Agriculture &Children &Climate &Coordination &Development &Elimination &Environment &Epidemiology &Food Security Bill Brieger | 15 Apr 2022
Malaria elimination challenges around the world
In the past week, news has featured challenges to malaria elimination around the globe. Starting in Papua New Guinea which accounted for accounted for 86% of all cases in the Western Pacific Region in 2020. While there are 39% fewer cases in the region since 2000, there was an increase of 300,000 cases between 2019 and 2020. It is mainly in the six countries of the Greater Mekong subregion where progress has been steady.
 Moving east to the Brazilian Amazon, one finds wildcat gold mining operations are not only destroying Native American ecosystems but are carving huge holes in the earth which are perfect breeding conditions for mosquitoes. This means that malaria cases among the Yanomami indigenous people living in the Brazilian Amazon have increased by more than 12 times since 2014.
Moving east to the Brazilian Amazon, one finds wildcat gold mining operations are not only destroying Native American ecosystems but are carving huge holes in the earth which are perfect breeding conditions for mosquitoes. This means that malaria cases among the Yanomami indigenous people living in the Brazilian Amazon have increased by more than 12 times since 2014.
Also within South America, one finds that although Paraguay was certified by the World Health Organization (WHO) as free of local transmission of malaria in 2018, experts are warning that travelers entering the country from areas with malaria transmission could easily reintroduce the disease. Hence vigilance is urged.
Crossing next to sub-Saharan Africa, one reads of studies showing an increasing link between malaria and agriculture across the region. As population expands in the region, more food, water and agricultural commodities are required. Irrigation and deforestation to clear land for agriculture increase the risk of childhood malaria in sub-Saharan Africa. The experts recommend that African ministries of agriculture, health, and environment need to collaborate on safer development policies and practices, not only to curb malaria, but the devastating effects of climate change.
Finally continuing back to Asia, one finds what might be termed an epidemiological conflict between Nepal, which is nearing malaria elimination for 2025, and its southern neighbor India, which is a source of imported malaria. Although the number of indigenous cases is nearing zero, health authorities fear that imported cases of of malaria from India are so high that local transmission could be reignited.
Malaria is clearly a global health problem. Collaboration and coordination across continents is needed to eliminate the scourge.
Coordination &COVID-19 &Ebola &Microscopy &Mosquitoes &Vector Control Bill Brieger | 04 Sep 2020
Malaria News Today 2020-09-04
Today, we are sharing more updates from newsletters and journal abstracts found online. Issues include citizens in Rwanda trapping mosquitoes, the need for standardizing microscopy, more information on Uganda’s Malaria fund, the challenge of containing three epidemics at once, an increase in cases in Namibia and genetic diversity of the parasite in Comoros. Click on links to read details.
Citizen science shows great potential to reduce malaria burden
 A year-long collection of mosquitoes with self-made traps and over a hundred volunteers in rural Rwanda reporting levels of mosquito nuisance revealed when and where malaria risks were the highest. In addition to their reporting, the volunteers appeared to distribute knowledge and skills on controlling malaria within communities. Studies by Wageningen University & Research and the University of Rwanda show that citizen science has great potential to reduce the disease burden across the globe.
A year-long collection of mosquitoes with self-made traps and over a hundred volunteers in rural Rwanda reporting levels of mosquito nuisance revealed when and where malaria risks were the highest. In addition to their reporting, the volunteers appeared to distribute knowledge and skills on controlling malaria within communities. Studies by Wageningen University & Research and the University of Rwanda show that citizen science has great potential to reduce the disease burden across the globe.
Uganda renews fight to eliminate malaria by 2030 – more on Malaria Free Uganda Fund
Uganda says it is fast-tracking efforts to eliminate malaria, which continues to take lives and bleed the country’s economy more than any other disease. The disease is responsible for 30 to 40 percent of outpatient hospital visits, 15 to 20 percent of admissions, and 10 percent of inpatient deaths, mostly pregnant mothers and children, according to the health ministry figures. The country on September 2 launched the board of directors of the Malaria Free Uganda Fund as part of its continued investment to eliminate the disease by 2030, as per the global target.
Malaria Free Uganda Fund is a nonprofit public-private partnership established to mainstream responsibility for malaria across all sectors and help remove financial and operational bottlenecks in fighting the disease. The National Malaria Control Program currently faces a three-year 206 U.S. million dollars budget gap, or 33 percent of the total, according to the ministry of health. External donors, according to the ministry, fund over 95 percent of the fight against the disease in the country. The country is now looking at domestic resourcing in view of the global uncertainties like the COVID-19 pandemic that is affecting foreign financing. “The talent and experience we have mobilized to this board from the private and civil society will help the government achieve a significant reduction of malaria cases and deaths in Uganda,” said Ruth Aceng, minister of health while launching the board here.
Namibia records 12,507 malaria cases, 40 deaths in 2020
Namibia’s malaria cases this year increased to 12,507 from 2,841 recorded in 2019, according to statistics from the Ministry of Health. The southern African country recorded 31,000 cases of malaria in 2018. The National Vector-borne Diseases Control Program from the Health Ministry which monitors the weekly malaria situation in the country shows that this year alone 12,507 malaria cases where recorded, while 40 deaths occurred.
The ministry said the huge difference between 2019 and this year is attributed to the fact that 2019, was a drought year and the rainfall pattern was not similar to 2020 and 2018, hence the decline in malaria cases happened in 2019. According to the ministry, currently the implementation of the program activities amid COVID-19 is on halt due to some bottlenecks.
Congo sees increase in plague, at least 10 deaths this year
DR Congo is seeing an upsurge in cases of the plague, as the vast Central African nation also battles outbreaks of COVID-19 and Ebola. Since June, Congo has recorded at least 65 cases of the plague, including at least 10 deaths, in the eastern Ituri province according to Ituri provincial chief of health Dr. Louis Tsolu. While the plague is endemic in Ituri province, the number of cases is increasing and has already surpassed the total recorded in 2019 which had 48 cases and eight deaths, according to WHO.
Towards harmonization of microscopy methods for malaria clinical research studies
Microscopy performed on stained films of peripheral blood for detection, identification and quantification of malaria parasites is an essential reference standard for clinical trials of drugs, vaccines and diagnostic tests for malaria. The value of data from such research is greatly enhanced if this reference standard is consistent across time and geography. Adherence to common standards and practices is a prerequisite to achieve this. The rationale for proposed research standards and procedures for the preparation, staining and microscopic examination of blood films for malaria parasites is presented here with the aim of improving the consistency and reliability of malaria microscopy performed in such studies.
These standards constitute the core of a quality management system for clinical research studies employing microscopy as a reference standard. They can be used as the basis for the design of training and proficiency testing programmes as well as for procedures and quality assurance of malaria microscopy in clinical research.
Genetic diversity of Plasmodium falciparum in Grande Comore Island
Despite several control interventions resulting in a considerable decrease in malaria prevalence in the Union of the Comoros, the disease remains a public health problem with high transmission in Grande Comore compared to neighbouring islands. In this country, only a few studies investigating the genetic diversity of Plasmodium falciparum have been performed so far. For this reason, this study aims to examine the genetic diversity of P. falciparum by studying samples collected in Grande Comore in 2012 and 2013, using merozoite surface protein 1 (msp1), merozoite surface protein 2 (msp2) and single nucleotide polymorphism (SNP) genetic markers.
Agriculture &Coordination &Food Security Bill Brieger | 23 May 2018
Global Frameworks Link Malaria and Food Security
 Forty years ago the Alma Ata Declaration on Primary Health Care became one of the first global frameworks to consider health in the context of development.[i] Specifically the Declaration stated that, “Economic and social development, based on a New International Economic Order, is of basic importance to the fullest attainment of health for all and to the reduction of the gap between the health status of the developing and developed countries.” Within that, 8 essential services were articulated. One was “Promotion of food supply and proper nutrition,” and another emphasized, “Prevention and control of locally endemic diseases.” This set the stage for future efforts that could place malaria control and food security on an integrated platform.
Forty years ago the Alma Ata Declaration on Primary Health Care became one of the first global frameworks to consider health in the context of development.[i] Specifically the Declaration stated that, “Economic and social development, based on a New International Economic Order, is of basic importance to the fullest attainment of health for all and to the reduction of the gap between the health status of the developing and developed countries.” Within that, 8 essential services were articulated. One was “Promotion of food supply and proper nutrition,” and another emphasized, “Prevention and control of locally endemic diseases.” This set the stage for future efforts that could place malaria control and food security on an integrated platform.
Twenty years later world leaders came together to establish the Millennium Development Goals (MDGs),[ii] an 8-goal framework for tackling the most pressing development challenges. As part of Goal 1, Eradicate extreme poverty and hunger, Target 1.C aimed to halve, between 1990 and 2015, the proportion of people who suffer from hunger, which was thought to be best understood by analysing the different dimensions of food security. One dimension was “Nutritional failures are the consequence not only of insufficient food access but also of poor health conditions and the high incidence of diseases such as diarrhoea, malaria, HIV/AIDS and tuberculosis.” Thus Goal 6, Combat HIV/AIDS, malaria and other diseases,” set Target 6.C to have halted by 2015 and begun to reverse the incidence of malaria and other major diseases.
While recognizing some major successes in the MDGs, the global community again came together to conceptualize a new framework to take off after the MDG process ended in 2015. The new Sustainable Development Goals (SDGs) had 17 components and many sub-goals with the purpose of painting as full a picture of a desired social, economic, environmental, health and political landscape as possible.[iii] Goal 2 focused on ending hunger, achieving food security and improving nutrition, and promoting sustainable agriculture. Unlike Alma Ata and the MDGs, the health goal appears a bit diffuse: Goal 3 was to ensure healthy lives and promote well-being for all at all ages. Among 13 sub-goals was 3.3 that stated by 2030, end the epidemics of AIDS, tuberculosis, malaria and neglected tropical diseases and combat hepatitis, water-borne diseases and other communicable diseases.
A thorough reading of the three mentioned documents/frameworks importantly shows that malaria and food security do not exist in isolation. Their potential interaction and intersection happen in a context of poverty, the environment and climate change.
[i] World Health Organization and UNICEF. Declaration of Alma-Ata, International Conference on Primary Health Care, Alma-Ata, USSR, 6-12 September 1978. http://www.who.int/publications/almaata_declaration_en.pdf
[ii] United Nations. The Millennium Development Goals Report 2014. New York, 2014. http://www.un.org/en/development/desa/publications/mdg-report-2014.html
[iii] United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development. A/RES/70/1. sustainabledevelopment.un.org
Advocacy &Coordination &Partnership &Private Sector Bill Brieger | 11 Sep 2014
UN General Assembly Resolves to Fight Malaria
 GhanaWeb reported this morning that, “The United Nations General Assembly at its 68th Session, adopted Resolution A/68/L.60, “Consolidating Gains and Accelerating Efforts to Control and Eliminate Malaria in Developing Countries, Particularly in Africa, by 2015” by consensus.”
GhanaWeb reported this morning that, “The United Nations General Assembly at its 68th Session, adopted Resolution A/68/L.60, “Consolidating Gains and Accelerating Efforts to Control and Eliminate Malaria in Developing Countries, Particularly in Africa, by 2015” by consensus.”
Likewise the UN itself issued a press release confirming that in a final act the Assembly adopted this resolution in order to call for increased support for the implementation of international commitments and goals pertaining to the fight to eliminate malaria. GhanaWeb reiterated the UN’s message that, “with just less than 500 days until the 2015 deadline of the MDGs, the adoption of this resolution by the General Assembly reiterates the commitment of UN Member States to keep malaria high on the international development agenda.”
The UN Press Release explained that, “The resolution urged malaria-endemic countries to work towards financial sustainability to increase national resources allocated to controlling that disease, while also working with the private sector to improve access to quality medical services. Further, the resolution called upon Member States to establish or strengthen national policies, operational plans and research, with a view to achieving internationally agreed malaria targets for 2015.”
 This effort is consistent with moves two years ago in the 66th General Assembly when it called for “accelerated efforts to eliminate malaria in developing countries, particularly Africa, by 2015, in consensus resolution” (document A/66/L.58) where the “Consolidating Gains …” document was first shared. The draft of the 2012 resolution, according to the UN Press release was sponsored by Liberia on behalf of the African Group, and called on Member States, particularly malaria-endemic countries, to strengthen national policies and operational plans, with a view to scaling up efforts to achieve internationally agreed malaria targets for 2015.
This effort is consistent with moves two years ago in the 66th General Assembly when it called for “accelerated efforts to eliminate malaria in developing countries, particularly Africa, by 2015, in consensus resolution” (document A/66/L.58) where the “Consolidating Gains …” document was first shared. The draft of the 2012 resolution, according to the UN Press release was sponsored by Liberia on behalf of the African Group, and called on Member States, particularly malaria-endemic countries, to strengthen national policies and operational plans, with a view to scaling up efforts to achieve internationally agreed malaria targets for 2015.
The sad irony of Liberia’s current predicament wherein the Ebola epidemic is rendering it nearly impossible to provide malaria services should give us pause. According to Reuters, “Treatable diseases such as malaria and diarrhea are left untended because frightened Liberians are shunning medical centers, and these deaths could outstrip those from the Ebola virus by three or four fold.”
The new resolution (A/68/L.60) in calling for increases national resources allocated to controlling that disease from public and private sources demonstrates the importance of national commitment to sustain and advance malaria control into the era of malaria elimination. It is now up to local malaria advocates to ensure that their governments, as well as private sector and local NGO partners, follow through to guarantee the needed quantity and quality of malaria services.
Community &Coordination &Integration Bill Brieger | 06 Mar 2014
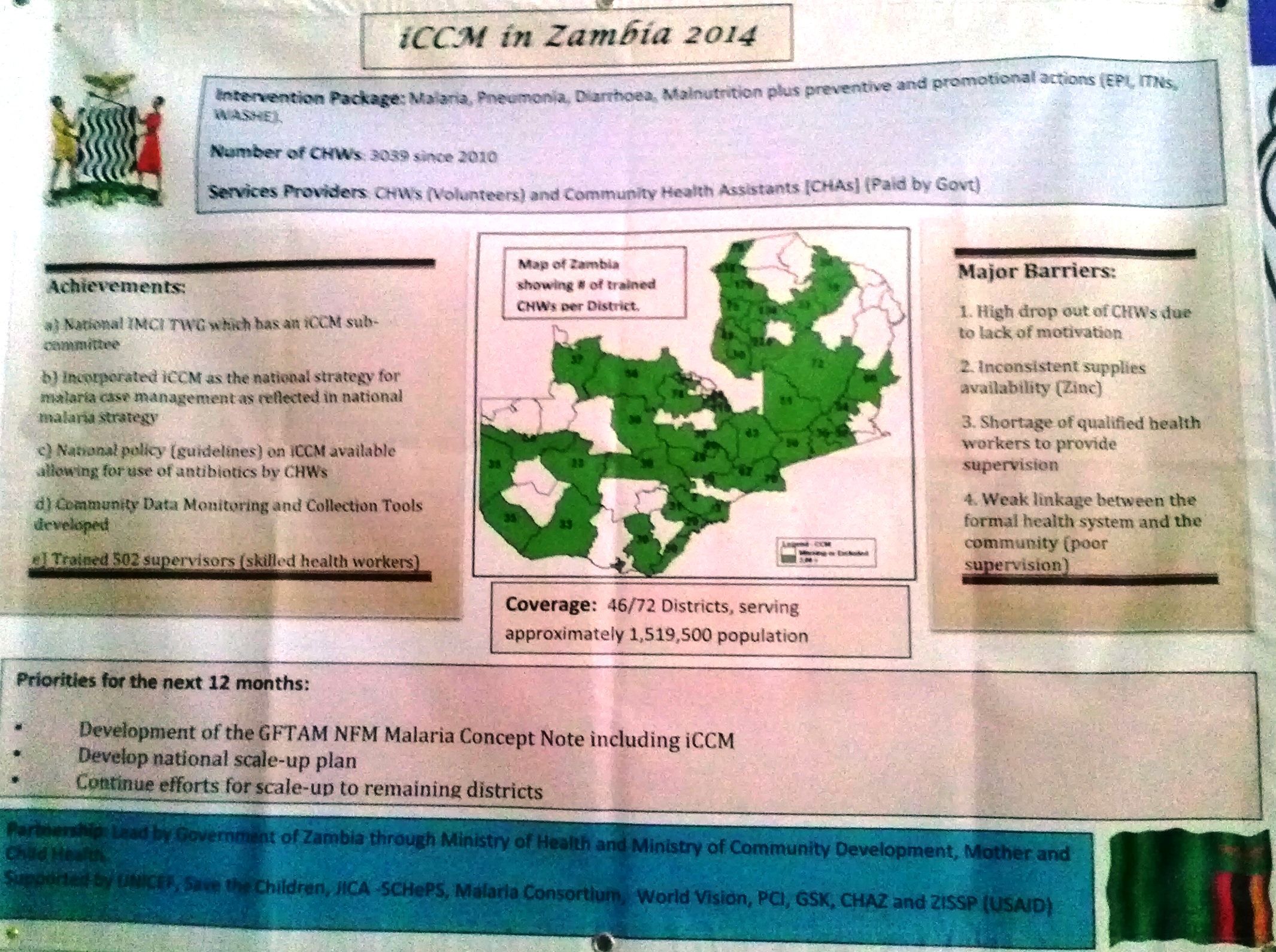
iCCM needs collaboration among varied stakeholders
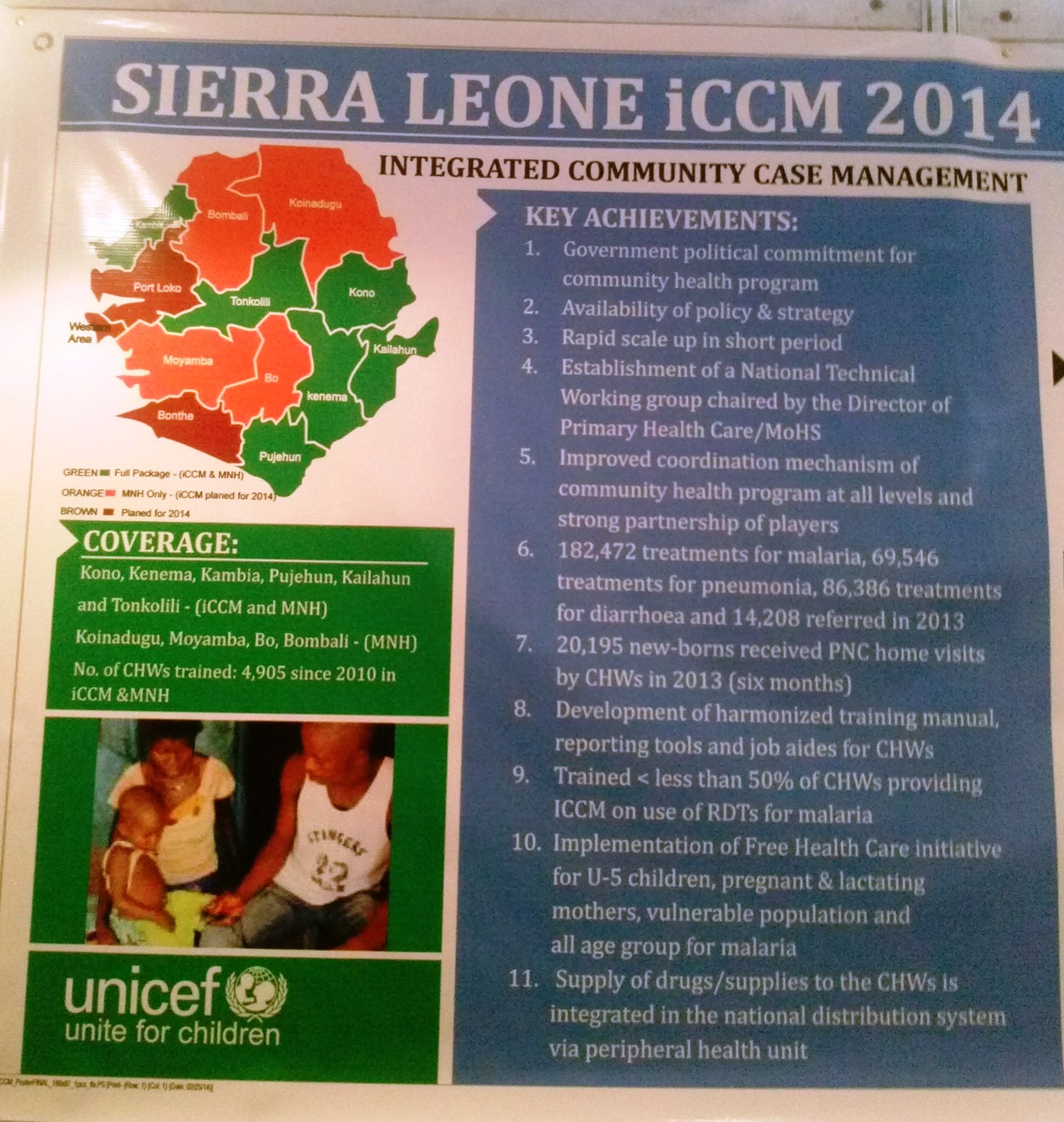 Integrated community case management (iCCM) of common illnesses, as we learned at the just completed evidence review symposium on iCCM in Accra, Ghana, requires a number of key inputs ranging from adequate procurement and supply of commodities, well stated supportive policies and human resources from the district to the clinic to the community. One input, the collaboration among stakeholders needs constant reinforcement.
Integrated community case management (iCCM) of common illnesses, as we learned at the just completed evidence review symposium on iCCM in Accra, Ghana, requires a number of key inputs ranging from adequate procurement and supply of commodities, well stated supportive policies and human resources from the district to the clinic to the community. One input, the collaboration among stakeholders needs constant reinforcement.
Although the project was not iCCM, an implementation research study in 8 sites in Africa that added a package of interventions to existing ivermectin distribution illustrates the need for stakeholder concurrence and collaboration. This 3-year community directed intervention (CDI) Tropical Disease Research Program effort (UNDP/World Bank/Unicef/WHO) was designed to add a package of interventions to the community’s ‘portfolio’ each year in a step-wise manner. These included antimalarials for community case management, insecticide treated nets, vitamin A and drugs for directly observed treatment of tuberculosis.
While ultimately the community directed approach to distributing these commodities resulted in better coverage in intervention districts than facility based service provision in the control areas, an important lesson from the project occurred in the start-up process the very first year. In fact no real commodity distribution took place that year as originally planned.
What the teams learned is that while community distribution of ivermectin had been taking place for at least 10 years in most of the districts, not all members of the district health teams (DHT) were fully aware of what the onchocerciasis focal person was doing. It had been hoped a bit naively that the DHT member in charge of immunization and vitamin A, the DHT focal point for malaria and the DHT member in charge of TB/Leprosy would gladly join their onchocerciasis colleague in making their services available through community volunteers.
 In reality the advocacy process took up the whole first year before other DHT members could be convinced that it was safe and appropriate for community members to take charge of a package of basic health commodities. In some locations, the TB/Leprosy program managers were never convinced.
In reality the advocacy process took up the whole first year before other DHT members could be convinced that it was safe and appropriate for community members to take charge of a package of basic health commodities. In some locations, the TB/Leprosy program managers were never convinced.
Even at start-up of onchocerciasis programs in the late 1990s it took much convincing of health workers to ‘allow’ communities to handle drugs like ivermectin. When introducing a larger package through CDI, it became necessary to start this process of convincing and seeking collaboration anew.
A basic iCCM package of ACTs, RDTs, ORS, Zinc and amoxicillin may not appear as complicated as the CDI package added to ivermectin distribution, but in truth a lot of stakeholder advocacy work is still needed. We learned at the Accra meeting that at minimum malaria and child health programs need to collaborate to provide the basic package and the funding that does with it. Different programs may in fact have different policies and guidelines. Different donors and different sections of the Ministry of Health must be willing to bring their efforts and resources together and share. This is as much a political as it is a technical process, and scientific evidence that health care interventions delivered in the community save lives may not be enough to overcome politics and vested program interests.
The 300+ delegates to the iCCM symposium are returning home over the next few days. Hopefully the momentum of the conference will carry them on to engage in collaboration, not only with their colleagues who also attended, but also with those who did not attend and benefit from the sharing of evidence and experience. It will take a team of people with varied interests to make iCCM a success.
Coordination &Monitoring Bill Brieger | 11 Nov 2013
Challenges in Malaria Health Information Collection and Coordination
Today This Day Live News reported on challenges of data coordination in the health system in Nigeria. Ndubuisi Francis reported that, “The multiplicity of conflicting data on health by various agencies is a major impediment to an effective and efficient health care delivery system in the country. Director, Disease Control and Immunisation, National Primary Health Care Development Agency (NPHCDA), Dr. Emmanuel Abanida, said resolving the conflict in the national health management information system (HMIS) is a step towards getting the system right.” The problem is not unique to Nigeria.

Health facility staff compile monthly data reports
To learn more about how this problem affects malaria data we discussed with two staff of the Jhpiego office in Abuja, Gbenga Ishola and Bright Orji, who have been involved for many years in malaria monitoring and evaluation activities at national, state and local levels. The results of this discussion follow:
1. Incorporating Community Health Worker Data into HMIS
As the country moved toward community case management to reach coverage targets, the HMIS has worked with NMCP to establish a community data collection template. However, the level of utilization of the community level register is poor. Also the integration of this into facility output remains a key challenge. Furthermore, there has not been a feedback mechanism to the community of data collected from them. So, it is not only collection of data but use of data for decision-making whether at the Local Government (LG) level, facility or community remains part of the challenge.
2. Movement of Data from Facility to District to State to National
There is an existing data flow pattern. Data from facility HMIS registers are expected to be collated on monthly basis into a monthly summary form at facility level. The summary forms are sent to the Local Government Monitoring and Evaluation Unit which then sends this to the state level. Data flow is also not as smooth as intended. Most often facilities do not collate and send to the LG, and thus state data reporting that is suppose to be quarterly is distorted. The obvious complaint is always logistics.
The National Malaria Control Program (NMCP) monitors state data reporting by aggregating total number of facilities reporting each month and determining reporting rate for the states. Each state reports total number of health facilities in the state, and how many of these facilities submitted a monthly report during review period. For example, if a state has 1,000 health facilities but only 500 submitted monthly reports, the state would have scored 50% in data reporting. This is to encourage state to improve on data collection and reporting and is part of the report and discussions at the annual malaria program’s manager meetings.
3. Parallel Reporting Systems
There are two examples of parallel systems through which malaria data move. The National Primary Health Care Development Agency, a section of the Ministry of Health responsible for assisting LGs strengthen their primary care systems collects health data from those facilities in addition to the facilities reporting through the HMIS. Recently the Director of the HMIS indicated that his unit is trying to harmonize the existing system. The completeness of each system varies depending on how LGs and states decide to report.
 Since the HMIS collects only a limited selection of malaria indicators, the NMCP makes an effort to collect more detailed statistics of all services. Some of the indicators monitored by NMCP are not in HMIS. The consequence is that health workers often abandon the NMCP register because it contains more entries than HMIS.
Since the HMIS collects only a limited selection of malaria indicators, the NMCP makes an effort to collect more detailed statistics of all services. Some of the indicators monitored by NMCP are not in HMIS. The consequence is that health workers often abandon the NMCP register because it contains more entries than HMIS.
The HMIS collects 1) Long-lasting insecticide-treated nets (LLINs) provided and 2) doses of Intermittent Preventive Treatment (IPTp) given (1st and 2nd). NMCP additionally tracks number of fever cases, Rapid Diagnostic Tests (RDTs) conducted (and whether RDT results are negative, positive or invalid), and antimalarial medicines administered (whether quinine or ACT).
While the National HMIS unit is working to harmonize the data collection formats for all diseases including malaria cases, bringing the NMCP to participate in meetings and discussions has been a major problem. This makes it very difficult for the HMIS to be able to quote data relating to specific diseases when necessary.
4. Special Data Requirements
As in other countries, the Global Fund expects countries to report of a regular, quarterly basis on achievements based on their currently operating grant. The data required for these reports is essential for maintaining the flow of funding, but this information is not necessarily within the basic HMIS set of indicators. Global Fund is interested in consumption data for forecasting for national needs, but this has been very difficult to collect due to some of the above challenges.
Bright Orji and Gbenga Ishola review malaria in pregnancy data with local government nurse-midwife
The number and detail of indicators reported to the Global Fund for Nigeria’s Round 8 malaria grant reflect the complexity of reporting required that would not be included in HMIS. Below are a few examples of the malaria treatment related indicators only. HMIS would not be collecting program process data like training and does not really reach the private sector.
- Number of children under five with uncomplicated malaria receiving ACT treatment according to National guidelines (all oints of care)
- Number of children under five with uncomplicated malaria receiving ACT treatment according to National guidelines through the public sector
- Number of people (over 5) with uncomplicated malaria receiving ACT treatment according to National guidelines through the public sector
- Number of person (over 5) with uncomplicated malaria receiving ACT treatment according to National guidelines through the private sector
- Percentage of participating health facilities in the public sector reporting no stock out of ACTs for 1 week or more within the last 3 months
- Number of health care providers trained in malaria case management and prevention
- Number of CSO members trained on case mangement and prevention of malaria
- Number of Health care providers trained on pharmacovigilance
In order eventually to eliminate malaria detailed monitoring and surveillance data are needed in real time. Coordinating these data needs with a routine national HMIS will always be challenging because disease elimination is anything but a routine process.
Burden &Coordination &Eradication Bill Brieger | 13 Jul 2013
900 Days Left to Make a Big Difference in Malaria as African Ministers of Health Learn in Abuja
A Breakfast Briefing was given to African Ministers of Health and Foreign Affairs on 13th July 2013 in Abuja, Nigeria to review progress in Africa’s fight against malaria and to announce a new initiative to support 10 high-burden countries as part of the Special African Union Summit on HIV/AIDS, Tuberculosis and Malaria.
 Dr Fatoumata Nafo-Traoré, Executive Director, Roll Back Malaria (RBM) Partnership in her welcome address) acknowledged the high level of commitment of partners and the high level of leadership from endemic countries over the past decade in the fight against malaria resulting on 44 countries seeing a > 50% reduction in malaria cases, but we cannot rest in the face of financial and technical challenges.
Dr Fatoumata Nafo-Traoré, Executive Director, Roll Back Malaria (RBM) Partnership in her welcome address) acknowledged the high level of commitment of partners and the high level of leadership from endemic countries over the past decade in the fight against malaria resulting on 44 countries seeing a > 50% reduction in malaria cases, but we cannot rest in the face of financial and technical challenges.
Dr Mustapha Sidiki Kaloko, the African Union Commission’s Commissioner for Social Affairs in his opening remarks reminded us that external funding has never been guaranteed, and as it is ebbing we need to scale up domestic financial support. The AU will work with all stakeholders to help close the $4b gap and not let gains reverse. In order not to lose momentum innovative domestic funding models are needed.
Joy Phumaphi, Executive Secretary of the African Leaders Malaria Alliance (ALMA) delivered the ALMA Scorecard update. She noted that the scorecard provides a roadmap and pushes countries to demonstrate results. Very positive results in terms of adopting policies that oppose artemisinin monotherapies and promote community case management are the norm now.
 The challenge is the low scores on public sector management and effective use of existing resources. Efficiency gains could deliver up to 40% more services with available money. Continued scorecard success also depends on global attention remaining focused on Africa as post MDG goals are being set.
The challenge is the low scores on public sector management and effective use of existing resources. Efficiency gains could deliver up to 40% more services with available money. Continued scorecard success also depends on global attention remaining focused on Africa as post MDG goals are being set.
Dr Robert Newman, Director of the WHO Global Malaria Programme (WHO-GMP) introduced the new Larval Source Management (LSM) Manual. He told the gathering that the new LSM Manual was a result of advocacy by Nigeria’s Minister for Health. IRS and ITNs have been success stories, but we need to use all available tools in appropriate manners. LSM has a unique niche where one finds discrete, fixed and definable water bodies as opposed to water in multiple diffuse sources like cattle foot prints on a rutted road that come and go over days.
Larvicides are expensive and labor intensive and need regular monitoring. People need to remember that environmental management is another larva control tool. With all vector measures “commodities don’t deliver themselvesâ€, but require commitment and action of people at all levels form the national to the community.
Dr Richard Kamwi, Hon. Minister of Health, Namibia, shared that in the 1990s there were 7,000 malaria deaths in his country annually, but only 4 in 2012. Namibia has a mixed strategy especially in the northern border area, and is close to pre-elimination.
Dr Robert Newman, Director of WHO-GMP gave a presentation on the Malaria Situation Room concept and explained that even though progress has been made and millions of lives saved, there are over 219 million cases of malaria annually and 660,000 deaths/ A disproportionate burden of malaria deaths even now is in African children under five years of age. We have responsibility for these children. This burden is focused on 10 countries which account for 70% of malaria cases in Africa and 56% globally.
The Malaria Situation Room will be a way to collate data on funding, intervention, commodities and results. International partners will continue to support all endemic countries, but malaria elimination will remain elusive unless more coordinated action is aimed at high burden areas.
With only 900 days left before the MDGs reach their target date (end of 2015), we want to anticipate and prevent problems like stock-outs, but wait to hear that there have been no antimalarials in clinics for over a month. We want to be proactive in the face of potential dis-investment to protect 10 years of progress which could be undone in only one malaria transmission season.
 Dr Alexandre Manguale, Hon. Minister of Health, Mozambique noted that his country is one of the ten in the “situation room.†Mozambique has made great progress in case reduction in the south with support from the cross border Lubombo Spatial Development Initiative. The rest of the country poses special challenges with logistics and weather (flooding). Under these circumstances partners need to coordinate and be flexible in response to gaps and bottlenecks. Information gathered and shared through the situation room will make this possible.
Dr Alexandre Manguale, Hon. Minister of Health, Mozambique noted that his country is one of the ten in the “situation room.†Mozambique has made great progress in case reduction in the south with support from the cross border Lubombo Spatial Development Initiative. The rest of the country poses special challenges with logistics and weather (flooding). Under these circumstances partners need to coordinate and be flexible in response to gaps and bottlenecks. Information gathered and shared through the situation room will make this possible.
At this point Dr Newman, Dr Nafo-Traoré and Dr Kaloko officially launched the Malaria Situation Room with a ribbon-cutting. Now the work begins to make this ‘room’ a pro-active place to eliminate malaria.
Coordination &Funding Bill Brieger | 04 Dec 2012
RBM Harmonization Working Group Confronts Malaria Program Challenges
The 13th meeting of the RBM HWG is taking place in Dakar, Senegal this week. Some thoughts about the. Current status of malaria programs emerged from member experiences and are shared here.
Dakar, Senegal this week. Some thoughts about the. Current status of malaria programs emerged from member experiences and are shared here.
Since the cancellation of the Global Fund Round 11 may have been denied around one billion dollars annually. If funding does not fully resume until 2014, we could be looking at nearly $3B loss.
In the meantime there is need to help countries spent what remains most efficiently. Effort to secure approval for phase two renewal of existing grants is a priority.
Some countries may have many donor partners but still face problems due to lack of coordination. Problems come when countries do not budget for major activities likely implementation of LLIN (net) campaigns. Procurement and supply management problems persist. Stock-outs are the resulting “disease” but we need to find the root causes.
Not all partners bring funds and commodities, but their input is still important. For example Peace Corps has been making important contributions in advocacy and community education.
When there are funding gaps we need to document the impact. Lives may be lost. Advocacy is needed using country case studies.
As malaria prevalence reduces there is still a possibility of outbreaks, especially in context if cross border situations. Better epidemic response planning is needed with full collaboration of neighboring countries. The challenge is that funding is still country based.
Vigilance is needed to determine how the new Global Fund financing processes will affect malaria prospects.
Community &Coordination &Treatment Bill Brieger | 06 Dec 2011
The practical side of managing integrated Community Case Management
Jhpiego presented its recent experiences in building iCCM onto an existing malaria program in Akwa Ibom State, Nigeria, during the American Society of Tropical Medicine and Hygiene meeting today.
Establishing Integrated Community Management of Malaria, Pneumonia and Diarrhea in Two Selected Local Government Areas, Akwa Ibom State, Nigeria
William Brieger, Bright Orji, Emmanuel Otolorin, Eno Ndekhedehe, Jones Nwadike
Many intervention studies have demonstrated that local volunteers practicing integrated Community Case Management (iCCM) can increase access to appropriate lifesaving interventions. These interventions are important for giving us confidence in community capacity, but key management questions remain on how to establish, manage and expand iCCM efforts in order to reach Roll Back malaria Targets and Millennium development Goals.
The Nigeria MIS 2010 revealed inappropriate treatment andpPoor community response to malaria interventions. Among children (less than 5 years) with fever 2 weeks preceding the survey, only 26% took any antimalarial and only 3.2% took an ACT. Malaria treatment was largely by presumptive diagnosis.
A initial management decision for iCCM is what combination of interventions will comprise a start-up package. Nigeria’s Malaria Plus Package includes 19 potential health interventions at the community level, but clearly a program could not afford, let along manage the simultaneous implementation of all 19.
Jhpiego had successfully piloted community directed interventions (CDI) for malaria in pregnancy (MIP) control interventions. Further formative research in two selected Local Government Areas showed poor access to malaria treatment for all age groups due to distance from health facility, poverty, financial constraints, and perceptions of health services quality. Therefore, iCCM was added to CDI for MIP prevention to improve treatment access and coverage for all age groups.
Teamwork was a necessary part of the process to guarantee sustainability. This included Local Government Health departments, Technical Assistance from Jhpiego (affiliate of Johns Hopkins University), World Bank Booster Project in State Ministry of Health Malaria Unit, a core Training and Supervisory team from the Ministry and iCCM/Malaria Plus Package Guidelines from National Malaria Control Program.
Stakeholder Challenges posed management problems including State Program Manager’s skepticism that community members can perform RDTs correctly, Health facility workers’ poor acceptance of RDTs as opposed to using their clinical judgment, and provider’s reluctance to trust communities with antibiotics.
 Health Facility Management Challenges were numerous including procurement problems as needed medicines come from different funding sources. There was difficulty in sourcing RDTs that come with ready and easy to use components.
Health Facility Management Challenges were numerous including procurement problems as needed medicines come from different funding sources. There was difficulty in sourcing RDTs that come with ready and easy to use components.
Procurement and supplies of AMFm drugs were delayed due to cumbersome, delayed drug registration processes. Sharps and waste disposal for RDTs needed attention. Finally there were multiple statistics tracking registers, as no one register captures all the indicators – a burden M&E personnel.
Community Challenges started with the belief that ‘blood of someone alive cannot be buried’ such that disposing of RDT cassette by burial would mean burying the person alive. Community members perceived that person has malaria even if RDT is negative. Cpommunity volunteers requested for incentives and motivation as new tasks included.
Addressing Stakeholder Challenges we held Stakeholders consensus meetings helped address reluctance by the health ministry to allow RDT use at the community level. Consensus meetings created an opportunity for programs to integrate as IMCI, RH and Malaria departments trained providers
Solving health facility management Challenges required that We work with other malaria partners to identify reliable sources of RDTs and drugs. Linking with a local pharmaceutical company already registered with AMFm helped fast tract supplies of ACTS.
 Community Dialogue was essential to overcome village concerns. Through dialogue the community agreed on incineration as an acceptable method of RDT disposal. Engaged communities accepted that only positive RDT-results need ACTs. Volunteers’ demands for incentives challenged by leaders who reminded the volunteers that they were accountable to their neighbors, friends and relatives in the village. Community self-monitoring was undertaken and two volunteers who did not deliver their ACTs were fined one-goat each by the community for failing to provide services.
Community Dialogue was essential to overcome village concerns. Through dialogue the community agreed on incineration as an acceptable method of RDT disposal. Engaged communities accepted that only positive RDT-results need ACTs. Volunteers’ demands for incentives challenged by leaders who reminded the volunteers that they were accountable to their neighbors, friends and relatives in the village. Community self-monitoring was undertaken and two volunteers who did not deliver their ACTs were fined one-goat each by the community for failing to provide services.
Lessons Learned were foremost the need for consensus building among partners on roles and extent of services to be provided by volunteers. Continual community education and dialogue prior to the initial start-up iCCM provision and throughout is required. Without attention to these start-up processes we cannot expect to reach our endpoint coverage indicators and develop a scalable and sustainable program.
Coordination &Treatment Bill Brieger | 05 Jul 2011
Malaria Treatement: right hand, left hand
Nigeria adopted artemisinin-based combination therapy as its first line of malaria treatment in 2005. While it did not ban chloroquine, it has actively discouraged its use since efficacy studies across the country showed high levels of parasite resistance. Likewise Nigeria has tried to confine sulphadoxine-pyrimethamine (SP) for use at intermittent preventive treatment during pregnancy (IPTp), and discourage its use for case management.
Specifically the National Malaria Control Program (NMCP) recommends artemether-lumefantrine and artesunate-amodiaquine, for which there are only few WHO ‘prequalified’ producers, for first line treatment of uncomplicated malaria. Based on WHO recommendations the NMCP also recommends against artesunate monotherapies (i.e. medicines not containing a combination of drugs).
 One is not surprised to find inappropriate malaria drugs in patent medicine shops around the country (see picture). Unfortunately the National Agency for Food and Drug Administration and Control approves drugs based more on safety than on appropriateness to control efforts. Thus, the chloroquine found in shops will not kill you, but it will not cure your malaria either.
One is not surprised to find inappropriate malaria drugs in patent medicine shops around the country (see picture). Unfortunately the National Agency for Food and Drug Administration and Control approves drugs based more on safety than on appropriateness to control efforts. Thus, the chloroquine found in shops will not kill you, but it will not cure your malaria either.
With this in mind it came as a shock to see local government clinics stocking chloroquine and artesunate monotherapies, among others. These were in clinics that were being supplied by the National Health Insurance Scheme using Millennium Development Goals special funds to provide free treatment for pregnant women and children less than five years of age. This laudable goal of reaching the poor can be undermined when drugs with questionable therapeutic value are provided.
The NHIS drug list for malaria includes the following in various forms (tablets, syrups, suspensions, injections):
- Artesunate
- Chloroquine
- SP+Meflaquine
- Dyhydroartemisinin
- Proguanil+Pyrimethamine
- Quinine
- SP
- Mefloquine
- Artemeter
While the SP in the list should ideally be used for antenatal clinic services, one is not sure this happens since several of the clinics visited had no stock of SP, but plenty of chloroquine syrup bottles – a formulation that is not very stable in these climates.
We encourage the NMCP to take stock of malaria drug stocks – basically, there are many national and international agencies supplying malaria medicines at national, state and local government level. They should be brought together so that one coordinated national malaria drug policy is enacted. Only then will the public receive effective malaria treatment.