Anemia &coronavirus &COVID-19 &IPTp &IRS &ITNs &Larvicide &Malaria in Pregnancy &Morbidity &Mortality &Mosquitoes &Sahel Bill Brieger | 03 Oct 2020
Malaria News Today 2020-10-02/03
Recent news and abstracts include mosquito control using solar disruption of of larval habitats and plants that repel the insects around homes. The challenges of malaria related anemia in pregnancy is discussed. Malaria cases increase in Mali and Mozambique, but in the latter, deaths actually decrease. Malaria parasites have ways of making people more attractive to mosquito bites. Finally covid-19 has not disrupted malaria work as much as anticipated. Read more at the links in the sections below.
Improved Mosquito Control with Solar Power Machine that Causes Ripple Effect
Kristina Panos writes that mosquito haters of the world, rejoice! A few years ago we told you about the first version of this solar-powered mosquito repellent that works by disturbing the surface of standing water. Since then, the project has received worldwide attention, and [Pranav] is back with Solar Scare Mosquito version 2.0 in time for the the 2020 Hackaday Prize.
The idea’s still the same as before: let mosquitoes lay their eggs in the standing waters of tanks and swamps, then disturb the water with vibrations so the larvae on the surface can’t breathe. As smart as this simple idea is, version 2.0 is even smarter. It has a microphone that listens to the wing-beat frequencies of mosquitoes that like to hang around places like that. Inside there’s an Arduino MKR GSM to run the ripple-generating air pump, detect water from the sensor, and gather data from the microphone.
With a network of these devices all reporting data, [Pranav] envisions an early warning system for mosquito-borne epidemics that works by alerting the locals through their phones. Solar Scare Mosquito has come a long way since 2014.
Malaria cases spike in northern Mali
Malaria cases in northern Mali have spiked, according to medical workers, claiming 23 lives in the often lawless desert region last week alone. Mali’s ministry of health said this week that 59 people have died of malaria in the north since the start of the year, almost double the number of deaths over the same period last year.
Already struggling to curb coronavirus, the poor Sahel country is also fighting a brutal jihadist insurgency active in the north and centre of the country.
A powerful attractant: Malaria parasites lure blood-sucking mosquitoes
The malaria parasite’s gametocyte-stage has been demonstrated in the field to heavily manipulate the blood-seeking behaviour of vector mosquitoes through increasing the appeal of biting an infected host.
Plasmodium parasites, the causative agents of Malaria in humans and animals, are well known for manipulating both their human and mosquito hosts as a way of maximising the probability of interactions between them, thereby increasing the chance malaria parasites are transmitted from host to host. One way in which these devious parasites have been shown to increase the probability of host interaction is during their transmissible (gametocyte) stage.
This is achieved by inducing host red blood cells to produce volatile compounds that attract malarial vector species, such as mosquitos in the Anopheles family. The increase in production of volatile compounds, such as certain aldehydes and terpenes, by host red blood cells was shown back in 2017 to be specifically induced by a gametocyte-produced molecule called (E)-4-hydroxy-3-methyl-but-2-enyl pyrophosphate, also known as HMBPP.
Malaria campaigns fight off Covid disruptions to deliver programmes
Almost all planned work against the disease has gone ahead this year, delivering nets, drugs and the world’s first malaria vaccine. More than 90% of anti-malaria campaigns planned this year across four continents are on track, despite disruptions caused by the coronavirus pandemic, according to new research.
The delivery of insecticide-treated nets and provision of antimalarial medicines in the majority of malaria-affected countries across Africa, Asia and the Americas were still going ahead, a high-level meeting organised by the RBM Partnership to End Malaria heard on Thursday.
Malaria associated with increased prevalence of anemia during pregnancy
Ken Downey Jr. and colleagues conducted a study in seven sub-Saharan African countries demonstrated an association between malaria and an increased prevalence of anemia among pregnant women, according to findings published in BMC Pregnancy and Childbirth.
“Pregnant women in sub-Saharan Africa suffer a double burden of malaria and HIV infections, and these infections interact with each other to cause anemia,” Ssentongo told Healio. “If not treated, the risk of the mother and the unborn baby dying is high. Multipronged strategies to prevent and treat malaria in HIV pregnant women are critical to ensure the survival of the mothers and their unborn babies.”Paddy Ssentongo, MD, MPH, a research assistant professor at Penn State University,
Mozambique: Malaria Cases Increase, Malaria Death Toll Declines
 From January to August, 442 people in Mozambique are known to have died from malaria, according to Health Minister Armindo Tiago. Speaking at the launch of a National Home Spraying Campaign, Tiago said the malaria death toll, in the first eight months of the year, was significantly lower than that recorded in the same period in 2019, when 562 people died of the disease.
From January to August, 442 people in Mozambique are known to have died from malaria, according to Health Minister Armindo Tiago. Speaking at the launch of a National Home Spraying Campaign, Tiago said the malaria death toll, in the first eight months of the year, was significantly lower than that recorded in the same period in 2019, when 562 people died of the disease.
But although fewer people are dying of malaria, the number of malaria cases has actually increased – from 7.86 million cases in January-August 2019 to 8.36 million in the same months this year. The number of cases rose by 6.4 per cent, but the number of deaths fell by 21.4 per cent. Thus there is the drive to persuade families to change their behaviour.
The Plants That Keep Mosquitoes Away
Protect outdoor areas from mosquitoes and bugs to enjoy evenings outside. Including the following plants in a home garden can provide homeowners with some important weapons in the war against mosquitoes.
 1. Citronella Plants: You may already be familiar with citronella plants, as they are known for emitting a strong smell that mosquitoes find objectionable. This group of plants contain citronellal, the active ingredient commonly found in mosquito repellents like citronella patio candles or sprays.
1. Citronella Plants: You may already be familiar with citronella plants, as they are known for emitting a strong smell that mosquitoes find objectionable. This group of plants contain citronellal, the active ingredient commonly found in mosquito repellents like citronella patio candles or sprays.
2. The Mint Family: Some members of the mint family have the power to repel mosquitoes, or at least take the sting out of their bites. Check Lemon Balm, Peppermint, Basil, Lavender, Sage, and Catnip.
3. Flowers: Believe it or not, ornamental plants can actually do double duty and function as mosquito repellents. Even better, these plants love sun and are drought resistant. Marigolds, and their relative, tarragoncontain pyrethrum, an ingredient found in many insect repellents. Verbena is a lemon-scented, easy-to-grow perennial. Citrosum is also named “the mosquito plant,” and is one of the best plants in the game for repelling mosquitoes.
Epidemiology &IPTp &ITNs &Malaria in Pregnancy &Morbidity &Treatment Bill Brieger | 26 Jun 2017
Burundi: when will citizens see real protection from malaria?
Preliminary findings from Burundi’s 2015-16 DHS have been made available. The country has a long way to go to meet targets for basic control of malaria.
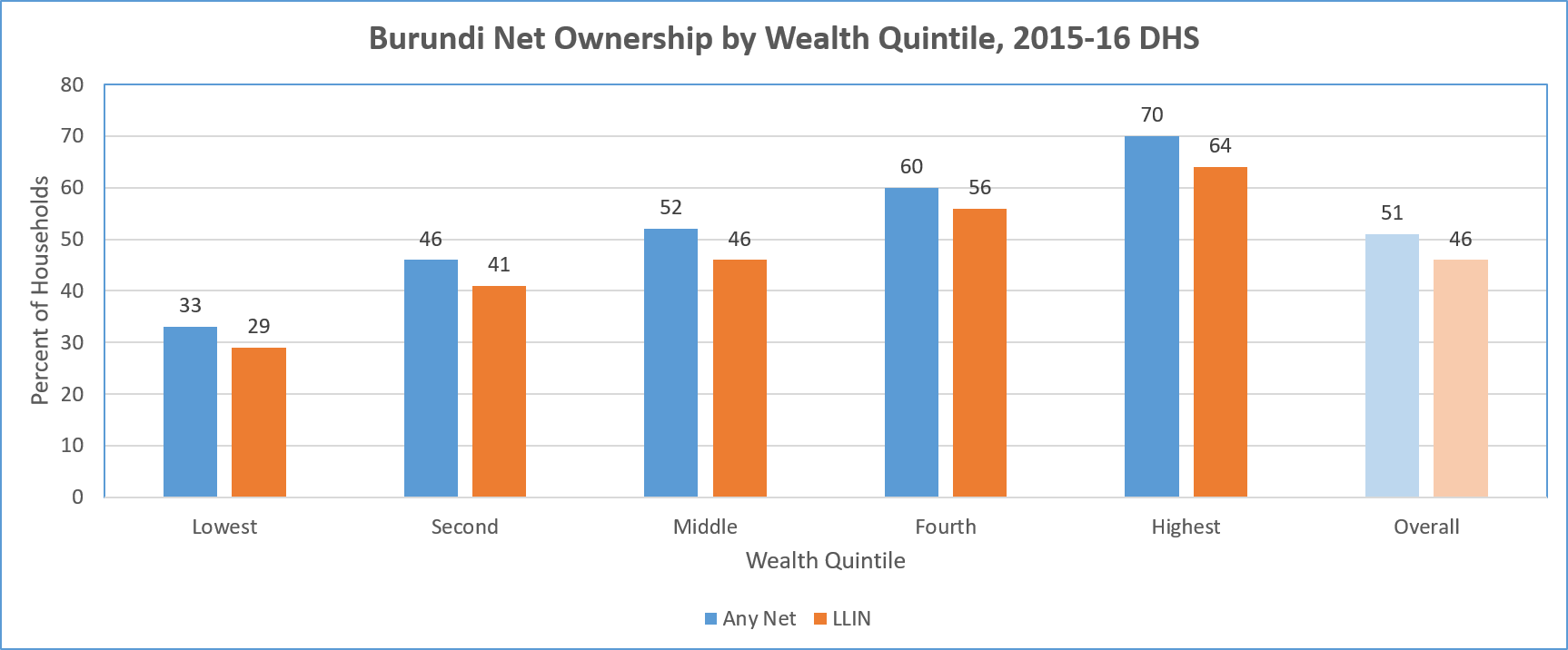 LLIN availability by household is an overall disappointing 32%. Ironically there is greater coverage of households in in urban areas (50%) than rural (30%). There is also great variation among the provinces with 52% coverage in Bujumbura metropolitan but only 19% in Canzuko. The overall average is less than one treated net per household.
LLIN availability by household is an overall disappointing 32%. Ironically there is greater coverage of households in in urban areas (50%) than rural (30%). There is also great variation among the provinces with 52% coverage in Bujumbura metropolitan but only 19% in Canzuko. The overall average is less than one treated net per household.
A major concern is equity. The chart above shows a steep gradation from 19% coverage among the lowest fifth of the wealth quintile, up to 48% in the highest. Even in households that have at least one net, only 17% of of people slept under a net the night before the survey.
In terms of use by those traditionally defined as vulnerable, the DHS shows only 40% of children below 5 years of age overall slept under a treated net the night prior to the survey. Even in households that own at least one net, 78% of these children slept under one.
A similar pattern is seen for treated net use by pregnant women. Overall 44% slept under a treated net, and 84% did so in households that owned at least one treated net. The internal household dynamics of net use where one is available does appear to favor these two groups.
Overall coverage of Intermittent Preventive Treatment for pregnant women is very low. Less than 30% of pregnant women received even the first dose of SP. This decreased to 21% for two doses and 13% for three. In contrast to net coverage, more rural women (31%) received the first dose of IPTp than urban ones (19%).
 Nearly 40% of children below five years of age were found to have had a fever in the two weeks preceding the survey. Among those care was sought for only two-thirds. Eleven percent of those with fever received an artemisinin-based combination therapy drug. The report did not mention whether these children had received any testing prior to treatment, so appropriateness of treatment cannot be judged. Prevalence testing of the children in the sample found 38% with parasitemia. Therefore one might assume that more children should have received ACTs.
Nearly 40% of children below five years of age were found to have had a fever in the two weeks preceding the survey. Among those care was sought for only two-thirds. Eleven percent of those with fever received an artemisinin-based combination therapy drug. The report did not mention whether these children had received any testing prior to treatment, so appropriateness of treatment cannot be judged. Prevalence testing of the children in the sample found 38% with parasitemia. Therefore one might assume that more children should have received ACTs.
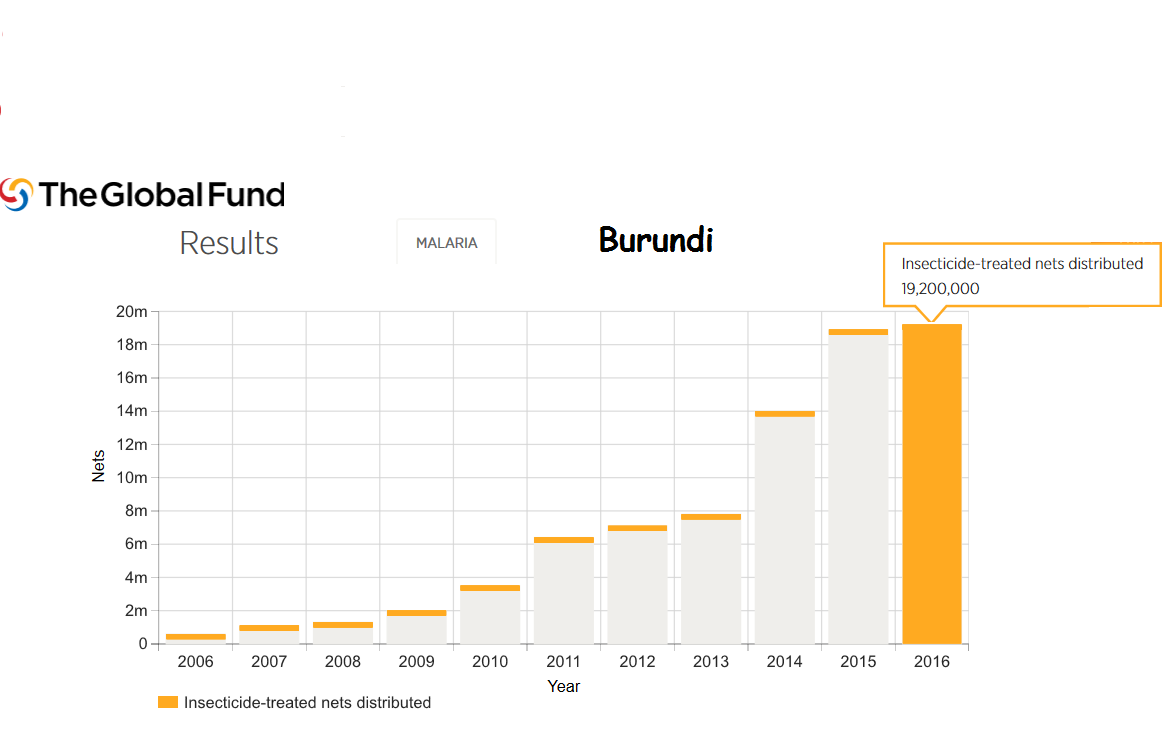
Burundi still faces major political and social challenges. Even so Burundi is the recipient of malaria support from the Global Fund. For example 18 million LLINs were distributed in 2015 and 19 million in 2016.
Much work is needed to bring Burundi even close to universal coverage of malaria interventions. In today’s climate of questionable donor commitment, it is hoped that regional partners may play a role since malaria knows no boundaries.
IPTp &ITNs &Morbidity &Treatment Bill Brieger | 22 Jun 2016
Tanzania – Malaria Indicators Low, Still Need Work
Success in the war against malaria is not guaranteed. Two articles to that effect have appeared The Citizen of Dar es Salaam following presentation of findings from the most recent (2015-16) Tanzania Demographic and Health Survey (DHS)/Malaria Indicator Survey (MIS).
 On Tuesday (21 June 2016) the news story noted the increase in malaria prevalence among children below the age of 5 years, which was attributed to “the decline in the use of mosquito nets and low distribution of nets to households.” Then in a Wednesday (22 June 2016) Editorial, the paper noted that this “backtracking” is a “worrisome situation, for malaria is a problem that puts such a heavy burden on the government and the country’s economy.”
On Tuesday (21 June 2016) the news story noted the increase in malaria prevalence among children below the age of 5 years, which was attributed to “the decline in the use of mosquito nets and low distribution of nets to households.” Then in a Wednesday (22 June 2016) Editorial, the paper noted that this “backtracking” is a “worrisome situation, for malaria is a problem that puts such a heavy burden on the government and the country’s economy.”
 A look at the preliminary DHS does confirm the concerns about insecticide treated nets (ITNs). After nearly 10 years of progress, reported ITN availability in households declined. This was reflected in a drop in reported use by children below 5 years of age as well as pregnant women. It should be noted that targets set in 2000 in the Roll Back Malaria Abuja Declaration had been 80% by the year 2010, and those had almost been achieved in 2012, but the fall to around 50% in 2015-16 is discouraging.
A look at the preliminary DHS does confirm the concerns about insecticide treated nets (ITNs). After nearly 10 years of progress, reported ITN availability in households declined. This was reflected in a drop in reported use by children below 5 years of age as well as pregnant women. It should be noted that targets set in 2000 in the Roll Back Malaria Abuja Declaration had been 80% by the year 2010, and those had almost been achieved in 2012, but the fall to around 50% in 2015-16 is discouraging.
Another preventive measure has also faced difficulty. Pregnant women should receive doses of Sulfadoxine-pyrimethamine (SP) as part intermittent preventive treatment (IPT) during antenatal care (ANC). Until 2012 the recommendation was two contacts, but the World Health Organization has raised this to three or more depending on the number of times a woman attends ANC. So far IPT has not reached 40% or half of the Abuja target.
 This low IPT coverage is ironic since most women attend ANC at least once in Tanzania. At present only 68% of women who had been pregnant received the first dose of IPT even though 98% registered for ANC. Granted that some may have registered in their first trimester when they would not yet be eligible for IPT, but the gap is quite large and signals missed opportunities, which are often caused by stock-outs. Even though the proportion of women attending up to ANC visits could be better, these attendances should produce better delivery of the 3rd IPT dose.
This low IPT coverage is ironic since most women attend ANC at least once in Tanzania. At present only 68% of women who had been pregnant received the first dose of IPT even though 98% registered for ANC. Granted that some may have registered in their first trimester when they would not yet be eligible for IPT, but the gap is quite large and signals missed opportunities, which are often caused by stock-outs. Even though the proportion of women attending up to ANC visits could be better, these attendances should produce better delivery of the 3rd IPT dose.
 Malaria can also be controlled through prompt and appropriate treatment. While testing and treatment of children with appropriate artemisinin-based combination therapy (ACT) has increased, this are is still problematic. In particular, while WHO recommends that all cases of fever should be tested, less than a third received a test (rapid diagnostic test – RDT or microscopy). Testing helps distinguish malaria from other fevers, and ACTs should not be given unless malaria is confirmed. We can see that more ACTs are provided than the number who were tested, so treatment based solely on signs and symptoms is still the norm. Again there is need to explore the availability of both RDTs and ACTs as factors that have made these targets difficult to achieve.
Malaria can also be controlled through prompt and appropriate treatment. While testing and treatment of children with appropriate artemisinin-based combination therapy (ACT) has increased, this are is still problematic. In particular, while WHO recommends that all cases of fever should be tested, less than a third received a test (rapid diagnostic test – RDT or microscopy). Testing helps distinguish malaria from other fevers, and ACTs should not be given unless malaria is confirmed. We can see that more ACTs are provided than the number who were tested, so treatment based solely on signs and symptoms is still the norm. Again there is need to explore the availability of both RDTs and ACTs as factors that have made these targets difficult to achieve.
Tanzania continues to receive support from the Global Fund and the US President’s Malaria Initiative, among other partners. It is incumbent on all partners, global and national, to use these results as a wake up call to to plan for better delivery of malaria services and thus a reduction of both the economic and health burden of malaria in Tanzania.
Burden &ITNs &Morbidity Bill Brieger | 25 Jul 2014
Attaining and Sustaining – malaria targets
Recent reports on the Global Burden of Disease with a focus on Millennium Development Goal #6 has stressed the improvement in malaria morbidity and mortality indicators since the Abuja Declaration of 2000. In particular, “Global malaria incidence peaked in 2003, with 232 million new cases, subsequently falling by about 29% to 165 million new cases in 2013.”
The improvements are attributed in part to the large increase in funding. The remaining challenge derives in part from the fact that four countries, India, Nigeria, Democratic Republic of the Congo and Mozambique account for nearly two-thirds of the global case load. Global progress in reducing disease has been achieved despite the fact that in these and many other countries, achievement of 2010 targets for malaria intervention coverage (80%) have lagged. In some cases national surveys have shown some declines in coverage (e.g. Nigeria).
 Ghana provides a good example of the challenges. National surveys in 2006, 2008 and 2011 have shown mixed results in the use of insecticide treated nets by children below the age of 5 years. While the proportion rose from 20% to 39% between the first two surveys, it stayed steady in 2011. A new survey in underway, but as of 2012 there were still areas of the country that needed nets, and we know that nets wear out in between distributions and need to be replaced through routine services as seen in the photo.
Ghana provides a good example of the challenges. National surveys in 2006, 2008 and 2011 have shown mixed results in the use of insecticide treated nets by children below the age of 5 years. While the proportion rose from 20% to 39% between the first two surveys, it stayed steady in 2011. A new survey in underway, but as of 2012 there were still areas of the country that needed nets, and we know that nets wear out in between distributions and need to be replaced through routine services as seen in the photo.
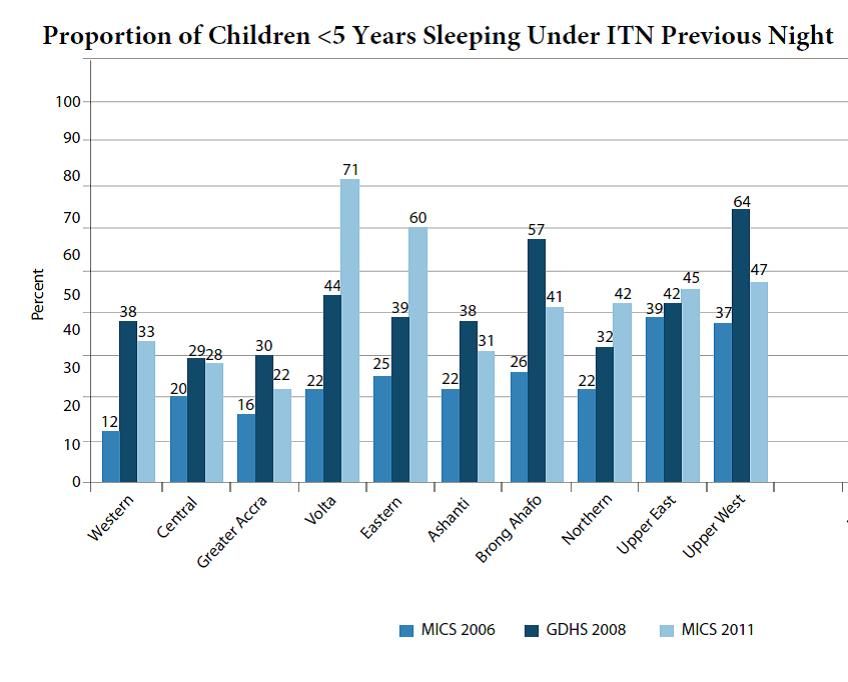 The three surveys so far in Ghana paint a mixed picture as seen in the attached graph. In six of the ten regions, net coverage for young children declined and in four it increased over the period. This on balance led to the lack of overall improvement.
The three surveys so far in Ghana paint a mixed picture as seen in the attached graph. In six of the ten regions, net coverage for young children declined and in four it increased over the period. This on balance led to the lack of overall improvement.
Thinking back to the reduced burden of disease overall, one can surmise that even some level of malaria intervention can impact on incidence of the disease, but the goal was no mortality for 2015, just one year from now. If the trend seen in Ghana (which is reflective of other countries) continues, we will pass 2015 without attaining the 2010 coverage targets and still experience an unacceptable malaria disease burden. Malaria elimination looks farther away each day.
Morbidity &Treatment Bill Brieger | 29 Jan 2014
Ronald McDonald House Charities Awards Jhpiego Grant to Reach Thousands of Children with Lifesaving Malaria Services
 FOR IMMEDIATE RELEASE
FOR IMMEDIATE RELEASE
Contact: 410.537.1829; www.jhpiego.org
Baltimore, Md. (January 28)—Jhpiego, an affiliate of Johns Hopkins University, received a $150,000 grant from Ronald McDonald House Charities (RMHC) to strengthen and expand malaria prevention and treatment services to vulnerable pregnant women and children in Chad.
 Jhpiego, a global health non-profit working in more than 50 countries, was among nine organizations selected by the global office of RMHC to improve the skills of health care workers through innovative approaches that directly benefit the health and welfare of vulnerable children around the world. The RMHC grant will build on Jhpiego’s current work in Chad to reduce deaths from malaria, the leading cause of death of children under five in the central African country.
Jhpiego, a global health non-profit working in more than 50 countries, was among nine organizations selected by the global office of RMHC to improve the skills of health care workers through innovative approaches that directly benefit the health and welfare of vulnerable children around the world. The RMHC grant will build on Jhpiego’s current work in Chad to reduce deaths from malaria, the leading cause of death of children under five in the central African country.
“Jhpiego is thrilled to begin this new relationship with RMHC to ensure that children receive quality health care services in Chad and survive,’’ said Leslie Mancuso, President and CEO of Jhpiego. “More children under five in Chad die from malaria than from any other cause. In cooperation with the government, we will build the capacity of community health volunteers to educate families on malaria prevention and promote home use of insecticide-treated nets. These volunteers who go door to door are often the first line of care in many countries, providing basic health messages and connecting families to health facilities.”
 The goal of the project funded by RMHC is to allow more children under five and pregnant women to receive much-needed services by training 10 Master Trainers, who will then educate and train 100 community health volunteers in malaria prevention activities. This approach will build a sustainable method for serving pregnant women and children in their communities. Jhpiego will target 109,571 children under five and 25,466 pregnant women who live in malaria-endemic districts in the East Logone region of Chad.
The goal of the project funded by RMHC is to allow more children under five and pregnant women to receive much-needed services by training 10 Master Trainers, who will then educate and train 100 community health volunteers in malaria prevention activities. This approach will build a sustainable method for serving pregnant women and children in their communities. Jhpiego will target 109,571 children under five and 25,466 pregnant women who live in malaria-endemic districts in the East Logone region of Chad.
Through its Global Grants and matching grants program to local U.S. RMHC Chapters, the Charity has awarded nearly $97 million in grants in the last 11 years. “Child mortality rates around the globe continue to be alarming. There is a need to invest in resources and training to create lasting change,” said David C. Herman, MD, MSMM, President and CEO, Vidant Health, and RMHC Board of Trustees member. “For 40 years, RMHC has been part of the solution in helping to eliminate some of the barriers that make it more difficult for families and children to get the health care they need.”
For more information about Jhpiego and its lifesaving mission, contact Melody McCoy, 410-537-1829 or melody.mccoy@jhpigeo.org.
About Jhpiego: Jhpiego (pronounced “ja-pie-go”) is an international, non-profit health organization affiliated with Johns Hopkins University. For 40 years, Jhpiego has empowered front-line health workers by designing and implementing effective, low-cost, hands-on solutions to strengthen the delivery of health care services for women and their families. For more information, go to http://www.jhpiego.org.
About Ronald McDonald House Charities: Ronald McDonald House Charities® (RMHC®), a non-profit, 501 (c) (3) corporation, creates, finds and supports programs that directly improve the health and well-being of children. Through its global network of local Chapters in 58 countries and regions, its three core programs, the Ronald McDonald House®, Ronald McDonald Family Room® and Ronald McDonald Care Mobile®, and millions of dollars in grants to support children’s programs worldwide, RMHC provides stability and resources to families so they can get and keep their children healthy and happy. All RMHC-operated and -supported programs provide access to quality health care and give children and families the time they need together to heal faster and cope better. For more information, visit www.rmhc.org, follow us on Twitter (@RMHC) or like us on Facebook (Facebook.com/RMHC Global).
The following trademarks used herein are owned by McDonald’s Corporation and its affiliates: Ronald McDonald House Charities, Ronald McDonald House Charities Logo, RMHC, Ronald McDonald House, Ronald McDonald Family Room and Ronald McDonald Care Mobile.
ITNs &Morbidity &Mortality Bill Brieger | 26 Aug 2012
Mosquito Nets – are we ready to restock?
The 2012 Millennium Development Goals annual report/update has been released. Progress for malaria has been noted, but below target. In summary the report notes that …
“The estimated incidence of malaria has decreased globally, by 17 per cent since 2000. Over the same period, malaria-specific mortality rates have decreased by 25 per cent. Reported malaria cases fell by more than 50 per cent between 2000 and 2010 in 43 of the 99 countries with ongoing malaria transmission.”
 While the overall tenor of the report veers toward the positive, the authors had to explain that, “Although these rates of decline were not sufficient to meet the internationally agreed targets for 2010 of a 50 per cent reduction, they nonetheless represent a major achievement.” Ironically, the map at the right, taken from the report does not even include a shading for 80% and higher – the Roll Back Malaria target for 2012. Inadequate intervention coverage and the financial and health systems weaknesses contributed to the coverage gap, in spite of calls for universal coverage in 2009.
While the overall tenor of the report veers toward the positive, the authors had to explain that, “Although these rates of decline were not sufficient to meet the internationally agreed targets for 2010 of a 50 per cent reduction, they nonetheless represent a major achievement.” Ironically, the map at the right, taken from the report does not even include a shading for 80% and higher – the Roll Back Malaria target for 2012. Inadequate intervention coverage and the financial and health systems weaknesses contributed to the coverage gap, in spite of calls for universal coverage in 2009.
The big push toward universal coverage did result in more nets, but some countries are still in the process of trying to get the first round of mass distribution finished. In light of Global Fund Round 11 cancellation and the world economic crisis, fears exist that replacement nets, likely needed by 2013, can be bought. The MDG report echos this concern: “There are worrisome signs, however, that momentum, impressive as it has been, is slowing, largely due to inadequate resources.”
Fortunately there is a bight light. Rwanda just announced that –
Over six million treated mosquito nets will be distributed to households in 2012 and 2013 and around 500,000 Long Lasting Insecticidal Nets (LLINs) will be given to pregnant women and children under five years in 2012, the National Malaria Control Program Director, Dr. Corine Karema, has said. “Currently we are in the phase of replacing the Long Lasting Insecticidal Nets (LLINs) distributed in 2010,” Dr Karema said, adding that families which didn’t receive them in 2010 will be assessed so that they can also get nets.
Not only does Rwanda’s effort represent replacement of the old nets, but also recognizes the need to provide nets in an ongoing manner during routine health services like antenatal care. Let’s hope that this sets a good example for other countries to make a commitment to find the funds – locally and/or internationally to ensure that the MDG for malaria morbidity and mortality reduction will not be sidetracked.
Elimination &Integration &Morbidity &Mortality Bill Brieger | 25 Apr 2012
Investing and Sustaining: Lessons from Rwanda on World Malaria Day
Rwanda on track to zero deaths from malaria by 2015
By Dr. Corine Karema
Today, April 25th, the world will be commemorating Malaria Day as stipulated in the Abuja Declaration of 2000. Just like the previous years, Rwanda will join the rest of the world in commemorating this day by highlighting achievements in controlling Malaria while also renewing commitment of achieving zero targets of malaria related deaths by 2015.
The theme for this year’s World Malaria Day is “Sustain Gains, Save Lives: Invest in Malaria”, a theme that is testimony to the renewed global commitment of finding lasting solutions for eliminating Malaria from our midst. For Rwanda, a country that has registered significant progress in combating Malaria, this commitment is a shared vision for which we attach greater value.
Coming up with sustainable and investment solutions for Malaria control is a new discourse which underlines the importance of continued investment in combating this disease with the view of propelling malaria-endemic countries along the path of achieving the health and poverty related Millennium Development Goals by 2015. Here in Rwanda, the battle against Malaria has not been an easy one. It has called for strategic interventions, committed leadership of our government and support from development partners to register progress that we see today across the country.
I will share with you some of the outstanding achievements we have registered over the past years, many of which are captured in the recently released 2010 Demographic Health Survey (DHS). The recent scaling up of interventions has made significant progress:
- reductions in morbidity by 87% from 1,669,614 malaria cases in 2005 to 212,200 cases in 2011 and
- reduced mortality by 76% from 1,582 deaths in 2005 to 380 deaths in 2011.
 This reduction is as a result of scaling up of preventive measures especially coverage and use of long lasting insecticidal nets (LLINs) which according to the 2010 DHS results…
This reduction is as a result of scaling up of preventive measures especially coverage and use of long lasting insecticidal nets (LLINs) which according to the 2010 DHS results…
- 82% of households have at least one LLIN
- 72% of pregnant women slept under their nets and
- 70% of children under-five years were using bed nets
Previously and as the case is in most developing countries, Malaria is treated based on signs and symptoms. However, Rwanda is one of the few countries in the world today where up to 94 percent of Malaria cases are laboratory through microscopy or rapid diagnostic tests at all levels of health care structure including the community level.
The involvement of Community Health Workers (CHWs) in early diagnosis and treatment of children Under-five years has also had an impact on malaria incidence throughout the country as currently 95% of children are tested and treated for malaria within 24 hours of symptoms onset.
In addition, Malaria control activities have been integrated and decentralized at all levels including –
- a strong CHWs network which facilitates community involvement and participation,
- the community health insurance scheme also known as Mutuelles de Sante and
- a strong Health Management Information Systems (HMIS) including the web based community health information system (SIS.com)
The above interventions are strengthened by use of mobilisation and sensitisation campaigns using different channels of communication. The advocacy and social mobilisation is oriented towards intensifying different efforts to sustain the gains made as the country moves towards pre-elimination phase of malaria as outlined in the new Malaria Strategic Plan (2012-2017).
To emphasize on the importance of the World Malaria Day, this year’s event will be held during the scheduled Rwanda Malaria Forum that will be held in Kigali in mid June 2012. The Forum will bring together malaria experts from international community who will deliberate on the challenges African countries and in particular, Rwanda, face in malaria control and how to overcome them.
The recommendations of the forum will guide our sector in finalizing the new Malaria Strategic Plan that outlines Rwanda’s strategies from malaria control to pre-elimination phase by 2017. A series of activities to run for a week have also been planned to reach community levels where different interventions of promoting awareness on preventive measures will be discussed with input from community leaders.
Therefore, as we mark this day in Rwanda, we take pride of our achievements but also remain mindful and conscious of the challenges ahead a in realising the ambitious target of having a Rwanda that is free from Malaria.
The Author is Head of Malaria and Other Parasitic Diseases Division Rwanda Biomedical Center/IHPDPC, Follow: Twitter @ckarema
Advocacy &Morbidity Bill Brieger | 25 Jan 2010
When the media goes home
The malaria threat to Haiti may not be as immediate as the terrible injuries and potential infections from inadequate water and waste disposal. Malaria will be lurking – but will anyone be paying attention when it arises?
Anderson Cooper of CNN was quoted in the New York Times as saying “We all know what’s going to happen. People are just going to lose interest in this as a story. They’re going to stop watching.†Already today the BBC has only one small headline on its world news homepage referring to Haiti and one feature piece far at the bottom of the page.
 More importantly, according to the Times, the major news organizations also have ‘money worries’ about the extensive coverage. The costs of coverage, and the boost it gives to donor organization efforts to raise funds, were outlined by the Times as follows: “News outlets rushed to charter airplanes and snap up extra seats on aid flights, but that was the easy part. Upon arrival, they had to establish supply lines, mostly through the neighboring Dominican Republic.”
More importantly, according to the Times, the major news organizations also have ‘money worries’ about the extensive coverage. The costs of coverage, and the boost it gives to donor organization efforts to raise funds, were outlined by the Times as follows: “News outlets rushed to charter airplanes and snap up extra seats on aid flights, but that was the easy part. Upon arrival, they had to establish supply lines, mostly through the neighboring Dominican Republic.”
News executives acknowledge that the media can move in and out of Haiti quickly, but efforts to scale back are already in evidence. One network reported on running out of water for its staff twice. Overall it was estimated that each news organization would be spending $US 1.5 million on its Haiti coverage.
Well recognized media figures like Dr. Sanjay Gupta have been serving an advocacy role encouraging potential partners to reach difficult areas and provide better quality services. The Times recognizes the importance of the visual element in this advocacy process. Will scaled back coverage reduce this advocacy avenue?
Over 150,000 people have been confirmed dead so far in Haiti, and final estimates reach as high as 200,000. The World Malaria Report still estimates over 800,000 malaria deaths world wide annually. These deaths may not occur in as dramatic a fashion as a natural disaster, but they add up and are still disastrous to families and nations.
The media has been an essential partner in highlighting malaria interventions and progress at all levels, especially as we count down to universal coverage. We need all partners to ensure that the media spotlight remains on malaria, and especially right now on malaria in Haiti.
As morbidity reduces and we get closer to malaria elimination, this task may become harder – but media advocacy will be needed up to the very end to ensure adequate funding to maintain surveillance and certify elimination even when malaria seems less pressing.
Monitoring &Morbidity Bill Brieger | 02 Nov 2008
The Gambia joins small club of reduced incidence countries
“Incidence of malaria in Gambia has plunged thanks to an array of low-cost strategies, offering the tempting vision of eliminating this disease in parts of Africa, a study published Friday by The Lancet said,” according to AFP. The Gambia now joins four countries featured in the World Malaria Report that “reduced the malaria burden by 50% or more between 2000 and 2006–2007.” The four, Eritrea, Rwanda, Sao Tome and Principe, and Zanzibar (in the United Republic of Tanzania), are distinguished by “relatively small populations, good surveillance, and high intervention coverage.”
Reuters explained that, “Providing pregnant women and children with insecticide-treated bed nets has sharply cut malaria deaths.” The findings raise hopes that, “Other parts of Africa could eliminate the disease as a public health problem in a region where malaria kills a child every 30 seconds.”
Gambia News carried a caution in comments by David Conway, one of the authors of the Lancet article who said, “We have seen that it has gone down and stayed down. There is no evidence of an upsurge but we are aware that with an infectious disease you can never know for sure.” This caution is relevant bearing in mind this year’s World Malaria Day theme – a disease without borders.
Achievements in the Gambia have been facilitated by grants in Rounds 3 and 5 from the Global Fund in which its performance has been ‘A’ and ‘B1’ respectively. Neighboring Senegal also had Global Fund malaria grants, but it experienced serious grant performance problems not long ago, reinforcing the caution that malaria is waiting at the Gambia’s borders.
While the Gambia may not be able to eradicate malaria all by itself, as implied in a February 2008 article in The Observer, it is certainly on track for elimination using available control technologies. Even though eradication is not on the immediate horizon, the government official quoted in The Observer was on target when she said, “My government has therefore not relented in waging a continuous war against the disease. We have also embraced all policies and implemented all programmes formulated by the WHO and its sister UN agencies on malaria prevention and control.†Other nations with larger malaria burdens need to be as vigilant as The Gambia.
Morbidity &Mortality Bill Brieger | 19 Sep 2008
Malaria cases reduced … through better statistics
For years the standard figure of malaria morbidity has been half a billion cases a year. Now, “The World Health Organization halved its estimate of the number of people who get malaria each year, saying Thursday that better measurement techniques had cut the number from 500 million people to 247 million.”
 Previous figures apparently were based on estimates that mapped where people were likely to be exposed to malaria, but data collection is deemed to be more accurate in 2006, the most recent information as presented in the new World Malaria Report 2008. Even with reduced morbidity, “WHO left unchanged the figure of malaria deaths. An estimated 881,000 people were killed by malaria in 2006 — most of them were children under 5.” But even with better data, “Less than one-third of the agency’s 192 member countries have acceptable registration of malaria cases and deaths.”
Previous figures apparently were based on estimates that mapped where people were likely to be exposed to malaria, but data collection is deemed to be more accurate in 2006, the most recent information as presented in the new World Malaria Report 2008. Even with reduced morbidity, “WHO left unchanged the figure of malaria deaths. An estimated 881,000 people were killed by malaria in 2006 — most of them were children under 5.” But even with better data, “Less than one-third of the agency’s 192 member countries have acceptable registration of malaria cases and deaths.”
Science Magazine cautioned that, “the report’s authors say that the drop isn’t a sign we’re winning the battle, just that the methodology of gathering data is better.” Health statistics are challenging. Science also noted that, “Determining the burden of malaria is notoriously hard because many patients don’t seek or receive medical attention, and even if they do their case may not be lab-confirmed or entered into government statistics. One result is that WHO’s numbers have huge error bars: For instance, the estimate for Kenya ranges from 5 million to 19 million cases.”
Robert Snow of the University of Oxford, U.K. and the Kenya Medical Research Institute in Nairobi was quoted by Science as sayingthat “WHO still relies too heavily on weak government data, resulting in too rosy a picture.” Fortunately donors are recognizing more and more the importance of strengthening malaria data and monitoring and evaluation (M&E) capacity in endemic countries.
The Global Fund offers M&E guidance and encourages countries to write into their proposals means for strengthening their health information systems. Countries do not always take full advantage of these health system strengthening components. Partners should therefore, continue to provide guidance and encouragement to countries to improve their M&S and health statistics so that the next World Malaria Report will truly reflect both reality and hopefully progress.