() Severe malaria is a life threatening medical condition that requires emergency interventions including prompt and effective treatment to prevent death (WHO 2000). The AQUAMAT* study showed a relative reduction in mortality of 22.5% with use of parenteral artesunate compared to quinine in the management of severe P. falciparum malaria and the Nigeria national policy on malaria diagnosis and treatment has been revised based on this evidence.
Severe malaria is a life threatening medical condition that requires emergency interventions including prompt and effective treatment to prevent death (WHO 2000). The AQUAMAT* study showed a relative reduction in mortality of 22.5% with use of parenteral artesunate compared to quinine in the management of severe P. falciparum malaria and the Nigeria national policy on malaria diagnosis and treatment has been revised based on this evidence.
However, implementation of this guideline is still a challenge. The goal of this study was to determine baseline capacity and management practices for severe malaria in selected secondary health facilities in Nigeria with the aim of designing interventions to address specific gaps identified.
A cross?sectional study was conducted to assess twenty?four secondary public health facilities in three states (Benue, Kogi and Oyo States) in Nigeria in August 2013. Data on the capacity of health care providers; malaria services provided at different service delivery points (three months preceding the survey).
Medical supplies were collected using modified WHO severe malaria assessment tools. Data entry was done using the SPSS software programme and analysis done with STATA version 10.0.
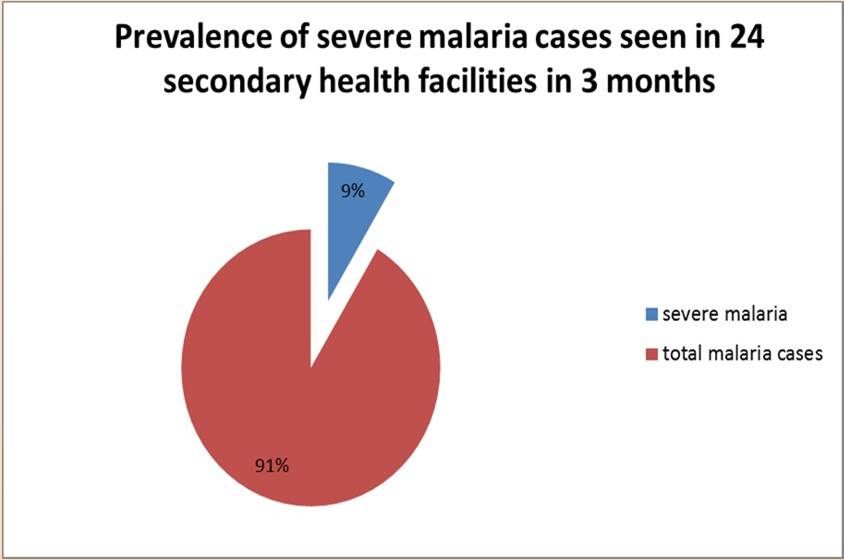 Total number of confirmed malaria cases reported in the three states over the three months preceding the assessment was 18, 695 and diagnosis of severe malaria was made in 8.6% of the total malaria cases. Out of the severe malaria cases, 75.9% were discharged, 3.8% referred and 1.5% died.
Total number of confirmed malaria cases reported in the three states over the three months preceding the assessment was 18, 695 and diagnosis of severe malaria was made in 8.6% of the total malaria cases. Out of the severe malaria cases, 75.9% were discharged, 3.8% referred and 1.5% died.
Fifty per cent of the health care providers had attended training on malaria case management 12 months preceding the survey. The majority of providers managed severe malaria with injectable artemether (45.8%), quinine (37.5%) compared with artesunate (29.2%).
 Most of the health facilities (95.8%) practiced parasite-based diagnosis of malaria but only (29.2%) monitored the parasite clearance of patients with severe malaria. 70% of the facilities did not have basic supplies for ancillary management of severe malaria. 66.7% and 30% of the health facilities experienced stock?out of parenteral artesunate and parenteral quinine respectively in the previous three months.
Most of the health facilities (95.8%) practiced parasite-based diagnosis of malaria but only (29.2%) monitored the parasite clearance of patients with severe malaria. 70% of the facilities did not have basic supplies for ancillary management of severe malaria. 66.7% and 30% of the health facilities experienced stock?out of parenteral artesunate and parenteral quinine respectively in the previous three months.
Health system strengthening with emphasis on capacity building of health care providers, medical commodity security and improvement in supportive/ancillary management of severe malaria is needed to reduce the mortality attributable to severe malaria.
Health Systems &IPTp &Malaria in Pregnancy Bill Brieger | 07 Nov 2014
Health Systems Strengthening: Achieving Lasting Results for IPTp
 At the Call to Action for Intermittent Preventive Treatment of Malaria in Pregnancy (IPTp) during the just concluded American Society of Tropical Medicine and Hygiene Annual Meeting, Elaine Roman of Jhpiego/MCSP advocated for strengthened health systems as a basic approach to enhancing IPTp coverage. Below is a summary of her remarks.
At the Call to Action for Intermittent Preventive Treatment of Malaria in Pregnancy (IPTp) during the just concluded American Society of Tropical Medicine and Hygiene Annual Meeting, Elaine Roman of Jhpiego/MCSP advocated for strengthened health systems as a basic approach to enhancing IPTp coverage. Below is a summary of her remarks.
Why should we strengthen the Health System? Addressing the health system at all levels leads to improved outcomes and comprehensive coverage. Increasing IPTp uptake requires strengthening antenatal care (ANC) and other components of the health system.
ANC within a strong health system provides an opportunity to improve the health of pregnant women and their newborns. Malaria in pregnancy (MIP) is a maternal and newborn health issue. When health systems are weak, there is greater likelihood of negative consequences on mother and newborn.
 Improving Health Systems for enhanced IPTp addresses the following health systems components:
Improving Health Systems for enhanced IPTp addresses the following health systems components:
- Integration: Reproductive Health Programs and National Malaria Control Programs
- Policies and Guidelines: Consistency across national documents
- Capacity Development: Bother In-Service Training and Pre-Service Education
- Quality Assurance: Linked directly with support supervision
- Community Engagement: Promotion of early ANC and Promotion of IPTp uptake
- Commodities: Ensuring availability at ANC of sulfadoxine-pyrimethamine (SP) and supplies, as well as long-lasting insecticide-treated bed nets
- Monitoring and Evaluation: Facility-level data collection and Data for decision- making
- Finance: Sustained and comprehensive services
 Systems strengthening works. Strengthened Health Systems for IPTp in Kenya resulted from community engagement, training, supervision: leading to IPTp1 coverage of 91.6% and IPTp2 (or more doses) coverage at 61.1%.
Systems strengthening works. Strengthened Health Systems for IPTp in Kenya resulted from community engagement, training, supervision: leading to IPTp1 coverage of 91.6% and IPTp2 (or more doses) coverage at 61.1%.
In Ghana, Capacity development, commodities, community engagement improvements resulted in IPTp2 (or more doses) coverage of 44% to 65%
In Zambia development of clear policy, integrated training, supervision led to IPTp2 (or more doses) coverage increasing from 63% in 2007 to 72% in 2012.
Moving forward we must advocate for strengthening health systems that will lead to increased IPTp uptake and lasting gains. We must focus on ANC, complemented by efforts at community and policy levels. Finally we must address each health system component, based on country context.
Community &Health Systems &Treatment Bill Brieger | 05 Nov 2014
Expanding Health Ministry Capacity to Deliver Malaria and Other Health Commodities at the Community Level in Nigerian States
Bright Orji of Jhpiego‘s Nigeria office presents a poster at the American Society of Tropical Medicine and Hygiene 2014 Annual Meeting at noon on 5th November. The poster represents Jhpiego’s technical assistance provided to seven Nigerian States as part the World Bank Malaria Booster Program. The abstract follows:
 The highly participative process of community directed interventions (CDI) was first pioneered in 1996 by the African Program for Onchocerciasis Control for the delivery of ivermectin. CDI was further tested and found effective in delivering other health commodities.
The highly participative process of community directed interventions (CDI) was first pioneered in 1996 by the African Program for Onchocerciasis Control for the delivery of ivermectin. CDI was further tested and found effective in delivering other health commodities.
In 2007 Jhpiego began a proof of concept project in Akwa Ibom State, Nigeria and learned that CDI could be a useful vehicle for increasing access to and coverage of malaria in pregnancy interventions. Building on this success, Jhpiego expanded this work to include integrated community case management of malaria, diarrhoea and pneumonia. through community led efforts.
 The World Bank Malaria Booster Program, observing Jhpiego’s efforts in Akwa Ibom State, asked the Nigeria National Malaria Control Program to enlist Jhpiego’s help in building the capacity of seven State Ministries of Health (MOH) to organize CDI for what was termed the malaria plus package consisting of community case management and health promotion activities. The scale-up process started with workshops for state CDI implementation teams consisting of staff from malaria control and primary health care in the MOHs.
The World Bank Malaria Booster Program, observing Jhpiego’s efforts in Akwa Ibom State, asked the Nigeria National Malaria Control Program to enlist Jhpiego’s help in building the capacity of seven State Ministries of Health (MOH) to organize CDI for what was termed the malaria plus package consisting of community case management and health promotion activities. The scale-up process started with workshops for state CDI implementation teams consisting of staff from malaria control and primary health care in the MOHs.
 Then these state teams developed their own intervention packages and organized workshops for local government teams, who in turn trained staff from their front line health facilities. These facility staff mobilized communities in their facility catchment areas (wards) to select volunteers for training on the CDI process and intervention package.
Then these state teams developed their own intervention packages and organized workshops for local government teams, who in turn trained staff from their front line health facilities. These facility staff mobilized communities in their facility catchment areas (wards) to select volunteers for training on the CDI process and intervention package.
Although technical assistance was provided to each state, challenges arose including commodity supplies and coordination among different program units within the state MOHs. In conclusion, state teams can train local government teams, ultimately cascading CDI to the community in order to scale up maternal and child health interventions.
IPTp &Malaria in Pregnancy &Private Sector Bill Brieger | 04 Nov 2014
A role for the private sector increasing uptake of intermittent preventive treatment for malaria in pregnancy in Kenya
Jhpiego staff will again present a poster at the Tuesday noon (Nov 4) session of the American Society of Tropical Medicine and Hygiene Annual Meeting. Augustine M. Ngindu, Muthoni M. Kariuki, Sanyu Kigondu, Johnstone Akatu, Isaac M. Malonza, with support from USAID’s Maternal and Child Health Integrated Project (MCHIP) will share experiences with a poster titled, “Improving maternal and neonatal health: Complementary role of the private sector increasing uptake of intermittent preventive treatment for malaria in pregnancy in Kenya.” The abstract is provided below.
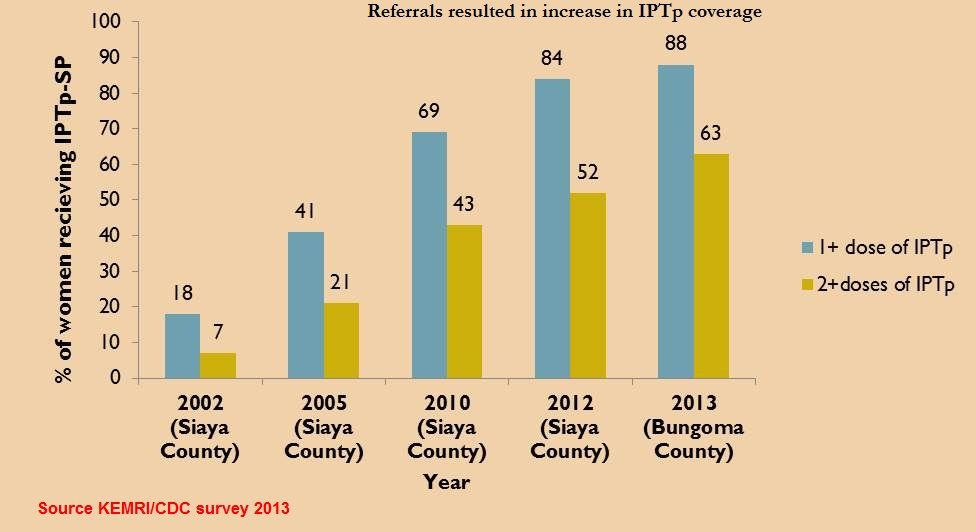
 Malaria in pregnancy (MIP) is associated with poor pregnancy outcomes including maternal anaemia, intrauterine growth retardation and low birth weight. Kenya changed its policy on intermittent preventive treatment using Sulfadoxine Pyrimethamine (IPTp-SP) in 1998. However, IPTp coverage rates have remained low: 4% in 2003, 14% in 2007, 15% in 2008 and 25 % in 2010.
Malaria in pregnancy (MIP) is associated with poor pregnancy outcomes including maternal anaemia, intrauterine growth retardation and low birth weight. Kenya changed its policy on intermittent preventive treatment using Sulfadoxine Pyrimethamine (IPTp-SP) in 1998. However, IPTp coverage rates have remained low: 4% in 2003, 14% in 2007, 15% in 2008 and 25 % in 2010.
To increase the coverage rate, MCHIP supported malaria control and reproductive health divisions of the ministry of health, first to harmonize knowledge among service providers on provision of IPTp-SP in 2011, and second to train community health workers (CHWs) on sensitization of pregnant women to start early antenatal care (ANC) attendance in 2012.
 A community survey conducted in 2013 showed a significant increase in the proportion of pregnant women receiving two or more IPTp doses from 25% to 63%, the highest increase in IPTp uptake since 1998. Following the successful scale up of IPTp, one sub-county conducted an assessment of its health facilities to determine quality of data on ANC clients accessing IPTp-SP.
A community survey conducted in 2013 showed a significant increase in the proportion of pregnant women receiving two or more IPTp doses from 25% to 63%, the highest increase in IPTp uptake since 1998. Following the successful scale up of IPTp, one sub-county conducted an assessment of its health facilities to determine quality of data on ANC clients accessing IPTp-SP.
A total of 15 (58%) out all 26 health facilities in the sub-county (public – 6 out of 8, faith-based – 2 out 3 and private – 7 out of 15) were selected. Data on new ANC clients, revisits and IPTp doses given was collected from the ANC registers.
Among th e assessed health facilities 13 (87%) out of the 15 were registering new ANC cases, revisits and provided IPTp-SP (public 6, faith based 2, private 5. One private clinic provided ANC services to revisits and IPTp2 doses only after the clients had been registered in public facilities, the second did not offer ANC services.
e assessed health facilities 13 (87%) out of the 15 were registering new ANC cases, revisits and provided IPTp-SP (public 6, faith based 2, private 5. One private clinic provided ANC services to revisits and IPTp2 doses only after the clients had been registered in public facilities, the second did not offer ANC services.
In 2013 the government declared provision of free maternity services in public facilities but ANC clients have continued to utilize services from the private sector. This is an indication of the untapped potential in the private sector in increasing access to high impact interventions and importance of supporting the sector by all partners to provide these interventions.
Such complementary efforts if implemented will not only result in enabling the country to move towards achievement of set targets but also improve pregnancy outcomes through reduction in effects of
malaria in pregnancy.
IPTp &Malaria in Pregnancy Bill Brieger | 03 Nov 2014
Call to Action at ASTMH – Intermittent Preventive Treatment of Malaria in Pregnancy
If you are interested in preventing malaria in pregnancy (MIP) join a special symposium at the American Society of Tropical Medicine and Hygiene 2014 Annual Meeting on Wednesday afternoon/evening, November 5th. The seminar is organized by the Malaria in Pregnancy Consortium and the Roll Back Malaria Malaria in Pregnancy Working Group, with support from Medicines for Malaria Venture (MMV) and London School of Hygiene and Tropical Medicine (LSHTM). The agenda can be found below.
SESSION 1 Current coverage and delivery of IPTp 3:45 – 4:15
- Welcome Koki Agarwal, Roll Back Malaria MIP Working Group, Jhpiego / Maternal and Child Survival Program
- Current coverage estimates of IPTp Annemieke van Eijk, Liverpool School of Tropical Medicine
- Factors affecting delivery of IPTp: Findings from quantitative and qualitative studies in Mali and Kenya, Jayne Webster: London School of Hygiene & Tropical Medicine
 SESSION 2 MOVING FORWARD: OPPORTUNITIES TO SCALE UP IPTp: 4:15 – 5.15
SESSION 2 MOVING FORWARD: OPPORTUNITIES TO SCALE UP IPTp: 4:15 – 5.15
- IPTp and WHO’s Global Malaria Programme, Pedro Alonso, Global Malaria Programme of the World, Health Organization
- Interventions to improve uptake of IPTp in Ghana, Harry Tagbor, Kwame Nkrumah University of Science & Technology
- Studies of cost-effectiveness of IPTp-SP: IPTp-SP2 vs. placebo in Mozambique and a meta analysis of IPTp-SP3 + vs. SP2 in a range of African settings, Elisa Sicuri Barcelona Centre for International Health Research
- Can acceptability be enhanced? Findings from quantitative and qualitative studies on IPTp against malaria and curable STIs/RTIs, Matthew Chico, London School of Hygiene & Tropical Medicine
- Delivering IPTp in the antenatal care platform, Kate Mitchell, Harvard School of Public Health/ Maternal, Health Task Force
- Health systems strengthening: Achieving lasting results for IPTp, Elaine Roman. Jhpiego / Maternal and Child Health Program
SESSION 3 Call to Action: 5:15 – 6:00
- Defining the Call to Action (group facilitation) – Koki Agarwal, Roll Back Malaria MIP Working Group, Jhpiego / Maternal and Child Survival Program, Intermittent Preventive Treatment of Malaria in Pregnancy
Community &IPTp Bill Brieger | 03 Nov 2014
Prevention of Malaria in Pregnancy with Community Health Volunteers in Kenya: Jhpiego at ASTMH
 Augustine M. Ngindu of Jhpiego’s USAID-MCHIP Project in Nairobi, Kenya will present a poster entitled, “Prevention of Malaria in Pregnancy: Community Health Volunteers (CHVs) promote community-based activities to increase uptake of Intermittent Preventive Treatment of malaria in pregnancy (IPTp) in Kenya,” at the ASTMH Annual Meeting at noon on Monday 3 October. Below is the abstract – stop by the session to learn more.
Augustine M. Ngindu of Jhpiego’s USAID-MCHIP Project in Nairobi, Kenya will present a poster entitled, “Prevention of Malaria in Pregnancy: Community Health Volunteers (CHVs) promote community-based activities to increase uptake of Intermittent Preventive Treatment of malaria in pregnancy (IPTp) in Kenya,” at the ASTMH Annual Meeting at noon on Monday 3 October. Below is the abstract – stop by the session to learn more.
Malaria in pregnancy is associated with poor pregnancy outcomes including maternal anaemia, miscarriages and intrauterine growth retardation. In an effort to increase IPTp coverage, Kenya is implementing the community strategy by using community health volunteers (CHVs) to promote community-based activities to increase uptake of malaria in pregnancy interventions (MIP).
 The CHVs visit each household every month to register new pregnant women, collect data from existing pregnant women including last IPTp dose taken and gestation, sensitize them to continue ANC visits and refer late starters and defaulters of scheduled ANC visits.
The CHVs visit each household every month to register new pregnant women, collect data from existing pregnant women including last IPTp dose taken and gestation, sensitize them to continue ANC visits and refer late starters and defaulters of scheduled ANC visits.
In Bungoma sub-county with a catchment population of 169,000, 382 CHVs from 14 community units identified a total of 4,925 (95%) out of an expected 5,092 pregnant women and followed them up between February to April 2014.
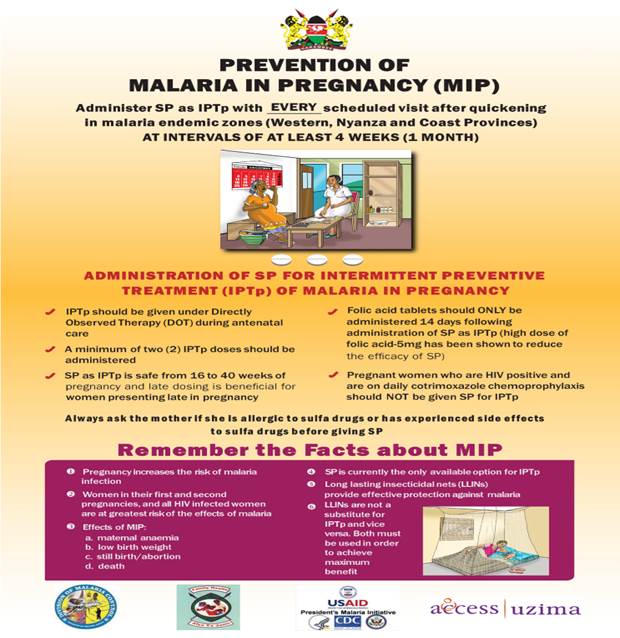
In Kenya the recommended time for starting IPTp is from weeks of pregnancy or after quickening.
 Results showed that among the registered pregnant women 92% had taken at least IPTp1 and 61% IPTp2 doses respectively. IPTp doses taken by weeks of pregnancy showed that 1.3% had accessed IPTp by 16 weeks of pregnancy, 8.6% between 16-20 weeks, 4.7% between 21-25 weeks, 5.7% between 26-30 weeks, 6.5% between 31-35 weeks and 3.7 % between 36-40 weeks.
Results showed that among the registered pregnant women 92% had taken at least IPTp1 and 61% IPTp2 doses respectively. IPTp doses taken by weeks of pregnancy showed that 1.3% had accessed IPTp by 16 weeks of pregnancy, 8.6% between 16-20 weeks, 4.7% between 21-25 weeks, 5.7% between 26-30 weeks, 6.5% between 31-35 weeks and 3.7 % between 36-40 weeks.
 However, 1.5% had not started IPTp at 40 weeks of pregnancy. The data further showed that among those who started IPTp early 1% completed 7 IPTp doses at 40 weeks of pregnancy.
However, 1.5% had not started IPTp at 40 weeks of pregnancy. The data further showed that among those who started IPTp early 1% completed 7 IPTp doses at 40 weeks of pregnancy.
CHVs can be used to effectively promote community-based activities including collection of data on the number of IPTp doses taken during pregnancy, which is a good indicator of the proportion of pregnant women protected against the adverse effects of malaria during pregnancy. This practice if scaled up can serve as an alternative method of monitoring coverage rates of interventions without waiting for the 3-5 year community survey data
Human Resources &Training &Treatment Bill Brieger | 03 Nov 2014
Inspiring Quality in Pre-Service Education on Malaria in Tanzania: Jhpiego at ASTMH
Monday at noon (3 October 2014) at the American Society for Tropical Medicine and Hygiene Annual Meeting in New Orleans, Jhpiego will be presenting two posters. Grace Qorro of Jhpiego’s Tanzania office has one entitled: #Quality Inspired Project – A Key to Achieving Results with Malaria Interventions.” Her abstract is shared below.
 With an aim to accelerate malaria case management, Tanzania Ministry of Health and Social Welfare (MoHSW) is strengthening its pre-service education program to ensure graduates have the right knowledge and skills to diagnose and treat malaria. Investment in pre-service education lessens the burden on in-service training since those entering the workforce will have the knowledge and skills they need to provide.
With an aim to accelerate malaria case management, Tanzania Ministry of Health and Social Welfare (MoHSW) is strengthening its pre-service education program to ensure graduates have the right knowledge and skills to diagnose and treat malaria. Investment in pre-service education lessens the burden on in-service training since those entering the workforce will have the knowledge and skills they need to provide.
 Jhpiego, through MAISHA (Mothers And Infants Safe, Healthy and Alive) program, provided technical assistance to the MoHSW to help develop a pre-service malaria case management-updates Learning Resource Package (LRP), which includes: Facilitator’s Manual, Participant’s Manual, Activity Worksheets and Training Modules addenda.
Jhpiego, through MAISHA (Mothers And Infants Safe, Healthy and Alive) program, provided technical assistance to the MoHSW to help develop a pre-service malaria case management-updates Learning Resource Package (LRP), which includes: Facilitator’s Manual, Participant’s Manual, Activity Worksheets and Training Modules addenda.
 The LRP was developed based on national malaria policy, guidelines and in-service training materials; it is taught using job aids, power point presentations, video demonstration and numerous case scenarios which reflect what actually happens in real life situations at service delivery points. The LRP aims at reinforcing appropriate practices for care of malaria patients and management of commodities with emphasis on parasite-based diagnosis and compliance to results, proper recording and reporting; and management of malaria in special situations and groups.
The LRP was developed based on national malaria policy, guidelines and in-service training materials; it is taught using job aids, power point presentations, video demonstration and numerous case scenarios which reflect what actually happens in real life situations at service delivery points. The LRP aims at reinforcing appropriate practices for care of malaria patients and management of commodities with emphasis on parasite-based diagnosis and compliance to results, proper recording and reporting; and management of malaria in special situations and groups.
 The training package is well organized with laboratory and medical supplies which gives each participant an opportunity for hands-on activity to acquire and strengthen their skills. Checklists to guide Quality Assurance/Quality Improvement (QA/QI) processes have been included in these training materials.
The training package is well organized with laboratory and medical supplies which gives each participant an opportunity for hands-on activity to acquire and strengthen their skills. Checklists to guide Quality Assurance/Quality Improvement (QA/QI) processes have been included in these training materials.
The project successfully provided competence-based orientation on malaria case management updates to 210 medical instructors. Annually, it reaches more than 4,000 students from eight Zonal Health Resource Centers and 480 students from Medical Universities.
There is a need to incorporate the addenda developed into these training modules for easy use. In the near future, clinical skills-mentorship will be conducted in selected schools using the nationally approved QA/QI checklists.