IPTp &ITNs &Malaria in Pregnancy Bill Brieger | 21 Jun 2016 04:34 pm
Kenya – the long road to controlling malaria in pregnancy
Augustine Ngindu, the Technical Advisor for Malaria in Kenya’s Maternal and Child Survival Program (USAID, Jhpiego) shares with us the steps and processes in building a national response to controlling malaria in pregnancy (MIP) in Kenya.
Recently Stephanie Dellicour and colleagues wrote about the challenges in the delivery of interventions to prevent malaria in pregnancy in Kenya in Malaria Journal. They examined MIP services in Nyanza Province of western Kenya between February and May 2010. At that time they found that, “… delivery of IPTp (intermittent preventive treatment in pregnancy) and ITNs (insecticide treated nets) through ANC (antenatal care) was ineffective and more so for higher-level facilities. This illustrates missed opportunities and provider level bottlenecks to the scale up and use of interventions to control malaria in pregnancy delivered through ANC.”
 Since that time the National Malaria Control Program (NMCP) has made efforts to address these problems by building on the national malaria strategy (NMS) 2009-2017 that recommend provision of IPTp only in high malaria transmission areas based on strong epidemiological evidence. In 2010 NMCP revised the national guidelines on diagnosis, treatment and prevention of malaria in line with the NMS 2009-2017. Then in 2011 NMCP in collaboration with Jhpiego developed simplified MIP guidelines on provision of IPTp in line with the national guidelines (each pregnant woman to receive at least 2 IPTp doses starting from 16 weeks of pregnancy at 4 weeks interval). Also in 2011 Maternal and Child health care workers in all 14 high malaria transmission areas were trained on provision of MIP using the simplified guidelines.
Since that time the National Malaria Control Program (NMCP) has made efforts to address these problems by building on the national malaria strategy (NMS) 2009-2017 that recommend provision of IPTp only in high malaria transmission areas based on strong epidemiological evidence. In 2010 NMCP revised the national guidelines on diagnosis, treatment and prevention of malaria in line with the NMS 2009-2017. Then in 2011 NMCP in collaboration with Jhpiego developed simplified MIP guidelines on provision of IPTp in line with the national guidelines (each pregnant woman to receive at least 2 IPTp doses starting from 16 weeks of pregnancy at 4 weeks interval). Also in 2011 Maternal and Child health care workers in all 14 high malaria transmission areas were trained on provision of MIP using the simplified guidelines.
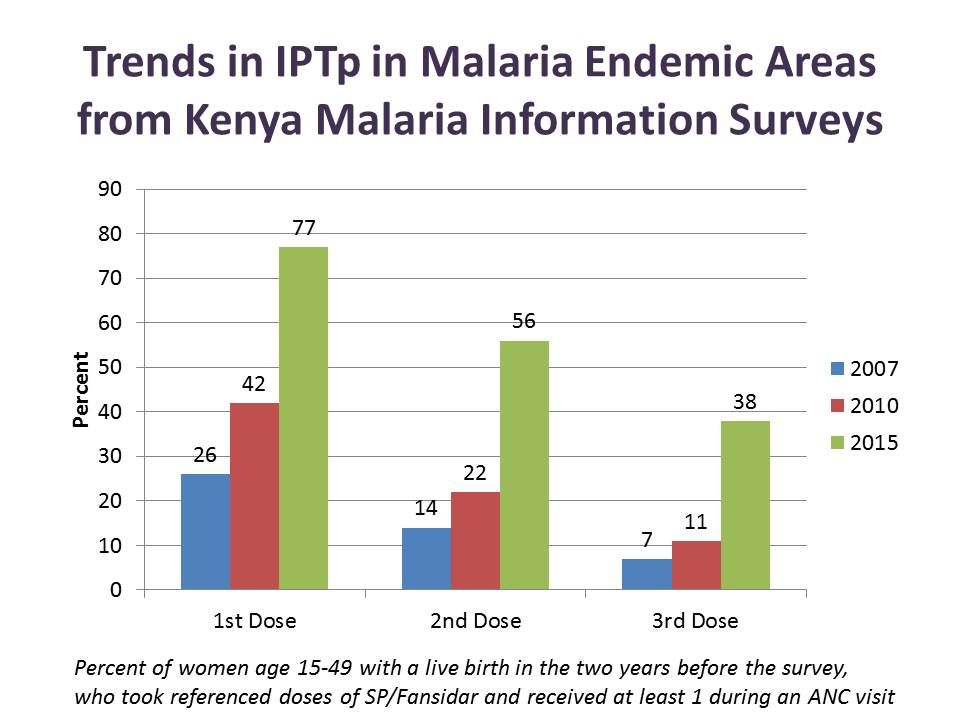 In 2012 health facility in-charges in the same high transmission areas were trained on MIP quality performance improvement. Then in 2013 promotion of early start of IPTp in the second trimester through sensitization of pregnant women was started in two out of the 14 malaria endemic counties. This resulted in increased IPTp2 coverage from 25% as reported in the kenya Malaria Indicator Survey) (KMIS 2010) to 63% (US-CDC survey 2013).
In 2012 health facility in-charges in the same high transmission areas were trained on MIP quality performance improvement. Then in 2013 promotion of early start of IPTp in the second trimester through sensitization of pregnant women was started in two out of the 14 malaria endemic counties. This resulted in increased IPTp2 coverage from 25% as reported in the kenya Malaria Indicator Survey) (KMIS 2010) to 63% (US-CDC survey 2013).
From 2014 to date the practice of sensitizing pregnant women using community health workers/volunteers has been replicated in other counties. IPTp2 coverage has increased from known 25% (KMIS 2010) to 56% (KMIS 2015) in the malaria endemic counties. Likewise use of ITNs by pregnant women increased from 50% in 2010 to 79% in 2015.
Although IPTp coverage is still below national target, the lost opportunities are being addressed. Kenya is still confronting multiple challenges including SP stock-out and devolution of health services to county governments but is set on making progress and saving mothers’ lives.