IPTp &Malaria in Pregnancy Bill Brieger | 09 Nov 2013
Ghana: Progress on IPTp, but not yet sustained high coverage
The 2011 Multiple Indicator Cluster Survey (MICS) from Ghana demonstrates the challenges we have in moving along the pathway toward malaria elimination. People will recall that the Roll Back Malaria indicators were for endemic countries achieve 80% coverage on basic malaria interventions by 2010 and sustain these to achieve Millennium Development goals by 2015 and then move on to pre-elimination of the disease where less than 1/1000 people at risk in a country actually experienced malaria. Now of course, everyone is talking about universal coverage of basic services, not just 80%.
The 2011 Ghana MICS reports on the standard RBM indicator of two doses of intermittent preventive treatment (IPTp) with sulphadoxine-pyrimethamine (SP) during antenatal care (ANC), although Ghana has for some time aimed at three doses. Also current WHO guidance for IPTp recommends IPTp in stable endemic countries at one dose for every antenatal care visit after quickening, which could mean three or four times. So the 2011 MICS shows 83% of recently pregnant women surveyed got one dose of IPTp during ANC while only 65% received two.
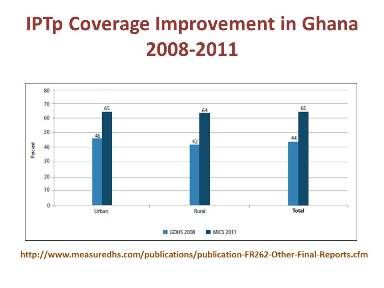 The chart to the right does show progress in IPTp coverage between the 2008 Demographic and Health Survey and the 2011 MICS. a jump from 44% to 65% for the two doses, and progress should be acknowledged, but as pointed out at the recent Pan Africa Malaria Conference in Durban, we must not work around the edges to eliminate malaria, but tackle the higher prevalence countries and areas directly and ensure that malaria is truly eliminated.
The chart to the right does show progress in IPTp coverage between the 2008 Demographic and Health Survey and the 2011 MICS. a jump from 44% to 65% for the two doses, and progress should be acknowledged, but as pointed out at the recent Pan Africa Malaria Conference in Durban, we must not work around the edges to eliminate malaria, but tackle the higher prevalence countries and areas directly and ensure that malaria is truly eliminated.
Why are coverage figures low – and this is not just a problem in Ghana? At least 96% of pregnant wom en in Ghana attend ANC with a skilled provider: 95% make two ANC visits, 89% make three and 86% are reported to make four. What we may be seeing are missed opportunities.
en in Ghana attend ANC with a skilled provider: 95% make two ANC visits, 89% make three and 86% are reported to make four. What we may be seeing are missed opportunities.
Are gaps due to health worker errors, SP stock-outs or client refusals? This needs to be investigated and rectified.
Ideally pregnant women should also get an insecticide treated net on their first ANC visit regardless of distribution through mass campaigns. Unfortunately the MICS 2011 shows that only 32% of pregnant women overall had slept under a treated net the previous night, and even in households with nets, only 58% had slept under them. Clearly malaria in pregnancy control and scale-up needs higher priority in Ghana as well as the rest of Africa.
Malaria in Pregnancy &Treatment Bill Brieger | 04 Nov 2013
Improving case management of malaria during pregnancy by antenatal care providers in Akwa Ibom State, Nigeria
Bright Orji, William Brieger, Emmanuel Otolorin and John Orok presented today at the 141st APHA Annual Meeting in Boston of Jhpiego’s  experiences with malaria in pregnancy in Akwa Ibom State Nigeria. A summary appears below.
experiences with malaria in pregnancy in Akwa Ibom State Nigeria. A summary appears below.
In Nigeria malaria causes approximately 11% of maternal deaths. Malaria is responsible for 63% of hospit al admissions and 70% of illness among pregnant women. While intermittent preventive treatment (IPTp) and Long Lasting Insect icide-treated Nets (LUNs) are supposed to be given to pregnant women to prevent the dis·ease, coverage is poor.
Unfortunately since malaria is often being treated presumptively, pregnant women st ill die from other fever-related illnesses. Use of rapid diagnostic test (RDTs) to confirm malaria before treatment provides an opportunity for earlier recognition of febrile illnesses not due to malaria.
This study assessed the pattern of malaria diagnosis and treatment in pregnant women attending Antenatal care (ANC) in Akwa Iborn State, Nigeria. Record cards of pregnant women attending six government owned ANC before and after staff training on malaria diagnosis using RDTs.
The patients’ cards were drawn from ANC clinics with first non- follow-up visit of the year before training (February 20 10) and after (March 20 11) by three nurses/midwives.
Health care providers fever gave 85% of 3 13 women attending ANC antimalarial drugs before the introduction of RDTs training. Afterwards 82% of 179 febrile women were tested with RDTs. All 29 with positive RDT received artemisinin-based combination therapy, 6 RDT-negative women got ACTs, and no women who were not tested were treated for malaria.
Training encouraged health workers to adherence rational prescribing of antimalarials and made it possible t o offer better management of other fever-related illnesses during pregnancy. Support is now needed to scale-up RDTs use in ANC clinics in Nigeria.
Community &IPTp &Malaria in Pregnancy Bill Brieger | 09 Oct 2013
Jhpiego at MIM2013 – Use of Community Health Workers to Improve Pregnancy Outcomes in Kenya
Augustine Ngindu, Sanyu Kigondu, Rose Mulindi, Christine Ayuyo, Muthoni Magu-Kariuki, Isaac Malonza, Julius Kimiteiand Elizabeth Washikaof Jhpiejo, the Ministry of Health (Kenya) and the Maisha/USAID Project reported on using Community Health Workers to identify and refer pregnant women to access intermittent preventive treatment (IPTp) in Kenya

Community Health Worker Training
Malaria in pregnancy is associated with anemia, low birth weight, miscarriages and death. Despite availability of effective MIP interventions intermittent preventive treatment using Sulfadoxine Pyrimethamine (IPTp-SP) and insecticide treated nets (ITNs), coverage rates in Kenya have remained low; IPTp2 uptake- 25% and ITN coverage- 41%.
To increase coverage rates Kenya has adapted a community strategy approach sensitizing pregnant women to start antenatal care (ANC) early to receive comprehensive care throughout pregnancy. This includes access to an ITN at first ANC visit and IPTp uptake beginning in the second trimester to increase coverage rates.
Trained community health workers (CHWs) registered pregnant women in their Community units for follow up monthly. CHWs conducted monthly follow up of all registered pregnant women to identify those not attending ANC and referred them for ANC services as well as counseled those not using ITNs.
CHWs received supportive supervision from district managers and MCHIP staff to assess performance skills on quality of data and mentorship on MIP interventions. Data collected was analyzed for pregnant women registered, accessing IPTp and referred for ANC services.
3,212 pregnant women were registered and 1,541 (48%) of the registered pregnant women were referred for ANC services because they were either late in starting ANC attendance or IPTp after 1st trimester or defaulters of scheduled visits. Among the registered pregnant women 81% had taken one or more IPTp doses.
Use of CHWs in identification of pregnant women not accessing IPTp and referral of 48% of them has shown an effective methodology of identifying defaulters in IPTp uptake among pregnant women. Scaling up of this community-based approach would ensure early ANC attendance and access to the available effective MIP interventions including IPTp.
Malaria in Pregnancy Bill Brieger | 08 Oct 2013
MIM2013: IPTp policy in Zanzibar towards pre-elimination of malaria: results from a study of placental parasitemia
 Mwinyi Issa Ramadhan Khamis, Elaine Roman, Raz Stevenson, Chonge Kitojo, Julie Msellem, Marya Plotkin, Khadija Said; Natalie Hendler; Asma Gutman, and Peter McElroy developed this presentation for the MIM2013 6th Pan-African Conference on Malaria in Durban. They represent the Zanzibar National Malaria Control Programme, Zanzibar Ministry of Health, Jhpiego Tanzania, Jhpiego Baltimore, United States Agency for International Development, US Centers for Disease Control and Prevention and the US President’s Malaria Initiative and were involved in the bilateral Maisha Project.
Mwinyi Issa Ramadhan Khamis, Elaine Roman, Raz Stevenson, Chonge Kitojo, Julie Msellem, Marya Plotkin, Khadija Said; Natalie Hendler; Asma Gutman, and Peter McElroy developed this presentation for the MIM2013 6th Pan-African Conference on Malaria in Durban. They represent the Zanzibar National Malaria Control Programme, Zanzibar Ministry of Health, Jhpiego Tanzania, Jhpiego Baltimore, United States Agency for International Development, US Centers for Disease Control and Prevention and the US President’s Malaria Initiative and were involved in the bilateral Maisha Project.
Due to scale up of malaria prevention and treatment by the Zanzibar Malaria Control Programme (ZMCP) of the Ministry of Health (MOH), Zanzibar is in the pre-elimination phase of malaria control P. falciparum prevalence in the general population is currently less than 0.5% [1], and the diagnostic positivity rate among febrile patients was 1.2% in 2011 [2]
Control of Malaria in Pregnancy (MIP) follows the 3 pronged approach recommended by WHO:
- Intermittent preventive treatment for pregnant women (IPTp) with sulfadoxine-pyrimethamine (SP) distributed through antenatal care (ANC) services
- Long lasting insecticide treated nets
- Case management of malaria in pregnancy
IPTp-SP was implemented in 2004 when malaria prevalence exceeded 20%. Coverage among pregnant women remains low. In their last pregnancy:
- 69% women reported taking any SP
- 43% women reported taking 2+ doses of SP [3]
The MOH of Zanzibar is reconsidering provision of IPTp through ANC services in light of very low malaria prevalence. ZMCP has introduced screening for malaria in ANC services. In 2011 and 2012, 0.2% of ANC clients tested positive for malaria using mRDT (19,724 malaria tests were performed in 2011 and in 27,186 performed in 2012) [4]
 The Placental Parasitemia Study was a prospective observational study was conducted in selected health facilities in Zanzibar with the objective of measuring placental parasitemia rates among pregnant women who did not receive IPTp. The study addressed the Policy question: Is IPTp useful at current level of transmission in preventing maternal and neonatal morbidity?
The Placental Parasitemia Study was a prospective observational study was conducted in selected health facilities in Zanzibar with the objective of measuring placental parasitemia rates among pregnant women who did not receive IPTp. The study addressed the Policy question: Is IPTp useful at current level of transmission in preventing maternal and neonatal morbidity?
A Convenience sample of pregnant women enrolled at six hospitals in Zanzibar on day of delivery was recruited from September 2011 – April 2012. Client card checked for documentation of provision of IPTp (eligible= no doses of SP, resident of Zanzibar). Informed consent obtained from eligible clients.
Samples were taken from maternal side of placenta by labor ward midwives. Dried blood spots (DBS) on filter paper were prepared from placental blood specimens DBS were analyzed via polymerase chain reaction indicating active Plasmodium infection (all species).
1,423 deliveries were enrolled from Pemba (52%) and Unguja (48%), representing 6% of the total deliveries at the six facilities. The Average age of women was 26.9 years and 376 (32%) were primigravidae.
In 9 of 1,349 (0.8%, 95% confidence interval 0.2–3.3%) placental specimens were PCR positive. Only P. falciparum detected. Six (66%) of the nine placental infections were from Unguja deliveries. Eight placental infections were accompanied by a normal birth weight delivery (? 2500 g). Placental infections were not more common during the seasonal transmission increases of 2011-12.
In Conclusion, Malaria infection among pregnant women who have not had IPTp is extraordinarily low (0.8%). Given the low prevalence of placental malaria infection among women who had not had IPTp, in combination with the overall low prevalence of malaria on the islands, a policy shift away from IPTp is not an unreasonable option, if this is done with expanded surveillance of MIP and strengthening of detection and case management of women with MIP.
We Recommend Enhanced surveillance of MIP through expansion of the existing surveillance system, MEEDS, to capture symptomatic pregnant women diagnosed at ANC and ensure that pregnancy status is recorded for women diagnosed at the outpatient department. Case management of MIP should be strengthened and continued high ownership and use of ITNs should be ensured, particularly among women of reproductive age.
A internal review of costs and findings from surveillance to inform on whether the cost of screening every pregnant woman in antenatal care is justified
References
- Bhattarai A, Ali AS, Kachur SP. Impact of artemisinin-based combination therapy and insecticide-treated nets on malaria burden in Zanzibar. PloS Med 4(11): e309.
- Zanzibar Malaria Control Programme. Zanzibar Malaria Epidemic Early Detection System Biannual Report, Mid-Year 2011; Vol. 3, (No.1); 2011.
- Tanzania HIV/AIDS and Malaria Indicator Survey (THMIS) 2011-12.
- Zanzibar Malaria Control Programme. Unpublished 2012 National surveillance data.
Malaria in Pregnancy &Treatment Bill Brieger | 08 Oct 2013
Jhpiego at MIM2013 – Improving malaria case management by health care providers in antenatal clinics in Akwa Ibom State of Nigeria
William R Brieger, Bright C Orji, and Emmanuel Otolorin, of Jhpiego shared Jhpiego’s work on improving the health of pregnant women in southeastern Nigeria at the MIM2013 6th Pan-African Malaria Conference in Durban.
 In Nigeria approximately 11% of maternal deaths are caused by malarial in pregnancy (MIP). Use of Long Lasting Insecticide-treated Nets (LLINs), intermittent preventive treatment (IPTp) and prompt and effective case management have been recognized as key interventions to control MIP. Of these three MIP interventions, case management is the less well developed with fever in pregnancy often being treated presumptively as malaria, possibly leaving pregnant women to die from other illnesses.
In Nigeria approximately 11% of maternal deaths are caused by malarial in pregnancy (MIP). Use of Long Lasting Insecticide-treated Nets (LLINs), intermittent preventive treatment (IPTp) and prompt and effective case management have been recognized as key interventions to control MIP. Of these three MIP interventions, case management is the less well developed with fever in pregnancy often being treated presumptively as malaria, possibly leaving pregnant women to die from other illnesses.
The use of rapid diagnostic tests (RDTs) to confirm malaria before treatment provides an opportunity for earlier recognition of febrile illnesses not due to malaria and appropriate treatment for those that are due to malaria. This study sought to learn whether the introduction of RDTs into antenatal care (ANC) would influence the pattern of malaria fever and malarial case management in Akwa Ibom State, Nigeria.
The study reviewed record cards of pregnant women attending government owned ANC clinics before and after introducing and training health staff on parasitological diagnosis of malaria using RDTs. The ANC client cards were drawn from first non-follow-up visits where a complaint of ‘fever’ was recorded. Data extraction was conducted between February 2010 and March 2011 by trained nurses/midwives across six primary health care centers in two Local Government Areas of the state.
At baseline 597 cards were reviewed, and 472 at endline. At baseline presumptive malaria treatment took place among 506 (84.8%) of the febrile women using ACT (23%), Quinine (32%) and other antimalarials (30%). At endline 361 (76%) of febrile women were tested with RDTs, with 71 (20%) of tests being positive.
All RDT+ women received an antimalarial, with 76% getting either ACT or quinine as recommended. Among the 290 RDT- women, 28% were given an antimalarial drug. In contrast 60% of RDT- women received an antibiotic, although most of them had complained of a respiratory illness.
The review of records did show that nursing and midwifery staff at government clinics could in a relatively short time period adopt the use of RDTs. They did improve their prescribing of appropriate antimalarials, but still were using some inappropriate ones and did treat a small proportion of RDT- women for malaria. Continued follow-up and supervision will be needed to ensure that correct malaria diagnostic and treatment guidelines are fully practiced.
Malaria in Pregnancy Bill Brieger | 08 Oct 2013
Jhpiego at MIM2013 – Persistence of Malaria in Pregnancy as Rwanda Targets Pre-Elimination
 William Brieger, Corine Karema and Beata Mukarugwiro from Jhpiego/MCHIP and the Malaria and Other Parasitic Diseases Program of the Rwanda Ministry of Health reported on the prevalence of malaria in pregnancy in Rwanda as the country moves toward elimination at the MIM2013 6th Pan-African Malaria Conference in Durban.
William Brieger, Corine Karema and Beata Mukarugwiro from Jhpiego/MCHIP and the Malaria and Other Parasitic Diseases Program of the Rwanda Ministry of Health reported on the prevalence of malaria in pregnancy in Rwanda as the country moves toward elimination at the MIM2013 6th Pan-African Malaria Conference in Durban.
Through universal coverage of long-lasting insecticide treated nets and access to artemisinin based combination treatment Rwanda has achieved a national malaria prevalence estimated at 1.4% among children aged 6-59 months and 0.7% among women aged 15-49 years (2010 DHS). Slide positivity rates at health centers have dropped over 85% since 2005, and yet malaria persists.
Pregnant women remain vulnerable. While Rwanda no longer practices IPTp, it is interested in offering the best malaria protection to pregnant women. In order to plan appropriately, there was need for a malaria in pregnancy prevalence study.
Pregnant women were studied at first ANC registration in 38 health centers in two districts each of low, moderate and relatively higher malaria transmission areas (as determined by health information system laboratory reports) using microscopy, rapid diagnostic test (RDT) and polymerase chain reaction (PCR). Ethical clearance was provided by the ethical review board within the Ministry of Health.
ANC staff were trained to obtain data during normal client visits. RDTs were performed by the ANC staff. They also prepared blood slides to be analyzed in health center laboratories and PCR papers that were analyzed at the Johns Hopkins Bloomberg School of Public Health. Information on parity, age, bednet use, anemia, HIV status and fever were normally collected for ANC records and also recorded on project data forms.
Among 3,781 women studied, malaria prevalence with microscopy was 1.6%, RDT was 2.4%, and PCR was 5.6%. Negative tests were associated with LLIN use the night before. Positive tests were associated with anemia, but none of the other variables. The highest positivity for all three tests (4.5%, 6.9% and 12.5% respectively) was in the designated high prevalence districts on the eastern border of the country.
Results show that even with low apparent levels of malaria, health services need to continue to protect pregnant women and their unborn children in Rwanda through consistent use of LLINs and identification and tracking women with anemia. Cross-border collaboration will also be needed to prevent reintroduction of the disease as the country moves towards elimination.
Malaria in Pregnancy &Uncategorized Bill Brieger | 07 Oct 2013
Jhpiego at MIM2013 – Harmonizing Malaria in Pregnancy Guidance: A Review from 5 African Countries
Elaine Roman, Patricia Gomez, Aimee Dickerson from Jhpiego (An Affiliate of Johns Hopkins University) and MCHIP developed the following abstract for a poster presentation at MIM2013 in collaboration with the US President’s Malaria Initiative. A copy of the full report is available at MCHIP.
 Thirty-nine countries in sub-Saharan Africa have malaria in pregnancy (MIP) policies in place, including intermittent preventive treatment (IPTp), insecticide treated bed-nets (ITNs) and effective case management. Nonetheless, IPTp and ITN coverage among pregnant women remains well below international goals. MIP policies are typically produced by National Malaria Control Programs (NMCP), but are implemented by National Reproductive Health Programs (RHP).
Thirty-nine countries in sub-Saharan Africa have malaria in pregnancy (MIP) policies in place, including intermittent preventive treatment (IPTp), insecticide treated bed-nets (ITNs) and effective case management. Nonetheless, IPTp and ITN coverage among pregnant women remains well below international goals. MIP policies are typically produced by National Malaria Control Programs (NMCP), but are implemented by National Reproductive Health Programs (RHP).
We reviewed MIP policy documents from the NMCP and RHP in Kenya, Mali, Mozambique, Tanzania and Uganda to understand 1) how closely national MIP documents reflect WHO MIP guidance and 2) how consistent documents produced by the NMCP and RHP are with each other. We developed a framework to compare MIP documents from RHP and NMCP according to WHO guidance for MIP, including IPTp timing and dosing, directly observed therapy, linkages to HIV prevention programs, promotion and distribution of ITNs, and diagnosis and treatment.
All countries have national documents promoting IPTp, ITN use, and case management of MIP. WHO guidance was not always reflected in these documents: four countries restrict dosing of the first and second IPTp doses to specific gestational weeks, provide inconsistent guidance on MIP prevention in HIV+ women, and fail to provide clear guidance on the different antimalarial treatment that should be administered in the first vs. later pregnancy trimesters. . All countries had discordant guidance between RH and NMCP in at least one official MIP guidance document. For example, all countries had conflicting guidance on the timing or dosing of SP and the mechanism pregnant women should use to obtain ITNs. Considerable discrepancies exist between MIP guidance documents from NMCP and RHP.
These discrepancies contribute to confusion by health workers implementing MIP programs, contributing to the low coverage of IPTp and ITNs. Harmonization of national MIP documents is urgently needed, with effective re-orientation and supervision of health workers to updated materials to help accelerate implementation. While this review is targeted primarily at country level stakeholders, the information is important for regional and global level stakeholders as well. This exercise is being repeated in other President’s Malaria Initiative countries.
Drug Quality &IPTp &Malaria in Pregnancy Bill Brieger | 26 Aug 2013
Time to Stop Selling SP in Pharmacy and Medicine Shops
The use of sulphadoxine-pyrimethamine (SP) intermittent preventive treatment of malaria in pregnancy (IPTp) has been offered in stable malaria transmission countries for over a decade. As observations continued that SP resistance was growing in children treated for malaria, SP was dropped as a recommended treatment drug in all malaria-endemic countries in Africa. Ironically SP is still commonly found in pharmacy and medicine shops in many countries.
While SP resistance in child treatment has been documented, studies directly testing this in pregnant women have not been designed due to the usual concerns about the effect of medicines in pregnancy. Already the recommendation for IPTp excluded its use in the first trimester. What has been observed though not that SP does not work, but that its half-life or period of effectiveness has been reduced. Therefore WHO still recommends SP for IPTp, but more frequently.
The new guidelines call for SP as IPTp to be given at every focused antenatal care (FANC) visit after quickening. There are four FANC visits recommended and depending when a woman comes for her first FANC visit, she may be eligible for 3 or 4 monthly IPTp doses.
In order to prevent SP efficacy as used in IPTp from eroding further, there have been strong calls for stopping its use for treatment. This has proved challenging since SP may cost less that one US dollar per dose, while ACTs, if not available free in government clinics (if no stock-outs), cost up to $6-$8 for adult doses. No wonder there is an economic appear to continue to stock SP in private shops for sale as an antimalarial. Even in public clinics SP meant for IPTp may be used by staff when there are ACT stock-outs.
 It would seem that most of our national health authorities believe more in the economic laws of supply and demand than in the technical guidelines of WHO. Otherwise SP would not be so widely available in shops. Whether private sector sales of SP are ignored by health authorities or actually tolerated by them, the result is still a threat to mothers and unborn children whose lives can be saved by maintaining the efficacy of SP and banning sales and inappropriate use of SP. Courage to stand up to private sales is needed.
It would seem that most of our national health authorities believe more in the economic laws of supply and demand than in the technical guidelines of WHO. Otherwise SP would not be so widely available in shops. Whether private sector sales of SP are ignored by health authorities or actually tolerated by them, the result is still a threat to mothers and unborn children whose lives can be saved by maintaining the efficacy of SP and banning sales and inappropriate use of SP. Courage to stand up to private sales is needed.
On a closing note, you will have noticed the picture of the SP packet attached here. It is produced by a Kenyan company and was found in a pharmacy in Malawi. The manufacturer is clearly hoping to rebrand its product. The pharmacist admitted though that few have been sold since pregnant women get SP free at ANC.
Fortunately the shop is not promoting this SP for treatment but instead sells a brand of artemether-lumefantrine. Even this newly repackaged SP product for home use is inappropriate as IPTp should be given as directly observed treatment by a health worker. We should not let such inappropriate use of SP be hidden behind clever packaging. National Malaria Programs and Drug Authorities must join hands to restrict SP use for IPTp.
IPTp &Malaria in Pregnancy Bill Brieger | 20 Aug 2013
Burundi- Reduce Neonatal-Mortality by Preventing Maternal Malaria
This guest blog has been re-posted from The blog by Chioma Anigbogu who is in our course, Social and Behavioral Foundations of Primary Health Care.
Malaria continues to severely burden many Sub-Saharan countries, including the nation of Burundi. In Burundi, 78% of the country lives in high or low transmission areas. Â In this population, pregnant women are at greater risk of experiencing spontaneous abortions, low birth weight, neonatal deaths and even anemia due to malaria. Â However, researchers have found that prevention treatment (Intermittent prevention therapy or IPT) during pregnancy can significantly reduce neonatal mortality and morbidity.

The WHO has a three-pronged recommendation for the prevention of malaria, including IPT, distribution of insecticide treated nets (ITNs) and proper management of disease. Burundi adopted an ITN policy in 2004 and has many in-country and international programs that distribute ITNs. Burundi even reports 100% treatment coverage for tested malaria cases. However, unlike some other African countries, Burundi has not adopted an IPT policy for malaria, leaving pregnant women and children extremely vulnerable.
")
In 2011, the government of Burundi (GOB) developed the Global Health Initiative, in partnership with international organizations, that is aimed at reducing maternal, neonatal and child health disease. The GHI holds a specific tenet regarding the “prevention and treatment of malariaâ€. In 2009 Burundi also received funds from the US- Agency for International Development (USAID) to complement already existing malaria activities. These activities sometimes include IPT but there is no formal requirement or enforcement of the treatment. WHO suggests that confusion amongst health workers may contribute to the lack of recommendation for this preventative treatment. A national policy that is developed and properly implemented would train health officials and workers in assuring that this treatment is integrated to the provision of services for women.
It would increase the overall health of the country and further bolster the work of other organizations such as Doctors without Borders and the Canadian Red Cross who are invested in Burundi’s malaria management. Adoption of this policy in Burundi will also reduce the negative impact of malaria, and may even reduce overall health spending by helping to maintaining better health for mothers and neonates.
In order to contribute your voice, leave a comment for the USAID (who works directly with Burundi), encouraging them to work with the Burundi government to adopt an IPT policy.
Photo Credit: Médecins Sans Frontières (Doctors without Borders)
IPT Table:Â http://www.plosone.org/article/info:doi/10.1371/journal.pone.0009438
Elimination &Epidemiology &Malaria in Pregnancy Bill Brieger | 25 Jun 2013
Low levels of placental parasitemia among women delivering in health facilities in Zanzibar: policy implications for IPTp

Presented at Jhpiego’s Mini-University on 24 June 2013 in Baltimore by Marya Plotkin, Elaine Roman, and Maryjane Lacoste
Malaria in pregnancy (MIP) is a threat to the pregnant women, the unborn child and the newborn and infant. Intermittent Preventive Treatment during pregnancy (IPTp) is one of the few interventions available that specifically targets and protects pregnant women. As malaria prevalence drops when countries aim at malaria elimination, we need to examine the continued role of IPTp and search for alternatives.
 From August 2011 to September 2012, Jhpiego partnered with the Zanzibar Ministry of Health to conduct a study looking at the prevalence of placental malaria infection among women delivering in selected health facilities in Zanzibar who had not had IPTp during the course of their pregnancy. The community-level malaria positivity rate in Zanzibar declined from as high as 20% in 2005 to 1.6% in 2011. In Zanzibar as in the rest of Tanzania, IPTp coverage has been quite low, but pregnant women have access to long-lasting insecticide-treated nets (LLINs) and indoor residual spraying (IRS) is practised in the islands.
From August 2011 to September 2012, Jhpiego partnered with the Zanzibar Ministry of Health to conduct a study looking at the prevalence of placental malaria infection among women delivering in selected health facilities in Zanzibar who had not had IPTp during the course of their pregnancy. The community-level malaria positivity rate in Zanzibar declined from as high as 20% in 2005 to 1.6% in 2011. In Zanzibar as in the rest of Tanzania, IPTp coverage has been quite low, but pregnant women have access to long-lasting insecticide-treated nets (LLINs) and indoor residual spraying (IRS) is practised in the islands.
Midwives in six clinics in in Unguja and Pemba tested the women using PCR at delivery. Of the 1,356 women with no IPTp exposure enrolled in the study, only nine (0.6%) were found to have placental malaria (95% CI 0.2–1%). Thus, even without benefit of IPTp, other interventions appear to be protecting pregnant women to some degree.
 Estimations of the costs of IPTp program put the annual expenditure at $114,678, while the annual cost of intermittent screening and treatment with RDTs (ISTp) would be $155,294. Given the extraordinarily low prevalence of malaria in pregnancy, as well as pilot experience of testing in the ANC setting, there is a strong argument for adopting ISTp and dropping IPTp in Zanzibar.
Estimations of the costs of IPTp program put the annual expenditure at $114,678, while the annual cost of intermittent screening and treatment with RDTs (ISTp) would be $155,294. Given the extraordinarily low prevalence of malaria in pregnancy, as well as pilot experience of testing in the ANC setting, there is a strong argument for adopting ISTp and dropping IPTp in Zanzibar.
To do so, the authors argue, thresholds of prevalence or incidence of malaria infection must be set in advance in order to trigger a reconsideration of the IPTp decision, and surveillance of malaria infection in pregnancy must be strengthened.
WHO has recently issued new guidance recommending continuation of IPTp where it is currently being practiced, making Zanzibar’s decision to maintain or discontinue IPTp of particular interest to the malaria in pregnancy community. Better guidance is needed on MIP services as countries move closer to malaria elimination.