Eradication &Health Systems Bill Brieger | 21 Dec 2013
Remembering a Pioneer in International Health and Health Systems: Tim Baker
Honoring people in their lifetime is important, and fortunately Prof. Timothy Baker and his wife Prof Sue Baker were jointly recognized for their many years of service, not only to the Johns Hopkins University Bloomberg School of Public Health, but generally to the fields of global health systems and management. A portrait of the couple was presented and hangs at the School to remind all of their contributions. Unfortunately Tim Baker left us earlier this week.
 While such departures are not often surprising when people have passed their three score and ten, Tim Baker at 88 was still active in teaching, research and service. In fact we served together on the School’s MPH Admissions Committee where Tim Baker brought his wealth of experience and compassion for training students to bear at each meeting. From the student’s point of view, I can saw that even though Tim Baker was not my adviser in during my DrPH at JHU (1989-91), he always looked after my academic progress and was the one to nominate me for Delta Omega (Public Health Honor Society) membership.
While such departures are not often surprising when people have passed their three score and ten, Tim Baker at 88 was still active in teaching, research and service. In fact we served together on the School’s MPH Admissions Committee where Tim Baker brought his wealth of experience and compassion for training students to bear at each meeting. From the student’s point of view, I can saw that even though Tim Baker was not my adviser in during my DrPH at JHU (1989-91), he always looked after my academic progress and was the one to nominate me for Delta Omega (Public Health Honor Society) membership.
On the occasion of the portrait unveiling in 2011, the school shared these brief notes on Dr. Baker’s career: “
Timothy Baker, MD, MPH, a professor in International Health, joined the School as a faculty member in the Department of Public Health Administration and as an assistant dean. In 1961, he founded the School’s Division of International Health and served as acting director. Over the next five years, he was instrumental in building the Division into the Department of International Health. Baker’s fundamental contributions to the Department include faculty recruitment, curriculum development, student mentoring and fundraising. He was instrumental in establishing one of the School’s first endowed professorships—the Edgar Berman Professorship in International Health.
“In more than 50 years as a researcher and consultant, Baker—who holds joint appointments in Health Policy and Management and Environmental Health Sciences—worked in over 40 countries, focusing on health services and assessment of disease and injury burden. He also held leadership positions in several international public health agencies.”
Dr Baker touched many lives. Prof. Peter Winch, Director of International Health’s Social and Behavioral Interventions Program expressed the following in his e-mail to colleagues:
Tim Baker passed away today at the age of 88. I first met him in 1987 as an MPH student when he lectured in Introduction to International Health. It is truly impossible to summarize all of his contributions to the Department of International Health, and to the field of Global Health. This is a quick of superficial overview of his contributions. It is always difficult to know who originated any given idea. But if Tim was not the first one to push the elevator button, he was definitely at the ground floor before the elevator went up. So here is my partial list of his conceptual contributions. This is my paraphrasing of his thinking. He usually expressed such ideas in a more circuitous manner, or did not make a statement at all but rather demonstrated the idea through his actions.
- Public health professionals from low and middle-income countries need training not only on disease prevention and control, but also the design of health systems, management and supervision, leadership and advocacy.
- A central task of global health spending by the US government in low and middle-income countries needs to be capacity-building of local institutions and health professionals. If we don’t do good capacity building, the investments will not yield any lasting results.
- Health systems in low and middle-income countries need to address not only infectious causes of morbidity and mortality, but also occupational health, environmental health, injuries and chronic disease.
- Health workforce development is a complex matter, and warrants high-quality planning, evaluation and research.
- Our School of Public Health benefits from a dynamic, multi-disciplinary, problem-based Department of International Health. Such a Department is an asset to other more disciplinary departments, rather than a threat or a problem.
- Finally: There are no problem students. Every student is an asset. If the faculty identify a student as a problem, there is a good chance the problem lies with the faculty.
Likewise Prof. Adnan Hyder, Director of the Health Systems Program with which Dr. Baker was most recently associated expressed these thoughts:
It is with great sadness that I email you to announce that our beloved Dr. Tim Baker passed away yesterday. This is an incredible loss for our program, the department, and the school to start; but really the entire global health community. As the founder of our department, he was a powerhouse of knowledge, inquiry, and persistence; as a teacher and mentor he was a giant in the field; and as a proponent of the poor and vulnerable, he hid a warm and glowing heart under his witty exterior. So many of us were fortunate to be his students, colleaugues and friends; and how lucky we were to receive his wisdom, insight and sharp advice. Not a man to appreciate praise, he always cut it short; not one to stand pomp and ceremony he often avoided it; and not one to accept failure he believed in the power of humanity to succeed. We will dearly miss him, his humor, his flowers (for ladies only) and his raisin bread – and always remember that he asked us to work harder, and better than anyone else in the world for the cause of social justice and international health.
Let us make sure we never forget his legacy.
Although tropical diseases per se were not Tim Baker’s primary focus, he was concerned about the health systems implications of control programs. In 1962 as the first global effort to eradicate malaria was underway, Tim Baker made the following observations in the American Journal of Public Health:
Malaria eradication “contributes to our own protection. Malaria can be reintroduced into the United States, as several local epidemics have conclusively proved. Just as in the case of yellow fever, where our shores were not safe from imported epidemics until the disease had been controlled in the major ports throughout the world, so it is with
malaria; the world is not safe from the threat of disastrous epidemics until malaria has been eradicated everywhere.” Dr Baker was well aware of challenges that still face us today when he noted that, “widespread development of insecticide resistance lends overwhelming urgency to the completion of eradication.”
He further explained that, “health workers are presented with the opportunity of developing and proving a new method of attack on disease that has tremendous economic import.” The economic impact of malaria remains today one of the driving forces behind efforts to eliminate the disease.
More recently (2007), Dr Baker demonstrated the importance of maintaining a long term perspective. Concerning India’s efforts at controlling malaria from its first through 10th five-year plan, Dr Baker drew on 50+ years of experience to comment that, “The drop from a million to a thousand deaths underscores the value of the malaria program.” It may be another 50 years until malaria is truly eradicated, but if we keep a critical long term view as exemplified by Dr Baker we will be alert to both the challenges and opportunities to bring malaria to an end.
Community Bill Brieger | 17 Dec 2013
Community-Based versus Community-Directed Approaches
Guest Blog Posting: Meike Schleiff is a DrPH Candidate in International Health Systems at JHSPH. She has a background in agriculture and natural resources and holds a Master of Science in Public Health (MSPH) from JHSPH as well. Meike is the Founder and Executive Director of The GROW Project (www.thegrowproject.org) based in West Virginia and working in communities in and around Cap Haitien, Haiti.
The Declaration of Alma Ata (WHO, 1978) sets out a vision for equitable, multi-sectoral, and locally relevant, effective, and affordable health care in holistic terms. The role the community is central, and the local health workers and primary level of contact with the health system create the “central function and main focus” on which other development and levels of care can be built. Ken Newell wrote eloquently in Health by the People (1975) about the importance of “self-sufficiency” of communities to the greatest extent feasible as being the most cost-effective, appropriate, and immediate option to further health.

Mac Henri, a young local leader, heads a cholera information session in the Baptist Church at Soufriere, Haiti.
In 2009, Paul Freeman, Henry Perry and others conducted a Review of Community-Based Primary health Care (CBPHC) approaches to achieving the MDG for child health. Although many projects in the review effectively incorporated a community-based component and delivered Primary Health Care (PHC) interventions, the level of involvement and leadership of the community varied and was difficult to ascertain and may not have been the main reason for conducting the intervention outside of a facility. The findings of the review (which are ongoing) show the difficulty of finding evidence of empowerment and leadership given to communities. The projects seem to have overall positive affects, but there a wide range of levels of engagement and community roles.

A local woman explains to Meike and a Ministry of Health representative where the different drinking water sources (mostly springs and the river) for her neighborhood are. She is helping us decide on the best location for a community water system that will protect and treat a water system against cholera and other water-borne diseases.
Several publications from Africa use language of Community-Directed Initiatives (CDIs) as a model built on PHC principles in order to deliver health interventions in communities. In the CDI model, communities are the driving force of planning and implementing the interventions, and gain a sense of ownership and motivation far beyond financial gains that help ensure sustainability (The CDI Study Group, 2010). This model has been used effectively in Nigeria, Cameroon and Uganda (Ajiyi et al, 2013 & The CDI Study Group, 2010).
In my experience, what is called community-based versus community-directed in the literature can be difficult to differentiate. However, as Dr. Carl Taylor aptly pointed out, empowerment—and I would venture to include leadership and true initiative by communities—can easily be recognized because “you know it when you see it”. When a community feels heard and is effectively engaged, a process to fulfill the original vision of PHC from Alma Ata is possible.
To me, the central argument that spans both CBPHC and CDI is that building capacity and leadership are essential. This can be done within local facilities as well as in people’s homes. Conversely, so-called community projects can still be very much driven by outside agendas and voices. Volunteers, resources, and data should be accountable and shared first with the community and secondly with supervisors. Both are important, but too often in Public Health the latter is only direction of knowledge-sharing to which funds, time, and patience are allocated.
To conclude, terminology can easily become blurred and can be used for a variety of different levels of engagement, leadership, and capacity-building for communities. The importance to me is whether the community has a voice and some level of leadership, control, and responsibility of the destiny of their health and well-being.
————————

The Community Council of Soufriere, Haiti meets along with some spectators to problem-solve and discuss the most important priorities for health–beyond cholera–in their community. The Council includes a Ministry representative and the local judge, but is mostly composed of religious and educational leaders, the local Agent Sante (community health workers), and the nurses who staff the cholera treatment center.
References: Ajayi, I., Jegede, A., Falade, C., Sommerfeld, J. (2013). Assessing Resources for Implementing A Community Directed Intervention (CDI) Strategy for Providing Multiple Health Interventions in Urban Communities in Southwestern Nigeria: A Qualitative Study. Infectious Diseases of Poverty, 2:25. (http://www.ncbi.nlm.nih.gov/pubmed/24156481)
Freeman, P., Perry, H. B.,, Gupta, S.K., Rassekh, B. (2009). Accelerating Progress in Achieving the Millennium development Goal for Children Through Community-Based Approaches. Global Public Health: An International Journal for Research, Policy and Practice, 7:4, 400-419. (http://www.ncbi.nlm.nih.gov/pubmed/19890758)
Newell, K. (1975). Health by The People. World Health Organization, Geneva, Switzerland.
The CDI Study Group. (2010). Community-Directed Interventions Against Health Problems in Africa: Results of a Multi-Country Study. Bulletin of the World Health Organization. 88:509-518. (http://www.who.int/bulletin/volumes/88/7/09-069203/en/)
WHO. (1978). Declaration of Alma Ataz: International Conference on Primary Health Care, Alma-Ata, USSR, 6-12 September, 1978.
Elimination &IPTp &ITNs &Treatment Bill Brieger | 06 Dec 2013
Draft Nigeria 2013 DHS Shows Slow Progress for Malaria
The Nigeria Demographic and Health Survey (DHS) 2013 Draft Preliminary Report from the National Population Commission, Abuja, Nigeria and MEASURE DHS, ICF International, Calverton, Maryland, USA was released in-country in September 2013. These are the same organizations that conducted the 2010 Malaria Information Survey (MIS).
From the malaria perspective this has been a long anticipated event since the country has distributed over 60 million long lasting insecticide-treated nets since 2009. The 2010 MIS showed some progress over the 2008 DHS, but since it took place near the beginning of the massive net distribution effort, there was hope that a subsequent survey would highlight an improvement. If that were the expectation, people will be quite disappointed.
Lets start with nets. Our attached table shows only a slight improvement in the proportion of households owning at least one net. The idea behind the massive net campaigns from 2009-12 were achievement of universal coverage where there would be at least one net for every two people in a household. Where did these nets go? Were they damaged beyond use in the relatively short time that elapsed?
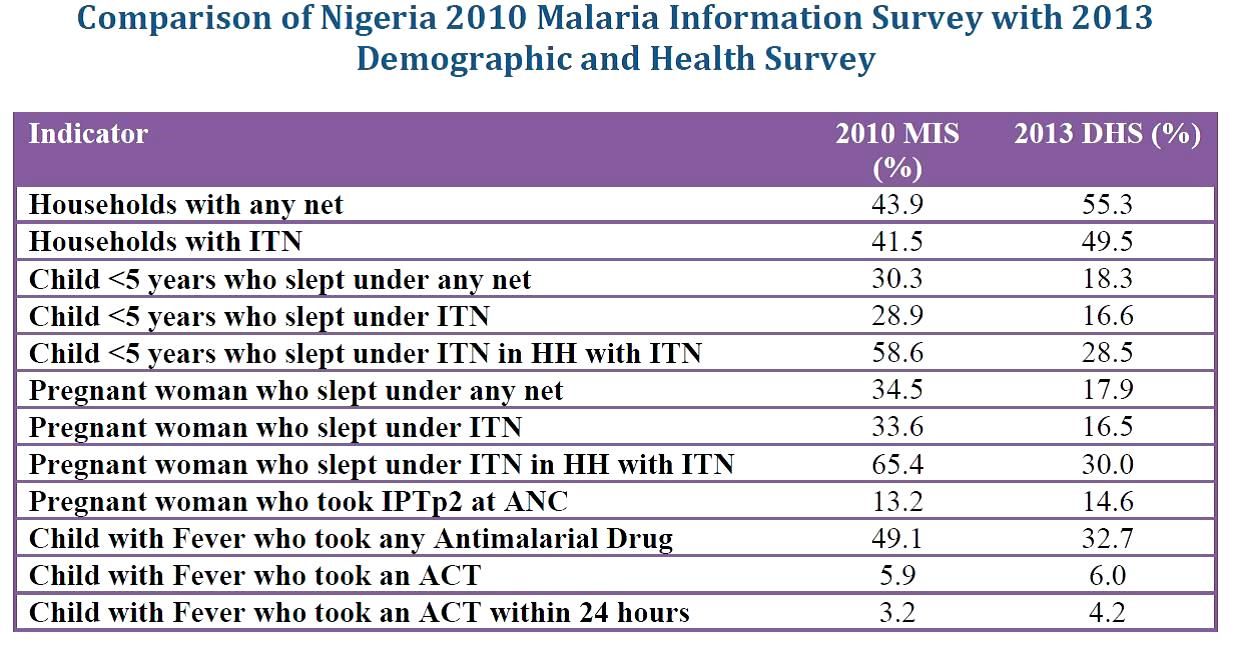 What is more disappointing is that th proportion of young children and pregnant women sleeping under an insecticide treated net (ITN) reduced to just slightly over half of the 2010 figure. This reduction also happened even in households that actually owned ITNs. This is mysterious to say the least.
What is more disappointing is that th proportion of young children and pregnant women sleeping under an insecticide treated net (ITN) reduced to just slightly over half of the 2010 figure. This reduction also happened even in households that actually owned ITNs. This is mysterious to say the least.
Prevention of malaria in pregnancy has been a neglected part of malaria control in many countries, but since the drug used for intermittent preventive treatment (IPT), sulphadoxine-pyrimethamine (SP) is so cheap, it was assumed that most health systems could afford to guarantee every woman attending antenatal care the required dosed. Unfortunately the status of IPT showed almost no improvement between 2010 and 2013 and remained far, far below the 2010 Roll Back Malaria target of 80% coverage. SP is produced in Nigeria; why can it not reach pregnant women?
Finally appropriate malaria treatment of young children is also in the doldrums. The actual number of children who received any anti-malarial drug declined, while those receiving the appropriate artemisinin-based combination therapy (ACT) remained essentially level at around 6%. Where have all the ACTs brought in through Global Fund, the US President’s Malaria Initiative and other donors gone? How can we expect infant and child mortality to decrease in the absence of appropriate treatment for one of the most common child killer diseases?
At the recently concluded 6th Pan African Malaria Conference in Durban, South Africa, participants were told that the only way to truly eliminate malaria is to tackle the high burden countries like Nigeria head on. If these data indicate how we are waging the malaria battle in Nigeria, our hopes for elimination in the near future will be dashed.