Capacity Building &Climate &Elimination &Malaria &Migration &PAHO &Refugee &Treatment &Urban Bill Brieger | 17 May 2025
Malaria in the Americas: Colombia and the Challenge of Refugees
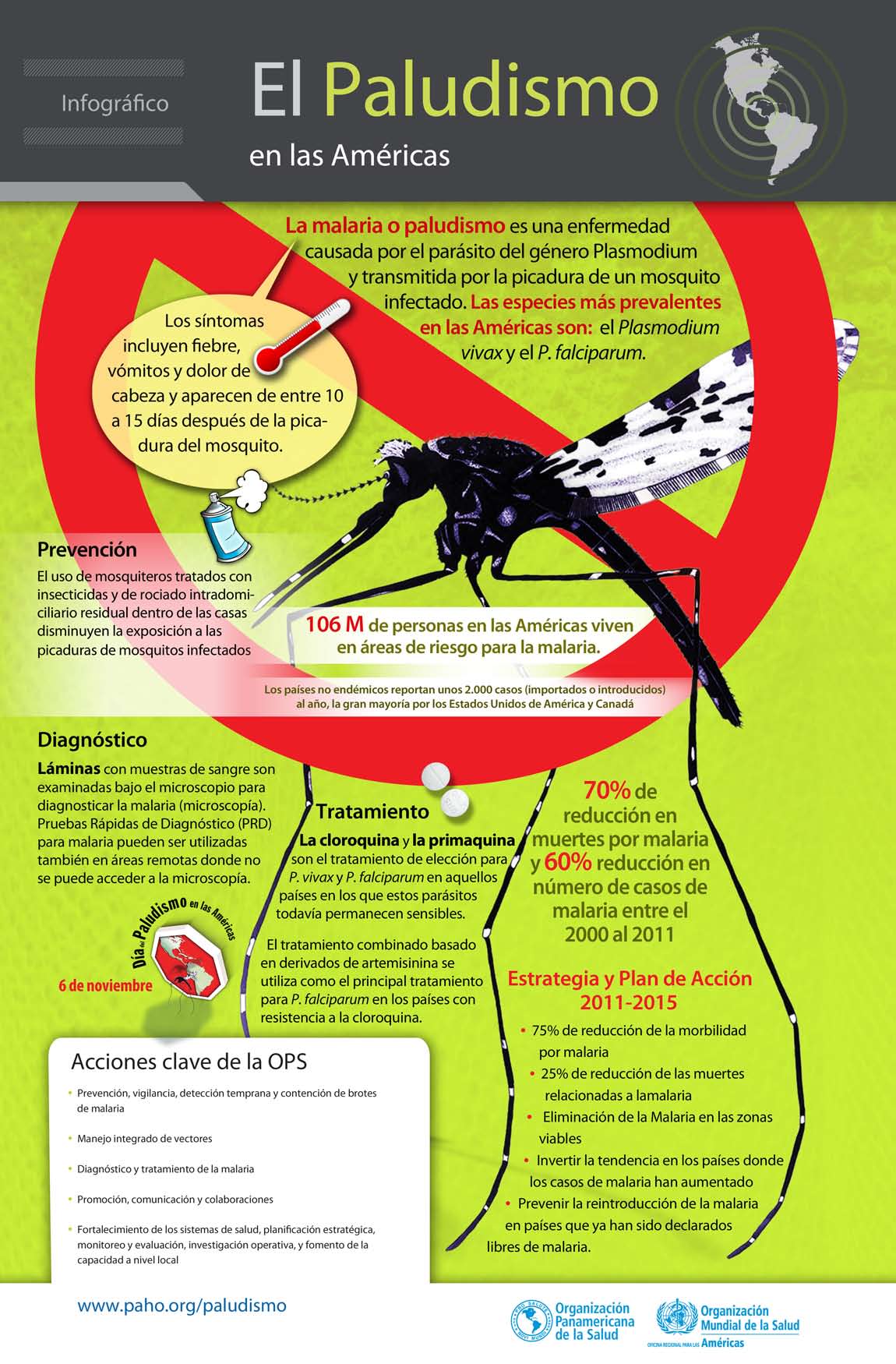
Malaria is one of the more than 30 diseases and conditions included in the Elimination Initiative and targeted for elimination in the Region of the Americas by 2030. Colombia provides a useful example of the progress and challenges. Of the over 72,000 reported malaria cases in 2022, About 61% were caused by P. vivax, 38% by P. falciparum, and 1% were mixed. The Ministry of Health explains that unlike other South American countries, the most malaria endemic regions are not in the Amazonian forest but lie in the northwest of the country in the Pacific coastal forests, populated by Afro-Colombian and indigenous communities.

The Ministry also notes that malaria transmission is characterized by the presence of epidemic cycles that occur every 2 to 7 years, related to the occurrence of the Niño-Southern Oscillation phenomenon. Malaria control is particularly challenging in provinces where illegal mining, logging and the growing of illicit crops are conducted. The World Malaria Report of 2023 traced annual malaria trends in Colombia and showed a peak in 2018-19 with a reduction in subsequent years that points toward efforts at elimination
The International Rescue Committee identifies a particular challenge for Colombia. At least 4 million Venezuelans have crossed the border to seek refuge, and that number continues to rise. Venezuela continues to be plagued by malnutrition, lack of medical supplies, high homicide rates and the spread of diseases such as malaria and measles. Since outbreaks of measles, diphtheria and malaria have been reported across Venezuela, it would be surprising that refugees would enter Colombia with malaria infections.

A study of malaria among migrants in a university hospital in Colombia during 2018 found that imported malaria has increased in Colombia since 2015 and has been attributed to migrants coming from Venezuela. To address the challenge, we need to know where are the refugees? Regular migration is usually located in the main cities and in places where tourism or the mining industry are active. Many of the destinations are in areas where malaria is not endemic, onward transmission would be less likely. Unfortunately, the following migration destinations overlap with malaria transmission: Nariño, Antioquia, Cundinamarca, Cauca, and Chocó, such that those migrants can acquire new infections.
The challenge is that as Colombia makes progress toward eliminating malaria, it still must maintain high capacity to tackle imported cases as well as new cases among a particularly vulnerable refugee population.
Equity &Gender &Health Systems &Migration &Nomadic People &poverty Bill Brieger | 05 Mar 2021
Nomads in Mali Face Barriers to Health Care
We are sharing the abstract of a just published article by Moussa Sangare and colleagues entitled, “Factors hindering health care delivery in nomadic communities: a cross-sectional study in Timbuktu, Mali,” that appears in BMC Public Health. As COVID-19 has been disrupting health services generally, we need greater awareness of the serious barriers faced by more vulnerable populations even in better times.
 Background: In Mali, nomadic populations are spread over one third of the territory. Their lifestyle, characterized by constant mobility, excludes them from, or at best places them at the edge of, health delivery services. This study aimed to describe nomadic populations’ characteristics, determine their perception on the current health services, and identify issues associated with community-based health interventions.
Background: In Mali, nomadic populations are spread over one third of the territory. Their lifestyle, characterized by constant mobility, excludes them from, or at best places them at the edge of, health delivery services. This study aimed to describe nomadic populations’ characteristics, determine their perception on the current health services, and identify issues associated with community-based health interventions.
Methods: To develop a better health policy and strategic approaches adapted to nomadic populations, we conducted a cross-sectional study in the region of Timbuktu to describe the difficulties in accessing health services. The study consisted in administering questionnaires to community members in the communes of Ber and Gossi, in the Timbuktu region, to understand their perceptions of health services delivery in their settings.
Results: We interviewed 520 individuals, all members of the nomadic communities of the two study communes. Their median age was 38?years old with extremes ranging from 18 to 86?years old. Their main activities were livestock breeding (27%), housekeeping (26.4%), local trading (11%), farming (6%) and artisans (5.5%). The average distance to the local health center was 40.94?km and 23.19?km respectively in Gossi and Ber. In terms of barriers to access to health care, participants complained mainly about the transportation options (79.4%), the quality of provided services (39.2%) and the high cost of available health services (35.7%). Additionally, more than a quarter of our participants stated that they would not allow themselves to be examined by a health care worker of the opposite gender.
Conclusion: This study shows that nomadic populations do not have access to community-based health interventions. A number of factors were revealed to be important barriers per these communities’ perception including the quality of services, poverty, lifestyle, gender and current health policy strategies in the region. To be successful, future interventions should take these factors into account by adapting policies and methods.
Asymptomatic &Borders &Children &Elimination &Indoor Residual Spraying &IRS &Migration &Mosquitoes &Pharmacovigilence Bill Brieger | 08 Oct 2020
Malaria News Today 2020-10-08: the role of travel, asymptomatic disease and gut microbiome from AJTMH
![]() The American Journal of Tropical Medicine and Hygiene has several new articles on malaria. Abstracts are shared. Two articles examine the role of travel in malaria transmission, both cross-border and rural-urban. Another considers the effect on pharmacokinetics of lumefantrine due to gut bacteria. In Uganda indoor spraying has reduced transmission, but asymptomatic cases remain among children. The challenges of asymptomatic malaria to elimination efforts is also examined in India. Links to the articles are found below.
The American Journal of Tropical Medicine and Hygiene has several new articles on malaria. Abstracts are shared. Two articles examine the role of travel in malaria transmission, both cross-border and rural-urban. Another considers the effect on pharmacokinetics of lumefantrine due to gut bacteria. In Uganda indoor spraying has reduced transmission, but asymptomatic cases remain among children. The challenges of asymptomatic malaria to elimination efforts is also examined in India. Links to the articles are found below.
Evidence of Microbiome–Drug Interaction between the Antimalarial Lumefantrine and Gut Microbiota in Mice
The antimalarial drug lumefantrine exhibits erratic pharmacokinetics. Intersubject variability might be attributed, in part, to differences in gut microbiome–mediated drug metabolism. We assessed lumefantrine disposition in healthy mice stratified by enterotype to explore associations between the gut microbiota and lumefantrine pharmacokinetics. Gut microbiota enterotypes were classified according to abundance and diversity indices from 16S rRNA sequencing. Pharmacokinetic parameters were computed using noncompartmental analysis. Two distinct enterotypes were identified.
Maximal concentration (C max) and total drug exposure measured as the area under the drug concentration–time curve (AUC0–24) differed significantly between the groups. The mean and standard deviation of C max were 660 ± 220 ng/mL versus 390 ± 59 ng/mL (P = 0.02), and AUC0–24 was 9,600 ± 2,800 versus 5,800 ± 810 ng × h/mL (P = 0.01). In healthy mice intragastrically dosed with the antimalarial drug lumefantrine in combination with artemether, lumefantrine exposure was associated with gut bacterial community structure. Studies of xenobiotic–microbiota interactions can inform drug posology and elucidate mechanisms of drug disposition.
Malaria Transmission, Infection, and Disease following Sustained Indoor Residual Spraying of Insecticide in Tororo, Uganda
Tororo, a district in Uganda with historically high malaria transmission intensity, has recently scaled up control interventions, including universal long-lasting insecticidal net distribution in 2013 and 2017, and sustained indoor residual spraying (IRS) of insecticide since December 2014. We describe the burden of malaria in Tororo 5 years following the initiation of IRS. We followed a cohort of 531 participants from 80 randomly selected households in Nagongera subcounty, Tororo district, from October 2017 to October 2019. Mosquitoes were collected every 2 weeks using CDC light traps in all rooms where participants slept, symptomatic malaria was identified by passive surveillance, and microscopic and submicroscopic parasitemia were measured every 4 weeks using active surveillance. Over the 2 years of follow-up, 15,780 female anopheline mosquitos were collected, the majority (98.0%) of which were Anopheles arabiensis.
recently scaled up control interventions, including universal long-lasting insecticidal net distribution in 2013 and 2017, and sustained indoor residual spraying (IRS) of insecticide since December 2014. We describe the burden of malaria in Tororo 5 years following the initiation of IRS. We followed a cohort of 531 participants from 80 randomly selected households in Nagongera subcounty, Tororo district, from October 2017 to October 2019. Mosquitoes were collected every 2 weeks using CDC light traps in all rooms where participants slept, symptomatic malaria was identified by passive surveillance, and microscopic and submicroscopic parasitemia were measured every 4 weeks using active surveillance. Over the 2 years of follow-up, 15,780 female anopheline mosquitos were collected, the majority (98.0%) of which were Anopheles arabiensis.
The daily human biting rate was 2.07, and the annual entomological inoculation rate was 0.43 infective bites/person/year. Only 38 episodes of malaria were diagnosed (incidence 0.04 episodes/person/year), and there were no cases of severe malaria or malarial deaths. The prevalence of microscopic parasitemia was 1.9%, and the combined prevalence of microscopic and submicroscopic parasitemia was 10.4%, each highest in children aged 5–15 years (3.3% and 14.0%, respectively). After 5 years of intensive vector control measures in Tororo, the burden of malaria was reduced to very low transmission levels. However, a significant proportion of the population remained parasitemic, primarily school-aged children with submicroscopic parasitemia, providing a potential reservoir for malaria transmission.
Malaria Diagnosed in an Urban Setting Strongly Associated with Recent Overnight Travel: A Case–Control Study from Kampala, Uganda
Malaria is frequently diagnosed in urban Kampala, despite low transmission intensity. To evaluate the association between recent travel out of Kampala and malaria, we conducted a matched case–control study. Cases were febrile outpatients with a positive malaria test; controls were febrile outpatients with a negative test. For every two cases, five controls were selected, matching on age. Data were collected on recent overnight travel out of Kampala (past 60 days), destination and duration of travel, and behavioral factors, including sleeping under an insecticide-treated net (ITN) during travel. From July to August 2019, 162 cases and 405 controls were enrolled. The locations of residence of cases and controls were similar. More controls were female (62.7% versus 46.3%, P < 0.001). Overall, 158 (27.9%) participants reported recent overnight travel.
Travelers were far more likely to be diagnosed with malaria than those who did not travel (80.4% versus 8.6%, OR 58.9, 95% CI: 23.1–150.1, P < 0.001). Among travelers, traveling to a district not receiving indoor residual spraying of insecticide (OR 35.0, 95% CI: 4.80–254.9, P < 0.001), no ITN use (OR 30.1, 95% CI: 6.37–142.7, P < 0.001), engaging in outdoor activities (OR 22.0, 95% CI: 3.42–141.8, P = 0.001), and age < 16 years (OR 8.36, 95% CI: 2.22–56.2, P = 0.03) were associated with increased odds of malaria. Kampala residents who traveled overnight out of the city were at substantially higher risk of malaria than those who did not travel. For these travelers, personal protection measures, including sleeping under an ITN when traveling, should be advocated.
Prevalence of Asymptomatic Malaria Parasitemia in Odisha, India: A Challenge to Malaria Elimination
The prevalence of malaria in India is decreasing, but it remains a major concern for public health administration. The role of submicroscopic malaria and asymptomatic malaria parasitemia and their persistence is being explored. A cross-sectional survey was conducted in the Kandhamal district of Odisha (India) during May–June 2017. Blood samples were collected from 1897 individuals for screening of asymptomatic parasitemia. Samples were screened using rapid diagnostic tests (RDTs) and examined microscopically for Plasmodium species. Approximately 30% of randomly selected samples (n = 586) were analyzed using real-time PCR (qPCR), and the genetic diversity of Plasmodium falciparum was analyzed.
The prevalence of Plasmodium species among asymptomatic individuals detected using qPCR was 18%, which was significantly higher than that detected by microscopy examination (5.5%) or RDT (7.3%). Of these, 37% had submicroscopic malaria. The species-specific prevalence among asymptomatic malaria-positive cases for P. falciparum, Plasmodium vivax, and mixed infection (P. falciparum and P. vivax) by qPCR was 57%, 29%, and 14%, respectively. The multiplicity of infection was 1.6 and 1.2 for the merozoite surface protein-1 gene (msp1) and (msp2), respectively. Expected heterozygosity was 0.64 and 0.47 for msp1 and msp2, respectively. A significant proportion of the study population, 105/586 (18%), was found to be a reservoir for malaria infection, and identification of this group will help in the development of elimination strategies.
Travel Is a Key Risk Factor for Malaria Transmission in Pre-Elimination Settings in Sub-Saharan Africa: A Review of the Literature and Meta-Analysis
By sustaining transmission or causing malaria outbreaks, imported malaria undermines malaria elimination efforts. Few studies have examined the impact of travel on malaria epidemiology. We conducted a literature review and meta-analysis of studies investigating travel as a risk factor for malaria infection in sub-Saharan Africa using PubMed. We identified 22 studies and calculated a random-effects meta-analysis pooled odds ratio (OR) of 3.77 (95% CI: 2.49–5.70), indicating that travel is a significant risk factor for malaria infection.
Odds ratios were particularly high in urban locations when travel was to rural areas, to more endemic/high transmission areas, and in young children. Although there was substantial heterogeneity in the magnitude of association across the studies, the pooled estimate and directional consistency support travel as an important risk factor for malaria infection.
Diagnosis &Elimination &Funding &IPTp &ITNs &Journalists/Media &Malaria in Pregnancy &Migration &Zero Malaria Bill Brieger | 26 Sep 2020
Malaria News Today 2020-09-26: supporting and strengthening malaria programs
Today’s selection of abstracts and news looks at the role of the media in supporting malaria programs, mass treatment to prevent Imported malaria, problems managing malaria in pregnancy services, malaria research in Mali and health systems strengthening to support malaria control in Guinea. Follow links to read mor details.
GHS calls for media support to eradicate malaria

The media has a role in supporting malaria programs
The Ghana Health Service (GHS) has called on journalists to support the Service to deliver integrated health package through accurate messages towards malaria eradication in the country.“Also, we need your support to set malaria as a national development agenda. This will drive advocacy for political will, increase partnership, availability and accessibility of effective tool for prevention, diagnoses and treatment of malaria in all the vulnerable populations.”
Dr Anthony Adofo Ofosu, the Deputy Director General, GHS, said this at the launch of “Zero malaria starts with me” campaign in Accra. The launch coincided with a sensitisation programme by the African Media and Malaria Research Network (AMMRN), the National Malaria Control Programme and the Speak Up African Organisation. The Deputy Director General said “It is the belief of the GHS that with effective engagement…we will be able to eradicate malaria from the country in the near future.”
Mass radical treatment of a group of foreign workers to mitigate the risk of re-establishment of malaria in Sri Lanka
Following malaria elimination, Sri Lanka was free from indigenous transmission for six consecutive years, until the first introduced case was reported in December 2018. The source of transmission (index case) was a member of a group of 32 migrant workers from India and the location of transmission was their residence reporting a high prevalence of the primary vector for malaria. Despite extensive vector control the situation was highly susceptible to onward transmission if another of the group developed malaria. Therefore, Mass Radical Treatment (MRT) of the group of workers for Plasmodium vivax malaria was undertaken to mitigate this risk.
The workers were screened for malaria by microscopy and RDT, their haemoglobin level assessed, and tested for Glucose 6 phosphate dehydrogenase deficiency (G6PD) using the Care Start RDT and Brewers test prior to treatment with chloroquine (CQ) 25 mg/kg body weight (over three days) and primaquine (PQ, based on G6PD test results) (0.25 mg/kg/day bodyweight for 14 days) following informed consent. All were monitored for adverse events. None of the foreign workers were parasitaemic at baseline screening.
Mass treatment may be an option in prevention of reintroduction settings for groups of migrants who are likely to be carrying latent malaria infections, and resident in areas of high receptivity. However, in the case of Plasmodium vivax and Plasmodium ovale, a more reliable and affordable point-of-care test for G6PD activity would be required. Most countries which are eliminating malaria now are in the tropical zone and face considerable and similar risks of malaria re-introduction due to massive labour migration between them and neighbouring countries. Regional elimination of malaria should be the focus of global strategy if malaria elimination from countries is to be worthwhile and sustainable.
Managing intermittent preventive treatment of malaria in pregnancy challenges: an ethnographic study of two Ghanaian administrative regions
Malaria in pregnancy (MiP) is an important public health problem across sub-Saharan Africa. The package of measures for its control in Ghana in the last 20 years include regular use of long-lasting insecticide-treated bed nets (LLINs), directly-observed administration (DOT) of intermittent preventive treatment with sulfadoxine-pyrimethamine (IPTp-SP) and prompt and effective case management of MiP. Unfortunately, Ghana like other sub-Saharan African countries did not achieve the reset Abuja targets of 100% of pregnant women having access to IPTp and 100% using LLINs by 2015.
This ethnographic study explored how healthcare managers dealt with existing MiP policy implementation challenges and the consequences on IPTp-SP uptake and access to maternal healthcare. Healthcare managers addressed frequent stock-outs of malaria programme drugs and supplies from the National Malaria Control Programme and delayed reimbursement from the NHIS, by instituting co-payment, rationing and prescribing drugs for women to buy from private pharmacies.
 Some clients did not receive the recommended 5?+?doses of SP, others did not obtain LLINs early and some did not obtain treatment for MiP. Healthcare providers felt frustrated whenever they could not provide comprehensive care to women who could not afford comprehensive maternal and MiP care. For Ghana to achieve her goal of controlling MiP, the Ministry of Health and other supporting institutions need to ensure prompt reimbursement of funds, regular supply of programme drugs and medical supplies to public, faith-based and private health facilities.
Some clients did not receive the recommended 5?+?doses of SP, others did not obtain LLINs early and some did not obtain treatment for MiP. Healthcare providers felt frustrated whenever they could not provide comprehensive care to women who could not afford comprehensive maternal and MiP care. For Ghana to achieve her goal of controlling MiP, the Ministry of Health and other supporting institutions need to ensure prompt reimbursement of funds, regular supply of programme drugs and medical supplies to public, faith-based and private health facilities.
Malaria prevention program continuation in Guinea
CRS Guinea is the Principal Recipient (PR) in Malaria prevention program continuation grant by the Global Fund for the new cycle of funding (NFM) (January 2021-December 2023). Community health is a top priority of the Ministry of Health as a primary strategy to increase accessibility and coverage to basic health services. Under the new Global Fund grant, the community health component will be expanded to six districts, in addition to two pilot districts, Kindia and Telimele. CRS will also support coordination with other donors, including World Bank, UNICEF, Gavi, European Union and the Guinea Ministry of Health to implement the national community health strategy in 12 health districts supported by Global Fund malaria project.
The United States and Mali Celebrate 60 Years of Friendship and Partnership
Thirty years ago, our National Institutes of Health created a Malaria Research and Training Center, which is now a component of the International Center for Excellence in Research in Mali. Until today, it serves as a reference center with over 700 Malian scientists and support staff who work on malaria and other infectious diseases. Together, we have dropped malaria prevalence rates in Mali by an astounding 60 percent since 2012.
Climate &COVID-19 &Dengue &Diagnosis &Environment &Invest in Malaria Control &Mapping &mHealth &Migration &Mosquitoes &Nomadic People &Surveillance Bill Brieger | 11 Sep 2020
Malaria News Today 2020-09-11
Today’s news and abstracts look at a variety of issues ranging from overall malaria funding funding needs to the effect of climate change on different types of mosquitoes and the diseases they carry (e.g. malaria vs dengue). We also examine the need for surveillance among nomadic groups and the use of cell phones in a saliva based malaria testing system. Please click the links below to read more on each subject.
Rwanda: Government Needs U.S.$70 Million to Fill Malaria Financing Gap
By Nasra Bishumba: The Government needs $73 million to bridge the funding in the funds needed to fight malaria between 2020 and 2024, The New Times can reveal. The Rwanda National Strategic Plan 2020-2024 to fight malaria drawn up in June this year indicates that although the implementation requires Rwf295bn ($280 million), the government already has funding commitment to the tune of $206.8m (equivalent to 74 per cent).
According to the strategic plan, a copy of which The New Times has seen, this leaves a gap of $73m which it hopes to mobilize from different sources. With these funds, the government is seeking to protect at least 85 per cent of the population with preventive interventions and to work towards promptly testing and treating suspected malaria cases by 2024. To achieve this, the biggest chunk of the funds will be invested in malaria prevention to a tune of $186m, an equivalent of 66 per cent of the entire budget.
Climate Change May Shift Risks of Mosquito-borne Diseases
By Asher Jones: More dengue, less malaria. That may be the future in parts of Africa on a warming planet, depending on where you live. New research says it’s all about which mosquitoes will thrive. And the methods to control one don’t necessarily work on the other.
The mosquito that spreads malaria prefers relatively cool temperatures of 25 degrees Celsius (77 degrees Fahrenheit). The dengue mosquito does best at 29 degrees Celsius (84.2 degrees Fahrenheit). Because of this difference in optimal temperatures, “We would actually predict that climate change might have opposing effects [on disease transmission],” said Erin Mordecai, assistant professor of biology at Stanford University and lead author on the study. “Climate change might make it less suitable for malaria to be transmitted but more suitable for dengue to be transmitted.”
Africa’s Nomadic Pastoralists and Their Animals Are an Invisible Frontier in Pandemic Surveillance
 @ASTMH The effects of COVID-19 have gone undocumented in nomadic pastoralist communities across Africa, which are largely invisible to health surveillance systems despite the fact that they are of key significance in the setting of emerging infectious disease. We expose these landscapes as a “blind spot” in global health surveillance, elaborate on the ways in which current health surveillance infrastructure is ill-equipped to capture pastoralist populations and the animals with which they coexist, and highlight the consequential risks of inadequate surveillance among pastoralists and their livestock to global health. As a platform for further dialogue, we present concrete solutions to address this gap.
@ASTMH The effects of COVID-19 have gone undocumented in nomadic pastoralist communities across Africa, which are largely invisible to health surveillance systems despite the fact that they are of key significance in the setting of emerging infectious disease. We expose these landscapes as a “blind spot” in global health surveillance, elaborate on the ways in which current health surveillance infrastructure is ill-equipped to capture pastoralist populations and the animals with which they coexist, and highlight the consequential risks of inadequate surveillance among pastoralists and their livestock to global health. As a platform for further dialogue, we present concrete solutions to address this gap.
Mobile phone-based saliva test wins NIH prize
Cornell researchers’ concept for a quick, non-invasive, mobile phone-based system to detect infectious diseases, inflammation and nutritional deficiencies in saliva was awarded a $100,000 National Institutes of Health Technology Accelerator Challenge prize. The NIH’s prize challenge encourages the development of new, non-invasive diagnostic technologies important for global health. For the group’s saliva-based test, a small 3D-printed adapter is clipped to a mobile phone and synced with a mobile app. The app uses the phone’s camera to image test strips to detect malaria, iron deficiency and inflammation, with results in under 15 minutes.
 The proposal builds on the FeverPhone and NutriPhone platforms developed by the team at Cornell’s Institute for Nutritional Sciences, Global Health and Technology (INSiGHT). The technologies, funded by the NIH and the National Science Foundation, evaluate infections and nutritional status using blood. According to Mehta, technologies using salivary biomarkers could revolutionize how conditions such as malaria and iron deficiency are identified and addressed, especially in settings where access to primary health care and traditional, laboratory-based tests is limited.
The proposal builds on the FeverPhone and NutriPhone platforms developed by the team at Cornell’s Institute for Nutritional Sciences, Global Health and Technology (INSiGHT). The technologies, funded by the NIH and the National Science Foundation, evaluate infections and nutritional status using blood. According to Mehta, technologies using salivary biomarkers could revolutionize how conditions such as malaria and iron deficiency are identified and addressed, especially in settings where access to primary health care and traditional, laboratory-based tests is limited.
Monsoon infections: How to tell the difference between dengue and malaria? Watch out for these symptoms
While both diseases are mosquito-borne and cause similar symptoms such as fever, joint/muscle pain, headaches, and fatigue, some differences between their symptoms can help you identify the specific infections. Unique symptoms of Malaria: Stomach problems such as vomiting, Diarrhoea, Dry cough, Shivering, Spleen enlargement Unique symptoms of Dengue: Pain behind the eyes, Swollen glands, Rashes
Epidemiology &History &Migration &Mosquitoes &Plasmodium/Parasite Bill Brieger | 12 Oct 2019
What to Observe on October 12th? Malaria’s Arrival in the Americas
Controversy exists about what historical event should be observed in the USA on 12th October. Ernest Faust explained many years ago that, “there is neither direct nor indirect evidence that the malaria parasites existed on this continent prior to the advent of the European conquerors,” while at the same time in the 16th through 18th Centuries, malaria  was common in England, Spain, France, Portugal and other European nations that arrived in the “New World.” Initially, with the first voyage of Columbus the European explorers and settlers brought the disease, primarily Plasmodium vivax, while the slave trade brought P. falciparum.
was common in England, Spain, France, Portugal and other European nations that arrived in the “New World.” Initially, with the first voyage of Columbus the European explorers and settlers brought the disease, primarily Plasmodium vivax, while the slave trade brought P. falciparum.
National Geographic in its May 2007 issue provided the story “Jamestown, The Real Story.” This article reported that, “Colonists carried the plasmodium parasite to Virginia in their blood. Mosquitoes along the Chesapeake were ‘infected’ by the settlers and spread the parasite to other humans.” Thus malaria became one of many imported diseases that decimated the indigenous population. The spread of P. vivax in Jamestown was not surprising since the settlement was “located on marshy ground where mosquitoes flourished during the summer.”
 Recent research has shown that the “Analysis of genetic material extracted showed that the American P. falciparum parasite is a close cousin of its African counterpart.” This research has documented two genetic groups in Latin America, related to two distinct slave routes run by the Spanish empire in the North, West Indies, Mexico and Colombia and the Portuguese empire to Brazil. Indigenous and remote rural populations of Bolivia, Colombia, Ecuador, Peru, Venezuela and Brazil remain at risk today.
Recent research has shown that the “Analysis of genetic material extracted showed that the American P. falciparum parasite is a close cousin of its African counterpart.” This research has documented two genetic groups in Latin America, related to two distinct slave routes run by the Spanish empire in the North, West Indies, Mexico and Colombia and the Portuguese empire to Brazil. Indigenous and remote rural populations of Bolivia, Colombia, Ecuador, Peru, Venezuela and Brazil remain at risk today.
In the South American continent the native American population might have brought Melanesian strains of P. vivax before the Europeans arrived, but colonizers brought new strains from both Europe and Africa, as well as P. falciparum. Clearly, human migration has played an important role in malaria parasite dissemination through the Americas.
But back to the North American Continent where the USA is observing the historical implications of 12th October, Mark Blackmore reminds us that, “Anthropological and archeological data provide no indication of mosquito-borne diseases among the indigenous people of North America prior to contact with Europeans and Africans beginning in the fifteenth century” (Wing Beats Volume 25 Winter 2015). The spread of malaria by European colonizers is certainly not something to celebrate today.
Migration &Refugee Bill Brieger | 20 Jun 2019
Refugees and Malaria
 The 2019 Theme of World Refugee Day is #StepWithRefugees – Take A Step on World Refugee Day. Taking steps in solidarity with refugees ensures that one recognizes that refugees experience several health problems, with malaria being especially devastating. Refugees may come from a malaria endemic area and move to one where there is no malaria and health workers may not recognize and treat it correctly. In contrast they may move from a non-endemic area into one with malaria transmission. Even if refugees move from one malarious area to another, the conditions of the camps where they shelter may lead to increased malaria morbidity and mortality.
The 2019 Theme of World Refugee Day is #StepWithRefugees – Take A Step on World Refugee Day. Taking steps in solidarity with refugees ensures that one recognizes that refugees experience several health problems, with malaria being especially devastating. Refugees may come from a malaria endemic area and move to one where there is no malaria and health workers may not recognize and treat it correctly. In contrast they may move from a non-endemic area into one with malaria transmission. Even if refugees move from one malarious area to another, the conditions of the camps where they shelter may lead to increased malaria morbidity and mortality.
In fact, Jamie Anderson and colleagues observe that, “Almost two-thirds of refugees, internally displaced persons, returnees and other persons affected by humanitarian emergencies live in malaria endemic regions. Malaria remains a significant threat to the health of these populations.” They found that, “an average of 1.18 million refugees resided in 60 refugee sites within nine countries with at least 50 cases of malaria per 1000 refugees during the study period 2008-2009,” a major disease burden. According to the authors, groups like UNHCR and the UN Foundation’s Nothing But Nets aim to increase LLIN coverage of vulnerable groups in emergency situations.
The US Centers for Disease Control and Prevention offers guidance to health staff in the United States who may encounter refugees coming from a malaria endemic country. These guidelines look at appropriate treatment regimens for either pre-travel or on arrival presumptive treatment. They address the challenges of sub-clinical disease, as well as testing and treatment for people with symptoms. Likewise, the Refugee Technical Assistance Center stresses the need for, “All refugees from malaria endemic areas, including those who have been presumptively treated for P. falciparum, should be tested for malaria if they develop clinical signs or symptoms of the disease.” Stefan Collinet-Adler et al. found that “Overseas presumptive therapy has greater cost-benefits than U.S. based screening and treatment strategies.”
The challenge of refugees moving from one endemic country, such as Burundi, to another was highlighted by MSF staff in Tanzania. Saschveen Singh reported that she, “was well versed in the emergency management of these cases from my previous training and from reading all the MSF clinical guidelines. But it was quite overwhelming to see how many admissions we had on the wards, and to see the outpatient area absolutely overflowing with patients with malarious fevers, and the number of our Burundian staff succumbing to the disease. With malaria, the worst of the worst cases are sadly always children.”
 A few years ago, the US President’s Malaria Initiative in Kenya contributed to indoor residual spraying at a refugee camp. “Malaria has also been a recurrent problem in Kakuma Refugee Camp, particularly following large-scale population influxes from South Sudan, where malaria is endemic. Both ITNs and IRS have been used historically for malaria prevention in the camp along with prompt, effective case management for persons diagnosed with malaria. With the pyrethroid donation from PMI-Kenya, NRC implemented a successful IRS program,” covering an estimated 143,000 people.
A few years ago, the US President’s Malaria Initiative in Kenya contributed to indoor residual spraying at a refugee camp. “Malaria has also been a recurrent problem in Kakuma Refugee Camp, particularly following large-scale population influxes from South Sudan, where malaria is endemic. Both ITNs and IRS have been used historically for malaria prevention in the camp along with prompt, effective case management for persons diagnosed with malaria. With the pyrethroid donation from PMI-Kenya, NRC implemented a successful IRS program,” covering an estimated 143,000 people.
It is encouraging to note that many agencies, international and domestic, and not just those specializing in refugee needs, lend a hand guaranteeing that refugees have a right to basic malaria prevention and treatment.
Case Management &Elimination &Epidemiology &Health Information &ITNs &Migration &Surveillance Bill Brieger | 20 Jul 2018
Establishing Mobile Outreach Teams (MOTs) for strengthening Active Case Detection with Mobile Populations in Vietnam 2016-2020
 Mobile migrant populations present a special challenge for malaria control and elimination efforts. Nguyen Ha Nam and colleagues* (Nguyen Xuan Thang, Gary Dahl, James O’Donnell, Vashti Irani, Sara Canavati, Jack Richards, Ngo Duc Thang, and Tran Thanh Duong) presented their study of this group at the recent Malaria World Congress. They are also sharing what they learned below.
Mobile migrant populations present a special challenge for malaria control and elimination efforts. Nguyen Ha Nam and colleagues* (Nguyen Xuan Thang, Gary Dahl, James O’Donnell, Vashti Irani, Sara Canavati, Jack Richards, Ngo Duc Thang, and Tran Thanh Duong) presented their study of this group at the recent Malaria World Congress. They are also sharing what they learned below.
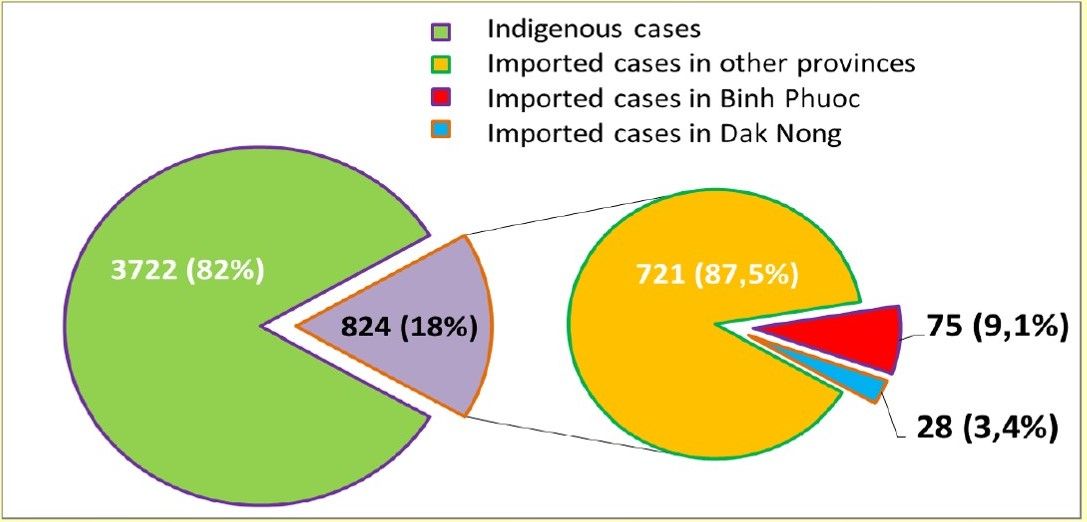
 Mobile Migrant Populations (MMPs) are a key population for containing the spread of malaria in the border areas between Cambodia and Vietnam. The number of imported cases in Viet Nam in 2017. 12,5% of such cases caught in Binh Phuoc and Dak Nong provinces and all of them came from Cambodia. The provinces bordering Cambodia and Vietnam have been had the highest malaria transmission intensity. This borders are frequented by MMPs who have proven difficult to target for surveillance and malaria control activities.
Mobile Migrant Populations (MMPs) are a key population for containing the spread of malaria in the border areas between Cambodia and Vietnam. The number of imported cases in Viet Nam in 2017. 12,5% of such cases caught in Binh Phuoc and Dak Nong provinces and all of them came from Cambodia. The provinces bordering Cambodia and Vietnam have been had the highest malaria transmission intensity. This borders are frequented by MMPs who have proven difficult to target for surveillance and malaria control activities.
 Mobile Outreach Teams (MOTs) provide a potential approach to target malaria elimination activities for MMPs who may not be strongly supported by the regular village-based and clinic-based health services. This work describes the implementation of MOTs in Binh Phuoc and Dak Nong Provinces, which are high-risk regions along the Viet Nam-Cambodia border. These activities were conducted as part of the Regional Artemisinin-resistance Initiative (RAI) in 2017. Each MOT was comprised of 2 Commune Health Staff and 1 Village Health Worker (VHW) from the village nearest to the outreach area.
Mobile Outreach Teams (MOTs) provide a potential approach to target malaria elimination activities for MMPs who may not be strongly supported by the regular village-based and clinic-based health services. This work describes the implementation of MOTs in Binh Phuoc and Dak Nong Provinces, which are high-risk regions along the Viet Nam-Cambodia border. These activities were conducted as part of the Regional Artemisinin-resistance Initiative (RAI) in 2017. Each MOT was comprised of 2 Commune Health Staff and 1 Village Health Worker (VHW) from the village nearest to the outreach area.
In the first phase of the pilot, 3 communes of 2 districts in Binh Phuoc and 2 communes of 1 district in Dak Nong with highest malaria cases reported from NIMPE are selected as targeted areas. The Objectives were to …
- Design/tailor Mobile Outreach Information Education and Communication/Behaviour change communication (BCC/ IEC) Toolkit
- Intensify case detection and quality management by increasing the coverage of diagnostics and treatment for hard to reach populations
- Strengthen outreach to high-risk and under-served populations through MOT scouting activities to locate unreached Mobile Communities and map their locations
- Link MMPs with health facilities and Village Health Workers
 All MOT members were provided with smartphones and were trained on how to use the EpiCollect5 app to track malaria cases, record mapping information and upload real-time reports of these malaria cases. MOTs conducted 5-day outreach activities every month. These activities began with scouting out locations of the MMP communities.
All MOT members were provided with smartphones and were trained on how to use the EpiCollect5 app to track malaria cases, record mapping information and upload real-time reports of these malaria cases. MOTs conducted 5-day outreach activities every month. These activities began with scouting out locations of the MMP communities.
Once located, the MOTs geo-tagged the location of the community, conducted a short epidemiological survey on the community and screened for malaria using Rapid Diagnostic Tests and blood smear microscopy. Active malaria cases were provided with treatment according to the National guidelines, and Long Lasting Insecticidal Nets were distributed based on results of diagnosis and the survey.
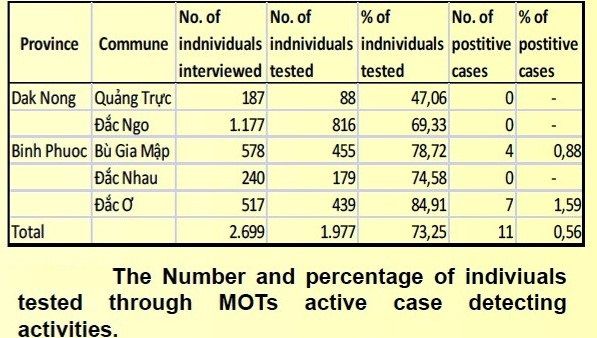 This action has led to increased diagnosis and treatment of hard to reach MMPs with increased access by those communities to malaria services. Improved understanding and increased use of malaria prevention practices hard to reach MMP communities/households. Mapped of previously unreached MMP Communities and unofficial border crossing points with malaria transmission hotspots and highly frequented crossing identified. The number of MMPs were monitored by MOTs were 2,699 accounting for 5.18% of the population in the project sites (2,699/52,095).
This action has led to increased diagnosis and treatment of hard to reach MMPs with increased access by those communities to malaria services. Improved understanding and increased use of malaria prevention practices hard to reach MMP communities/households. Mapped of previously unreached MMP Communities and unofficial border crossing points with malaria transmission hotspots and highly frequented crossing identified. The number of MMPs were monitored by MOTs were 2,699 accounting for 5.18% of the population in the project sites (2,699/52,095).
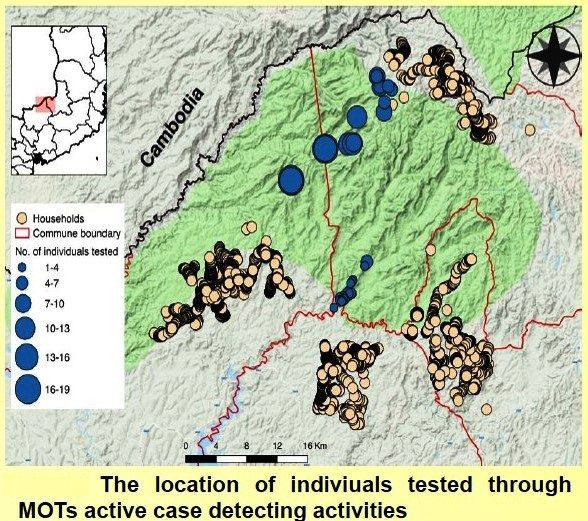
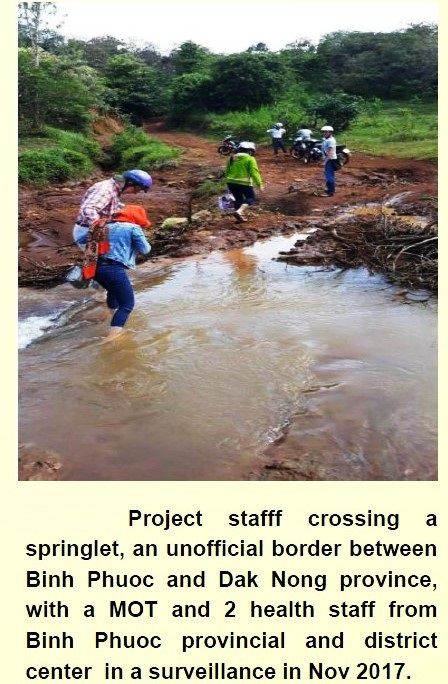
These screened MMPs were almost located along the border among project communes in Bu Gia Map National Forest where have a lot of unofficial border crossers, timber camp communities, and other revolving communities. 1,977 targeted people were tested for malaria. This number was achieved 73.25% of mobile migrant people (1,977/2,699). This work highlights how MOTs can target the previously unreached populations of MMPs to strengthen malaria surveillance and active case responses to reduce malaria transmission in Viet Nam.
 A system of real-time data collection of malaria cases from VHWs and MOTs using mobile phone uploads was established. Border screening and tracking hard to reach communities is a useful approach to implement to identify imported cases; however, it is labor-intensive, and misses subjects crossing at unofficial borders due to limited working time of MOTs (5 days a month).
A system of real-time data collection of malaria cases from VHWs and MOTs using mobile phone uploads was established. Border screening and tracking hard to reach communities is a useful approach to implement to identify imported cases; however, it is labor-intensive, and misses subjects crossing at unofficial borders due to limited working time of MOTs (5 days a month).
Positive cases in Binh Phuoc province are maintained for keeping track after receiving treatment due to no confirmed cases detected in targeted communes in Dak Ngo province, though these communes mainly have numerous transient timber camps moving in deep forests, and highly mobile border-crossers moving between regions and countries frequently. Future work will combine routine support from District health staff and expand the role of VHWs with motorbike provision for each MOT in order to not only to improve their quality outreach activities but also develop stronger Active Case Detection in the next phase of the project.
*Team members represent the National Institute of Malariology, Parasitology and Entomology, Hanoi, Viet Nam; Health Poverty Action, London, UK; and the Burnet Institute, Melbourne, Australia.
References
- Kheang ST, Lin MA, et al. Malaria Case Detection Among Mobile Populations and Migrant Workers in Myanmar: Comparison of 3 Service Delivery Approaches. 2018
- Shannon Takala-Harrison,a Christopher G. Jacob, et al. Independent Emergence of Artemisinin Resistance Mutations Among Plasmodium falciparum in Southeast Asia. 2014.
- Imwong M, Hien TT, et al. Spread of a single multidrug resistant malaria parasite lineage (PfPailin) to Vietnam. 2017.
- Richard J Maude,corresponding author Chea Nguon, et al. Spatial and temporal epidemiology of clinical malaria in Cambodia 2004–2013. 2014.
- Imwong M, Nguyen TN, et al.The epidemiology of subclinical malaria infections in South-East Asia: findings from cross-sectional surveys in Thailand–Myanmar border areas, Cambodia, and Vietnam. 2015.
- Hannah Edwards, Sara E. Canavati, et al. Novel Cross-Border Approaches to Optimise Identification of Asymptomatic and Artemisinin-Resistant Plasmodium Infection in Mobile Populations Crossing Cambodian Borders. 2015.
Eradication &Migration &Surveillance Bill Brieger | 06 Feb 2018
Malaria Should Lead to Compassion, Not Hate
In August 2017 the ‘Almost Impossible’ happened decades after the last of local malaria transmission stopped in Italy. NPR shared news from the Italian newspaper Corriere della Sera that, “A 4-year-old girl has died of malaria in Italy, where the disease is thought to have been wiped out. Troubled health officials are looking for answers.” By coincidence, two children from an African nation were being treated for malaria in the same hospital where the deceased was being treated for diabetes. No epidemiological link could be found.

World Malaria Report: http://www.who.int/malaria/publications/world-malaria-report-2017/en/
Unfortunately that has not stopped anti-immigrant politicians from using the incident to foster hatred. The political party of a “far-right extremist who wounded 6 African immigrants in a racially motivated shooting rampage in central Italy,” blamed the death of the child mentioned above “from malaria on migrants who ‘bring back to Europe’ once, eradicated illnesses.”
A new article in Malaria Journal reports that even though, “Malaria is no longer endemic in Italy since 1970 when the World Health Organization declared Italy malaria-free, … it is now the most commonly imported disease.” The study from Parma, Italy reports that, “Of the 288 patients with suspected malaria, 87 were positive by microscopy: 73 P. falciparum, 2 P. vivax, 8 P. ovale, 1 P. vivax/P. ovale, 1 P. malariae and 2 Plasmodium sp. All samples were positive by ICT except 6. ”
Malaria can travel with anyone who has been in an endemic area, whether migrant, tourist or business person. The likelihood of malaria re-establishing itself in currently non-endemic areas is low, but there is of course value in maintaining epidemiological and entomological surveillance world-wide in the current drive to eradicate the disease.
The identification of malaria anywhere in the world should be cause for concern and compassion, not hate and exclusion.
Elimination &Health Rights &Migration Bill Brieger | 13 Apr 2013
Malaria Elimination in a Challenging Human Rights Environment
A new article by Wickramage and Galappaththy raises numerous challenges facing a country like Sri Lanka that is approaching malaria elimination. Human trafficking takes people from a malaria free zone, transits them through malarious areas in West Africa, and then in this case they are rescued and returned home, some carrying malaria parasites.
 Other island nations are also addressing the problem of preventing future reintroduction of malaria, but they are not in a post-conflict situation that creates what Wickramage and Galappaththy euphemistically called “irregular migrants.” Seychelles has addressed both vector control as well as provision of malaria chemoprophylaxis and health education to outbound citizens.
Other island nations are also addressing the problem of preventing future reintroduction of malaria, but they are not in a post-conflict situation that creates what Wickramage and Galappaththy euphemistically called “irregular migrants.” Seychelles has addressed both vector control as well as provision of malaria chemoprophylaxis and health education to outbound citizens.
Trafficked citizens would obviously and unfortunately miss the opportunity to get prophylaxis (as well as many other opportunities in life). In Sri Lanka those returning from trafficking transit in West Africa were screened at the airport and treated. Seychelles could learn from this experience.
Mauritius has not had an indigenous malaria case in over a decade although the vectors are still present. Mauritius actively screens people return from malaria endemic areas at both airport and seaport.
Malaria Journal reports that in Sao Tome and Principe “A steep decline of ca. 95% of malaria morbidity and mortality was observed between 2004 and 2008 with use of the combined control methods. Malaria incidence was 2.0%, 1.5%, and 3.0% for 2007, 2008, and 2009, respectively. In April 2008, a cross-sectional country-wide surveillance showed malaria prevalence of 3.5%, of which 95% cases were asymptomatic carriers.”
So yes, countries approaching elimination must have a surveillance system that finds both obvious clinical cases as well as asymptomatic infections among residents and people returning to or visiting from the outside. Island nations are among the first to put this process to the test. But the bigger lesson from Sri Lanka’s ‘irregular migrants’ is that as long as conflicts, human trafficking and human rights violations persist, malaria will be difficult to eliminate. Malaria demonstrates that no man or woman is an island.