IPTp &ITNs &Morbidity &Treatment Bill Brieger | 22 Jun 2016
Tanzania – Malaria Indicators Low, Still Need Work
Success in the war against malaria is not guaranteed. Two articles to that effect have appeared The Citizen of Dar es Salaam following presentation of findings from the most recent (2015-16) Tanzania Demographic and Health Survey (DHS)/Malaria Indicator Survey (MIS).
 On Tuesday (21 June 2016) the news story noted the increase in malaria prevalence among children below the age of 5 years, which was attributed to “the decline in the use of mosquito nets and low distribution of nets to households.” Then in a Wednesday (22 June 2016) Editorial, the paper noted that this “backtracking” is a “worrisome situation, for malaria is a problem that puts such a heavy burden on the government and the country’s economy.”
On Tuesday (21 June 2016) the news story noted the increase in malaria prevalence among children below the age of 5 years, which was attributed to “the decline in the use of mosquito nets and low distribution of nets to households.” Then in a Wednesday (22 June 2016) Editorial, the paper noted that this “backtracking” is a “worrisome situation, for malaria is a problem that puts such a heavy burden on the government and the country’s economy.”
 A look at the preliminary DHS does confirm the concerns about insecticide treated nets (ITNs). After nearly 10 years of progress, reported ITN availability in households declined. This was reflected in a drop in reported use by children below 5 years of age as well as pregnant women. It should be noted that targets set in 2000 in the Roll Back Malaria Abuja Declaration had been 80% by the year 2010, and those had almost been achieved in 2012, but the fall to around 50% in 2015-16 is discouraging.
A look at the preliminary DHS does confirm the concerns about insecticide treated nets (ITNs). After nearly 10 years of progress, reported ITN availability in households declined. This was reflected in a drop in reported use by children below 5 years of age as well as pregnant women. It should be noted that targets set in 2000 in the Roll Back Malaria Abuja Declaration had been 80% by the year 2010, and those had almost been achieved in 2012, but the fall to around 50% in 2015-16 is discouraging.
Another preventive measure has also faced difficulty. Pregnant women should receive doses of Sulfadoxine-pyrimethamine (SP) as part intermittent preventive treatment (IPT) during antenatal care (ANC). Until 2012 the recommendation was two contacts, but the World Health Organization has raised this to three or more depending on the number of times a woman attends ANC. So far IPT has not reached 40% or half of the Abuja target.
 This low IPT coverage is ironic since most women attend ANC at least once in Tanzania. At present only 68% of women who had been pregnant received the first dose of IPT even though 98% registered for ANC. Granted that some may have registered in their first trimester when they would not yet be eligible for IPT, but the gap is quite large and signals missed opportunities, which are often caused by stock-outs. Even though the proportion of women attending up to ANC visits could be better, these attendances should produce better delivery of the 3rd IPT dose.
This low IPT coverage is ironic since most women attend ANC at least once in Tanzania. At present only 68% of women who had been pregnant received the first dose of IPT even though 98% registered for ANC. Granted that some may have registered in their first trimester when they would not yet be eligible for IPT, but the gap is quite large and signals missed opportunities, which are often caused by stock-outs. Even though the proportion of women attending up to ANC visits could be better, these attendances should produce better delivery of the 3rd IPT dose.
 Malaria can also be controlled through prompt and appropriate treatment. While testing and treatment of children with appropriate artemisinin-based combination therapy (ACT) has increased, this are is still problematic. In particular, while WHO recommends that all cases of fever should be tested, less than a third received a test (rapid diagnostic test – RDT or microscopy). Testing helps distinguish malaria from other fevers, and ACTs should not be given unless malaria is confirmed. We can see that more ACTs are provided than the number who were tested, so treatment based solely on signs and symptoms is still the norm. Again there is need to explore the availability of both RDTs and ACTs as factors that have made these targets difficult to achieve.
Malaria can also be controlled through prompt and appropriate treatment. While testing and treatment of children with appropriate artemisinin-based combination therapy (ACT) has increased, this are is still problematic. In particular, while WHO recommends that all cases of fever should be tested, less than a third received a test (rapid diagnostic test – RDT or microscopy). Testing helps distinguish malaria from other fevers, and ACTs should not be given unless malaria is confirmed. We can see that more ACTs are provided than the number who were tested, so treatment based solely on signs and symptoms is still the norm. Again there is need to explore the availability of both RDTs and ACTs as factors that have made these targets difficult to achieve.
Tanzania continues to receive support from the Global Fund and the US President’s Malaria Initiative, among other partners. It is incumbent on all partners, global and national, to use these results as a wake up call to to plan for better delivery of malaria services and thus a reduction of both the economic and health burden of malaria in Tanzania.
IPTp &ITNs &Malaria in Pregnancy Bill Brieger | 21 Jun 2016
Kenya – the long road to controlling malaria in pregnancy
Augustine Ngindu, the Technical Advisor for Malaria in Kenya’s Maternal and Child Survival Program (USAID, Jhpiego) shares with us the steps and processes in building a national response to controlling malaria in pregnancy (MIP) in Kenya.
Recently Stephanie Dellicour and colleagues wrote about the challenges in the delivery of interventions to prevent malaria in pregnancy in Kenya in Malaria Journal. They examined MIP services in Nyanza Province of western Kenya between February and May 2010. At that time they found that, “… delivery of IPTp (intermittent preventive treatment in pregnancy) and ITNs (insecticide treated nets) through ANC (antenatal care) was ineffective and more so for higher-level facilities. This illustrates missed opportunities and provider level bottlenecks to the scale up and use of interventions to control malaria in pregnancy delivered through ANC.”
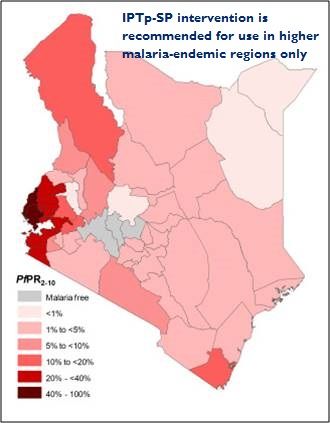
 Since that time the National Malaria Control Program (NMCP) has made efforts to address these problems by building on the national malaria strategy (NMS) 2009-2017 that recommend provision of IPTp only in high malaria transmission areas based on strong epidemiological evidence. In 2010 NMCP revised the national guidelines on diagnosis, treatment and prevention of malaria in line with the NMS 2009-2017. Then in 2011 NMCP in collaboration with Jhpiego developed simplified MIP guidelines on provision of IPTp in line with the national guidelines (each pregnant woman to receive at least 2 IPTp doses starting from 16 weeks of pregnancy at 4 weeks interval). Also in 2011 Maternal and Child health care workers in all 14 high malaria transmission areas were trained on provision of MIP using the simplified guidelines.
Since that time the National Malaria Control Program (NMCP) has made efforts to address these problems by building on the national malaria strategy (NMS) 2009-2017 that recommend provision of IPTp only in high malaria transmission areas based on strong epidemiological evidence. In 2010 NMCP revised the national guidelines on diagnosis, treatment and prevention of malaria in line with the NMS 2009-2017. Then in 2011 NMCP in collaboration with Jhpiego developed simplified MIP guidelines on provision of IPTp in line with the national guidelines (each pregnant woman to receive at least 2 IPTp doses starting from 16 weeks of pregnancy at 4 weeks interval). Also in 2011 Maternal and Child health care workers in all 14 high malaria transmission areas were trained on provision of MIP using the simplified guidelines.
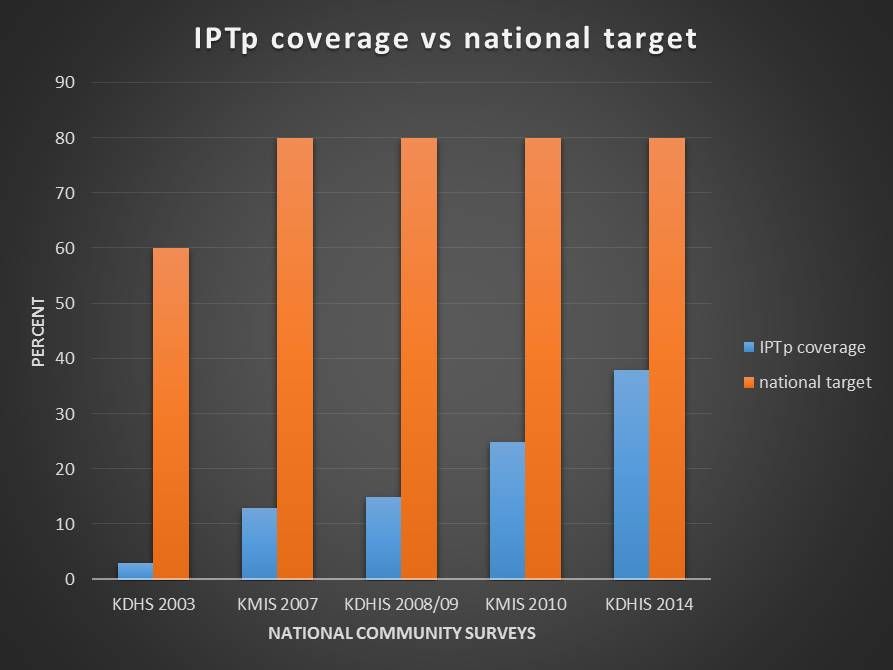
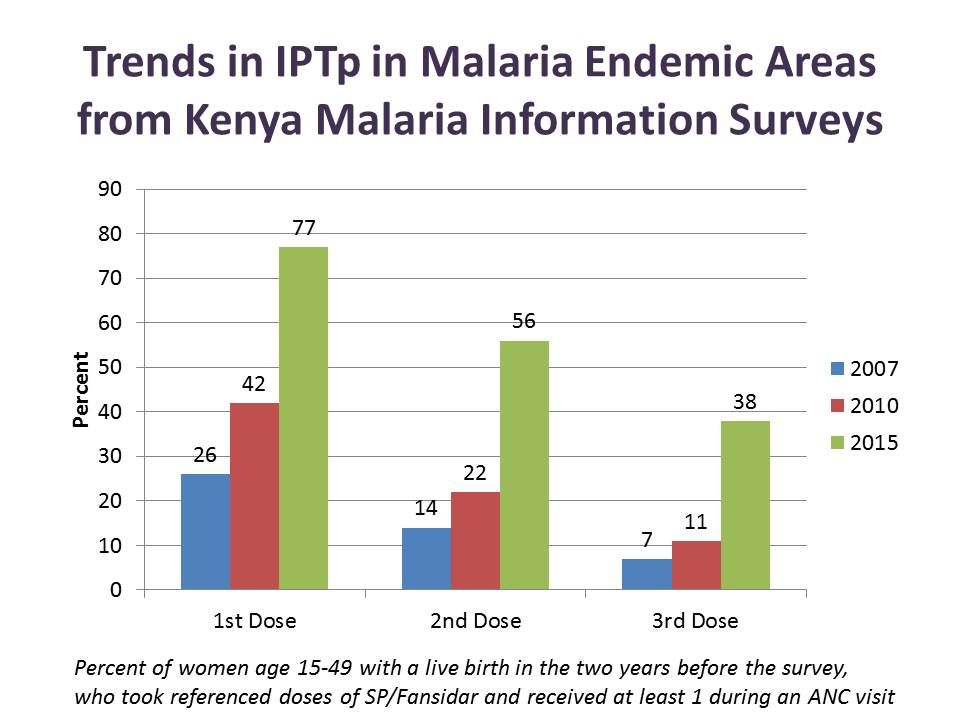 In 2012 health facility in-charges in the same high transmission areas were trained on MIP quality performance improvement. Then in 2013 promotion of early start of IPTp in the second trimester through sensitization of pregnant women was started in two out of the 14 malaria endemic counties. This resulted in increased IPTp2 coverage from 25% as reported in the kenya Malaria Indicator Survey) (KMIS 2010) to 63% (US-CDC survey 2013).
In 2012 health facility in-charges in the same high transmission areas were trained on MIP quality performance improvement. Then in 2013 promotion of early start of IPTp in the second trimester through sensitization of pregnant women was started in two out of the 14 malaria endemic counties. This resulted in increased IPTp2 coverage from 25% as reported in the kenya Malaria Indicator Survey) (KMIS 2010) to 63% (US-CDC survey 2013).
From 2014 to date the practice of sensitizing pregnant women using community health workers/volunteers has been replicated in other counties. IPTp2 coverage has increased from known 25% (KMIS 2010) to 56% (KMIS 2015) in the malaria endemic counties. Likewise use of ITNs by pregnant women increased from 50% in 2010 to 79% in 2015.
Although IPTp coverage is still below national target, the lost opportunities are being addressed. Kenya is still confronting multiple challenges including SP stock-out and devolution of health services to county governments but is set on making progress and saving mothers’ lives.
Communication &IPTp &ITNs &Treatment Bill Brieger | 04 Nov 2015
An Ideation Model: Attitudes, Beliefs and Practices Relevant to Malaria Prevention and Treatment in Madagascar and Liberia
Stella Babalola, Nan Lewicky, Grace Awantang, Michael Toso, Hannah Koenker, Arsene Ratsimbasoa, Monique Vololona of the Johns Hopkins Center for Communication Programs and the Division for Malaria Control, Madagascar Presented findings on how local perceptions help predict uptake of malaria interventions at the 143rd American Public Health Association Annual Meeting, October 31 – November 4, 2015, in Chicago. Their presentation on Liberia and Madagascar is summarized below.
While Liberia has an average malaria parasitemia prevalence of 28%, malaria is considerable less common in Madagascar and varies by region and altitude. This difference provides an interesting opportunity to observe similarities and contrasts in community perceptions of the disease.
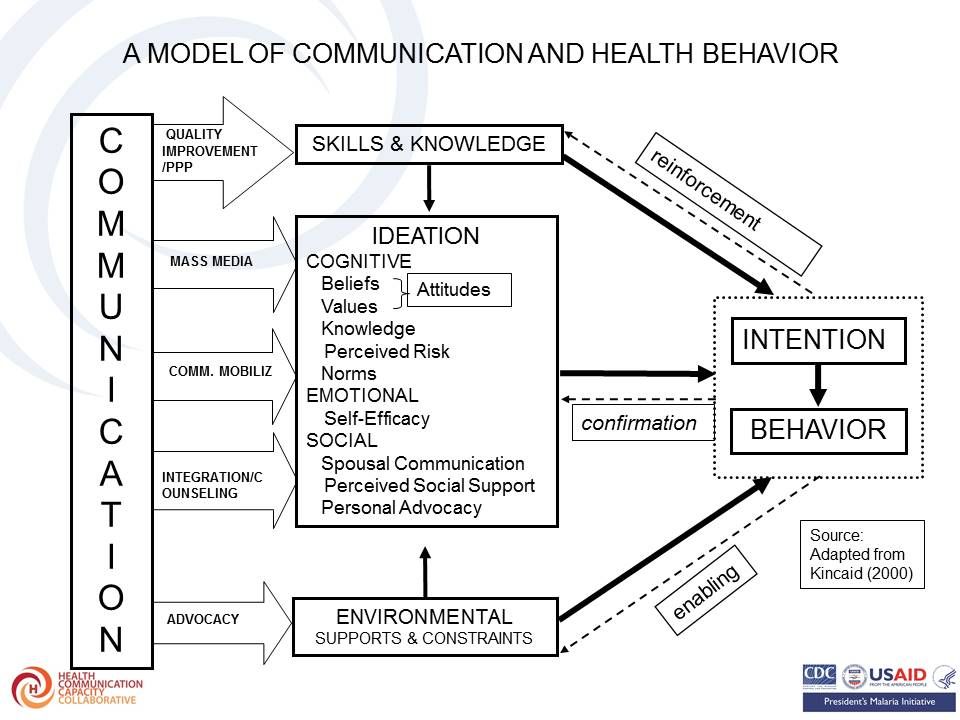 Theoretical basis of the research is based on the Ideation model which has been described as follows and as seen in the attached figures:
Theoretical basis of the research is based on the Ideation model which has been described as follows and as seen in the attached figures:
- “New ways of thinking and the diffusion of those ways of thinking by means of exposure to mass media and social interactions in local, culturally homogeneous communities” – Kincaid, 2000
- “views and ideas that people hold individually” – van de Kaa 1996
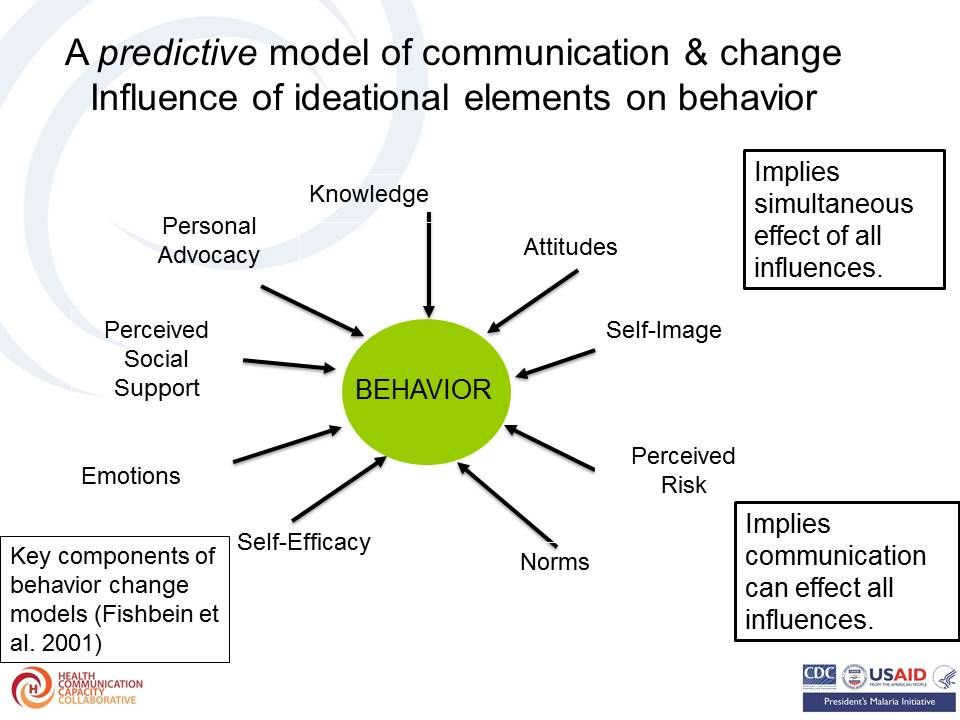 The ideation model has successfully predicted current use of a contraceptive method as well as accessing childhood immunization. The team took up the challenge to learn whether this model would be applicable to malaria interventions.
The ideation model has successfully predicted current use of a contraceptive method as well as accessing childhood immunization. The team took up the challenge to learn whether this model would be applicable to malaria interventions.
Malaria-related ideation was proposed to consist of: Malaria knowledge (cause, symptom, prevention); Perceived susceptibility to malaria; Perceived severity of malaria; Perceived self-efficacy to prevent malaria; and Social interactions about malaria. These may lead to uptake of malaria interventions.
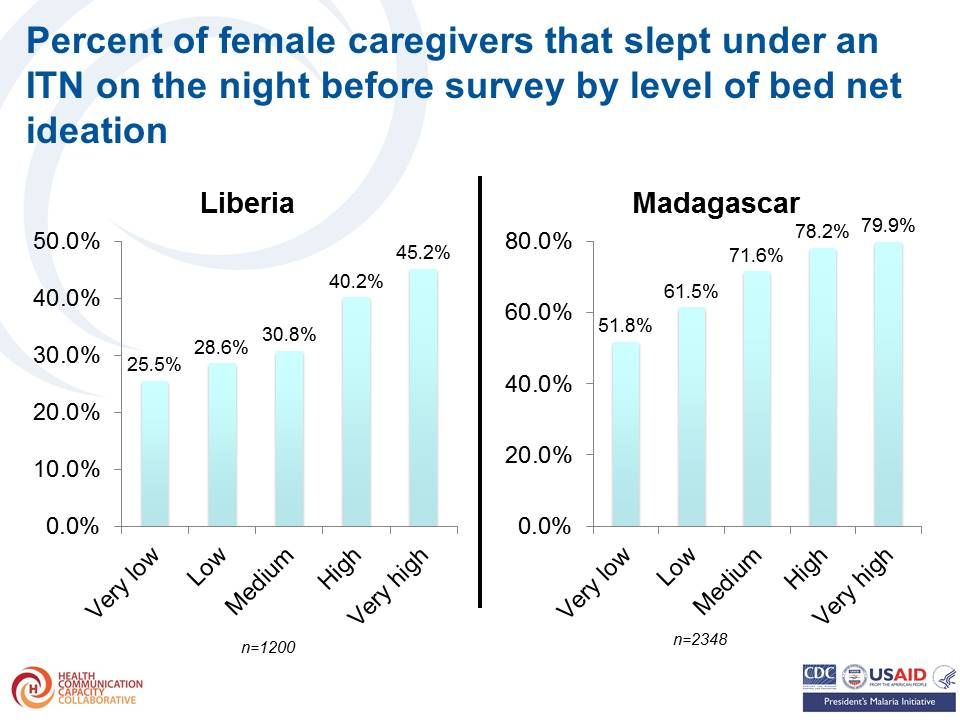
 Items for measuring bed net ideation could include – knowing where to procure a bed net, Willingness to pay for bed net, Having a positive attitudes towards bed net (derived from ten attitudinal statements), Perceived response-efficacy of bed nets, Perceived self-efficacy for procuring and using bed nets, Participation in household decisions about bed nets, Descriptive norm about bed net use and Social interactions about bed net use.
Items for measuring bed net ideation could include – knowing where to procure a bed net, Willingness to pay for bed net, Having a positive attitudes towards bed net (derived from ten attitudinal statements), Perceived response-efficacy of bed nets, Perceived self-efficacy for procuring and using bed nets, Participation in household decisions about bed nets, Descriptive norm about bed net use and Social interactions about bed net use.
Percent of female caregivers that slept under an ITN on the night before survey increased by level (score) of bed net ideation as seen in the graph. Results (odds ratio) of logistic regression of sleeping under an ITN on bed net ideation and other covariates showed a similar trend.
 Intermittent Preventive Treatment of Malaria in Pregnancy ideation measures included the following:
Intermittent Preventive Treatment of Malaria in Pregnancy ideation measures included the following:
- Knows name of the drug for malaria prevention during pregnancy
- Knows the timing of first dose of IPTp
- Has positive attitudes towards ANC and IPTp (derived from four attitudinal statements)
- Perceived response-efficacy of IPTp
- Woman participates in decisions about own health
- Social interactions about malaria and pregnancy
- Descriptive norm about ANC visits
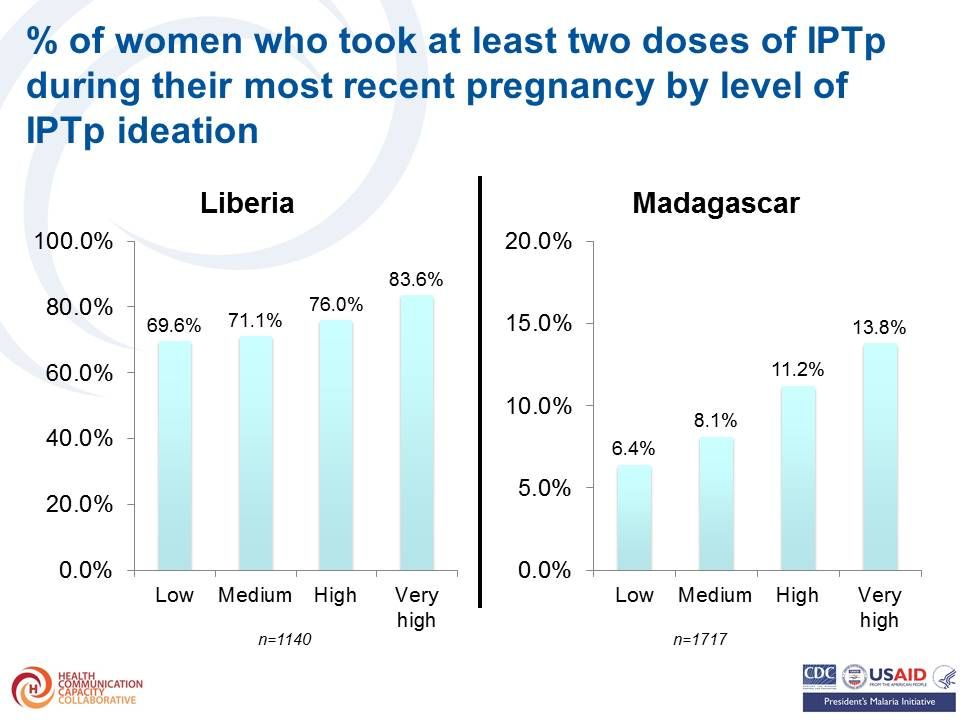 The percent of women who took at least two doses of IPTp during their most recent pregnancy also increased by level of IPTp ideation Likewise the results (odds ratio) of logistic regression of obtaining at least two doses of IPTp on IPTp ideation and other covariates were highest among those with highest levels of ideation.
The percent of women who took at least two doses of IPTp during their most recent pregnancy also increased by level of IPTp ideation Likewise the results (odds ratio) of logistic regression of obtaining at least two doses of IPTp on IPTp ideation and other covariates were highest among those with highest levels of ideation.
Items for measuring case management ideation included –
- Perceived response efficacy of malaria diagnostic test
- Perceived self-efficacy for detecting uncomplicated malaria
- Perceived self-efficacy for detecting severe malaria
- Descriptive norm about prompt treatment of malaria in children
- Social interactions about malaria treatment
- Participation in household decisions about child health
- Positive attitudes towards appropriate malaria treatment
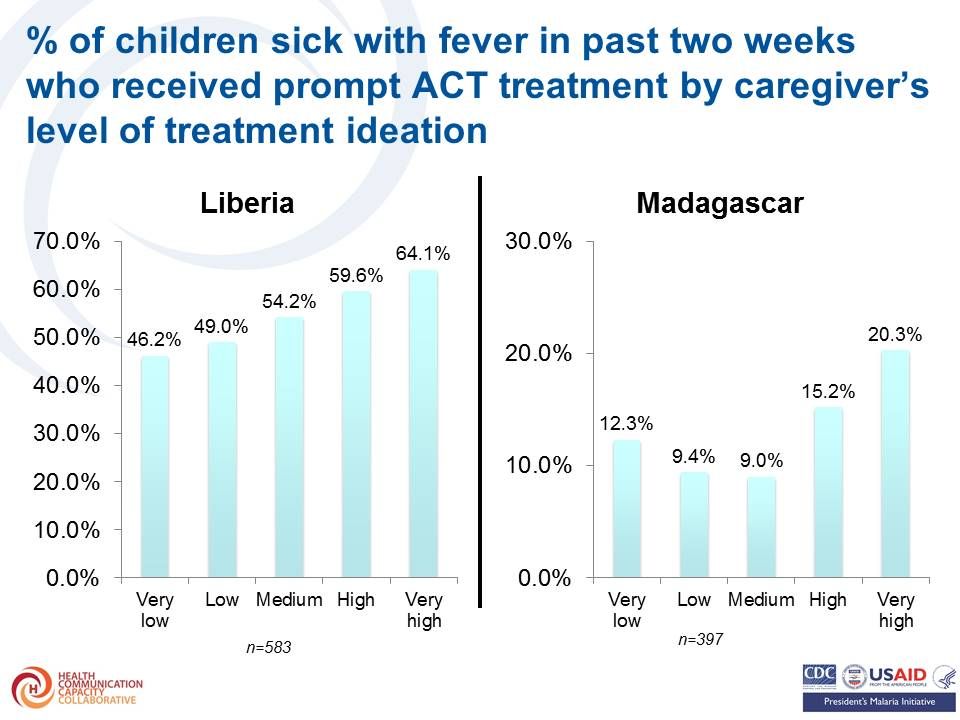 Again the percent of children sick with fever in past two weeks who received prompt ACT treatment by caregiver’s increased with increasing level of treatment ideation. As before the results (odds ratio) of logistic regression of prompt ACT treatment on caregiver’s treatment ideation and other covariates shows highest levels of ideation were associated with greated treatment seeking.
Again the percent of children sick with fever in past two weeks who received prompt ACT treatment by caregiver’s increased with increasing level of treatment ideation. As before the results (odds ratio) of logistic regression of prompt ACT treatment on caregiver’s treatment ideation and other covariates shows highest levels of ideation were associated with greated treatment seeking.
The team concluded that the same ideation model with demonstrated validity for family planning, child immunization, WASH and other health behaviors is relevant for malaria prevention and treatment. Strategically designed messages and interventions addressing ideational variables can help foster adoption of health-protective malaria prevention and treatment behaviors.
The authors acknowledge The US President’s Malaria Initiative (PMI) for technical guidance on the implementation of the surveys and The Ministry of Health and Social Welfare in Liberia and the Ministry of Health in Madagascar for their collaboration on the surveys.
Communication &IPTp &Malaria in Pregnancy Bill Brieger | 28 Oct 2015
Factors associated with the uptake of malaria prophylaxis during pregnancy among female caretakers in Madagascar
Grace N. Awantang, Stella O. Babalola, Hannah Koenker, and Nan Lewicky of the Johns Hopkins Bloomberg School of Public Health, Center for Communication Programs presented a poster today on IPTp uptake in Madagascar. Their Abstract follows:
 Intermittent preventive treatment of malaria in pregnancy (IPTp) is one of the key interventions promoted for combatting maternal mortality and malaria. In Madagascar, supply side factors such as SP availability and ANC attendance are barriers to practicing IPTp.
Intermittent preventive treatment of malaria in pregnancy (IPTp) is one of the key interventions promoted for combatting maternal mortality and malaria. In Madagascar, supply side factors such as SP availability and ANC attendance are barriers to practicing IPTp.
Less than one fifth of women (18.4%) at risk for malaria take the recommended two doses of sulfadoxine/pyrimethamine (SP) to prevent malaria during pregnancy whereas about half (49.7%) visit a health provider at least four times during pregnancy. Understanding the significant predictors of IPTp2 is crucial in order to inform interventions that can effectively promote this behavior.
Prior research has shown that both communication campaigns and individual cognitive, social and emotional factors, ideation, play a role in determining other health behaviors including malaria. We examined the correlates of IPTp2 using cross-sectional household survey data collected from female caretakers of children under five years of age.
 Caregiver recall of any anti-malaria messages during the past year was used to determine their exposure to health communication. Knowledge of IPTp, response-efficacy of IPTp, attitudes towards antenatal care (ANC), attitudes towards ANC, discussion of IPTp, and descriptive norm about ANC determined a person’s ideation score.
Caregiver recall of any anti-malaria messages during the past year was used to determine their exposure to health communication. Knowledge of IPTp, response-efficacy of IPTp, attitudes towards antenatal care (ANC), attitudes towards ANC, discussion of IPTp, and descriptive norm about ANC determined a person’s ideation score.
Of 1,589 female caretakers, over half (56.8%) were exposed to an anti-malarial message and a tenth (10.8%) mentioned SP as the drug used by pregnant women to prevent malaria. Message exposure, IPTp ideation and education level were all significant predictors of IPTp2 uptake in multivariate analysis.
Uptake was lowest among caretakers in the Highland transmission zone where transmission is unstable and highest in the Sub-desert transmission zone. Results suggest that both individual ideation and exposure to anti-malaria behavior change communication play a significant role in IPTp uptake among women in Madagascar.
The small portion of the variation in IPTp2 uptake explained by the measured covariates suggests that programmatic efforts should address supply-side factors that hinder access to ANC and preventive treatment of malaria during pregnancy.
IPTp &Malaria in Pregnancy Bill Brieger | 28 Oct 2015
“There is no free here, you have to pay” – IPTp in Mali
Colleagues[i] from the Johns Hopkins Bloomberg School of Public Health and the University of Sciences, Techniques, and Technologies of Bamako presented a poster today examining costs for obtaining IPTp at the American Society of Tropical Medicine 64th Annual Meeting. Their Abstract on actual and perceived costs as barriers to intermittent preventive treatment of malaria in pregnancy in Mali appears below.
 “There is no free here,” the words of a Malian husband, illustrate how perceptions of cost can deter uptake of intermittent preventive treatment of malaria in pregnancy (IPTp). Following WHO recommendations, the Malian Ministry of Health (MOH) recommends three doses of IPTp at monthly intervals. However, despite a national policy that IPTp be provided free of charge, only 35% of pregnant women receive at least one dose and less than 20% receive two or more doses.
“There is no free here,” the words of a Malian husband, illustrate how perceptions of cost can deter uptake of intermittent preventive treatment of malaria in pregnancy (IPTp). Following WHO recommendations, the Malian Ministry of Health (MOH) recommends three doses of IPTp at monthly intervals. However, despite a national policy that IPTp be provided free of charge, only 35% of pregnant women receive at least one dose and less than 20% receive two or more doses.
We explored perceptions and experiences of IPTp cost in Mali, and their impact on uptake, using qualitative interviews and focus groups with pregnant women, husbands and mothers-in-law. We also interviewed and observed health workers at four health centers two in Sikasso Region and two in Koulikoro.
 Despite national-level policies, actual IPTp costs varied widely at our study sites – between regions, facilities, and visits. Pregnant women may pay for IPTp, receive it free, or both at different times. Health centers often charge a lump sum for ANC visits that include both some free and some fee-based drugs and services. This makes it difficult for women and families to decipher which services are free and which require payments.
Despite national-level policies, actual IPTp costs varied widely at our study sites – between regions, facilities, and visits. Pregnant women may pay for IPTp, receive it free, or both at different times. Health centers often charge a lump sum for ANC visits that include both some free and some fee-based drugs and services. This makes it difficult for women and families to decipher which services are free and which require payments.
As a result, some forego even free care that, because it is not itemized, appears not to be free. Varying costs also complicate household budgeting for health care, particularly as women often rely on their husbands or husbands’ families for money.
While health facilities operating under the cost-recovery model strive to provide free IPTp, their own financial constraints often make this impossible. Preventing malaria in pregnancy depends upon women receiving the recommended doses of IPTp. However, it is clear that both actual and perceived costs are currently barriers to IPTp uptake.
Given the confusion around cost of services in the two study regions, more detailed national-level studies of both perceived and actual costs could help inform policy and program decisions promoting IPTp. These studies should evaluate both quantitatively and qualitatively the cost information provided by health facilities and pharmacies to pregnant women and their families.
[i] Emily A. Hurley, Namratha Rao, Meredith C. Klein, Hawa Diarra, Samba I. Diop, Seydou Doumbia, & Steven A. Harvey
IPTp &Malaria in Pregnancy Bill Brieger | 28 Oct 2015
Intermittent Preventive Treatment in Pregnancy: Increasing the Doses in Burkina Faso
 Colleagues[1] from the Jhpiego/USAID Burkina Faso Improving Malaria Care Program are presenting a poster at the American Society of Tropical Medicine 64th Annual Meeting Wednesday 28 October 2015. Visit Poster 1655. In the meantime review the abstract below.
Colleagues[1] from the Jhpiego/USAID Burkina Faso Improving Malaria Care Program are presenting a poster at the American Society of Tropical Medicine 64th Annual Meeting Wednesday 28 October 2015. Visit Poster 1655. In the meantime review the abstract below.
In Burkina Faso, Antenatal Care (ANC) is a national platform for malaria in pregnancy prevention and control. The 2010 Demographic and Health Survey showed a good initial ANC registration rate (95%), but over 56% of pregnant women in rural areas do not register until their second or third trimester. Thus they may have missed the full regimen of ANC services including Long Lasting Insecticide-treated nets and intermittent preventive treatment of malaria in pregnancy (IPTp). In 2010 only 10.6% of pregnant women nationally and 8.4% in rural areas received two doses of IPTp.
 The USAID-supported Improving Malaria Care (IMC) project in Burkina Faso has been providing technical assistance and training to health districts and their ANC staff on implementing updated (2012) WHO IPTp guidelines. The recommended provision of IPTp at every ANC visit from the 13th week of pregnancy onward leads to the possibility of 3 or more doses per woman. The new guidance was incorporated into the update of Burkina Faso’s malaria strategy and has been disseminated since September 2014.
The USAID-supported Improving Malaria Care (IMC) project in Burkina Faso has been providing technical assistance and training to health districts and their ANC staff on implementing updated (2012) WHO IPTp guidelines. The recommended provision of IPTp at every ANC visit from the 13th week of pregnancy onward leads to the possibility of 3 or more doses per woman. The new guidance was incorporated into the update of Burkina Faso’s malaria strategy and has been disseminated since September 2014.
Annual data from the Health Management and information System for 2014 from three districts (Batie, Po and Ouargaye) and 61 health clinics where IMC has been working were collected and summarized. A total of 26,909 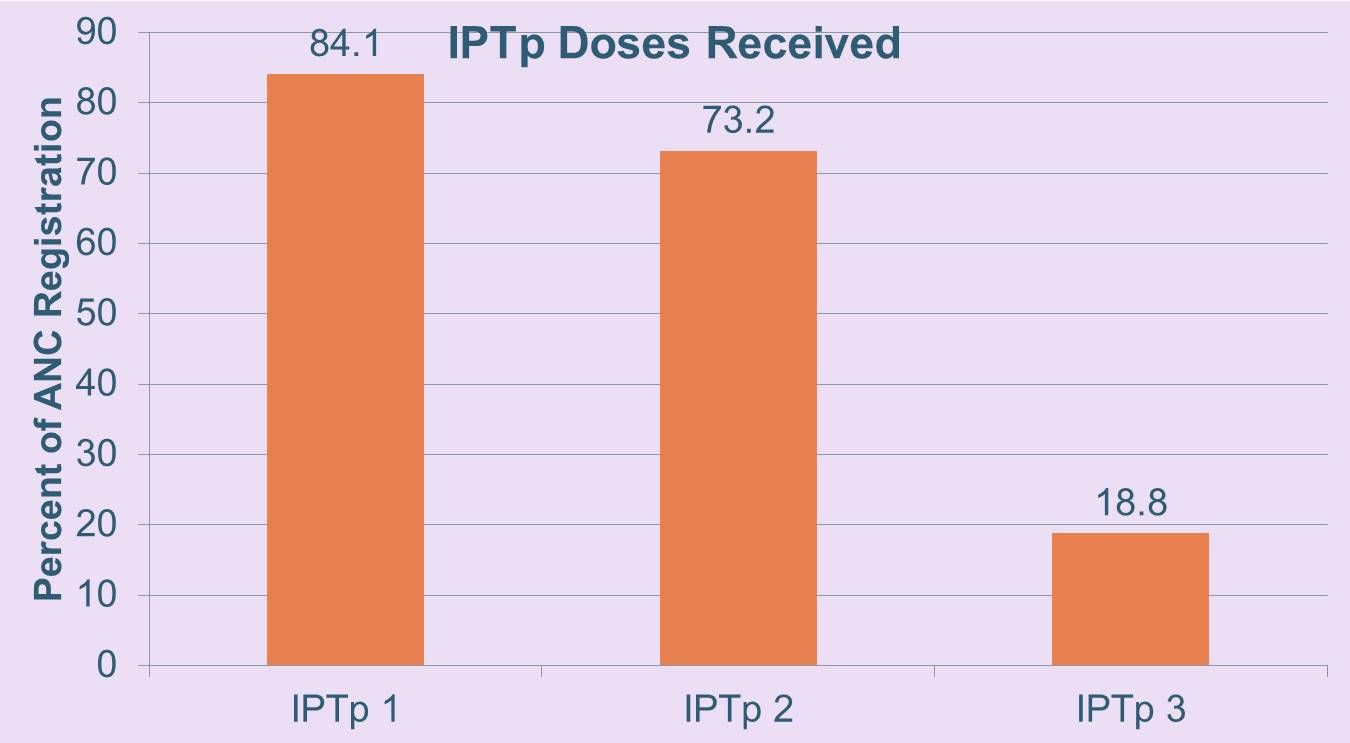 women registered for ANC. Of these 89.7%, 73.2% and 39.8% attended ANC twice, three and four times respectively. Of those registered 84.1%, 73.2% and 18.8% received IPTp once, twice and thrice. Eleven (17.7%) had not started the updated IPTp guidance. The Ministry of Health also experienced stock-outs of sulfadoxine-pyrimethamine.
women registered for ANC. Of these 89.7%, 73.2% and 39.8% attended ANC twice, three and four times respectively. Of those registered 84.1%, 73.2% and 18.8% received IPTp once, twice and thrice. Eleven (17.7%) had not started the updated IPTp guidance. The Ministry of Health also experienced stock-outs of sulfadoxine-pyrimethamine.
Based on this slow implementation and uptake of IPTp3+, the IMC project in collaboration with the National Malaria Control Program is examining ways to strengthen antenatal malaria prevention including capacity building for ANC staff and community IPTp provision.
[1] Ousman Badolo, Stanislas P. Nebie, Mathurin Dodo, Thierry Ouedraogo, Rachel Waxman, William R. Brieger
Elimination &IPTp &ITNs Bill Brieger | 27 Oct 2015
Winning the fight against malaria in Huambo Province, Angola
Colleagues[1] from the Ministry of Health, Huambo, Angola and Jhpiego are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Tuesday 27th October 2015. Please stop by Poster LB-5246 and discuss the results as presented in the Abstract below.
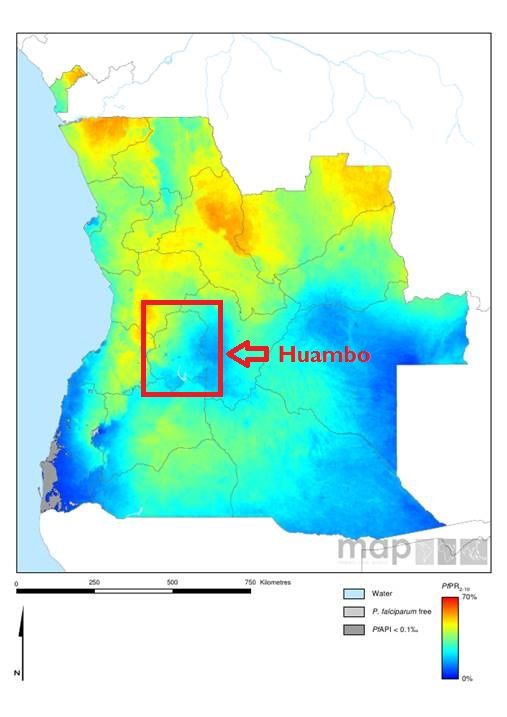 Huambo is on of Angola’s 18 provinces, with close to 2 million inhabitants. Traditionally malaria has accounted for a large portion of clinic consultations, hospitalizations, and child and maternal mortality. Angola has three epidemiological strata: hyper-endemic area (north), meso-endemic stable area (central area), where Huambo is located, and meso-endemic unstable area (south).
Huambo is on of Angola’s 18 provinces, with close to 2 million inhabitants. Traditionally malaria has accounted for a large portion of clinic consultations, hospitalizations, and child and maternal mortality. Angola has three epidemiological strata: hyper-endemic area (north), meso-endemic stable area (central area), where Huambo is located, and meso-endemic unstable area (south).
The main malaria vector is Anopheles gambiae (ss, melas and arabiensis) and Anopheles funestus. Parasitological studies show 85% of cases are P falciparum and 15% are P vivax.
The Huambo Provincial Health Directorate has been working with stakeholders including national and international NGOs, traditional leaders, churches, religious leaders, police, army and media to fight malaria. This collaboration is showing results.
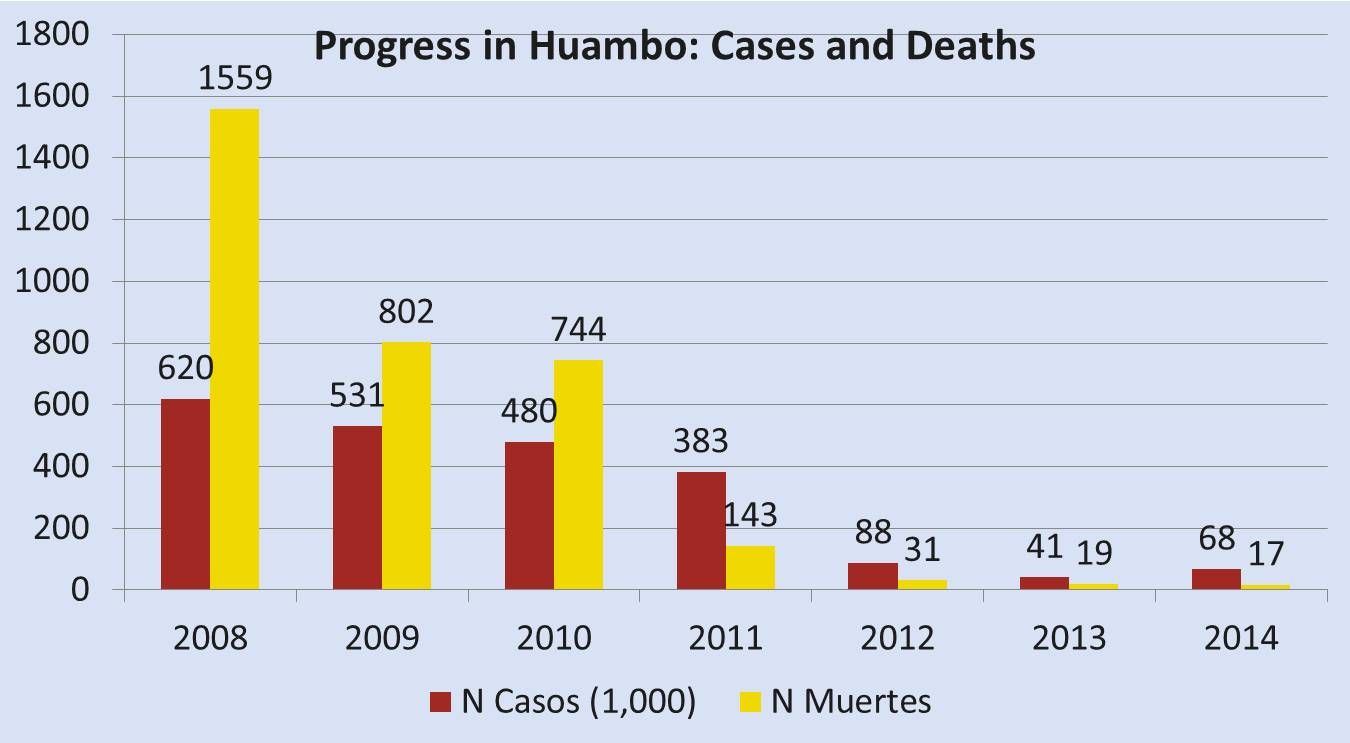 Cases have dropped steadily from 620,300 in 2008 to 68,547 in 2014. Likewise deaths have declined from 1,559 to 17 in the same period. During this period there has been an increase in training and supervision of health professionals to improve their malaria prevention, diagnosis and treatment skills.
Cases have dropped steadily from 620,300 in 2008 to 68,547 in 2014. Likewise deaths have declined from 1,559 to 17 in the same period. During this period there has been an increase in training and supervision of health professionals to improve their malaria prevention, diagnosis and treatment skills.
Rapid diagnostic tests have been deployed to all health units. Work with community organizations has resulted in health fairs (Uhayele Vimbo) in more remote locations. Over the most recent 5-year period the number of antenatal care clients receiving two doses of IPTp with SP has increased from 10,938 to 68,183 or from 30% to 54%.
Finally 330,000 ITNs were distributed between 2010 and 2014. The Province and its organizational and community partners are committed to sustaining these achievements in order to further reduce malaria morbidity and mortality.
[1] João Carlos F. Juliana, Jhony Juarez, Clementino Sacanombo, William R. Brieger
Advocacy &IPTp &Malaria in Pregnancy Bill Brieger | 26 Oct 2015
Health systems strengthening: Advocacy facilitates availability of sulfadoxine-pyrimethamine for prevention of malaria in pregnancy in Kenya
Colleagues[1] from Jhpiego’s Kenya office and the Ministry of Health are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Tuesday 27th October 2015. Please stop by Poster LB-5225 and discuss the results as presented in the Abstract below.
 In malaria endemic areas, infection with malaria during pregnancy is often associated with poor pregnancy outcomes. Although effective intervention measures are available including use of sulfadoxine pyrimethamine (SP) for intermittent preventive treatment of malaria in pregnancy (IPTp) coverage rates have remained low.
In malaria endemic areas, infection with malaria during pregnancy is often associated with poor pregnancy outcomes. Although effective intervention measures are available including use of sulfadoxine pyrimethamine (SP) for intermittent preventive treatment of malaria in pregnancy (IPTp) coverage rates have remained low.
In Kenya, IPTp2 is at 38% in malaria endemic counties some of the key factors influencing IPTp uptake being SP stock-outs. The national government has been supplying SP but on devolution of health services to county governments it became the responsibility of the counties. There are many competing financial demands at county level and SP stock out is frequent.
 In February 2015 the national government disseminated a memo to county governments advising them to procure SP to avert the worsening SP stock out situation. After issuance of the memo, USAID’S flagship Maternal and Child Survival Program (MCSP) held discussions with the County Directors of Health (CDHs) and shared the quantification formula for SP requirement for the respective counties.
In February 2015 the national government disseminated a memo to county governments advising them to procure SP to avert the worsening SP stock out situation. After issuance of the memo, USAID’S flagship Maternal and Child Survival Program (MCSP) held discussions with the County Directors of Health (CDHs) and shared the quantification formula for SP requirement for the respective counties.
MCSP advocated for procurement of SP especially during the peak malaria transmission period May-August 2015. The CDHs on realizing the cost was not high made immediate arrangements for procurement of SP.
Bungoma County procured enough SP tablets to cover the peak malaria transmission season and distributed them to the health facilities. Results on analysed ANC data from facilities showed that the number of pregnant women accessing IPTp had reduced from 7,845 in October 2014 to 3,856 in February 2015.
 One month after procurement and distribution of SP, the number accessing SP increased from 3,856 to 6,769. To improve pregnancy outcomes in malaria endemic areas it is vital to reduce the effects of malaria during pregnancy. Use of IPTp-SP during pregnancy has been shown to improve pregnancy outcomes however, coverage rates of the intervention have remained below the national target due to several influencing factors like the SP stock-out situation experienced in Kenya.
One month after procurement and distribution of SP, the number accessing SP increased from 3,856 to 6,769. To improve pregnancy outcomes in malaria endemic areas it is vital to reduce the effects of malaria during pregnancy. Use of IPTp-SP during pregnancy has been shown to improve pregnancy outcomes however, coverage rates of the intervention have remained below the national target due to several influencing factors like the SP stock-out situation experienced in Kenya.
The use of advocacy with relevant authorities in Bungoma County leading to improvement in the SP stock out situation is considered a best practice in ensuring health commodity security and is being replicated in other malaria endemic counties.
[1] Augustine M. Ngindu, Gathari G. Ndirangu, Wekesa Kubasu, Isaac M. Malonza
Human Resources &IPTp &Training Bill Brieger | 26 Oct 2015
Improving provision of malaria services through provider training in Burkina Faso
Colleagues[1] from Jhpiego’s Burkina Faso Improving Malaria Care USAID-supported project and the Johns Hopkins Bloomberg School of public Health are presenting a poster at the 64th ASTMH Annual Meeting in Philadelphia at noon on Tuesday 27th October 2015. Please stop by Poster 969 and discuss the results as presented in the Abstract below.
 In 2013, malaria was the main reason for consultation (53.90%), hospitalization (63.20%) and death (49.60%) in health facilities; children under 5 and pregnant women are most affected. Recent revisions to the World Health Organization’s (WHO) guidance to maintain effective approaches to defeating malaria, include monthly dosing of intermittent preventive treatment for pregnant women (IPTp), starting from the 13th week of gestation.
In 2013, malaria was the main reason for consultation (53.90%), hospitalization (63.20%) and death (49.60%) in health facilities; children under 5 and pregnant women are most affected. Recent revisions to the World Health Organization’s (WHO) guidance to maintain effective approaches to defeating malaria, include monthly dosing of intermittent preventive treatment for pregnant women (IPTp), starting from the 13th week of gestation.
To align with the latest WHO guidance, the Burkina Faso Ministry of Health, with support from the USAID-funded Improving Malaria Care (IMC) project, revised national malaria guidelines in March 2014. 68 trainers from 9 health regions were trained on the revised national malaria guidelines.
From June to September 2014, 744 providers from 524 health facilities in 21 districts (33%) were trained on the prevention and management of malaria cases. To ensure updated guidance reaches all health workers, the training included a module on how to update colleagues in their respective facilities.
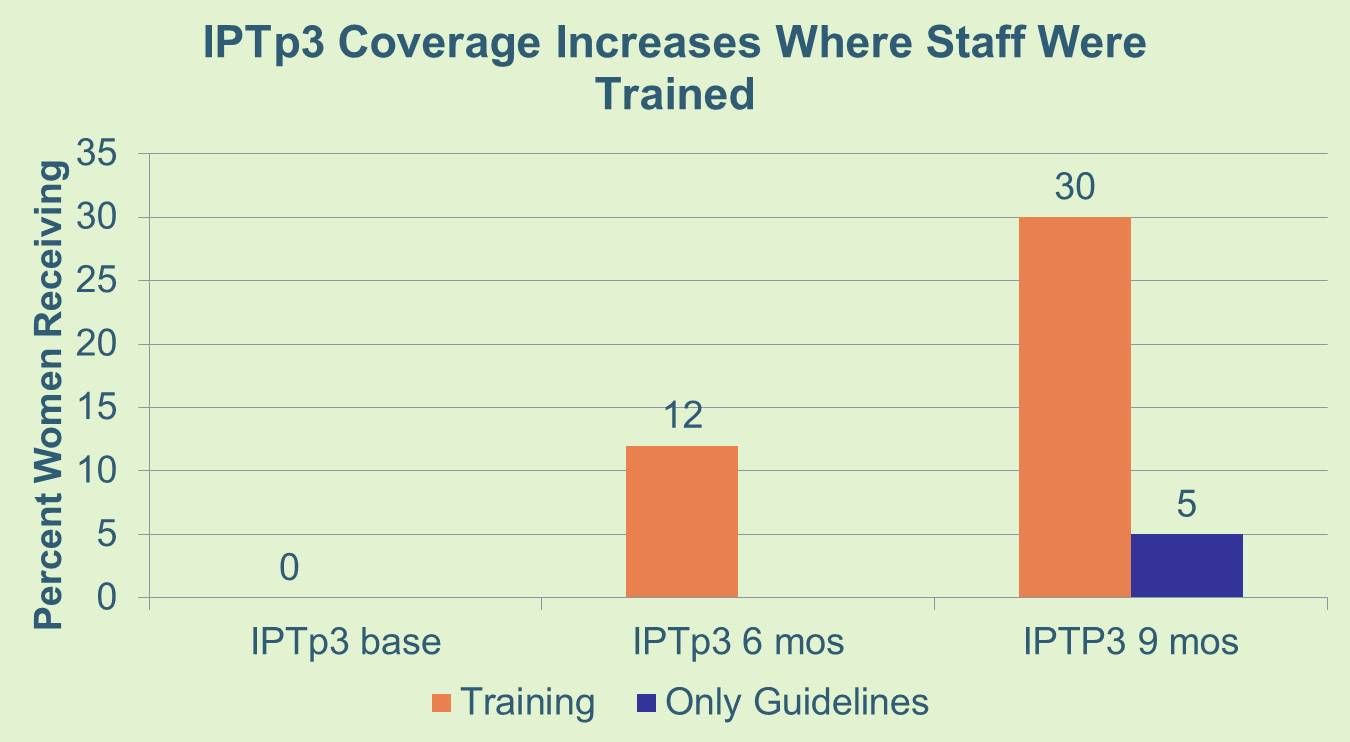 During supervision visits, most trained providers were using the new guidelines and pregnant women are increasingly receiving the third and higher doses of SP before delivery. In the first six months after the training sessions, pregnant women, who received the third dose of SP (IPTp3) increased from 0% to 12%. Three months later, that proportion rose to 30%. Comparatively, in the remaining 42 districts who received only the copies of the new guideline without training, IPTp3 was 5% nine months after receiving the guidelines.
During supervision visits, most trained providers were using the new guidelines and pregnant women are increasingly receiving the third and higher doses of SP before delivery. In the first six months after the training sessions, pregnant women, who received the third dose of SP (IPTp3) increased from 0% to 12%. Three months later, that proportion rose to 30%. Comparatively, in the remaining 42 districts who received only the copies of the new guideline without training, IPTp3 was 5% nine months after receiving the guidelines.
The training sessions contributed to improving the implementation of revised IPTp guidelines and uptake of IPTp 3 and higher better than distribution of the new guidelines alone. As a result the IMC project will scale-up the training in Year 2 to 600 more providers from 464 health facilities, and other partners have also agreed to support the National Malaria Control Program to reach remaining facilities. Challenges in increasing IPTp uptake include commodity distribution and inadequate engagement of private health facilities to update their practices and reporting of SP distribution.
[1] Ousman Badolo, Stanislas Nebie, Moumouni Bonkoungou, Mathurin Dodo, Thierry Ouedraogo, Rachel Waxman, William R. Brieger
Elimination &IPTp &ITNs Bill Brieger | 25 Oct 2015
Jhpiego Malaria Activities Featured in Posters at ASTMH Annual Meeting
 Today marks the start of the 64th annual meeting of the American Society of Tropical Medicine and Hygiene from 25-29 October 2015 in Philadelphia. Please stop by the poster sessions Monday, Tuesday and Wednesday to see a sampling of Jhpiego’s malaria programs. We are featuring Angola, Nigeria, Burkina Faso, Tanzania, Kenya and Rwanda. You can also discuss with Jhpiego staff at Booth #100 in the Exhibition Hall.
Today marks the start of the 64th annual meeting of the American Society of Tropical Medicine and Hygiene from 25-29 October 2015 in Philadelphia. Please stop by the poster sessions Monday, Tuesday and Wednesday to see a sampling of Jhpiego’s malaria programs. We are featuring Angola, Nigeria, Burkina Faso, Tanzania, Kenya and Rwanda. You can also discuss with Jhpiego staff at Booth #100 in the Exhibition Hall.
Poster Session A Monday 26 October 2015![]()
- LB-5094 – Readiness for Malaria Elimination: Using HMIS data to Map Malaria Test Positivity in Huambo Province, Angola – João Carlos F. Juliana1, William R. Brieger2, Jhony Juarez3, Connie Lee3, Clementino Sacanombo1 – 1Ministry of Health, Huambo, Angola, 2The Johns Hopkins University, Baltimore, MD, United States, 3Jhpiego, The Johns Hopkins University, Baltimore, MD, United States.
- 385 – Health Systems Strengthening: Improving quality of services for prevention of malaria in pregnancy through the Standards-Based Management and Reward approach in Kenya – Augustine M. Ngindu1, Gathari Ndirangu2, Sanyu N. Kigondu2, Isaac M. Malonza3 – 1USAID-MCSP, Kisumu, Kenya, 2USAID-MCSP, Nairobi, Kenya, 3Jhpiego Kenya, Nairobi, Kenya
Poster Session B Tuesday 27 October 2015
- 969 – Improving provision of malaria services through provider training in Burkina Faso – Ousman Badolo1, Stanislas Nebie1, Moumouni Bonkoungou1, Mathurin Dodo1, Thierry Ouedraogo1, Rachel Waxman1, William R. Brieger2 – 1Jhpiego, Baltimore, MD, United States, 2Johns Hopkins University, Baltimore, MD, United States
- 680 – Institutionalization of Quality of Care in Health Facilities Improves Management of Malaria in Pregnancy in Tanzania – Jasmine W. Chadewa, Rita Mutayoba – Jhpiego, Dar es Salaam, Tanzania, United Republic of Tanzania
- LB-5224 – Health systems strengthening – Advocacy facilitates availability of sulfadoxine pyrimethamine for prevention of malaria in pregnancy in Kenya – Augustine M. Ngindu1, Gathari G. Ndirangu2, Wekesa Kubasu3, Isaac M. Malonza4 – 1USAID-MCSP, Kisumu, Kenya, 2USAID-MCSP, Nairobi, Kenya, 3MOH, Bungoma, Kenya, 4Jhpiego,, Nairobi, Kenya Poster
- LB-5246 – Winning the fight against malaria in Huambo Province, Angola – João Carlos F. Juliana1, Jhony Juarez2, Clementino Sacanombo1, William R. Brieger3 – 1Ministry of Health, Huambo, Angola, 2Jhpiego, The Johns Hopkins University, Baltimore, MD, United States, 3The Johns Hopkins University, Baltimore, MD, United States
Symposium #83 Organized by Jhpiego, RBM Malaria in Pregnancy Working Group – Prioritizing Malaria in Pregnancy as Malaria Transmission Declines – Tuesday, October 27, 2015 1:45 – 3:30 PM
Poster Session C Wednesday 28 October 2015
- 1655 – Intermittent Preventive Treatment in Pregnancy: Increasing the Doses in Burkina Faso – Ousman Badolo1, Stanislas P. Nebie1, Mathurin Dodo1, Thierry Ouedraogo1, Rachel Waxman1, William R. Brieger2 – 1Jhpiego, Baltimore, MD, United States, 2Johns Hopkins University, Baltimore, MD, United States
- 1330 – Use of community health volunteers to increase coverage for integrated community case management in Bondo, Kenya – Savitha Subramanian1, Mark Kabue2, Dyness Kasungami1, Makeba Shiroya-Wadambwa3, Dan James Otieno4, Charles Waka3 – 1John Snow, Inc., Rosslyn, VA, United States, 2Jhpiego, Baltimore, MD, United States, 3Jhpiego, Nairobi, Kenya, 4John Snow, Inc., Nairobi, Kenya
- 1657 – LLIN distribution campaign processes: Lessons learned and challenges from Akwa Ibom State, Nigeria – John Orok1, Bright Orji2, Enobong Ndekhedehe2, William R. Brieger3 – 1Ministry of Health, Akwa Ibom State, Uyo, Nigeria, 2Jhpiego, Baltimore, MD, United States, 3Johns Hopkins University, Baltimore, MD, United States
- 1656 – Use of Long Lasting Insecticide-Treated Bednets in Akwa Ibom State Nigeria after a Major Distribution Campaign – Enobong U. Ndekhedehe1, John Orok2, Bright C. Orji1, William R. Brieger3 – 1Jhpiego, Baltimore, MD, United States, 2Ministry of Health, Akwa Ibom State, Nigeria, Uyo, Nigeria, 3Johns Hopkins University, Baltimore, MD, United States