CHW &Integration &IPTi &IPTp &Malaria in Pregnancy &Maternal Health &Seasonal Malaria Chemoprevention Bill Brieger | 12 Dec 2022
Malaria Chemoprevention in 2021 as Seen in The World Malaria Report of 2022
 Dr Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization, reminds us in this year’s edition of the World Malaria Report (WMR 2022) that, “Although hard hit, most countries held the line and were able to maintain services to prevent, detect and treat malaria – a remarkable feat in the midst of a pandemic. Nonetheless, more than 600 000 people still die of malaria every year – most of them children. Even with the heroic efforts to maintain services during the pandemic, malaria control efforts face many hurdles in addition to the already significant COVID-related disruptions and other health system challenges.”
Dr Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization, reminds us in this year’s edition of the World Malaria Report (WMR 2022) that, “Although hard hit, most countries held the line and were able to maintain services to prevent, detect and treat malaria – a remarkable feat in the midst of a pandemic. Nonetheless, more than 600 000 people still die of malaria every year – most of them children. Even with the heroic efforts to maintain services during the pandemic, malaria control efforts face many hurdles in addition to the already significant COVID-related disruptions and other health system challenges.”
Even though there was an increase in cases between 2020 and 2021, there are now more strategies in the malaria control and elimination toolkit than ever before. One in particular is an updated take on an old concept of chemoprophylaxis, which fell out of use due to mounting drug resistance. Years of research with pregnant women and young children led to the development over time of using regularly scheduled treatment doses of malaria medicines as chemoprevention. Intermittent Preventive Treatment for pregnant women (IPTp) and Seasonal Malaria Chemoprevention for young children, both targeted to appropriate epidemiological settings, are now common. Countries are also exploring IPT for children in other settings.
 We were, therefore, curious what the current WMR shares on chemoprevention initiatives. Specifically, the WMR summarized WHO recommendations as follows: “Updated guidelines provide recommendations on intermittent preventive treatment of malaria in pregnancy (IPTp), perennial malaria chemoprevention (PMC) and seasonal malaria chemoprevention (SMC), intermittent preventive treatment of malaria in school-aged children (IPTsc), post-discharge malaria chemoprevention (PDMC), mass drug administration (MDA) and elimination.”
We were, therefore, curious what the current WMR shares on chemoprevention initiatives. Specifically, the WMR summarized WHO recommendations as follows: “Updated guidelines provide recommendations on intermittent preventive treatment of malaria in pregnancy (IPTp), perennial malaria chemoprevention (PMC) and seasonal malaria chemoprevention (SMC), intermittent preventive treatment of malaria in school-aged children (IPTsc), post-discharge malaria chemoprevention (PDMC), mass drug administration (MDA) and elimination.”
In summary, WMR 2022 notes that, “The average number of children treated per cycle of SMC increased from about 0.2 million in 2012 to almost 45 million in 2021,” and “Using data from 33 countries in the WHO African Region, the percentage of IPTp use by dose was computed. In 2021, 72% of pregnant women used ANC services at least once during their pregnancy. About 55% of pregnant women received one dose of IPTp, 45% received two doses and 35% received three doses.” This is not just progress over time, but also represents an expansion targets and work required for success. For pregnant women the increase represented a change in target from only two doses during pregnancy to a minimum of three. Starting with pilot efforts, SMC now covers children in 15 countries.
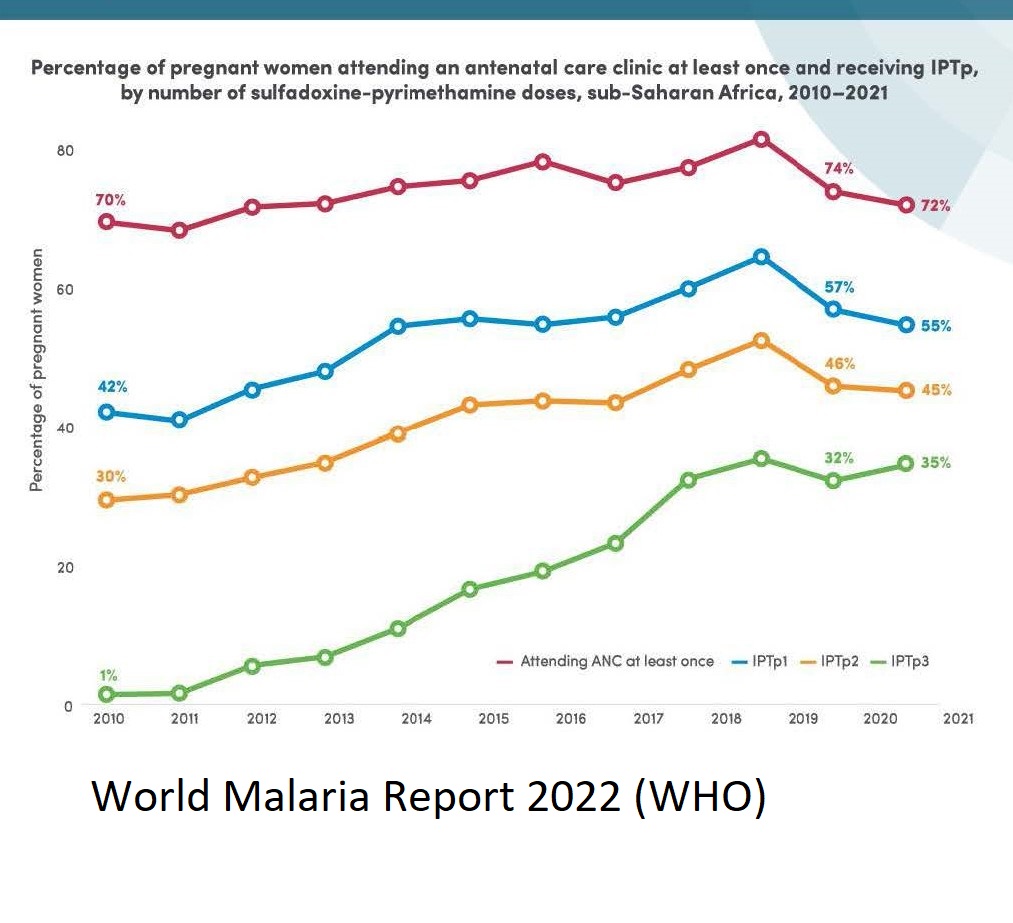 The targeted three doses for IPTp shows that two thirds of women who register for antenatal (prenatal) care (ANC), fail to achieve full coverage. Stronger collaboration is needed between malaria control and maternal health programs to ensure that pregnant women actually attend ANC and do so early and often enough to receive 3 monthly doses minimum in their second and third trimesters. More emphasis is needed on community IPTp distribution, since we know that community health workers have been crucial in achieving SMC as well as integrated community case management efforts.
The targeted three doses for IPTp shows that two thirds of women who register for antenatal (prenatal) care (ANC), fail to achieve full coverage. Stronger collaboration is needed between malaria control and maternal health programs to ensure that pregnant women actually attend ANC and do so early and often enough to receive 3 monthly doses minimum in their second and third trimesters. More emphasis is needed on community IPTp distribution, since we know that community health workers have been crucial in achieving SMC as well as integrated community case management efforts.
Similar challenges exist for SMC as research looks into whether additional doses are needed based on mosquito breeding and malaria transmission season factors in endemic countries. Adding extra months to the program will tax resources, but also save lives.
Both maternal and child efforts at chemoprevention will need to address research that first shows increasing resistance to the common medicines used, and the potential for introducing new drug combinations in light of that resistance. Challenges here reflect another aspect of SMC, the need for CHWs to guarantee that on any given distribution round, three doses on medicine are required. Recent reports show that within any given round, community adherence to SMC has been good. We need to apply those lessons to IPTp when the regimen changes.
Ultimately, chemoprevention has proven to be an important life saving tool. The challenges of multiple contacts and doses that lead to success rely not only on having effective medicines, but also on culturally appropriate behavior change strategies and well-funded efforts to strengthen the health systems that deliver preventive treatments.